
Abstract
Bioengineering strategies have demonstrated enormous potential to treat female infertility as a result of chemotherapy, uterine injuries, fallopian tube occlusion, massive intrauterine adhesions, congenital uterine malformations, and hysterectomy. These strategies can be classified into two broad categories as follows: (i) Transplantation of fresh or cryopreserved organs into the host and (ii) tissue engineering approaches that utilize a combination of cells, growth factors, and biomaterials that leverages the body's inherent ability to regenerate/repair reproductive organs. While whole organ transplant has demonstrated success, the source of the organ and the immunogenic effects of allografts remain challenging. Even though tissue engineering strategies can avoid these issues, their feasibilities of creating whole organ constructs are yet to be demonstrated. In this article we summarize the recent advancements in the applications of bioengineering to treat female infertility.
Introduction
A
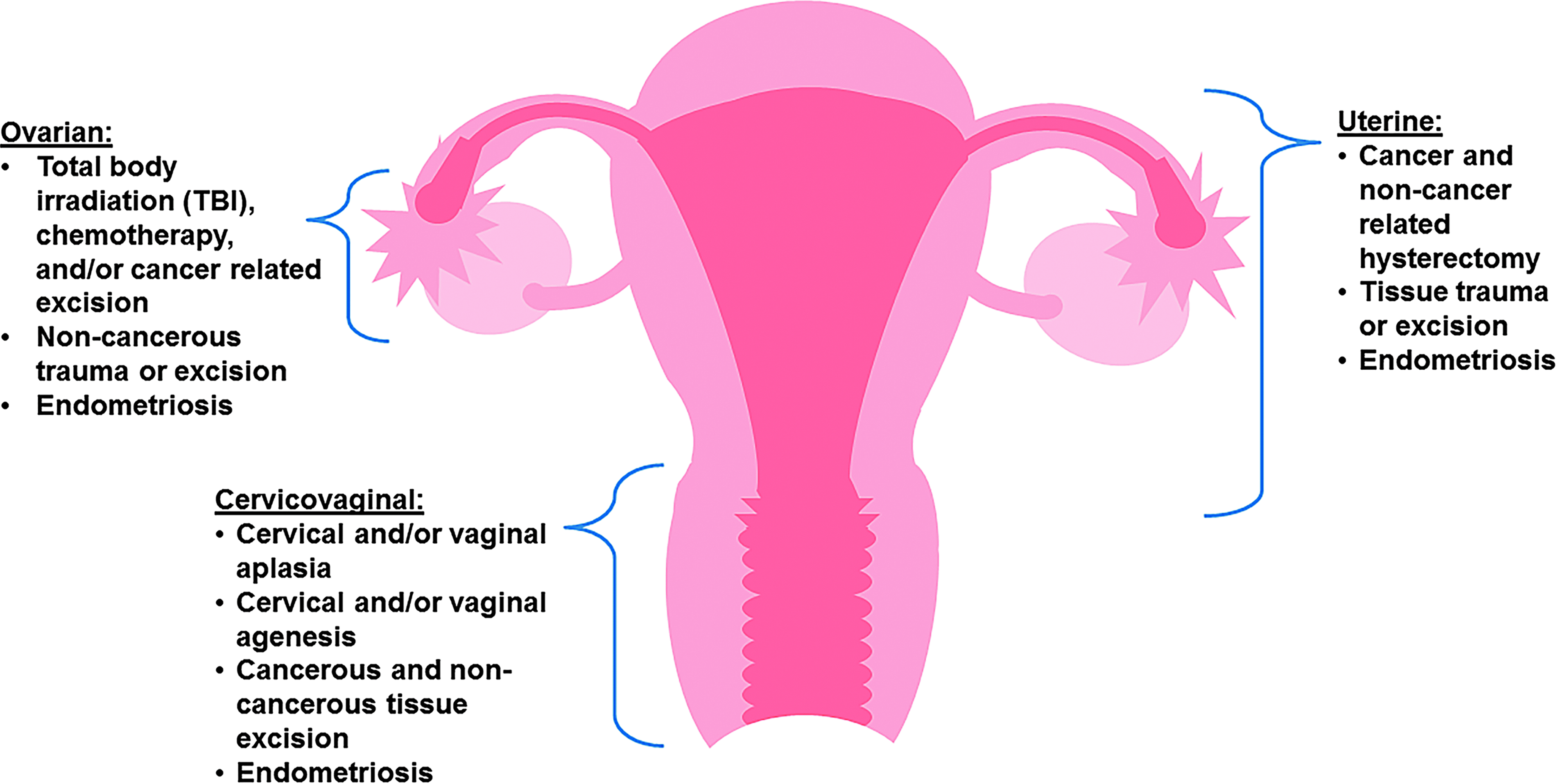
The female reproductive system and their contributions to female infertility. Cancer and its associated treatments are the major cause of female infertility as they often involve the removal of the entire organ. Other causes of female infertility include traumatic injuries and congenital defects that cause irreversible structural damage.
