
Abstract
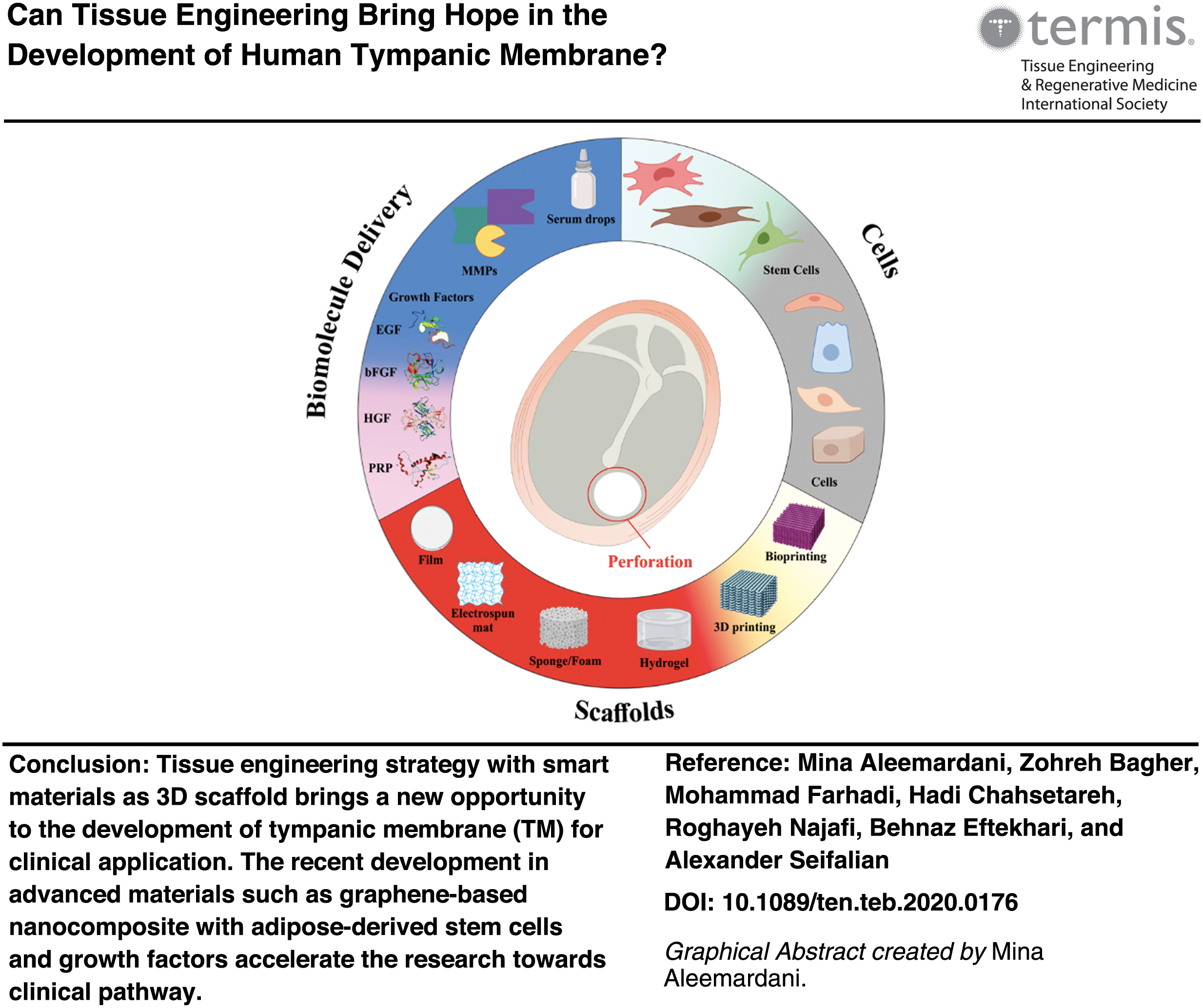
The tympanic membrane (TM), more commonly known as the eardrum, consists of a thin layer of tissue in the human ear that receives sound vibrations from outside of the body and transmits them to the auditory ossicles. The TM perforations (TMPs) are a common ontological condition, which in some cases can result in permanent hearing loss. Despite the spontaneous healing capacity of the TM to regenerate in the majority of cases of acute perforation, chronic perforations require surgical interventions. However, the disadvantages of the surgical procedure include infection, anesthetic risks, and high failure of graft patency. The tissue engineering strategy, which includes the applications of a three-dimensional (3D) scaffold, cells, and biomolecules or a combination of them for the closure of chronic perforation, has been considered as an emerging treatment. Using this approach, emerging products are currently under development to regenerate the TM structure and its properties. This research aimed to highlight the problems with the current methods of TMP treatment, and critically evaluate the tissue engineering approaches, which may overcome these drawbacks. The focus of this review is on recent literature to critically discuss the emerging advanced materials used as a 3D scaffold in the development of a TM with cellular engineering, biomolecules, cells, and the fabrications of the TM and its pathway to the clinical application. In this review, we discuss the properties of TM and the advantages and disadvantages of the current clinical products for repair and replacement of the TM. Furthermore, we provide an overview of the in vitro and preclinical studies of emerging products over the past 5 years. The results of recent preclinical studies suggest that the tissue engineering field holds significant promise.
Impact statement
This review highlights the problem with conventional surgical treatment of the tympanic membrane (TM), and critically focuses on the literature on emerging technology of tissue engineering and advanced materials in manufacturing the TM and its application to clinical setting. The advancement of the materials such as graphene as three-dimensional (3D) scaffold, stem cells technology with its growth factor, and fabrication through 3D printing made this biotechnology a possible option for treatment of TM perforations.
