
Abstract
Extensive dental and periodontal defects are frequent and with a limited regenerative potential. Tissue engineering could be a promising tool to obtain personalized oral grafts. However, current research shows a lack of in vitro engineered oral tissues. This is explained by the difficulty to engineer blood vessel systems, impairing the connection to the host tissue and the graft success. Various strategies were used to engineer vascularized tissues and reported successful results, thus needing a clear analysis of the current state of art in oral tissue engineering. This systematic review aimed at studying the critical factors and techniques used to engineer a prevascularized oral tissue graft. PubMed, Cochrane Library, and SCOPUS databases were searched over the last 5 years following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines. Out of 638 screened studies, 24 were included in the systematic review according to strict inclusion and exclusion criteria and focusing on higher connection to the host vasculature. Animal models were all rodents, and subcutaneous implantation was the most used intervention. Studies presented low-to-unclear risk of bias according to the Systematic Review Center for Laboratory Animal Experimentation tool. Endothelial cells were mainly human umbilical vein endothelial cells, while stromal cells were most of the time oral or mesenchymal stem cells. Coculture of both types of cells at a 1:1 ratio was the most common technique used to obtain vascular networks, and some studies precultured grafts up to 3 weeks to enable network formation before implantation. Prevascularized grafts were produced by various tissue engineering technologies, including cell seeding and/or embedding, cell sheets, and spheroids. All studies reported a statistically significant faster and higher connection to host of prevascularized constructs compared to controls. Vessel networks were indeed denser, with a higher portion of lumen containing erythrocytes and blood flow increased. By assessing the relevant studies on the subject, this systematic review showed that engineered prevascularization proved to be an interesting approach to improve graft connection to the host vasculature and respective specific cell and scaffold criteria. Further studies on enhanced scaffolds and larger animals seem necessary to confirm these promising results with more voluminous grafts and get closer to native human tissues and applications.
Impact statement
Autologous oral grafts display limitations in terms of revascularization and morbidity of donor sites, despite being the gold standard. This systematic review aimed at clarifying existing data regarding techniques to engineer prevascularized oral grafts. Tissue engineering techniques, using cocultures of endothelial and oral stromal cells, proved to be an efficient way to enhance and accelerate the connection of the graft to the host vasculature. Engineered prevascularization appears to be a promising way to improve the connection to the host and the vascularization of grafts, especially when voluminous. Large animal and human studies are necessary to allow clinical translation.
Introduction
Defects in oral and craniofacial structures concern different types and sizes of tissues, ranging from tooth decay to extensive oncologic resection. Treatment needs are tremendous in oral surgery, endodontics, periodontics, and maxillofacial reconstruction, to replace the various missing tissues since the regenerative potential of dental and periodontal tissues is limited. In 2016, oral diseases affected at least 3.58 billion people worldwide. 1 The autograft is the biological “gold standard” candidate, but is often mutilating, painful, or unavailable. In this context, tissue engineering can interestingly provide constructs of multilayered tissues in a personalized approach with limited sampling on the donor site. One of the critical factors in tissue grafting is adequate vascularization of the graft. Initial survival of large tissue substitutes depends on the rapid development of an adequate blood supply after implantation.2,3 This issue is well described for bone grafting, with an ischemic condition occurring before neo-bone can integrate the defect. 4 The lack of vasculature leads to insufficient oxygen and nutrition supply, waste removal, and ultimately to hypoxia and graft necrosis.
Current angiogenesis enhancement strategies in tissue engineering can be divided into three main approaches: (i) growth factor-releasing scaffolds, (ii) coculture of target and endothelial cells, and (iii) engineered vasculature using microfabrication techniques or decellularized tissue. 5 “Prevascularization” emerged as a concept mixing coculture and/or microfabrication techniques to generate preformed microvascular networks embedded in constructs/grafts/tissues before their implantation, leading to a faster connection to the host vasculature. Unfortunately, the heterogeneity of the studies performing prevascularization makes it difficult for a researcher to adapt a protocol to a specific tissue construct.
