
Abstract
Nipple–areola complex reconstruction is a common procedure that often accompanies breast reconstruction. Historically, local skin flaps were utilized for nipple reconstruction, with more recent techniques exploring the addition of implanted material. Tissue engineering and regenerative medicine (TE&RM) represents a potential source of stable and biocompatible implantable tissue, which may have a positive effect on cosmetic outcomes. Conventional TE&RM techniques involve seeding a scaffold with the patients' own cells and using growth factors to promote survival. The clinical applicability of these techniques is limited by its cost and ability to produce sufficient volumes of viable tissue. This article reviews the evolution of nipple reconstruction techniques and current TE&RM protocols; these two fields are then combined to propose a novel approach of using TE&RM scaffolds to augment conventional nipple reconstruction.
Impact Statement
This work provides a comprehensive overview and critique of nipple reconstruction techniques to date. It then explores different tissue engineering concepts and how these may improve clinical outcomes for patients undergoing nipple reconstruction. A novel technique is proposed, whereby a three-dimensional-printed tissue-engineered construct is used as an autologous graft to assist nipple reconstruction.
Introduction
The most common application of nipple–areola complex (NAC) reconstruction is in breast cancer patients who have undergone a mastectomy. The cosmetic success of NAC reconstruction is evaluated by position, shape, texture, pigmentation, and projection. Despite the countless flap and augmented-flap techniques reported in the literature, no gold standard has emerged, and to date, no one technique provides a consistently reliable method of nipple reconstruction.
This article reviews the currently available techniques and expected outcomes from the reported literature. We also report a promising novel technique utilizing three-dimensional (3D) printing to construct a nipple scaffold that is seeded with autologous tissue containing multipotent stem cells to produce a tissue-engineered construct (TEC).
Methods
A PubMed literature search was conducted with the base filters of “nipple” AND (augment* OR reconstruct*). The results were further refined toward an augmented-flap approach using the keywords “autologous,” “synthetic,” “cartilage,” “fat,” “adipose,” “dermis,” “collagen,” “transplant,” “prosthesis,” “graft,” and “implant.” Tissue engineering base search filters included “tissue engineer*” OR “regenerative medicine.” The results were further refined using the keywords “biomaterial*,” “additive manufactur*,” “3D print*,” “scaffold,” “vasculari?*,” and “adipose.” All searches included articles from database inception to May 24, 2016, with results being restricted to English articles.
Current NAC Reconstruction
The NAC is the defining feature of the breast mound. Its reconstruction may be necessitated by developmental absence, trauma, burn injury, or most commonly, breast cancer requiring mastectomy. The diagnosis of breast cancer and its subsequent treatment is a distressing event for patients, many of whom suffer lasting psychological sequelae.1,2
Breast reconstruction reduces the psychological strain, low self-esteem, and sexual dysfunction experienced by patients following mastectomy. 3 Moreover, reconstruction of the NAC has been found to further improve general and aesthetic satisfaction. 4 The nipple is often viewed as the finishing touch of the entire reconstructive process and holds considerable symbolic significance for patients. Wellisch et al. 5 proposed that nipple reconstruction confers a psychological benefit that extends past the purely physical–sensory realm; they found that patients who elected for a breast and nipple reconstruction reported an improved perception of breast symmetry, softness, and sensitivity compared with patients who underwent a breast-only reconstruction. 5 Thus, the presence of a nipple appears to subconsciously influence the patient's evaluation and acceptance of their overall breast reconstruction.
