
Abstract
Our goal was to understand the impact of regenerative therapies on the functional capacity of skeletal muscle following volumetric muscle loss (VML) injury. An extensive database search (e.g., PubMed, Cochrane Library, and ClinicalTrials.gov) was conducted up through January 2019 to evaluate the following: “In humans or animals with VML injury, is treatment better than no treatment at recovering functional capacity?” Study eligibility criteria required studies to have both an untreated and at least one treated VML injury group. From 2312 study reports, 44 studies met the inclusion criteria. Quantitative functional capacity data (absolute and/or normalized strength) or proportional measures (histological analysis quantifying viable muscle tissue, mitochondrial function, and/or exhaustive treadmill running) were extracted for use. While both human and animal studies were included in the searches, only animal studies met the eligibility criteria. Using a random-effects model, Hedges' g was used as the effect size (ES) and calculated such that a positive ES indicated treatment efficacy. The overall ES was 0.75 (95% confidence interval: 0.53–0.96; p < 0.0000001), indicating that the treatments, on average, resulted in a significant improvement in functional capacity. From network meta-analyses, it was determined that an acellular biomaterial combined with stem and/or progenitor cells had the greatest treatment effectiveness. The findings indicate that various treatments in animal models of VML improve the functional capacity of muscle compared to leaving the injury untreated; however, the ∼16% beneficial effect is small. Our results suggest that current regenerative therapy paradigms require further maturation to achieve clinically meaningful improvements in the functional capacity of the muscle.
Impact Statement
Our most salient findings are that (1) various treatment approaches used in animal models of volumetric muscle loss (VML) injury improve functional capacity compared to leaving the injury untreated and (2) an acellular biomaterial in combination with cellular components was the most effective treatment to improve functional capacity following VML injury to date. The nature of our findings has substantial implications for regenerative medicine, biomedical engineering, and rehabilitative techniques currently being evaluated and developed for VML injury repair, and are pivotal to the progression of the regenerative medicine effort aimed at restoring maximal function to traumatized and disabled limbs.
Introduction
Skeletal muscle injury is common in orthopedic trauma and can have a profound impact on a variety of treatment outcomes, including fracture healing,1,2 muscle and limb function, 3 and disability.4,5 Of particular significance are injuries in which a relatively large piece of muscle tissue is abruptly removed, such as the orthopedic wound pattern observed in soldiers following explosive blast trauma.6–8 This form of muscle trauma is referred to as volumetric muscle loss (VML) injury and differs in etiology from progressive conditions of muscle loss associated with aging or disease, such as disuse atrophy and cachexia. 9 Another key distinction of VML injuries is that endogenous mechanisms of repair and regeneration are unable to fully restore muscle function, as is typically observed in other types of injury models (e.g., eccentric contraction-, 10 ischemia reperfusion-, 11 toxin-, 12 crush-, 13 and freeze- 14 induced injury). The acute and chronic functional deficits following VML injury are primarily attributed to the frank and chronic loss of muscle fibers, that is, the muscle fibers ablated do not regenerate. 15
The little to no endogenous muscle fiber regeneration is due to three primary factors. First, the space from which the original muscle fibers were ablated is no longer resided by the satellite cells that are required to orchestrate canonical muscle fiber repair.16,17 Second, the native extracellular matrix that organizes the tissue and informs regenerative processes is lost.16,18 Third, the immune response to VML injury, which is characterized by a prolonged upregulation of proinflammatory gene programs, promotes insidious accumulation of fibrous tissue throughout the traumatized muscle compartment.19,20 Teleologically, this natural response appears to be directed at minimizing systemic infection, but predisposes to chronic dysfunction.
Traditional rehabilitative therapies (i.e., physical therapy) are the mainstay of care for VML injury, but have demonstrated limited benefit toward functional recovery in available clinical reports. 3 The high incidence of VML injury among battlefield-wounded soldiers in recent wars prompted a focused regenerative research effort supported by the United States Department of Defense and Veterans Administration.7,21 In response, a broad range of regenerative therapeutic approaches (i.e., treatments) have been developed for the explicit purpose of improving the functional capacity of the injured musculature principally by restoration of contractile tissue. 22
Generally, treatments tested have comprised biological extracellular matrices, or acellular biomaterials, with and without stem and progenitor cells and growth factors. In addition, physical therapy strategies have been implemented in isolation and in coordination with regenerative therapies. However, the benefit of treatment and if a single clinically significant treatment option for VML injury exists are unclear, primarily because similar treatments across studies have resulted in negative, modest, and positive effects on functional capacity compared to leaving the injury untreated (see for review22–25 ). Also, few studies comparatively evaluate various treatment approaches, limiting direct comparisons under identical experimental conditions. Therefore, a unique methodology to evaluate both the direct and indirect effect of treatments is necessary to determine treatment effectiveness.
