
Abstract
Hope is that tissue engineering will provide a solution to meet the growing needs for bone substitutes. Among the potential solutions, three-dimensional (3D) printing is a promising method to fabricate functional bone substitutes especially for treatment of complex and critical-sized bone defects. Despite its encouraging achievements, 3D printing of bone substitutes still faces serious challenges including mechanical strength, shape complexity, optimization of pore parameters, and vascularization. The newer approach, that is, 3D bioprinting, is also confronted with challenges, which have prevented the realization of the dream of fabricating functional patient-specific bone substitutes. This article reviews the major challenges toward 3D printing and bioprinting of bone substitutes and recent studies addressing them. Potential solutions for each challenge and future directions are also provided.
Impact Statement
This review provides a current overview of the challenges in 3D (bio)printing of bone substitutes and summarizes the potential solutions.
Introduction
Although bone has mechanisms for dynamic remodeling and self-healing, large bone defects need external interventions and/or regenerative techniques to be repaired. The smallest size intraosseous wounds unable to self-heal are called critical-sized bone defects (CSBDs).1,2 A CSBD can be caused by a disease or a trauma with lifetime regeneration rate of <10%. 3 Thus, external interventions are needed to repair CSBDs and larger defects. The main treatments to restore and regenerate CSBDs are bone grafting, bone transport, and bone tissue engineering.4–6
Bone grafting
Bone grafting has been a routine clinical practice in orthopedic and spine surgeries,7,8 reconstructive surgeries of traumatic/tumor bone lesions,9–11 corrective craniomaxillofacial surgeries,12,13 and bone augmentation procedures in dental implant dentistry.14,15 In 2012, the global number of annual bone grafting procedures was estimated to be 2.2 million. 16
Autografts, allografts, xenografts, and alloplastic (synthetic) grafts are different classes of bone grafts. 17 Each type of bone graft has its own advantages, disadvantages, indications, and limitations.
Autografts are usually harvested from a patient's iliac crest or fibula and possess osteogenic cells and osteoinductive growth factors, without the risk of immunogenicity. The main drawbacks of autografts include potential risk of infection at the donor and graft sites, pain and morbidity at the donor sites, and limited availability in elderly patients and children.18,19
Allografts are mainly derived from donated cadaveric bones. Rigorous chemical treatments and gamma irradiation during sterilization deteriorate osteoinductivity of allografts and decrease their fracture toughness and bending strength. 20 The other disadvantages of allografts are risk of infection transmission and costly laborious processes.7,21
Xenografts are obtained by decellularization, deproteinization, demineralization, and freeze drying of bovine, porcine, or equine bones. Xenografts suffer from low mechanical properties, 22 and the risk of the zoonotic disease transmission. 23