Introduction
Tympanic membrane (TM), also called eardrum, is a thin layer of tissue in the human ear that receives sound waves from the outer air and transmits them to the mechanical vibration to the cochlea of the inner ear (Fig. 1A). Infection in the middle ear, ventilation tube extrusion, and trauma can cause deterioration in sound transmission and TM perforation (TMP). 1 TMPs may lead to otorrhea, otitis media recurrence, conductive hearing loss and speech problems, and cholesteatoma formation. 3 Wound healing is a complicated physiological procedure, which includes epithelial migration, fibroblastic activity, and vascular proliferation. 4 Usually, most TMPs heal spontaneously within 7–10 days4,5; these rapidly healing perforations are classified as acute TMPs. Chronic perforation of the TM has been determined as a perforation that is present from 8 to 12 weeks. Large or chronic TMPs often fail to heal and may require surgery for closure.4,6 To date, tympanoplasty has been considered the most effective way to treat TMPs; also various autografts and allografts, such as paper patch, fascia temporalis have been used for repairing TM.4,7 This research aimed to critically review and give an overview of the most recent studies on the conventional and novel treatment methods of TMP. The cellular engineering/tissue regeneration is the next generation of the TMP treatment; the methodologies and its pathway to clinical setting will be discussed.
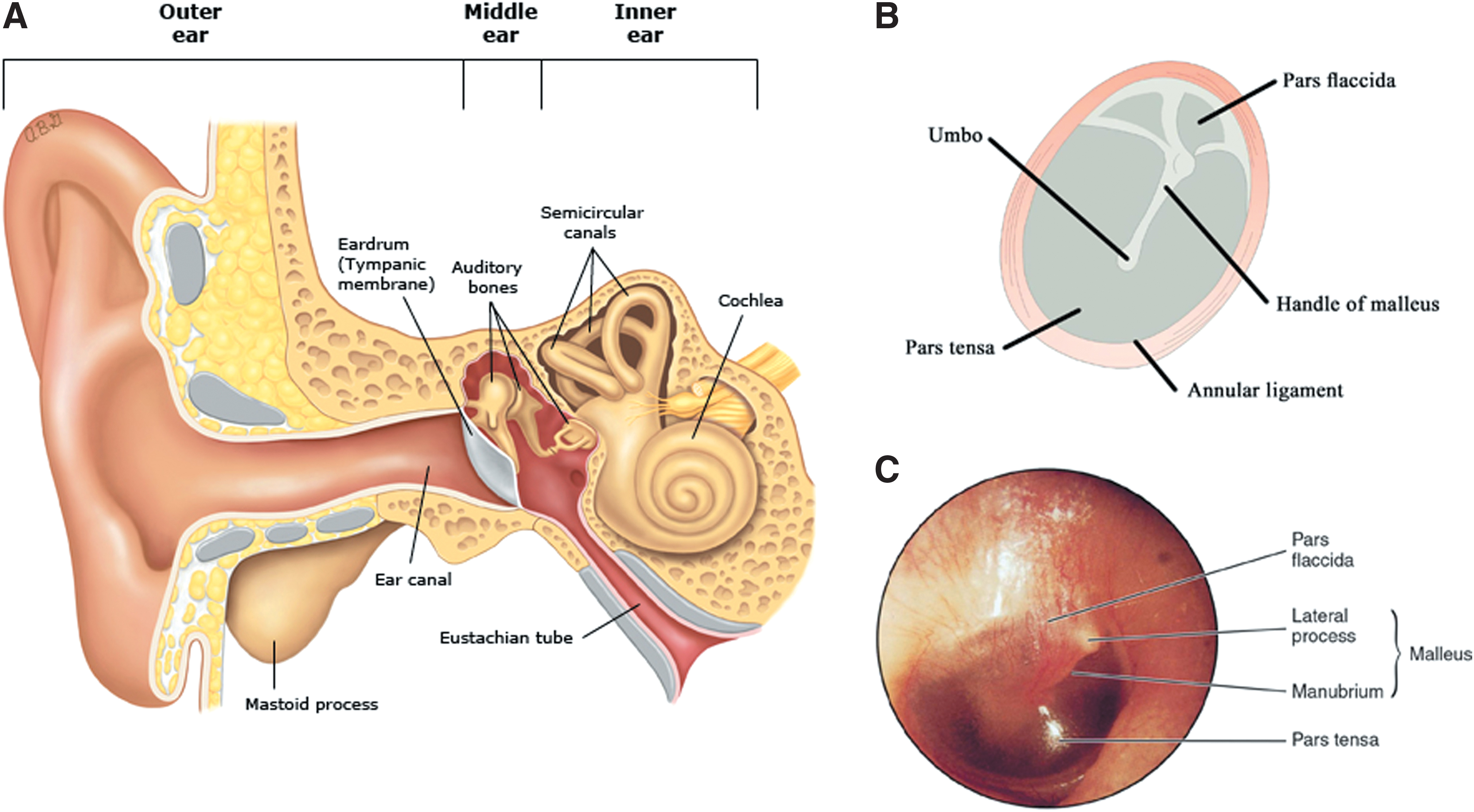
Illustration of ear anatomy and tympanic membrane (both schematic and real):
Ultrastructure of the TM
Anatomically, ear is composed of three main parts: the outer, middle, and inner ear (Fig. 1A). The outer ear consists of the visible portion called the pinna and the external auditory canal. The middle ear is a thin air-filled cavity in the temporal bone; it consists of three little bones, known as the malleus, incus, and stapes. The TM is an intermediate layer between the outer and middle ear. The inner ear consists of the cochlea, the balance mechanism, the vestibular and the auditory nerve. The function of the outer and the middle ear is to transmit sound to the inner ear. The sound waves transmutation to the external auditory canal impacts the TM, which subsequently results in TM vibration. The vibrations are conducted from the TM to the inner ear and into the fluid-filled hearing organ by three bones (Fig. 1A).8–10
The TM is in oval form located in the ear canal with a particular orientation (Fig. 1B, C). The horizontal and vertical axis length of TM is 8–9 mm and 8.5–10 mm, respectively. The TM circumference is tightly attached to the wall of the tympanic cavity that separates the outer from the middle ear. The manubrium of the malleus coupled to TM stretches from a spot on the superior edge of the TM to the umbo (its center). The manubrium may be placed symmetrically, or near to the anterosuperior edge of the TM (Fig. 1C).2,11 Round of the TM surrounded by annular ligament, this ligament is a fibrous thickening firmly anchored to a sulcus in the bony tympanic ring except for superior region. Annular ligament divides the TM into two main areas called the pars tensa (PT) and the pars flaccid (PF) (Fig. 1). 2
PT is a tightly stretched membrane covering a significant section of TM (Fig. 1B, C). The PT is composed of the following three layers from external to internal: epidermis, lamina propria, and lamina mucosa (Fig. 2). PF is a small portion of the TM, which is thicker and much more compliant. The PF of the TM layers includes two epithelial layers with a lamina propria layer (Fig. 2).8,12

A schematic of the various layers and cell types of tympanic membrane. The outer epithelial layer, entailing keratinocytes, is arranged within four layers: stratum corneum, stratum granulosum, stratum spinosum, and stratum basale. The middle layer, fibrous connective tissue (lamina propria), including fibroblasts and collagen, is arranged in the subepidermal layer, radial fibrous layer, circular fibrous layer, and submucosal layer. At last, an inner mucosal layer that consists of columnar epithelium. Reproduced from 7 (illustration prepared by Biorender). Color images are available online.