The diverse experimental conditions used across studies of VML injury restrict straightforward comparisons among treatments and thereby prevent a clear understanding of the impact of current regenerative treatment approaches on the recovery from VML. Studies investigating therapeutics for VML injury have primarily used rodent models, with only a few published3,26–28 clinical reports. Other VML models have been developed in large animals, such as in pigs 20 or dogs. 29 Across species, numerous isolated muscles have been used, including the tibialis anterior, gastrocnemius, rectus abdominis, and latissimus dorsi muscles; additionally, muscle groups, including the ankle dorsiflexors, knee flexors, and knee extensors, have been evaluated. Muscle performance has been assessed throughout the literature by electrically stimulated tetanic force or torque in in vitro, in situ, and in vivo testing preparations. Maximal exhaustive treadmill testing, mitochondrial function, and histological assessment of contractile muscle tissue content have also been measured as indicators of muscle performance. This diversity of experimental conditions warrants a rigorous and quantitative analysis of the literature.
The objective of this study was twofold. First, we sought to answer the following question: “In humans or animals with VML injury, is treatment better than no treatment at recovering functional capacity?.” Upon finding a benefit of treatment on VML injury, we sought to determine which treatment was most effective at improving functional capacity. These objectives were performed using a systematic review, traditional pairwise meta-analysis, and network meta-analysis. We are unaware of any previous attempts to address these objectives using these methodologies.
Methods
Systematic review
This systematic review and meta-analysis were conducted under the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA)-specified statement. 30 Functional capacity was operationally defined as direct muscle strength or measures that should be proportional to it. The preference for functional capacity data for this analysis was skeletal muscle strength, both absolute and/or normalized. Measures of functional capacity expected to be proportional to muscle strength, including maximal treadmill testing to exhaustion, histologic analysis of viable muscle tissue, and mitochondrial density, were also considered. For studies analyzed in this meta-analysis, functional capacity measures are noted in Table 1. Studies were required to have both a VML injury group that received no treatment and at least one VML injury group that did.
Study Characteristic and Demographics
“—” indicates information not provided or unable to be appropriately estimated (magnitude of VML injury).
Single treatment groups are as follows: acellular biomaterial (AB); cells (C); rehabilitation (R); and adjunction drug (D).
Injury model also included Achilles tendon.
Injury model also included extensor digitorum longus and extensor hallucis longus muscle ablation.
Two published articles resulting from one study.
In addition, treatments were considered if they fit into multiple categories: acellular biomaterial+cells (AB+C); acellular biomaterial+cells+drug (AB+C+D); acellular biomaterial+growth factors (AB+GF); acellular biomaterial+cells+growth factors (AB+C+GF); acellular biomaterial+rehabilitation (AB+R); acellular biomaterial+cells+rehabilitation (AB+C+R); and drug+rehabilitation (D+R).
VML, volumetric muscle loss.
Our search was conducted between July 2016 and January 2019 using PubMed, Cochrane Library, EBSCO, ProQuest, EMBASE, and ClinicalTrials.gov databases. There were no limitations on the time frame in which a study was completed. The search terms and strategy used for PubMed were as follows: “acellular biologic scaffold” AND (“volumetric muscle loss” OR “decellularized extracellular matrix” OR “laceration” OR “tissue regeneration” OR “muscle tissue engineering” OR “biological scaffold” OR “orthopedic trauma” OR “rehabilitation” OR “volumetric muscle graft” OR “muscle”) OR “volumetric muscle loss” AND (“decellularized extracellular matrix” OR “laceration” OR “tissue regeneration” OR “muscle tissue engineering” OR “biological scaffold” OR “orthopedic trauma” OR “rehabilitation” OR “volumetric muscle graft” OR “muscle”) OR “decellularized extracellular matrix” AND (“laceration” OR “tissue regeneration” OR “muscle tissue engineering” OR “muscle regeneration medicine” OR “orthopedic trauma” OR “biologic scaffold” OR “rehabilitation” OR “volumetric muscle graft” OR “muscle”) OR “laceration”: AND (“muscle regeneration medicine” OR “tissue regeneration” OR “orthopedic trauma” OR “neuromuscular strength” OR “volumetric muscle graft” OR “muscle”). These search terms and strategy were modified as needed for the other databases. Reference lists of relevant review articles9,22,24,25,31–33 and the 44 included studies were also screened.
Study inclusion and exclusion criteria
The accepted clinical definition for VML injury is “the traumatic or surgical loss of skeletal muscle with resultant functional impairment.” 34 Studies conducted on humans with VML injury or animal models of VML injury were included in our search criteria. Specific inclusion criteria for review were functional quantitative data, including muscle strength (absolute and/or normalized to an indicator of muscle size), maximal treadmill test to exhaustion, histological analysis quantifying viable and/or fibrotic muscle tissue, and/or mitochondrial density and/or function. Studies were required to have at least one treatment approach and a group that received no treatment. Studies on patients were required to be conducted as randomized controlled clinical trials, with a standard of care control group. Studies were excluded for the following reasons: (1) no untreated or standard of care VML control groups; (2) use of adjunctive immunomodulation in all experimental groups; (3) case study; (4) VML combined with another type of injury, such as bone injury; (5) qualitative studies; and (6) insufficient data to calculate effect size (ES).
