
Abstract
This meta-analysis was to systematically investigate all preclinical researches on the possible benefits of antiosteoporotic drugs on titanium implants. Also, we performed a subgroup analysis to examine if the methods of drug delivery (systemic vs. local vs. surface coatings) or the types of antiosteoporotic drug (anticatabolic vs. anabolic) have more effect on bone-to-implant regeneration. A total of 116 articles (animal studies) were included. Poor reporting was assessed in the majority of the included studies. Then, results of meta-analysis showed that the use of osteoporotic medications significantly increased the overall values of micro-CT bone volume (BV) (mean differences [MD]: 21.7%, confidence interval [CI]: 17.8–25.7), bone-to-implant contact (BIC) (MD: 12.1%, CI: 10.6–13.7), torque-out (MD: 5.7N.cm, CI: 4.6–6.8), and push-out (MD: 67.3N, CI: 54.6–79.9) compared with the values of implants without osteoporotic medications. Also, implants coated with drugs showed higher values of BIC (MD: 16.8%, CI: 12.4–21.3) compared with implants received drugs through systemic administration (MD: 12.2%, CI: 10.1–14.3) or local administration (MD: 8.6%, CI: 5.8–11.4). A positive effect of local delivery of antiosteoporotic drugs was significant on push-out testing (MD: 169.8N, CI: 120.1–219.6) compared with the use of drugs through systemic route (MD: 51.6N, CI: 38.7–64.6) or as surface coatings (MD: 24.1N, CI: 15.4–32.7). Finally, anabolic drugs showed a significant effect on push-out forces (MD: 125.5N, CI: 95.5–155.5) compared with the use of anticatabolic drugs (MD: 51.9N, CI: 39.5–64.5). In conclusion, the positive effect of antiosteoporotic drugs on osseointegration is observed in the present meta-analysis. Mainly, antiosteoporotic drug-coated implant surfaces showed an increase of BIC% compared with implants received drugs through local routes, but not with systemic routes. Also, the positive effect of anabolic drugs seems beyond the effect of anticatabolic drugs in terms of mechanical stability of implants as tested by push-out.
Impact Statement
This meta-analysis was to investigate literature on the administration of antiosteoporotic drugs as an effective adjunct therapy for implant osseointegration using in vivo animal models.
Introduction
Nowadays, oral rehabilitation using dental implant therapy is clinically well established for improving oral function and esthetics in either partially or completely edentulous patients. 1 Their efficacy predominantly relates to the capacity of titanium implants to osseointegrate directly with the surrounding bone without interference of intermediate fibrous connective tissue. 2 However, a decrease in oral bone quantity and quality related to systemic medical condition3,4 might influence dental implant treatment. 5
Worldwide, more than 200 million people have been diagnosed with osteoporosis.6,7 The occurrence of osteoporosis frequently coincides with menopause in women. The associated bone resorption results from estrogen deprivation and affects mostly trabecular bone.8,9 Considering that systemic osteoporosis may also affect the jawbones, osteoporotic women were further reported to have significant radiographic alterations in their maxillary and mandibular alveolar bone,10–15 being similar to type IV quality bone.16,17 Such poor quality of bone excessively attributed to the etiology of dental implant loss.16,18,19
Compromised osseointegration of titanium implants in osteoporotic conditions as compared with normal bone conditions has also been reported in preclinical models.20,21 The reason for implant failure might be correlated to the reduced regenerative capacity of osteoporotic bone. 22 Consequently, several strategies have been introduced to promote the biological performance of titanium implants in challenged bone conditions. 23 These strategies and modifications are in general accomplished by altering the implant design, the surgical procedures, or the physicochemical composition of implant surface.23,24 Although implant design and surgical techniques increase implant stability, they do not favor bone regeneration at the implant interface in challenged conditions.24,25
In recent decades, the use of antiosteoporotic drugs as an adjunct to titanium implant placement in challenged bone condition has been evaluated in vivo.26–28 This is based on the assumption that these drugs can regulate several biological events involving bone regeneration around titanium implants. 27 However, the dysfunction in regenerative capacity of challenged bone is the point of concern to many recent efforts in search for suitable drugs and their delivery routes that might improve bone implant healing.29–32
Although the use of antiosteoporotic drugs in bone regeneration is still in a preclinical stage, 27 interest in their use is increasing owing to their therapeutic potential to promote implant osseointegration. 25 For instance, the favorable effect of systemic administration of drugs that are already in clinical use for treatment of osteoporosis has been shown in animal studies to offer an easy, noninvasive manner to improve the healing of bone implants.33–35
Local administration of antiosteoporotic drugs associated with implant placement is suggested to direct a specific in situ process of bone regeneration and remodeling related to osteoporotic condition.36,37 In addition, new surface coating strategies with anticatabolic as well as anabolic drugs are being explored.38–40 For instance, the methods of immobilization of bisphosphonates, statin, strontium ranelate, or parathyroid hormone onto titanium surfaces are anticipated to promote osseointegration through the controlled delivery of these drugs at the desired sites. 41 Consequently, these drug-based modalities could potentially be translated into clinical benefit to the dental implants treatment. 42
It has to be noticed, however, that there is a lack of unambiguous evidence that antiosteoporotic drugs indeed favor the bone response around implants. In addition, several methods of drug administration have been proposed to increase therapeutic effect on implant osseointegration, but with no clear conclusion. This hampers further investigations as well as the final introduction of this technology into the dental practice.
We therefore performed this review to identify all the relevant evidence in a systematic manner for studying the efficacy of antiosteoporotic drugs on bone–implant response in osteoporotic and healthy animal models. For meta-analyses, bone-to-implant contact (BIC%), micro-CT bone volume (BV%), push-out (N) tests, and torque-out (N.cm) tests were selected as quantitative parameters to assess the overall effect of antiosteoporotic drugs on osseointegration; also, to assess the possible effect of using different methods for drug administration (systemic vs. local vs. surface coatings) or different types of antiosteoporotic drugs (anticatabolic vs. anabolic) on osseointegration.