The hypothesis of this study was that an engineered prevascularization can be obtained by respecting specific criteria concerning cells, technology, and scaffolds. The aim of this systematic review is to assess the critical factors and techniques to engineer a prevascularized oral tissue graft that successfully connects with the host vasculature. As human trials are not available yet, this review specifically focused on the closest step toward clinical applications, animal studies. The issue of these animal experiments is to analyze the connection of the graft to host tissues and, in a near future, to enhance graft success on humans.
Methods
Protocol and registration
This systematic review was developed and followed according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement.6,7 The review was registered on the Prospective Register of Systematic Reviews (PROSPERO) database with the registration number CRD42019122329. The protocol could be accessible at: https://crd.york.ac.uk/prospero/display_record.php?RecordID=122329
Review question
The focused question was the following one: “What are the critical factors/techniques needed to engineer a prevascularized oral issue graft?.”
Search strategy and terms
An electronic search was performed in the three following databases through the access of Bordeaux University: PubMed, The Cochrane Library, and SCOPUS. Gray literature was searched through Greylit. The search was limited to full texts available in English or French, with abstract, published from January 1, 2015 to December 31, 2019.
The following equation was used for the PubMed search: ((prevasculariz* OR prevascularis* OR pre-vasculariz* OR pre-vascularis*) OR ((pre-formed OR preformed) vascular* networks) OR (“capillary-like” OR “vessel-like” OR “vascular-like”) OR (initiat* vasculari*))
AND
(oral OR dental OR gingiva* OR tooth OR periodont* OR (“alveolar bone”) OR pulp OR (apical papilla)).
This equation was adapted to each database with the same keywords.
Inclusion and exclusion criteria
Controlled in vivo animal studies were included if they met the following criteria:
In vivo studies about engineering a graft containing functional vascular networks obtained by in vitro prevascularization. i) A graft containing oral cells and/or used to regenerate an oral tissue defect. ii) Grafted animals compared with a control (no graft or graft without prevascularization). v) Primary outcome measure: efficient vascularization of the graft (connection with the host vasculature).
In vitro models, ex vivo studies, and human studies were excluded. Studies about drug delivery devices and in vivo vascularization techniques (arteriovenous loops, autologous vascular bundles, …) were not considered. Studies without control were excluded as well.
Study selection
Two authors (R.S. and M.R.) independently screened the titles derived from the online search based on the inclusion criteria. Any disagreement over the eligibility of particular studies was resolved through discussion with a third reviewer. Subsequently, abstracts were screened, and full texts of selected abstracts were retrieved.
The selected full texts were checked by both reviewers. Any questions or disagreements were discussed between the authors concerning the remaining studies chosen for the systematic review.
Data extraction and method of analysis
Data extraction was performed independently by two reviewers using tables (R.S. and M.R.). Data were extracted from texts, as well as from tables and graphs, to answer primary and secondary outcomes.
The following parameters were extracted:
Study characteristics: author, year, country, treatment group(s), control group(s)
i) Animal model: sample size, gender, intervention, animal, age at which the graft was implanted
ii) Intervention of interest (characteristics of the graft): cellular parameters (type of tissue, endothelial and stromal cells, cell number and ratio) and technology type (tissue engineering technology, type of scaffold, in vitro preincubation).
The primary outcome was the study of vascularization characteristics and the techniques used to assess these parameters:
v) In vitro: Fluorescence activated cell sorting (FACS) (perivascular markers), quantitative polymerase chain reaction (qPCR)/quantitative reverse transcriptase-polymerase chain reaction (qRT-PCR), immunofluorescent staining, histology, identification and quantification of secreted angiogenic factors, and quantification of vascular structures.
In vivo (concerned the connection with the host): histology, immunofluorescent staining, presence of lumen, network quantification, other techniques used.
Secondary outcomes focused on the type of markers (endothelial, perivascular, and other) used.
Quality assessment of studies
Two authors independently (R.S. and A.N.) assessed the quality of included studies using the Systematic Review Centre for Laboratory animal Experimentation (SYRCLE) risk of bias tool. 8 Again, any disagreement led to discussions.
Results
Characteristics of included studies (Table 1)
Twenty-four in vivo animal studies were included in the systematic review. The flow chart of screening and selection processes is presented in Figure 1. Twelve studies originated from Asia,9–20 eight from North America (all from the United States),21—27 and four from Europe.28–31 Details concerning experimental groups and animal intervention are presented in Table 1. Animals used were essentially rodents, and subcutaneous implantation or injection was the procedure most applied (Table 1).