Selection of studies
In total, we identified 2321 relevant publications and of those, 2176 were excluded based on the review of titles and abstracts (Supplementary Fig. S1). Subsequently, 136 relevant full text publications were evaluated and 92 were eliminated for not meeting the a priori established study eligibility criteria. One publication provided evidence for two studies, with data for two different species. 20 A second publication also provided evidence for two studies, as it had two independent injury models, one VML injury to the tibialis anterior muscle and one to the gastrocnemius muscle. 35 Two studies were conducted with a shared control group and those were combined into one study for the analysis.36,37 All steps of the study selection process were conducted by two authors independently. In the event of disagreements, another author was used to mediate the disagreement.
While both human and animal studies were included in the database searches, only animal studies met the study eligibility criteria. To date, human studies have neither included both a standard of care control group and additional treatment group, nor been designed as randomized controlled trials. While clinical case studies have been published and provide important information, they did not fit the inclusion criteria. Even more, expanded case series 28 of VML-injured patients (n = 13) were not able to be included due to unique and individual data presented by patient. Notably, these (and other 3 ) clinical case studies provide extremely useful information on a relatively rare patient population that provides necessary information for this multidisciplinary field.
Primary data, including muscle strength values reported without (i.e., absolute strength) and with (i.e., normalized strength) normalization to animal body weight, muscle weight, muscle volume, or estimate of physiologic cross-sectional area, were extracted. In addition, quantitative histology of total muscle fiber number within the muscle belly region, as well as volitional run to exhaustion and mitochondrial function were also extracted and considered indices of functional capacity for this analysis. Histological analyses from isolated regions of interest were not considered indices of functional capacity, as the regions of interest are not universally applied to assess the whole musculature, but rather the defect area. If data for a measure of functional capacity were available for an uninjured control or sham group, those were extracted as well. The lack of control/uninjured data did not exclude a study. These data for uninjured groups were used to calculate the percent deficit (i.e., percent functional capacity difference) among treated and untreated groups. In all cases of insufficient data for study inclusion, multiple attempts were made to contact the corresponding author to recover these data.
Data extraction and assessment of study risk of bias
For each study, data were extracted as means, standard deviations, and sample size for the untreated and treated VML injury groups, when available p-values between paired samples were also extracted. Data were extracted for all post-VML injury and treatment time points. All data extraction was completed by two authors independently; disagreements were mediated by another author as necessary. In the nine studies where data were extracted directly from graphical form, means and standard deviations were extracted using the image analysis software, ImageJ. 38 Data extraction was completed by two authors independently and averaged. A Cochrane 39 risk of bias assessment was conducted by two authors independently on all studies based on six categories: random sequence generation, allocation concealment, blinding of personnel (participant blinding is not applicable since only animal studies were included), blinding of outcome assessment, incomplete data, and selective reporting bias. Information on funding sources and any noted disclosures or conflicts of interest were noted.
Meta-analysis
ESs for the extracted data were calculated as Hedges' g as previously described, 40 and the meta-analysis was conducted using a random-effects model to account for experimental variability across the included studies. Treatment types were then compared in a subgroup meta-analysis, which uses Q tests on the basis of analysis of variance. The extent of heterogeneity was assessed using both the I2 value and a chi-square test of the Q value. 40 The smallest group of variables analyzed was three studies with the same variable. Moderator variables specifically examined included the species, sex, animal age (i.e., mature vs. immature),41–43 muscle injured, weight bearing capacity of muscle, thickness (full or partial) of VML defect, muscle injury complexity (single or multiple muscle injury), outcome tool used, identified study bias, and if the study disclosed industry funding or authorship. To evaluate if an individual research group conducting studies could explain any between-study variation in ES, we designated research groups as a moderator variable. Collaborative research groups were identified by evaluating authors of the studies included in this meta-analysis, who were authors on multiple studies; authors were cross-referenced with each other to identify collaborative groups identified by senior authorship. Each collaborative group was required to have three or more studies in this analysis. We identified five research groups that met these criteria; studies not belonging to a research group (n = 15) were not used for this moderator. Meta-regression analyses were conducted using a method-of-moments model for the continuous moderator variables of time since VML injury induction, the percentage of tissue removed at the time of VML injury, and the functional capacity deficit induced by the VML injury.
Network meta-analysis
A network meta-analysis was conducted on absolute strength measures from the final time points of studies. Treatment subgroups were analyzed only if four or more studies that used the treatment and if three or more collaborative groups conducted these studies, to align with criteria of the network meta-analysis comparing different treatment approaches treatment in pairwise meta-analyses, used these same criteria. The network meta-analysis was conducted using frequentist framework and under the following three assumptions: similarity, transitivity, and consistency. Analyses were first evaluated assuming consistency and that was subsequently tested. When appropriate analyses were rerun assuming inconsistency, the summary of ranking effectiveness was evaluated and presented as probability of superiority.