Material and Methods
Search strategy
PubMed and EMBASE searches were performed as described previously. 43 The search was initiated in June 2015 and then updated every 3 months. Last update was in November 2017. In both PubMed and EMBASE databases, all search terms related to the subjects of “antiosteoporotic drugs” and “dental implants, surface coatings”—thesaurus terms as well as free text terms—were identified for animal studies.44,45 The complete search strategy is presented in Supplement 1. Additional search was performed manually by screening relevant reviews and publications.
Study selection
All records retrieved from the searches were imported into a bibliographic referencing software program (EndNote® X7, www.endnote.com), and duplicate references were identified and removed. Two independent reviewers (A.B., M.S.) screened the relevant titles/abstracts and subsequently full texts and reports. Publications were excluded when: (1) subject of title was clearly not relevant to implant osseointegration and antiosteoporotic drugs, (2) it was specifically mentioned in the title/abstract that only ex vivo or in vitro studies were performed, (3) an irrelevant animal model to osteoporotic or healthy conditions was specifically stated in title/abstract, and (4) non-English language publications.
Then, articles were retrieved in full text and assessed as following: (1) original animal research, (2) osteoporotic and/or healthy conditions, (3) implantation of titanium fixtures, (4) implantation site and period should be mentioned, (5) antiosteoporotic drugs were used with implantation procedures, (6) type of antiosteoporotic drug was stated, (7) route of drug administration was clearly described, and (8) English language was used for publication. During the screening process, only articles meeting all inclusion criteria were included. When both reviewers agreed on exclusion, the reasons for exclusion were recorded.
Data extraction and study characteristics
The data extraction process was guided by a data extraction sheet (Supplement 2) that specified the relevant study characteristics, including author, publication date, study design, animal model, information related to implantation procedures (number of implants, anatomical site, and healing time), data for the administration of antiosteoporotic drugs (type, route, dose, and duration), and reported implant outcomes that quantify bone formation around titanium implants. These outcomes included BIC%, micro-CT BV%, and biomechanical stability tests (push-out, N, or torque-out, N.cm).
Quality of studies reporting and risk of bias
SYRCLE risk of bias tool 46 was used to assess the quality of reporting and risk of bias for the included studies. None of the studies was excluded because of this quality appraisal. First, “Randomization” and “blinded assessment” were used as indicators for reporting quality. Second, the following criteria were used to assess the risk of bias: (1) selection bias, (2) performance bias, (3) detection bias, and (4) attrition bias. A “yes” score was given for studies with low risk of bias, “no” score for high risk of bias, and “?” for unclear risk of bias. Studies were scored by the two reviewers independently, with disagreements resolved by discussion.
Outcome data extraction and quantitative data synthesis (meta-analyses)
Data of the study groups were extracted in the format of mean, standard deviation (SD), and number of implants, for all outcome variables. For studies depicted data in graph, we used ImageJ (1.46r, National Institutes of Health USA) to measure the mean and SD. Also, sometimes the mean and SD were recalculated from the median, range, and the sample size. 46 When data only reported mean and confidence interval (CI), the SD was recalculated by the following equation: SD = √N × (upper limit − lower limit/3.92) for a 95% CI. 47
For meta-analysis, the treatment group consisted of titanium implants that were placed in animals with the adjunct administration of antiosteoporotic drugs. The control group consisted of implantation procedures without the use of antiosteoporotic drugs. Four outcome variables that quantify bone formation around titanium implants were studied: BIC%, micro-CT BV%, push-out testing (N), and torque-out testing (N.cm). Two subgroup variables were investigated: route of drug administration (systemic vs. local vs. surface coatings) and the type of drugs (anticatabolic vs. anabolic). Systemic administration refers to administration of drugs into the whole body through enteral administration (through the gastrointestinal tract) or parenteral administration (intravenous, IV, intramuscular, IM, intraperitoneal, IP, or subcutaneous, SC).
Differently, local administration refers to the method of drug delivery locally in the implantation sites. The method of immobilization of antiosteoporotic drugs onto titanium implants refers to surface coatings. For studies with several treatment groups, the groups were treated as independent comparisons. This was possible because data for different implantation sites, different implantation periods, different implantation conditions (osteoporotic or healthy animals), and different dosage of drugs were investigated independently in the same study.
For each outcome measure, a meta-analysis was performed to examine the overall benefit of using antiosteoporotic drugs on osseointegration, making a comparison between an “implantation with drug administration” as treatment group and “implantation without drug administration” as control group. Then, subgroup analyses were performed to compare the effect of different routes of drug administration (systemic vs. local vs. surface coating) and different types of drugs (anticatabolic vs. anabolic) on osseointegration.
Effect sizes were presented as mean differences (MD) and corresponding 95% CIs. Meta-analyses were completed using software provided by the Cochrane Collaboration, Review Manager 5 (RevMan 5, http://tech.cochrane.org/revman). Owing to expected heterogeneity among studies, meta-analyses used random-effects modeling. Heterogeneity was assessed using the I2 metric. We judged the difference between subgroups to be statistically significant if their CIs did not overlap. 47 Publication bias in the overall outcome of each study was assessed and presented using funnel plots.
Results
Study selection
The flow of the selection of studies through the review is shown in Figure 1. In total, the electronic searches identified 697 studies in PubMed and 1028 studies in EMBASE. These studies were initially screened for duplicates, resulting in consideration of 1247 studies. Screening titles and abstracts led to include 184 publication records at this stage. Finally, only 116 articles were selected for evaluation, data extraction, and interpretation.
