
Abstract
Sutures are synarthroses connecting the bones of the head with each other through a fibrous sutural ligament. The knowledge of their biomechanical properties is relevant in the application of regenerative techniques for the treatment of craniofacial conditions, such as the sutural distraction osteogenesis (SDO). However, their mechanical characterization has not received a systematic approach, and both clinical treatments and virtual simulations lack clear mechanical parameters. Online databases (PubMed©, Cochrane Library©, Google Scholar©), references of full-text articles, and previous reviews of the literature were searched. Articles quantifying the biomechanical properties of human sutures were included without date, language, or publication restrictions. A qualitative analysis was carried out based on source, sample, load, and measurement characteristics. Subsequently, mechanical parameters were discussed for each suture analyzed. No previous review was found debating the topic. Seven studies were included, only six sutures were analyzed among the about 39 existing ones, and important situations such as compressive and static loading were not considered. Only three studies analyzing the coronal, sagittal, and metopic sutures provided a clear description of the methods and determined parameters of sutures of infants and children. Although a selective load application on sutures is capable of modifying the craniofacial development, little is known about the optimal forces to be applied. The present findings may help to estimate the forces transferred to the sutural ligament during SDO when the strain is measured, and to advance the rationale of the application of certain parameters to optimize the clinical outcome.
Introduction
“C
Anatomy and morphogenesis
Sutures are articulations belonging to the synarthroses, that is, immovable or nearly immovable joints, and more specifically to syndesmoses, that is, fibrous articulations with a sutural ligament between the parts. Nine cranial bones (two parietal bones, two temporal bones, one ethmoid bone, two frontal bones, one sphenoid bone, and one occipital bone) and 17 facial bones (two inferior nasal conchae, two lacrimal bones, two nasal bones, two palatal bones, two zygomatic bones, two mandibular bones, one vomer bone, two maxillary bones, and two anterior maxillary bones) generally constitute an adult human cranium, and they are connected to each other through a complex system of about 39 sutures (Fig. 1). Sutures are characterized by a variable anatomy, which is related to a complex biomechanical function. For example, sutural morphology shows a specific relationship with the characteristics of the strain, with sutures under compression being generally more interdigitated than sutures under tension. 8 Accordingly, Byron et al. demonstrated that an increased jaw-muscle force is associated with an increased sutural interdigitation. 9 On the contrary, a stress modification from compression to tension is associated with a simplification of the growing fronts. 10
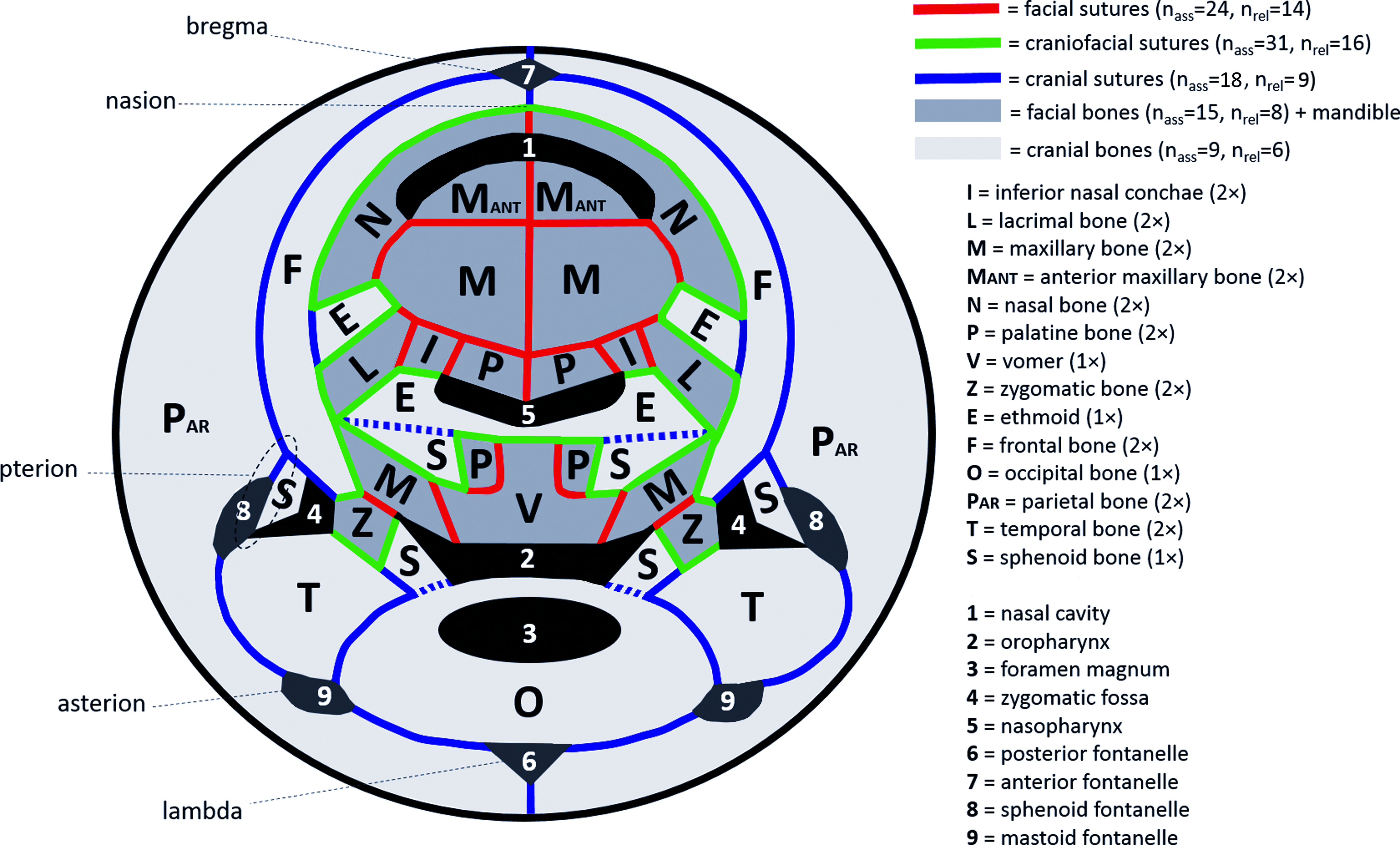
Schematic two-dimensional representation of the human craniofacial skeleton with respective bones and sutures. The spheno-occipital synchondrosis and the spheno-ethmoidal synchondrosis are dashed, since they are not synarthroses as the sutures. The ossicles of the ears (the malleus, the incus, and the stapes) and the mandibles were not represented. In order to illustrate all the actual articulations between bones, some bone are showed more times than the clinical reality (the sphenoid appears six times rather than one, the ethmoid appears three times instead of one, and the palatal bones and the nasal bones appear four times instead of two). Color images available online at www.liebertpub.com/teb
