
Abstract
Bioprinting is a recently developed technology that has great potential to manufacture artificial tissues and organs for transplantation. Recent studies have demonstrated promising results of small-scale bioprinted tissues with vascular structure and signs of their particular tissue functions. However, the recreation of a complex and multifunctional vascular network and the limitation of oxygen and nutrient diffusion in a human-scale tissue are still challenges in the current stage of this technology. Bioprinting technology has evolved different approaches to better create vascular networks in a small scale and high resolution. The use of patterned biomaterials and growth factors as well as the coculture of endothelial cells with other cell types has also been used to improve the angiogenesis and decrease the time for vascularization. Finally, the incorporation of materials for providing oxygen and suppressing cellular metabolism provides another strategy to overcome the limitations of oxygen and nutrient diffusion for bioprinted tissues.
Impact Statement
This review has a broad overview of the current challenges of bioprinted tissues towards clinical translations and future directions to overcome those challenges. The development of this field has a huge impact on the situation of an insufficient number of organ donors for life-saving organ transplantations.
Challenges of Bioprinted Tissues Toward Clinical Translation
V
The vascularization process can be divided into four stages: endothelial sprouts formation, sprouts anastomosis, lumen formation, and retraction of surplus capillaries. 3 Vascularization is initiated by pre-ECs that send out capillary sprouts. Then these sprouts anastomose with their adjacent sprouts to form a primitive capillary structure with multiple junction points. After anastomosis, the lumen is formed into each sprout away from their junction point followed by the formation of a continuous lumen, also called plexus, after several hours of the junction. 3 Finally, one of the sprouts is enlarged as the major pathway for blood flow, whereas other capillary sprouts are retracted as capillary blood vessels.
Tissue vascularization is crucial to ensure the cell viability and future clinical translation of tissue or organ substitutes that have a thickness >400 μm. 4 Unfortunately, this process occurs at a rate of several millimeters per day, which means the vascularization of a human-sized tissue should take several months to complete, 5 by which time the tissue will experience necrosis because of the lack of nutrients and oxygen.
Bioprinting is a technology that has great potential to create complex human vascular network. With the development of bioprinting technology, such as the use of coaxial/multiaxial nozzles and indirect bioprinting method, complex vascular network with the junction of intermediate microvessels and macrovasculature were successfully created.6–9 With further perfusion with ECs, bioprinted vascular structure showed lumen formation and enhanced the proliferation and differentiation of other cell types nearby.
Bioprinting has the advantages of high resolution, the ability to create complex 3D structures, increased reproducibility, and potential to create custom designs based on each individual patient's needs.10,11 By printing cells isolated from the recipients, we can expect the eventual ability to produce bioprinted tissues with complete biological functions without transplant rejection. Many simple tissues, such as muscle, cartilage, and bone, have been successfully printed at a small scale; however, the slow vascularization rate is still a crucial challenge in the creation of human-sized bioprinted tissues that are suitable for clinical translation.12–15
Therefore, a key challenge is to prevent tissue necrosis during the vascularization process. One solution is through the supply of nutrients and oxygen to cells or to reduce the cellular requirement of nutrients and oxygen. Another solution is to increase the vascularization rate. Bioprinting technology can be used for creating vascular channels to speed up the vascularization process; however, the recreation of a complex and multifunctional vascular network is still difficult and time-consuming. Besides that, adding growth factors, coculture ECs with other cell types, and the use of some biomaterials are other alternatives to enhance the vascularization process.
In this review article, we discuss the current approaches to address the challenges of bioprinted tissues and future directions to move bioprinted tissues from the proof-of-concept stage to clinical translation.
Current Approaches to Overcome the Challenges of Bioprinting Vascularized Tissues
In this section, current developments of bioprinted tissues toward clinical translation are discussed through four approaches: improving bioprinting technology, enhancing angiogenesis, adding oxygen-generating material, and suppressing cellular metabolism. To address the challenge of printing complex and high-resolution/small vascular structures, the development of bioprinting technology should improve the feasibility of bioprinting complex vascularized tissues. Enhancing angiogenesis should increase the proliferation and differentiation of vascular structure and shorten the vascularization period.
To prevent cell death because of oxygen and nutrient depletion in a human-sized bioprinted tissue, adding oxygen-generating materials and materials to suppress cellular metabolisms are potential answers. Adding oxygen-generating materials is an approach to provide in situ oxygen supply to tissues during the vascularization process to prevent their necrosis. Suppressing cellular metabolism works as an inhibitor to reduce the requirement of oxygen and nutrients for the cell growth. The combination of these approaches has the potential to move bioprinted tissues to clinical translation.
Improving bioprinting technology
Bioprinting is a relatively new engineering approach for fabricating vascularized structures. Another promising approach to product large, vascularized tissues is tissue decellularization and recellularization. However, tissue decellularization process can destroy some microvasculature that results in significant challenges in avoiding vascular leakage after recellularization.16–18
Compared with other engineering approaches, such as electrospinning and casting methods, the major advantage of bioprinting is its ability to control the distribution of materials and cells in different areas from the same bioprinted construct.19,20 Other advantages include the ability to customize the tissue based on the patients' requirements, the flexibility to control matrix materials to manipulate their mechanical properties, high manufacturing precision, high manufacturing reproducibility, and so on. 21
Current approaches for bioprinting vascularized tissues can be separated into two major categories: direct bioprinting and indirect bioprinting. Table 1 summarizes some of the advantages and disadvantages of these two approaches.
