
Abstract
Sharing the methods and results of clinical trials with full transparency is an ethical obligation for those involved in clinical research. In this regard, ClinicalTrials.gov requires reporting of results to the registry within 1 year of completion of the trial. However, a poor result reporting rate has been pointed out, with approximately half the trial results not been reported. It has been suggested that one of the reasons behind this could be the influence of sponsors who conduct the clinical trials. In the course of our previous trend analysis on regenerative medicine for stroke (STR) using ClinicalTrials.gov and the International Clinical Trials Registry Platform (ICTRP) portal site as data sources, we suspected whether the results of gene and/or cell therapy trials are poorly reported. For this reason, a multivariate analysis using data from ClinicalTrials.gov was performed to identify the factors suppressing the result reporting rate, expanding our study to four different kinds of neurological diseases and regenerative medicine as a treatment modality when small-molecule compounds and biologics were set up as controls, in addition to the sponsor type factor. As a result, we found gene and/or cell therapy (therapeutic modality) in addition to STR (disease area), trials completed in 2005-2007, and clinical phases II and IV as independent factors that suppressed the rate of reporting results to ClinicalTrials.gov. On the other hand, big pharmaceutical companies were identified as a factor that increased the reporting result rate to ClinicalTrials.gov. When we applied result reporting publications through PubMed as an index, our study data revealed that the following factors were not identified as the cause for a decrease in the reporting result rate: STR (as disease area), trials completed between 2005 and 2007, and gene/cell therapy (as treatment modality). In this context, our findings indicate that gene/cell therapy has led to the suppression of the result reporting rate to ClinicalTrials.gov. This confirmed our initial suspicion of the low result reporting rate of gene/cell therapy trials. We believe that further studies are required to elucidate the factors affecting the result reporting rate from the perspective of disease area and treatment modality.
Impact Statement
Several studies have addressed the poor result reporting rate of clinical trials, which still remains an issue. Regenerative medicine holds great promise for the future and the process of its practical application is expected to be challenging. Although having a limited disease area and small sample size, to the best of our knowledge, this is the first study to point out insufficient result reporting of clinical trials of regenerative medicine from the perspective of treatment modality. This report highlights an issue for discussing the path toward its translation through an overview of various factors in comparison with conventional treatment modalities.
Introduction
The need to share methods and results of clinical trials has been a long-standing issue, requiring those involved in research to report the results of registered clinical trials fully and transparently as part of their ethical obligations. Global clinical trial registries, such as the ClinicalTrials.gov, 1 EU Clinical Trial Register (EUCTR), 2 and International Clinical Trials Registry Platform (ICTRP), 3 require disclosure of trial results. Although the disclosure of results is mandatory, the compliance rate is unsatisfactory, with only approximately half the results being disclosed.4,5 In this regard, the ClinicalTrials.gov 1 and EUCTR 2 require reporting of results to the registry within 1 year of completion of the trial; however, the deadline is rarely met.4,5
The trend of clinical trials in regenerative medicine has been analyzed from the perspective of a general research worker of regenerative medicine, who is not an expert in clinical trials, using information from databases, that is, ClinicalTrials.gov.
In the course of our previous trend analysis on regenerative medicine for stroke (STR) using ClinicalTrials.gov and the ICTRP portal site as data sources, we suspected whether the results of gene and cell therapy trials are poorly reported. In this context, we conducted a pilot analysis of result reporting.
In this report, we will provide an overview of results reporting for neurological diseases, including Parkinson's disease (PD), spinal cord injury (SCI), and traumatic brain injury (TBI), in addition to STR, because their gene and/or cell therapy (GCT) clinical translation is in a relatively early stage and focus on their efficacy and safety issues.
PD is a relatively common disease, and thus, many patients and drugs have been investigated, whereas SCI and TBI are relatively in a growth stage, and effective treatments have been recently developed for these diseases. Although these four neurological diseases are not representative of clinical applications of GCT in all diseases, we believe that they can serve as a sample model for various other diseases currently in the early stages of research. For this purpose, clinical trials investigating low-molecular-weight compounds (LMWCs) and biologics (BLG; excluding GCT) were used as comparators in this study.