NAC reconstruction is typically performed 3–5 months after breast reconstruction, once the potentially distorting swelling and inflammation have subsided. 6 At present, the choice of technique is largely dependent on the surgeon's personal preference and, to a lesser extent, patient factors. Procedures may be complicated by partial or total flap necrosis, local infection, wound dehiscence, or seroma. 7
Long-term loss of nipple projection is an ongoing challenge for surgeons and is the primary source of patient dissatisfaction.7,8 Studies comparing several flap-based reconstructions reported that nipple projection stabilized at 12 months and that shrinkage during this period ranged from 40% to 70%. This was attributed to a combination of scar contracture, retraction forces from surrounding skin, and inadequate vascularization.9–11
Areola reconstruction
Areola reconstruction has been accomplished with autologous skin grafts,12,13 tattooing,14,15 and AlloDerm—a decellularized dermal matrix. 16 Skin grafts are the oldest of these techniques and are harvested from sites with the best texture and pigment match—commonly the inner thigh or contralateral areola.12,17–25 AlloDerm has been tested as an alternative graft material and represents an effective, although costly, solution to the donor site morbidity associated with skin grafts. 16
Current practice heavily favors intradermal tattooing for areola reconstruction due to its technical simplicity, lack of donor site morbidity, and superior pigmentation. It is mostly performed before nipple reconstruction as scarred skin and elevated structures are suboptimal sites for tattooing. Some degree of depigmentation is commonly observed months to years later, and secondary tattooing is often required to correct the color mismatch between natural and reconstructed areolae.15,26
Composite graft reconstruction
As with areola reconstruction, the initial challenge for nipple reconstruction was recreating the original nipple's pigment and texture. These features were first replicated in 1949 by Adams 27 who used a composite graft from the labia minora. Later, Millard 17 described a “nipple-sharing” technique, whereby a split-skin graft was obtained from the patient's contralateral NAC. Composite grafts have also been harvested from autologous toe pulp,28,29 auricular cartilage, 30 and skin from the superior inner thigh. 19
Initially, nipple-sharing was the predominant form of NAC reconstruction despite mediocre results; pain, depigmentation, scarring, infection, and loss of sensation frequently complicated donor grafts.24,25,27,28 There is questionable value in exchanging one normal nipple for two inferior ones, and patients are often reluctant to harm their remaining nipple. However, nipple-sharing does produce excellent pigment and texture match, and thus, this procedure may still be indicated for patients with hypertrophic nipples (>1 cm height).
Flap-based reconstruction
Local skin flaps have been used to recreate nipple projection from as early as 1946, although they were not widely adopted until the 1980s. 31 Flap techniques revolutionized nipple reconstruction as they caused fewer local tissue complications and less donor site morbidity, and ultimately, they replaced composite grafts as the preferred procedure (Fig. 1). 6 Although nipple-sharing techniques better preserve nipple projection compared with flap-based reconstruction, flaps allow surgeons to overbuild the nipple by 25–50% and thus pre-empt the ensuing shrinkage. 32 This overbuilding is effective in maximizing projection; however, the erratic vascularization and contracture of flaps make it difficult to predict the nipple's final appearance. As such, obtaining symmetry with the contralateral nipple remains an ongoing challenge. 6
