
Abstract
The complexity of the dermal layer of skin means that damage to this section can result in permanent impairment of function. Partial or total dermal loss is a feature of deep burns and chronic wounds such as pressure sores or diabetic ulcers. The issues posed by traditional skin grafts have led to substantial research being carried out in the fields of tissue engineering and biomaterials science to develop a vast array of alternative skin substitutes. Given the large number of different materials, manufacturing methods, and techniques for implementation described for artificial skin substitutes, many classification systems have been created to simplify their categorization. Some of these systems are oriented toward clinicians while others toward researchers. However, none address the needs of both groups and none are intuitive. The creation of an effective classification system would be particularly helpful in the regulation, distribution, organization, and selection of skin substitutes. The aim of this review is to examine existing methods of classification of skin substitutes, and to propose a new system that uses an algorithm that is inspired by factorial design. Our system allows multiple factors to be simultaneously investigated or in this case, described, since all skin substitutes possess multiple characteristics: (1) cellularity (acellular or cellular), (2) layering (single layer or bilayer), (3) replaced region (epidermis, dermis, or both), (4) materials used (natural, synthetic, or both), and (5) permanence (temporary or permanent). The factors and levels are combined into an algorithm where all the possible combinations are shown. The multifactorial and palindromic structure of our system should enable all users to quickly understand the makeup of a selected skin substitute, or search for a skin substitute depending on their specific requirements. We feel that our proposed classification can be used by clinicians and biomedical researchers alike, which should be an advantage given the multidisciplinary nature of the tissue engineering field and the science that underpins the development of skin substitutes. We also touch upon some of the state-of-the-art skin substitutes that are commercially available or under development to demonstrate how our new method of classification might work.
Introduction
T
Historically, burns have been treated with autografts, allografts, and xenografts. Autologous grafts (autografts) are used most frequently because of the problems of infection and rejection when using allografts or xenografts. 1 While autografts are successful at healing wounds after burns, this is often achieved at the expense of permanent damage to the skin at the donor site and this may be manifest as additional (sometimes severe) scarring. 2 Moreover, donor sites are often insufficient in cases of large area burns. These concerns have led to substantial research in the areas of tissue engineering and biomaterials to create a vast array of alternative skin substitutes1–4 to avoid these problems (Fig. 1).
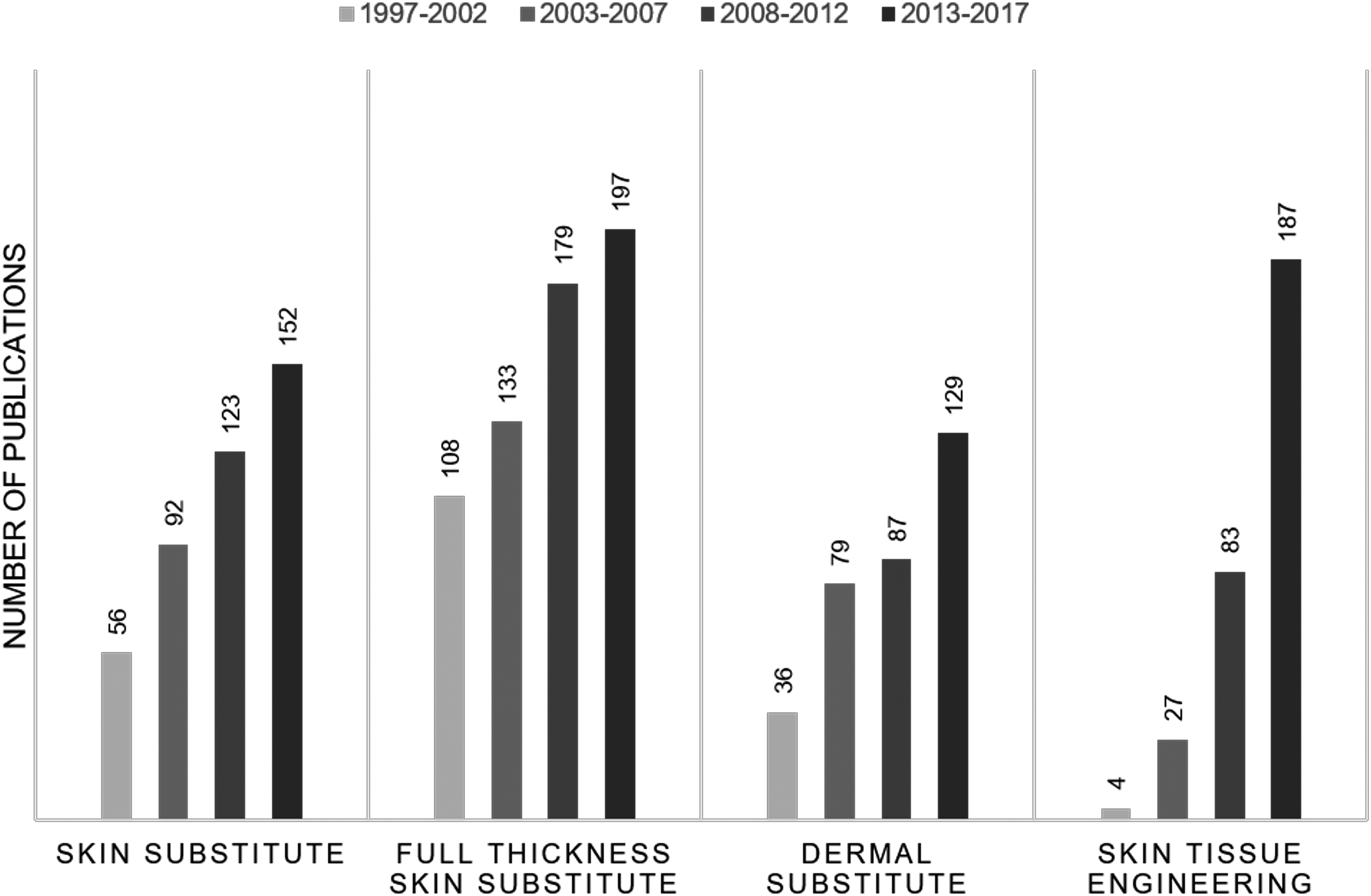
