
Abstract
Glaucoma is a major eye disease characterized by a progressive loss of retinal ganglion cells (RGCs). Biomechanical forces as a result of hydrostatic pressure and strain play a role in this disease. Decreasing intraocular pressure is the only available therapy so far, but is not always effective and does not prevent blindness in many cases. There is a need for drugs that protect RGCs from dying in glaucoma; to develop these, we need valid glaucoma and drug screening models. Since in vivo models are unsuitable for screening purposes, we focus on in vitro and ex vivo models in this review. Many groups have studied pressure and strain model systems to mimic glaucoma, to investigate the molecular and cellular events leading to mechanically induced RGC death. Therefore, the focus of this review is on the different mechanical model systems used to mimic the biomechanical forces in glaucoma. Most models use either cell or tissue strain, or fluid- or gas-controlled hydrostatic pressure application and apply it to the relevant cell types such as trabecular meshwork cells, optic nerve head astrocytes, and RGCs, but also to entire eyes. New model systems are warranted to study concepts and test experimental compounds for the development of new drugs to protect vision in glaucoma patients.
Impact Statement
The outcome of currently developed models to investigate mechanically induced retinal ganglion cell death by applying different mechanical strains varies widely. This suggests that a robust glaucoma model has not been developed yet. However, a comprehensive overview of current developments is not available. In this review, we have therefore assessed what has been done before and summarized the available knowledge in the field, which can be used to develop improved models for glaucoma research.
Introduction
Glaucoma is a major eye disease in which patients progressively lose parts of their visual field, which severely affects their quality of life. 1 This visual field loss is a result of retinal ganglion cell (RGC) death2,3 (indicated as red cells in Fig. 1). RGCs transport visual information from the outside world to the brain. They do so by connecting the photoreceptors to the visual cortex with their axons extending from the eye, through the optic nerve, to the brain.
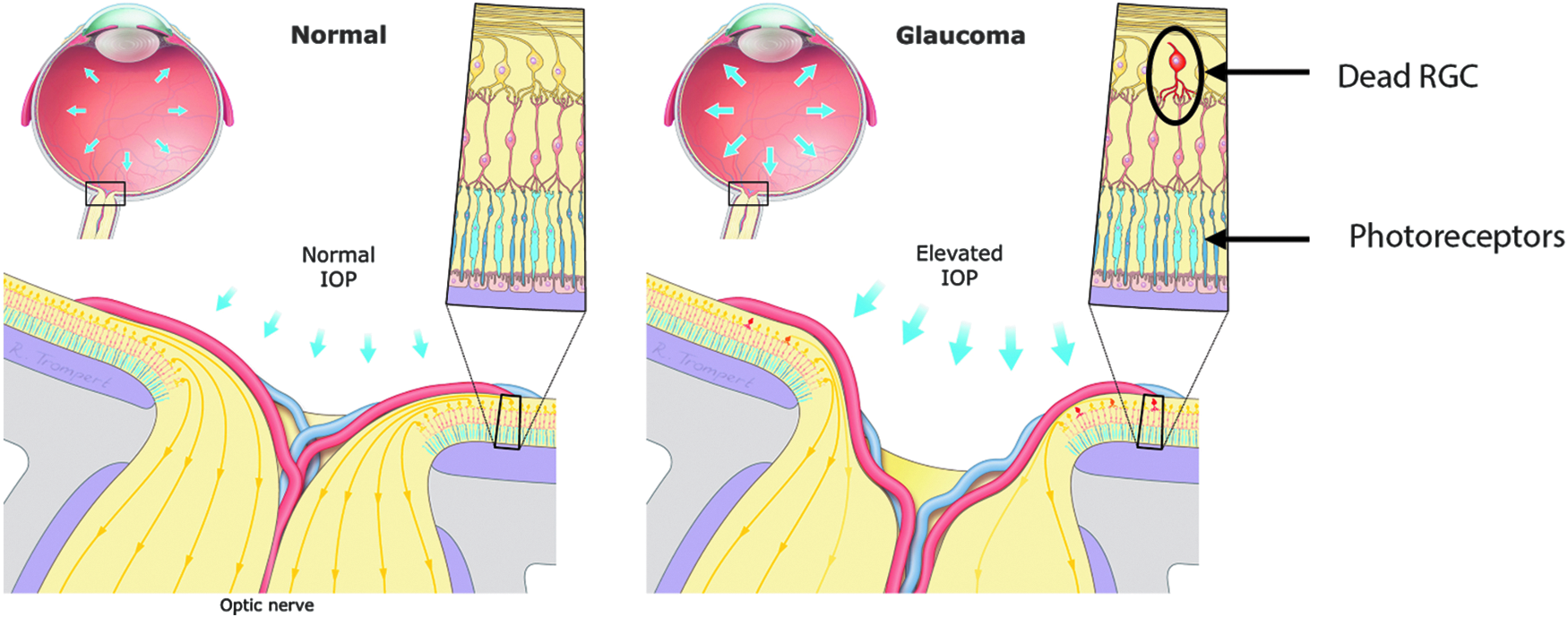
Close-up of the human optic nerve head under normal circumstances and glaucoma. RGCs die as a result of elevated hydrostatic pressure, causing degeneration of the axons and thereby the optic nerve. This is manifested as an excavation of the anterior part of the optic nerve (shown in the right panel). IOP, intraocular pressure; RGCs, retinal ganglion cells. Color images are available online.
RGCs die in the course of glaucoma and their death marks the irreversible step in the disease process because lost RGCs are not replaced. Currently, there is no approved medication that protects this important retinal neuron.4,5 Elevated intraocular pressure (IOP) is a major risk factor for glaucoma, 6 and is the only parameter that can be manipulated during glaucoma treatment. 6 Reduction of IOP is in most patients beneficial; however, the mechanisms by which elevated IOP translates into mechanical forces that damage RGCs are unknown. Current (IOP lowering) treatments cannot cure glaucoma, but they can delay its progression and thus prevent blindness toward the end of life.7,8 Lowering IOP does not stop disease progression in all patients, and on the other hand, some patients with glaucoma do not have an elevated IOP, which is referred to as normal pressure glaucoma. To protect RGCs from dying, beyond the therapeutic effect of lowering IOP, there is a need for new classes of drugs. It should be realized that preventing RGC death does not cure the disease, but protecting RGCs in combination with early diagnosis can prevent glaucoma blindness. To accelerate the development of new drugs, physiological in vitro models are needed. These models can also be used to increase the understanding of RGC loss in glaucoma, clarify the relationship between high IOP and RGC loss, and identify potential targets.