Therefore, significant amount of efforts is devoted to develop bioengineering approaches to restore fertility, which can generally be classified into two broad categories as follows: (i) Transplantation of fresh or cryopreserved organs transplanted into the host (Fig. 2); and (ii) tissue engineering approaches that utilize a combination of cells, growth factors, and biomaterials that leverages the body's inherent ability to regenerate/repair reproductive organs (Fig. 3). Tissue engineering often utilizes a variety of different cell types, which include (i) tissue specific stem cells; (ii) mesenchymal stem cells (MSCs); and (iii) pluripotent stem cells such as embryonic stem cells.
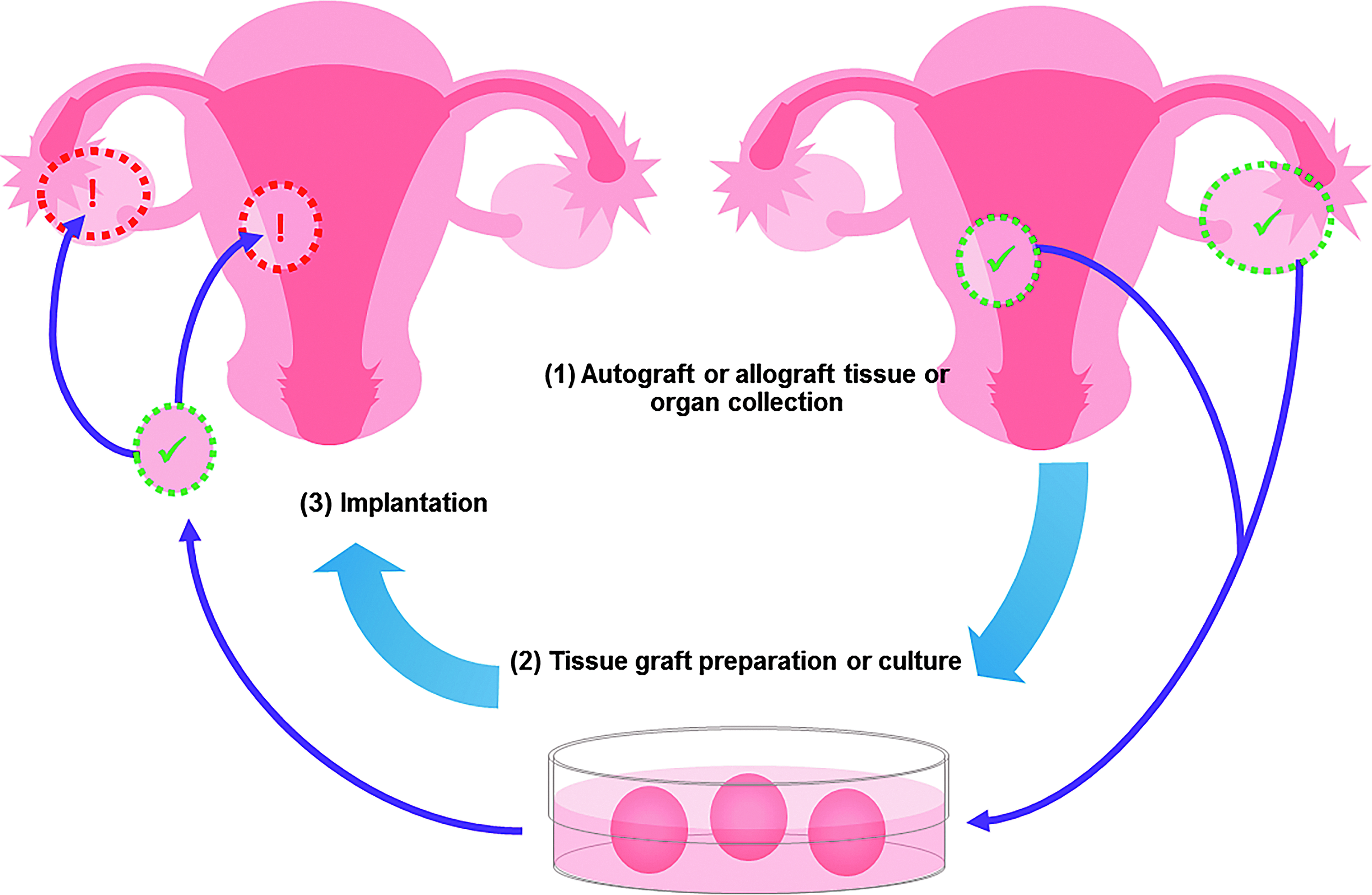
A schematic of using tissue/organ transplant based on autograft or allograft. First, healthy donor tissue or whole organs are explanted (1) and prepared, which may include static or dynamic culture conditions to apply additional biochemical/mechanical stimulus and/or to recellularize the organ/tissue (2). The processed organ/tissue is then used in repairing, reconstructing, or replacing host tissue or organs through surgical implantation (3).