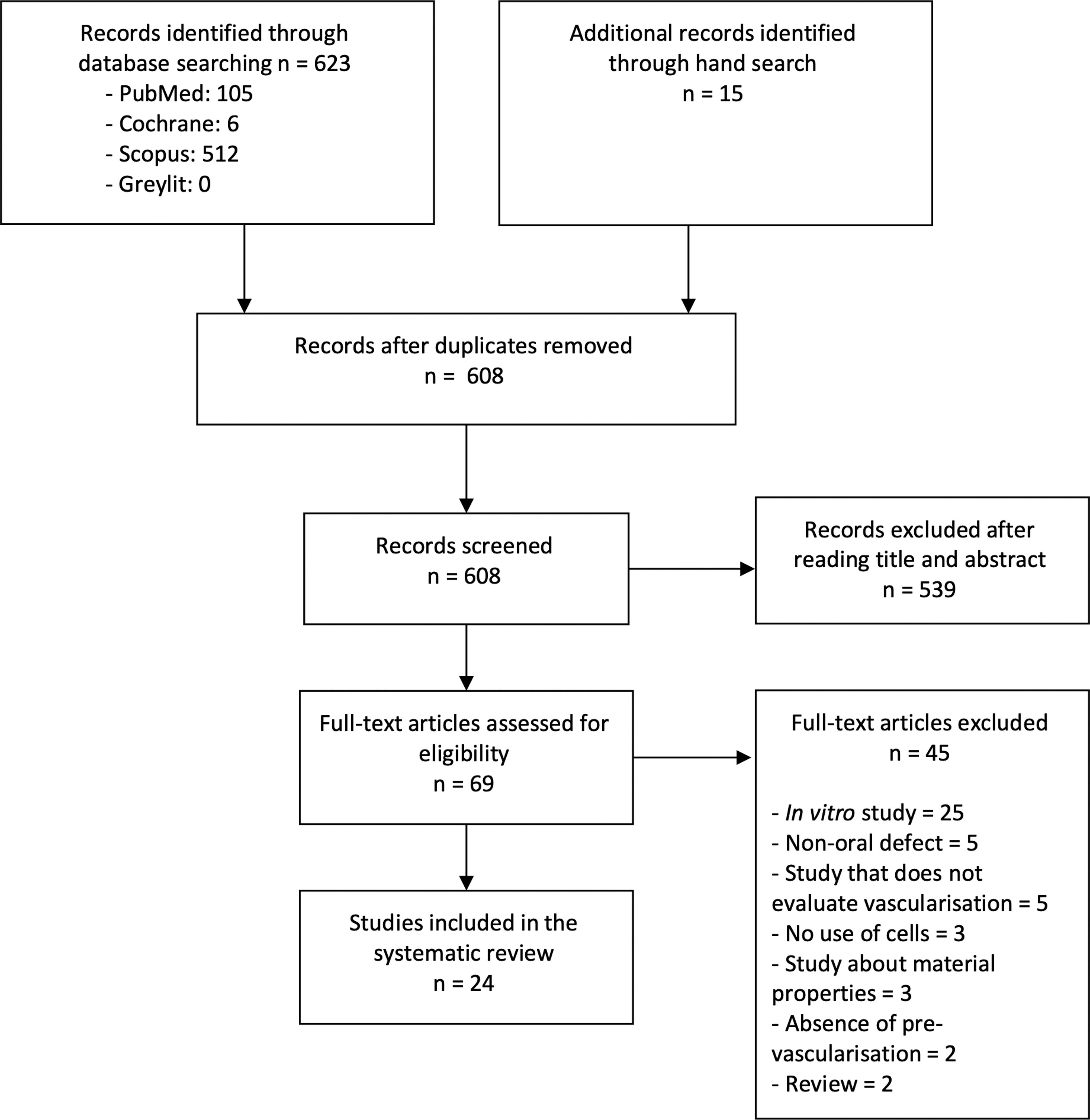
Preferred Reporting Items for Systematic Reviews and Meta-Analyses flow diagram.