As stated by the American Academy of Ophthalmology, there are two main theories to explain the development of glaucoma, the vascular and the mechanical theory.9,10 The vascular theory suggests that glaucoma is caused by decreased optic nerve perfusion, which causes neural ischemia. The mechanical theory, on the other hand, advocates that RGCs die as a result of direct deformation of the axons, cells, and support structures.
The pathways involved in RGC degeneration are currently investigated and there is increasing evidence for the theory that mechanical strain leads to cellular responses, which ultimately lead to RGC death and axonal degeneration.11,12 Dual leucine zipper kinase and leucine zipper kinase have been implicated in the signaling pathways leading to RGC death, 13 and are therefore considered potential drug targets to prevent RGC death. On the other hand, RGC axon degeneration can be delayed by targeting sterile alpha and TIR motif containing 1 (SARM1).11,14
Unfortunately, many molecular details of the pathway (Fig. 2) are still unknown, so investigating the molecular mechanism behind RGC death represents a valuable area of interest to explore a possible treatment for this severely disabling disease. As glaucoma is the leading cause of irreversible blindness worldwide 15 and current treatments for this disease are not sufficient, it is urgent that new drugs are developed. A valid physiological in vitro model is needed to achieve this goal; therefore, we reviewed the literature on models used to mimic the biomechanical forces that are at play in glaucoma.

Proposed pathways of somal and axonal RGC degeneration after injury by biomechanical strain, defects in axonal transport, disruption of cytoskeleton, and inhibition of trophic signaling, resulting in the activation of DLK signaling. This pathway is suggested to promote synaptic decline and neuronal death. Adapted from Asghari et al. 12 and Fernandes et al. 11 DLK, dual leucine zipper kinase. Color images are available online.
Biomechanical Strain in Glaucoma
Several biomechanical forces occur inside the eye. Increased IOP will lead to an overall increase in hydrostatic pressure on all tissues within the eye. Pressure builds up because of an imbalance in aqueous humor production and outflow 6 (the production and normal outflow pattern of aqueous humor are depicted in Fig. 3). This pressure transmits throughout the entire eye because of the rigidity of the sclera.
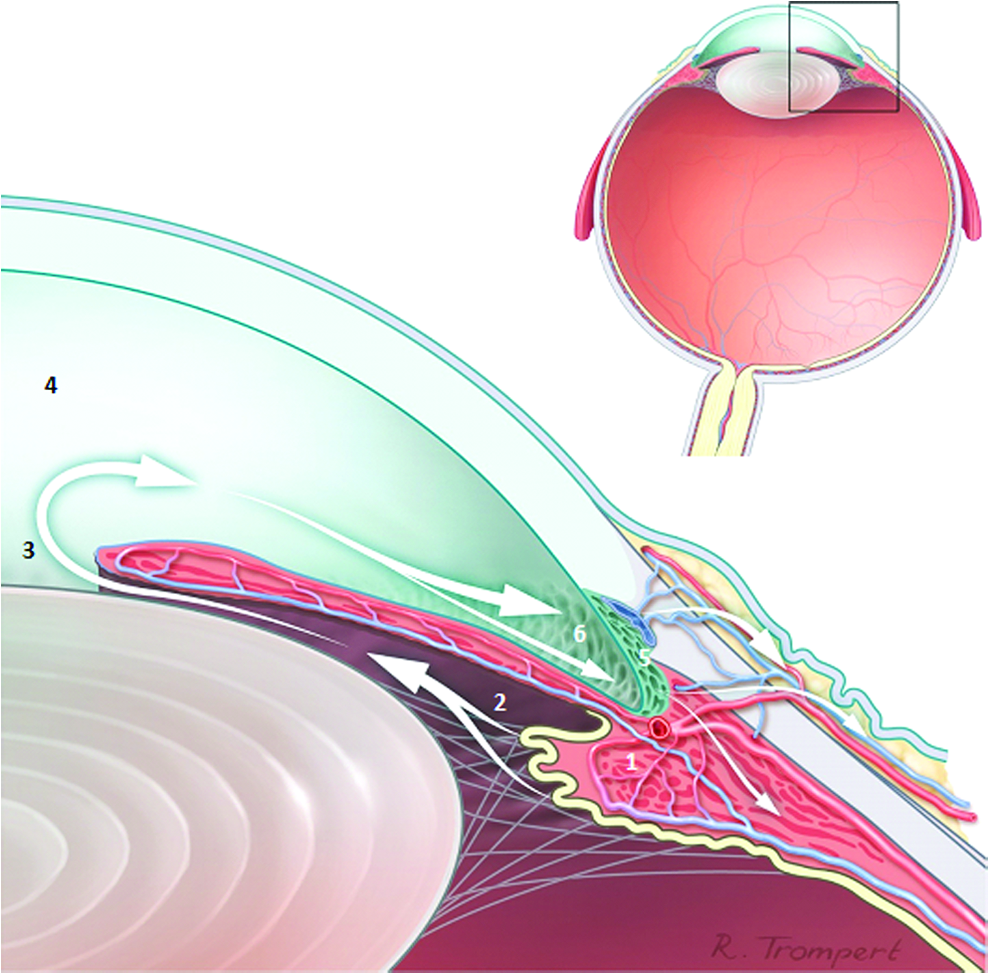
Magnification of the anterior segment showing a schematic drawing of the aqueous humor production and outflow pattern. Aqueous humor is produced by the ciliary body (1) and flows from the posterior chamber (2), through the iris (3), and to the anterior chamber (4). It is then (mostly) drained in the trabecular meshwork (5), located in the anterior chamber angle (6). Box shows area of magnification. Color images are available online.
