
Abstract
Collagen is one of the important components of collagen membranes as well as the extracellular matrix (ECM). Most previous studies have focused on combining collagen membranes with various cross-linking agents, grafting materials, and cytokines to enhance their mechanical properties and bioactivities. Moreover, collagen membranes are often designed to minimize foreign body reactions involving macrophages. However, macrophages were recently found to play a pivotal role during bone regeneration based on their polarization into both proinflammatory and anti-inflammatory phenotypes. Because of the abilities to modulate macrophage polarization and mediate the balance of proinflammatory and anti-inflammatory microenvironments, immune-responsive collagen membranes may be an innovative strategy for promoting bone regeneration. Herein, following a brief review of collagen membranes and the background of macrophages, recent modulations and studies of immune-responsive collagen are described to express the potential of collagen interacting with macrophages and the necessity of further studies in the field of immune-responsive collagen membranes.
Introduction
C
However, similar to other foreign materials, collagen can lead to inflammation, although it shows desirable biocompatibility and low antigenicity. The material-dependent inflammatory reaction elicited by the introduction of biomaterial is known as the foreign body reaction (FBR).5–7 It is reported that the imbalance of FBR may lead to peri-implantitis and further promote bone resorption, resulting in the failure of implant surgeries. 8 Therefore, it is crucial to embrace the concept of immune-modulating biomaterials to achieve the balance of FBR.
Macrophages play pivotal roles in the FBR, and their role in healing has been increasingly recognized in recent years because of their polarization into proinflammatory (M1) and anti-inflammatory (M2) phenotypes. The “classical” M1 macrophages are activated by bacterial lipopolysaccharide (LPS) and interferon-γ (IFN-γ), which promote an inflammatory response by secreting proinflammatory factors. 9 In contrast, “alternative” M2 macrophages are activated by cytokines such as interleukin-4 (IL-4), interleukin-10 (IL-10), and interleukin-13 (IL-13), which are mainly responsible for immune regulation and tissue remodeling.10–12
The body responds to biomaterials in several ways, depending on the degradability of the biomaterial. After implantation of nondegradable and slowly degradable biomaterials, macrophages cannot sufficiently spread and subsequently fuse into multinucleate giant cells that can be detected even years postimplantation. 6 In contrast, a study showed that M1 cells switch to enriched M2 cells by 7–14 days postimplantation of a scaffold composed of collagen-based materials.13–15 M1 cells are thought to secrete proinflammatory factors that orchestrate the degradation of such degradable materials.
However, delays or the prevention of macrophage-mediated degradation by cross-linking agents may inhibit the beneficial M2 response and result in decreased tissue formation, 13 which may occur through the interaction between immune cells and their degradation products. 16
In addition, immune cells play a pivotal role in promoting new bone formation around bone-implanted devices and are associated with inflammatory fibrous tissue encapsulation. It is important to focus on the integration of immune response to the materials and the effects of immune environment on bone cells during biomaterial-mediated osteogenesis. 17 Therefore, with advancements in the field of osteoimmunology, a better understanding of the immune cell response to various bone biomaterials is necessary, and collagen materials based on the modulation of macrophage polarization can be fabricated to promote bone regeneration ultimately.
Herein, this review aims to (1) characterize and review previous studies involving collagen membranes and their pivotal roles in GBR, (2) provide background knowledge on macrophages and their effects on bone regeneration, (3) review the current literature of collagen membranes interacting with macrophages, and (4) prospect the potential of the immune-mediated collagen materials in GBR.
Application of Collagen Membranes in GBR
In GBR applications, a barrier membrane is typically utilized to prevent epithelial cell and connective tissue migration and create a space for osteoblast growth, which is beneficial for bone and tissue healing.18–20 The nonabsorbable expanded polytetrafluoroethylene (e-PTFE) membranes may lead to exposure of membranes and the inconvenience of a second surgery.21–23 Improvements have been made with the use of controlled biodegradable collagen membranes, and advantages of collagen membranes include their naturally low antigenicity and high biocompatibility.
However, pure collagen lacks mechanical properties and will be resorbed in a relatively degradation rate. Previous studies have mainly focused on promoting bone regeneration by enhancing the mechanical properties of collagen membranes, combining collagen with other materials or cytokines, or reducing the inflammatory response, which will be reviewed in this section.
Improvement of mechanical properties
Collagen membranes must maintain their structure for a sufficient period of time to prevent epithelial migration and keep space for bone ingrowth during early wound healing. 24 Cross-linking agent can effectively prolong the degradation time of collagen membranes. Glutaraldehyde is the most widely used chemical cross-linking agent and is reported to improve mechanical properties of various implantable collagen devices.25,26 However, it may also induce adverse effects such as inflammatory response, calcification, and cytotoxicity.26–28
However, a prolonged degradation time may not always result in greater bone regeneration. Bresaola et al. 29 evaluated the effects of low- and rapid-resorption-rate bioabsorbable collagen membranes using a maxillary sinus augmentation procedure and observed similar healing patterns and bone histomorphometry results among groups. In addition, the exposure of barrier membranes, which is the primary factor contributing to GBR failure, is often observed for nonabsorbable e-PTFE membranes and highly cross-linked collagen membranes. 23 Early exposure may lead to the invasion of bacteria, resulting in early degradation of the biomaterials. 30
To overcome the limitations of cytotoxic residues of chemical cross-linking agents, other cross-linking agents have been developed. 1-Ethyl-3-(3-dimethylaminopropyl) carbodiimide hydrochloride (EDC) shows great potential, particularly for tissue-engineered scaffolds composed specifically of native polymers (e.g., collagen), because it is a zero-length cross-linking agent (the agent itself is not incorporated into the macromolecule) and has not been shown to cause any cytotoxic reactions. Barnes et al. 31 used 20 mM EDC alone in an ethanol solvent, which showed significantly greater cross-linking and mechanical properties compared to glutaraldehyde.