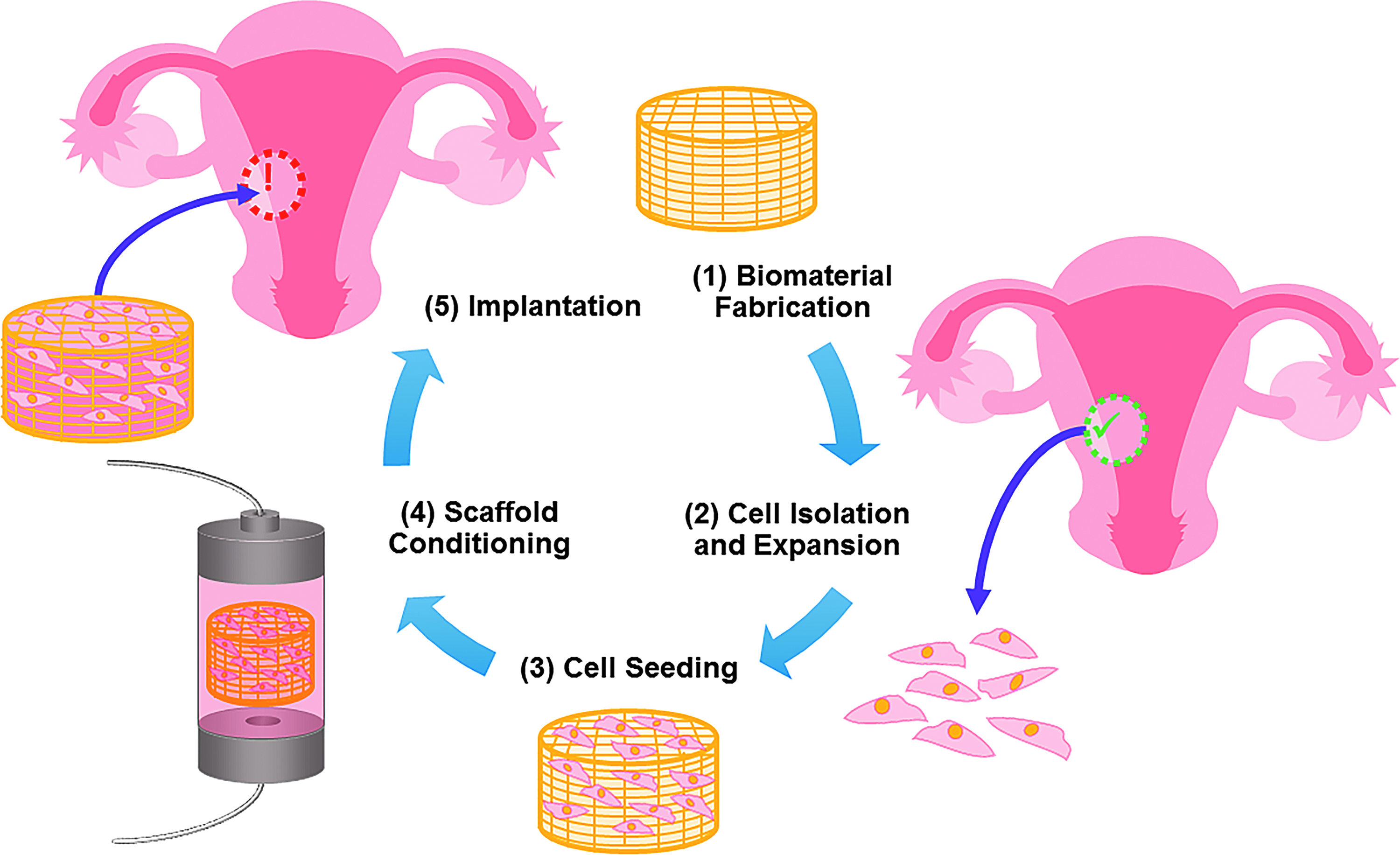
The fabrication of tissue engineered grafts for female reproductive organ repair involving biomaterials, cells, and/or biochemical signals. A typical process involves a biomaterial scaffold that is either molded or three-dimensionally printed (1). This scaffold then acts as a carrier that may be loaded with appropriate cell populations (e.g., stem cells or endometrial cells) or bioactive molecules (e.g., epidermal growth factors, vascular endothelial growth factors) (2, 3). The scaffolding loaded with appropriate cells and biochemical signals is then subject to further preconditioning in a bioreactor to apply additional mechanical/biochemical signals, if needed, (4) which is then surgically implanted (5).
Fresh and cryopreserved organ/tissue transplant is often preferred because they retain the integrity of the extracellular matrix (ECM) structure and the complex cellularity that exist in the natural tissue. The source of tissues/organs can either be allogeneic or autologous. Autologous sources are often preferred as they avoid immune rejections and the significant negative effect of immunosuppressive drugs, but autologous organs/tissues' harvest is often difficult to perform. Due to the limited availability of autologous and allogeneic sources, many researchers have turned to decellularized tissues/organs. Some of the most popular decellularized tissue matrices used in female reproductive organ regeneration are porcine small intestinal submucosa (SIS), peritoneum, and amniotic membrane. While decellularization preserves the architecture of the ECM and minimizes the effect of immune rejections, the use of decellularization agents can disrupt the ultrastructure of the decellularized organ, and residual cellular components not removed during processing (e.g., nucleic acid material) can have untoward effects on the host. In addition, preservation of the exact composition of ECM is difficult to characterize, and the residual cellular materials remain a continued concern. Therefore, to allow better control over the composition of biological implants, many researchers have turned to purified natural (e.g., collagen, gelatin, and alginate) or synthetic (e.g., polyethylene-glycol and polypropylene-fumarate) biomaterials.