Meta-analysis procedures were conducted using Comprehensive Meta-Analysis (version 3.3; Biostat, Inc.) and the network meta-analysis was conducted using Stata (version 14; StataCorp LLC) and the network package.44,45 An α level of 0.05 was used in all analyses, except when a nominal moderator variable with more than two levels was being probed in a subgroup meta-analysis. ESs of 0.2, 0.5, and 0.8 were considered to be small, moderate, and large, respectively. I2 values of 25%, 50%, and 75% were considered to indicate low, medium, and large degrees, respectively, of heterogeneity. Publication bias in the primary meta-analysis was assessed using a funnel plot of study ES versus standard error, and Duval & Tweedie trim-and-fill correction to the overall ES was evaluated.
Results
In total, this analysis included 44 studies (Supplementary Fig. S1), published between 2009 and 2019; these studies assessed the effectiveness of treatments for VML-injured skeletal muscle. Studies included unpublished work, conference proceedings, or work published in peer-reviewed journals, and characteristics of the studies are provided in Table 1. To determine if treatment is better than no treatment at recovering functional capacity following VML injury, Hedges' g ESs were calculated from the 44 studies with ∼7 ESs per study (range 1–37 per study; total 292 ESs). The Hedges' g ES is a standardized mean difference adjusted for study sample size. The adjustment is greater in studies with smaller sample sizes. Each study's ESs were combined into a single ES. The range of study ESs was from −1.14 to 2.87. A positive ES indicates that the treatment approach was effective in improving functional capacity over leaving the injury untreated. The meta-analysis was conducted using a random-effects model to account for experimental variability across the included studies. The overall ES was calculated to be 0.75 (95% confidence interval = 0.53–0.96; p < 0.0000001; Fig. 1), indicating that the treatments employed typically resulted in a significant improvement in functional capacity. Based on benchmarks from Cohen, 46 the overall ES would be considered large in magnitude, although we estimate it to equate to ∼16% smaller functional capacity deficit for treated VML injuries compared to those left untreated.
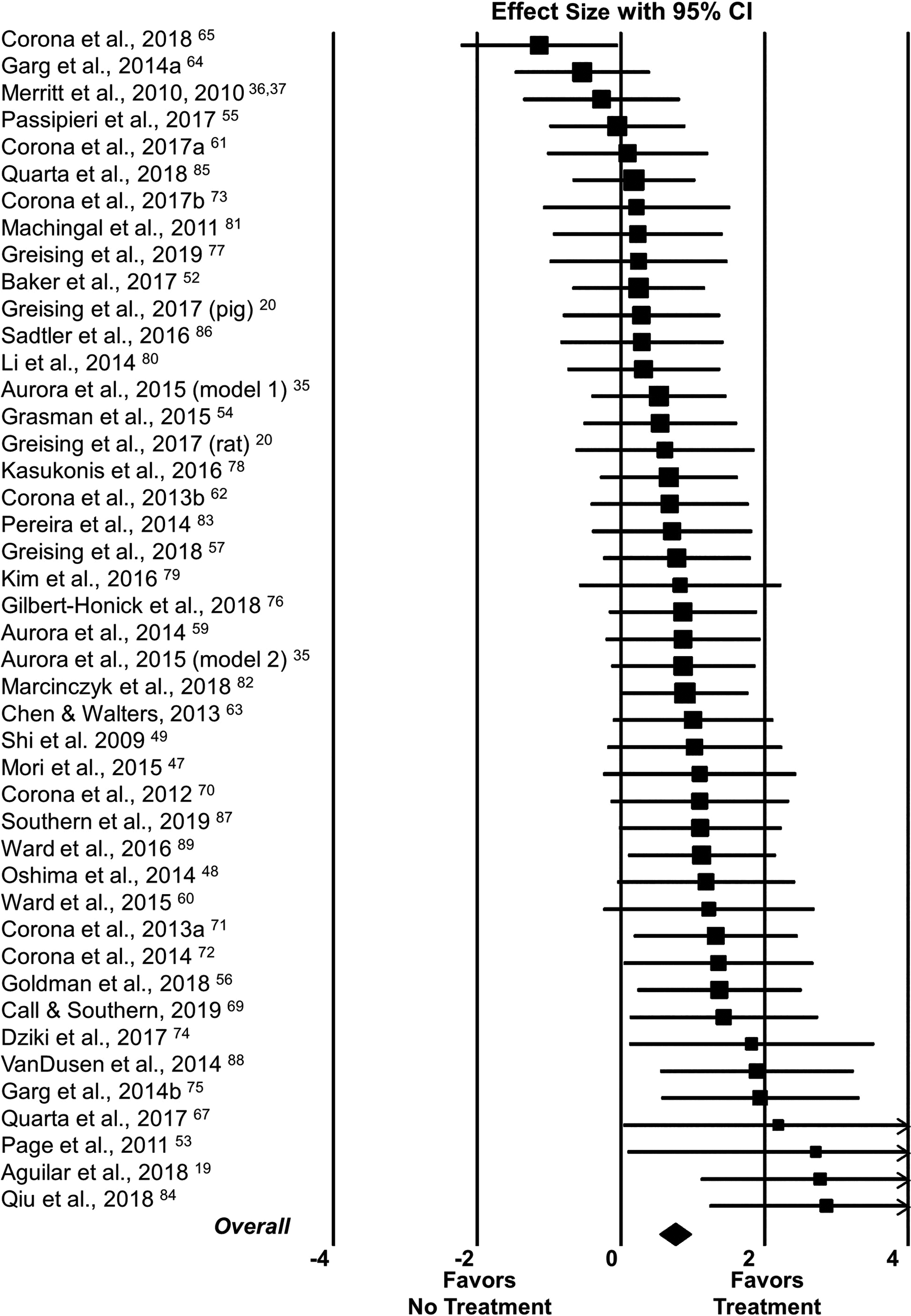
Forest plot of study ESs and 95% CI of the 44 included studies evaluating if any treatment is better than no treatment at recovering functional capacity following VML injury. Study and overall ESs were calculated using Hedges' g and a random-effects model. For each study, the superscripted number after the publication year is the reference number (see Table 1 for expanded study information). For each study, the square represents its ES and the square's size is proportional to the weighting of the study in the meta-analysis. Studies are organized in ascending order of ES. A study's 95% CI is indicated by the horizontal line running through the square. The diamond at the bottom represents the overall ES, with the diamond width representing the 95% CI. The overall ES was 0.75 (95% CI = 0.53–0.96; p < 0.0000001). CI, confidence interval; ES, effect size; VML, volumetric muscle loss.