TM Physical Properties
Elasticity
Mechanical properties of the TM play a crucial role in the functionalization of the middle ear system. The hardness of a particular section of the TM depends on the density of the fibers in that zone. The hardness varies in various parts of the TM under the physiological conditions. Collagen is massively abundant in the extracellular matrix (ECM) in the TM, which aids in maintaining the resilience and integrity of the TM. Besides, the collagen fibers are responsible for the mechanical hardness of the TM. Young's modulus of a human TM at strain rates 300–2000 s−1 is reported as 45.2–58.9 MPa in the radial orientation and 34.1–56.8 MPa in the circumferential orientation. 13 The linear viscoelastic behavior of human TM has been measured in vivo using a novel nanoindentation technique. The viscoelastic values were 17.4 MPa and 19.0 MPa for posterior and anterior portions of TM, respectively. 14 TM also has some stretchability. 15
Thickness
The TM thickness is nonuniform, narrowed from the annular ring to the umbo. By moving away from the annular ring, the circular fiber layer becomes thinner; also, the thickness at the umbo reaches approximately zero. The radial fiber layer is tapered, although thickness decreases slightly.2,8,16 Thickness values across the PT ranged between 79 and 97 μm; thickness was found to be 50–70 μm in the central region between umbo and manubrium, and 100–120 μm near the peripheral rim of the PT and around the umbo. 16 Results from new technology using confocal laser microscopy and optical coherence tomography indicated that the mean across TM thickness is approximately between 50 and 120 μm. 17
Density
The volume density of the TM is variable, somewhere between that of water (1000 kg/m3) and that of undehydrated collagen (1200 kg/m3). The epidermal, mucosal, and loose connective tissue layers are maybe somewhat less thick than the fibrous layers.18,19
Cause of TM Perforations and Conventional Treatments
The TM is perforated by factors such as high-rise sounds, hot and sharp objects, middle ear infections, water entering with high pressure, accident, and during cleaning with sharp subjects.20,21 The conventional methods for the repair of the TMPs are tympanoplasty and myringoplasty. Tympanoplasty entails grafting of the TM with inspection of ossicular chain (three bones namely malleus, incus, and stapes that transmit the sounds from the TM to the inner ear) with/without reconstruction of the middle ear hearing mechanism (Fig. 1A). In other words, tympanoplasty is a clinical procedure for the reconstruction of the TM and sometimes alongside the ossicles.4,22 Myringoplasty refers to the grafting of the TM without inspection of the ossicular chain, and it is an operation performed only on TM. 23
Type I tympanoplasty is a surgical technique that involves the repair of the TM in cases where the merely existing lesion is a TMP; it is the most common otological procedure after myringotomy. It is classified based on the placement of graft concerning the remnant TM: (a) the underlay technique: a graft is placed medial to the mucosal layer; (b) the overlay technique: a graft is placed lateral to the fibrous layer of TM after elevating all squamous epithelium; and (c) the interlay technique: a graft is placed between the fibrous layer and the endothelial (mucosal) layer of the drum remnant.24–27
Today, cartilage, perichondrium, and temporalis fascia “golden standard” is commonly used as graft materials.23,28,29 In addition to the common grafts, numerous other graft materials are applied, including autologous (e.g., perichondrium, fat, vein, periosteum, sclera, and dura), cadaveric (e.g., fascia, dura, and skin), xenograft (e.g., bovine collagen, porcine pericardium, and intestinal basement membrane), and nonorganic sources (e.g., Gelfoam®, gelfilm, silastic, and paper) (Fig. 3). Autologous grafts compared with other grafts have some disadvantages, such as the scarcity of the donor tissue and surgical risks.30,31 Although temporalis fascia has long been regarded as the ideal graft material for TM repair, other ENT surgeons dismissed its application as it often failed to withstand negative middle ear pressure in the postoperative period. Therefore, some surgeons considered tragal perichondrium cartilage as a suitable alternative to temporalis fascia. This is due to the customizing of the cartilage with appropriate thickness. The thickness of <500 μm considered to have similar acoustic properties to the TM. 23 The cadaveric and xenograft may suffer from biocompatibility and immunogenicity. In general, all the grafts have a series of complications and disadvantages, such as the return of TMP, nerve damage, hearing loss, tinnitus, ear canal constriction, middle ear injury, adhesion in the middle ear, otorrhea, facial nerve injury, middle ear infection, cholesteatoma, and squamous cysts. These limitations created the impetus for alternative materials (Table 1).7,32–34

A timeline overview for the treatment of tympanic membrane perforations. Color images are available online.
The Key Conventional Surgical Repair of Tympanic Membrane with Various Materials
Surgical type tympanoplasty.
Surgical type myringoplasty.
CPI, Cartilage perichondrium island; FGM, fat graft myringoplasty; FtR, failure to repair; HAFGM, hyaluronic acid fat graft myringoplasty; L, large; M, medium; S, small; P, perforation; Pts, patients; TempF, temporalis fascia; WsCCG, wheel-shaped composite cartilage; TM, tympanic membrane; ↑, improved or increased; ↓, decreased.