Even though all retinal cells experience the pressure, RGCs seem to be the most vulnerable. 16 IOP will push soft tissue outwards (e.g., the unmyelinated axons of the optic nerve head) and compress these structures when they encounter resistance of deeper and stiffer layers such as the lamina cribrosa. The optic nerve head is where the axons of RGCs leave the eye and most blood vessels enter and exit, and is considered the weak spot of the eye since it is a major passage through the sclera. The lamina cribrosa is the connective tissue mesh that separates the eye from the orbit and brain, and permits the axons to pass, and is thought to deform most in glaucoma.17,18 Since most deformation in glaucoma takes place in the lamina cribrosa, and RGC axons pass through this structure, they experience strain in this region. Jiang et al. 19 showed in vivo evidence of this strain by optic nerve head measurements. They found a statistically significant association between widening and deepening of the optic cup as well as condensation of the prelaminar tissue, that is, excavation of the optic nerve head (Fig. 1), for an IOP increase >15 mmHg.6,19
Lamina cribrosa deformation has been studied in vivo using optical coherence tomography, 3 demonstrating up to 9% strain, which will be transmitted to the RGC axons. 20 Any movement or deformation will strain RGC structures, in particular the unmyelinated RGC axons in the optic nerve head area. Finally, it must be realized that eye pressure is not constant, but fluctuates along with many factors (e.g., body position, eye movement, Valsalva maneuvers [increase internal pressure and decrease venous return], wind instrument playing, and circadian rhythm). Therefore, all the described biomechanical forces are dynamic.
Lowering IOP delays disease progression, but elevated IOP (ocular hypertension) does not always lead to glaucoma. 21 On the other hand, glaucomatous visual field defects can occur in conditions of normal IOP (normal tension glaucoma) 22 Biomechanical strains play a major role in the pathophysiology of glaucoma and variation in tissue stiffness (patient-specific biomechanical properties) could offer an explanation for the difference between ocular hypertension and normal tension glaucoma, and therefore play a role in the susceptibility of glaucoma. It is likely that IOP fluctuations cause the major part of biomechanical strain, as these are also strongly associated with glaucoma progression.20,23 A rigid sclera seems to provide a biomechanical advantage, while a rigid lamina cribrosa is associated with a biomechanical disadvantage.20,23
The susceptibility for glaucoma in myopic patients could be due to lower rigidity of the sclera,24,25 as stated by Girard et al., 23 probably due to the biomechanical disadvantage of larger globe diameter and thinner sclera. Biological variations in sclera and lamina cribrosa rigidity probably contribute to the wide variety of damage seen in glaucoma patients and may explain why some people with elevated IOP have no glaucomatous defect or damage, but biological variation (in, for example, mitochondria 26 ) should be taken into account as well. Therapies that interfere with the biomechanical properties of these structures could therefore be a possible novel target and are currently under investigation, for example, through increasing the level of collagen crosslinking to increase scleral stiffness.27,28
Need for Experimental Glaucoma Models
There is a need for model systems to study concepts and test experimental compounds. Clinical studies have provided valuable information, such as the effect of Rho kinase inhibitors as neuroprotective agents, 29 but the development of treatments cannot be performed in vivo, as cell or tissue samples are not readily available, as well as the tremendous time consumption and cost involved in clinical studies. Samples of the retina cannot be obtained from healthy volunteers or patients, and the process to obtain viable cells or tissues from deceased patients often takes too long. Animal models are available, but many lack the specific anatomical features relevant for glaucoma. Mice, for example, lack a lamina cribrosa and genetic factors of glaucoma cannot all be mimicked in animal models. More than 100 mutations and genetic polymorphisms have been identified to be involved in glaucoma, but they are too multifactorial to study their complex interplay in genetic animal models.
Disease models are crucial for biomedical discoveries, from understanding pathophysiology to developing vaccines and new drugs. 30 To develop new treatments for a disease, it is often required to study the molecular and cell biological aspects of the disease. This knowledge can then be used to identify specific targets and we believe that the eye is an ideal organ for research. Compared to other organs, it is small and easily accessible. The different tissues of the eye can be accessed using noninvasive or minimally invasive techniques. 31 Furthermore, the eye is a relatively immune-isolated organ due to the blood-retina barrier and its immunosuppressive microenvironment, resulting in better opportunities for tissue/cell transplants and stem cell therapy. 32
Current in vitro models to study glaucoma have their limitations. Several glaucoma models have been developed by adding substances or depriving growth factors, applying mechanical strain to cells, tissues, or the entire organ, or mimicking disease development in vivo, but the outcomes of these studies vary widely, suggesting that this does not represent a robust glaucoma model. To develop suitable models, we first need to assess what was done before and gather the knowledge that is available. The goal is to develop new classes of drugs to protect RGCs from dying in glaucoma; for this, we need a drug screening model. Since in vivo models are unsuitable for screening purposes, we focus on in vitro and ex vivo models in this review.
Literature Search Strategy
A PubMed search was conducted to identify in vitro and ex vivo glaucoma models published in the English language. The search was updated until February 7, 2019. Two separate searches were conducted to identify the published studies with hydrostatic pressure, and with stretch or strain.
(hydrostatic pressure) AND ((glaucoma) OR (glaucoma[MeSH Terms])) AND ((in vitro) OR (in vitro[MeSH Terms]) OR (ex vivo))
((stretch) OR (strain)) AND ((glaucoma) OR (glaucoma[MeSH Terms])) AND ((in vitro) OR (in vitro[MeSH Terms]) OR (ex vivo))
Abstracts were reviewed for relevance, where 2 of the 31 hydrostatic pressure articles dropped out because of the lack of a biomechanical model or published language. Thirteen of the 36 strain articles dropped out because of lack of a mechanical model (mouse strain, bacterial strain, etc.) A total of 52 articles were used to assess the different biomechanical models used to study glaucoma. The reference lists of the 52 articles were screened to find 3 additional publications, resulting in a total of 55 reviewed articles. See Table 1 and Table 2 for the list of articles used in this review with corresponding characteristics; Figure 4 shows a flowchart of the selection of studies.