Biomechanical characteristics
Any exogenous force applied to the sutures is transmitted as mechanical stress that is measurable as bone strain either on the cortical bone surface or along the sutural interface itself. 11 In mammals, sutures are structured to allow an efficient load transmission, with mature sutures characterized by a well-developed system of fibers resistant to deformations in tension, compression, or both. 12 Although sutures are areas of flexure and energy absorption, they may even show a stress resistance that is close to the bones they join. 13 On a small scale, their biomechanical properties are consequences of the viscoelastic behavior generated by the interactions between cells and components of the extracellular matrix. In fact, this physical heterogeneity leads to a nonlinear reaction to forces, influenced by load characteristics, fluid movement, fiber rearrangement, and cell deformation. 3 In addition, biomechanical properties may vary among different sutures depending on factors such as the interdigitation, 14 and within the same suture because of specific fiber orientation to resist peculiar strain patterns. 15
Despite several variables having been simulated through virtual reconstructions, such as different degrees of interdigitation, 16 these computer evaluations are very likely far from the true biological complexity. On the other hand, even though animal experiments represent a far more detailed model, mechanical characteristics may differ from humans. As a consequence, although laboratory studies analyzing human material cannot exactly replicate in vivo conditions, they still represent one of the best possible options for the mechanical evaluation of the sutural ligament. 17
Loading of the sutures
Load characteristics add further variables in sutural biomechanics. For example, load may come from exogenous sources, for example, in case of distortion of the skull during birth or trauma. Load can be exogenous, for example, generated by impacts, or endogenous, for example, related to intracranial pressure. Further, load type can be quasi-static, for example, screw-rack orthopedic distraction devices, or nonstatic, for example, small shocks while walking. In addition, its distribution can have different directions, such as tension generated by distraction devices, and shear or compression forces during trauma. In this regard, sutural strain varies depending on the orientation of the force. 18
The quantity of load can have different characteristics as well, in terms of modulus, angulation, and frequency. Load modulus may affect sutural biological reactions and it has been shown that an increased load generates a greater osteogenic response in rats. 19 However, it seems that the behavior of sutures toward increasing load is not linear, and different responses may occur at different force ranges in both tension and compression. 20
The load direction can affect the biological response as well, such as in the case of curved bones because of fractures or malformations, in which tissue resorption is present on the convex side, that is, area under tension, and bone deposition on the concave one, that is, area under compression. 21 This behavior is apparently contrasting with principles of distraction osteogenesis (DO) 22 or orthodontic tooth movement, 23 and it indicates the importance of the discrimination between axial and nonaxial load.