In a recent study by Park and colleagues, an EDC cross-linked type-I collagen membrane was found to be biocompatible, showed adequate tissue integration and resorption kinetics, and promoted bone regeneration when used with bone grafts, indicating the potential of EDC cross-linked collagen membranes in GBR.
In addition, hexamethylene diisocyanate is a commonly used cross-linker and is less toxic than glutaraldehyde. 32 The potential of hexamethylene diisocyanate cross-linked acellular porcine dermal collagen mesh was reported for onlay parastomal hernia repair, showing good recovery with no complications.
In conclusion, most cross-linking agents are used to enhance the mechanical properties of collagen membranes. However, few cross-linking agents show low cytotoxicity and possess the ability to recruit proregenerative macrophages to promote healing. Therefore, additional studies of cross-linking are needed.
Combination of collagen membranes with grafting materials
In addition to improving the mechanical properties of collagen membranes, many studies have been conducted to enhance bone regeneration outcomes by combining other materials (Table 1). Previous studies showed that bone grafts not only maintained the space but also exhibited osteoinductive and osteoconductive capacity. Macroporous calcium phosphates, including hydroxyapatite (HA), betatricalcium phosphate, and biphasic calcium phosphate are the most common bone grafts used with collagen membranes in GBR due to their osteoconductivity. They also possess abilities to form a direct bond to host bone and provide a local calcium source for bone regeneration.33–36
Gupta et al. 37 evaluated the efficacy of naturally derived bovine HA with collagen membranes and collagen plug-in ridge preservation, which significantly reduced bone loss compared to naturally healing extraction sites. In addition, chondroitin sulfate is an important structural component of cartilage, and also provides its resistance to compression. 38 The benefits of this HA/collagen/chondroitin-sulfate spacer have been observed in several animal and human studies,39–42 demonstrating its potential in bone regeneration. Benqué et al. 43 used collagen membranes with an HA/collagen/chondroitin-sulfate spacer and observed significant reduction in pocket depth (the depth of the gingival sulcus near the point at which the gingival tissue contacts the tooth) and gain in attachment level (the distance between junctional epithelium and enamel-cementum junction).
In recent years, the biomimetic mineralized collagen materials, including nanoapatite/collagen composites, attracted much attention. Liao and Cui
44
reported a biomimetic bone scaffold composite, nanohydroxyapatite/collagen/poly(
In summary, additional bone grafting materials for space creation, osteoinduction, and osteoconduction may improve bone formation outcomes. However, macrophage homeostasis is difficult to achieve when using a combination of biomaterials, including the collagen membranes and bone grafting materials applied in bone regeneration. To prevent inflammation caused by various biomaterials, some studies focus on the combination of collagen membranes and cytokines to improve outcome of bone regeneration, which will be discussed in “Addition of growth factors and immune-related cytokines to collagen membranes” section.
Addition of growth factors and immune-related cytokines to collagen membranes
Many attempts have been made to promote bone regeneration by combining growth factors and immune-related cytokines with collagen. 47 Li et al. 48 prepared a double-layered collagen membrane incorporated with basic fibroblast growth factor (bFGF)-loaded chitosan–heparin nanoparticles. bFGF maintained its bioactivity after release from the membranes, which may have potential applications in tissue repair for significantly improving cell proliferation when the cells are seeded onto different layers of the membrane in vitro. Bone morphogenetic proteins (BMPs) can trigger angiogenesis and the migration and proliferation of mesenchymal cells, and their differentiation into osteoblasts. 49 In rat calvarial defects, Jo et al. investigated the effect of sequential delivery of BMP-2 and BMP-7 on bone regeneration with a HA/tricalcium phosphate bone graft covered with a collagen membrane, which significantly induced new bone formation. 50 In addition, growth/differentiation factor 5 is essential for the development and formation of bone, joints, tendons, and ligaments in the axial and appendicular skeleton.51,52 Yamano et al. demonstrated that growth/differentiation factor 5 released from collagen membranes significantly increased cell proliferation osteogenic gene expression without showing cytotoxicity in MC3T3-E1 cells, and significantly enhanced and accelerated bone regeneration in a mandibular defect model. 53
In addition, some studies applied the immune-related cytokines on collagen materials. Minardi et al. 54 fabricated a collagen scaffold releasing IL-4, which revealed an overexpression of anti-inflammatory associated genes (Il-10, Mrc1, and Arg1) at the first 48 h, resulting in acceleration of resolution of the inflammatory phase. Moreover, IFN-γ and IL-4 were loaded on a collagen scaffold to harness the angiogenesis, which was done by Spiller et al. 55
Overall, collagen membranes associated with cytokines are beneficial for bone regeneration and can be used as reservoirs to achieve spatiotemporal control of cytokine delivery. However, the amount as well as the release of cytokines and drugs is difficult to control, and the achievement of spatiotemporal delivery is challenging. This was recently exemplified in a study by Chu et al., 56 who showed that a higher concentration of epigallocatechin-3-gallate (EGCG), a component extracted from green tea with various biological effects, did not improve cell viability and even had an inhibitory effect, although a lower concentration of EGCG significantly improved the mechanical properties of collagen membranes and cell viability compared to pure collagen.