Regeneration of TM Tissue Engineering Strategy
The healing of TMPs encounters difficulties, especially in the chronic case due to severe deficiencies, namely the absence of structural support, the lack of ECM, and the need for regenerative factors (e.g., angiogenesis and growth factors, GFs). 7 For overcoming these features, the tissue-engineered strategy has been applied to the development of functional TM (Figs. 3 and 4). 35
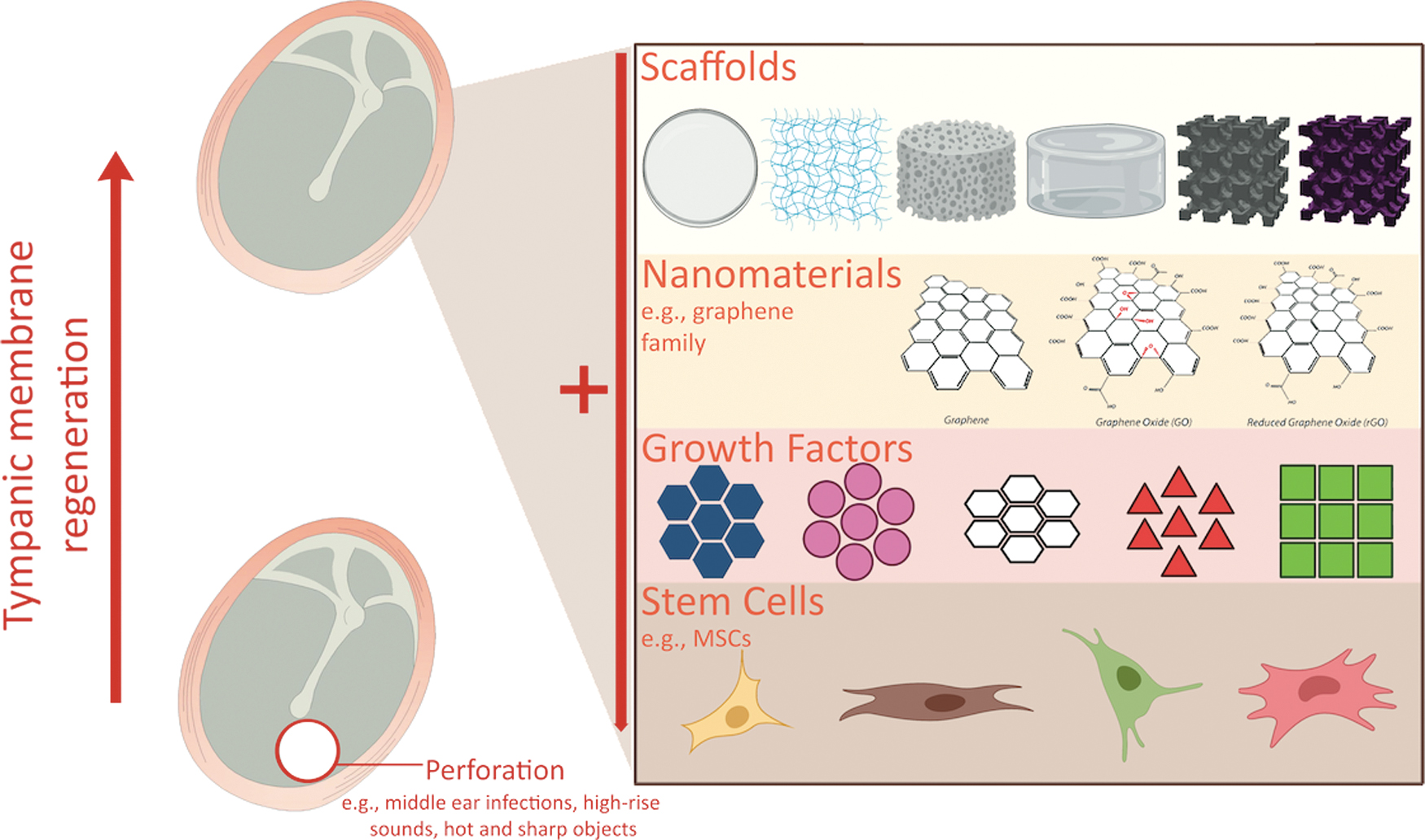
A tissue engineering TM consisting of 3D scaffold made from synthetics or biological biomaterials, cells/stem cells, and growth factors. Currently graphene-based materials are emerging 3D scaffolds, due to their superior mechanical and physiochemical properties (illustration prepared by Biorender). TM, tympanic membrane. Color images are available online.
In general, TE comprised of a three-dimensional (3D) scaffold, cells, and GFs/molecules (Fig. 4). The use of cells responds to various signals, and the seeding of cells into matrices involves creating tissue-like constructs to repair or replace the damaged organs. Besides, the use of bioactive molecules, such as GFs, encourages tissue induction. TE enables the regeneration of a patient's tissues, and thus provides the potencies for reducing the need for donor organ transplants. 36 All of these components play significant roles in either cell differentiation, proliferation, and migration or providing the proper biochemical microenvironment for preparation and stimulation of healing.7,37 A variety of manufacturing techniques and biomaterials have been used to create a 3D scaffold.38–40 Up to now, various forms of scaffolds such as films, electrospun membranes, sponges/foams, hydrogels, and 3D printed based on myriads of biomaterials have been developed for the treatment of TMPs41–43 (Fig. 4).
