
Abstract
Reconstruction of degenerated temporomandibular joint (TMJ) structures remains a clinical challenge. Tissue engineering (TE) is a promising alternative to current treatment options, where the TMJ is either left without functional components, or replaced with autogenous, allogeneic, or synthetic grafts. The objective of this systematic review was to answer the focused question: in experimental animal models, does the implantation of biomaterial scaffolds loaded with cells and/or growth factors (GFs) enhance regeneration of the discal or osteochondral TMJ tissues, compared with scaffolds alone, without cells, or GFs? Following PRISMA (Preferred Reporting Items for Systematic reviews and Meta-Analysis) guidelines, electronic databases were searched for relevant controlled preclinical in vivo studies. Thirty studies reporting TMJ TE strategies in both small (rodents, rabbits; n = 25) and large animals (dogs, sheep, goats; n = 5) reporting histological and/or radiographic outcomes were included. Twelve studies reported ectopic (subcutaneous) implantation models in rodents, whereas 18 studies reported orthotopic, surgically induced defect models in large animals. On average, studies presented with an unclear-to-high risk of bias. In most studies, mesenchymal stem cells or chondrocytes were used in combination with either natural or synthetic polymer scaffolds, aiming for either TMJ disc or condyle regeneration. In summary, the overall preclinical evidence (ectopic [n = 6] and orthotopic TMJ models [n = 6]) indicate that addition of chondrogenic and/or osteogenic cells to biomaterial scaffolds enhances the potential for TMJ tissue regeneration. Standardization of animal models and quantitative outcome evaluations (biomechanical, biochemical, histomorphometric, and radiographic) in future studies, would allow more reliable comparisons and increase the validity of the results.
Background
T
The most common subtypes of TMDs include (1) pain-related disorders, such as myofascial pain and arthralgia, (2) TMJ-related diseases, such as internal derangements (IDs), and (3) osteoarthritis (OA) and arthritis. IDs are defined by an abnormal position of the TMJ disc relative to the condyle and eminence, and are reported to affect between 20% and 90% of TMD patients.7–9 Degenerative joint disease is a frequent finding in the TMJ 10 —which can alter the TMJ structures, that is, subchondral bone and fibrocartilage. 11 Approximately 5% of these TMDs do not respond to conservative treatment, and are considered for surgery. 12 Surgical treatment includes arthrocentesis, arthroscopy, condylotomy, disc repositioning, partial or complete disc removal (discectomy), arthroplasty, and removal with replacement of the condyle, fossa, or both components with a TMJ prosthesis.8,13–17
TMD progression has been surgically categorized through imaging from “normal” to “severe” and “catastrophic changes,” where few or none of the TMJ components are salvageable. 18 In these cases, patients may experience constant pain with painful crepitus and mild limitations of mouth opening. Radiographically, there are signs of changes in the condylar morphology such as flattening and beak-shaped deformities of the condylar head, and the clinical picture is that of severe IDs with early OA. 18 In these cases, discectomy, that is, removal of the diseased disc, is often performed, but whether this treatment alone is effective in the long term, or if it leads to further degenerative changes, is still unclear.8,19–22 Therefore, to avoid progressive degenerative changes following discectomy, and in severe cases, ankylosis of the mandible to the temporal bone, placement of an interpositional material is often recommended. 13 Due to several reports of clinical failures and complications with alloplastic implants, for example, infections and foreign body reactions, autogenous grafting materials have been preferred.23–26 Current treatments include temporal muscle/fascia flap, dermis, fat, or a combination of dermis and fat. However, due to lack of long-term stability, scar tissue formation, donor-site morbidity and difficulty in anchoring these graft materials—there is to date no ideal TMJ disc replacement material. 23 Moreover, if the remodeling capacity of the load-bearing joint is exceeded, the TMD may advance into OA or arthritis, which leads to progressive cartilage degradation, subchondral bone remodeling, erosion, and flattening of the condylar surface, synovitis, and chronic pain.10,27,28
Due to the limitations of current technologies for the treatment of patients with severely debilitating end-stage TMDs, new technologies using autogenous grafts, alloplastic implants, or their combinations, with the potential to replace anatomic components, are being investigated. 11 In this regard, tissue engineering (TE) strategies offer a promising alternative for regeneration of damaged or lost TMJ structures, especially in “severe” TMDs, where few joint components are salvageable. 18 The TE approach often involves the use of one or a combination of the following: progenitor cells (most commonly mesenchymal stem cells [MSCs]), usually harvested from an autologous source (e.g., bone marrow [BM], adipose tissue, etc.); inductive signaling molecules or growth factors (GFs); and an appropriate carrier scaffold for implantation in vivo. 29 The “triad” of multipotent cells, inductive and conductive scaffolds, replicate the properties of the native tissue, without the need for invasive secondary tissue harvesting and donor-site morbidity.30,31
Preclinical testing of new regenerative therapies in clinically relevant animal models is an important aspect of translational research and, in most cases, a requirement of regulatory health agencies before initiating human clinical trials. 32 The advantage of animal models, in addition to testing therapeutic safety and efficacy, is the possibility for better understanding of the underlying biological processes through methods that may be considered too invasive for human applications (e.g., repeated harvesting of biological samples, biopsies, etc.). 33 Small animal models (rodents and rabbits) usually constitute a starting point for proof-of-principle or feasibility studies, whereas studies in large animal models (dogs, pigs, sheep, and nonhuman primates) attempt to simulate clinical conditions more closely and predict therapeutic efficacy.34,35 Experimental animal models may be further categorized as ectopic, that is, evaluation of tissue regeneration in a non-TMJ-specific site, for example, subcutaneous or intramuscular, usually in small animals, or orthotopic, that is, evaluation of regeneration in chemically or surgically created defects in TMJ tissues. Several authors have proposed in vivo models, both ectopic and orthotopic, in small and large animals to study the effect of various treatments on TMJ regeneration. Therefore, the aim of the present study was to systemically review the available literature to answer the focused “PICO” (population, intervention, comparison, and outcome) question: in experimental animal models, does the implantation of biomaterial scaffolds loaded with cells and/or GFs enhance regeneration of discal or osteochondral TMJ tissues, compared with scaffolds alone, without cells, or GFs?