However, after applying polyethylene glycol (PEG) modification on the surface by Chu et al., collagen membranes cross-linked by a higher concentration of EGCG also possessed an improved cell viability with lower level of secretion of tumor necrosis factor alpha (TNF-α). 57 In addition, another study by Mah et al. 58 suggested that the osteogenic effect of EGCG depended largely on the concentration and may switch from promotion to inhibition at increasing concentrations. Therefore, the amounts of cytokines and drugs loaded onto collagen membranes for bone regeneration require further analysis and are difficult to control, risking the outcomes of healing. Nevertheless, after the implantation of collagen materials, it is crucial to achieve the balance of biomaterial-caused FBR.
Regulation of collagen-based FBR
Collagen can also elicit a material-dependent inflammatory reaction. Moreover, the inappropriate FBR will lead to peri-implantitis and boss loss, resulting in failure of implant surgeries. 8 Therefore, many efforts have been made to reduce the FBR caused by the introduction of collagen membranes. Wang et al. 59 fabricated an anti-inflammatory cell-free collagen/resveratrol scaffold with improved mechanical strength and excellent cytocompatibility. After implantation into osteochondral defects in rabbits, inflammatory-related genes were downregulated and bone- and cartilage-related genes were upregulated compared to untreated defects. In addition, a recent study by Chu et al. 56 presented a novel collagen membrane cross-linked by EGCG and successfully enhanced the mechanical properties and regulated levels of inflammatory cytokines secreted by preosteoblast cells.
However, the rapid physiological resolution of inflammation is beneficial for bone healing60,61 and an initial M1 population is required to clear the wound site. Therefore, the design of implantable collagen membranes for bone regeneration should attempt to modulate the inflammatory response, while also avoiding the presence of chronic inflammation, 62 but not blindly repressing the inflammatory reaction.
Applications as pseudo-periosteum in bone regeneration
Because numerous studies have focused on scaffolds as alternatives for bone defects,63–67 the periosteum has not been widely examined. However, the periosteum can supply sufficient blood and nutrition for bone tissue. Therefore, GBR based on functions of periosteum have gained increasing focus these years. 68 The periosteum not only provides mechanical support to tendons but also plays a key role in bone regeneration,69–73 and is involved in cell arrangement, collagen fiber alignment, direction of bone development, and osteoblast formation, which are necessary for remodeling injured bones.74–76 In addition, studies have also indicated that the periosteum increases the rate and quantity of bone formation and improves vascular invasion in large segmental defects. 77
Collagen is the main component of the fibrous layer of the periosteum; moreover, it has been reported that collagen fiber orientation in the periosteum is preferentially associated and aligned in the direction of long bone growth. 71 Therefore, collagen membranes may serve as pseudo-periosteums. Shi et al. 78 used a stem-cell- and endothelial-cell-laden collagen membrane as a pseudo-periosteum to cover a three-dimensional porous scaffold and observed remarkable osteogenesis compared to that in periosteum-free scaffolds. In addition, collagen membranes can support and promote the proliferation of human periosteal cells. 79
However, the requirement for the hierarchical topographic surface of the periosteum, which is important for bone elongation, may not be satisfied by collagen membranes, as they cannot effectively anchor bone scaffolds as nanoscale materials. 80 In addition, osteal macrophages (OsteoMacs) were found to be distributed within both the endosteum and the periosteum, 81 which are closely associated with bone modeling and will be discussed later. Moreover, it was reported that macrophages are responsible for both the initiation and the progression of early endochondral ossification by periosteal callus formation. 82 However, few studies have examined the mechanism of action of the pseudo-periosteum on the immune system, including the interaction with OsteoMacs. Further studies of applications of collagen membranes as pseudo-periosteums are needed.
Collagen membranes have been widely used in GBR, and studies have mainly focused on its direct effects on osteoblasts and bone by prolonging the degradation time, incorporating with grafting materials, adding cytokines, and downregulating the inflammatory response, or serving as the pseudo-periosteum. However, the importance of immune cells and their reactions with materials that facilitate new bone formation have not been widely examined in the field of bone regeneration and collagen-based materials, which will be later discussed in this article.
Macrophages: Key Roles in GBR
Immune cells play a pivotal role in the process of healing after implantation of collagen materials, which involves a characteristic sequence of events, including hemostasis, inflammation, proliferation, and remodeling. 83 After the hemostasis phase, molecular factors secreted by immune cells are involved in inflammatory reactions. In addition, macrophages mediate cellular proliferation, angiogenesis, new ECM deposition, and granulation tissue formation in the proliferation cascade by secreting cytokines, including epidermal growth factor (EGF), bFGF, transforming growth factor alpha and beta (TGF-α, TGF-β), and vascular endothelial growth factor (VEGF).83–85
Moreover, the outcome of the subsequent remodeling phase may involve macrophage participation and polarization during the proliferation stage. The remodeling phase involves matrix metalloprotease (MMP) and tissue inhibitor of metalloproteinase-mediated degradation and remodeling of the newly deposited collagen, which also involves macrophages.83,86 Macrophages are thought to mainly reside in the peripheral blood and tissue and play different roles depending on their functional diversity, which will be discussed in “Blood-resident macrophages” and “Tissue-resident macrophages” section.