Many investigators have used natural biomaterials because they inherently support cell adhesion, migration, proliferation, and differentiation. However, the composition of the natural biomaterial must be characterized and there is often significant batch-to-batch variability. Synthetic biomaterials, on the other hand, are well defined and can be fabricated with modifications to molecular structure to enhance biocompatibility. Nevertheless synthetic biomaterials have major disadvantages, including a structure and composition that can only mimic native tissues/organs and a decreased capacity to induce cellular and tissue remodeling.
In addition, cell source remains a critical challenge in regenerating female reproductive organs. Specifically, a tissue biopsy may not yield sufficient number of normal cells for expansion and transplantation. In other instances, the cells of interest may not be expanded in vitro. Therefore, other investigators explored the possibility of using stem cells as an alternative cell source. Stem cells, with the majority of the work done in syngeneic models, can be obtained from discarded human embryos (human embryonic stem cells [hESCs]), fetal tissue, adult sources (bone marrow, fat, and skin), or may be molecularly induced from differentiated cells (induced pluripotent stem cells). The goal of this review is to present an overview and the most recent advancements in the applications of bioengineering to reestablish female fertility by structural restoration and the associated functions.
Uterus
Uterine factor infertility, which affects 3–5% of the general population, can arise from congenital abnormalities or acquired causes such as hysterectomy due to malignant or benign tumor or intrauterine adhesions.3,4,8 Adoption and/or gestational surrogacy are currently the only options for having children in these patients. 8 Current bioengineering approaches for uterine tissue restoration can be broadly classified into uterine transplant and tissue engineered constructs for partial uterine regeneration, which are summarized in Table 1.
N/A, not applicable.
Uterus tissue transplant
The first human trial of whole uterus transplant was performed in 2000 on a female (age 26) who, after a postpartum hemorrhage, lost her uterus 6 years earlier. 9 The donor was a 46-year-old patient with multiloculated ovarian cysts who underwent a hysterectomy modified to preserve tissue and vascular integrity. 9 The transplanted uterus responded well to combined estrogen–progesterone therapy, but developed acute vascular thrombosis 99 days after transplantation and hysterectomy became necessary. 9 Therefore, it was evident that further preclinical studies are necessary to demonstrate the establishment and maintenance of revascularization, as well as successful pregnancy of the transplanted uterus.
Since achieving adequate blood supply for the transplanted uterus is essential to clinical success, there have been significant amount of efforts invested in developing different surgical techniques to improve perfusion and viability of uterine autografts.10–13 Although these studies only used an autotransplant model and did not test the function/fertility of the uterus, the authors demonstrated surgical techniques and procedures that resulted in successfully perfused uterine tissue with decent viability. In addition to demonstrating uterine perfusion, other studies have shown successful implantation and pregnancy in autotransplanted uterus and that the offspring are healthy and fertile.14–16 Based on these results surrounding autotransplantation, another research group moved forward with an allogenic uterus transplantation study. 17 After uterine transplantation, with vascular anastomoses unilateral to the internal iliac artery and the external iliac vein, the uterus recipients received two different immunosuppressive treatments as follows: (i) monotherapy with tacrolimus and (ii) standard triple therapy. 17 All the recipients and the donors survived the surgery with recipients presenting rejection to some extent within the first few weeks following uterine transplant. The authors did not conclude which immunosuppressive treatments had better clinical outcomes or if immunosuppressive drugs caused any uterine damage. 17
Overall, these findings suggest that allogeneic uterine transplant in primate species is feasible and that fresh uterus transplant is capable of restoring female fertility. However, there have not been successful term pregnancies in primates to date. Based on these results, there have been 12 human uterus transplantation attempts worldwide but with only one study, performed by Brannstrom et al. in 2013, result in live birth. 18 In this study, the male baby that was delivered prematurely (31 weeks and 5 days) with preeclampsia with body weight was normal for the gestational age. 18 Nevertheless this provides a proof-of-concept for the procedure of whole uterine transplant. While issues surrounding immunogenic effects and availability of allogenic tissues remain, uterine transplant is currently the only viable option for whole uterus regeneration. Impact of the medications needed for immunosuppression on the developing fetus will also need continuing evaluation.