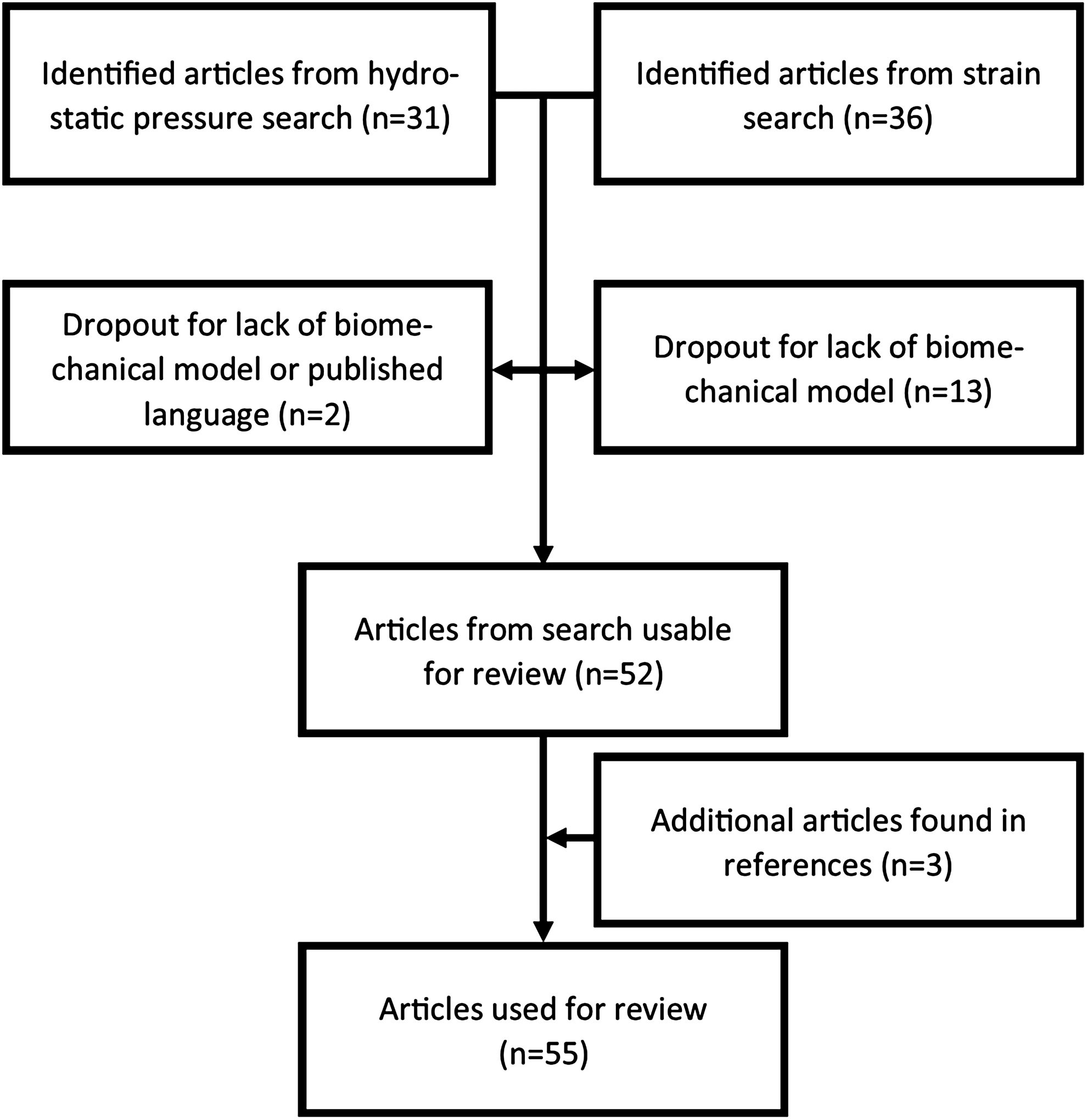
Flowchart of the article selection used for the review.
Characteristics of Articles Used Regarding Hydrostatic Pressure Application
ADAMTS, a disintegrin and metalloproteinase with Ttrombospondin motifs family; DITNC1, immortalized rat neocortical astrocyte-derived cell line; DRP1, dynamic-related protein; GSK3β, glycongen synthase kinase 3 beta; LC, lamina cribrosa; LPS, lipopolysaccaride; MMP-2, matrix metalloproteinase-2; MYOC, myocilin; NOS-2, nitric oxide synthase-2; OAG, open angle glaucoma; PC12, rat pheochromocytoma-derived cell line-12; PEDF, pigment epithelium derived factor; RT-qPCR, real time quantitative polymerase chain reaction; SAC, stretch activated channel; TRPV1, transient receptor potential vanilloid channel 1; TUNEL, terminal deoxynucleotidyl transferase dUTP nick end labeling.
Characteristics of Articles Used Regarding Strain Application
Cellular Models
In glaucoma, many tissues experience biomechanical forces, which lead to effects as subtle as slight alterations of signal transduction pathways or as harsh as cell death or tissue function loss. 33 Molecular or cell biological models can investigate small changes at a cellular level, but can also investigate cell death. Effects at tissue level can, however, not be studied using these models, but this is where tissue, explant or animal models come in.
Biomechanical forces mimicking glaucoma have been modeled in different ways, but the main principles come down to fluid- or gas-controlled hydrostatic pressure application, and mechanical membrane stretching (leading to strain). For the cell-biological model systems, several conditions were used depending on the cell type and the study aim.
Elevated IOP is the main risk factor for glaucoma, which acts on the tissues as hydrostatic pressure. This pressure spreads throughout the tissues of the eye and is present as a more general biomechanical force instead of a localized force. This pressure is more straightforward to mimic than strain and the global pressure that is present due to elevated IOP has been attempted using two main techniques: gas-controlled pressure chambers and fluid pressure systems. Gas-controlled pressure chambers consist of a pressure vessel that can contain cultured cells, which can be placed in an incubator, and a gas regulator that applies and controls the pressure using a humidified 5% carbon dioxide (CO2) and 95% air mixture (an example of such a gas-controlled pressure system is depicted in Fig. 5).