Blood-resident macrophages
Macrophages derived from circulating monocytes circulate in the peripheral blood after leaving the bone marrow and become activated after migration into inflamed tissue (Fig. 1). Related to their functional diversity, they polarize into the proinflammatory M1 and anti-inflammatory M2 state (Table 2 for details and the following studies),10–12,87–93 mirroring the T helper cell 1/T helper cell 2 (Th1/Th2) described for T helper cells. 94
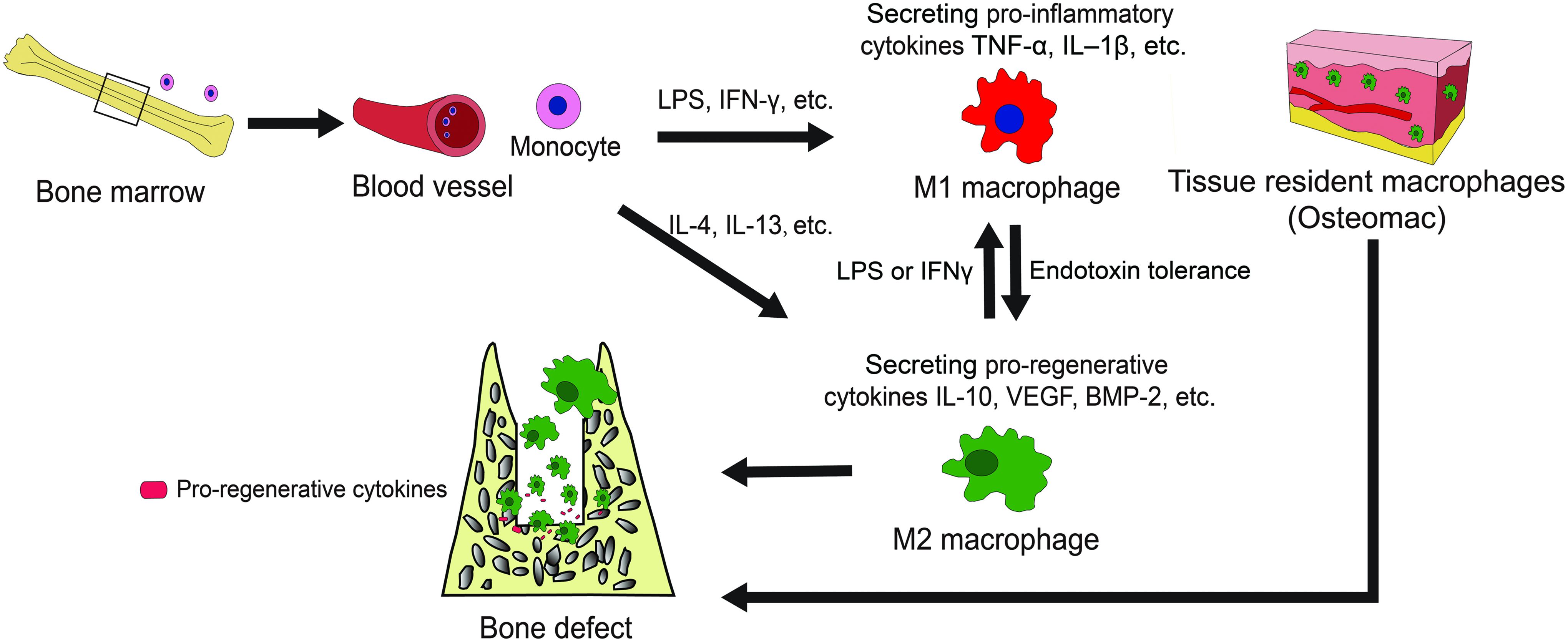
The roles of macrophages on bone regeneration. Monocytes leaving from bone marrow circulate in blood and differentiate into M1 and M2 macrophages. M1 phenotype is induced by IFN-γ and LPS, and may have characteristic of M2 cells when it becomes endotoxin tolerance. Meanwhile, M2 macrophages is induced by signals such as IL-4 and IL-13, and can be induced to be M1-like cells when exposed to LPS or IFN-γ. In addition, tissue-resident macrophages (OsteoMacs) also play roles in bone regeneration. After arriving at the bone defects, M2 macrophages and OsteoMacs promote bone regeneration by secreting proregenerative cytokines, including IL-10, VEGF, and BMP-2, while M1 phenotype functions by secreting proinflammatory cytokines such as IL-1β and TNF-α. BMP, bone morphogenetic protein; IFN-γ, interferon-gamma; IL, interleukin; LPS, lipopolysaccharide; TNF-α, tumor necrosis factor alpha; VEGF, vascular endothelial growth factor. Color images available online at www.liebertpub.com/teb
BMP, bone morphogenetic protein; CCL, chemokine ligand; CD, cluster of differentiation; CXCL-α, chemokine ligands; FR, folate receptor; GF, insulin-like growth factor; GR, galactose receptor; IFN-γR, IFN-γ receptor; IFN-γ, interferon-gamma; IL, interleukin; IRF, IFN regulatory factor; Jak, Janus kinase; LPS, lipopolysaccharide; MHC, major histocompatibility complex; MR, mannose receptor; PDGF, platelet-derived growth factor; PTX3, pentraxin 3; RNI, reactive nitrogen intermediate; ROI, reactive oxygen intermediate; SR, scavenging receptor; STAT, signal transducers and activators of transcription; TGF, transforming growth factor; Th1, T helper cell 1; TLR, toll-like receptor; TNF-α, tumor necrosis factor alpha.