Synthetic bone grafts lack osteogenic and osteoinductive properties. Yet, because of the precise control of structural composition and porosity, and the lack of disease transmission and donor site morbidity, majority of the studies in the recent two decades have focused on developing synthetic bone grafts.24–26
Bone transport
Bone transport technique, also known as Ilizarov surgery, is a widely practiced method that has been used to repair bone fractures and defects. The method is based on distraction osteogenesis, in which controlled directional mechanical stresses are applied on the bones at the defect site to induce new bone formation.27,28 The major applications of bone transport technique include repairing femoral and tibial fractures, correction of limb shortening, and reconstruction of maxillofacial deformities.29–32 Compared with bone grafting, bone transport is easier, safer, and cheaper. Furthermore, it allows for simultaneous bone and soft tissue repair. However, this method suffers from long-lasting treatment period that results in patient discomfort and imposes psychosocial distress over the patients and their families.30,33
Bone tissue engineering
Tissue engineering has emerged as a promising solution to meet the ever-increasing demand for tissue substitutes. Despite the obstacles and limitations, innovations of tissue engineering have attracted great scientific and public interests during the past decade.34,35
One of the promising approaches in tissue engineering is three-dimensional (3D) printing of tissues and organs.36,37 Using an additive approach, 3D printing is developed to position biomaterials and biomolecules precisely in a layer-by-layer 3D order resembling the extracellular matrix. 38 The ultimate goal of 3D printing is to fabricate and assemble various tissues and organs, including skin, liver, bone, cartilage, cardiovascular, and neuronal structures.39–46 3D printing is in its early days of creating functional tissues and organs; however, it has found unprecedented applications in high-throughput drug screening and discovery47–49 and fabrication of research models especially for cancer studies.50,51
More than 40 different 3D printing methods have been devised, among which fused deposition modeling (FDM), stereolithography (SLA), selective laser sintering (SLS), photopolymer jetting, and powder binder jetting are the most widely used modalities. 52 For 3D printing of cellular microenvironments, several biomaterials are used as inks, including natural biomaterials (gelatin, alginate, collagen, fibrin, hyaluronic acid, and hydroxyapatite [HA]), synthetic biomaterials (polyethylene glycol [PEG], polycaprolactone [PCL], polylactic acid [PLA], polyglycolic acid, poly(lactic-co-glycolic acid) [PLGA]), and hybrid biomaterials. Recent progress had led to the emergence of advanced inks with high printability, high strength, high viscoelasticity, and high cell viability and the ability to regulate cellular functions. 53
3D printing of bone substitutes
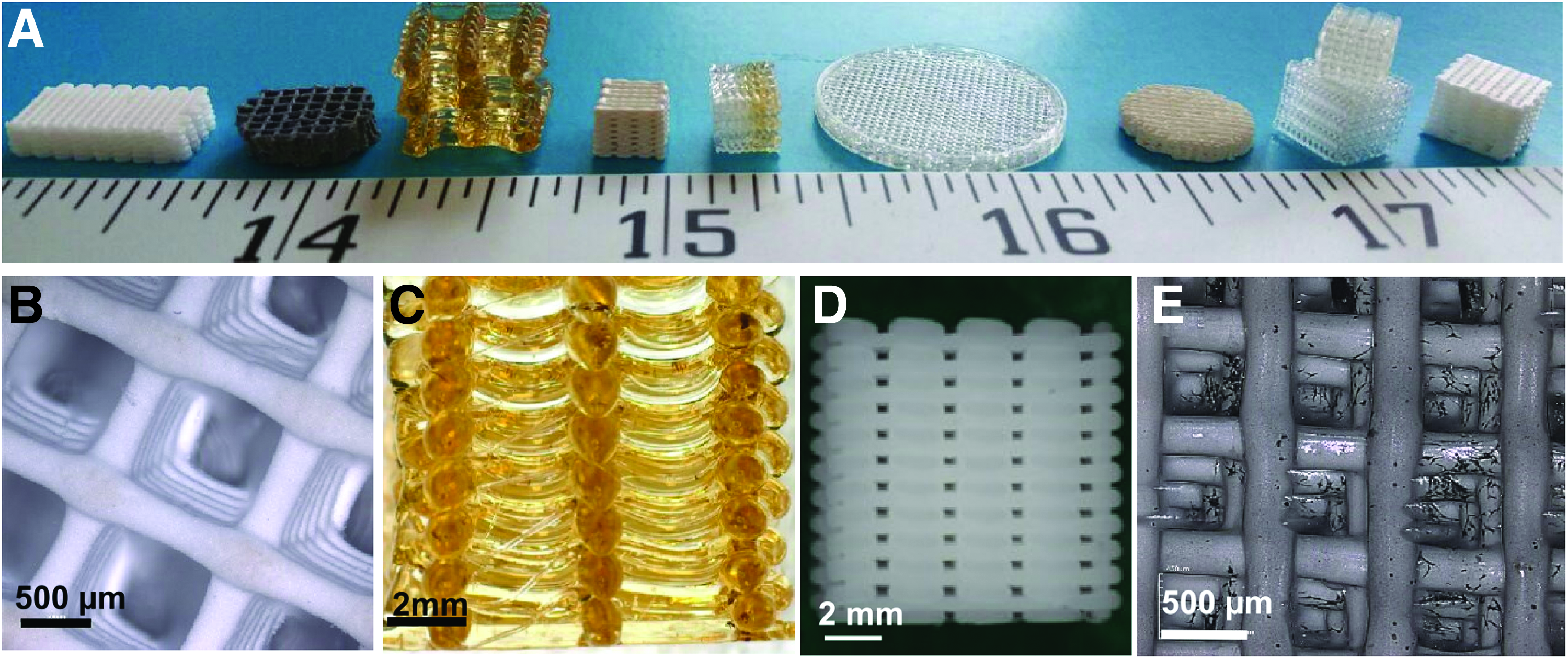