Direct bioprinting using single axial nozzle is not an excellent tool for creating vascularized tissues because of the lack of multidimensional resolution and accuracy required for fabricating microvessels. Recently, coaxial or multiaxial printing nozzles are used in the direct bioprinting for the preparation of vascularized structure with microvasculature.6,22–28 This system constitutes one or multiple channels within the same nozzle tip. Luo et al. reported a shell/core coaxial nozzle for the bioprinting of a hollow vascular structure using concentrated alginate bioink. 26 The diameter of the microchannel created by this nozzle was ∼100 μm, which is difficult to achieve using other engineering approaches.
Jia et al. reported a novel method to prepare perfusable vascularized constructs by a bioprinter equipped with a multiaxial nozzle system and a formula of bioink containing 4-arm poly(ethylene glycol)-tetra-acrylate (PEGTA), sodium alginate, and gelatin methacryloyl (GelMA). 6 A two-step cross-linking was used for the preparation of vascular constructs. Ionic cross-linking was applied between calcium chloride (CaCl2; inner and outer channels) and sodium alginate (middle channel) resulting in temporary printability and structural stability of the bioink. Covalent photo cross-linking was conducted by the cross-linking between PEGTA and GelMA under the ultraviolet (UV) exposure leading to final vascular constructs that were mechanically strong. A maximum compressive modulus of 50.7 ± 3.0 kPa was achieved by adding 3% (w/v) PEGTA into GelMA. The vascularized constructs showed beneficial biological properties including supporting the attachment, proliferation of encapsulated ECs and stem cells, and the formation of well-organized and perfusable artificial blood vessels.
In another study, Gao et al. reported a novel approach to manufacture tissue engineered constructs with built-in vascular microchannels through a bioprinter with a coaxial nozzle, as given in Figure 1A. 22 A maximum tensile strength of 0.116 MPa was achieved using 4% sodium alginate and 0.9 mm spacing between adjacent filaments. In addition, the presence of built-in vasculature significantly increased the viability of L929 mouse fibroblasts compared with the control, as given in Figure 1B; however, the overall cell viability kept decreasing over the 7 days of culture. 22
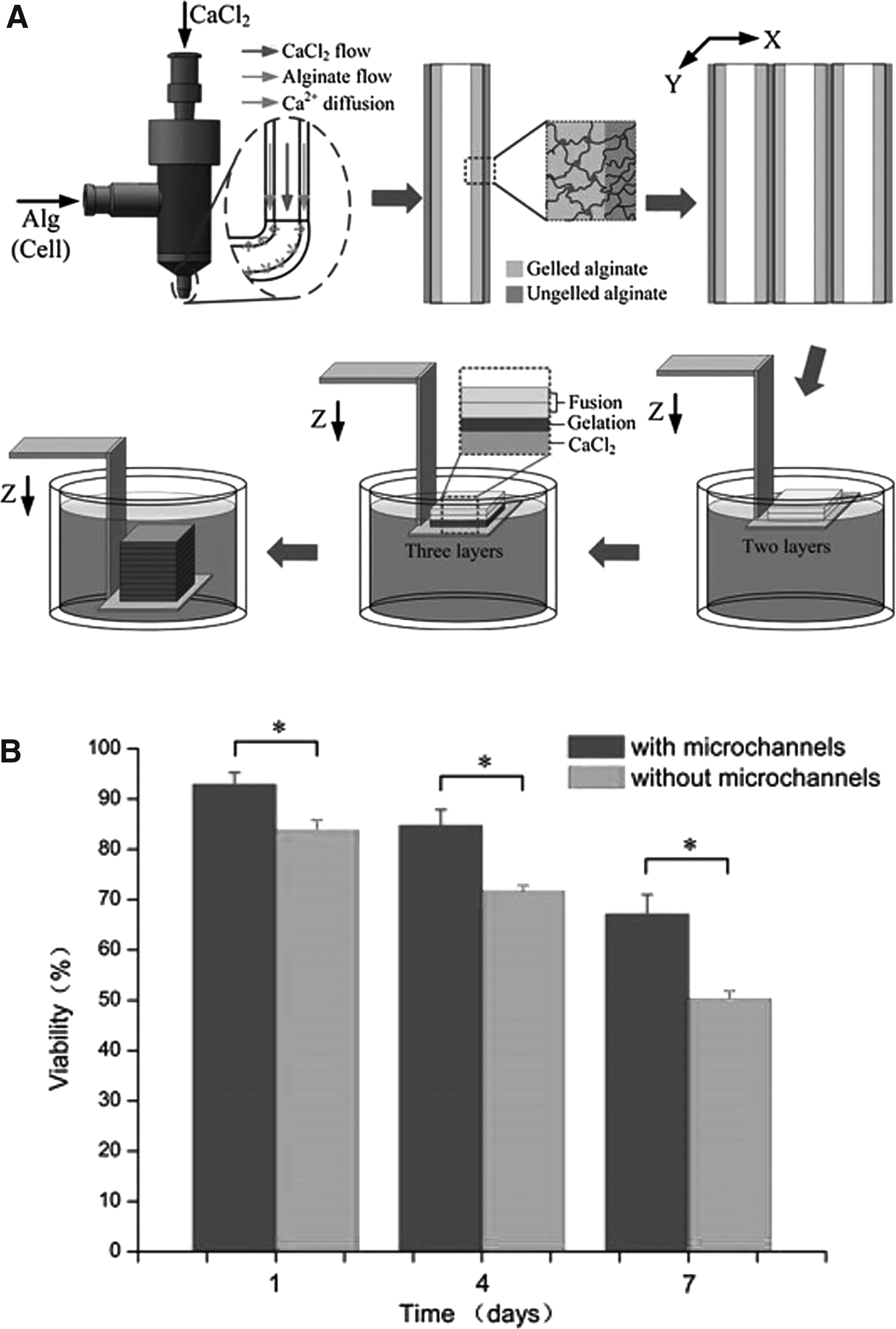
One possible reason for the decreased viability might be the use of alginate-based bioinks that might be a substandard bioink for supporting tissue vascularization. 29 The development of other bioinks compatible with the coaxial or multiaxial nozzle system is crucial for this approach to further advance to clinical translation. Another reason might be the limited vascular orientation. Microchannels only in the horizontal direction can restrict the transportation of oxygen and nutrient through the entire construct.