Materials and Methods
Study design
A review protocol was developed based on the Preferred Reporting Items for Systematic reviews and Meta-Analysis (PRISMA) guidelines, 36 and predetermined inclusion/exclusion criteria.
Inclusion criteria
Studies with English language abstracts, aiming for regeneration of TMJ structures.
Randomized or nonrandomized controlled animal experimental studies with at least one experimental group and a control group.
Transplantation of cultured autologous, allogeneic or human-derived chondrogenic cells (MSCs or chondrocytes [CC]) and/or GFs, with or without a scaffold in at least one experimental group.
A control group receiving an autologous graft, a scaffold without cells/GFs, or no implant. Studies that included a control group receiving a different TE implant than the experimental group were also included.
Histological (qualitative and/or quantitative [histomorphometry]) and/or radiographic (computed tomography [CT], cone-beam CT [CBCT], micro-CT [μ-CT], and/or magnetic resonance imaging [MRI]) evaluation of outcomes.
Exclusion criteria
In vitro studies
Absence of control group.
Scaffold-free TE strategies
Search strategy, screening, and study selection
Electronic databases of MEDLINE (through PubMed) and Web of Science were searched for relevant English literature up to and including November 2017. Unpublished literature was searched for through Google and Google Scholar search engines. Bibliographies of the studies selected and relevant review articles were checked for crossreferences. A specific search strategy was developed for MEDLINE and Web of Science (see the Supplementary Table S1; Supplementary Data are available online at www.liebertpub.com/teb). Titles and abstracts of the search-identified studies were screened by two authors (E.H. and S.S.) and full texts of all eligible studies were obtained. Uncertainty in the determination of eligibility was resolved by discussion with the other authors. Two authors (E.H. and S.S.) reviewed the selected full texts independently and final inclusion was based on the aforementioned inclusion criteria. A summary of the screening process is presented in Figure 1.
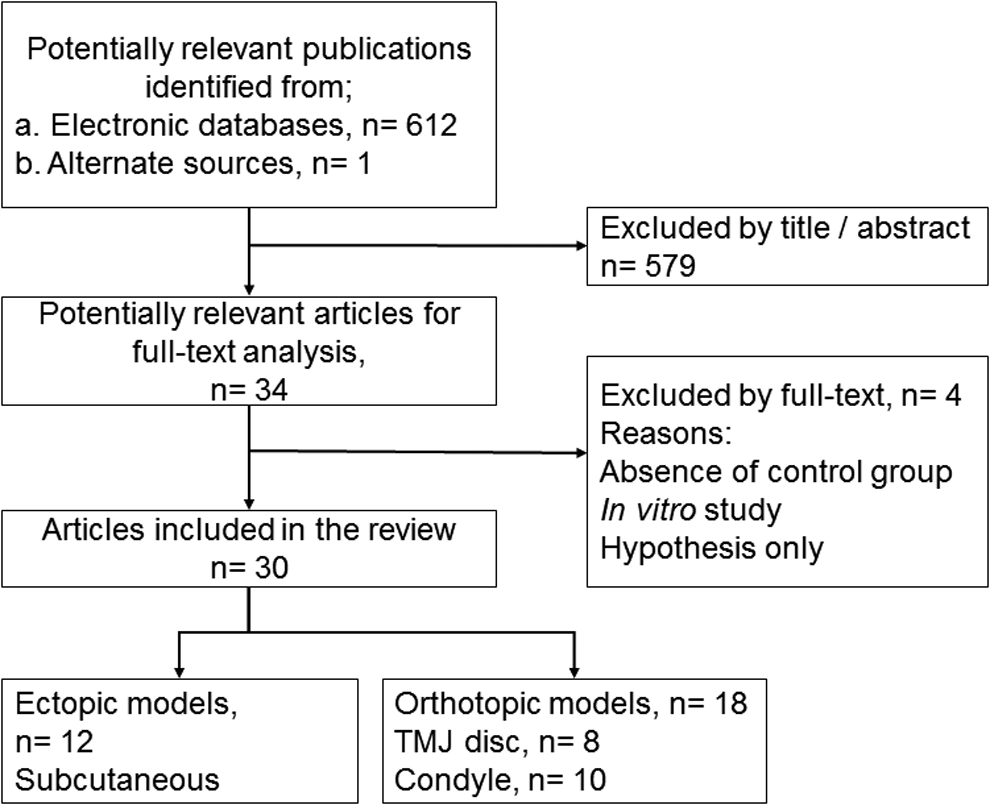
Flowchart for study screening and selection. n, number of articles; TMJ, temporomandibular joint.