Further, even though some in vitro studies found that the strain rate has little influence on the biomechanical behavior of sutures sampled postmortem, 24 velocity still deserves attention because of its in vivo importance in the amount of bone formation during both sutural SDO 25 and traditional DO. 26
Finally, the load frequency should be considered, since the loading may be single, constant, or multiple, and characterized by different waveforms with peculiar biological effects. In fact, previous studies applied tensile stress alternatively with relaxation periods, and sutural reactions were modulated by the frequency of the exogenous forces. 27
As a consequence, the load parameters are of fundamental importance, and they play a relevant role in the biological response during procedures such as SDO. Indeed, as previously stated by Mao, 3 expecting bone apposition under tension whereas bone resorption under compression may be an oversimplification of the complex strain distribution and respective reactions of the skeletal tissue. In fact, variables such as the amount of strain, its rate, and its frequency should not be neglected while debating the mechanical properties of sutures and their reaction under loading.
Objectives
The objective of this study was to summarize the biomechanical properties of the human sutures while taking into consideration variables related both to sutural intrinsic features, such as characteristics of the subject and of the analyzed specimen, and to the respective applied load.
This review aimed at clarifying which parameter of which specific suture was available in the published literature. A summary of the biomechanical data was presented and discussed to advance the rational application of determined stimuli during SDO. Further, the findings will be relevant for numerical simulations of craniofacial biomechanics.
Methods
Eligibility criteria
No search limitations were applied with regard to publication date, language, or status. Studies testing bone material without sutures, or using animal sources were excluded. Only studies quantitatively testing physical properties, for example, stress, strain, and respective mechanical derivates, of human sutures were included, and studies assessing the general biomechanics of the craniofacial skeleton were not considered. No exclusion criteria related to the quality of the studies was applied at the screening stage. The present literature review is exempt of institutional review board (IRB) evaluation because of the use of previously published data.
Search strategy
Databases were searched (PubMed®, Cochrane Library®, Google Scholar®), performing the last search on January 1, 2017. References from full-text articles and previous reviews of the literature were included in a later stage. Key words were selected, and the following searches were performed:
(“skull” [MeSH Terms] OR “skull” [All Fields] OR “cranial” [All Fields] OR “craniofacial” [All Fields]) AND (“mechanics” [MeSH Terms] OR “mechanics” [All Fields] OR “mechanical” [All Fields] OR “mechanic” [All Fields] OR “biomechanics” [All Fields] OR “biomechanic” [All Fields] OR “biomechanical” [All Fields]) AND (“suture” [MeSH Terms] OR “suture” [All Fields] OR “sutures” [All Fields] OR “sutural” [All Fields]).
(“human” [MeSH Terms] OR “human” [All Fields]) AND (“mechanics” MeSH Terms] OR “mechanics” [All Fields] OR “mechanical” [All Fields] OR “mechanic” [All Fields] OR “biomechanics” [All Fields] OR “biomechanic” [All Fields] OR “biomechanical” [All Fields]) AND (“suture” [MeSH Terms] OR “suture” [All Fields] OR “sutures” [All Fields] OR “sutural” [All Fields]).
(“suture” [MeSH Terms] OR “suture” [Title] OR “sutures” [Title] OR “sutural” [Title]) AND (“mechanics” [MeSH Terms] OR “mechanics” [Title/Abstract] OR “mechanical” [Title/Abstract] OR “mechanic” [Title/Abstract] OR “biomechanics” [Title/Abstract] OR “biomechanic” [All Fields] OR “biomechanical” [Title/Abstract]).