Acellular tissue engineering approaches for partial uterus repair
In an effort to overcome immunogenic and organ availability issues surrounding fresh organ transplant, many investigators have developed tissue engineered constructs for partial uterus repair. Decellularized ECM biomaterials are widely used in these endeavors. ECM based constructs benefit from native tissue protein presence and arrangement, which serve to enhance cell adhesion and migration. For example, Miyazaki and Maruyama aimed to partially regenerate and reconstruct the rat uterus through recellularization of decellularized uterine matrix. 19 The rat uteri were decellularized by perfusing detergents through the aorta. 19 Efficient in vitro recellularization was achieved by reseeding of the decellularized uterus, resulting in a reconstitution of an endometrium-like tissue. 19 This procedure was capable of partially regenerating structurally and functionally competent uterine tissues when placed onto partially excised uterus in rats. 19
Moreover, Young et al. created a neo-myometrial tissue patch fabricated from culturing isolated myocytes into decellularized rat and human myometrial scaffolds that could be placed over a uterine defect before pregnancy to enhance structural support and reduce the risk of uterine rupture. 20 The author successfully developed xeno-neo-myometrial grafts that expressed coordinated contractions, which can also serve as a model to study myometrial contractility. 20 These results are very promising for the use of decellularized ECM for uterine regeneration. However, one of the major disadvantages of using decellularized tissue matrices, as previously mentioned, is the risk of residual cellular materials (e.g., DNA, cells, and antigens), which could trigger significant immune response of the host, which were not considered in these studies.21–23
Collagen scaffolds in combination with growth factors have also been investigated as a biomaterial for uterine tissue engineering due to their abundance, biocompatibility, and biodegradability. In one case, a collagen-based basic fibroblast growth factor (bFGF) targeting delivery system was created by fusing a collagen-binding domain (CBD) to the N-terminal of native bFGF (NAT). 24 Overall, the collagen/CB-bFGF group led to higher endometrium thickness with higher alpha-smooth muscle actin positive areas, more collagen remodeling, neovascularization, and cellularization, 24 and the collagen scaffold was completely degraded and replaced by endometrial cells and muscle fibers. Embryos were found in grafted and normal tissue only in the collagen/CBD-bFGF group and having comparable size to those implanted in the normal tissue. 24
Using a similar approach, collagen-binding vascular endothelial growth factor (CB-VEGF) was also explored as a potential growth factor for uterine repair, where collagen and CB-VEGF were directly injected into the injury site. 25 In vivo results showed that the CB-VEGF group resulted in a greater thickness of uterine wall regenerated, increased presence of glands, presence of smooth muscle cells, and observed vascular growth. 25 In terms of fertility, embryos were implanted both in the normal and scar tissue areas of rats in the CB-VEGF group, and the pregnancy rate at scar sites in the CB-VEGF group was higher than in the NAT-VEGF group and the phosphate buffered saline (PBS) group. 25 These results are encouraging for restoration of fertility in mammals, but in vivo testing in larger animal models would serve to further minimize the translational distance for these therapies. However, while useful for patch-type applications for partial uterine wall regeneration for implantation, these approaches cannot be used to perform whole uterine regeneration.
Cell-laden tissue engineering approaches for partial uterus repair
To enhance the regenerative capacity of tissue engineered scaffolds, cell-laden tissue engineered constructs were also explored as a treatment option for uterine regeneration. For instance, collagen membranes seeded with bone marrow-derived mesenchymal stem cells (BM-MSCs) were evaluated for their healing capability for severe uterine injury. 26 Compared with cell-free scaffolds and untreated controls, the collagen/BM-MSC system increased proliferative abilities of uterine endometrial and muscular cells, facilitated microvasculature regeneration, and restored the ability of the endometrium to receive the embryo and support its development to a viable stage. 26
Endometrium-like cells were generated from the hESCs and were encapsulated within a collagen scaffold to repair uterine damage using rat model of uterine full-thickness injury. 27 Twelve weeks after transplantation, the authors discovered that the hESC-derived cells could survive and recover the structure and function of uterine horns in a rat model of severe uterine damage. 27 The pregnancy rate of the cells/collagen group (80%) was comparable to that of the sham-operated group (100%) and higher compared to the collagen only group (33%) and the untreated group (26.7%). 27 Cell-laden tissue engineered constructs have clearly demonstrated superior regenerative capability over scaffold-only approaches. However, the immunogenic effect and the source of cells need to be considered before clinical translation as autologous cells are typically difficult to obtain.
Cell-based bioengineering approaches for partial uterine repair
To ensure that the matrix implanted to promote tissue regeneration is biomimetic, some investigators chose to construct a tissue engineered therapy using a cell-only scaffold-free approach. For example, Lu et al. aimed to construct uterine tissue containing a smooth muscle cell layer, an epithelial cell layer, and an endometrial layer. 28 The engineered uterine tissues (EUTs) were generated by first seeding epithelial cells on top of the constructed stromal layer over the smooth muscle layer. 28 Then the author mixed the rabbit epithelial cell and stromal cells in collagen/Matrigel to form an endometrial layer and seeded this on top of the rabbit smooth muscle layer. 28 The constructed EUTs had three layers, including the epithelial layer, stromal layer, and smooth muscle layer, which supported development of fertilized eggs up to blastulas. 28
Moreover, another research group demonstrated an endometrium tissue engineering approach using a scaffold-free, cell sheet engineering strategy based on primary endometrial cells isolated from immature mice and rats. 29 After 3 days of culture of the mouse endometrial cells, culture temperature was lowered to induce the detachment of endometrial cells. 29 After detaching from the dish, an endometrial cell sheet was allowed to shrink significantly by cytoskeletal reorganization, recultured for 3 days to construct a thicker endometrial cell sheet, and then harvested. 29 Cell sheets were transplanted onto exteriorized muscle using a supporting plate. In vitro results demonstrated that the recultured endometrial cell sheets showed an endometrium-specific hormonal response to estrogen and progesterone, demonstrating that the endometrial cell sheets were found to maintain uterine function in culture. 29 These cell-only, scaffold-free approaches have shown promise, but their efficacy in supporting the growth of fertilized eggs is yet to be tested against other tissue engineered approaches in animal models.