Data extraction
Data were extracted from the full texts of selected articles on: author(s), study design, animal species; strain, age and gender, model type, number of animals (n), observation time(s), cell type, source and number, induction of cells, scaffold biomaterial(s), GF(s), control group(s), outcome(s), method(s) of outcome evaluation, main findings, and conclusions. Descriptive summaries of studies included were entered into tables. Due to high heterogeneity among included studies, a meta-analysis was not performed.
Quality assessment and risk of bias
Reporting quality assessment of all studies was performed based on a modification of the ARRIVE (Animal Research: Reporting In Vivo Experiments) guidelines regarding relevant items37,38 (Supplementary Table S2). Compliance with the guidelines was evaluated using a predefined grading system applied to each of the 20 items. 39 Reporting quality was judged as “high,” “moderate,” or “low.” Risk of bias (RoB) assessment was performed using a modification of SYstematic Review Center for Laboratory animal Experimentation (SYRCLE) RoB tool for animal studies, and graded as “high,” “low,” or “unclear” 40 (Supplementary Table S3). Any disagreement between the reviewers during study selection, data extraction, and quality assessment was resolved by discussion and consensus.
Results
Search results and study characteristics
Of the 613 search-identified studies, 30 studies41–70 performed in mice (n = 12), rabbits (n = 13), dogs (n = 2), goats (n = 2), and sheep (n = 1), were included in the review. Excluded studies by full-text and reasons for exclusion are reported in the Supplementary Table S4. The included models were either ectopic (n = 12)42–44,48,50–52,57–59,62,63 or orthotopic (n = 18)41,45–47,49,53–56,60,61,64–70 (Tables 1 and 2). All ectopic models included were subcutaneous implantation on the dorsum of mice. Orthotopic models were performed in the TMJs of rabbits (n = 13),41,46,47,49,53–56,60,67–70 dogs (n = 2),65,66 goats (n = 2),61,64 and sheep (n = 1). 45 Sample sizes ranged from 2 to 25 and 5 to 60 animals in ectopic and orthotopic models, respectively. Observation times varied between species: mice (2–12 weeks), rabbits (3 weeks to 12 months), goats (12–24 weeks), and sheep (4 months).
Allo, allogeneic; ASC, adipose-derived stem cells; Athy, athymic; bFGF, basic fibroblast growth factor-modified cells; BMP-7, bone morphogenetic protein 7-modified cells; BMSC, bone marrow-derived stem cells; CaSO4, calcium sulfate; C, chondrogenic; CC, chondrocytes; FB, fibroblast; FLP, forelimb periosteum; FLS, fibroblast-like synoviocytes; FCSC, fibrocartilage stem cells; GFs, growth factors; GHJ, glenohumeral joint; HA, hydroxyapatite; IC, immunocompromised; n, number of animals; NR, not reported; O, osteogenic; OB, osteoblasts; PCL, polycaprolactone; PEGDA, polyethylene glycol diacrylate; PGA, poly glycolic acid; PLA, poly-
ASC, adipose tissue-derived stem cells; Auto, autologous; BM, bone marrow; CTGF, connective tissue growth factor; DO, distraction osteogenesis; EC, Eastern Cross goats; FGF, fibroblast growth factor; GFP, green fluorescent protein; H, house rabbits; inj, injection; JA, Japanese rabbits; LIPUS, low-intensity pulsed ultrasound; m+f, male and female; NELL-1, NEL-like protein-1-modified cells; NZ, New Zealand White rabbits; OC, osteochondral; PLGA, poly lactic-co-glycolic acid; PRP, platelet-rich plasma; rhBMP-2, recombinant bone morphogenetic protein-2; TE, tissue engineering; TGF-β, transforming growth factor beta; UB-ECM, urinary bladder extracellular matrix.
Risk of bias
Most studies provided adequate information regarding title, abstract, background, study objectives, ethical approval, experimental design, and procedures (Fig. 2). Information about housing and husbandry was generally inadequate and the majority of studies lacked complete information regarding animals' age and/or gender (Tables 1 and 2). No studies reported information on sample-size calculation and half of them provided basic baseline characteristics of the animals. In seven studies, (23%) animals were randomly allocated to different treatment groups to minimize selection bias, although no details of the randomization procedure were reported. Two studies (15%)45,64 reported blinding of outcome assessors to treatment groups, to minimize detection bias. Most studies reported detailed outcome evaluation, including statistical analyses, and some reported information on adverse reactions or complications. Overall, RoB in most studies was judged to be unclear (Fig. 3). Information regarding study limitations and implications for translation to human models was limited, and none of the studies referred to the principal of the “3Rs” (replacement, refinement, and reduction) for experimental models. 37

Frequency distribution (%) of the scores assessed for each item of the modified ARRIVE guidelines in all studies included. Items 2, 3, 5, 7–10, 12, 13, and 15–20 were scored 0, 1, or 2 (clearly inadequate, possible adequate, or clearly adequate). All other items scores 0 or 1 (no or yes).

Frequency distribution (%) of the risk of bias assessment for each item of the modified SYRCLE RoB tool in all studies included. Items 1–8 were judged as “yes,” “no,” or “unclear”; items 9 and 10 were judged as “yes” or “no” (risk of bias; yes = low, no = high, unclear = unclear). SYRCLE RoB, SYstematic Review Center for Laboratory animal Experimentation Risk of Bias.