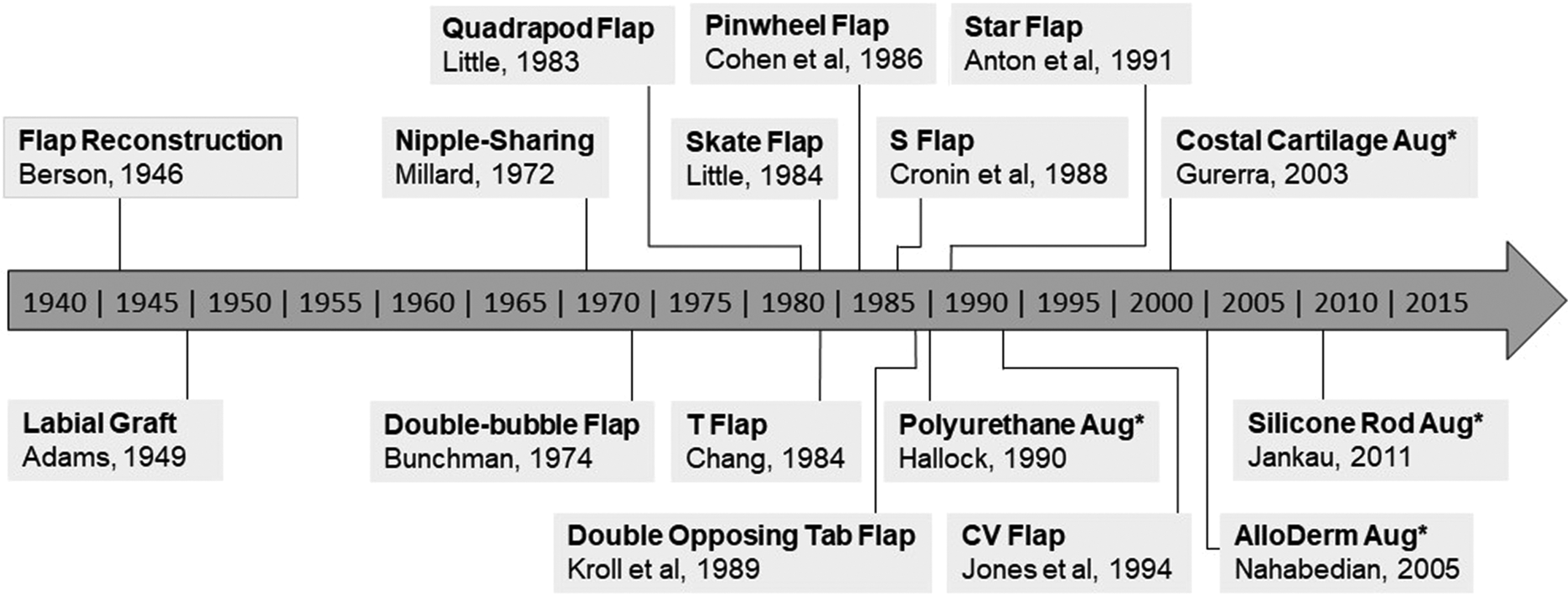
History of prominent nipple reconstruction techniques. *Augmented-flap reconstruction.
Flaps are classified as “centrally based” or “subdermal pedicle” techniques, with the latter being further stratified into single or double pedicle techniques. Centrally based flaps are the older of the two and experience greater retraction forces, and subsequently greater shrinkage, because the entire base is affected by contracture of the underlying tissue and surrounding skin. Subdermal pedicle flaps decrease retraction forces by employing only a small base with the remainder of the flap being released from the underlying tissue.
A redefining event in NAC reconstruction was Anton et al.'s 33 use of the star flap. Jones and Bostwick 34 later modified this into the C-V flap, a technique still frequently used in current procedures.35–37 Before these techniques, flap-based reconstruction involved de-epithelializing the surrounding skin and future areola site; a skin graft would then be used to cover this area. However, the star and C-V techniques did not require such extensive de-epithelialization subsequently obviating the need for skin grafts and averting the associated donor site morbidity.
Autologous augmented-flap reconstruction
Today, flap-based NAC reconstruction continues to be plagued by poor long-term cosmetic outcomes. 8 It has been hypothesized that nipple shrinkage is exacerbated by the absence of rigid connective tissue support, and it is this notion that provided the impetus behind the current augmented-flap techniques being developed. 38
Augmented-flap NAC reconstruction aims to increase structural integrity by incorporating a central core of material into the flap. Autologous tissue was the first material to be tested and produced only modest improvement in nipple projection over traditional techniques. 30 Guerra et al. 39 pioneered the use of a costal cartilage graft obtained from the third rib at the costochondral–sternocostal joint. Several studies replicated this technique and reported marginal improvement in the maintenance of nipple projection and a nonsignificant change in patient satisfaction compared with traditional flap reconstruction.40–42 The advantage of costal cartilage augmentation lies in its convenience: free-flap breast reconstruction necessitates the exposure of the internal mammary artery, after which costal cartilage can easily be accessed. The cartilage graft is then harvested and banked subcutaneously on the chest wall for NAC reconstruction in the following months. Costal cartilage grafts are not applicable in patients with prosthesis-based breast reconstruction as this procedure does not require internal mammary artery exposure, and the increased invasiveness of obtaining a graft outweighs the marginal cosmetic benefit.40–42
Cartilage grafts have also been harvested from the auricular concha.30,43,44 This approach is beneficial in the context of less invasive prosthesis-based breast reconstruction. However, there is a risk of greater donor site morbidity due to the limited blood flow to the external ear. Tanabe et al. 44 reported an excellent maintenance of projection (94.7%) with no flap complications; however, further research may be warranted due to the study's small sample size (n = 8) and failure to comment on donor site conditions.