Number of publications on research of alternative skin substitutes during the last 20 years. Sourced from PubMed. Searched keywords: “skin substitute,” “full-thickness skin substitute,” “dermal substitute,” and “skin tissue engineering.”
van der Veen et al.
3
outlined the general principles for functional skin substitutes as follows:
Protection of the integument from loss of fluid and infection: the magnitude of fluid loss is primarily the result of the materials used within the skin substitute, and the layering of the material; those that contain both a dermal and epidermal component retain water much more effectively than those that only act as a single-layered dermal or epidermal replacement. Provision of a stable, biodegradable scaffold to promote the synthesis of new dermal tissue: the speed of degradation often dictates the stability of the scaffold and thereby influences the synthesis of new dermal tissue. If the scaffold degrades too rapidly, cells will be unable to migrate within the scaffold sufficiently quickly to start depositing a new extracellular matrix. On the other hand, if the material degrades too slowly this will render the material biologically and mechanically inert for too long, which may generate a foreign body response, leading to an immune response that hinders the success of newly formed dermal tissue. Allowing host or other cells to proliferate within the scaffold that will act as functional dermal cells, rather than scar tissue: the overall success of a skin substitute can often be determined by the level of vascularization it encourages, and its ability to prevent scar tissue formation. If the material is unable to effectively induce vascularization, scar tissue will often form in the place of healthy, functional dermal cells. The ability to resist tearing forces while being easy to handle: while it is important for the skin substitute to maintain resistance to tearing, it is also of pivotal importance that it remains flexible, allowing it to conform to the contour irregularities present in all wounds.
Given the large number of different materials, manufacturing methods, and techniques for implementation described for artificial skin substitutes, many classification systems have been created to simplify their categorization.5–7 Some systems are oriented toward clinicians while others are directed toward researchers. However, none address the needs of both groups and none are intuitive. The creation of an effective classification system would be particularly helpful in the regulation, distribution, organization, and selection of skin substitutes. The purpose of this review is to examine existing methods of classification, and to propose a new classification system that uses an algorithm that is inspired by factorial design. We feel that our proposed classification can be used by clinicians and biomedical researchers alike, which should be an advantage given the multidisciplinary nature of the tissue engineering field and the science that underpins the production of skin substitutes. We also touch upon some of the state-of-the-art skin substitutes that are commercially available or under development to demonstrate how our new method of classification might work.