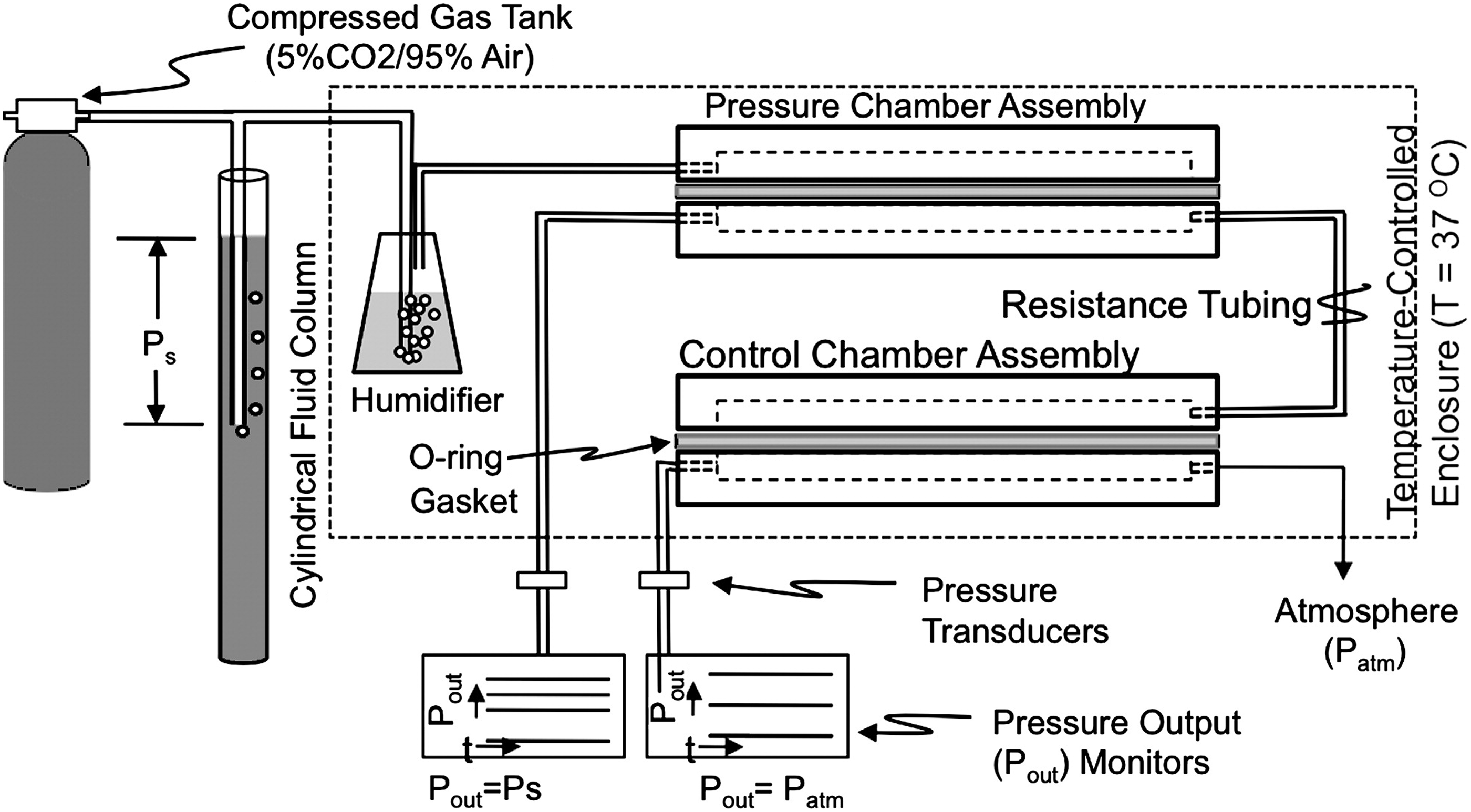
Experimental setup of a gas-controlled hydrostatic pressure model. A humidified gas mixture is fed to a pressure chamber in which cells are located. Adapted from Shin et al. 40 CO2, carbon dioxide.
It is possible to investigate different types of glaucoma by applying different pressures. Sixty to 75 mmHg was used most frequently, which resembles the clinical pressures measured in acute angle closure glaucoma patients. Pressures of 25–35 mmHg can be used to mimic clinical pressures of primary open-angle glaucoma, where 0–20 mmHg resembles the normal IOP.
Across the different studies, a hydrostatic pressure of 15 mmHg34,35 to 100 mmHg 34 was applied for as short as 30 min 36 or 2 h 34 to up to 72 h,37–40 or even 7 days 41 (Table 1 summarizes force application, cell type, and outcome per study).