The use of coaxial or multiaxial nozzle provides an efficient way to directly prepare vascularized structure with a small diameter and high resolution close to 100 μm, which is a step forward to overcome the challenges of manufacturing vascularized tissues through bioprinting. Overall, the direct bioprinting is a simple and fast approach to fabricate micron-range capillary networks; however, the disadvantages of direct bioprinting including the limitation of available bioinks, the inability to create branched vascular structure over a range of scales, and the decrease of cell viability because of the extrusion pressure are hindering the development of this approach to clinical translation.
Another approach to fabricating the vascularized structure is through indirect bioprinting, where the vascular structure is not directly printed by the nozzle but by the removal of a fugitive material.
Pluronic F127 is a commonly used fugitive bioink for creating microchannels as the vascular network.9,30–32 It is composed of poly(propylene oxide) (PPO)x-poly(ethylene oxide) (PEO)y-PPOz that experiences a thermally reversible gelation. 30 When the temperature is above the critical micellization temperature, a Pluronic F127 bioink with the concentration above the critical concentration will present its hydrophobicity and gel-like rheological properties, which is appropriate for the bioprinting. 33 However, below the gelation temperature, the Pluronic F127 bioink will show its hydrophilicity and water-like rheological properties to make this material easy to be removed. 33 This gel-to-fluid transition makes Pluronic F127 a perfect fugitive bioink for fabricating the vascular structure.
Kolesky et al. reported an approach to fabricate a tissue engineered construct with multiple cell lines and vascular structure. 30 Pluronic F127 at 40 wt% was used as the fugitive bioink for making microchannels as the vascular structure. These microchannels were further vascularized by the ECs. GelMA was used to mix with two different cell lines for cell printing. Results showed the ability of this method for fabricating both intermediate microvessels and macrovasculature with diameters ranging from 100 μm to 1 mm. In addition, lumen formation was observed during the cell culture, and the built-in vascular network significantly enhanced the cell viability of human neonatal dermal fibroblasts and 10T1/2 fibroblast cells.
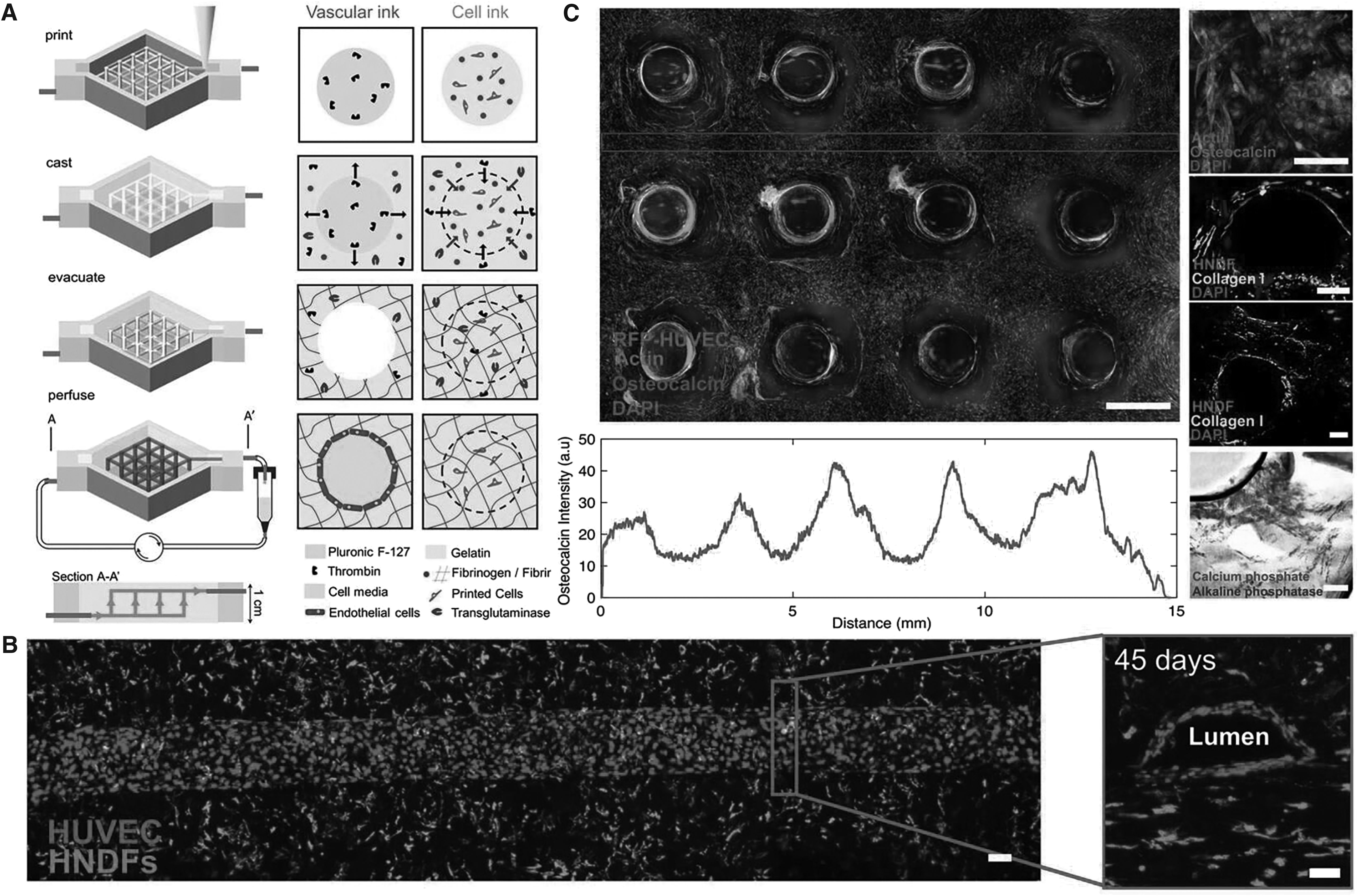
In a follow-up study, the same group reported the manufacture of 3D cell-laden and vascularized tissues with a thickness >1 cm by bioprinting, as given in Figure 2A. 9 Pluronic F-127 and thrombin were mixed as the first bioink for printing the vascular structure. Then human mesenchymal stem cells (hMSCs), human neonatal dermal fibroblasts, fibrinogen, and gelatin were mixed as the second bioink for printing the bone tissue. A solution with the composition of fibrinogen, gelatin, CaCl2, and transglutaminase was used as the extracellular matrix (ECM) to cast the whole tissue engineered construct followed by the rapid cross-linking. Pluronic F-127 was evacuated for creating