Because 3D printing allows control of the shape, size, and distribution of interconnected pores, it has found many applications in the construction of bone tissue substitutes. The most widely used materials for 3D printing of bone are bioactive glasses,54–56 HA,57–59 brushite,60,61 monetite,62,63 β-tricalcium phosphate (β-TCP),64–66 tetracalcium phosphate,67,68 biphasic calcium phosphate (BCP),69,70 and PCL71,72 (Fig. 1). Furthermore, the lack of osteoinductivity of synthetic bone grafts are compensated by possible entrapment of growth factors and osteogenic drugs in 3D printed scaffolds. Controlled sustained and localized delivery of these additives improves tissue ingrowth and bone formation. 73
Challenges in 3D Printing of Bone Substitutes
3D printing has created opportunities for the development of functional bone substitutes; however, it still faces challenges. The major challenges in 3D printing of bone substitutes include mechanical strength, shape complexity, porosity, and vascularization.74–76 Although the solutions proposed for these challenges have optimized printing parameters and led to emergence of advanced powders and binders, development of 3D printing materials and methods is still ongoing.
In recent years, many studies have been conducted to find effective solutions to the aforementioned challenges, and the number of these studies is progressively increasing. These studies are summarized hereunder.
Mechanical strength
3D printed constructs with inadequate strength are usable only in nonload-bearing defects. Chemical composition, structural design, processing conditions, and postprocessing changes are the main factors that determine mechanical properties of the final constructs.
Many efforts have been made to improve the strength of 3D printed bone scaffolds by modifying the chemical/structural composition and optimizing processing and postprocessing conditions. Thermally induced densification, 77 liquid phase sintering,78,79 microwave sintering,80,81 monomer/polymer infiltration,82,83 and doping84–87 are the main solutions offered to improve the mechanical properties of bone substitutes.
In 2014, Feng et al. studied the effects of zinc oxide (ZnO) doping on mechanical properties of β-TCP scaffolds fabricated by SLS. Results indicated that adding 2.5 wt% ZnO to β-TCP powder increases hardness, stiffness, compressive strength, and fracture toughness of β-TCP scaffolds. 88 Another study conducted by Castilho et al. was to develop a ceramic–polymer composite suitable for 3D printing of tricalcium phosphate (TCP) bone scaffolds with improved mechanical and biological properties. Results showed that direct mixing of TCP and 2.5% alginate powders improves mechanical properties, cytocompatibility, and proliferation rate. The authors concluded that homogeneously distributed polymers in ceramic matrices could be promising for fabrication of bone substitutes. 89
Table 1 summarizes some of the recent studies performed to enhance the mechanical properties of 3D printed bone substitutes.
Solutions to Enhance Mechanical Properties of Three-Dimensional Printed Bone Substitutes
HA, hydroxyapatite; HDPE, high-density polyethylene; MgO, magnesium oxide; PCL, polycaprolactone; PLGA, poly(lactic-co-glycolic acid); SiO2, silicon dioxide; SrO, strontium oxide; TCP, tricalcium phosphate; ZnO, zinc oxide.