Characteristics of Included Studies
ADMSC, adipose derived mesenchymal stem cells; AF, aortic fragments; AFSC, amniotic fluid-derived stem cells; AFSC-EC, amniotic fluid-derived stem cells-endothelial cells; BMSC, bone marrow stem cells; CHA, coral hydroxyapatite; CHAN, channel; COCULT, coculture; COL, collagen; CPC, calcium phosphate cement; DCS, double cell sheet; DPSC, dental pulp stem cells; ECFC-EC, endothelial colony-forming cell-derived endothelial cells; E-EPC, early-endothelial progenitor cells; EPC, endothelial progenitor cells; ESM, embryonic stem cells; F, female; GEC, gingival epithelial cells; GF, gingival fibroblasts; HAP, hydroxyapatite; BTCP, beta tricalcium phosphate; hBMSC, human bone marrow mesenchymal stem cells; HDMEC, human dermal microvascular endothelial cells; hESC-MSC, human embryonic stem cells-marrow mesenchymal stem cells; hiPSC-MSC, human induced pluripotent stem cells-mesenchymal stem cells; HSC, human mesenchymal stem cell sheet; hMSC, human mesenchymal stem cells; hUCMSC, human umbilical cord mesenchymal stem cells; HUVEC, human umbilical vein endothelial cells; L-EPC, late-endothelial progenitor cells; iPM, induced pluripotent stem cells; M, male; MSC, mesenchymal stem cells; NHLF, normal human lung fibroblasts; NR, not reported; OF, oral fibroblasts; OK, oral keratinocytes; OLC, osteoblast-like cells; PCL, polycaprolactone; PDLSC, periodontal ligament stem cell; PCS, prevascularized cell sheet; PLGA, poly(lactic-co-glycolic acid); PU, polyurethane; PV, prevascularized; SHED, stem cells from human exfoliated deciduous teeth; SVFC, stromal vascular fraction derived cells; UCM, umbilical cord.
Quality assessment of included studies (Table 2)
The SYRCLE risk of bias tool was used but difficult to apply because most studies lacked information regarding randomization procedures (items 1, 3, 4, and 6), caregivers, investigators, and outcome assessor blinding (items 5 and 7), as well as animal housing and husbandry (items 4 and 5). Most items were “Unclear” (Table 2). However, all studies provided ethical statements by indicating the nature of ethical permission and national or institutional guidelines for the use and care of animals, mostly Institutional Animal Care and Use Committees. Four studies mentioned the use of National Institute of Health guidelines.16,26,28,31 One study cited European legislation, the Directive 2010/63/EU about the protection of animals used for scientific purposes. 28 Two studies used the Animal Research Reporting In Vivo Experiments (ARRIVE) Guidelines18,19 that were first published in 2010 to improve animal studies reporting. 32
Quality Assessment of Included Studies Using the Systematic Review Center for Laboratory Animal Experimentation Risk of Bias Tool
+, indicates low risk of bias; ?, indicates unclear risk of bias.
ARRIVE, Animal Research Reporting In Vivo Experiments.
Factors needed to obtain the prevascularized grafts (Table 3)
Sources of cells
The oral cavity contains various types of tissues with specific functions, and this variability was found in the review. Ten studies focused on bone as its reconstruction is a critical issue in tissue engineering,16,18,24–29,31 while eight studies dealt with soft tissues, particularly oral mucosa,14,17,19,30 dental pulp9,12 two studies, periodontium, 15 and skin 20 (Table 3). Six studies used autologous animal cells.11,14,17,28,29,31
Characteristics of Prevascularized Grafts: Cellular Parameters and Technology Type
BCP, bicalcium phosphate; ERM, epithelial rest of Malassez; HERS, human Hertwig's epithelial rest sheath; PEG, polyethylene glycol; PPF, polypropylene fumarate; VECS, vascular endothelial cell sheet.