microchannels as the built-in vascular structure. Then human umbilical vein endothelial cells (HUVECs) were seeded into the microchannels to vascularize the vascular network. The final tissue engineered constructs were further perfused for a time period of >6 weeks. Lumen formation was clearly observed after 45 days of the perfusion, as given in Figure 2B. In addition, the differentiation from hMSCs to osteoblasts and observation of new bone formation were found by the expression of osteocalcin, collagen I, calcium phosphate, and alkaline phosphatase, as given in Figure 2C. 9
Other bioinks, such as gelatin,20,34,35 agarose,36–38 and carbohydrate glass, 8 have also been used as the fugitive material for fabricating vascularized tissues through indirect bioprinting. Gelatin and agarose are biocompatible materials and easy to remove to form microchannels as vascular structure. Lee et al. reported a new method for producing a vascularized tissue that has microvasculature with a diameter of 1 mm surrounded by the capillary network. 34 The macrovasculature was created by removing the gelatin. The capillary vascular network was connected to the macrovasculature through the angiogenetic sprouting within the fibrin hydrogel matrix. This connection was clearly observed by the confocal microscope.
Similar to gelatin, the vascular structure was also prepared by removing the agarose rods that were created by a bioprinter. 37 Surrounding the vascular network, osteoblast-laden GelMA hydrogel was cross-linked by UV light. The created vascular structure was further vascularized by the perfusion of HUVECs suspension. Results showed that the presence of the vascular network significantly improved the cell viability and differentiation of osteoblasts.
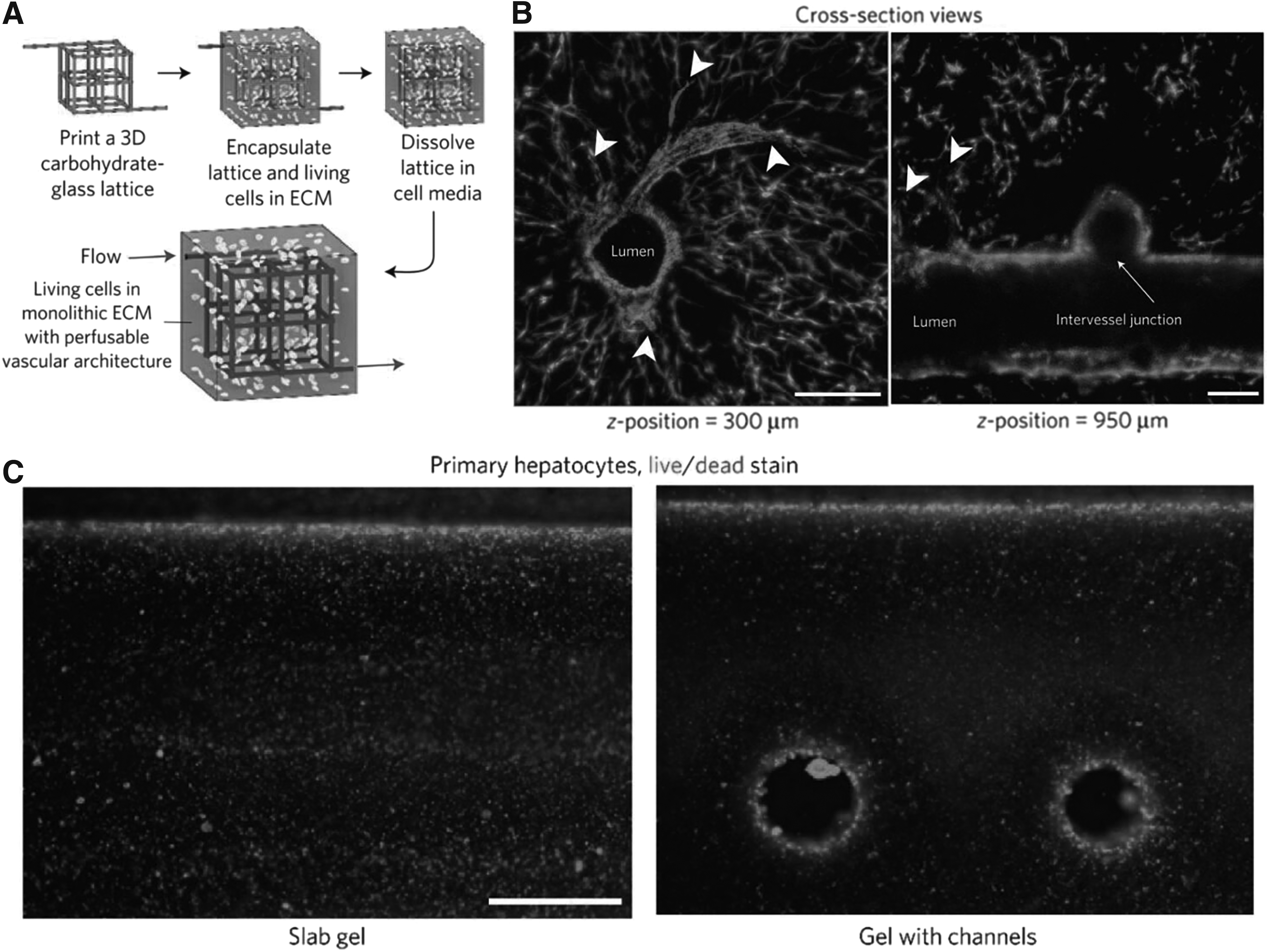
In addition, Miller et al. reported a novel carbohydrate glass fugitive material for creating the vascular structure, as given in Figure 3A. 8 At room temperature, this carbohydrate glass was mechanically stiff and brittle, but could be easily removed by immersing into cell medium to create a vascular network. After the seeding of HUVECs over the vascular network for 9 days, the endothelialized lumen formation was achieved (Fig. 3B), which enhanced the cell viability of hepatocytes, as given in Figure 3C. 8
The advantages of indirect bioprinting include the ability to create branched vascular structure, high printing resolution without concerns of decreased cell viability because of the extrusion pressure and a wide range of material selection for bioinks and fugitive materials. However, the removing fugitive material in a large-scale and complex structure can be difficult and time-consuming, which is the major drawback to this approach. Additional disadvantages include the requirement for postprocessing, such as the perfusion of vascular structure with endothelium cell suspension, whereby consistent cell seeding and endothelialization is not guaranteed.
A novel droplet-based bioprinting technique has also been used for making vascularized tissues.39–43 This approach can create cell-seeded subordinate millimeter-sized droplet modules from the nozzle and allow them to assemble into structures with interstitial space that is similar to the vascular structure for the perfusion of medium or blood. 1