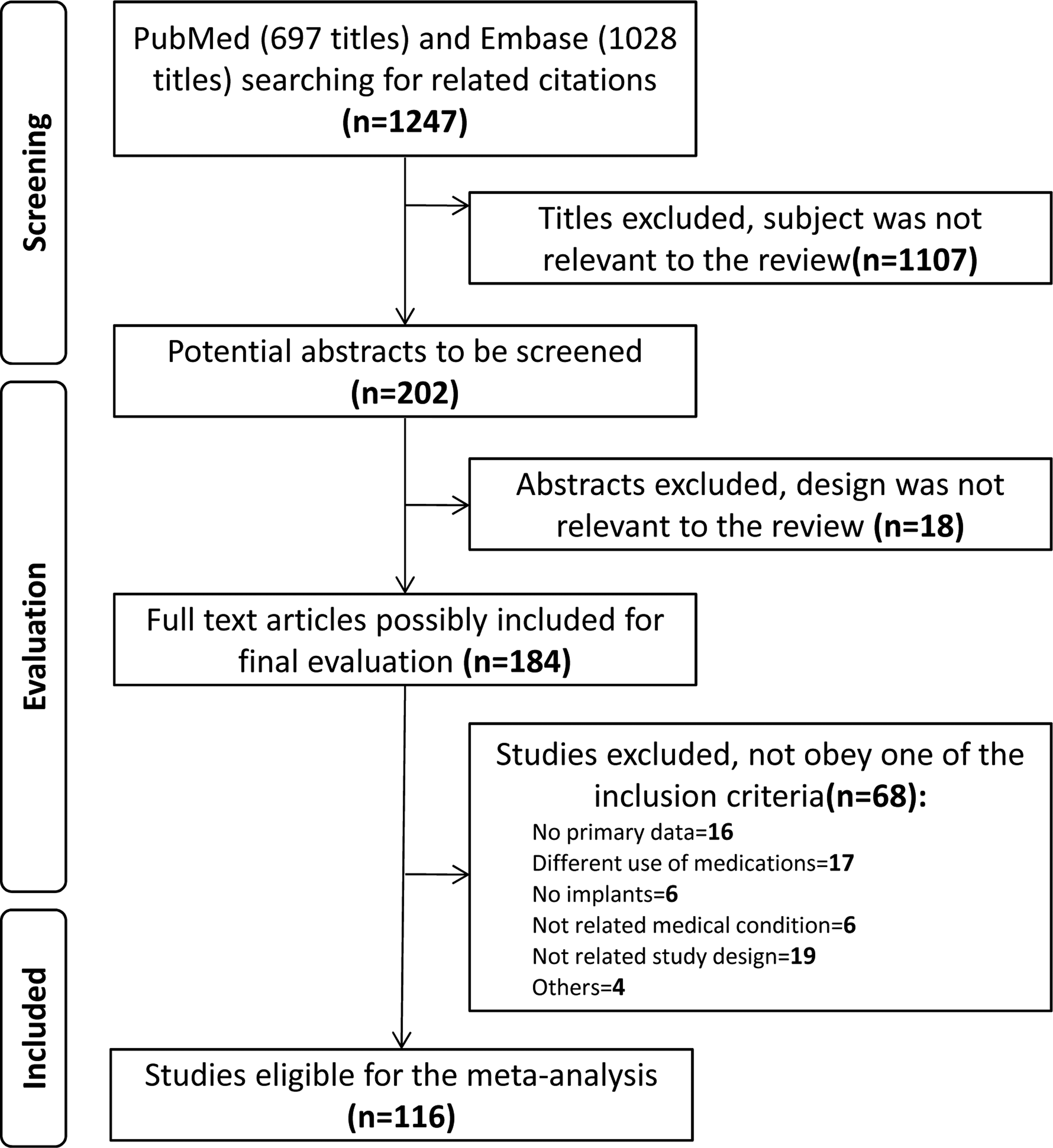
Flow chart of the systematic search of literature and the process of study selection according to PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-analysis).
Study characteristics
For a full list of the characteristics of the included studies, please see Supplement 3. It shows that several animal species were used, including small (mice in 2 studies, rats in 77 studies, rabbits in 12 studies) and large animal models (minipigs in 1 study, dogs in 12 studies, pigs in 1 study, sheep in 1 study). Healthy animals were used in 73 studies. Osteoporotic conditions were induced in the animals of 32 studies, mainly in rats and rabbits. Only two studies used dog and minipig osteoporotic models. In 11 studies, animal models with both medical conditions (healthy and osteoporosis) were experimented.
Substantial variations were observed in the implantation protocols of the studies. Several anatomical bone sites were assigned to place implants (i.e., tibia, femoral condyle, vertebra, ulna, humerus, iliac crest, lumber, mandible, and maxilla). In addition, the implantation period differed between the studies. The shortest period of implantation was ≤2 weeks, while the maximum implantation time was a year in one study. In the majority of the studies, implant healing time ranged from 1 to 6 months.
Concerning the route of drug administration, several differences could be noticed in the included studies and defined as systemic or local administration or surface coatings. Of the included studies, a majority (74 studies) investigated the benefit of anticatabolic drugs (mainly bisphosphonates) on osseointegration. Bisphosphonate drugs included alendronate, pamidronate, zoledronate, and ibandronate. The remaining 42 studies reported on the effect of three types of anabolic drugs (parathyroid hormones, strontium ranelate, and statin) on implant osseointegration.
Assessment of quality of studies
In Figure 2, we present the results of reporting quality and risk of bias for the included studies. A blinded experiment was only performed in 35% studies (Fig. 2A). On the other hand, we found that more than 50% studies reported the presence of randomization at any level. However, in most studies, there were no details describing the method of randomization, thereby we were not able to assess the adequacy of randomization. In Figure 2B, it shows that, for selection bias, more than 80% studies scored an unclear risk of bias because they did not describe the allocation sequence and/or did not report that the allocation had been concealed. Also, less than 20% studies gave details on performance bias (i.e., animals were randomly housed, a blind experiment was followed).