The utilization of tissue-engineered scaffolds brings prominent advantages such as reducing the difficulty of surgery, reducing costs, increasing the percentage of recovery, using bioactive agents, and the possibility of generating a commercially available TM. It also eliminates some of the disadvantages of other methods, such as poor biocompatibility, functionality, and immune rejection.4,7,46 The otoscopic observations related to the various forms of tissue-engineered scaffolds [film: silk fibroin scaffold (SFS), sponge/foam: acellular collagen type I/III scaffold (ACS), film: paper patch, and sponge/foam: Gelfoam] during TM healing are given in Figure 5. Each scaffold brings specific characteristics and results; for instance, SFS (fully transparent) and ACS (semitransparent) allowed observation of the TM healing directly and after complete treatment (after 28 days); there is no sign of scar formation. Unfortunately, some scaffolds cause difficulties and act improperly for TM regeneration. To exemplify, in Figure 4 it is observed that paper patch and Gelfoam caused difficulty with examination due to their opacity, partial detachment (at 7 days), and scar formation. 40

Otoscopic observation of TM healing by utilizing SFS, acellular collagen type I/III scaffold (ACS), paper patch, and Gelfoam®. White arrows indicate scaffolds; white arrowheads indicate the scar formation; asterisk indicates perforation. Photograph used with permission from Tissue Engineering: Part A 40 and Mary Ann Liebert, Inc. SFS, silk fibroin scaffold. Color images are available online.
In this review, the outcomes of different types of tissue-engineered scaffolds (films, electrospun membranes, sponges/foams, hydrogels, and 3D/bioprinted) have been reported. To the best of our knowledge, this categorization was done for the first time. The summary of studies related to the various types of scaffolds is listed in Table 2 (restricted to clinical studies), Table 3 (restricted to preclinical studies), and Supplementary Table S1 (restricted to in vitro studies). Table 4 highlights the disadvantages and advantages of emerging tissue engineering products with different 3D scaffolds.
The Clinical Study of Tissue Engineering Composite for Tympanic Membrane Healing
CR, closure rate; CT, closure time; OA, oral antibiotics; IR, inflammatory response; HL, hearing loss; CPAM, cellular proliferation, adhesion, and migration; P, perforation; Pts, Patients; PDMS, polydimethylsiloxane; FGF, fibroblast growth factor; ↑, improved or increased; ↓, decreased; NR, not reported.
The Preclinical Study of Tissue Engineering Composite for Tympanic Membrane Healing
CR, closure rate; CT, closure time; OA, oral antibiotics; IR, inflammatory response; IGFBP2, insulin-like growth factor-binding protein 2; cellular proliferation, adhesion, and migration; P, perforation; ↑, improved or increased; ↓, decreased; NR, not reported.
Advantages and Disadvantages of Various Tissue Engineering Strategies for the Tympanic Membrane Perforations Treatment
For specific materials or cells, see Tables 1–3 and Supplementary Table S1.
ECM, extracellular matrix; TMP, tympanic membrane perforations.
Films
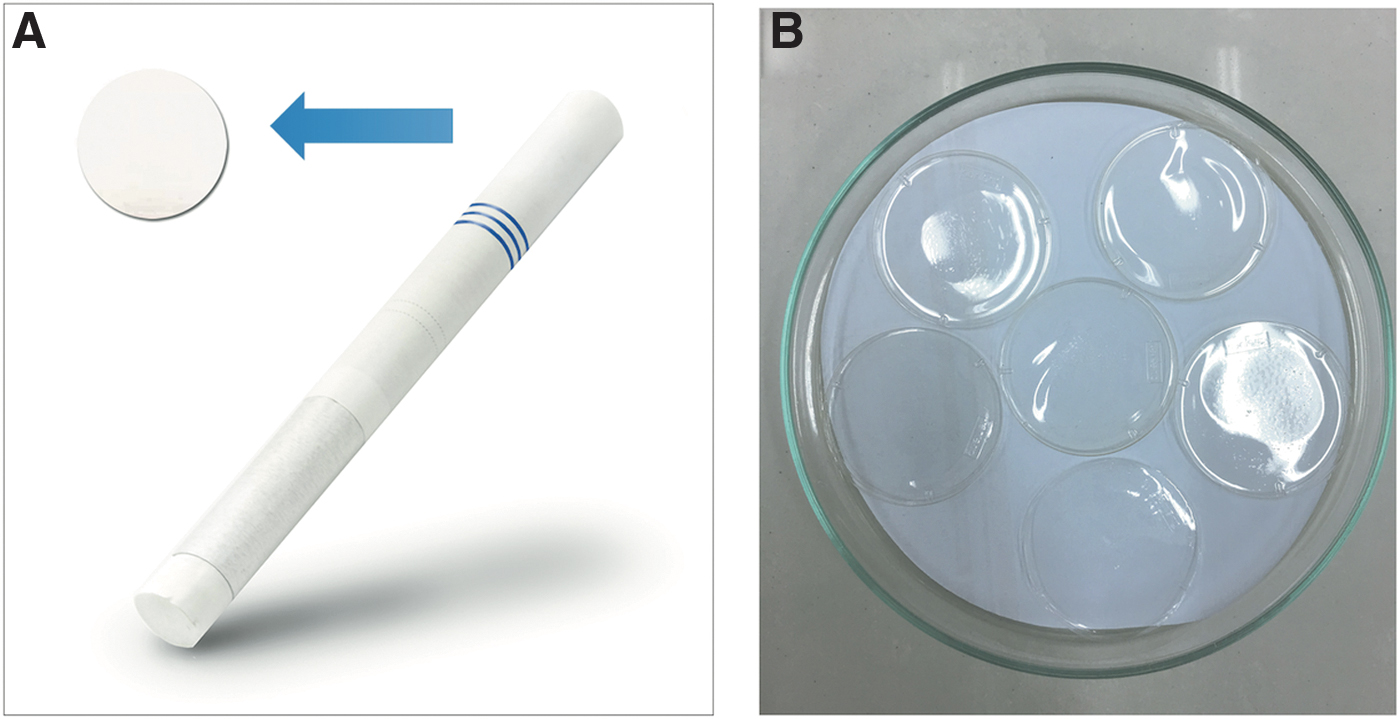
Undoubtedly, making films mostly by casting technique is the simplest way of scaffold fabrication. Owing to the simplicity and cost-effectivity of this method, in TM treatment, it is the most popular using strategy of patch production. The most common patch in the form of film that has been used worldwide is a paper patch 47 (Fig. 6A). Despite lots of studies conducted on scaffolds for TM regeneration, the paper patch still has its particular proponents mainly due to the low cost and availability. Howbeit, the paper patching process also has noticeable issues, for instance, displacement, inflammation, nontransparency, nonflexibility, nonbiocompatibility, and nonbiodegradability.48,49 For eliminating the mentioned disadvantages, further surveys have been carried out. To overcome the displacement and detachment, other biopolymers such as collagen and silk fibroin have been utilized. These biomaterials also result in the enhancement of cell adhesion.41,50,51 Fabricated patches through casting method are mostly transparent (e.g., from collagen, silk fibroin, chitosan, and bacterial cellulose) (Fig. 6B). One of the essential characteristics of film patches is transparency that lets the examination during the TM healing, and if the infection occurs, proper antibiotics will be prescribed.31,41,52,53 The thickness of the films is attempted to resemble the human/natural TM, although due to the nonuniform thickness of the natural TM (as mentioned in section TM physical properties, Thickness), usually an average is considered for film making (casting).40,54,55 The usage of the abovementioned biomaterials also leads to flexibility, biocompatibility, and biodegradability.