Screening and data collection
During the screening, a standardized form for the initial evaluation of titles and abstracts was applied, with key questions: “Does the research test human material?”; “Does it involve craniofacial sutures?”; and “Does it perform direct measurement of mechanical properties?.” Articles with all the three answers “YES” were included, and duplicates were removed.
Variables were identified as independent variables and outcome measurements, and information from each study was reported in respective tables. The quality of the information relative to protocol variables, source, and outcome measurements was rated while adopting a color code, that is, LIGHT GRAY = “proper/complete”; MEDIUM GRAY = “unclear/incomplete”; and DARK GRAY = “improper/missing.”
Results
Study selection
Out of 2278 articles identified from databases, 2224 were excluded during the title analysis. After screening, 54 articles were eligible for inclusion, eight additional articles were identified from previous literature reviews, and 33 more resulted from references of full-text articles. After the duplicate removal, 71 full-text articles were analyzed, resulting in seven studies included in the qualitative analysis, and three included in the quantitative analysis (Fig. 1).
Sample characteristics
The age of the subjects varied between 21-week-olds and 101-year-olds, with four studies involving infants or children (21-week-olds–6-year-olds), and two studies involving adults or elders (52–101-year-olds). Three studies did not declare the gender, and one involved only women. 24 The number of sources from which the samples were extracted was variable, ranging from 1 to 20. Except for the study of Davis et al., 24 in which it is clear that the source was a Caucasian, the ethnicity was not clearly stated by the others. Only six sutures were analyzed: the sagittal,13,28–31 the coronal,29–32 the lambdoid, 13 the metopic, 28 the frontozygomatic, and the zygomaticotemporal. 30 Davis et al. 24 did not declare which suture was analyzed. Apart from Grau et al. analyzing samples from surgical suturectomy of synostosed sutures on live patients, 28 all studies sampled the specimens from postmortem individuals. The sample sizes and specimen dimensions had some variation among the experiments, and different preservation methods were adopted, for example, specimens were tested fresh, fresh-frozen, fresh-refrigerated, and either embalmed or unembalmed (Table 1).
In case that the ethnicity of the source was not stated, despite nationality not having an equivalent meaning, the country where the study was conducted was reported between brackets. Light gray = “proper/complete”; medium gray = “unclear/incomplete”; and dark gray = “improper/missing.”
Load characteristics
Four studies applied a nonstatic load of undetermined modulus at a constant velocity. Coats and Margulies 32 applied an undetermined impact load, and, apart from the indentation adopted by Grau et al., 28 none of the studies applied a quasi-static load. Coats and Margulies 32 applied the load in tension with an axial displacement; the other studies applied either 3-point bending (3PB) or 4-point bending (4PB) with an orthogonal displacement, except Grau et al. 28 loading the specimen in indentation. None of the studies applied a compressive force and, apart from Grau et al. 28 performing a constant indentation, all the studies performed tests to failure. 28 Coats and Margulies 32 applied high velocities between 1.20 and 2.38 m/s, and the other studies chose lower velocities ranging from 0.00017 to 0.4 m/s. Coats and Margulies 32 analyzed a single event, Grau et al. 28 indented the specimens at 14 Hz, and the other authors adopted a continuous load regime. However, several studies did not clearly explain quality and quantity of the load (Table 2).
Light gray = “proper/complete”; medium gray = “unclear/incomplete”; and dark gray = “improper/missing.”
Measurements
Results from Hubbard et al. 13 were explained with a graphic representation only. On the other hand, three studies provided average values belonging to different sutures instead of their specific respective data, and Davis et al. 24 did not clarify which sutures were analyzed. Values of ultimate stress (σ, MPa), ultimate strain (ɛ, mm/mm), elastic modulus (E, MPa), and stiffness (K, N × m) are represented in Table 3. Eventually, only three studies reported the mechanical properties of the respective sutures analyzed (Table 4).
Light gray = “proper/complete”; medium gray = “unclear/incomplete”; and dark gray = “improper/missing.”