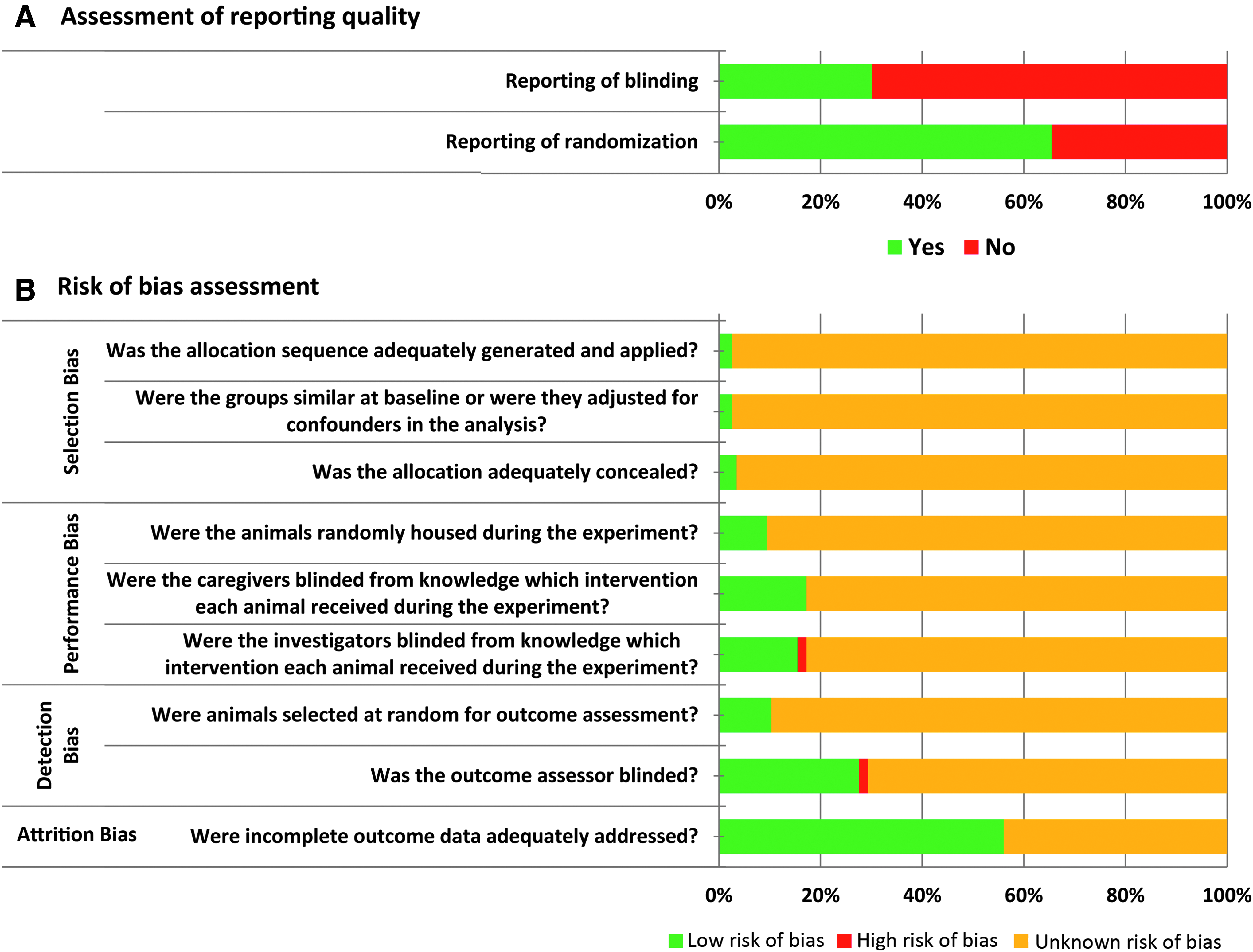
Bar chart shows the assessment of study quality and risk of bias for the included 116 studies.
A 5% of studies showed high risk of performance bias, because they did not follow blind experiment interventions. However, it was difficult to provide judgments on the presence of performance bias in the remaining studies or not due to the lack of information. For detection bias, we also found that more than 80% studies failed to state whether animals were randomly selected for the outcome assessment.
Also, less than 30% studies had low risk of detection bias because they followed blinded assessment protocol for their outcomes. Finally, we did not find incomplete outcome data in more than 50% reports and scored low risk of attrition bias. However, it was difficult to discern from the remaining studies if there were any missing information-related outcomes. For example, these studies did not mention the number of animals at the end of experiment, and if still same as at the start of the study.
Quantitative data synthesis (meta-analysis)
All 116 studies selected for the review were also included in the meta-analysis. Out of the 116 articles, more than one comparison (treatment vs. control) could be retrieved separately with regard to one or more implant outcomes. In Table 1 and Supplement 4 (forest plots), we present an overview of the meta-analysis results. Also, in Table 2, the total number of comparisons that showed positive effect (+ve), negative effect (−ve), or no effect are presented.
Number of Comparisons/Implants as Measured for Each Outcome Variable
Effect estimate meta-analysis presented as MD and 95% CI according to overall, route of administration, and type of drug.
BIC, bone-to-implant contact; CI, confidence interval; MD, mean difference.
The Total Number of Comparisons Measured for Each Outcome Variable that Showed Positive Effect (+ve), Negative Effect (−ve), or No Effect
BV, bone volume.
Overall results of using antiosteoporotic drugs related to osseointegration
Overall, the meta-analyses indicate a significant improvement in implant osseointegration adjunct to the administration of antiosteoporotic drugs compared with implantation without the use of drugs, as quantified by histomorphometrical BIC% (MD: 12.1%, CI: 10.5–13.7; Fig. 3), micro-CT BV% (MD: 21.7%, CI: 17.8–25.7; Fig. 4), mechanical push-out testing (MD: 67.3N, CI: 54.6–79.9; Fig. 5), and mechanical torque-out testing (MD: 5.7N.cm, CI: 4.6–6.8; Fig. 6). However, not all studies/comparisons showed the same (direction of) effect. As shown in Table 1, a total of 3204 implants were used in 210 comparisons to estimate the overall benefit of osteoporosis medications on implant osseointegration based on BIC% outcome variable.