The “classically activated” M1 phenotype, induced by chemoattractants such as IFN-γ and LPS, 9 is capable of producing proinflammatory cytokines (such as IFN-γ and interleukin-2 [IL-2] in response to intracellular pathogens by promoting Th1 differentiation of lymphocytes). These cells also kill intracellular pathogens by iron restriction, preventing the growth of bacterial infections. 10 In addition, an increased proinflammatory response of M1 macrophages may harm nearby cells by producing toxic reactive oxygen intermediates. 88 In addition, a severe FBR as well as fibrous encapsulation escalated by M1 macrophages may result in the failure of biomaterial integration. 16
However, participation of M1 macrophages is essential for promoting healing by the implantation of degradable biomaterials such as collagen. As discussed in the Introduction, a delay or prevention in macrophage-mediated degradation by cross-linking agents may inhibit the beneficial M2 response and decrease tissue formation, 13 which may occur through interactions between host cells and their degradation products. 16
The “alternatively activated” M2 phenotype of macrophages, induced by signals such as IL-4 and IL-13, release anti-inflammatory cytokines such as IL-10, 11 which contribute to tissue remodeling 10 in contrast to M1 macrophages. M2 macrophages are further divided into different subsets (i.e., M2a, M2b, and M2c) based on their functional diversity. 89 Briefly, M2a is associated with Th2 anti-inflammatory responses. The M2b phenotype performs immune regulatory functions (both proinflammatory and anti-inflammatory function). 90 In contrast, the M2c phenotype plays a major role in matrix deposition, tissue remodeling, and prohealing.
Although M2 macrophages have been identified as prohealing cells that promote ECM production by secreting IL-4 and TGF-β, overstimulation of ECM deposition may lead to unfavorable fibrosis, as both IL-4 and TGF-β are strong inducers of fibrosis without tight regulation. 95 In addition, monocyte chemotactic protein 1/chemokine ligand 2 (MCP-1/CCL-2) has been identified as a profibrotic mediator implicated in the stimulation of M2 polarization.96,97 However, inhibition of M2 macrophages and these molecules may terminally lead to impaired tissue healing. 98 Therefore, identifying a method to stimulate sufficient functional ECM deposition without collagen encapsulation and fibrosis remains a primary challenge in bone regeneration.
In summary, the presence of macrophage polarization in response to various microenvironments may be advantageous for constructive remodeling, while minimizing undesirable inflammatory reactions.
Tissue-resident macrophages
In contrast to the original theory that macrophages derived from circulating monocyte precursors are recruited to sites of inflammation, more recent research has confirmed that some tissue-resident macrophages subdivide and proliferate to sustain their local populations during injury events.99,100 Previously, monocyte subsets in human blood were categorized into two main subpopulations, CD14+ monocytes and CD14lowCD16+ monocytes. 101 Mouse studies have suggested that CD14+ monocytes in humans terminally represent classical monocytes in the blood stream. In contrast, resident macrophages102,103 may be differentiated by CD14lowCD16+ monocytes. OsteoMac is a CD68+ cell type of macrophage in bony tissues and is derived from resident macrophages such as macrophages in other tissues, serving as a special canopy structure overlying mature osteoblasts (Fig. 1).99,104,105
The general role of OsteoMacs has been described as immune surveillance in the bone microenvironment. Previous studies have shown that OsteoMacs can detect bacterial products106,107 and are highly involved in antigen presentation.108,109 Further evidence suggests that these cells respond to LPS. 81 Collectively, OsteoMacs may also function as phagocytes with some characteristics of the M1 macrophage discussed in “Tissue-resident macrophages” section.
However, Chang et al. observed a 23-fold reduction in mineral deposition after removing macrophages from primary osteoblast cultures. 81 Currently, OsteoMacs are known to produce a wide variety of either proinflammatory or anti-inflammatory cytokines. OsteoMacs have been shown to secrete proinflammatory factors, including TNF-α,110,111 IL-6, 112 IL-1β,110,113 and IFN-γ114,115 under various conditions. However, further studies showed that OsteoMacs produce a number of bioactive cytokines, including TGF-β, 116 osteopontin, 117 1,25-dihydroxy-vitamin D3, 118 and BMP-2, 119 which are classical characteristics of the M2 macrophage and serve as inducers of ECM deposition and new bone formation. These observations demonstrate that the specific functions of OsteoMacs are difficult to clearly define because of the potential cross-lineage plasticity and cross talk between cells.
OsteoMacs were found to encapsulate functionally mature osteoblasts, described as “forming a canopy-like cell structure,” suggesting that they are heavily involved in the bone modeling process.81,120 Moreover, in a macrophage Fas-induced apoptosis (Mafia) transgenic mouse model, inducing macrophage depletion, the complete loss of mature osteoblasts and bone modeling at the bone interface was observed when the OsteoMac canopy architecture was disrupted, demonstrating the functional importance of OsteoMacs. 121 Moreover, OsteoMacs are involved in bone regeneration by secreting VEGF and BMP-2. 119
In contrast to bone modeling, the process of bone remodeling involves a careful and coordinated balance between bone-resorbing osteoclasts and bone-forming osteoblasts.122,123 TGF-β and ephrin B2 are possible coupling factors between osteoclasts and osteoblasts.122,124–126 Previous studies showed that OsteoMacs are capable of producing TGF-β 116 and ephrin B2127,128 as discussed in “Tissue-resident macrophages” section, and OsteoMacs may also be required for bone remodeling. Moreover, based on their close proximity to bone surfaces as a canopy structure and well-known ability to detect dying cells, OsteoMacs may be candidates for detecting and responding to bone damage, which is critical for osteoclast recruitment that initiates the bone remodeling phase. 129
Regulation of macrophage polarization
Macrophages polarization into proinflammatory (M1) and anti-inflammatory (M2) phenotypes based on functional diversity has been increasingly recognized these years. Many studies have focused on the mechanisms of macrophage polarization. The global regulatory landscape controlled by the E26 transformation-specific (ETS) family transcription factor PU.1 represents the general transcription factors regulated by external stimuli to modulate macrophage function. 130