Definition and Existing Classifications for Skin Substitutes
A “skin substitute” describes a group of materials (biological, synthetic, and/or a mixture of the two), employed to provide wound cover after damage to the skin that extends deeper than the epidermal layer. These products vary in their material composition, time of permanence, intended layer of replacement, and the presence or lack of cellular components. Although knowledge about the replacement, repair, and regeneration of skin has grown exponentially over the past several years, the language and classification of skin substitutes has developed in a variety of overlapping and conflicting ways.
In 2001, Balasubramani et al. 5 proposed a classification based on the plasticity of the composition and preparation procedures. They put skin substitutes into three groups: Class I, substitutes consisted of cultured epidermal equivalents alone; Class II substitutes consisted of dermal components coming from processed skin or are manufactured with extracellular matrix proteins—mainly collagen; and Class III substitutes included both dermal and epidermal components. The classification system did not include materials fabricated from synthetic polymers that act as dermal substitutes (e.g., Dermagraft®, a polyglactin mesh seeded with allogenic neonatal fibroblasts). In addition, the system proposed by Balasubramani et al. 5 did not differentiate between acellular and cellular products.
This was replaced by Kumar's three category system, which is currently the most frequently used classification system in this field. 6 In a Letter to the journal Burns, published in 2008, Kumar proposed a new system consisting of three categories: Class I, temporary, impervious, dressing materials; Class II, single layer, durable, skin substitutes; and Class III, composite skin substitutes.
Class I skin substitutes exhibit many of the mechanical traits of the epidermis, while lacking its cellular components that is, keratinocytes. This class of skin replacements functions to protect against pathogenic agents and water loss, thereby facilitating healing by maintaining a moist environment. The class is split into two subcategories: single-layered materials, and bi-layered tissue-engineered materials. Single-layered materials can be naturally occurring materials or synthetic. Examples of the former include Biomembrane®, made of human amniotic membrane, and biocompatible vegetal membranes such as those derived from the Hevea brasiliensis (the “rubber tree”). 8 Examples of synthetic materials would include (1) Tegaderm™, a polyurethane film coated with a layer of acrylic adhesive allowing the wound site to retain water while preventing infection 9 ; (2) the biosynthetic film Nexfill®, a microcellular cellulose membrane synthesized by bacteria that create a random network of cellulose microfibrils 10 ; and (3) Gelapin, which are genipin cross-linked gelatin hydrogels with controllable degeneration times through alterations in material composition and genipin to gelatin concentrations. 11 An example of a double-layered tissue-engineered material would be Transcyte®, which is a silicone-covered composite membrane composed of a nylon mesh and porcine collagen, on which neonatal human fibroblasts derived from neonatal foreskin are cultured for several weeks.12,13 During the culture period, the fibroblasts secrete human dermal collagen, along with matrix proteins and growth factors. This skin substitute is subsequently frozen, which effectively halts any metabolic activity, while retaining the intact extracellular matrix. The method of application allows autologic epithelial cells to migrate to the wound site, encouraging wound healing.