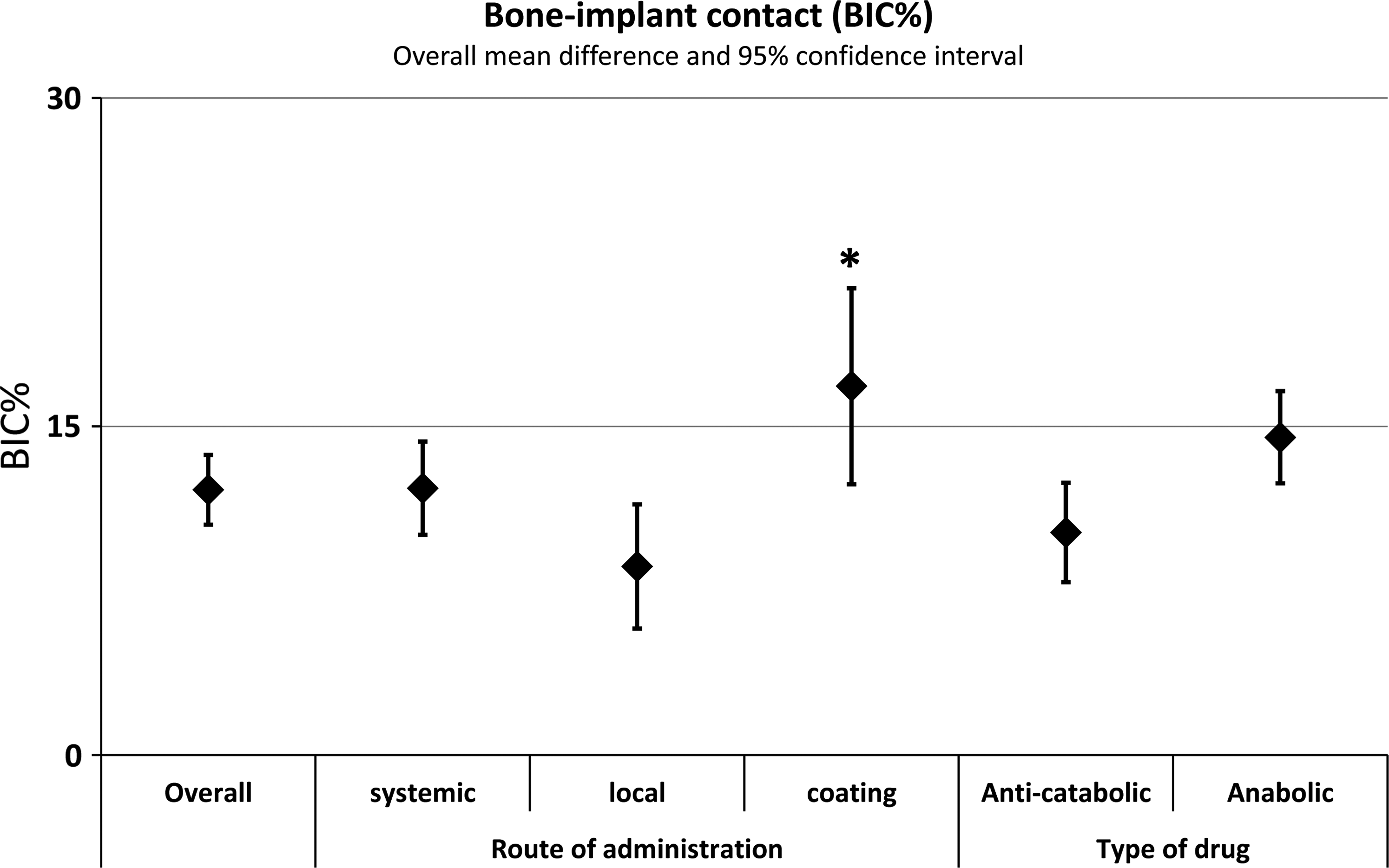
The BIC%. A scatter plot depicts the effect estimate (MD) with the 95% confidence interval for overall and subgroup analyses (per route and type of drugs). There is a significant difference between subgroups when their confidence intervals do not overlap. *p < 0.05. BIC, bone-to-implant contact; MD, mean difference.

The micro-CT bone–implant volume (BV%). A scatter plot depicts the effect estimate (MD) with the 95% confidence interval for overall and subgroup analyses (per route and type of drugs). There is a significant difference between subgroups when their confidence intervals do not overlap.