Discussion
The care of patients affected by craniofacial deformities can be complex and requires a multidisciplinary approach. 5 Treatment options may not be permanent because of the growth process in association with the need of early interventions. 5 In these regards, orthopedic treatments, including SDO, that is, without a surgical fracture, instead of DO, that is, requiring a surgical fracture, may present advantages. 7 SDO has already been applied in the treatment of craniosynostosis, 11 that is, the premature ossification of cranial sutures, and it is routinely performed during rapid maxillary expansion in case of a narrow upper jaw. 33
Although the study of SDO devices has received considerable interest by researchers so far, sutural growth is more likely a function of optimal parameters of mechanical stimulation that remain to be determined, rather than a particular type of orthopedic appliance to be used. 17 However, it seems that no previous work attempted to summarize the data on the biomechanical behavior of human sutures.
Because of the paucity of records included in the qualitative synthesis, and for the benefit of providing a complete overall description of the state of the art, all the studies were included in the discussion and their respective limitations were analyzed in due course (Tables 1, 2, and 3). Subsequently, specific attention was given to the studies included in the quantitative synthesis (Table 4 and Fig. 3).
This description may help in the understanding of the optimum forces required for SDO, and in enhancing the quality of numerical simulations through the finite element method as well.
Biomechanical properties
Most of the studies involved infants or children younger than 52 years. Conversely, Delille et al. 29 and Maloul et al. 30 involved adults or elders older than 6 years old. Ages in between were not considered and, since sutural development determines morphological changes such as in the amount of interdigitation 34 and sutures may progressively undergo ossification throughout adulthood, 35 mechanical properties can significantly be affected. Nevertheless, bone regeneration through SDO is of principal interest in growing subjects and the data related to infants and children are of primary importance (Table 1).
Specific evaluation for each suture is recommended, as different mechanical properties may derive from peculiar anatomy of each region. 36 As a consequence, averaging data of different sutures such as in the studies of Maloul et al. 30 and Delille et al. 29 may not be advisable because specific distraction forces might be required for each suture (Table 3).
Surprisingly, among the about 39 sutures present in the human head, the only ones analyzed were the sagittal,13,28–31 the coronal,29–32 the lambdoid, 13 the metopic, 28 the frontozygomatic, and the zygomaticotemporal 30 (Table 1). These sutures are all either cranial, that is, connecting cranial bones with each other, or craniofacial, that is, joining cranial bones with facial bones. Research interests should be directed toward facial sutures, that is, between facial bones, as well (Fig. 2).

Flowchart of the review process.
Although the use of specific load parameters should be justified by clear aims, for example, during application of static tension in spring-assisted cranioplasty, 37 the rationale of the choice of parameters was often unclear (Table 2). For example, no study applied a quasi-static load, which is probably the closest to the orthopedic movement when springs are used, 37 or fixed displacements that are representative of rigid distractors.7,33,38 Grau et al. applied a constant force on a nano-scale, 28 but only a microscopic part of the sutural ligament was loaded and it might be not well representative of the general sutural behavior. Surprisingly, notwithstanding the role of compressive stress in craniofacial orthopedics, 39 none of the studies applied such load type. The great variability found among results, such as ɛ ranging from 0.187631 to 1.5 mm/mm, 32 σ from 4.432 to 213 MPa, 30 and E from 0.528 to 1100 MPa, 24 underlines the importance of source, specimen, and load variables in the approach to the problem (Table 2). The proportionality between the increase of the strain, ergo the stress relative to the elastic modulus, and the amount of osteogenesis is valid until a certain threshold, after which the fibers may be extended beyond their elastic limits, restricting the sutural growth. 25 Thus, the success of SDO may be affected by the biomechanical parameters of the sutural ligament.
Load characteristics and biological response
Tensile stresses have been observed across several sutures during function, 18 and low-velocity tensional stresses are the foundation of SDO. Accordingly, in vivo animal studies revealed that tension could increase the width of the suture and the respective cell proliferation rate, leading to enhanced vascularization, matrix production, and mineralization.40–42 Further, low-speed tensional stress has high relevance in intracranial pressure and brain expansion, which may have direct 43 and indirect 44 consequences on sutural development. In fact, previous studies showed that skulls from infants with hydrocephalus may appear thin and enlarged. 45 Oppositely, a reduction of the intracranial pressure may be related to small and thick skulls with frequent synostosis. 46 Moreover, tensile strain was found to delay or prevent fusion of the metopic suture in rats. 47 Surprisingly, no study in humans has analyzed the biomechanical properties of the sutures simulating such relevant conditions.