Treatment approaches used in the 44 studies varied considerably. Acellular biomaterial-type treatments ranged from laboratory derived to commercially available and were used solely in 25 of the 44 studies. Cell treatment approaches alone (i.e., intramuscular injection of cells) were used in only four studies, three of which came from the same research group.47–49 Combinations of acellular biomaterials and cells were used in 27 studies. Drugs administered were immunomodulatory or antifibrotic agents. Rehabilitation approaches (i.e., models of physical therapy) were implemented using chronic intermittent electrical stimulation, passive range of motion exercises, eccentric and concentric contraction training, voluntary wheel running, and/or forced treadmill running.
To determine if differences among treatment types existed, ESs were calculated for each treatment as if it originated in a separate study in studies that employed more than one treatment type. Treatment subgroups were only evaluated statistically if four or more studies used the treatment and if three or more collaborative groups conducted these studies. There was no difference among acellular biomaterial, acellular biomaterial and cells combined, acellular biomaterial and growth factors combined, or rehabilitation treatment subgroups when analyzed using a pairwise subgroup meta-analysis (p = 0.53; Fig. 2). Since the overwhelming majority of studies evaluated herein, and in the literature, used acellular biomaterial or acellular biomaterial and cells combined, those were evaluated separately for differences across treatments using the same methodology. Again, there was no statistical difference in ESs between the two treatment types when evaluated by the traditional pairwise meta-analysis (p = 0.28).
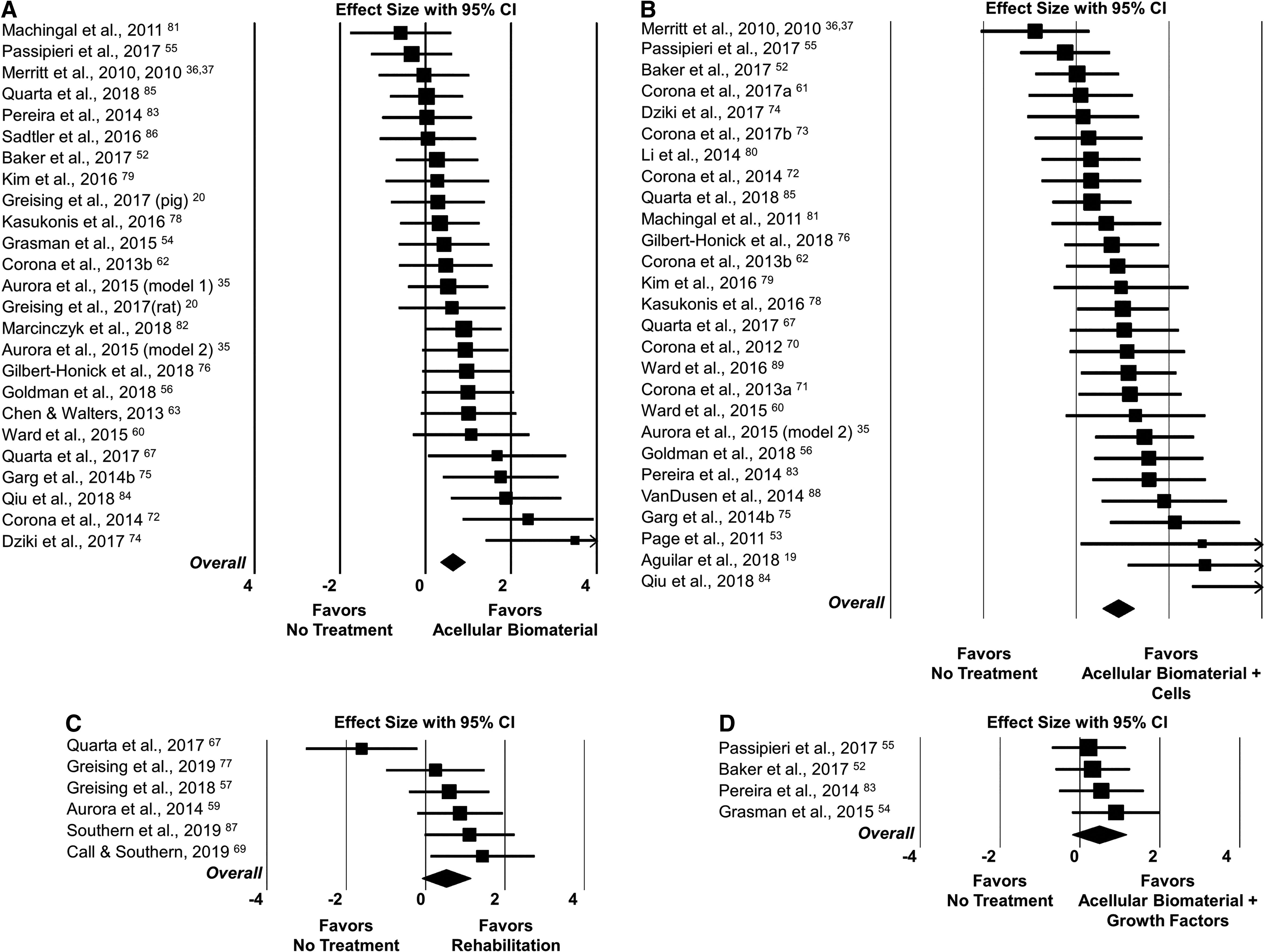
Forest plot of study ESs and 95% CI of the studies analyzed in subgroup analysis of different treatment types;
Across the 44 included studies, heterogeneity was moderate and statistically significant (Q-df = 19.7, p = 0.03; I2 = 31.4%). It is possible that the differences in treatment approaches used could explain this between-study variance. Using a network meta-analysis, the magnitude of treatment options evaluated to date is shown by the network geometry of included studies (Fig. 3A). Visibly, the overwhelming majority of treatments were acellular biomaterial or acellular biomaterial and cells combined. To align with the pairwise meta-analyses, treatments were statistically evaluated by network meta-analysis using the same criteria noted above (Fig. 3B). Using both the direct comparisons (connecting lines in Fig. 3B) and logical inference to determine indirect comparisons, a treatment of acellular biomaterial seeded with cells was determined to have the greatest effectiveness (Fig. 3D). The next two most effective treatments were acellular biomaterial by itself and acellular biomaterial with growth factors. Rehabilitation was found to be detrimental because it was ranked lower than untreated VML injury (ranking of 5 vs. 4, respectively, in Fig. 3D). Notably, ranking probabilities were similar for acellular biomaterial seeded with cells, acellular biomaterial by itself, and acellular biomaterial with growth factors. Again, since the majority of studies evaluated used acellular biomaterial or acellular biomaterial and cells combined, a separate network meta-analysis was performed (Fig. 3C), which determined that an acellular biomaterial combined with cells has the greatest probability of treatment effectiveness, followed by an acellular biomaterial. In this case, both treatments evaluated were more effective than leaving the VML injury untreated (Fig. 3E).