PU.1 is constantly expressed at high levels to induce and maintain macrophage differentiation.131–133 PU.1 binding is sufficient to create small open regions of accessible DNA that can be bound by other transcription factors that probably contribute to the differentiation of macrophages, such as IFN regulatory factor 8 (IRF8), 134 or for functional specialization, such as IRF4 and IRF5 (which are involved in M2 and M1 polarization, respectively) and CCAAT/enhancer-binding protein-β (C/EBPβ).135–137
Some key transcription factors translate signals in the microenvironment into a polarized macrophage phenotype. The signal transducers and activators of transcription (STAT) family play an important role in M1 and M2 macrophage polarization. M1 characteristics (major histocompatibility class II molecules, nitric oxide synthase 2, and IL-12) 99 are mainly promoted by IFN-γ-mediated Janus kinase–signal transducer and activator of transcription (JAK–STAT) signaling. 138 In addition, polarization of M1 macrophages is activated by LPS, which depends on the autocrine production of IFN-β through TRIF-dependent signaling from Toll-like receptor 4 (TLR4) to IRF3. 139
M2 factors, including arginase 1, macrophage mannose receptor 1 (also known as Cd206), resistin-like α (also known as Fizz1), and chitinase 3-like 3 (also known as Ym1), 90 are regulated by IL-4Rα signals through a JAK–STAT6 pathway. 140 Importantly, IL-4 triggers the activation of phosphoinositide 3-kinase, 141 which is also crucial for in M2 macrophage polarization. Adipose tissue macrophages typically have an anti-inflammatory M2-like phenotype. Peroxisome proliferator-activated receptor-gamma (PPAR-γ) is a master regulator of lipid metabolism in M2 polarization, 142 which can also be induced by IL-4 and IL13. 143
The reciprocal regulation of M1 and M2 genes by the same transcription factors is common in macrophage polarization, as is exemplified by the mutual antagonism of STAT1 and STAT6. cAMP responsive element binding protein (CREB) may be a crucial transcription factor in macrophage polarization by promoting M2 polarization, while repressing M1 activation. CREB-induced C/EBPβ is responsible for arginase 1 expression in response to TLR ligands, which promote M2 macrophages. In addition, CREB plays an anti-inflammatory role in response to LPS, which represses M1 activation by mediating p38 mitogen-activated protein kinase and mitogen- and stress-activated kinases 1 and 2.144,145
IFN regulatory factors also direct the differentiation of M1 and M2 macrophages. IL-4-induced IRF4 was shown to specifically regulate M2 macrophage polarization in response to fungi and helminthes involving JMJD3, which is also controlled by the expression of IRF4.138,146,147 However, overexpression of IRF5 is associated with granulocyte–macrophage colony-stimulating factor-induced human macrophages (an M1-like phenotype), which also showed that the IFN regulatory factor is one of the reciprocal regulations of M1 and M2 genes.
Moreover, macrophages possess dynamic and plastic phenotypes in response to local microenvironmental signals,148–151 which depend on the type, concentration, and duration of the polarizing signals. It is found that a mixture of macrophage phenotypes is shown at any time among macrophage population. There are even macrophages in a state that express markers of both M1 and M2 phenotypes. 16 This may due to the changes in stimuli. Experiments have shown that secretion of LPS-stimulated macrophages may change from proinflammatory cytokines to anti-inflammatory factors such as IL-10, when the macrophages become TLR tolerant.151–153 Similarly, M2 cells can be readily induced to have characteristic of M1 cells when exposure to LPS or IFN-γ. However, the mechanisms of macrophage phenotype plasticity are not well understood.
Modulation of Collagen Membranes Based on Response to Immune Cells
As described above, the introduction of collagen membranes may cause the FBR involving macrophages, which may impair biomaterial integration. A previous study contributed to reducing the material-based inflammatory response.56,59 However, with advancements in the understanding of macrophage responses to implanted biomaterials, immune-mediated tissue regeneration elicited by biomaterials such as collagen is emerging as an innovative regenerative strategy. 154
The integration among immune cells, bone cells, and collagen membranes
Generally, after the implantation of collagen membranes, a layer of proteins from the surrounding vasculature adsorbs onto the surface, leading to infiltration and adherence of cells such as platelets, monocytes, and macrophages. Macrophages then recruit tissue repair cells (e.g., fibroblasts and mesenchymal stem cells) to the inflammation site by releasing cytokines and chemokines. These sequences constitute the natural innate immune response following biomaterial implantation. 155
The close relationship that exists between the immune systems and collagen membranes is a double-edged sword. To be specific, a favorable FBR creates an osteogenic microenvironment, while an inappropriate FBR may lead to the chronic inflammation and the formation of a fibrous capsule around the implant. The fibrous capsule prevents direct interaction between surrounding environment and the biomaterials so that the materials can be maintained in the host body for sufficient time. 156 However, the fibrous encapsulation also separates the biomaterials with bone marrow. Undesirably, bone cells cannot attach to the surface of materials to form new bone, and the defect will be filled by fibrous tissue instead.
It is reported that the process of bone biomaterial-mediated de novo bone formation process can be divided into three phases: early, bone formation, and remodeling phase. The early stage is dominated by the inflammatory phase, when the majority of macrophages would be the inflammatory M1 phenotype. It is crucial to have a timely switch from M1 to M2 macrophage phenotype, which will lead to osteogenic cytokine release and new bone formation. However, a prolonged M1 polarization phase leads to an increase in polarization of M2 macrophages that have fibrosis-enhancing cytokine release pattern, resulting in fibrous encapsulation and the failure of bone biomaterials. 157
Therefore, the osteoimmunomodulation (OIM) is important during biomaterial-mediated osteogenesis. The OIM not only considers the immune response to the materials but also focuses on the effects of the immune environment on the behavior of bone cells after biomaterial implantation. 17 The immune and bone cells are closely related by sharing a number of cytokines, receptors, signaling molecules, and transcription factors,158,159 and immune cells, including OsteoMacs, play a key role in bone homeostasis. For instance, immunomodulatory cytokines such as IFNs participate in the regulation of RANKL (an osteoclastogenic cytokine) signaling and inflammatory bone loss.