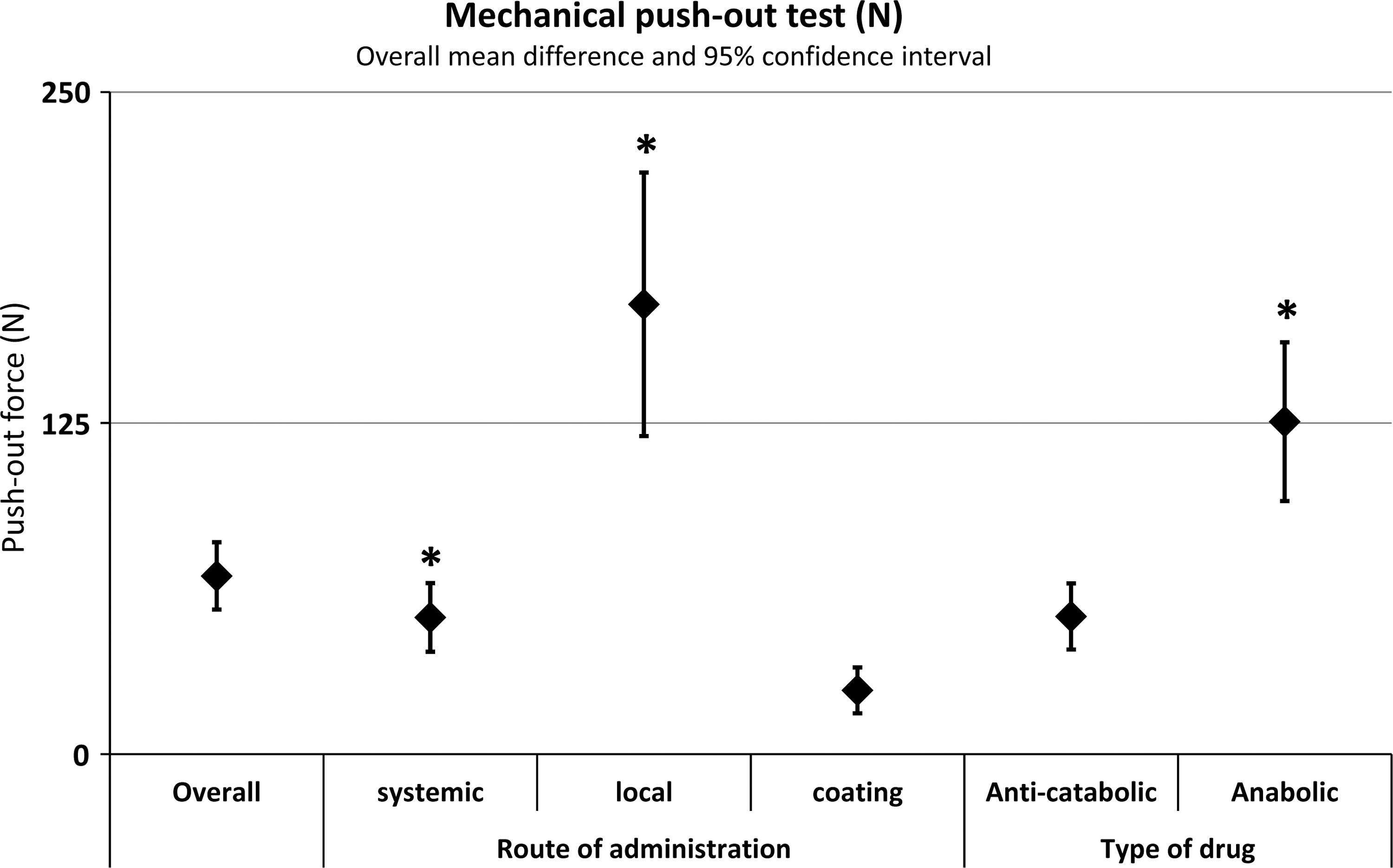
The mechanical push-out test (N). A scatter plot depicts the effect estimate (MD) with the 95% confidence interval for overall and subgroup analyses (per route and type of drugs). There is a significant difference between subgroups when their confidence intervals do not overlap. *p < 0.05.
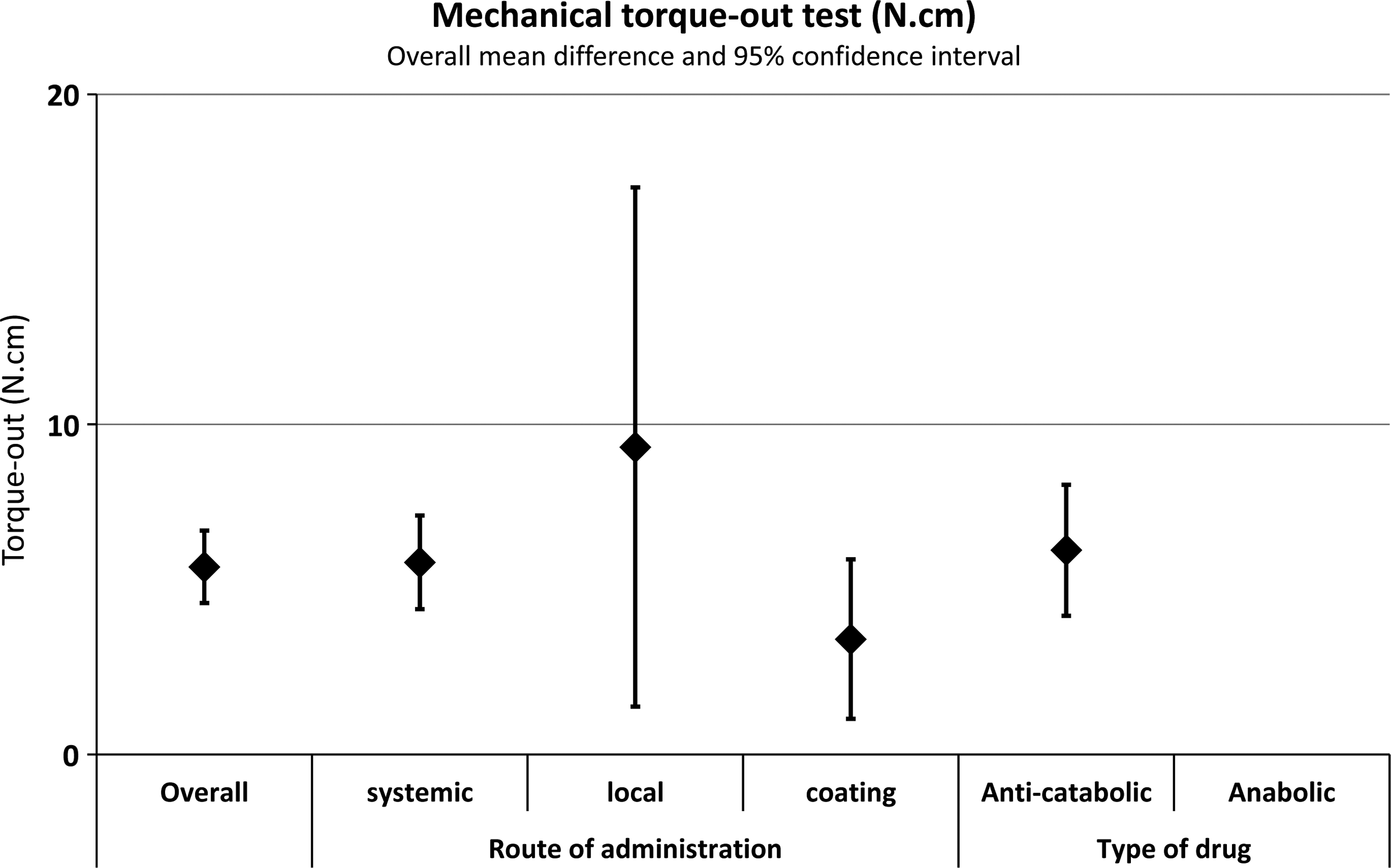
The mechanical torque-out test (N.cm). A scatter plot depicts the effect estimate (MD) with the 95% confidence interval for overall and subgroup analyses (per route and type of drugs). There is a significant difference between subgroups when their confidence intervals do not overlap. There are no available data for anabolic drugs subgroup.