The different methods of applying hydrostatic pressure show us that different groups think differently about the application of hydrostatic pressure. Some use gas-induced pressure, while others use a fluid column to induce hydrostatic pressure. However, gas pressure changes influence CO2 exchange between medium and gas, which has to be taken into account in the experimental setup. In some cases, a gas mixture of 8% CO2 and 92% air36,39,41–45 was used. This mixture was chosen to counteract the pH effect of a pressurized gas over a liquid, since the solubility of gases changes under pressure. However, we propose that it is better to mimic hydrostatic pressure by using a fluid column as described in the article of Sohn et al. 46 In this study, trabecular meshwork cells were cultured under direct hydrostatic pressure to investigate gene expression changes. The pressure was applied using a fluid column, where the height of the fluid column determines the pressure according to Pascal's law [ΔP = ρg(Δh)]. A similar technique was used in the organoid model of Ishikawa et al., 47 shown in Figure 6. Other groups have used similar systems as well to study different pressures and cell types.48–50
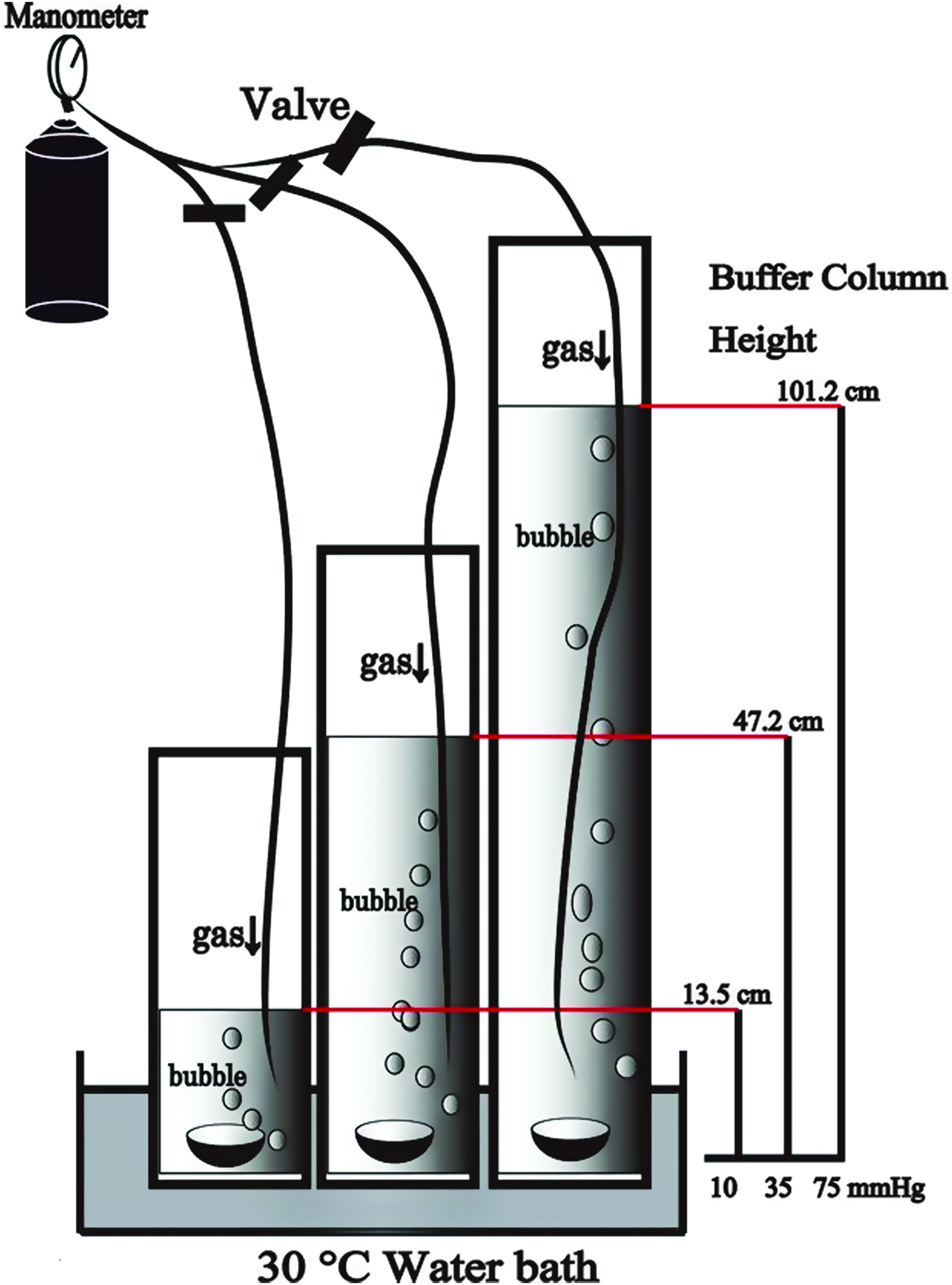
Experimental setup of a fluid column-induced hydrostatic pressure model. Ex vivo eye cups are placed at the bottom of cylinders filled with medium. Different hydrostatic pressures are applied by varying the height of the fluid column. Adapted from Ishikawa et al. 47 Color images are available online.
These studies have taught us many things, like astrocyte migration is only affected under hydrostatic pressure combined with hypoxia, 49 hydrostatic pressure causes messenger RNA expression changes in, for example, lamina cribrosa cells, 41 and hydrostatic pressure causes RGC death.34,38 However, we can also learn from other fields, such as the bone, tendon, and muscle field, which have a lot more experience with biomechanical strain since it is widely known that these tissues experience various strain forces. Tendon proliferation is, for example, induced by mechanical strain 51 and the discovered pathways in these studies can be translated to the field of ophthalmology and increase the knowledge.
Biomechanical strain in the form of cell/tissue stretch can be considered a model for glaucoma in the optic nerve head region, as this structure moves up and down with fluctuations in eye pressure. This causes uniaxial movements in the structures of the optic nerve head such as lamina cribrosa, RGC axons, and astrocytes. In vivo measurements have shown ∼9% strain in this region. 20
Other parts of the RGCs could experience other types of strain, for example, isotropic or anisotropic strains. The commercially available Flexcell® device (FX-2000™ to FX-6000™; Flexcell International Corporation, Hillsborough, NC) is able to induce strain in vitro. It uses vacuum pressure and positive air pressure to deform a flexible-bottomed culture plate (shown in Fig. 7), leading up to 33% strain. The strains can be carefully defined and controls static or cyclic strain to cells growing in six-well plates. Flexcell plates can induce an equibiaxial (isotropic strain; equal in all directions) or uniaxial strain to cells cultured in a monolayer on an elastic membrane. The membranes can be coated to provide the appropriate surface for specific cells (e.g., type I collagen, fibronectin, and laminin).