On the other hand, if tensile stress is present in one area of the craniofacial skeleton, a compressive gradient is often present in an adjacent one. For example, compression at one suture may generate tension at others, as demonstrated both in humans 48 and animals. 49 Further, loading the dentition may produce mechanical stresses that are transferred to the sutures with both tensile and compressive strains.17,18 In addition, direct compressive forces, such as generated by head-gear devices in macaques,18,39 or indirect compression, as a result of mini-plates applied on elongating bony fronts of fetal lambs, 50 showed that osteogenic fronts lengthened less under compression, and presented a thicker bone with a narrowed suture, with some osteogenic fronts becoming resorptive. 39 Human intrauterine movements, which can be mainly considered compressive, were associated with the formation of cartilage and occasional synostotic connections in the sagittal suture. 51 In spite of the evident interest in compressive load regimes, no study was found discussing the mechanical parameters of human sutures under compression.
The present review could not find any mechanical test including cyclic loading, which has been demonstrated to characterize specific sutural features. Indeed, artificial cyclic loading in tension resulted in potentially stimulating both osteogenesis and osteoclastogenesis in animals, 52 showing greater osteogenesis related to cyclic loading compared with the static one. 53 On the contrary, compressive cyclic stimulation of low magnitude was found to cause fusion of the sagittal suture in rats, characterized by more cellular and collagen-rich osteogenic fronts but less mineralized growing bone tissue. 54
Despite the structural complexity of the suture can eventually translate forces of various orientation into localized shear stresses, 55 the fibers of the sutural ligament still tend to be oriented based on specific load-resistance requirements, 12 and the general mechanical response along different axes may not be uniform. With regard to this, since load orientation affects the optimal forces to achieve bone modeling during orthodontic tooth movement, 56 that is, the DO of the gomphosis and its periodontal ligament, it is reasonable to expect the suture to exhibit similar behavior.
Quantitative synthesis
Only three studies provided enough information to allow the attribution of their measurements to a clear context. These data were mainly related to infants and children and, although some details were missing or some nonhomogeneity existed among protocols, they still provided an important starting point for the understanding of the sutural behavior under loading. Especially, σ, ɛ, and E of the coronal suture were determined during impact tension, 32 during indentation at high frequencies, 28 and to failure during bending at low velocities. 31 In addition, E of the metopic suture was estimated during indentation at high frequencies 28 (Table 4 and Fig. 3).