Electrospun membranes
Electrospinning is a well-known method in biomedicine that has been utilized extensively over the past decades. The most attractive characteristic of the electrospun fibers is mimicking the ECM structure. 56 This initiation is related to the nonadhesive (e.g., collagen and elastin) and adhesive proteins (e.g., laminin and fibronectin) in the range of 5–500 nm, and amorphous matrix, proteoglycans, in the range of 450–1000 nm, which was counted as a primary reason for this popularity. 57 Based on the piles of studies, mimicking the ECM structure steers to higher regeneration by improving cellular behavior. To exemplify, the electrospun fibers supply adequate porosity that is massively beneficial for cell migration and attachment.58,59 Compared with conventional patches, nanofibrous scaffolds could lessen the inflammation during the process of implantation, and as a result, the healing and regeneration can accelerate. 60 Recently, for TM regeneration, the electrospun mat has been employed. For instance, Danti et al. have reported that the high porosity of poly(ethylene oxide terephthalate)-co-poly(butylene terephthalate) (PEOT/PBT) electrospun scaffolds resulted in improvement of cell infiltration and viability. 46 In another study, by preparing an electrospun patch made of poly (L-lactic acid) and poly (lactic-co-glycolic acid), it was shown that the fabricated scaffold had no inflammatory response. 61 Unfortunately, the critical drawback of electrospun patches is low mechanical properties in comparison with films. 62 However, in recent electrospun technology with nanofiber production and emerging materials such as graphene-based composite, the outcome of the membranes is much stronger, as well as the stiffness and elasticity of the membranes can be changed to simulate the natural TM.
The utilization of electrospun fibers as a scaffold for TM regeneration is still unique. Thus, the recognition of various influences of electrospun membranes on the process of healing is mandatory.
Sponges/foams
Sponges or foams are 3D porous scaffolds; the porosity could facilitate cell migration and infiltration. Being porous enhances the rate of biodegradation, which was counted as another advantage. 63 Lyophilization is one of the usual techniques that has been used for the fabrication of this type (sponges/foams) of scaffold. It is worthwhile to notice that Gelfoam is the utmost type among the sponges for TM regeneration (Fig. 7). 64 Gelfoam facilitates the closure of perforations in a short time,64,65 although it has some hindrances such as infection64,66 and scar, edematous and granulation formation. 65 Howbeit, the mentioned issues also could be seen in chitosan and collagen sponges.49,63 Another attempt for developing the function of sponges is the addition of GF [e.g., fibroblast growth factor (FGF), 66 FGF-2, 43 and basic fibroblast growth factor (bFGF) 67 ], which in turn enhances the cellular proliferation and tissue regeneration. The immersion is a method that has been used for loading the GFs, so low efficiency and moistening are the main limitations within this process.43,66,67

Various shapes of Gelfoam in the clinics and markets. Color images are available online.
Hydrogels
A hydrogel is a 3D network made by chemical or physical crosslinking among the hydrophilic polymer chains; therefore, it can significantly absorb a large amount of water while preserving its structure. Hydrogels also have a great capacity for cell encapsulation and loading the bioactive molecules.68,69 In other words, hydrogels are remarkable candidates for TE and regenerative medicine due to the resemblance of ECM. 70 Keeping the moisture plays a critical role in wound healing, so hydrogels have high potency for all kinds of tissue regeneration like TM. So far, hydrogels have been made of gelatin and hyaluronic acid (HA) for TM applications.44,71 These hydrogels not only lead to the complete perforation closure but also the generation of three layers of TM tissue (skin, fibrous tissue, and mucosa). However, the possibility of sensorineural hearing loss (in particular for HA) 71 and moistening for several times during the healing are serious barriers. 44 The enhancement of mechanical properties of hydrogel with nanofiller has been successful in the development of the orthopedic and cardiac field. This may also help in the development of TM.
Three-dimensional printed scaffolds
Three-dimensional printing has been a very popular tool for industrial application; in medical 3D printing has been used to print synthetic materials. It is simply a tool that can print precise complex design.72,73 A clinical example is the surgical treatment of intra-articular distal radius fractures with the assistance of 3D printing methodology. 74 In TM, 3D printer can be used with synthetic materials with different thicknesses and different mechanical properties. 75 However, although a very useful tool, the translational to the clinic has been slow due to the suitability of material be able to use as a melting for 3D printer and with melting not easy to get viscoelasticity required on the membrane for TM.
Bioprinted scaffolds
Bioprinting is an additive manufacturing process (like 3D printing) where a combination of biomaterials (e.g., hydrogels or other biopolymers) with cells and GFs is defined as a bioink. Using bioink in bioprinting, it is possible to create tissue-like structures that imitate natural tissues.75,76 In a study, a cell-laden scaffold has been fabricated by utilizing the hydrogels (fabricated by bioprinting) entailing the mesenchymal stem cells (MSCs) and micro/nanofibers (made by the centrifugal spinning process). The prepared polycaprolactone/collagen/alginate-MSC enhanced the cell viability and resulted in complete TM healing in Sprague-Dawley rat model. The main problem of this scaffold was the regeneration of thicker fibrous layers of TM. 45 Owing to limited studies in this field, more surveys need to be performed.