Rolled dermal tissue obtained during the revision of breast reconstruction scars has used to augment nipple reconstruction.37,45
Synthetic augmented-flap reconstruction
Several synthetic structures have been used in augmented-flap NAC reconstruction, and while they were considerably efficacious in maintaining nipple projection, all materials were associated with a host of adverse complications. In a preliminary study of two patients, Hallock 46 used polyurethane-coated silicone gel prostheses. These produced qualitatively superior projection compared with purely flap-based reconstruction, although an absence of recorded measurements makes such comparison unreliable. The author expressed concern for patient safety with regard to the established risks of polyurethane: hematoma, toxicity, allergic and immune reactions, and potential carcinogenicity. 47 Similar risks were noted in Wong et al.'s 48 implementation of polytetrafluoroethylene for nipple reconstruction; again, this study reported high levels of patient satisfaction but failed to record quantitative values.
Jankau et al. 49 experimented with implantable silicone rods; they reported a 100% rate of local flap necrosis and rod extrusion in patients who received a latissimus dorsi flap breast reconstruction, and nipple shrinkage of 33.9% in patients who received a transverse rectus abdominis flap breast reconstruction. 49 The increased pressure from the latissimus dorsi flap combined with the rigidity of silicone compared with natural tissues likely caused extrusion of the prostheses. Given that there is often a paucity of skin following breast reconstruction, there appears to be limited applicability for silicone rod-augmented NAC reconstruction.
Allogeneic augmented-flap reconstruction
Under the right conditions, allogeneic implants undergo neovascularization, which is thought to contribute to graft survival and produce lasting results. 11 AlloDerm is an acellular matrix of human dermal collagen, elastin, and laminin and is the most heavily researched material for allogeneic augmented-flap NAC reconstruction. 50 Despite the theoretical advantages, AlloDerm-augmented nipples displayed shrinkage of 50–70% and failed to produce a statistically significant improvement in long-term projection compared with traditional flap-based reconstruction.51,52 Furthermore, the cost of the material, US $480–$1500 per nipple implant, all but excludes it as a viable material for augmented-flap NAC reconstruction. 53
Kim and Lee 54 explored the potential for lyophilized cadaveric costal cartilage to be used as a cost-effective alternative to AlloDerm. Although lyophilized cartilage has been used successfully in rhinoplasty and nasal reconstruction, it provided no discernible benefit for nipple projection at 1 year.55,56
Tissue Engineering and Regenerative Medicine
Tissue engineering and regenerative medicine (TE&RM) is a burgeoning field, which combines knowledge of cell biology and chemistry with the engineering concepts of materials and structure design. At present, significant volumes of skin, 57 cartilage, 58 and bone 59 have been cultured in vivo. Further innovations in TE&RM have led to practices, whereby a scaffold, a solid or gel-based support structure, is seeded with a host's cells to form a TEC. TECs are employed as tissue grafts, providing the necessary bulk for reconstructive procedures while avoiding donor site morbidity; however, the ultimate goal of TE&RM is not only the replacement of tissue bulk but also the restoration of tissue function. 60
The term “microenvironment” describes the complex physical and biochemical interactions that occur on a molecular level between the scaffold, seeded cells, and host tissue. These interactions dictate the attachment, migration, proliferation, and differentiation of adipose-derived stem cells (ASCs). 60 Cell culture was traditionally performed in a two-dimensional environment, a process that proved ineffective in facilitating cell and extracellular matrix (ECM) interactions. 61 The development of 3D biomaterial scaffolds addressed this problem and was the first step in producing a customizable microenvironment.