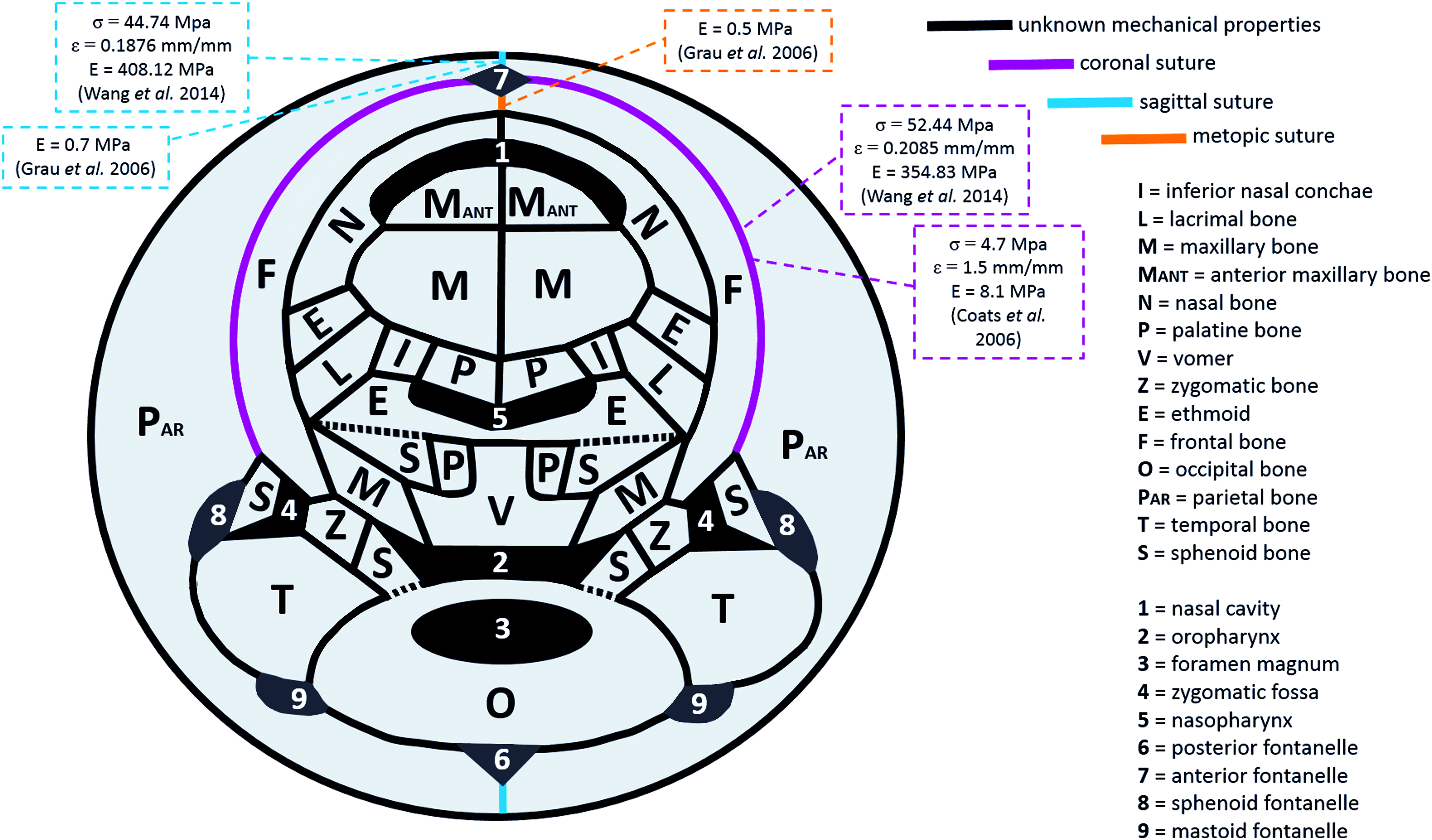
Schematic illustration of the human craniofacial sutures of known (colored) and unknown (black) biomechanical properties, with respective values. The spheno-occipital synchondrosis and the spheno-ethmoidal synchondrosis are dashed, since they are not synarthroses as the sutures. The ossicles of the ears (the malleus, the incus, and the stapes) and the mandibles were not represented. In order to illustrate all the actual articulations between bones, some bone are showed more times than the clinical reality (the sphenoid appears six times rather than one, the ethmoid appears three times instead of one, and the palatal bones and the nasal bones appear four times instead of two). Color images available online at www.liebertpub.com/teb
Even though some clinically relevant load types did not receive attention, other conditions were simulated such as impact loads in tension 32 (Table 4). In this regard, despite direct tension shocks are uncommon in humans, they may indirectly arise as a response to compressive impacts in a surrounding region. In this context, the role of sutures can be relevant in terms of energy absorption, as noticed by Jaslow and Biewener 57 and Jaslow 58 in goats. However, the complex sutural anatomy, associated with variable characteristics of the load, probably generates a composed displacement that is constituted by simultaneous bending and sharing as well. With regard to this, bending received extensive attention in previous mechanical evaluations,13,24,29,30 and the study by Wang et al. described the parameters of the human coronal and sagittal sutures 31 (Table 4).
Despite each suture probably deserving a specific analysis for each age stage, sutures of infants and children were described with ultimate stress in the order of 1 to 1 × 101 MPa, elastic modulus in the order of 1 to 1 × 102 MPa, and ultimate strain between 10% and 150%. For each suture, these parameters should be interpreted according to source, specimen, and load characteristics (Table 4 and Fig. 3).
Based on load type, the elastic modulus of the sutures was consistently lower than the values reported by previous studies on the cortical bone. In fact, the values of 354.83 ± 44.86 MPa of the coronal suture and 408.12 ± 59.08 MPa of the sagittal suture during bending 31 were lower than the cortical bone values of 17.85 ± 1.01 GPa undergoing bending as well. 59 Accordingly, sutures showed an elastic modulus of 7.6 ± 1.4 MPa during tension of the coronal suture 32 and higher values of 17.8 ± 2.1 GPa were reported for the cortical bone. 60 Lastly, the sutural ligament offered a resistance of 0.7 ± 0.2 MPa for the sagittal suture and 0.5 ± 0.1 MPa for the coronal suture, 28 compared with 25.8 ± 0.7 GPa of the cortical bone, 61 both of which were subject to indentation. Interestingly, for sutures, variations were larger than for bone, enhancing the importance to consider load orientation during SDO.