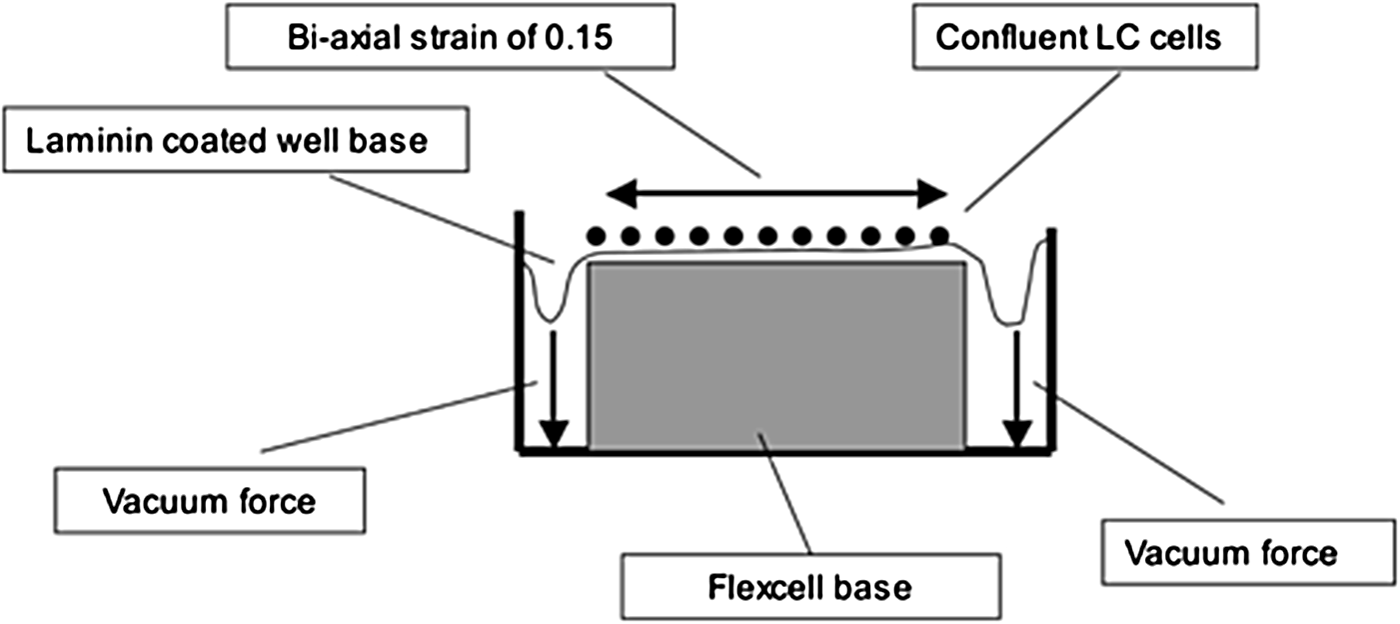
Schematic representation of the Flexcell device. A single well of the six-well plate is shown. A negative pressure draws a coated elastic membrane with cells downwards, inducing a biaxial strain on top of the well base. Adapted from Kirwan et al. 63 LC, lamina cribrosa.
Besides this model, some studies developed a similar custom-made device.52–54 Instead of pulling a membrane down over a pillar, threaded cylinders can be used to pull an elastic membrane over a circular culture unit, thereby generating equibiaxial strain.52,55 A membrane can be deflected into a spherical cap by a uniform hydrostatic pressure that is applied below the substrate, resulting in biaxial tension and biaxial strain in the cells cultured on top of the membrane.53,56 Another strain device was made by placing a glass bead under a membrane, producing a defined upward bowing of the membrane and strain of 10%.54,57
Strain forces of 3% 58 to 20%52,58,59 were applied in a cyclical33,53,58,60–64 or static52,54,59 manner for a duration of 2 min 53 to up to 48 h 54 (Table 2 summarizes force application, cell type, and outcome per study). Cyclical strain is mostly applied at 1 Hz to mimic pulsatile blood flow and in some cases at 0.3 Hz to mimic short-term IOP changes.
The study of Albalawi et al. 33 is a good example of an in vitro biomechanical model. They used isolated optic nerve head astrocytes and strained them in two different ways, using a hypotonic solution to increase cell volume by promoting osmosis and using an in vitro Flexcell device. In their study, they aimed to investigate the link between inflammation and biomechanical strain. Mechanical forces or trauma can, for example, induce inflammation, which in turn has shown to damage neurons. 65 They showed that straining optic nerve head astrocytes leads to a release of adenosine triphosphate (which is indicative of damaged cells) and upregulation of inflammation-related genes. The optic nerve head is the region that is thought to experience most strain, because—as described above—it is the weak spot of the eye; in vivo studies in the living human eye under elevated IOP and cerebrospinal fluid pressure have shown this strain in the optic nerve head. 66
Molecular and cell biological models are ideal for gene expression and protein analysis, and many studies have used real time quantitative polymerase chain reaction (RT-qPCR) and immunoblots to analyze glaucoma pathways. Immunofluorescence provides valuable information on specific markers as well as basic parameters like cell counts and apoptosis. These techniques have, for example, shown the involvement of the immune system, matrix metalloproteinases, and many mechanically activated membrane channels like pannaxins and transient receptor potential vanilloid (TRPV) channels in the mechanobiological pathway of glaucoma.33,53,64,67,68 Mechanosensitive membrane channels have, for example, been studied in vitro using specific channel antagonists, and have shown to be robustly upregulated with biomechanical strain.53,67,68 While these findings are largely validated in vivo (with knockout mice, glaucoma animal models, etc.), the precise pathways are unfortunately unknown.
Explant Models
Tissue and whole eye explant models would be easier to manipulate than the in vivo models, and are closer to the in vivo situation than the molecular or cell biological models. These models have been used to study mechanobiology. Similar to the molecular and cell biological models, tissue and explant model were subjected to biomechanical strain by applying hydrostatic pressure or strain using pressurized gases or fluid columns. The study of Ishikawa et al., 47 for example, showed the effect of 24-h hydrostatic pressure on the upregulation of endogenous neuroprotective neurosteroids in ex vivo rat retinae, which may therefore serve as a potential therapeutic target. This study is a good example of pure hydrostatic pressure by using a fluid column.
However, gas exchange can be problematic in this kind of approach, because the larger tissues and explants have a higher demand for oxygen. The reduced diffusion of gases can be counteracted by infusing a CO2/air gas mixture in the medium. Using a similar setup, other studies also investigated different pressure 69 or used the fluid column to induce strain.70–72 Instead of a fluid column, some studies used pressure-controlled injection in a closed pressure chamber or directly cannulated in the whole explanted eye to achieve the desired strain with73–75 or without IOP fluctuation.76–78 Gas-controlled pressure chambers were used as well to apply hydrostatic pressure to retinal cups or explants.68,79–84 These studies again showed the involvement of the immune system, and membrane channels like TRPVs, but also showed us possible neuroprotective agents like hydrogen sulfide, 24(S)-hydroxycholesterol, or A2AR antagonists.