All scaffolds must abide four key principles: biodegradability, low immunogenicity, porous architecture, and structural integrity. A biomaterial scaffold, by definition, must undergo biodegradation and integration into host tissue. This process has proved advantageous for wound healing, vascularization, and bacterial clearance.62,63
Immunogenicity and foreign body reactions are driven by macrophage and giant cell attachment at the tissue–material junction with the extent of these reactions being dictated by the scaffold's complex surface chemistry. 64 In a review of breast prosthesis materials, Puskas and Luebbers 65 found that biomaterial implants produced fewer foreign body reactions compared with traditional implants. 65 As such, a biomaterial nipple scaffold could be expected to reduce the incidence of postoperative flap necrosis and local infection in reconstructed nipples.
The long-term deformation and loss of projection that currently plagues nipple reconstruction is partly due to inadequate vascularization. Tanabe et al. 44 noted superior long-term projection in bi-lobed flaps, supplied by a rich subdermal vascular plexus, compared with tri-lobed variants, which received their circulation only from the inferior floor. Moreover, inadequately vascularized adipose tissue has been associated with volume losses of up to 60%. 66 The porosity of a scaffold is intimately linked with its capacity to undergo vascularization and support adipose tissue ingrowth and survival; thus, pore size and distribution is a critical factor when considering nipple scaffold design. 67
The structural integrity of a scaffold is essential for maintaining appropriate nipple shape during the process of adipocyte proliferation. Once implanted, the TEC is subjected to considerable forces both from wound contracture and daily activity, and as such, it must be sufficiently robust to withstand these deforming mechanical loads. An important consideration in scaffold design is the trade-off that exists between the TECs structural integrity and its porosity. 68
The advent of additive manufacturing, otherwise known as 3D printing, conferred a range of advantages to scaffold production: better control of architectural complexity, high reproducibility, and access to a diverse range of raw materials. 69 Given the rate at which this technology is advancing, it is quickly becoming a realistic and cost-efficient option for scaffold fabrication. However, additive manufacturing was not initially designed with biological applications in mind; traditional substrate preparation and extrusion methods are often hazardous to biomaterials, and thus, it is an ongoing challenge to find a biomaterial that (i) is compatible with the 3D printing process and (ii) demonstrates physical–biochemical properties appropriate for a TE&RM scaffold. Current practices employ either naturally derived materials such as collagen, alginate, decellularized ECM, fibrin, gelatin, hyaluronic acid, and silk or synthetic polymers such as polylactic acid (PLA), polyglycolic acid (PGA), and polycaprolactone (PCL).70–74 Generally, natural biomaterials demonstrate superior biocompatibility; however, with the exception of collagen, there has been limited success in fabricating these materials into 3D structures.71,75
The advantage of synthetic polymers lies in the capacity to customize their mechanical and chemical properties toward a specific goal. The body metabolizes PLA and PGA at different rates so by blending these materials into the copolymer polylacto-co-glycolic acid (PLGA), it is possible to customize the rate of degradation. 76 Despite this, long-term in vivo longevity of both natural and synthetic biomaterial scaffolds leaves much to be desired.77,78 In the interests of expediting clinical applications of 3D-printed nipple scaffolds, it may be prudent to focus on synthetic biomaterials such as PLGA or PCL, which have already been approved in a number of devices by the Food and Drug Administration.76,79
Common TE&RM practice is to seed scaffolds with cells to improve graft viability and longevity. ASCs are a subset of mesenchymal stem cells with a multipotent differentiation capacity that includes adipocytes, chondrocytes, myocytes, and osteoblasts. 80 They are favored for their extensive profile of cytokine and growth factor secretion, which produces proangiogenic, antiapoptotic, and anti-inflammatory effects.81,82 As a result, superior outcomes in graft retention and vascularization have been reported in ASC-augmented grafts compared with traditional autologous adipose grafts.83–85 Lipoaspirate is commonly obtained from patients' abdominal fat and consists of mature adipocytes and a heterogeneous mixture of ASCs, preadipocytes, endothelial cells, smooth muscle cells, fibroblasts, mast cells, and pericytes—collectively referred to as stromal vascular fraction (SVF). 86 To obtain isolated ASCs, the SVF is subjected to a lengthy process of centrifugation and enzymatic degradation. However, instead of isolating the ASCs, it appears that simply removing triglycerides from the lipoaspirate via centrifugation is sufficient to promote adipogenesis.86,87 Such “purified lipofilling” procedures have been extensively utilized in breast reconstructions and have the benefit of being easily performed on-site while minimizing laboratory manipulation. 88 Furthermore, Bernard and Beran 89 reported “satisfactory” results following their experimental use of lipofilling to correct failed nipple reconstructions in 13 patients. As such, seeding scaffolds with concentrated lipoaspirate seems a practical and cost-effective alternative to using isolated ASCs.