The “gold standard” in oral surgery being the autologous graft, main limitations concerning the use of autologous tissue cells are the necessity to perform a first surgery to harvest cells and its invasiveness with the possibility to use diseased cells. 33 Therefore, stem cells became a new target, especially with recent studies showing that the oral cavity provides multiple sources of stem cells such as oral soft tissues, the periodontal ligament, or the dental pulp. 34
As in literature, selected studies reported the following target cells used:
Mesenchymal stem cells (MSC) mainly from bone marrow or adipose tissue10,11,16,18,20,24,27–29,35
i) Oral stem cells: Periodontal ligament stem cells,13,15 dental pulp stem cells, 9 and stem cells from human exfoliated deciduous teeth 12
ii) Oral stromal cells: fibroblasts and keratinocytes14,17,19,30
Other cells: normal human lung fibroblasts, 21 osteoblast-like cells, 31 pericytes 26
Endothelial cells being a crucial element to provide vascularization, their provenance was evaluated as well. Human umbilical vein endothelial cells (HUVEC) were used in 13 studies (Table 3). Other endothelial cell types used to a lesser extent were endothelial progenitor cells,14,17,19,29 human dermal microvascular endothelial cells, 30 cells from aortic fragments, 31 amniotic fluid-derived stem cells-endothelial cells, 22 and stromal vascular fraction derived cells 25 (Table 3).
Selected studies did not report the use of additional growth factors than those included in culture media and/or scaffolds. Cell concentrations ranged from 125,000 to 10 × 106 cells/mL or per construction, depending on the technique used. Many authors worked with cell concentrations of ∼1 × 106 cells/mL, while the most reported and used cell ratio between endothelial and target cells was 1/1.
Scaffolds and biofabrication techniques
Scaffolds aim at creating tissue-specific environments and architectures to provide cells optimal conditions to survive, proliferate, and perform their specific roles as in the native tissue. To enhance vascularization, different approaches to functionalize scaffolds and tissue engineering technologies were described in selected studies (Table 3).
Spheroids
One study used scaffold-free microtissue spheroids. 9 This prevascularization technique aimed at integrating cocultures into the spheroids to obtain capillary-like networks that are fusing to a larger scale pulp-like tissue. In addition, since spheroids fuse with each other, they can be used as building blocks to scale up engineered tissues using bottom-up tissue assembly methods. This was particularly the case of three studies aiming at recreating bone.24,28,35 For instance, Mishra et al. produced a three-dimensional (3D)-printed porous polypropylene fumarate scaffold that was filled with a fibrin gel containing the MSC/HUVEC spheroids. 24 This composite approach was necessary to promote both vascularization and bone formation as (i) higher vessel formation is better allowed in softer gels, 36 whereas (ii) stiffer materials are preferred to obtain differentiation to the bone lineage. 37
Cell sheets
Cell sheet is a recent scaffold-free approach that was used in seven studies.10,14,15,17–20 This technique seems promising as it only contains cells and secreted extracellular matrix, and the sheet is manipulable and used as a building block by stacking to obtain microtissue constructs. All studies displayed an association of cell sheets containing vascularization but in different ways: Ren et al. seeded HUVEC on top of MSC sheets, folding the sheets and stacking them 10 ; Lee et al. used prevascularized sheets (composed of endothelial progenitor cells, fibroblasts with fibrin glue on top of which keratinocytes were cultured), 14 while other authors such as Panduwawala et al. prepared triple layer cell sheets using either monoculture or coculture sheet stacks. 15
Biofabrication approaches
Common biofabrication techniques to obtain vascular networks include:
Material used as scaffolds
Scaffolds used could be divided into different categories:
Naturally derived soft polymers such as matrigel,12,13 collagen,21,30 fibrin,14,17,19,35 as well as associations like collagen/fibrin 21 and fibrin/polyethylene glycol hydrogel 22
i) Synthetic polymers: Polypropylene fumarate
Stiffer scaffolds, including calcium phosphate cements, 26 polycaprolactone/hydroxyapatite,25,27 and hydroxyapatite 18 as calcium phosphates, one of the main components of bone and teeth, were among the first materials used to treat hard tissue damage.
Composite scaffolds mainly associate materials of different stiffness such as bicalcium phosphate/Matrigel, 29 β-tricalcium phosphate/collagen, 23 polypropylene fumarate/fibrin, 24 or poly(lactic co-glycolic acid)/matrigel. 31 These associations aim at enhancing biological and mechanical properties of grafts to achieve an ideal microenvironment for the cells. Remarkably, no study mentioned scaffolds mechanical characteristics (shear and elastic moduli) before and after cell loading or before and after preincubation. This could provide data about the impact of vessel network formation on scaffold behavior.