Characteristics of animal models
Ectopic models
One, three, and eight studies reported ectopic models for synovial membrane 50 disc regeneration48,51,59 or condylar regeneration,42–44,52,57,58,62,63 respectively. All studies involved subcutaneous implantation on the dorsum in mice (Table 1).
Orthotopic models
Eight and 10 studies reported orthotopic models of disc regeneration41,49,55,65–69 or condylar regeneration,45–47,53,54,56,60,61,64,70 respectively. Orthotopic models involved surgically created disc defects (n = 5) in rabbits49,55,67–69 or disc removal (n = 3) in rabbits 41 or dogs.65,66 Condylar regeneration models included surgically created defects (n = 7) in rabbits46,53,54,60,70 or goats,61,64 or condylectomy models (n = 3) in rabbits47,56 or sheep 45 (Table 2).
Characteristics of TE strategies
Scaffolds
The majority of studies reported the use of scaffolds—either natural,44,47–50,53,54,59,60,62,63,65–70 synthetic,41–43,46,51,52,55,58,61,64 or a combination of natural and synthetic biomaterials.45,56,57 Fifteen studies reported the use of a single natural scaffold material, like collagen,48–50,53,54,60,67–70 coral,44,62,63 or porcine urinary bladder extracellular matrix (UB-ECM).65,66 Two studies used a composite natural polymer scaffold—UB-ECM in combination with collagen sponge
47
or fibrin/chitosan.
59
Four studies reported the use of a single synthetic polymer scaffold material—either poly-
Cells
The use of a variety of cells was reported—whole BM, bone marrow-derived stem cells (BMSCs), adipose tissue-derived stem cells (ASCs), synovial-derived MSCs (SDMSCs), fibrocartilage stem cells (FCSCs), CC, osteoblasts, or fibroblast-like synoviocytes (FLSs). The most frequent reported cell-type was BMSCs (n = 10); two studies reported the use of gene-modified BMSCs using NEL-like protein-1 (NELL-1)—a chondrogenic-inducing factor of BMSCs, 64 or basic fibroblast growth factor (bFGF). 62 In addition, one study 52 reported the use of bone morphogenetic protein 7 (BMP-7)-modified human fibroblasts. Four studies reported the use of autologous BMSCs,47,64 ASCs, 41 or BM. 49 Four studies reported the use of human cells—BMSCs from iliac crest 62 or condyle, 63 fibroblasts from gingival, 52 or FLSs from the TMJ synovial membrane. 50 Six studies reported the use of CC alone51,60,61 or in combination with either osteoblasts, 58 fibroblasts, 52 or BMSCs. 57 Three studies reported chondrogenic induction of ASCs, 41 SDMSCs, 59 or CC 57 before implantation. Six studies reported osteogenic induction of cells—either alone, 44 or in addition to chondrogenic induction,42,43,47,62,63 before implantation.
Growth factors
Six studies reported the use of GFs, such as BMP-2,53,56 transforming growth factor β3 (TGF-β3) combined with connective tissue growth factor (CTGF), 55 platelet rich plasma (PRP), 45 fibroblast growth factor 2 (FGF-2), 54 or TGF-β1+BMP-246—either alone46,53–56 or in combination with cells 45 (Table 2).
Outcome measures
Biochemical
Two studies reported assessments of organic contents of regenerated tissue in the implanted constructs of aggrecan, collagen type-I (Col-I) and collagen type-II (Col-II), 41 and glycosaminoglycan (GAG), 65 respectively. Other studies also immunohistochemically assessed organic contents of regenerated tissues, such as Col-I,43,59,61,62,69 Col-II,43,59,61,62,64,69 and collagen type X. 43
Biomechanical
Two studies51,65 performed biomechanical testing of the TE constructs. Cylindrical samples with a diameter of 4 and 6 mm were measured by hydrodynamic closed chamber compression testing 51 or MTS mechanical testing apparatus, 65 respectively. Two studies45,55 measured mechanical properties (e.g., compressive modulus and ultimate strength) of the scaffolds, preimplantation.
Histological
All included studies reported histological evaluation of tissue regeneration of discal or osteochondral tissues. Two studies65,66 additionally reported evaluation of regenerated vessels, muscles, and ligaments. In addition to qualitative histology, two studies45,47 reported quantitative histomorphometric outcomes of condyle regeneration, that is, percentage of bone regeneration calculated as a ratio of the regenerated bone tissue volume (or area) divided by the total defect area. Five studies46,56,57,61,64 reported semiquantitative evaluation of histological outcomes using predefined grading/scoring systems.
Radiographic
Eight studies reported radiographic evaluation of tissue regeneration, using μ-CT,47,64 CBCT, 41 MRI,46,51,67 or conventional 2D radiography.44,62 Both studies using μCT reported quantitative outcomes, whereas CBCT, MRI, and 2D radiography reported qualitative outcomes only.