Data evaluated by network meta-analysis were completed at the terminal time point of evaluation for the absolute strength outcome measure, which represented data available in 43 of the 44 included studies. Network plot of direct effects of leaving the VML injury untreated or treating with various approaches. Each circle size is proportional to the number of observations (n of number of studies) within a given treatment approach. The thickness of the interconnecting lines is proportional to the number of direct comparison between any two treatments (noted in
Heterogeneity was moderate and statistically significant (Q-df ≥13.6, p ≤ 0.04; I2 ≥36.2%) in both the acellular biomaterial compared to untreated and acellular biomaterial and cells combined compared to untreated groups. This heterogeneity was similar to the overall analysis; thus, the diverse experimental conditions used in the 44 included studies (Table 1) were evaluated as moderator variables that could potentially explain between-study variance. All studies were conducted using animals, with 15, 25, and 4 studies using mice, rats, and pigs, respectively. There were 21 studies that used male animals and 20 that used female; 3 studies did not note animal sex. Animals were characterized as immature (14 studies) or mature (27 studies) at the time of VML injury; 3 studies did not report animal age. The VML injury either fully or partially encompassed the entire thickness of the muscle in 15 and 29 studies, respectively. Studies either noted the approximate percentage of tissue removed or it was estimated; the percentage of tissue loss at the time of VML injury ranged from 10% to 50% of the muscle volume and most (38 studies) of the injuries were to a single muscle. Functional capacity assessments were conducted as early as 1 week and as late as 4 months postinjury. The injuries were to muscles of the anterior (31 studies) or posterior (7 studies) compartments of the hind leg, latissimus dorsi muscle (4 studies), or knee extensor muscle group (2 studies). These were categorized as weight bearing (i.e., ankle plantar flexors and knee extensors) or non-weight bearing (i.e., ankle dorsiflexors and latissimus dorsi muscle) for analysis of moderator variables. Neither the time since injury (p = 0.08) nor percent of tissue removed (p = 0.82) at the time of VML injury was significantly related to study ES. The range of functional capacity defects between uninjured control and the untreated VML injuries (range: ∼1% to 80%) was not significantly related to study ES (p = 0.06). For the nearly significant findings of time since injury (p = 0.08) and range of functional capacity deficit (p = 0.06), there was no change in significance if analyzed within the acellular biomaterial or acellular biomaterial and cell-treated groups individually. Collectively, moderator variables, including outcome measure type, animal sex, age, species, thickness of injury, injury complexity (i.e., single or multiple muscles), muscle or muscle group injured, and weight bearing nature of the muscle, could not statistically explain any between-study variance (Table 2).