Pataky et al. reported a microdroplet-based bioprinting system for the preparation of vascularized structure with different geometries. 41 Alginate droplets were printed onto a CaCl2-loaded gelatin substrate for the gelation with upward-diffusing Ca2+ ions. Through this gelation process, microchannels were formed as the vascular structure showing great biocompatibility with fibroblasts. In addition, the authors combined collagen and alginate in the bioink for the preparation of the vascular network to simulate the natural ECM; however, the limitation of this droplet-based bioprinting includes nozzle clogging because of small nozzle diameter, thermal and mechanical stress on cells during droplet extrusion, and limited cell types that are suitable for this bioprinting technique. 44
Enhancing angiogenesis through biomaterials, growth factors, and coculture
Enhancing angiogenesis is an approach to enhance the regeneration rate of de novo vascular network formation. Some biomaterials, such as collagen,45–47 fibrin/fibrinogen,34,45,48–50 and hyaluronic acid,51,52 have been reported to improve angiogenesis.
Collagen is a natural hydrogel that has been widely used in 3D printing technology for biomedical applications. 53 Stratesteffen et al. reported a novel GelMA–collagen blend bioink that was used in a drop-on-demand bioprinting system for inducing in vitro angiogenesis. 47 Annularly shaped hydrogel constructs were co-printed using a bioink blend of GelMA, type I collagen, and Irgacure 2959 and also cells including hMSCs and HUVECs followed by UV cross-linking. The vascular structure was observed in vitro in the bioprinted structure after 14 days. In addition, the presence of collagen in GelMA improved hMSCs spreading and showed spindle-like cell morphology.
Fibrin is also a natural hydrogel formed through the conversion of soluble fibrinogen with the presence of thrombin. 54 It has been reported to promote lumen formation with polarized ECs sprouting.8,55,56 In a previous study, it was used as the EC carrier for the preparation of multiscale vascular structure through the bioprinting technique. 34 The embedded HUVECs within fibrin hydrogel showed the morphological transition from initial plexus to complete capillary network and then finally to lumen formation. The morphological features, vascular network distribution, and diameter of the capillaries in this work were close to the natural vascular system.
In addition to inducing angiogenesis using biomaterial ques, vascular endothelial growth factor (VEGF) is a crucial growth factor that has been reported to stimulate angiogenesis in vitro and in vivo.34,57–60 It was reported that adipose-derived stromal cells transfected with an adenovirus encoding the cDNA of VEGF on a large poly(lactide-co-glycolide) (PLGA) scaffolds induced vascular network growth inside the scaffolds. 61 People have also utilized VEGF in bioprinted tissue engineered constructs to stimulate vascular network formation.