A novel approach to TEC generation is to seed scaffolds after implantation into the graft site, in contrast to traditional in vitro culture methods. This approach employs the host tissue as a bioreactor where local endothelial cells are allowed to first infiltrate the scaffold and initiate neovascularization before in vivo seeding procedures. This follows the TE&RM principle of “angiogenesis before adipogenesis” and may compensate for the decreased proliferative capacity of heterogeneous lipoaspirate compared with isolated ASCs.
TEC-Based Nipple Reconstruction
To date, a TE&RM approach to nipple reconstruction has been mentioned twice in the literature. Cao et al. 90 recreated nipples in porcine models using an injection of autologous auricular chondrocytes and a reverse thermosensitive polymer gel-based scaffold. They placed an intradermal purse-string suture at the site of injection to improve the shape and contour of the reconstructed nipple. Pashos et al. 91 also proposed a method of reconstruction whereby the NAC of a rhesus macaque primate was excised and decellularized to produce a scaffold. Their intention was to seed this natural scaffold with bone marrow-derived stem cells and reimplant it into the primate.
The TEC represents a promising and underexplored avenue for nipple reconstruction that may address the inadequacies of current flap and augmented-flap techniques. A gap exists in the literature for an accessible and mass-producible method of reconstruction that also minimizes nipple shrinkage, local complications, and donor site morbidity. We propose a TEC-based “flapless” technique of nipple reconstruction, where a 3D-printed biomaterial scaffold is seeded with autologous adipose tissue; this structure would then be implanted subdermally at the future NAC site. As with Cao et al.'s 90 procedure, a purse-string suture may be necessary to achieve optimal contour. Given the considerable role of psychological factors in patients' postsurgical satisfaction, the concept of regenerating one's own tissue may appeal to patients, thus further advocating for a TE&RM approach to nipple reconstruction.
Flapless nipple reconstruction better preserves the underlying vasculature, thus facilitating superior skin/graft vascularization, and thus superior long-term nipple projection, compared with traditional flap techniques. In addition, the absence of complex incisions or flap manipulation decreases the incidence of postoperative scarring, contracture, and wound dehiscence. 6 This approach has been proposed for cases where prosthesis-based breast reconstruction results in a thin soft-tissue envelope. In such scenarios, there is a greater risk that flap-based NAC reconstruction may expose the underlying breast implant. Moreover, the stretched tissue exerts internal pressure on the reconstruction, which exacerbates long-term shrinkage. 48 Colwell and Breuing 92 described their flapless approach in 55 nipple reconstructions; they implanted a subdermal cylinder of AlloDerm, which was then circumscribed with a purse-string suture. The authors were “pleased with long-term maintenance of low profile projection” at follow-up 3 years later.