Class II skin substitutes can be epidermal or dermal. Epidermal skin substitutes have a form and function that is similar to human epidermis. Products in this category are prone to breakdown, and produce poor wound healing results. They include cultured epithelial autograft (CEA), Epicel® and Epidex®.14,15 Kumar 6 also included Apligraf® in this category. However, we believe this was a mistake since Apligraf is a bi-layer composite composed of allogenic neonatal keratinocytes and fibroblasts contained within collagen conferring to the product epidermal and dermal components.16,17
Dermal substitutes include substances that are similar to those found in the dermis. Products in this category include bovine collagen sheets and dermal matrices, human dermal matrices, and porcine collagen sheets. Some examples include (1) Köllagen®, an extracellular matrix derived from bovine collagen, encouraging epithelialization and protecting the wound from infection and fluid loss 6 ; (2) Matriderm®, an acellular bovine dermal matrix, composed of collagen and elastin, which encourages angiogenesis, cell migration, and proliferation18–20 ; (3) Alloderm®, an acellular human dermal matrix derived from cadaveric skin21,22; and (4) Permacol®, an acellular porcine dermal collagen matrix, cross-linked with noncalcifying hexamethylene diisocyanate to slow degradation by collagenase. 23
Finally, Class III skin substitutes include those materials that replace both dermal and epidermal layers, and any cellularized full-thickness substitutes. In this category, many of the synthetic epidermal components are removed once cellular migration and angiogenesis have occurred, and are substituted for a split-thickness autograft or allograft. Class III materials include skin grafts (autografts, allografts, and xenografts) and tissue-engineered skin such as Integra® Bilayer Matrix (acellular cross-linked bovine tendon collagen and glycosaminoglycan matrix combined with a semipermeable polysiloxane backing, which prevents water loss, thereby acting as an artificial epidermis)24–26 or Biobrane® (filamentous nylon mesh, bonded to a semipermeable silicone membrane that acts as an artificial epidermis).27,28
Table 1 summarizes Kumar's 6 classification system giving examples for each category. Although thorough, Kumar's system has been criticized for being confusing and nonintuitive. As an example, Integra (acellular) and Apligraf (cellular), which are very different materials, would be placed in the same category.
CEA, cultured epithelial autograft.
Subsequently, Ferreira et al. created a more clinically oriented method of categorization, in which skin substitutes and scaffolds are classified according to their location, time of permanence, and the materials used. 7 According to Ferreira et al. 7 current classification systems, such as that proposed by Kumar, 6 fail to include all available products and do not define their indications. Ferreira et al. 7 suggested using a lettering system to distinguish various skin substitutes that might be helpful to assist clinicians in determining which product was most suitable for a particular application (Table 2). Although a lettering system is helpful in determining the specifics of a skin substitute, we do not feel it is sufficiently intuitive or useful for clinicians or researchers.
New Classification System
The creation of an effective classification system would be particularly helpful in the regulation, distribution, organization, and selection of skin substitutes. A recent review of wound healing products by Vyas and Vasconez outlined the necessity of differentiating products based on the presence of live cells, followed by the tissue layer the product is replacing and the permanence of the skin substitute. 8 We agree completely with this philosophy and acknowledge that each of the classification systems already discussed attempts to address at least some of these criteria. Balasubramani et al. 5 categorizes skin substitutes according to the tissue layer that the product would replace but does not differentiate between acellular and cellular products. Nor does it consider the permanence of the material. Kumar's system does address all three criteria but is difficult to use. 6 Ferreira et al. 7 categorize skin substitutes on the basis of tissue layer and permanence but completely forgo any mention of the cellular components within the dermal substitute.
We have now taken elements from all the systems already described to create a multifactorial and palindromic system that we believe will be intuitive for clinicians, while also allowing biomaterial scientists to reference classifications in the literature, which can be easily understood and applied in a variety of settings. Our system will allow multiple factors to be simultaneously investigated or in this case, described, since all skin substitutes possess multiple characteristics. The factors that we feel are important include (1) cellularity, (2) layering, (3) replaced region, (4) materials used, and (5) permanence. Each of these factors, and our justification for using them (Table 3), will now be discussed separately.
Cellularity
We agree with Vyas and Vasconez 8 that the most important discriminator should be the presence or absence of cellular components in the skin substitute. In our classification system skin substitutes can be either acellular or cellular. The presence of cells within a skin substitute has major implications with regards to the clinical application, storage, cost, and availability of the product. Cellularized products also run a higher risk of host rejection, especially if the cells are not autologous. Cellularity also increases manufacturing and regulatory complexity.
Layering
Skin substitutes may be either a single layer or a bilayer. Skin substitutes that are composed of a bilayer will generally replace both the epidermal and dermal components of the skin, whereas those with a single layer only replace one or the other.