Out of these, 109 comparisons showed a positive effect, 9 comparisons negative effect, and 92 comparisons showed no effect (Table 2). For micro-CT BV%, 1046 implants were involved in 71 comparisons (Table 1). Positive overall effects were observed in 51 comparisons. Only 1 comparison showed a negative effect, whereas there were no effects in 19 comparisons (Table 2). Regarding push-out testing, there were 68 experiments that used 972 implants to prove the overall benefit of osteoporosis medications on implants' mechanical stability (Table 1).
In Table 2, it shows that 38 comparisons confirmed the presence of positive effects of drugs on implants' stability, whereas 29 comparisons showed negative effects. There was only 1 comparison with no effect. Also, torque-out testing was applied on 776 implants to estimate a possible mechanical overall effect of antiosteoporotic drugs on titanium implants (Table 1). Out of 43 comparisons, it shows positive effects in 19 comparisons, negative effects in 2 comparisons, and no effect in 22 comparisons (Table 2). The heterogeneity for the overall analyses was very high (I2 = 99%).
Method of antiosteoporotic drug delivery
In Table 1 and Figures 3 to 6, we present the findings of subgroup analyses based on the method of drug delivery with implantation. Statistically, there was a significant effect of surface coatings on BIC% compared with local administration (Fig. 3). Also, it shows no significant differences between systemic administration and surface coating or local.
For micro-CT BV% (Fig. 4), it shows no differences between subgroups. Concerning implant fixation, a significant increase in push-out results was reported for local administration compared with systemic administration or surface coating (Fig. 5). Also, push-out testing showed significant difference in relation to the subgroup of systemic administration compared with surface coatings. For torque-out values, there were no significant differences between the three methods of drug delivery related to implantation (Fig. 6). The heterogeneity for the subgroup analysis was also very high (I2 = 99%). This indicates that subgroup analyses based on the route of administration did not explain the high heterogeneity found in the overall analyses.
Type of antiosteoporotic drugs
Table 1 and Figures 3 and 4 depict no statistical difference between anabolic drugs versus anticatabolic drugs in terms of BIC% and micro-CT BV% data. In Figure 5, it shows that anabolic drugs significantly increased push-out force compared with anticatabolic drugs. For torque-out outcome, there was no available data in the included studies to compare between the effects of anabolic drugs versus anticatabolic drugs on implant stability. Also, heterogeneity was very high (I2 = 99%) in the subgroup analyses based on the type of drugs and did not explain the high heterogeneity found in the overall analyses.
Publication bias
As shown in Supplement 5, the shapes of funnel plots (per main outcome variable) have no clear indications for the presence of small study effects as may be related to publication bias.
Discussion
The benefit of osteoporosis medication as used to enhance osseointegration of bone implants has been evaluated in several preclinical studies. However, it is always recommended to assess the translational potential of preclinical findings to a clinical population using systematic review and meta-analysis.48,49 The aim of the present review was to assess the benefit of using antiosteoporotic drugs during implant placement in animals. Then, we performed subanalyses to evaluate whether the treatment effect on osseointegration was related to the use of different delivery methods (systemic vs. local vs. surface coatings); or different types of drugs (anti-catabolic vs. anabolic).
Using random-effects meta-analyses, the results indicate overall improvements in implant osseointegration when adjunct administration of antiosteoporotic drugs is applied compared with without drug administration. Interestingly, the use of antiosteoporotic drugs showed positive effects on micro-CT BV% and BIC% in more than 50% of the evaluated comparisons.34,50–53 Moreover, the use of drugs showed in favor of push-out in 38 out of 68 comparisons. Also, increased torque-out values were observed in 19 out of 43 comparisons.54–56
In contrast, it has to be emphasized that several studies33,37,57–59 also presented no effects or negative effects of the use of drugs related to osseointegration. For example, Kim et al. 33 and Cuairán et al. 37 found that an administration of antiosteoporotic drugs did not improve the bone–implant contact and showed adverse histological features in bone healing, suggesting a negative effect on implant osseointegration.
Indeed, the current pooled results were sparse and not homogeneous across the whole review (I2 = 99%). Therefore, it has to be emphasized that the present findings should not be generalized because subgroup analyses did not explain the high heterogeneity found in the overall analyses. In addition, these results suggest that preclinical research is still limited, and generally unable to offer conclusive evidence about the benefit of using osteoporosis drugs with implant placements, and it also suggests that further (pre) clinical researches are warranted.