Discussion
The aim of this study was to systematically review preclinical studies using scaffold-based TE strategies for TMJ regeneration. Overall, the results showed that TE strategies with implantation of biomaterials with cells or GFs, resulted in superior regenerative outcomes compared with implantation of biomaterials alone. Furthermore, implantation of scaffold alone was superior to no implant/empty defect. Systematic reviews and meta-analyses of in vivo experiments can be useful to detect knowledge gaps, for the design of future preclinical and clinical trials, to detect treatment effects, and to improve the methodological quality. 71 Guidelines for the design of preclinical animal models have been proposed in the context of bone tissue engineering (BTE), and may be extrapolated to TMJ TE. The guidelines suggest that the selected animal model should (1) simulate the target clinical and biological environment, (2) allow the use of quantifiable parameters to evaluate success and functional performance of regenerated tissues, and (3) allow detection of clinically relevant differences in biological performances between the regenerative therapies assessed. 72 Consideration of these guidelines is critical when selecting the appropriate animal model and species to test new therapeutic interventions.
Animal models
In the present review, the majority of the studies reported the use of small animal models. In musculoskeletal research, small animal models primarily include two species—rodents (i.e., rats and mice) and rabbits. 73 Significantly lower costs, easier housing and handling, and minimal social concerns are some of the reasons why they are preferred. 74 The possibility to define and control the genetic background of the experimental animals creates less variation and need of fewer animals to achieve statistically valid data. 75 Thus, small animals usually constitute a starting point for proof of principle studies 32 using ectopic models, which evaluate tissue regeneration in a distant site, most commonly subcutaneous, as was observed in the present review. The lack of endogenous chondrogenic and/or osteogenic cells, cytokines, and mechanical factors (all of which can potentially stimulate cartilage and bone formation) within the local intradermal environment, ensures that, theoretically, any resulting cartilage or bone formation after cell and/or scaffold transplantation is of exogenous origin. 76 In addition to their low cost, immunodeficient animals allow xenograft-based experiments, and their lax skin permits large-volume implants. 76 However, separating the implant from surrounding tissue, and migration of small implants in the lax skin, can be challenging in subcutaneous implantation models. 76 Ectopic models in the included studies were performed in immunocompromised mice and aimed for disc,48,51,59 synovial membrane, 50 or condyle42–44,52,57,58,62,63 regeneration. However, a major drawback using mice in TMJ TE studies is the physical difficulty of an orthotopic approach, due to limitations in size of the joints.77,78 Rabbits provide the same advantages as rodents, in terms of their small size and easy handling, but are large enough to allow experimental TMJ surgery.41,49,55,79 A majority of included studies reported the use of orthotopic models in rabbits. Orthotopic models are performed in an environment with the presence of tissue-specific endogenous factors and cells. 72 Rabbit TMJ discs share many similarities to humans, given their biochemical composition, morphology, collagen fiber organization, and attachments.80–82 They may therefore more closely reflect the human clinical situation when compared with ectopic models in rodents. At the same time, results of (osteo)chondral regeneration in rabbit models should be interpreted with caution, due to the high potential for spontaneous healing reported in orthopedic experimental models, and considerable differences in size and loading conditions, as compared with the human situation.83–85
Although no single species can provide the optimal experimental model for TMJ research, 86 large animal models are reported to more closely mimic the clinical situation and predict therapeutic efficacy. 75 High costs, ethical issues (e.g., in the case of dogs), and handling difficulty (e.g., in the case of pigs) are some limitations of large animals. 79 In context, mini pigs represent a more suitable model because of more easily handling than farm pigs 86 and morphological similarities to human bone and TMJ structures than other large animal models.34,87 There has been an increase in preclinical in vivo publications on TMJ-related research along with a considerable change in species used, 78 which may partly be explained by the high costs and pressure from animal protection groups. 81 In the present review, orthotopic models in large animals were used for regeneration of the TMJ disc in dogs,65,66 and condyle, in either sheep 45 or goats.61,64 The TMJ of the dog has a slight laterotrusion movement, 88 although it is a hinge joint and mainly rotate. Considering that dogs are carnivores, 86 their TMJ loading is reportedly greater than that of both rodents and primates, 78 and may more closely mimic the strain in a human joint. Sheep TMJ disc and condyle anatomy have similarities to humans, in addition to easy surgical access, and have therefore been proposed as a prime model for TMJ research, 89 despite the fact that both sheep and goats are herbivores and mainly have translational TMJ function. 86 No studies reported TMJ models in pigs or mini pigs, which have been reported to most closely resemble human TMJ disc morphology,80,87 anatomy, and function.87,90,91 However, additional drawbacks to high cost, as difficult surgical access through lateral prearuicular approaches, due to the zygomatic arch anatomy, might be the explanation. 87
TE strategies
Ectopic models—subcutaneous implantation
All included ectopic studies involved subcutaneous implantation of GF-free scaffolds with or without cells, aiming for disc, synovial membrane, or condyle regeneration. Qualitative histological evaluations of outcomes were reported in all studies, whereas only one study 57 reported semiquantitative assessment using a predefined grading scale. A majority of studies reported superior outcomes with cell-seeded scaffolds (most commonly BMSCs) compared with cell-free scaffolds, and with (chondrogenically) differentiated cells compared with undifferentiated cells. One study reported the use of TMJ synovium-derived cells. Interestingly, synovium-derived MSCs from the knee joint have been reported to possess higher chondrogenic potential than MSCs from various tissue sources, including BM and adipose tissue. 92 A variety of biomaterials were used for scaffold fabrication, most of them composites of synthetic polymers, to mimic the natural composition of the native TMJ structures. However, heterogeneity between studies (in terms of study design, models, observation times, etc.) and the lack of quantitative measurements make the results less comparable. Moreover, since translation of results from ectopic models to the clinical situation is challenging, due to frequent use of immunocompromised animals, lack of mechanical stimulation, and biochemical environment, 76 the discussion herein will be focused on results from studies reporting orthotopic TMJ models.