Shape complexity
Fabrication of patient-specific anatomically shaped bone substitutes is challenging because of the large anatomical variation of patients and variable defect size and shape. 3D printing is a promising method to realize this goal, because it has the potential to be combined with medical imaging techniques and acquire the anatomical data required to fabricate personalized bone substitutes. Furthermore, it offers high control over micro- and macroarchitecture of the constructs and allows for creating complex-shaped structures.90,91
Generally, layer-by-layer fabrication of complex-shaped constructs is limited because of excessive increase of construct's horizontal cross-section that causes deviation from the desired shape. In industrial production methods, this problem is resolved using structural/sacrificial layer processes in which the sacrificial layers provide mechanical support for structural layers. 92 However, because of the lack of biocompatibility of the materials used in these procedures, this solution is not always applicable to fabricate tissue substitutes. This problem can be overcome through indirect 3D printing (casting the powder into preprinted molds).93,94 Indirect 3D printing has made it possible to fabricate complex-shaped large-scale porous scaffolds with pore sizes up to 500 μm. However, difficult demolding limits the variety of shapes manufacturable by this method, and incomplete porogen packing reduces the uniformity of the microstructure.95,96
In 2014, Castilho et al. 97 used BCPs with different HA-to-TCP ratios and performed their setting through a hydraulic reaction to obtain scaffolds with precisely controlled shapes. The dimensional accuracy of scaffolds was >96.5% with the minimum size of macropores ∼300 μm. Although the resultant scaffolds lacked sufficient strength to bear loads, they could be used as individual nonload-bearing bone implants because of their excellent shape fidelity.
Optimization of pore parameters
Tissue responses and mechanical properties should be balanced in accordance with the intended use for bone substitutes. One approach to achieve this is controlling pore parameters. Minimum pore size required for infiltration and migration of bone cells is 100–150 μm. Larger pores (>300 μm) enhance new bone formation and vascularization 98 but decrease constructs' strength. 99 Pore parameters including volume, distribution, and geometry affect tissue responses, strength, and degradation kinetics of the 3D printed constructs.100,101
In 2016, Roohani-Esfahani et al. designed a novel triphasic bioactive glass ceramic consisted of a glass phase, strontium-doped hardystonite (Sr-Ca2ZnSi2O7) and submicron crystals of gahnite (ZnAl2O4) to fabricate 3D hexagonal interconnected porous scaffolds with large pores required for bone ingrowth and effective solute diffusion. Compressive strength of the resultant scaffolds was in the range of cortical bones, implying their possible application in load-bearing bone defects. 102 In another study, Sears et al. used high internal phase emulsions of propylene fumarate dimethacrylate shelled with PCL or PLA to fabricate high-strength 3D porous bone scaffolds. The printed constructs possess hierarchical macropores (250 μm) and micropores (5–30 μm) with compressive strength similar to trabecular bones. The authors concluded that this dual modality printing could be considered as a promising approach for developing complex tissue scaffolds. 103
Table 2 provides recent studies aimed at optimization of pore parameters.
Findings from Some Studies Addressed Pore Parameters of Three-Dimensional Printed Bone Constructs
PBT, polybutylene terephthalate; PVA, polyvinylalcohol.
Vascularization
It has been well proven that a rich blood supply is required to meet nutritional needs of bone cells and removal of their waste products. Therefore, successful function of engineered bone substitutes in clinical conditions is dependent on the formation of hierarchical vascular networks throughout the construct. Furthermore, vascularization is a determining factor in integration of bone substitutes within defects.110,111
Many studies have focused on improving vascularization in bone substitutes (Table 3). Growth factor delivery, coculturing, mechanical stimulation, utilization of angiogenic biomaterials and microfabrication of biomimetic constructs are the most used strategies to regeneration of vascularized bone tissues. 112
Solutions to Induce Vascularization in Three-Dimensional Printed Bone Scaffolds
ADMSC, adipose-derived mesenchymal stem cell; ASC, adipose-derived stem cell; GelMA, gelatin methacryloyl; HUVEC, human umbilical vein endothelial cell; PEG-Da, polyethylene glycol diacrylate; PLA, polylactic acid; TGF-β1, transforming growth factor-β1; VEGF, vascular endothelial growth factor.