Mechanical Modeling in Animals and Clinical Research
Animal models try to mimic human disease in different ways. Albalawi et al., 33 for example, used an in vivo rat model where they mimicked glaucoma by inserting a needle connected to a fluid reservoir in the anterior chamber and increasing the IOP to 50–60 mmHg by raising the reservoir. With this study, they linked biomechanical strain to neuroinflammation. The study of Kim et al. 85 is also a good example of an in vivo study; the possible neuroprotective targets to rescue RGCs in mice with elevated IOP were investigated. Neuroprotective compounds were applied and the involved pathway was simulated in other ways (by overexpressing genes), to study the effects of the treatment under glaucoma conditions. With this setup, they discovered that dynamin-related protein 1 inhibition is a potential target for treating glaucomatous neurodegeneration.
The main ways of inducing glaucoma in animal models is done through elevation of IOP achieved by inserting a needle in the anterior chamber or vitreous and infusing the eye with a buffer,33,82,86 by obstructing aqueous humor outflow due to the introduction of microbeads that obstruct the trabecular meshwork,43,79,87 or by increasing IOP with secondary treatments like laser-induced retinal inflammation. 42 Undeniably, these models only replicate parts of the pathology that causes glaucoma in humans. Clinical research is unfortunately very limited and most analysis can only be performed postmortem. The postmortem time for enucleation of eyes is extremely variable among different countries and combined with the limited time window in which healthy cells can be harvested, it is difficult to obtain human cells for glaucoma research. Some tissue samples can be taken during surgery, but these are mostly in a diseased state without the availability of healthy controls. In vivo imaging, like three-dimensional strain mapping, 20 does provide new opportunities for clinical research.
Future Perspectives
Biomechanical models can be analyzed in many ways. Most studies used (immuno) histochemistry to investigate basic parameters such as cell count or morphology, but it can also be used to analyze the purity of primary cell isolations or organoid cultures before using them in biomechanical models. 88 Moreover, gene expression is analyzed using qPCR to study specific markers. Apoptosis is also one of the endpoints that are studied often, for example, with a terminal deoxynucleotidyl transferase dUTP nick end labeling assay.89,90 Functional analysis can be done as well, for example with patch-clamp 91 and intracellular calcium measurements. 67
High-throughput screening in the biomedical field is a method of scientific experimentation to screen a large number of a particular parameter (e.g., compounds, substrates, and cells) for biological effects through automated and miniaturized experimentation on a large scale. These screening tools would be of great value to facilitate the development of new drugs for protecting RGCs in glaucoma. Current models are mostly unsuitable for high-/medium-throughput analysis. Multiwell platforms could be used to identify glaucoma mimicking conditions through high-throughput analysis (e.g., high-throughput imaging) by comparing the effects of the in vitro model to the disease situation. After the identification of the best mimicking conditions, these can be multiplied in a medium-/high-throughput device for high-content analysis, such as drug or small molecule screening to find new therapeutic targets.
We think there is a need for simultaneous application of strain and hydrostatic pressure to mimic glaucoma best, since these biomechanical forces are simultaneously at play. Therefore, we are currently developing such a high-throughput biomechanical model. Sinha et al.92,93 developed a medium-throughput device to apply strain and shear stress to cells; we adapted this model to apply hydrostatic pressure with culture medium together with strain. The Flexcell device could be an alternative, but this model would have to be adapted to allow high-throughput screening.
Induced pluripotent stem cell (iPSC) technology and retinal organoids are relatively advanced, but have not been used for studying biomechanical strain. Other organoid fields suffer from the limitation that the organization of the cells does not fully resemble the in vivo architecture. Although retinal organoid are immature tissues, they have the correct alignment and layered structure as in vivo. This makes retinal organoids a very attractive model. To advance more, these organoid and iPSC cultures should become more consistent in yield and purity, and should become less time-consuming to conduct. After solving these challenges, they could easily be used in the biomechanical models.
Using retinal organoids and iPSCs in a biomechanical model would greatly benefit drug development. By getting closer to the human disease state, drug screening and development could be more efficient, since currently the majority of treatments fail in clinical trials after testing in in vitro and in vivo models.94,95 By mimicking more aspects of the disease, models would be more disease specific and drug screening could be more directed at the pathways that are at play, resulting in a greater success rate of possible compounds.
Greater disease specificity could be achieved by mimicking more aspects of the disease, for example, both hydrostatic pressure and strain, or using human cells. Since it is not possible to test drugs in humans in an early development stage, iPSC technology would be the optimal alternative. Using patient cells, it would be possible to identify factors that contribute to disease vulnerability (personalized risk assessment) or identify protective properties (personalized medicine). These factors could be identified by comparing the different types of glaucoma with each other or with ocular hypertension.
Comparing angle-closure glaucoma or primary open-angle glaucoma with normal tension glaucoma could elucidate the reason why patients without elevated hydrostatic pressure still develop glaucomatous visual field defects. This may, for example, be caused by an inability to cope with strain. By contrast, ocular hypertensive patients may provide details on protective mechanisms, which could be used as a target for new treatment. These protective mechanisms or vulnerabilities could then be tackled using techniques like gene editing. CRISPR-Cas9 treatments are, for example, used in the development for treating glaucoma 96 by editing defective genes, and biomechanical models can provide more valuable targets for possible treatments. RNAi is, for example, used to study the possible neuroprotective effects of kinases. 97 The identified compounds and reagents could easily be introduced to the retina by intravitreal injection. 98 These are great opportunities for the future.
Footnotes
Acknowledgments
We would like to thank the following foundations for their support coordinated by UitZicht: Glaucoom fonds, Oogfonds, Landelijke Stichting voor Blinden en Slechtzienden (LSBS), and Rotterdamse Stichting Blindenbelangen. The funders had no role in study design, decision to publish, or preparation of the manuscript.
Disclosure Statement
No competing financial interests exist.