Methods
Data collection
This is a retrospective cohort study using the ClinicalTrials.gov database and is not human-subject research. At first, data in the CSV format were downloaded from the ClinicatTrials.gov website as of August 9, 2019, using the following keywords: “interventional studies” as the study type and “PD,” “stroke,” “SCI,” or “TBI” as the condition or disease. Next, trials evaluating the targeted treatment modalities (LMWC, BLG, or GCT) were screened and classified among these trials using reference databases, for example, AdisInsight, 6 DrugBank, 7 and KEGG. 8 Other modalities such as devices, procedures, behaviors, radiopharmaceuticals, and diagnostics were excluded. Next, trials with a Primary Completion Date of August 9, 2019, or earlier were selected. We excluded studies that had no description for the “Primary Completion Date.” In cases where there was no date in the “Primary Completion Date” field, the date in the “Study Completion Date” was used instead. Other trials without a description of “Primary Completion Date” were excluded. We excluded studies described as “withdrawn” in the “status” field.
The dataset was subsequently updated on July 12, 2021, to follow up on the reported results of the selected trials above. We further selected trials with an “Actual Primary Completion Date” to ensure that only completed trials were included for analysis. If the Actual Primary Completion Date field is not filled in, the date in the “Actual Primary Study Completion Date” field is used instead. Among all trials with an Actual Primary Completion Date from January 1, 2005, to June 30, 2019, we examined whether their results were reported to ClinicalTrials.gov or published by PubMed through to July 5, 2021; thus, even if a trial was completed on June 30, 2019, trials with a maximum lag time of 2 years to report the results were added to the dataset.
Among clinical trials with “No Results Available” in the “Study Results” field, if it was described as “Results Submitted,” we excluded it from our analysis because it indicated that the study is still under review and has not yet been reported; therefore, it should not be counted as “No Results Available.” However, trials whose results are disclosed by PubMed publications were counted as PubMed publications.
Data of result reporting
We considered a study to be “reported” if the field “Study Results” was filled with “Has Results” in the ClinicalTrials.gov registry, and the date “Results First Posted” was used as the disclosure date.
We reviewed articles that disclosed trial results (1) by searching for links to “Publication of Results” or by investigating the link “Publications automatically indexed to this study by ClinicalTrials.gov Identifier (National clinical trial number [NCT number])” in the “More Information” section of individual trials on ClinicalTrials.gov and (2) by searching the PubMed database using the NCT number assigned to each clinical trial as an index. For each article, we manually checked if the results corresponded to the primary outcome criteria. Then, if confirmed, we adapted those trials as results have been disclosed by PubMed. Trials without corresponding results, only trial protocols (including design and plan) published, and those withdrawn were eliminated as “no results reported.”
The PubMed publication date or an earlier electronic publication date, if available, was used as the actual publication date of the article. Articles published before the “Primary Completion Date” were excluded. As for the number of article publications, since this method relies only on NCT numbers and PubMed, please note that it is a numerical index when PubMed is searched using NCT numbers, rather than showing the total number of journal publications.
Time lag to date of result reporting
Time courses due to time lag in the no-result reporting rate were depicted using the Kaplan–Meier method. The event date was defined as the date when the results of the study were reported (“Results First Posted” in ClinicalTrials.gov, the publication date in PubMed, or the earlier of the two dates if both were reported). If none of the events was reported by the data collection date (July 5, 2021), this collection date was used as the censoring date, and the number of days from the actual primary completion date was calculated and analyzed.
Sponsor classification
To investigate the relationship between result reporting and study sponsors, we classified the organizations responsible for studies as BIG, SMALL, or academic institution (AC). The top 66 companies, with revenues exceeding $2 billion in the global pharmaceutical industry in 2018, 9 were classified as “BIG”; smaller companies were designated as “SMALL”; and noncommercial organizations, that is, universities, hospitals, and government organizations, were designated as “AC.”
Phase classification
For convenience, we classified the trial phases as follows: Phase I as Phase I; Phase I/II and II as Phase II; Phase II/III and III as Phase III; and Phase IV as Phase IV.