Overall, bioengineering approaches based on fresh whole uterus transplant have demonstrated success in restoring infertility using animal models. This approach is preferred as the majority of the cells, growth factors, and the ultrastructure is intact, which have proven difficult to replicate. However, most of the studies are performed using syngeneic organ transplant models, which limit clinical translation because autotransplantation of uterus is unlikely to occur in a clinical setting. Allotransplant, on the other hand, is more likely to take place in a clinical setting and this concept has been proven by Brannstrom et al. 18 where the first live birth after uterus transplantation was demonstrated. However, issues associated with immune rejection, organ source, and ethical issues need to be addressed for allotransplantation for this procedure to be widely used in the clinic. Due to these limitations, many investigators have turned to tissue engineering approaches using cells, growth factors, and biomaterials.
Tissue engineering approaches have advantages over tissue transplant because cell and material sourcing are less of an issue compared to auto- and allograft sourcing. Using animal models, tissue engineering approaches demonstrated partial regeneration of the uterine wall and supported pregnancy and produced fertile offspring. However, current fabrication approaches used in tissue engineering face the difficulties of recreating organ ultrastructure and scaling-up for feasible use in whole uterus regeneration. We expect that these issues will be gradually resolved with the development of more advanced biofabrication approaches such as three-dimensional (3D) bioprinting. 30
Ovary
Primary ovary deficiency is a leading cause of female infertility that affects one in every 10,000 women before the age of 20, one in every 1000 women before 30, and one in 100 women before 40.31,32 Potential causes include radiotherapy and/or chemotherapy, environmental factors, viral infections, metabolic and autoimmune diseases, and genetic alterations.3,4,32 These patients are not able to produce normal levels of hormones or to release oocytes. Current bioengineering approaches to restore ovarian function can be broadly classified as ovarian tissue transplant, tissue engineered ovarian scaffold, and ovarian culture system, as well as cell based therapy (Table 2).
ECM, extracellular matrix; DMSO, dimethyl sulfoxide; FSH, follicle-stimulating hormone.
Ovarian follicles and tissue transplant
Transplantation of cryopreserved ovarian follicles has been a standard clinical practice for decades, with demonstrated clinical success. Likewise, ovarian preservation is presently a vital practice for pediatric cancer patients who have chemotherapy and/or pelvic radiotherapy. This typically involves the transplant of autologous ovaries to areas outside the radiation beam or maintained ex vivo until completion of chemotherapy, when they are returned to the donor. This treatment utilizes autologous ovaries so there are no issues related to rejection or need for immunosuppression. Recently researchers have shown, for the first time, recovered fertility after total body irradiation in addition to chemotherapy.33,34 In addition, Silber et al. reported a single series of both fresh and cryopreserved ovarian transplants from one center and demonstrated the success of allogeneic and autologous ovarian transplantation. 35 Moreover, Laronda et al. demonstrated the feasibility of using decellularized ovary transplants by creating a decellularized ovarian scaffold, recellularized it, and transplanted it to successfully initiate puberty in mice. 36 However, the authors did not show viable offspring, which is essential for this strategy to be used for human transplants.
The strategies presented in this section based on ovarian tissue transplant have displayed excellent clinical outcome, but they are not suitable for ovarian cancer due to the high risk for reintroducing the tumor from carcinogenic material that may still exist in the ovarian tissue.5,32,36,37 Therefore, significant efforts have been invested in developing tissue engineered ovarian tissues and in vitro oocyte culture systems for in vivo implantation.