Orthotopic models simulating clinical TMDs
Disc regeneration
Orthotopic models related to TMJ disc disorders included either disc perforations or total discectomy with replacement. Disc perforations are associated with IDs and a major cause of TMD symptoms, especially in patients with TMJ OA.93–95 Such cases may be treated with regenerative approaches, whereas discectomies are usually performed in cases of severely damaged or displaced discs, which seriously inhibit jaw function and are no longer salvageable. 18
Two included studies reported TE strategies to repair surgically created disc defects, of either 1.6 or 2.5 mm, in rabbits.49,55 The TMJ disc defect model aims to simulate disc perforations commonly associated with IDs, 96 and can be compared with the calvarial critical-size defect model (CCSD) often used in BTE research. 79 CCSD is considered the smallest-size experimental defect in the cranium of the animal that will not heal spontaneously and completely regenerate bone within a defined period without intervention,97,98 and reliable dimensions of CCSD have been established in different animal models.98,99 Critical-size defects have been reviewed in different animals in the context of hyaline articular cartilage of long bones.83,85 In the context of TMJ discs, 1 mm incisions have been reported to spontaneously heal after 6 months in mature goats (2 years old). 100 Defect sizes between 1.6 mm (rabbits) and 6 mm (monkeys), have been reported in the literature,49,101 although reliable evidence for what may be the optimal size of a nonhealing or critical-size defect in specific animal models, with the exception of goats, is currently lacking. This is further complicated by the limited intrinsic healing capacity of avascular articular cartilage and the differences in structure of TMJ components between different animals. 83 However, standardization of animal models is important to allow reliable comparisons between different studies. Only one included study 49 used empty defects (1.6 mm) in a control group to investigate spontaneous healing in rabbit TMJ discs, although it may be argued that the observation times (4–8 weeks) could have been extended to confirm no spontaneous healing. Nevertheless, both included studies49,55 reported superior healing outcomes following implantation of PLA or PCL/PLGA scaffolds, combined with cells (ASCs) or GFs (TGF-β3+CTGF), respectively, compared with scaffolds alone, in rabbit TMJ defects.
Three included studies reported total discectomy with replacement in dogs65,66 or rabbits, 41 thus leaving the TMJ without a functional component that facilitates smooth movements and stability against tensile, compressive, and shear forces. 102 The excised discs were replaced with either bioscaffolds (UB-ECM)65,66 (i.e., decellularized tissue 103 ) or PLA scaffolds seeded with either undifferentiated or chondrogenically differentiated (with TGF-β1) ASCs. TGFs, for example, TGF-β1 and TGF-β3, are reported to be potent inducers of MSC chondrogenic differentiation.104,105 After 6 and 12 months, joints with differentiated cell-seeded scaffolds showed enhanced condylar integrity compared with undifferentiated cells. Another included study 43 reported superior outcomes with differentiated BMSC in an ectopic model. Advantages of using differentiated versus undifferentiated cells for cartilage regeneration have been discussed. 106 In the former study, 41 the challenge of stabilizing the bioengineered disc was highlighted, and this could potentially present a challenge in clinical situations.11,107,108 Thus, it would be desirable to also regenerate the supporting discal tissues, such as muscles and ligaments. 109 Two included studies65,66 observed the presence of skeletal muscle bundles in the periphery of the remodeled scaffold, when using acellular UB-ECM scaffolds, secured with slow resorbing sutures. No included studies applied animal models for IDs and anterior disc displacement, although attempts to simulate these clinical conditions have been previously reported.110–112
In the context of TMJ disc regeneration, scaffold selection is critical, given the complex nature and composition of the native fibrocartilaginous structures. Scaffold material can have a significant impact on regenerative outcomes. For example successful regeneration of TMJ discs has been reported in studies using cell-free collagen scaffolds 68 or bioscaffolds, 103 such as porcine UB-ECM,65,66,68 whereas others have reported fibrous tissue formation only, when using cell-free PCL/PLGA 55 or PLA/PGA 51 scaffolds. The abovementioned bioscaffold demonstrated functional tissue formation, without scarring or encapsulation. However, additional antigen removal strategies to decellularization may aid in translation of allogeneic organ-derived scaffolds. 113
Novel approaches, such as 3D (bio)printing, can offer advantages with regard to scaffold fabrication, for example, high precision, accuracy, and the ability to fabricate complex shapes with homogenous cell distribution, and to mimic the native ECM.114,115 In one included study, 55 polymeric disc constructs were 3D printed to accomplish zonal recapitulation by incorporating specific GFs (TGF-β3+CTGF) within PLGA microspheres in different regions of PCL scaffolds, as a controlled spatiotemporal delivery system. In the context of knee meniscus, compositional differences in the meniscus' inner and outer regions are reported to make regeneration challenging. 108 Similar compositional differences have been reported within TMJ discs,107,116 thus demanding different regenerative strategies in different zones of the same tissue. A previous study reported a similar zonal recapitulation approach with GFs (TGF-β3+CTGF) incorporated in 3D printed PCL/PLGA scaffolds to reconstruct knee meniscus (after meniscectomy) in a sheep model, 117 as for TMJ disc (defect) regeneration in rabbits. 55 Interestingly, in the latter study, complete degradation of the PCL/PLGA scaffold and replacement by new tissue after 4 weeks in vivo was reported. This is in contrast to another included study, 57 reporting considerably slower degradation of PCL; previous literature has reported a degradation time of ∼2 years.57,118 In the former study, 55 the superior degradation of PCL was attributed to the high surface-to-volume ratio and PLGA integration within the scaffold. Moreover, differences in defect/construct sizes might explain the variation in results between studies. However, 3D printing is restricted to the use of biomaterials with desired printable properties, and the production time increases with complexity of the printed structures. 119 Nevertheless, 3D printing has overcome many limitations of conventional scaffold fabrication techniques, and serves as a promising tool for cartilage and bone TE.120,121