In 2016, Cui et al. suggested an innovative dual 3D printing method consisting of SLA and FDM to fabricate bone substitutes with improved osteogenic and angiogenic properties. The printed constructs were composed of PLA fibers arranged in a Haversian-like structure, with human umbilical vein endothelial cells (HUVEC)-laden gelatin methacrylate (GelMA) hydrogels penetrated into the hollow spaces. Furthermore, vascular endothelial growth factor (VEGF) and bone morphogenetic protein 2 were regionally immobilized in constructs to promote angiogenesis and osteogenesis, respectively. Results revealed efficient vascularized bone regeneration of the dual printed constructs. The authors concluded that the proposed method could be utilized in clinical translation. 120
In another study, Fahimipour et al. designed a TCP-based scaffold containing VEGF-loaded PLGA microspheres to induce osteogenesis and angiogenesis simultaneously. They used gelatin and alginate as hardening and thickening agents, respectively, and optimized the formulation of the ink to be printable at room temperature. Results showed that the proliferation rate of seeded HUVECs doubled because of controlled release of VEGF. Furthermore, mechanical properties of the scaffolds were similar to cancellous bone. The authors proposed the fabricated 3D printed porous scaffolds for bone regeneration in critical craniofacial defects. 121
3D Bioprinting of Bone Substitutes and Its Challenges
3D bioprinting is an emerging tissue engineering approach that allows for direct printing of cell-laden constructs. The bioink, which is a collection of biomaterials, biological molecules, and living cells, is printed based on the computer-aided designed model of the tissue.122,123 Compared with the conventional tissue engineering methods, 3D bioprinting provides more control on cell distribution within the construct. Furthermore, it makes it possible to fabricate tissue blocks and organoids, thus facilitating the construction of tissue and organ substitutes. The main drawbacks of 3D bioprinting include the limited choice of bioinks and the possibility to reduce the cell viability during the printing process.124,125
Among the different modalities, inkjet, microextrusion, and laser-assisted bioprinting are the most commonly used 3D bioprinting methods. 122 Several efforts have been made to fabricate blood vessels,126–129 neuronal tissues,130,131 liver,132–134 skin,40,135,136 cartilages,137–140 and bones117,141–145 through bioprinting.
The main challenge of bioprinting is the design of the appropriate bioink. In 3D bioprinting of bone substitutes, the bioink must meet a number of required properties including biocompatibility, biomimicry, biodegradability, bioprintability, and mechanical integrity.125,146 Many efforts have been made to find a bioink with an optimal balance of properties to overcome the limitations of the bioprinted constructs.
One major limitation of the bioprinted bone substitutes is their inadequate mechanical properties. In 2015, Gao et al. designed a bioink with adequate mechanical properties to create bone and cartilage substitutes. The bioink was composed of human mesenchymal stem cells (hMSCs) loaded in poly(ethylene glycol) dimethacrylate (PEG-DMA)–GelMA hydrogel. During the inkjet bioprinting process, PEG and GelMA were photo-crosslinked to enhance the mechanical properties of the constructs. Results obtained 21 days after printing showed the improvement of elastic modulus of hMSC-PEG-GelMA constructs by 100% compared with the cell-laden PEG or GelMA constructs. The findings of the study demonstrated that photo-crosslinkable multimaterial hydrogels are promising bioinks to create bone and cartilage substitutes. 141
In another study conducted by Daly et al. in 2016, cartilaginous templates were created by printing bone marrow-derived MSCs into the Arg-Gly-Asp-modified alginate hydrogels. To improve the mechanical properties of the constructs, the MSC-laden bioink was co-deposited with PCL fibers. Results showed 350-fold increase in compressive modulus of bioink/PCL templates. The constructs had the potential to be implanted as vertebral bodies in load-bearing locations. 142
In 2017, Bendtsen et al. formulated a novel hydrogel with optimal printability and biocompatibility to fabricate bone substitutes. The bioink composed of alginate, polyvinyl alcohol (PVA), and HA showed excellent rheological properties and high shape fidelity. Furthermore, its osteoconductivity made it a favorable environment for new bone formation. The mouse calvaria 3T3-E1 (MC3T3) cells encapsulated into the alginate-PVA-HA hydrogels had viability of 95.6%. The authors concluded that the proposed formula is a promising solution for repairing bone defects. 143