In vitro preincubation before implantation was studied (Table 3). Eight studies described preincubation times of a week or less, while the remaining studies were preincubated at least 14 days, and up to a month. The aim of this procedure was to allow time for the vascular networks to form within the graft before surgery. Mishra et al., who studied different durations, showed a significant increase of the vessel network area over 3 weeks of preculture. 24 Kang et al. used static and perfusion culture, enabling HUVEC formation from the microchannel into the surrounding collagen of the graft. 23
Hypoxic conditioning of the 3D bioprinted cell laden constructs was performed in one study for at least 7 days. 25 Kuss et al. showed by qPCR that short-term hypoxia promoted vascularization by upregulating VEGFA and HIF1A expression and expressing higher levels of PECAM and VE-cadherin. 25
Vascularization characteristics of grafts (Table 4)
In vitro characterization
In vitro assessment of prevascularization within constructs before their implantation was performed in 18 studies, insisting on the necessity to validate vessels' network formation and identify the ideal preincubation conditions (Table 4). Six studies performed in vivo analyses only.9,15,21,22,29,31
In Vitro and In Vivo Evaluation of the Vascularization
H&E, hematoxylin and eosin; vWF, Von Willebrand factor; qPCR, quantitative polymerase chain reaction; qRT-PCR, quantitative RT-polymerase chain reaction; ROI, region of interest; RFU, relative fluorescence unit; α-SMA, alpha-smooth muscle actin.
Flow cytometry was used in two studies to characterize stem cells from human exfoliated deciduous 12 and periodontal ligament stem cells (PDLSCs) 13 perivascular potential by looking at the markers NG2, PDGFR-β, and CD146. Given the essential role of the crosstalk between endothelial and perivascular cells in vasculogenesis and angiogenesis, 38 these data suggested that some oral stem cells could behave as perivascular cells and improve current prevascularization approaches.
qPCR or qRT-PCR analyses were performed in six studies identifying either perivascular markers12,13 or vascularization key indicators such as VEGF, VEGFA, CD31, vWF, and VE-Cadherin16,25–27 (Table 4). Studies showed increased expression of vascularization related genes in prevascularized constructs in vitro.
Six studies did histological analysis before implantation and assessed vascular structures with either hematoxylin and eosin or Masson-Goldner trichrome staining.11,14,17,19,28,30 Immunofluorescent staining and confocal microscopy was the most practiced in vitro analysis, mainly CD31 staining counterstained with 4′,6-diamidino-2-phenylindole. The obtained staining enabled to appraise network formation and quantification by measuring total vessel length,16,20,35 endothelial cell network area,20,24,35 vessel diameters, 35 and total number and density of junctions 20 (Table 4).
In vivo characterization
The same way as in in vitro studies, histology was performed. Immunofluorescent staining identified CD31 in 21 studies, alpha-smooth muscle actin (α-SMA),12–14,17,19,22,25,27 Ki67,14,19 mitochondria, 15 and lectin24,35 (Table 4). Ki67 staining provided supplemental information by counting the proliferating cell number.
All studies reported connection with host by identifying lumen containing erythrocytes and/or leukocytes, and vessel quantification was performed in all studies but three.12,13,30 The main values of vessel density are presented in Table 5.
In Vivo Vessel Density
The results of the group with the highest vessel density were represented in italics, and the corresponding condition was added in bold letters. *p < 0.05, **p < 0.05, ***p < 0.05.
One study performed RT-qPCR of growth factors and cytokines essentially to study early wound closure and limited scar tissue formation. 17 Concerning vascularization, VEGFA expression was increased while TGFB1 and alpha 2 smooth muscle actin (ACTA2) were reduced. 17
Vascular volume and blood flow in scaffolds were evaluated with photoacoustic imaging and/or high-frequency Doppler ultrasound imaging systems in three studies.11,20,23
Main findings
All studies showed that coculture of stromal and endothelial cells was necessary to obtain vessel-like structures in vitro and in vivo, coculture providing enhanced vasculature. Indeed, acellular controls and constructs containing monocultures of endothelial or stromal cells showed significantly lower results in terms of vascular network formation. However, Lee et al. proved that controls presented higher vessel density 2 and 4 weeks after implantation, while the prevascularized sheet provided better results at week 1. 14 This result pinpointed the capacity of prevascularized sheets to provide an early neovascularization of the wound that is essential for the survival of the graft. The new tissue obtained was less fibrotic than the control healed tissue. 14
Despite the heterogeneity of studies, prevascularization approaches used in selected studies proved to induce accelerated integration of the graft by increasing the vessel density (Table 5), as well as the number of functional vessels, which are identified in histology by lumen containing red blood cells.