A TE&RM approach may broaden the clinical applicability of nipple reconstruction in patients who have undergone radiotherapy. Radiotherapy is a common adjunct to the surgical management of breast cancer, and although it is effective in damaging the rapidly dividing cancer cells, it also has adverse consequences for nearby tissue. A state of chronic ischemia is induced in the tissue, which results in impaired healing, subcutaneous fibrosis, and, in severe cases, radionecrosis. 87 In a review of 146 nipple reconstructions performed on irradiated breasts, Satteson et al. 93 found that radiation was associated with a statistically significant increase in postoperative complications. 93 Centrifuged lipoaspirate has been shown to ameliorate such complications through the initiation of neovascularization and oxygenation of radiotherapy-damaged tissue. The damaged tissue underwent considerable structural transformation and did not require surgical excision. 87 The regenerative capability of this lipoaspirate was attributed to the SVF, which is in line with the current literature heralding the proadipogenic and proangiogenic properties of ASCs.81,87
Challenges
Current TE&RM practices have difficulty generating sufficient vascular networks in TECs, which limits the total volume of potential grafts. In the absence of endothelial infiltration and angiogenesis, the size of the TEC is limited by the diffusion range of oxygen (100–200 μm). 94 This is especially pertinent for adipose tissue, which has a low ischemic tolerance due to its high metabolic activity. 95 Strategies such as in vitro scaffold prevascularization with endothelial cells,96,97 implantable arteriovenous loops,98,99 3D printing with proangiogenic bio-ink, 100 and the co-administration of growth factors86,101 (vascular endothelial growth factor [VEGF], platelet-derived growth factor, fibroblast growth factor-2, and insulin-like growth factor 1) have been explored. A common limitation of these procedures is that their success has been restricted to small volumes of adipose tissue (<2 cc). While this may be problematic for larger reconstructions, current injectable methods of autologous and allogenic augmented-flap nipple reconstruction use volumes ranging 1.0–2.5 cc.38,89,102,103 Thus, an adequately vascularized nipple TEC appears to be achievable goal given the current state of TE&RM.
Patient safety should always be at the forefront of the development of any novel procedure. There is concern that the ASCs contained in SVF may contribute to tumor growth and metastasis via signaling molecules (cytokines and growth factors), myofibroblast differentiation, and ECM alterations. 104 For all the advantages that vascularization confers to TEC proliferation and survival, it may, in fact, be a double-edged sword. VEGF has a prominent role in supporting TEC angiogenesis and adipogenesis, although is also a prominent target for cancer-preventing therapies. 105 The use of heterogeneous lipoaspirate may represent a more measured approach as the concentration of ASCs is lower than that of isolated preparations. Visscher et al. 106 noted that although the potential carcinogenicity of lipoaspirate is concerning, at present, the risk remains entirely theoretical. In their review of the literature, they found no significant evidence of increased breast cancer recurrence following lipofilling procedures. Though, the authors did stress the necessity for further high-quality studies into this matter.
Future directions
The current state of TE&RM and scaffold design suggests that clinical trials using nipple TECs may already be technologically possible. Our group has been investigating an alternative approach to breast reconstruction using joint TE&RM and lipofilling principles. A smaller volume structure, for instance the nipple, may be an appropriate stepping-stone in the development of such techniques. An important consideration in animal trials will be the selection of an implant site that appropriately mimics the tension and thickness of the overlying skin following breast reconstruction.
Conclusion
The optimization of nipple projection and donor site morbidity following NAC reconstruction has been an enduring pursuit for surgeons. Despite the breadth of flap and augmented-flap techniques that have been proposed, one singly effective technique is yet to emerge. Modern TE&RM practices demonstrate improved morbidity rates and graft survivability due to the ability of TECs to stimulate vascularization along with stem cell proliferation and differentiation. A TEC-based approach to nipple reconstruction is now within reach given the recent advancements in biomaterials, additive manufacturing, and lipofilling; however, before clinical trials can commence, further research into the potential carcinogenic effects of ASCs is necessary. A TE&RM approach to nipple reconstruction represents a promising reimagining of conventional techniques, and its development will pave the way for host of future TE&RM applications.
Footnotes
Disclosure Statement
D.W.H. is a founder and shareholder of Bella Seno. D.K., O.U., D.B. have no competing financial interests.