Tissue engineered ovarian scaffold and ovarian culture system
To avoid reintroducing the disease, researchers have developed tissue engineered oocyte maturation systems to activate oocytes isolated from cryopreserved ovarian tissues. In 2003, Pangas et al. developed a 3D in vitro culture system based on alginate beads for the growth and the development of individual granulosa cell–oocyte complexes (GOCs). 38 Ovaries from 12-day-old female mice were dissected. GOCs were collected and encapsulated in alginate beads. Granulosa cells proliferated and oocytes grew in volume in alginate beads with spatial arrangement of GOCs. 38 The 3D alginate culture system could yield far more oocytes than conventional IVF, as the majority of mammalian oocytes are contained in immature and quiescent follicles. 38 Moreover, Xu et al. isolated immature follicles from prepubescent, 16-day-old female mice. 39 Single follicles were pipetted into the middle of each alginate droplet and cross-linked in calcium chloride. 39 After 8 days of culture, IVF and embryo transfer were performed. The embryos derived from cultured oocytes fertilized in vitro and transferred to pseudopregnant female mice were viable, and both male and female offspring were fertile. 39
The potential of agarose gels, another polysaccharide-based biomaterial that is widely used in tissue engineering, for in vitro maturation of oocytes was investigated. 40 The authors created a 3D artificial human ovary to mature human oocytes by utilizing the three follicular cell types—theca, granulosa, and oocytes. 40 The results presenting maturation of early antral follicle (<10 mm) oocytes into metaphase II oocytes represented the first success in using 3D tissue engineering principles for in vitro oocyte maturation. 40 However, these approaches using polysaccharide biomaterials alone lack ECM proteins that are essential to the phenotypes of mammalian cells. 30
As such, other studies utilizing biomaterials which incorporate ECM components such as RGD, collagen (type I and IV), and/or fibronectin into the polysaccharide-based matrix have demonstrated improved growth, differentiation, and meiotic competence of the oocyte.41–43 In addition, fibrin was also explored as a potential biomaterial for ovarian tissue engineering. 44 Fibrin gels with early-stage ovarian follicles encapsulated for transplantation supported their engraftment and, ultimately, development to antral follicles. The fibrin graft was able to reduce systemic follicle-stimulating hormone (FSH) levels and restore cyclicity in a previously noncycling infertile mouse. 44 These exciting results using hydrogel as model ovarian tissues to provide the necessary cues to activate frozen oocytes created new opportunities for discovery in follicle biology and established a core technology for human egg banks for preservation of fertility. These approaches can potentially develop into a robust system that can be used to consistently activate and mature oocyte. However, issues surrounding natural biomaterials, such as batch-to-batch variability and less-defined molecular composition, need to be resolved before these approaches can be widely utilized clinically.
Cell-based therapy to restore ovarian function
Many investigators have also explored ovarian tissue engineering approaches without using biomaterials. For example, Lai et al. used human endometrial mesenchymal stem cells (EnSCs) to restore ovarian function through improving the renewal of germline stem cells in a murine model of premature ovarian failure. 45 Transplanted EnSCs derived from menstrual blood were injected into the tail vein of sterilized mice. EnSC transplantation increased body weight, improved estrous cyclicity, and restored fertility in sterilized mice. 45 Migration and localization of green fluorescent protein (GFP)-labeled EnSCs as measured by live imaging and immunofluorescent methods indicated that GFP-labeled cells were undetectable 48 h after cell transplantation, but were later detected in and localized to the ovarian stroma. 45
Moreover, human mesenchymal stem cells isolated from the umbilical cord (HUMSCs) were also tested for their ovarian regeneration capacity. 46 Membrane-labelled HUMSCs were injected directly into ovary tissue or the tail veins of infertile rats. 46 HUMSCs injected into the ovary only distributed to the ovary and uterus, while HUMSCs injected through tail vein were detected in the ovary, uterus, kidney, liver, and lung. 46 The estrous cycle and levels of sex hormones of the treated rats were recovered to a certain degree, and fertility was restored in some transplanted rats with normal development of their offspring. 46 While ovary injection of HUMSCs could recover ovarian function faster, both delivery methods produced similar results in the later stages of observation, which indicate that transplantation of HUMSCs by tail vein injection represents a minimally invasive and effective treatment method for ovarian injury. 46
In another study, human amniotic epithelial cells (hAECs) were used to inhibit granulosa cell apoptosis induced by chemotherapy and to restore fertility by injecting cultured hAECs intravenously into infertile mice. 47 Their results demonstrated that hAEC significantly inhibited cell apoptosis induced by chemotherapeutics, reduced the inflammatory reaction in ovaries, promoted the development of follicles, and increased the number of oocyte complexes in chemoablated mice. 47 Furthermore, hAECs improved ovarian mass and increased the number of follicles compared to those of the chemoablated group, and hAEC translation partially rescued the fertility of chemoablated mice. 47 In addition, female germline stem cells (FGSCs) were also shown to rescue ovarian function in chemoablated ovaries. 48 FGSCs were isolated and purified from adult female mice 2 weeks after chemotherapy. After infection with GFP-carrying virus, the FGSCs were transplanted into ovaries to other genetically identical mice with infertility caused by chemotherapy. Ovarian function was restored and the recipients produced offspring long term. 48 These findings showed that FGSCs are able to restore ovarian function and avoid immune rejection from exogenous germline stem cells in a chemoablated, infertile mouse model. 48
Cell-based, scaffold-free approaches to restore ovarian-caused infertility are promising based on the results presented in murine models. However, these approaches will need to demonstrate successful pregnancies in larger animal models before clinical translation.