In addition, immunoglobulin-like receptors are critically involved in bone homeostasis. 160 Altogether, better understanding and treatment of bone augmentation by immune-mediated biomaterials are greatly emerging. As the new generation of bone biomaterials, they should possess abilities to modulate the local immune environment that favors osteogenesis and osseointegration, 17 including mediation of macrophages recruitment and polarization, which will be discussed in “Regulation of immune cells by biomaterials, including collagen” section.
Regulation of immune cells by biomaterials, including collagen
The behaviors of immune cells can be regulated by the biomaterial surface properties, particle size, porosity, and the released ions from the biomaterials. Previous studies developed strategies for reducing protein adsorption, initial cell adhesion, and foreign body giant cell fusion around biomaterials, 161 such as collagen, to reduce the FBR by changing the surface chemistry of the materials.
Accordingly, biomaterial surface properties, including wettability and surface charge, are strong regulators of macrophages in tissue engineering. 162 Studies have demonstrated that the release of IL-1β, TNF-α, IL-6, IL-8, and macrophage inflammatory protein-1β preferred hydrophilic surfaces, reducing the adhesion of macrophages compared to hydrophobic surfaces.162–164 These may be determined by the interaction of absorbed protein with immune cells and subsequent behaviors of immune cells. 165
Most proteins are hydrophilic on their outside and thus tend to bind on the hydrophobic surfaces. 166 In addition, it is also generally accepted that positively charged surfaces are more feasible to promote inflammatory response than negatively charged and neutral surfaces. 167 Therefore, changes on surface properties of collagen membranes may be beneficial for the modulation of macrophages.
In addition, porosity and pore size of bone materials are two important factors to determine the ingrowth tissue types (inflammatory granuloma tissue, vascular tissue, and bone tissue). 168 It is more beneficial for the ingrowth of bone tissue when the scaffolds possess higher porosity of 80–88% and macroporosity (pore size >50 mm). 168 Moreover, porosity and pore size are involved in macrophage polarization, which has been studied in the collagen-based materials.
Koyal et al. 169 investigated the effect of fiber and pore size of a collagen-based scaffold on the polarization of mouse bone marrow-derived macrophages toward regenerative (M2) or inflammatory (M1) phenotypes. As fiber diameter, pore size, and porosity increased, expression of the M2 marker arginase 1 increased and expression of the M1 marker inducible nitric oxide synthase decreased. Secretion of the angiogenic cytokines VEGF, TGF-β1, and bFGF was also higher in larger fibers and larger pore-size scaffolds.
Moreover, their results showed that pore size is more crucial for macrophage polarization than fiber diameter. This may be because macrophages are more prone to infiltrate in materials with larger pores. In addition, it is reported that maximum vascularization and minimal fibrotic response, with an increased number of M2 phenotype macrophages, are observed in the cardiac implantation of hydrogels with pore diameters of 30–40 mm. 170
Meanwhile, ions released from the biomaterials during degradation can alter the local biological environment, resulting in modulation of immune response. Calcium (Ca) is found to enhance inflammation through the Wnt5A/Ca2+ signaling pathway. 171 Silicon (Si) participates in the early mineralization phase of bone regeneration around active calcification sites. 172 Mg2+ ions can downregulate secretion of inflammatory cytokine by inhibiting the TLR pathway, 173 which is the pathway macrophages used to recognize foreign bodies during the process of rejection. 7 TLR3 can only signal by the adaptor protein toll-like receptor adaptor molecule (Ticam), which is also known as TIR domain containing adapter inducing IFN-β. However, TLR4 can proceed by both pathways (TRIF and MyD88 pathways). Both MyD88-dependent and TRIF-dependent pathways express inflammatory cytokines by recruiting NF-κB. 174
However, the related irons released from collagen membranes have not been studied. Further studies can investigate the effects of Ca2+, Si, and Mg2+ released from collagen membranes on regulation of immune cells.
Collagen based on modulation of macrophages in GBR
Several studies have shown that collagen can recruit macrophages. It was reported that the molecular events of the collagen membrane in the GBR are associated with the upregulation of cell recruitment and bone remodeling genes in early and late periods and accumulation of FGF-2 and BMP-2 proteins and immunoreactive cells were found around the implanted membranes. 175
Moreover, Sicari et al. 176 used an acellular biologic scaffold (the main component of the scaffold is collagen) to aid in volumetric muscle loss. They found that acellular scaffold implantation was associated with the mobilization and accumulation of perivascular stem cells and de novo formation of skeletal muscle cells at the injury site, resulting in functional improvement.
Sadtler et al. 154 demonstrated that an ECM scaffold enhanced the development of a proregenerative immune response characterized by the Th2 pathway, which guides IL-4 macrophage (also known as M2 macrophages) polarization. Brown et al. 14 clearly demonstrated that increased numbers of M2 macrophages and higher ratios of M2:M1 macrophages within the site of remodeling at 14 days can lead to more positive remodeling outcomes, indicating a strong correlation between the early macrophage response to implanted ECM scaffold materials and outcome of tissue remodeling.