Similar to 3D printed bone substitutes, bioprinted constructs also suffer from poor vascularization that could result in the failure of the constructs after implantation. This limits the application of bioprinting constructs, especially in large bone defects. To provide functional vasculature in large bone defects, Byambaa et al. developed a novel hydrogel that allows for coculturing of bone marrow-derived hMSCs and HUVECs. The GelMA hydrogel conjugated by VEGF and loaded with silicate nanoplatelets promoted simultaneous angiogenesis and osteogenesis. Three weeks after in vitro culture, the constructs demonstrated high cell viability, high proliferation rate, and excellent structural stability. The results also indicated the formation of a mature bone niche after 21 days of culture. 117
Recently, Anada et al. fabricated a highly vascularized biomimetic hydrogel suitable for bone tissue engineering applications. The dual ring bone-mimetic construct composed of a GelMA/octacalcium phosphate external ring and a central ring of GelMA loaded with HUVECs. The HUVEC spheroids promoted angiogenesis by forming capillary networks within the construct and the octacalcium-containing ring-stimulated bone formation. 145
Future Directions
In the near future, demands for bone substitutes will increase, especially in aging populations.147,148 3D printing and bioprinting have the potential to fabricate complex-shaped patient-specific bone substitutes.
In the coming years, hardware and software advancements will allow for fabricating constructs with intricate hierarchical structural details close to that of natural bones. Moreover, multimaterial (bio)inks and multihead (bio)printing machines will make it possible to create constructs with chemical composition similar to bones. Besides, prevascularized bone substitutes will facilitate host vascular ingrowth. Therefore, soon after implanting the construct, its capillary network will undergo anastomosis with host tissue's microvasculature. This will dramatically reduce the failure rate of 3D (bio)printed bone substitutes because of the occurrence of hypoxia, apoptosis, or immediate cell death at the implantation site. In addition, advanced (bio)inks with optimal printability and biocompatibility along with optimized fabrication processes will enable us to create bone substitutes with adequate mechanical properties and stability to withstand physiological stresses at load-bearing sites.149–151
3D printing and bioprinting are yet facing challenges in fabricating functional bone substitutes. Once the existing challenges have been resolved, the fabrication processes could be scaled-up and mass production of patient-specific functional bone substitutes will be feasible.
Conclusion
Despite its promising achievements during the last two decades, 3D printing of bone substitutes is still challenging. Mechanical properties, shape complexity, optimization of pore parameters, and vascularization are the main challenges in 3D printing of bone substitutes. Many efforts have been made to resolve these challenges by optimizing materials and methods for 3D printing of bone substitutes.
Studies have demonstrated that thermally induced densification, liquid-phase sintering, microwave sintering, monomer/polymer infiltration, and doping can improve mechanical properties of bone substitutes. On the contrary, pore volume, distribution, and geometry should still be optimized to improve tissue responses, strength, and degradation kinetics of 3D printed constructs. Considering the importance of angiogenesis and its undeniable role in the formation of functional bone substitutes and their integration with the surrounding tissues, many studies have been performed to induce vascularization in 3D printed bone grafts through growth factors delivery, coculturing, mechanical stimulation, utilization of angiogenic biomaterials, and microfabrication of biomimetic constructs.
In 3D bioprinting, the main challenge is to design a bioink with optimal balance of biocompatibility, biomimicry, biodegradability, bioprintability, and mechanical integrity. Besides, vascularization of bioprinted constructs is still challenging. Innovations are still needed to translate 3D (bio)printed bone substitutes from the laboratory to the clinic.
Ethical Approval
This article does not contain any studies with human participants or animals performed by any of the authors.
Funding Information
No funding was received for this article.
Disclosure Statement
No competing financial interests exist.