Cervicovaginal Tissue
Preterm births are a common cause of morbidity and mortality in newborn infants, 49 and maintenance of the anatomic shape of the cervix during fetal and uterine growth is crucial for a normal pregnancy. 3 Studies have shown that the relative risk of preterm delivery increases as the length of the cervix decreases, as determined by vaginal ultrasound measurement during pregnancy. 50
In 2005, Alborzi et al. used a peritoneal graft to treat cervical aplasia. 51 Through an abdominoperineal approach, a plastic stent was inserted between the endometrial cavity and the upper part of the vagina, and a graft of peritoneum was applied over the stent. 51 After more than 1 year of observation, all four patients had regular menstrual cycles with normal menstruation with empty uterine cavities, which challenged the standard approach of uterus hysterectomy in case of cervical aplasia recommended by standard gynecological practice. Amniotic membrane and acellular porcine SIS were also demonstrated to be viable options for cervical reconstructions.52,53
Then in 2010, House et al. used a tissue engineering approach aimed to develop cervical-like tissue constructs that would be suitable for investigating cervical remodeling. 54 Specifically, cervical cells were isolated from two premenopausal women undergoing hysterectomy for benign gynecological conditions, and the cells were seeded on collagen-coated porous silk scaffolds. Cervical cells proliferated in three dimensions and synthesized an ECM with biochemical constituents and morphology similar to native tissue, and outcomes were enhanced through dynamic culture. 54 Even though these studies demonstrated the feasibility of constructing cervix-like tissues through bioengineered approaches, which are summarized in Table 3, none of the studies described herein tested the function of cervix during pregnancy and/or under labor conditions. Success in these situations would be critical to translate these technologies to treat female infertility. Nonetheless these strategies have challenged the current standard clinical approach of uterus hysterectomy in cases of cervical aplasia.
Vaginal agenesis, the congenital underdevelopment of the vagina, occurs in 1 out of 5000 females.55–57 Various biomaterials have been used to fabricate vaginal grafts, including dermal matrix,55,56,58–61 SIS,53,62–67 and human amniotic membrane. 68 Recently, there have been several investigators that explored different biomaterials and cell sources to create tissue engineered constructs for vaginal agenesis therapies (Table 3). For example, using a rabbit model, vaginal epithelial and smooth muscle cells of female rabbits were grown and expanded in culture and seeded on polyglycolic acid scaffolds. 69 The cell-seeded scaffolds were subcutaneously implanted into nude mice and the retrieved polymer scaffolds demonstrated multilayered tissue strips of both cell types and penetrating native vasculature noted with contractile properties in response to electrical stimulus. 69
In addition, adipose-derived MSC seeded silk fibroin scaffolds had a similar failure force and a higher Young's modulus than normal vaginal wall tissue, indicating the potential of this tissue-engineered approach for pelvic floor reconstruction. 70 To test the approach clinically, human trials involving autologous epithelial and muscle cells were performed. 71 Tissue engineered vaginal constructs were then surgically implanted using a perineal approach, and biopsies showed a tri-layered structure, consisting of an epithelial cell-lined lumen surrounded by matrix and muscle, with expected components of vaginal tissue present. The magnetic resonance imagings, which showed the extent of the vaginal aplasia before surgery, showed the engineered organs and the absence of abnormalities after surgery. A validated self-administered Female Sexual Function Index questionnaire showed variables in the normal range in all areas tested.
The potential of other cell sources was also evaluated by other investigators. For example, skeletal muscle-derived stem cells seeded on SIS were demonstrated to stimulate vaginal repair in rats, indicating a promising approach for vaginal repair. 64 In another study, BM-MSCs were stimulated to acquire phenotypes of vaginal epithelial cells (VECs) by coculturing with VECs. 62 BM-MSCs combined with SIS were implanted in the place of the native vagina in rats to observe the potential for vaginal reconstruction. In vivo results demonstrated significant matrix infiltration and expressed epithelial markers in neovagina. 62 These studies showed that cell-seeded polymer scaffolds were able to form vascularized vaginal tissue in vivo with phenotypic and functional properties similar to those of normal vaginal tissues. However, these studies used autologous cells that were isolated from the host, which can sometimes be limited. Therefore, cell sources need to be identified before we can translate these therapies for use in the operating room. Even so, with the advancement in tissue engineering and the understanding of vaginal biology, we expect to see more tissue engineered strategies being introduced to the clinic.
Conclusion
Bioengineering approaches have demonstrated enormous potential in treating female infertility, which can be broadly classified into whole organ transplant (Fig. 2) and tissue engineering approaches (Fig. 3). While whole organ transplant has demonstrated success in large animal models, including nonhuman primates, the source of the organ needs to be identified and the immunogenic effects of allografts need to be characterized before the technology becomes a standard clinical practice. Therefore, there has been a growing interest in using tissue engineering approaches to develop substitute tissues/organs as replacements for nonfunctional organs, which would be easier to scale-up for translation. In spite of many investigations into tissue engineered therapies, the feasibility of creating whole organ constructs through these approaches still needs to be demonstrated. Nevertheless, bioengineering strategies demonstrate enormous promise as potential treatments and cures for female infertility, with clinical translation of these technologies undoubtedly on the horizon.
Footnotes
Acknowledgment
This study was funded by the Sheikh Zayed Institute for Pediatric Surgical Innovation, Children's National Health System.
Disclosure Statement
No competing financial interests exist.