Summary of Subgroup Meta-Analyses Assessing the Effect of Nominal Potential Moderator Variables
ES, effect size calculated as Hedges' g.
Values inside square brackets represent the 95% CI for the overall ES.
CI, confidence interval.
Potential limitations of these analyses include the following: (1) studies with high risk of bias, (2) publication bias, and (3) the likelihood of this review missing published or unpublished studies. First, Cochrane risk of bias assessment 39 was conducted for all studies; overall, risk of bias was apparent, particularly in two categories. Identification of random group assignment was only noted in 39% of the studies and blinding of study personnel was only noted in 23%. It is possible this is a limitation in study reporting and not a limitation in how the studies were conducted. Eight included studies were identified as having a high risk for bias, specifically for selective reporting, meaning that they did not report all of the study's a priori specified outcomes. There is no method to directly determine the effect the omitted data may have on the overall ES; however, if those eight studies were removed, the overall ES would decrease slightly, but would still be highly significant. Second, publication bias occurs when published literature is systematically unrepresentative of the population of completed research. There is a tendency for studies with nonsignificant and/or negative findings to not be published,50,51 and therefore meta-analyses tend to be biased toward published studies. Assessment of publication bias was conducted by evaluating asymmetry of the funnel plot (Supplementary Fig. S2). Publication bias was observed within the included studies of this meta-analysis; some asymmetry was present and thus the Duval & Tweedie trim-and-fill adjustment was applied. The adjustment reduced the overall ES from 0.75 (Fig. 1) to 0.49. The adjusted overall ES was still highly significant and its magnitude would be considered moderate. Potential conflicts of interest were evaluated by involvement of the company developing the treatment tested, noted in one study 35 that disclosed funding, support, or gift in kind for the treatment tested (this study had two independent injury models) directly, and four studies52–55 noted authors with roles in various corporations. Five collaborative research groups were identified across the included studies. Collectively, noted publication bias, disclosed company funding, and work from collaborative research groups could not explain any between-study variance (p ≥ 0.29). Finally, while possible, we do not expect that our search strategy missed any published work on VML injury. Unpublished studies and studies from conference proceedings were included in this analysis, two of which were subsequently published56,57 during the interpretation of this analysis.
Discussion
The main finding of this systematic review and meta-analysis is that various treatment approaches used in animal models of VML injury improve functional capacity compared to leaving the injury untreated. Subsequent findings of this network meta-analysis determined that an acellular biomaterial combined with cellular components was the most effective treatment to improve functional capacity following VML injury to date. Analyses were conducted on outcome measure evaluated, animal sex, age, species, thickness of injury, injury complexity, muscle or muscle group injured, weight bearing of the muscle, research group, study bias, time since injury to evaluation, the percentage of tissue removed at the time of VML injury, and percentage of functional capacity difference between uninjured control and the untreated VML injury; and none of these variables could explain the between-study variance in ES.
The observed overall improvement in functional capacity with treatment versus no treatment reflects an incremental improvement (∼16%) in functional deficits. The beneficial effect of treatment, in animal models, equates to functional capacity deficit of ∼36%, compared to those VML injures that were left untreated and had a functional capacity deficit of ∼43%. This magnitude of treatment efficacy is in line with published clinical case reports using acellular biomaterial repair of quadriceps VML injuries in two wounded service members.26,27 In one report, the patient presented with a 72% strength deficit before surgical acellular biomaterial repair and ∼4 months posttreatment, a 68% deficit compared to the presurgical contralateral limb remained. 27 The second patient presented an 89% strength deficit to the uninjured contralateral limb and ∼6 months posttreatment, an 87% deficit remained. 26 Overall, these results highlight a consistent positive effect of current therapies on functional capacity that elaborates statistical, although potentially equivocal clinical significance.