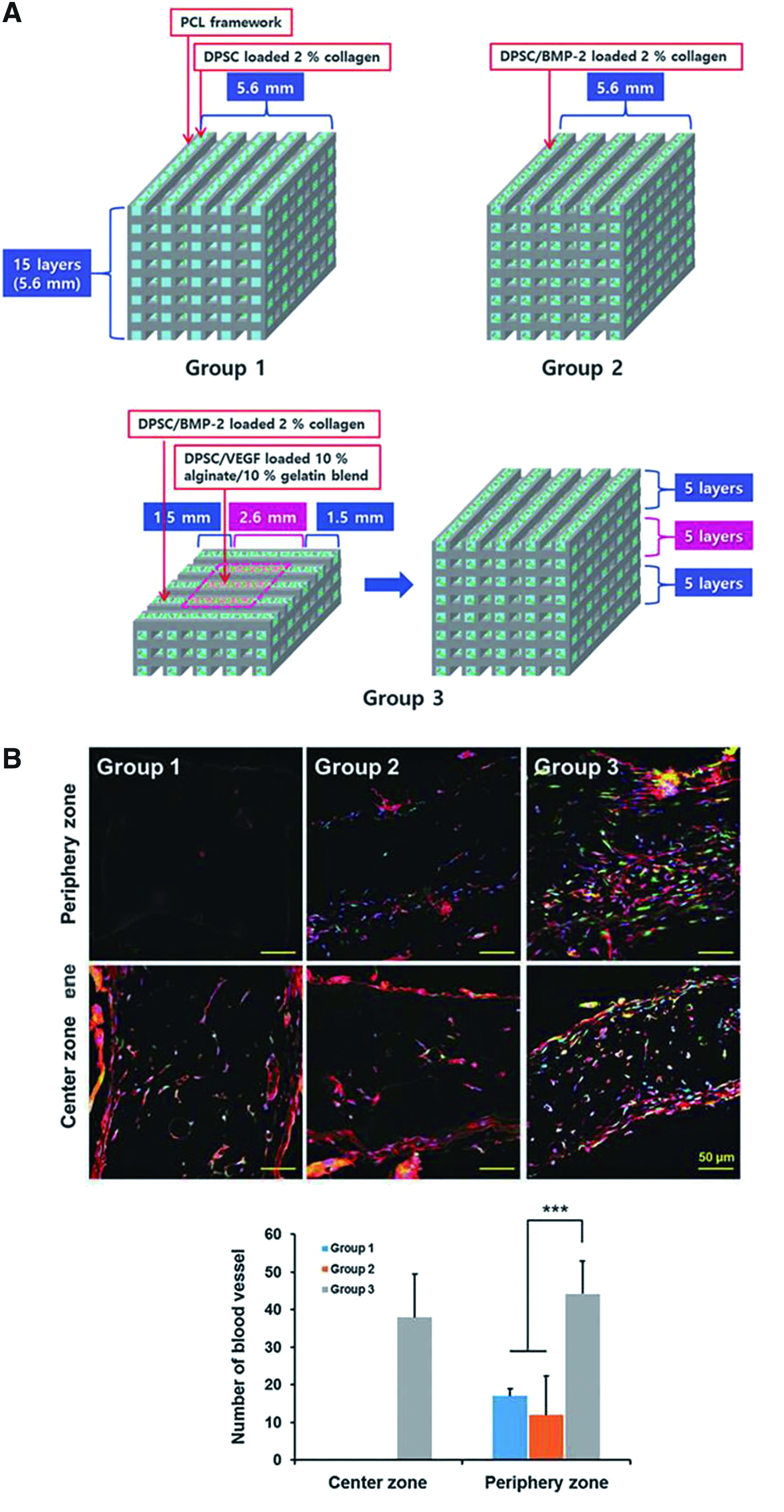
Park et al. reported a novel approach to load bone morphogenetic protein 2 (BMP-2) and VEGF in the peripheral and central regions of bioprinted scaffolds, respectively, to induce vascularized bone regeneration, as given in Figure 4A. 60 The framework was printed by polycaprolactone and the peripheral region was printed using mesenchymal dental pulp-derived stem cells (DPSCs)/BMP-2 loaded 2% collagen, whereas the central region was printed by DPSCs/VEGF loaded 10% alginate/10% gelatin blend. The bioprinted construct was implanted subcutaneously in a mouse for 28 days for in vivo characterizations. Results showed significantly enhanced vascularization in the peripheral and central regions from group 3 compared with the bioprinted construct without the prevascularized central region, as given in Figure 4B. 60
ECs are able to proliferate and differentiate to create vascular networks; however, the presence of other cell types, such as fibroblasts,34,45,62 smooth muscle cells (SMCs),63–66 and MSCs,9,47,67,68 can further promote the angiogenesis of ECs. The coculture of fibroblasts and ECs was reported to promote the angiogenesis because fibroblast can produce endogenous growth factors, such as VEGF,69,70 platelet-derived growth factor, 71 and transforming growth factor-β 72 that are necessary for the blood vessel formation. The use of the coculture to induce the angiogenesis of ECs has extended to bioprinted tissues. In a previous study reported by Kreimendahl et al., the enhanced capillary-like vascular network was observed in the bioprinted agarose/collagen scaffolds because of the effects of the coculture of fibroblasts and ECs. 45
SMCs are the major cell type located in the blood vessel wall and play a crucial role in the maturation of vascular regeneration during the wound healing processes.73,74 It was reported that the coculture of SMCs and ECs could enhance the angiogenetic response of ECs through the secretion of VEGF and ECM by SMCs.75–80
In another study, a novel laser bioprinting method was used to co-print HUVECs and SMCs. 66 This approach utilized the focused laser pulses to transfer cell-laden material from the carrying support to the receiving substrate. For the coculture of HUVECs and SMCs, HUVECs were first printed followed by incubation for 24 h. Then SMCs were printed on top and around the previously patterned HUVECs. With the coculture of SMCs, it limited the overgrowth and migration of HUVECs compared with the monoculture of printed HUVECs. In addition, the coculture of HUVECs and SMCs showed lumen-like vascular structure with multiple junctions indicating a synergistic effect on developing their cellular morphologies.