Regarding the subquestions, we first looked at the evidence of how the different methods of drug delivery (systemic vs. local vs. surface coatings) may affect implant osseointegration. Indeed, surface coatings significantly favored BIC outcomes compared with local administration but not to systemic administration. Besides, local administration favored push-out testing more than surface coatings or systemic administration. Also, systemic administration increased push-out forces more than surface coatings. In fact, the effectiveness of an osteoporotic medication depends on its ability to target and control a specific cellular/molecular process. Also, the concentration of medication at the target site is very important to control abnormal condition. 32 However, uncontrolled delivery of drugs (i.e., systemic administration) to the defected tissues may decrease the benefits of medications. 60
Currently, several technical approaches have been developed to provide a controlled release of medications, especially at the implantation sites.60,61 For instance, the method of surface coating has been used to carry drugs at the local site of titanium implants.32,60 In the present review, we found that implants coated with antiosteoporotic drugs showed increased osseointegration. 38 But, in another study, 62 antiosteoporotic drugs as placed onto titanium surfaces did not improve osseointegration. Thus, one can conclude that the techniques of implant surface coatings would meet several challenges before they can be transferred to the clinical population. Furthermore, it remains a challenging task for biomaterials scientists to develop a novel design of implants coated with antiosteoporotic drugs.
Second, we assessed all included data that examined if the type of drugs (anticatabolic vs. anabolic) has a different effect on implant osseointegration. Both types of drugs have similar results of micro-CT BV and BIC. However, anabolic drugs showed only a superior effect on the mechanical push-out testing outcomes. For example, Fu et al. 54 reported that simvastatin significantly enhanced the stability of pedicle screws by more than 400N (maximum force).
Also, in other studies, strontium ranelate 56 and parathyroid hormone 1–34 63 showed increased biomechanical findings of titanium implants in osteoporotic bone. Intriguingly, Linderbäck et al. observed no therapeutical effect of strontium treatment on implants fixation. 64 Consequently, the direct translation of present results to the clinic is not recommended. In general, it can be mentioned that the benefits of osteoporotic medications on osseointegration may be related to their ability to interfere in a positive manner with the bone regeneration process.27,65 Typically, osteoporotic medications are expected to serve in restoring the damaged tissue at the implantation site.37,50,59,66
In the present review, we have observed a wide variety of implantation models used to investigate the benefits of osteoporotic medications around titanium implants using different types of animals (i.e., mice, rats, rabbits, minipigs, dogs, pigs, and sheep). These animals were healthy or osteoporotic to mimic the clinical situation. Moreover, different outcome measures to evaluate implant osseointegration were extracted and used in our meta-analysis. These analytical methods to evaluate osseointegration through histological sections, 3D micro-CT, or mechanical tests are commonly provided in dental implant literatures.
The histomorphometrical quantification of BIC is the “gold standard,” although it only provides information based on 2D histological sections from a 3D complex bone–implant structure. The micro-CT is providing a volumetric set of data that needed to quantify bone tissues surrounding implants. As a disadvantage, it is worth mentioning that micro-CT is not an accurate method for examining bone at implant contact due to metallic scattering artifacts of X-rays. 67 Also, the various ways of testing implant stability are not very representative for osseointegration. 68 Therefore, we decided to use data of all these outcome measures as most presented in the included studies and it allows quantitative comparison between groups as well as subgroups in a meta-analysis.
Considering the fact that bone–implant healing takes place within the first few weeks, it is demanding to find a method to examine osseointegration at the early stage. However, conventional methodology of analysis does not allow visual discrimination of overlapping phases of bone healing around implants, and it is necessary to bear in mind the shortcoming of using these parameters to evaluate osseointegration. In addition, using appropriate analytical methods, a superior quantification of the healed bone–implant area can be performed to investigate the benefit of osteoporotic medications on osseointegration.
Some limitations of the present meta-analysis should be considered. For instance, the present findings are based on pooled data from different animal implantation models of 116 included studies. The presence of high heterogeneity may be caused by diversity in the included studies in terms of animal models, different anatomical sites of implantation, different healing periods, different bone conditions, different dose and time of drug administration, and different outcome measures. However, the subgroups performed did not explain the high heterogeneity found in the overall analyses. In addition, we were not able to provide details regarding the quality of studies and if there is a potential risk of bias per study.
Also, poor reporting of studies did not allow us to precisely assess the presence of risk of bias in the included studies. For this reason, there is obvious risk that we can overestimate the true effect of antiosteoporotic drugs on implant osseointegration in the present review. Also, because it was difficult to explore asymmetry in the funnel plot, we are not able to judge on the incident of publication bias. Consecutively, all studies should obey the ARRIVE guidelines to improve the quality of their animal studies.48,69
Finally, for successful clinical application, it is important to take into account the dose and concentration of drugs to be delivered with the implantation procedures. Systemic delivery of drugs combined with dental implant placement has potential limitations and benefits. The benefits include the ease of application, while problems relate to nonspecific distribution of drugs and side effects (i.e., osteonecrosis). Local application of bisphosphonates as well as anabolic drugs into implantation sites could be very advantageous in view of drug concentration directly into the healing site, controlled delivery, and preventing a possible systemic side effect. Utilization of antiosteoporotic drugs administered through the implant surface will advance in dental implant therapy in a challenged bone condition.
Conclusions
This meta-analysis indicates significant improvement in all outcomes of implant osseointegration due to the administration of antiosteoporotic drugs compared with implants without drug administration as observed in osteoporotic or healthy animal models. Concerning the route of administration, surface coatings showed an increase of bone formation onto implants. Also, the positive effect of anabolic drugs seems beyond the effect of anticatabolic drugs in terms of mechanical stability of implants as tested by push-out. These results show the biological benefits of osteoporotic medications on osseointegration. Further pre(clinical) trials on this subject are warranted.
Footnotes
Acknowledgment
The authors extend their appreciation to the Deanship of Scientific Research at King Saud University for funding this work through the research project No: (RG-1439-026).
Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.