As for prevascularized cell sheets, it seemed efficient for skin regeneration,17,19 periodontal regeneration, 15 as well as oral mucosa regeneration, 14 providing accelerated healing with less scarred tissue and early wound closure. Interestingly, enhanced vasculature was observed in grafts made of coculture sheets compared with PDLSC–HUVEC–PDLSC sheet grafts. 15 Quantification showed a significantly higher amount of blood vessel lumens in coculture groups, underlining the importance of having close contact between cells to promote vascularization. 15
White et al. underlined relevant evidence concerning early healing by finding rapid clotting after initial anastomosis between the host and implanted vessels at 1–6 days postimplantation. 21 However, the network within prevascularized tissues was progressively remodeled and became functional by day 7. 21
When data were given, 70–75% of endothelial cells used in the prevascularization system were found in the in vivo vascular structures 2 weeks after implantation. 10 After 1 month, only 50% of these cells remained, 23 probably because of the remodeling of the graft and its integration to the host tissue.
Furthermore, the number of vessels increased in prevascularized tissues obtained with cell sheets, enabling a rapid irrigation of the graft postimplantation. 23 A decrease was observed after 1 month in this study, 23 as well as in another study between 8 and 12 weeks postimplantation. 18
Vascularization seemed to be slowed when associated to predifferentiated osteogenic tissues, being either sheets 23 or spheroids. 28 In the spheroid model, 44% of endothelial cells remained when seeded with mesenchymal stromal cells, while 3% remained when seeded with osteo-differentiated MSC. 28
Discussion
This systematic review aimed at reporting the specifications of efficient engineered prevascularized substitutes for oral tissue grafting. Our main findings were that:
Stromal and endothelial cells cocultured at 1:1 is a key to obtain vessel-like structures in grafts and increase vessel density and fast connection to the host vasculature.
i) Scaffolds (when used) must possess biological and mechanical properties to support interaction between cells and enable them to behave as in the native tissue (specific secretions and remodeling).
ii) In vitro preculture before implantation allows time for a vascular network to form, and a short time hypoxic preconditioning can enhance the secretion of pro-angiogenic molecules.
v) Engineered prevascularization could be achieved by a variety of tissue engineering techniques and materials, mainly functionalized composite/hybrid scaffolds and technologies such as cell sheets, 3D bioprinting of cell-laden bio-inks, as well as patterning of microchannels.
In vitro analyses are often performed to validate the preformed networks before any in vivo study mainly using histology and immunofluorescent staining.
i) In vivo implantation showed a statistically significant efficiency of the prevascularized constructs by reporting increased vessel density and area, higher number of lumen containing erythrocytes, as well as higher blood flow, thanks to quantification and in vivo imaging, confirming the promotion of vascularization and the successful early connection to the host vasculature.
It was one of the few reviews focusing on oral tissue engineering and vascularization, and our results were in accordance to a recent review concentrating on craniofacial bone regeneration. 39
Concerning cell sources, it appeared that authors often used stromal cells in accordance with the tissue they want to reconstruct. Meanwhile, most selected studies used HUVEC as a source of endothelial cells, as found in literature. HUVEC is a well-established model for angiogenesis and vasculogenesis. These cells, which were first isolated and cultured in the 1970s, are readily available, quite easy to culture, highly proliferative, and possess a high migration and invasion potential. However, HUVEC may not represent actual in vivo conditions and may differ significantly from adult vascular endothelium as they do not express some adult endothelial markers. It could explain why some authors tried to use tissue-specific microvascular endothelial cells, trying to get the closest to the native tissue.