It is also worth to consider that, since sutures are integral parts of the skull, the reaction force resulting during clinical SDO does not represent the force applied only to the suture. In fact, it is the consequence of the reaction of the craniofacial skeleton as a whole, 62 rather than the resistance offered by the sutural ligament itself. As a consequence, despite in vitro studies showing that an optimal force to induce osteogenesis may exist, 63 the knowledge of the force experienced by the sutural ligament per se is still controversial. However, the strain is a far easier parameter to be measured during SDO 25 and, if the mechanical properties of the suture are known (Table 4 and Fig. 3), the force applied to the sutural ligament could be calculated.
The present review provided a summary of the currently available data for the indirect estimation of potentially optimal parameters for the SDO of the analyzed sutures. This information may contribute toward enhancing the rationale behind the calibration of the forces to be adopted during SDO for specific sutures and subjects. Further, the reported values are applicable to calculations of the general biomechanics of the craniofacial skeleton, for example, in case of stress evaluation during physiological functions such as mastication 12 or to analyze its mechanical response in other conditions such as trauma. 32
Limitations
Regarding the source, although visually closed sutures of macerated human heads showed some degree of bone movement under orthopedic forces, 64 and animal studies revealed that sutural strain patterns are similar between dry skull models and in vivo, 65 the magnitude of bone strain in postmortem material may exhibit higher stiffness. 65 Moreover, the interpretation of the results should take into consideration the anatomical levels as well. For example, the analysis of nano-mechanical properties by Grau et al. 28 might be more related to single components of the sutural ligament, such as fibers or vessels, rather than being representative of the response of the suture as a whole. In fact, despite authors analyzing synostosed sutures, which are supposed to have a higher degree of ossification leading to increased rigidity, the elastic modulus of the sagittal suture (0.7 ± 0.2 MPa) was lower than what was reported by Wang et al. for the same suture (408.12 ± 59.08 MPa) 31 (Table 4 and Fig. 3).
Regarding the testing protocols, although the real surface area of the sutural interface is often not planar, it has been a common assumption of the specimen to act as a beam, and to use its simple geometrical cross-section in the mechanical calculation.13,29,31,32 A better approximation may be achieved by measuring the actual cross-sectional surface by using more detailed techniques such as micro-computed tomography, 24 and the degree of interdigitation should be considered in the interpretation of the results because it influences the extension of the sutural interface. 30 In addition, even though the strain generated in the suture is typically an order of magnitude larger than the strain present in the adjacent bone, 12 assuming the bone to be nondeformable and, subsequently, relating the deformation to the sole sutural ligament may overestimate its strain values.
Despite the mentioned limitations in both data acquisition and computation, the values summarized in the present work provide a reasonable estimation of the mechanical behavior of sutures. These parameters are relevant especially compared with the representation of the sutural ligament with values related to bone 66 or other soft tissues, 67 as reported in previous studies.
Conclusions
This first attempt to summarize the biomechanical properties of the human sutures under loading revealed that only six sutures out of the about 39 sutures were analyzed. Besides the frequent clinical application of distractors on the face, cranial sutures received far more interest than facial ones. The data that were provided with sufficient information to identify source and load characteristics, were mainly related to infants and children, and described mechanical parameters of the coronal, sagittal, and metopic sutures.
These findings may help to estimate the forces transferred to the sutural ligament during SDO when the strain is measured, and to advance the rationale of the application of certain parameters to optimize the clinical outcome. Still, although sutures offer the possibility to modify the craniofacial growth through distraction techniques, little is known about the optimal forces required for SDO, and their therapeutic potential is probably far from being used in its completeness.
Footnotes
Acknowledgment
This study is part of the PhD thesis of Dr. F.S., which is supported by The Hong Kong PhD Fellowship Scheme 2014–2015 of the Research Grants Council of Hong Kong.
Disclosure Statement
No competing financial interests exist.