According to the outcomes listed in Table 2, it could be concluded that the mere hydrophilic biomaterials (i.e., gelatin and HA) despite some effects on the healing are not suitable for TM regeneration due to the severe complications such as hearing loss, infections, and quick dissolvement. The scaffolds based on HA not only led to sensorineural hearing loss but also randomized treatment; therefore, it is not an appropriate candidate, and even after 2012, very few surveys have been performed on this material. Among the obtained results, silk fibroin has adequate potencies to be named as the best choice. It seems the biomaterials have played a dominant role in the given outcomes of the healing process. Howbeit, it could be mentioned that no significant difference was observed between the scaffold forms (i.e., films, foams/sponges, and hydrogels); hence owing to the lower cost, films are a notable option.
Myriads of studies are conducted on various biomaterials, as listed in Tables 2, 3, and Supplementary Table S1, although chitosan, silk fibroin, and crosslinked collagen and gelatin have promising results (particularly in Table 3). In other words, the mentioned materials are essentially drastic on TM treatment, and by adding other factors such as GFs, their effectiveness (e.g., healing large perforations) increases. In terms of several forms of the scaffold, based on the in vivo experiments (Table 3), electrospun membranes and hydrogels could lead to the formation of three layers of TM (skin, fibrous tissue, and mucosa), which is a plus. Still, these forms also have a lack of suitable mechanical properties. With regard to the 3D printed or bioprinted scaffolds, yet, there are no adequate research studies, but it is noticeable that it resulted in resembling vibration velocity to TM.
Cell Therapy for TM Regeneration
Utilizing cells is a crucial component in TE that facilitates the regeneration of tissues and organs remarkably. Besides, the utilization of cells enhances the likelihood of better integration of regenerated tissue with the surrounding tissues. To this aim, various cell types, mainly stem cells (SCs), have been used.77–79 SCs are promising candidates among other cells due to their specific characteristics: (1) releasing various factors, (2) recruiting other host cells by different cytokines and matrix protein release, (3) differentiating into the cells of target tissue under appropriate stimulation, and (4) being self-renewable. 80 This strategy, the usage of cells, was carried out for the TM regeneration, based on the concept of in situ TE. 1 Some surveys correlated with cell therapy for TMP treatments have been conducted. 81 For instance, the potency of latent progenitor cells, SCs within TM epithelial layers, for TM regeneration has been studied. The presence of SCs could be seen in all areas of normal TM tissue, and even at the perforated TM; therefore, staining of epithelial SC markers is additionally possible. Through this study, it has been found that latent SCs of TM have high potential for regulating the TM regeneration. 82 Due to the significant features of SCs, other kinds of SCs (i.e., except the SCs of TM) have been employed for the treatment of TMPs. Unge et al. have investigated the influences of embryonic SCs on TM healing after 5 days of myringotomy in Mongolian gerbils. According to their findings, these SCs enhance the healing of TMPs (tested by closure time, functional measures by moiré interferometry, and morphological changes by fluorescence microscopy), probably by differentiation and integration into the TM tissue. To exemplify, in this study, the strength of the SCs treated TM was 120 daPa, which compared with the treated TM (control), 60 daPa, was significantly higher. 83
The effects of MSCs on TM healing have been evaluated; some studies conducted on delivery of either MSCs alone or a combination of MSCs with GFs and biomaterials at the perforated TM sites. With the hope that these surveys may affect the activation of epithelial stem cell markers and enhance the migration and proliferation of keratinocytes, and as a result, faster closure of TMPs. 84 Through research, murine bone marrow cocultured with bone marrow MSCs (BM-MSCs) embedded within porcine-derived collagen [Gelita-Spon (GS)] or hyaluronate-derived [EpiDisc (ED)] scaffolds in C57BL/6 mice. These scaffolds accelerated the closure of TMP almost within 7–14 days, although BM-MSCs/ED had higher closure and thicker neotympanum. 85 In a mice animal model, a composite product of HA membranes seeded with BM-MSC tested for the regeneration of TM. It was concluded that BM-MSC is good cell type for cell therapy of chronic TMPs. 86
Epidermal cells are located in the umbo and annulus regions TM; these cells with stem cell-like features play an essential role in TM regeneration. In a study, Liew et al. illustrated the impacts of these cells on the reconstruction of TM. After the TMP, the biomarkers of the epidermal cell (e.g., Integrin β1 and cytokeratin 19) have been observed; then the activation of the perforated TM to proliferation and cell production indicated. 87 There are a number of reports as alluded above on cell therapy and tested in rodents but the translation to clinically been slow. This is maybe due to not easy standardized the protocol and carry out under GMP/GLP. This involved industrial collaboration and sources of the cells and cost.
Biomolecule Delivery for TM Healing
Biomolecules such as GFs have played a key role in the regeneration of TM. GFs has shown specially beneficial when the long closure time of TMPs and risk of failure of closure, in the acceleration of the TMPs healing.88–90 GFs are naturally occurring biomolecules, and are essential for regulating a variety of cellular processes and pathways. Typically, GFs remarkably increase wound healing and stimulate cellular growth. 91 Recently, GFs, such as epidermal growth factor (EGF), bFGF, hepatocyte growth factor, and vascular endothelial growth factors, have been used experimentally and clinically to promote TM healing and improve the closure rate.92,93 Therefore, several recent studies have evaluated the effect of these GFs and their effective delivery systems in preclinical and clinical trials.