Condyle regeneration
Chronic or untreated OA may ultimately lead to degenerative structural changes in the TMJ. This is further complicated by the avascular nature and limited regenerative capacity of TMJ fibrocartilage. 122 Condyle defects, which may be a result of a degenerative OA progression, are often used in animal models to test regenerative therapies. In the present review, condyle defects in small (rabbits) and large (goats) animals were regenerated with the use of scaffolds in combination with either cells60,61,64,70 or GFs.46,53,54 All studies reported superior healing outcomes with cell- or GF-loaded constructs, compared with cell- or GF-free constructs of natural or synthetic polymer materials. Natural polymers are highly biocompatible and biodegradable. However, rapid enzymatic degradation and poor mechanical properties make them less optimal for load-bearing scaffold materials. Synthetic polymers are versatile and the properties can be manipulated and tailor made to a great extent. 123 On the other hand, these materials may not be efficient in functionalizing CC and do not match the natural polymers' structural compatibility to the native cartilage tissue. 124 Two of the three studies53,54 that implanted cell-free scaffolds with GFs showed enhanced healing compared with empty defect and one 46 reported no semiquantitative differences between scaffolds with or without GFs.
In severe cases of condylar injury, for example, ankylosis following trauma; or in skeletally immature patients with acquired TMJ pathologies, for example, hemifacial macrosomia, Treacher Collins syndrome etc.; or hyperplasia, tissue-engineered condyle implants may be beneficial.11,57 In the present review, three studies performed condylectomy with replacement, using scaffolds loaded with cells 47 and/or GFs.45,56 Results showed that bone regeneration was enhanced by (1) cell delivery with low-intensity pulsed ultrasound (LIPUS) treatment compared with cell-loaded scaffolds alone, 47 and (2) scaffolds loaded with PRP and BMSCs compared with empty scaffolds. 45 Meanwhile, condyle implants of scaffolds with GFs showed no differences between the groups receiving rhBMP-2 or not. 56 This is in accordance with another study, where condyle defect regeneration was not significantly enhanced by the addition of GFs (TGF-β1+BMP-2) within scaffolds. 46
The most widely studied GFs for cartilage repair include three members of the TGF-β superfamily—TGF-β1, BMP-2, and BMP-7. 125 TGF-β1 and BMP-2 stimulate BMSCs synthetic activity and promote collagen formation. 126 BMP-2 has been proven to significantly enhance bone regeneration in limited-sized bone defects, such as alveolar socket healing and sinus-lift procedures. 127 Similar positive in vivo outcomes were reported in mandibular condyle head defects, 53 with enhanced regeneration with increasing concentrations of BMP-2. However, in regeneration of larger defects, such as a condyle implant after condylectomy, BMP-2 did not show significant differences compared with empty scaffolds. 56 For larger bone defects, a combination of angiogenic and osteogenic GFs is reported to be more beneficial. 128 Vascular endothelial growth factor (VEGF) is a crucial factor in angiogenesis during bone formation, but conflicting results of VEGF combined with BMP-2 have been reported, and a complimentary, rather than supplementary, effect of GFs on implanted cells has been suggested. 129 FGF is another family of GFs involved in cartilage repair and regeneration by stimulating proteoglycan synthesis and cell proliferation. 125 In the present review, one study 54 reported enhanced effect of low-dose FGF-2, before high dose, for repair of condyle defects in rabbits. Similar results have been reported in repair of large femoral osteochondral defects in rabbits, 130 suggesting an inverse dose–response. 125 However, delivery of GFs must be performed with caution, given the previous reports of side-effects associated with their use. For example, TGF-β1 has been reported to induce synovial proliferation and fibrosis, and attraction of inflammatory cells. In addition, TGF-β1 and FGF-2 may contribute to osteophyte formation,126,131 whereas intra-TMJ injection of VEGF in rats, has been reported to induce OA. 132 Use of combinations of, rather than individual, GFs have been reported to be beneficial and the effects are related to the concentration used. 133 For example, one included study reported the use of CTGF and TGF-β3 combined in a 3D printed scaffold for TMJ disc regeneration 55 due to their combined fibrocartilage differentiation effect on BMSCs. 117 Determination of the optimal dosage, delivery method, spatiotemporal release profile, and reliance on host cell responses are some of the reported limitations of current GF delivery strategies.134,135 Surgery is generally considered a last-resort treatment option for TMD patients, 19 and innovation of minimally invasive treatment alternatives is of great interest. However, TE strategies included in the present review are limited to scaffold-based approaches and studies aiming for TMJ regeneration through direct intra-TMJ injection of cells- and/or GFs are beyond its scope.