Coculture strategies were widely described in literature in the field of tissue engineering. 40 For instance, in 2004, Koike et al. showed that a coculture of HUVEC and mesenchymal precursor cells could provide a network of long-lasting blood vessels in mice, avoiding genetic modifications. 41 Positive staining of α-SMA in MSC, upon responding to the presence of endothelial cells, was found to be located in surrounding blood vessels, suggesting that MSC act in a perivascular role during the development of functional microvasculature. 42 Such results were completed by FACS analysis of perivascular markers and suggest that oral stem cells could also play the role of pericytes, knowing their specific participation in the creation and maturation of blood vessels.43,44 Coculturing of different cell types requires the optimization of different factors such as cell choice, culture media composition, phenotypic characterization, and cell ratio underlining the complexity of cell–cell interactions occurring in vivo. 45
Various materials were used as scaffolds to mimic the native tissue. Choosing the right type of scaffold can be tricky as it must enable both volume stability and cell proliferation. For instance, pore size is an essential feature that determines the blood-vessel ingrowth. A balance must be reached between adequate ability for cell migration and, as suggested in a recent review about craniofacial bone tissue engineering, porous structures and stiffness are critical factors to optimize vascularization. 46 Cell sheet technology is a relevant solution to obtain scaffold-free prevascularized tissues, getting rid of materials that could induce an immunological response or lack biodegradability. 47 It was shown that this type of technology could be used to create vascular networks, as well as reproduce complex native tissues, such as full oral mucosa equivalent by associating keratinocyte layer, endothelial layer, and fibroblast layer. 30 The main issue remains the engineering substitutes possessing mechanical properties similar to life-like tissues. As explained in a very recent review, rigidity or stiffness does not possess a strict definition. 48 However, its simplest form would be a highly elastic modulus or shear modulus, meaning that a high load would be necessary to deform a stiff material. 48 The human body displays a wide range of stiffness, and current possibilities to reproduce it include mixing materials with different properties to obtain composite scaffolds. 48 Besides, current progress in chemical composition and modification can transform any soft polymer into a more rigid matrix, providing smart materials.
Limitations were met, especially concerning the risk of bias within studies. Despite using the SYRCLE risk of bias tool, many studies did not report all elements and we could not give an accurate evaluation of the risk of bias. However, in vivo procedures start being more standardized by the use of tools such as the ARRIVE Guidelines. These new elements could enhance in vivo study quality and enable more comparability to provide concrete development toward human applications. Another missing information was materials' mechanical properties before and after cell loading and implantation, a critical factor as mentioned above.
Last advances in the subject imply a deep focus on the tissue engineering triad with relevant associations between target cells and endothelial cell coculture strategies, functionalized scaffolds, and progressive growth factor delivery. However, despite all technologies available to obtain highly tunable materials, the perfect scaffold does not exist yet. 49 The first challenge is to adapt to the oral and maxillofacial region complexity that exists in terms of 3D architecture and tissues. It is clear that we still lack the optimal scaffold to suit every clinical situation. Refined models using exosomes and pro-angiogenic micro-RNAs recently described in regenerative dentistry applications could take scaffolds to the next level in terms of angiogenesis enhancement. 50 Finally, another challenge is to get closer to in vivo and human scale. It is of crucial importance since human defects found clinically are orders of magnitude larger than defects provided by small animal studies. Larger animal models and more voluminous grafts before any human application seem unavoidable to assess the capacity to produce preformed vessels at a higher scale and reproduce the positive results presented in selected studies.
Conclusion
Based on the findings of this systematic review, we were able to show that in vitro engineered networks can provide an efficient prevascularization of grafts in oral tissue engineering and give the key features studies have in common. All studies showed earlier and increased vascularization compared to controls without prevascularization. Methods mostly used coculture of stromal cells and endothelial cells at 1/1 ratio and with preculture before implantation. The obtained networks could be adapted to all types of technologies, including cell seeding, spheroids, and cell sheets. However, further studies seem necessary to find the most suitable scaffolds according to the type(s) of tissue(s) reconstructed, as well as validate these promising concepts on larger animal models and more voluminous grafts before any human application.
Footnotes
Acknowledgment
The authors thank Séverine Carrier for proofreading.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.