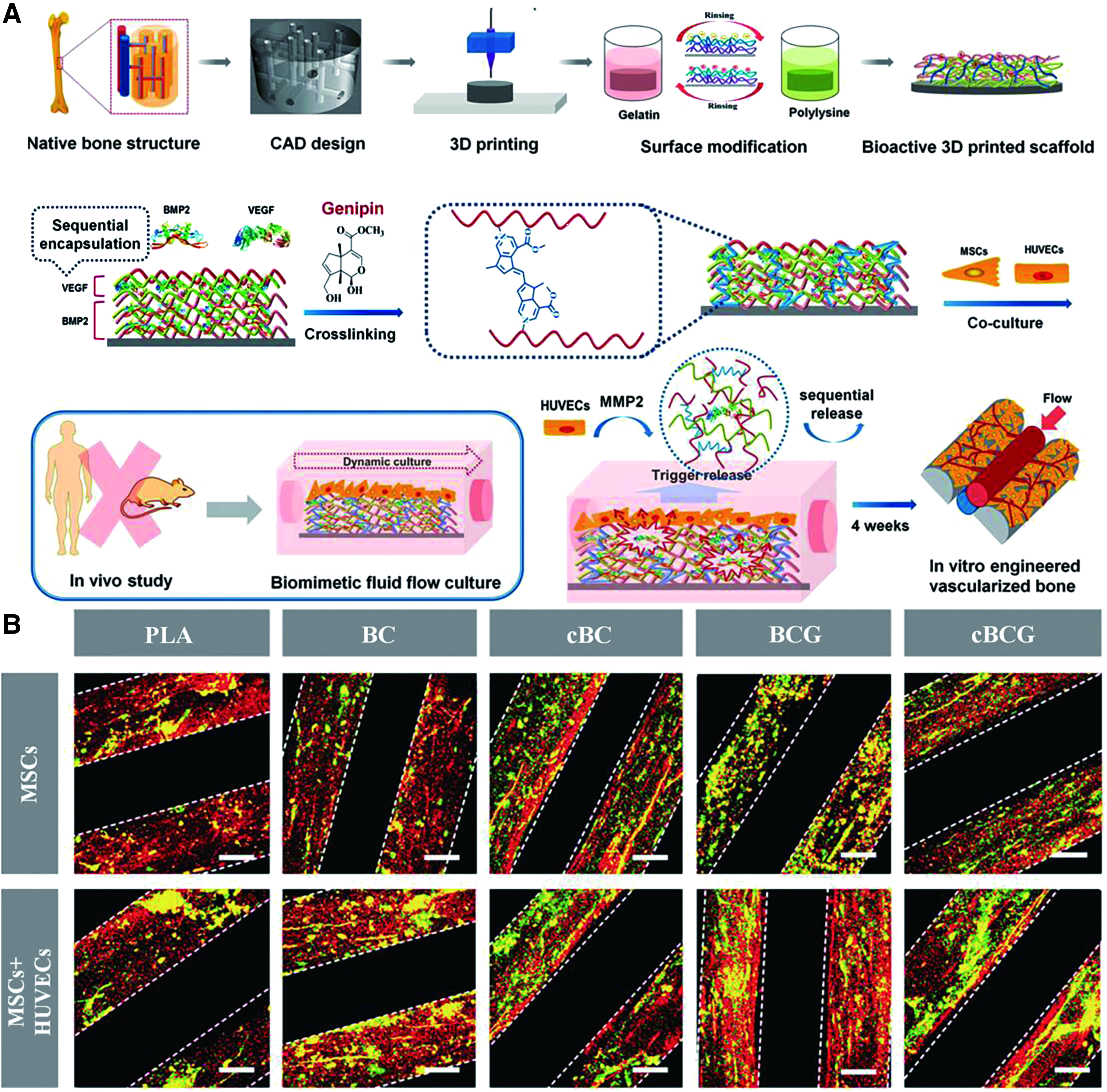
It was reported that the combination of ECs and MSCs enhanced angiogenesis and helped in the formation of robust vascular network in a construct implanted into a murine model.81–83 This coculture system was applied in the bioprinted perfusable scaffold for the vascularized bone tissue formation, as given in Figure 5A. 68 To simulate the native bone structure, a series of interconnected vertical and horizontal channels were designed in a cylinder-shaped scaffold. Then the scaffold was printed followed by the bioactive nanocoating using electrostatic assembly. At the same time, growth factors, such as recombinant human (rh)BMP-2 and rhVEGF, were absorbed in the nanocoating to control their release. The coculture of MSCs and HUVECs was conducted on the scaffold in a bioreactor to simulate the in vivo environment. After 4 weeks, the coculture of MSCs and HUVECs showed mature vascular structure compared with the limited vascular formation in the dynamic MSCs monoculture, as given in Figure 5B. In addition, with the presence of nanocoating loaded with rhBMP-2 and rhVEGF on the scaffold, the vascularized bone formation was significantly enhanced. 68
The vascularization process is improved significantly by adding growth factor and coculture with other cell types; however, the vascularization of a human-sized construct might still take several months to complete. To further improve angiogenesis, genetic engineering, or the combination of multiple cells, different biomaterial types and growth factors may be future approaches.
Oxygen-generating materials
Oxygen is a key factor for the functionalization of a bioprinted tissue; however, oxygen supply is normally inhibited by the diffusion process. 84 Cells in the central region of a human-sized bioprinted construct will suffer from the hypoxic condition and start necrosis if they are >200 μm from a vascular structure. 85 Even with current progress in improving bioprinting technology and enhancing angiogenesis, vascularization rate is still not fast enough to provide sufficient oxygen for a bioprinted construct with clinically relevant size.