Future design of preclinical models
Overall, the RoB of included studies was considered to be unclear. When designing future in vivo studies, increased focus on the ARRIVE37,38 and SYRCLE 40 guidelines, would be preferable to lower the RoB, establish consistency, and minimize discrepancy. Reporting of species age, gender, strain, weight, source, and housing and husbandry, is important for comparing methodology and outcome, and was frequently inadequately reported in the present review. Sample size and power calculations should be reported, to detect and confirm statistically significant differences between experimental groups and to justify the number of animals used. Randomization and blinding procedures, should be applied to limit selection bias and detection bias, respectively. Standardization of animal models would decrease the heterogeneity observed and improve translation to clinical applications. 136 A recent review 86 suggests the possibility of exploring naturally occurring TMJ disorders in companion animal models, that is, dogs and cats. This could more closely mimic the “true” progression of OA than surgically created defects, in addition to reflect the genetic diversity and variations seen in humans. 137 Although, it might be difficult to standardize such models, it could potentially benefit both animals and humans in the future.
Selection of appropriate controls is essential. Several studies41,65,66,68,69 used the contralateral joint as a control which could be efficient in reducing the number of animals used. No included studies reported contralateral healthy controls, which may bias the results in terms of contralateral overload, 136 and therefore a bilateral intervention may be favorable. Quantitative measures of outcome to evaluate success, for example, histomorphometry and radiography, would ease the comparison between studies and increase the validity of the results. Only two included studies51,65 reported biomechanical assessment of TMJ implants to detect clinically relevant differences in functional performance. However, the first study (published in 1994) 51 compared compressive load of ectopically regenerated fibrocartilage to native rib and glenohumeral hyaline cartilage, which do not represent the ideal controls. More recent studies have contributed to increased knowledge about differences between tissue-specific characteristics of cartilage. 116 Since the human TMJ is a highly functional ginglymoarthrodial joint with a capacity for multidirectional activity, that is, rotation and translation,86,138 assessment of biomechanical parameters, for example, compressive modulus and ultimate strength, 55 may be important indicators of functional performance. Furthermore, inclusion of biochemical assessments of organic content of in vivo regenerated tissues, for example, collagen and GAG's, 65 would support standard histological and radiographic data, and strengthen the structural comparison to native tissues.
Clinical relevance
When diagnosing symptomatic clinical TMDs through arthroscopy and imaging, 139 favorable treatment options are currently limited. Discectomy of unsalvageable discs may trigger a more degenerative state of the disease, whereas replacement with an interpositional graft material, of temporal muscle, dermis, or fat grafts, would result in extensive donor-site morbidity and scar tissue formation. Treatment options for more severe TMDs consist of autogenous grafts or TMJ reconstruction prosthesis.14,16 Costochondral or sternoclavicular grafts are associated with donor-site morbidity, technical sensitivity, and delayed functional loading with unpredictable results such as high failure rates due to graft overgrowth and risk of reankylosis.17,140 TMJ prosthesis allow the patient to return to function sooner, result in lower postoperative pain scores, avoid donor-site morbidity, and offer better replication of functional anatomy and earlier postoperative rehabilitation. 141 However, the high costs preclude their applicability among all socioeconomic groups of patients, in addition to concerns regarding potential material wear/failure, long-term stability, and function. 142 Distraction osteogenesis of the posterior border of the ramus is another approach of condyle regeneration. However, the method is technically difficult due to surgery and vector control, and the prolonged consolidation period makes the method prone to infections. 143 Thus, due to the limitations of current treatment modalities, TE may offer promising alternatives for treatment of TMDs.11,23,122,144 While successful clinical outcome of TE for knee meniscus regeneration has been reported,145–147 it is unclear whether these results can be translated to the TMJ. To our knowledge only one study 142 so far has reported the use of HA scaffolds loaded with BM aspirates for condyle regeneration in seven pediatric patients (mean age 9.71 years) with high success in terms of clinical (mouth opening) and radiographic (CT) outcomes, after 1 year follow-up. However, considering their young age and short follow-up, the long-term results may still be unpredictable.
Conclusions
The reviewed preclinical in vivo evidence can be summarized as follows:
Based on the results of orthotopic models in rabbits (n = 6) and dogs (n = 2), TMJ disc regeneration is enhanced by cell-loaded scaffolds, compared with cell-free scaffolds. Cell-free collagen scaffolds and porcine UB-ECM may serve as promising replacement solutions to partial or complete discectomy, respectively. Based on the results of orthotopic models (n = 4) in small (rabbits) and large animals (sheep, goats), TMJ condyle regeneration is enhanced by the addition of chondrogenic or osteogenic cells to biomaterial scaffolds. Standardization of models (e.g., animal species, defect sizes, blinding, randomization etc.) and methods for quantitative evaluation of outcomes (biomechanical and biochemical assessment, histomorphometry, and radiography) in future studies would ease comparison between studies and increase the validity of the results. The results of the present review should be interpreted with caution due to the large heterogeneity between studies resulting from biological and methodological variability.
Footnotes
Acknowledgments
The authors thank all the corresponding authors of the primary studies who provided additional information for the review, and Dr. Ying Xue for the Chinese translation.
Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.