To further understand the mechanisms behind macrophage phenotype transition and the enhanced M2:M1 ratio associated with ECM scaffold, another study by Sicari et al. shows that products degraded from ECM scaffolds are associated with promoting M2 macrophage polarization in vitro, which eventually facilitates migration and myogenesis of skeletal muscle progenitor cells. 177 These studies demonstrate the importance of collagen in recruiting immune cells and modulating the polarization of macrophages.
The course of bone healing is also influenced by sufficient revascularization at injury sites. 178 A study by Spiller et al. 179 found out the role of macrophage phenotype in the vascularization of tissue engineering scaffolds. The authors found that porous collagen scaffolds were surrounded by highly expressed M2 macrophage markers, which promoted the vascularization of tissue engineering. They also suggested that the coordinated efforts by both M1 and M2 macrophages are required for angiogenesis and scaffold vascularization, as M1 macrophages secrete the highest levels of potent angiogenic stimulators, including VEGF, and M2 macrophages secrete high levels of platelet-derived growth factor BB (PDGF-BB) and MMP-9, contributing to the anastomosis of sprouting endothelial cells and vascular remodeling, respectively (Fig. 2).

The schematic diagram of the new generation of GBR membranes. The new generation of GBR membranes is based on regulation of foreign body reaction. By surface modification, the new GBR membranes may possess ability to promote recruitment and adhesion of M2 macrophages (proregenerative phenotype), which further increases secretion of proregenerative cytokines such as VEGF, PDGF, and BMP-2 for revascularization and bone growth. Meanwhile, they should also maintain the functions as barriers to prevent the migration of fibroblasts and maintain space for osteoblast adhesion, proliferation, and differentiation. GBR, guided bone regeneration; PDGF, platelet-derived growth factor. Color images available online at www.liebertpub.com/teb
Spiller et al. 55 recently designed scaffolds for bone regeneration based on the modulation of macrophage polarization from the M1 to M2 phenotype because M1 macrophages initiate angiogenesis, while M2 macrophages promote vessel maturation. Therefore, scaffolds were modified to release IFN-γ to promote the M1 phenotype at first, followed by the release of IL-4 to promote the M2 phenotype, showing impressive vascularization outcomes.
In conclusion, recruitment of macrophages and macrophage polarization on collagen materials may be modulated by the biomaterial surface properties, particle size, porosity, and the released ions. Collagen materials have shown great potentials in regulating behaviors of macrophages, including the recruitment, polarization, and the cytokines secreted by different phenotypes during every stage of healing process, which result in promoting outcome of bone regeneration.
Potentials of Collagen Membranes Based on Macrophage Polarization
Using collagen materials to manipulate the adaptive immune system may promote both systemic and local proregenerative immune responses and ultimately stimulate tissue repair. 154 Modulation of collagen membranes based on the response to immune cells is still faced with obstacles, including the reactions of macrophage phenotypes in response to different microenvironments and the interactions among various biomaterials, macrophages, and bone cells.
Putten et al. 180 suggested that many macrophages in the FBR induced by hexamethylene diisocyanate-cross-linked dermal sheep collagen do not always fit into the classical M1 or M2 dichotomy, as some macrophages exhibited an M2 phenotype, while the M1 phenotype was not detected. This may be because macrophages present different phenotypes in response to different microenvironments of the FBR. Macrophage phenotypes are associated with the outcome of bone regeneration.
However, it is reported that the time of M1 macrophages present during the first stage of healing process may be involved with polarization of M2 macrophages that have osteogenesis cytokine release pattern or fibrosis cytokine release pattern. 157 This phenomenon may explain why unexpected results still exist even though the phenotypes are defined. Therefore, further studies are needed to determine whether macrophage phenotypes can be used to predict remodeling following implantation of collagen membranes.
Moreover, the influence of various biomaterials is unknown. In dental implant treatment, collagen membranes are usually in contact with two materials, including a titanium dental implant and bone grafting material within the tiny 1-mm region, when collagen membranes are introduced to promote bone regeneration. It is possible that, while these types of biomaterials favor macrophage homeostasis and tissue integration, the others may cause a severe inflammatory reaction.
Therefore, deeper understandings of the interaction between collagen membranes and macrophage, and the correlation among various biomaterials are urgently needed, considering its great potential in the field. Moreover, further studies can investigate the effects of Ca2+, Si, and Mg2+ released from collagen membranes on regulation of immune cells because the studies of the related irons released from collagen membranes are few.
Conclusion
Modulation of collagen membranes in bone regeneration was used to focus on enhancing mechanical properties and loading grafting materials or cytokines. However, the results were not satisfied. The recent surge in the application of collage membranes has advanced to modulating inflammatory reactions based on the improved understanding of macrophage polarization. By modifications of surface properties, particle size, porosity, and the released ions, an ideal immune-mediated collagen membrane should promote anti-inflammatory M2 macrophages and secretion of proregenerative cytokines, with the abilities of preventing migration of epithelium and maintaining space for bone ingrowth.
Further research should aim to increase the understanding of blood- and tissue-resident macrophage polarization and the inflammatory reactions caused by various biomaterials because the interactions among materials may lead to complicated FBR that make the outcome unpredictable. Improvements in collagen materials based on immune modulation will have great potentials and ultimately lead to better outcomes in applications of GBR.
Footnotes
Acknowledgments
This work was supported by grants from the National Natural Science Foundation of China (No. 81671023) and the National Key Research and Development Program of China (No. 2016YFA0201703/2016YFA0201700). In addition, special appreciation was sent to Dr. Zetao Chen for his helpful contribution and advice to this work.
Disclosure Statement
No competing financial interests exist.