Two separate analyses were performed to identify differences in efficacy among acellular biomaterial, acellular biomaterial and cells combined, acellular biomaterial and growth factors combined, or rehabilitation approaches. The first strategy was to evaluate between-study variance in treatment ESs by a subgroup meta-analysis. Treatments were evaluated to determine if an individual treatment had a greater effect on improving functional capacity compared to leaving the VML injury untreated, and there was no indication of differences in the efficacy of treatments. However, traditional meta-analyses are not able to evaluate comparative effectiveness of more than two interventions. Thus, a second strategy was used to evaluate treatment efficacy by a network meta-analysis, allowing for direct and indirect comparison of multiple interventions simultaneously. Probability of effectiveness of treatment superiority ranking induced a slightly better effect for acellular biomaterial combined with cells than an acellular biomaterial alone, and both were superior to leaving the injury untreated. Evaluation of two additional treatments indicated that an acellular biomaterial and growth factor-combined treatment was slightly worse than an acellular biomaterial alone, but still superior to leaving the injury untreated. Rehabilitation was found to result in worse outcomes than leaving the VML injury untreated in this comparison, which is in line with clinical observations using the Army Physical Evaluation Board, indicating that disability ratings following VML-related injuries do not improve even if given temporary retirement status for additional rehabilitation time. 5
The findings of the network meta-analyses suggest that the efficacy of biomaterial approaches is currently optimized when co-delivered with stem cells, but do not elaborate mechanism, or optimal stem cell(s) or biomaterial technologies. 58 Treatment approaches combined of acellular biomaterial and cells could have improved effectiveness when combined with other approaches, such as rehabilitation; however due to inadequate numbers of studies for inclusion, this and many combinations of treatment options could not be evaluated with these methods. Since the regulatory pathways for the various approaches to repair VML injury may carry varying levels of complexity, clinical translation plans may require a balance of efficacy and regulatory burden.
The observed improvement in functional capacity with treatment does not necessarily reflect regeneration of functional skeletal muscle tissue. The vast majority of studies evaluated herein used physiological functional outcomes (absolute strength n = 43; normalized strength n = 12; running distance n = 1; and mitochondrial function n = 2) to assess treatment efficacy, while only three studies were identified that reported a quantitative analysis of the entire cross-section of the muscle (e.g., total fiber number) that would allow inference of functional capacity.59–61 Prior studies have demonstrated that functional capacity can be improved following VML injury repair in the absence of skeletal muscle regeneration, potentially secondary to augmentation of force transmission across the tissue defect.35,62,63 In support, antifibrotic therapies have been shown to decrease isometric torque, expression of genes related to extracellular matrix metabolism, and fibrous tissue deposition in rodent and porcine models of VML injury.64,65 These data therefore indicate consistent benefit of repairing the VML defect with a space-occupying therapy, which may impart improvement of functional capacity through multiple mechanisms (e.g., force production and transmission). 66
The studies included in the meta-analysis involved the immediate repair of isolated, sterile VML models, which reflects the design of the vast majority of current VML studies, but may not reflect clinical scenarios of VML injury repair. For instance, surgical management of concomitant fracture and infectious or neoplastic disease processes is of greater priority than definitive soft tissue repair, and may therefore delay treatment of VML injuries with regenerative therapies. A recent study by Quarta et al. 67 reported a similar treatment effect between immediate and delayed repair using an acellular biomaterial with a stem cell approach. The conserved efficacy observed may be related to the relatively similar wound responses in muscle tissue following primary and secondary (surgical debridement of primary) VML injuries observed in a porcine model, and thus similar environments that a therapy encounters. 68 Likewise, the impact of concurrent infection, fracture, denervation or neuropathy, and vascular disruption on the improvement of functional capacity in isolated VML injury was not included in the current analysis, and reflects important considerations that may impact the effectiveness of regenerative therapies.
In conclusion, VML injury, especially among battlefield-wounded soldiers, is a continuing problem with an unmet clinical need. Findings herein indicate that in animal models of VML injury, current treatment approaches to date result in an improvement in functional capacity after injury, and that therapies that include biomaterials combined with stem cells currently achieve the greatest improvement in functional capacity among the therapeutic approaches investigated. It has been stated that, “the ultimate goal of regenerative medicine is to completely restore missing or damaged tissues to a level functionally and aesthetically indistinguishable from the preinjury/diseased state” 21 ; the modest magnitude of functional improvement observed to date with therapies for VML injury marks significant progress and invites continued innovation.
Data Availability
The datasets used and/or analyzed during this study are primarily presented in this article and are available from the corresponding author on reasonable request.
Footnotes
Acknowledgments
The authors thank Sharon Leslie, Public Health and Science Librarian at Georgia State University, for her assistance in searching the research literature during the early stages of the study.
Authors' Contributions
All authors (S.M.G., B.T.C., C.M., J.K.F., and G.L.W.) contributed to the design, data extraction, and analyses for this article. S.M.G. and B.T.C. drafted the article. G.L.W. critically reviewed and edited the article. All authors (S.M.G., B.T.C., C.M., J.K.F., and G.L.W.) have read and approved the final submitted article.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding associated with this work.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.