One way to overcome this challenge is to have the in situ delivery of oxygen to cells during the vascularization period. There are two major types of oxygen delivery approaches, high adsorbing fluid oxygen delivery and chemically generated oxygen delivery. High adsorbing fluid oxygen delivery, such as Lifor® and perfluorocarbons, utilizes materials that have a high saturation of oxygen for the delivery of oxygen to areas of need.86–88 However, the oxygen delivery using this approach is fast and is in a linear manner that restricts its use in tissue engineering applications. Chemically generated oxygen delivery produces oxygen through the chemical reaction of oxygen-generating materials. This approach has a slower oxygen release rate than high adsorbing fluid oxygen delivery, which is more appropriate for tissue engineering applications.
Most common oxygen-generating materials for chemically generated oxygen delivery include hydrogen peroxide, sodium percarbonate (SPO), and calcium peroxide (CPO). Some studies reported the effectiveness of oxygen-generating materials for the short-term oxygen supply in several healthcare applications, such as the prevention of ischemic muscle injury, but the research of them in long-term oxygen supply for tissue engineering applications was limited.89–93
One in vitro study reported by Oh et al. showed that the presence of CPO enhanced cell viability under hypoxic condition for up to 10 days in poly(lactic-co-glycolic acid) (PLGA) scaffolds. 89 Another study reported the use of SPO as the dressing material to treat ischemic tissue in a mouse model; however, the oxygen release could only be observed for 24 h and the dressing with SPO could only prevent tissue necrosis for 3 days. 90 Then a follow-up study was performed by combining SPO and CPO in the dressing to prolong the release of oxygen. 91 This approach significantly extended the oxygen release period for >3 days and enhanced the wound healing process in a dermal wound model of old pigs.
Recently, a novel approach was reported using hydrogen peroxide-releasing microspheres to control the oxygen release.92,94 Hydrogen peroxide was bound to poly(N-vinylpyrrolidone) as the core of microspheres, whereas PLGA was used as the shell of microspheres to control the release kinetics of hydrogen peroxide. This successfully supplied the oxygen to cardiosphere-derived cells (CDCs) and maintains their viability for 14 days. 92 Oxygen was still detected after 28 days under 1% O2 hypoxic condition. 94 In addition, CDCs with the presence of the hydrogel containing hydrogen peroxide-releasing microspheres showed similar cTnT, MYH6, and CACNA1c expression compared with normal CDCs after 14 days of culture under hypoxic condition. 92
With current promising results, the use of oxygen-generating materials in bioprinting might be a promising next step to move the bioprinting forward to clinical translation. However, one major challenge is to control kinetics for a long-term oxygen release. In addition, the high oxygen levels may cause oxidative stress that can reduce the cell growth. Further research should focus on achieving a low rate but constant oxygen release through coating or chemical modification using oxygen-generating materials. Meanwhile, the size of coated or chemically modified oxygen-generating materials should be optimized to prevent the clogging issue during the bioprinting process.
Suppressing cellular metabolisms
Another approach to address the challenge of tissue necrosis during the vascularization process is to suppress the cellular metabolism. Similar to placing cells into temporary hibernation, suppression of cellular metabolism can reduce the survival requirement of oxygen and nutrient for cells to increase their viability during the vascularization process. Adenosine is a purine nucleoside that functions as an energy transferring molecule. 95 It has been reported to play a crucial role in decreasing neuronal excitability and neurotransmitter release resulting in effectively reduced neuronal energy requirements. 96
The suppression of cellular metabolism through the use of adenosine has been shown to increase the cell viability under hypoxic condition. 95 The presence of adenosine was reported to suppress the metabolism of muscle cells and maintained their viability under hypoxic condition for 11 days. After transferring back to normoxic conditions, cells restored their growth rate comparable with those maintained under normoxic condition.
However, 11 days are still too short for vascularization to complete. It was also reported that the high concentration of glucose could improve the cell viability under hypoxic condition. 97 Temporomandibular joint disc cells cultured under 25, 5, and 1.5 mM glucose media showed significantly higher viability compared with the 0 mM glucose control under 1% O2 environment after 48 h; however, it is also too short for any type of vascular structure formation in a human-sized bioprinted tissue.
The use of adenosine or glucose demonstrates its promising applications in bioprinting; however, the limitation is to match the effective time of adenosine or glucose with the vascularization period. As adenosine suppresses localized cellular metabolism, there is a risk that this approach may also suppress neovascularization. A central challenge to this approach is to induce vascularization while suppressing the metabolism of other cell types that are sensitive to low oxygen and nutrient levels. Optimization and innovative strategies must be developed to prolong the effective time of adenosine/glucose suppression and induce vascular structure formation.
Conclusions
In summary, the use of bioprinting for biofabrication of human tissues for transplantation has developed substantially over the past decade. Many studies have demonstrated promising in vitro and in vivo results to overcome the challenges of achieving vascularization and functionalization in bioprinted tissues. However, bioprinted tissues are still restricted to small-size constructs with only immature vascular networks achieved thus far. Current bioprinting techniques, such as coaxial/multiaxial bioprinting, indirect bioprinting, and droplet-based bioprinting, have their own advantages and disadvantages. Combining several printing techniques together can be an approach to facilitate the biofabrication of vascularized tissues. In addition, the development of new bioprinting technologies that can achieve the specific patterning of a wide range of biomaterials, growth factors, and cells types should induce the formation and maturation of a vascularized tissue and facilitate the progress of bioprinted tissues toward clinical translation.
Some approaches, such as the addition of oxygen-generating materials and adenosine/glucose, have not been used in bioprinting, whereas they are very promising to be incorporated in bioinks for realizing the goal of clinical translation of bioprinted tissues. The combination of all these approaches is the future of bioprinting and should advance the progress of bioprinted tissues toward clinical translation.
Footnotes
Acknowledgment
The authors acknowledge the funding from the Armed Forces Institute for Regenerative Medicine (AFIRM) under the grant numbers W81XWH-14-2-0003.
Disclosure Statement
No competing financial interests exist.