EGF, a cytokine that exists in many mammalian species, simulates the in vitro and in vivo proliferation of keratinocytes, endothelial, epithelial cells, and fibroblasts. Due to the common EGF receptor (EGFR) has been found in TM of animals and humans, many studies have investigated the potential of EGF for the acceleration of TM regeneration. 94 Santa Maria et al. reported that in a mouse model with chronic TMP, heparin-binding EGF-like growth factor (HB-EGF) delivered by an injectable hydrogel could restore the vibration characteristics of TM.95,96 Based on other surveys, EGF also acts remarkably in TM keratinocyte proliferation and migration during the treatment process of TMP. 84 Many other studies proved that the usage of EGF for treatment of TMP decreases the closure time and increases the healing rate.93,94,97 A clinical study, in China, represented that the time of closure was shortened by the treatment of EGF in 44 patients with traumatic TMPs. By following up for ∼6 months, complete closure in the EGF-treated group was 96.2%, with 9.1 ± 3.9 of days closure time, which were significantly higher than the control group. 94
Several clinical and experimental studies have proved that the local application of bFGF, either direct or combined with a patch, can reduce the TM closure time and amend the closure rate without conventional operative procedures.1,98–100 As an example, a clinical study carried out in China recruited 104 patients with small (<25%) perforations. The bFGF-treated group utilized bFGF drops directly each day for 3 months. The closure rate was 100% and was significantly higher in comparison with the control group, 77%. The average closure time was 12.6 ± 1.2 days for the bFGF-treated group, notably <43.1 ± 2.5 days for the control group. 101 Despite the beneficial effect of bFGF on the acceleration of tissue formation and wound healing, there are many disagreements between research studies surrounding the appropriate dose and time of bFGF application.102,103 Many studies explored the best dose of bFGF for direct application to achieve the greatest treatment effect and manage its side effect. 103 Lou et al. in a clinical study in China have demonstrated that the combination of EGF, FGF-2, and 0.3% (w/v) ofloxacin drops could expedite the closure of large TMPs. 92
Several studies have examined the involvement of other GFs [such as keratinocyte growth factor and transforming growth factor (TGF)-a], their receptors, cytokines (e.g., IL-19, IL-24), and various enzymes (e.g., hyaluronan synthase 2) in TM regeneration.96,104,105 It is found that the TGF-a TGF-a/HA treatment increased cell–cell adhesion, cell proliferation, and migration that lead to the promotion of TM healing. 106
Platelet-derived growth factor (PDGF) releases from platelet c-granules, endothelial cells, fibroblasts, smooth muscle cells, and macrophages, is one of the several GFs that are involved in wound healing, besides it has an impact on TM closure. A clinical trial was carried out in Switzerland with 25 patients (with chronic perforated TM and chronic suppurative otitis media) by applying PDGF weekly to the TM for 6 weeks. The outcomes of this study were not satisfying; hence, it was reported that the topical application of PDGF for chronic otitis media is not a favorable alternative to surgery. 107 On the contrary, utilizing the platelet-rich plasma (PRP) increases the complete healing rate of TMP and acts as a growth-promoting agent.108,109 A clinical study in Egypt entailed 50 patients who had the TMPs. Randomly patients underwent myringoplasty with group 1, fat graft enriched with PRP or group 2, cartilage perichondrium graft as “gold standard.” After a 3-month follow-up, the improvement in pure-tone average was 18.08 dB for group 1 and 18.24 dB for group 2, and successful closure rate was 88% (group 1) and 92% (group 2), which shows that fat graft enriched with PRP is a promising choice for treatment of TM, comparable with conventional cartilage perichondrium myringoplasty. 109
KB-R7785[4-(N-hydroxyamino)-2R-isobutyl-3S-methylsuccinyl)-L-phenylglycine-N-methylamide] is a matrix metalloproteinase (MMP) that has been used to inhibit TM regeneration through an inhibitory action on MMP-2, MMP-9, disintegrin, and metalloproteinase domain-containing protein 12 (ADAM12). It has been reported that the TMPs would need to persist for ∼6 months. Therefore, they delivered KB-R7785 within a sustained-release chitosan hydrogel to 20 mice with bilateral acute TMPs and preserved 75% of perforations beyond 6 months.95,96
The autologous serum eardrops also have illustrated the successful therapy for TMP treatment; to this aim, serum eardrops are introduced within a chitin membrane as a promising noninvasive and office-based procedure for the closure of chronic TMPs. However, they must perform the additional studies to separately analyze the specific benefits of the serum drops and the chitin membrane. 110
Conclusion and Future Perspective
TMP present significant morbidity to the patients and challenge both for the clinician in term of management and surgical treatment as well as to multidisciplinary research team to bring their preclinical development to the clinical setting. There have been many surgical grafts and techniques for the treatment of TMPs, which are highlighted in Table 1. These grafts include cartilage perichondrium island with supporting materials associated with complications such as retraction, infection, and reperforation. Tissue engineering as emerging biotechnology over the past 20 years has promised a product for replacement of diseased TM, but unfortunately it has been slow to the clinical applications. This is due to complication in terms of ethics using cells/stem cells, cost and reproductivity of the product. There have been billions of dollars spent on tissue engineering products by grant councils and industries, but no products emerged as replacement or treatment of TM or any other organs. However, recently advances in material science, a large number of materials have emerged into the market, such as nanomaterials and smart materials, these stand-alone or combination with cellular engineering may bring hope to the treatment of TMP. Despite the challenges, a significant progress has been made toward the development of TM using these technologies. The listed cons and pros of tissue engineering techniques for TMP treatment are given in Table 4. The mechanical properties and biocompatibility of the materials for the 3D scaffold are important components of the TM construct. The other important factor is the integration of TM product to the surrounding tissue.
We have been working toward the development of TM using graphene-based nanocomposite copolymer. 143 Graphene is a two-dimensional honeycomb, mono- or multilayer, with sp2 hybridization. It harbors unique electrical, chemical, optical, and mechanical properties. It is 200 times stronger than steel; at the same time it is elastic and very light.144,145 Graphene can withstand enormous deformation without permanent damage; this is a crucial factor in the development of TM. We have been using a 3D printer to print a thin membrane from functionalized graphene oxide nanocomposite with different thicknesses to simulate the mechanical and physical properties of the TM. The data on 3D printing are compared with those on electrospinning membranes. The biocompatibility and toxicity of the product are also important for cellular engineering. These types of materials can also be used as a 3D scaffold for tissue engineering products.
The results of recent preclinical studies obtained from the tables suggest that the tissue engineering field holds significant promise. We hope there would be several products toward clinical application within the next 5 years.
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.