Replaced region
This can be the epidermis, dermis, or both. The specific layer that is being replaced by the skin substitute will have an impact on the materials used, number of layers, and efficacy of the product. Simple epidermal substitutes include materials such as CEA. 6 When used alone, these often result in worse clinical outcomes. In contrast, use of dermal substitutes or full-thickness substitutes provide greater stability, resulting in much more effective wound healing, and decreased scar tissue formation. 8
Materials used
The materials used to manufacture skin substitutes can be derived from synthetic or natural sources. Synthetic polymers are not derived from biological sources and may include polyesters (e.g., polycaprolactone, poly-glycolic acid, poly-lactic acid), nylon or polyglactin meshes, and silastic or silicone membranes. Materials derived from natural sources include natural polymers, such as proteins (e.g., collagen, elastin, fibrin, gelatin, silk fibroin), polysaccharides (e.g., hyaluronic acid, chondroitin sulfate, alginate), or decellularized matrices, which are (typically) composites of extracellular matrix proteins such as collagen and glycosaminoglycans. The materials used can also be composed of both natural and synthetic materials. A composite is a material composed of two or more substances that are different in composition and morphology to obtain specific biological, chemical, physical, and mechanical properties. Thus, skin substitutes that combine two different natural materials (e.g., collagen and elastin in the case of Matriderm) are also composites. This can be confusing; therefore, in our classification system we chose to avoid the term composite.
Permanence
Although the relative permanence of a skin substitute is often considered as important, using the actual degradation time for a particular material as a criterion for classification is impractical. Instead, we suggest using the simpler distinction of biodegradable (temporary) or nonbiodegradable (permanent) to differentiate the many different materials in use. All natural materials such as collagen, elastin, and other biological proteins are considered biodegradable, as are the many different types of completely decellularized matrices. The degradation of synthetic polymers varies according to the specific material used. Thus, some polyesters can be degraded through natural metabolic pathways, 35 whereas materials such as silicones and nylons are bioinert. 36
We have combined our five factors into an algorithm where all the possible combinations are shown (Fig. 2). The multifactorial and palindromic structure of our system should enable all users to quickly understand the makeup of a selected skin substitute, or search for a skin substitute depending on their specific requirements. Moreover, any existing or new skin substitute can be easily classified using this system. In Table 4 we classify some of the existing skin substitutes, in alphabetical order, according to our system. In addition, we describe three scenarios to illustrate the advantages of our proposed system over those described in this review:
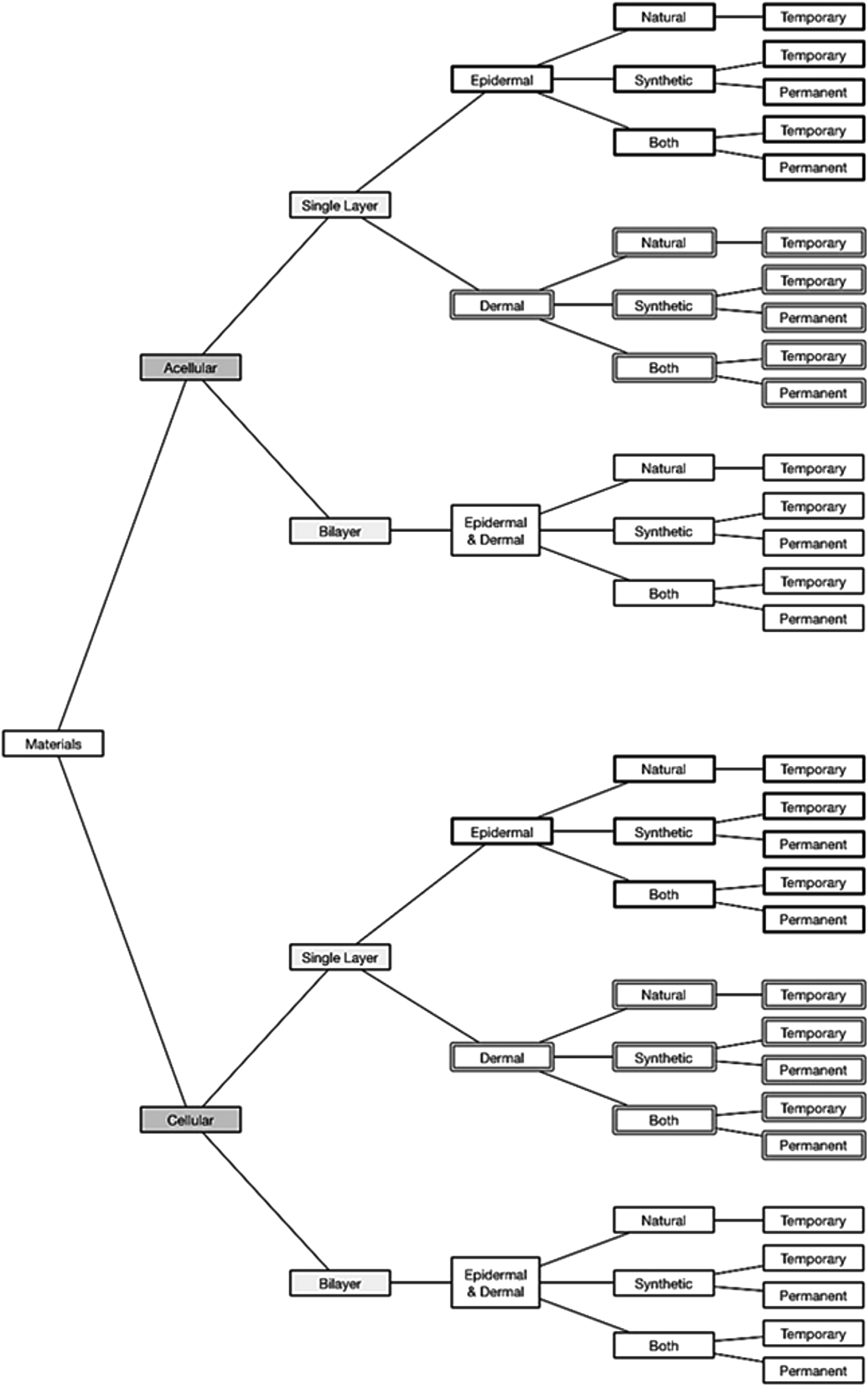
Algorithm where all the possible combinations in Table 3 are shown.
Apligraf is a bilayer of allogenic keratinocytes (epidermal component) and fibroblasts contained within collagen (dermal component). According to Balasubramani et al.' 5 system it would be classified as a “Class III substitute,” while in Kumar's 6 system it would be “Class III tissue-engineered skin.” “T bs C” would be its designation in Ferreira et al.'s 7 system. In our system, its classification would be “Cellular bilayer natural temporary substitute,” thus offering a clearer and more descriptive designation compared to the nonintuitive and indeterminate denomination of the aforementioned systems.
Suprathel® is an acellular single epidermal layer of microporous and degradable poly-
Laserskin® is composed of autogenic keratinocytes on a laser micro-perforated hyaluronic acid membrane. It is therefore an epidermal substitute that would be classified as a “Class I substitute” by Balasubramani et al.'s 5 system. “Class II epidermal substitute” and “T bs E” would be their denominations according to Kumar's 6 and Ferreira et al.' 7 systems respectively. It is worth noting that the designation of this product according to Ferreira et al.' 7 system would be the same as for Suprathel, even though both products are very different. In our system, Laserskin would be designated as a “Cellular single layer epidermal natural temporary substitute.”
We believe that an important advantage of our proposed classification system is its potential for expansion and adaptation. New types of skin substitutes, containing new types of materials (e.g., bioglass)51,52 are constantly being investigated. Our proposed system would easily accommodate the introduction of new sublevels within our five proposed factors or even the addition of entirely new factors in the future.
Conclusions
The issues posed by traditional skin grafts have led to substantial multidisciplinary research being carried out in the fields of tissue engineering and biomaterials science. This in turn has led to the development of a vast array of alternative skin substitutes. There is now a need to create a simpler classification system to assist in the process of regulation, distribution, organization, and selection of skin substitute products. We believe that our proposed system meets these requirements and will be easily used and understood by clinicians and scientists alike.
Footnotes
Acknowledgment
This work was supported by the Restoration of Appearance and Function Trust (United Kingdom, registered charity number 299811) charitable funds.
Disclosure Statement
No competing financial interests exist.