Software
The downloaded CSV file was subjected to data cleaning and tagging using Microsoft Excel. IBM SPSS Statistics v28 was used for all statistical analyses. Sankey diagram was depicted using Origin Pro (LightStone Corp., Tokyo).
Statistical analysis
Multivariate analysis was performed for disease area, primary completion date (year), status, phase, sponsor, and treatment modality with LCON = 0.000000001. The significance level was set to 0.05. To analyze the time lag to date of result reporting, we tested for significant differences in three combinations between the three groups (BLG, GCT, and LMWC) using the log-rank method and Bonferroni method (significance level changed to 0.0166).
Results
Data collection
Data collection and processing of this study are summarized in Figure 1. Trial data were downloaded from the ClinicatTrials.gov database in CSV format as of August 9, 2019, using the following keywords: “study-type” field to “interventional” and “condition/disease” field to “PD,” “stroke (STR),” “SCI,” or “TBI.” Next, trials evaluating the targeted three different types of treatment modalities, namely, LMWC, BLG, and GCT, were screened and classified. Trials as of August 9, 2019, or earlier in the “Primary Completion Date” field were further extracted. However, trials described as “withdrawn” in the “status” field were excluded. The resulting dataset, including 1731 clinical trials, was designated as 20190809. The dataset 20190809 was updated on July 12, 2021, about 2 years after the original data collection date, to gather possible collectible information.
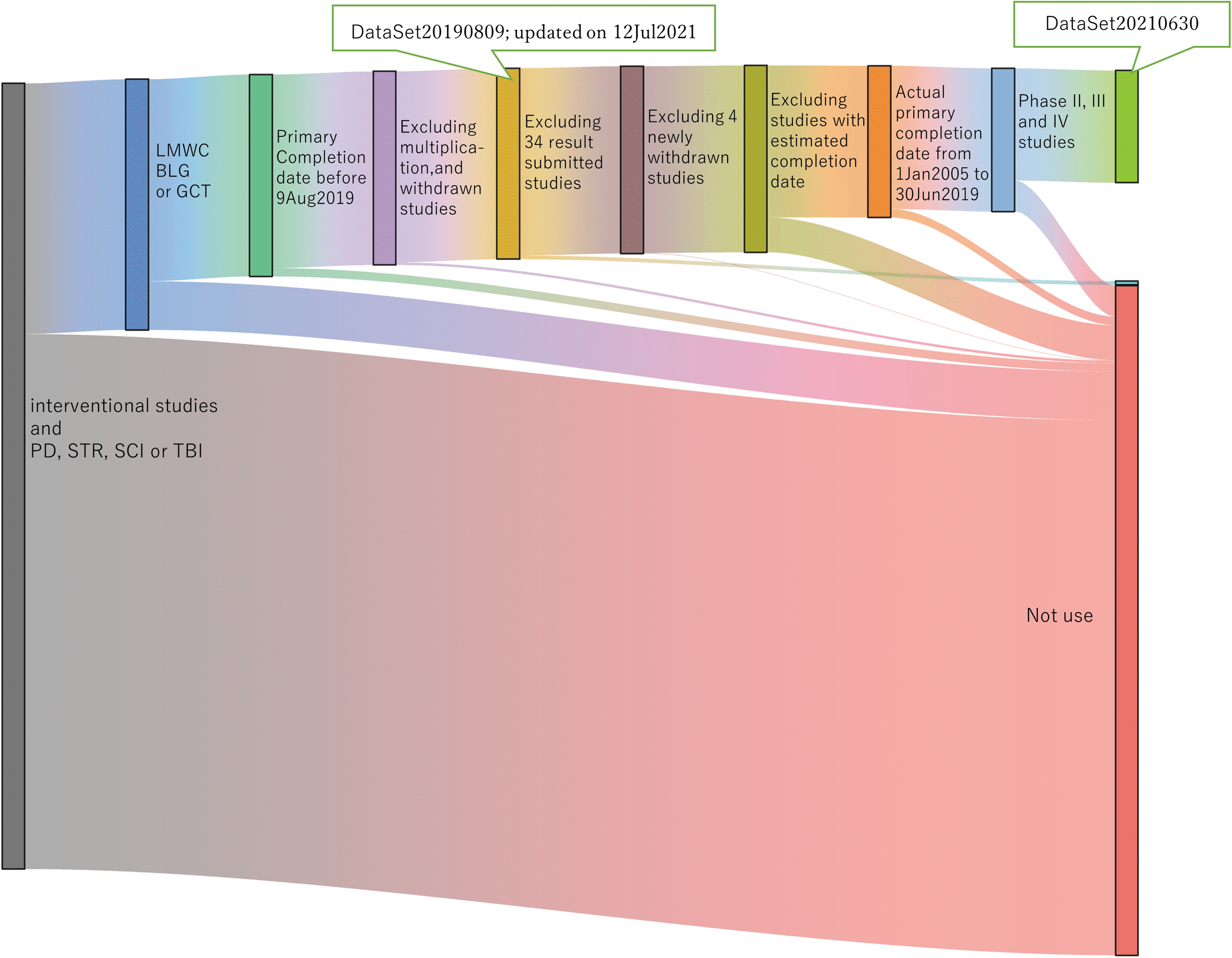
Sankey diagram for data processing. PD, Parkinson's disease; SCI, spinal cord injury; STR, stroke; TBI, traumatic brain injury.
The reported status as of July 5, 2021, was reviewed in both the ClinicalTrials.gov registry and PubMed, and 34 trials whose reports were under review in ClinicalTrials.gov, but not listed in PubMed were excluded. Then, four trials that are additionally withdrawn from the registry were also excluded. Furthermore, we considered trials as “actually completed trials” when the “Actual Primary Completion Date” field was filled, which yielded 1376 trials. To extract the relevant subset, the “Actual Primary Completion Date” was narrowed from January 1, 2005, to June 30, 2019, and obtained 1298 trials. Finally, all Phase II–IV trials were selected, for which the result reporting rate is mandatory, resulting in 1017 trials designated as 20210630 datasets.
Analysis of result reporting
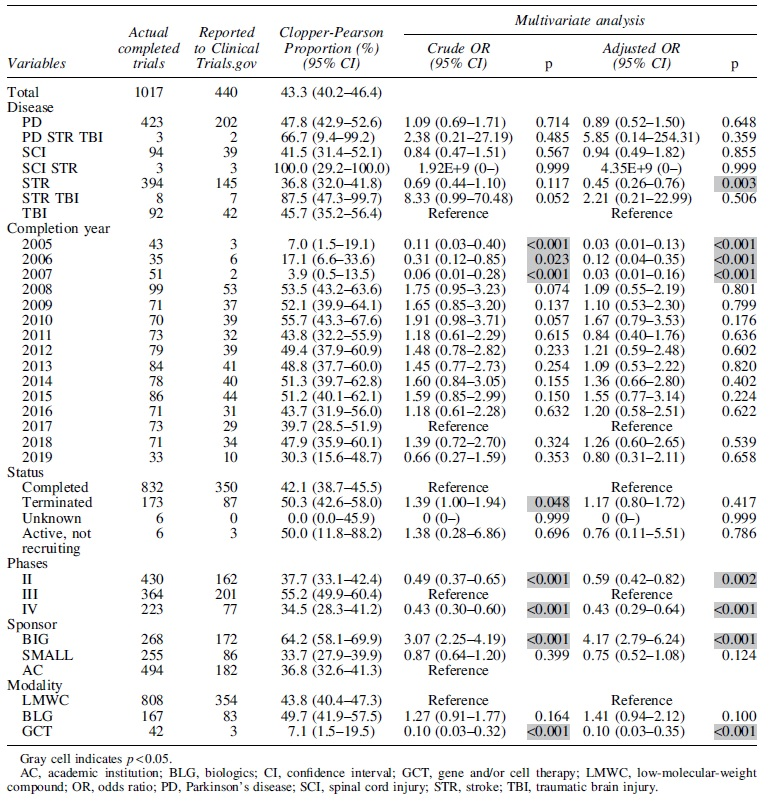
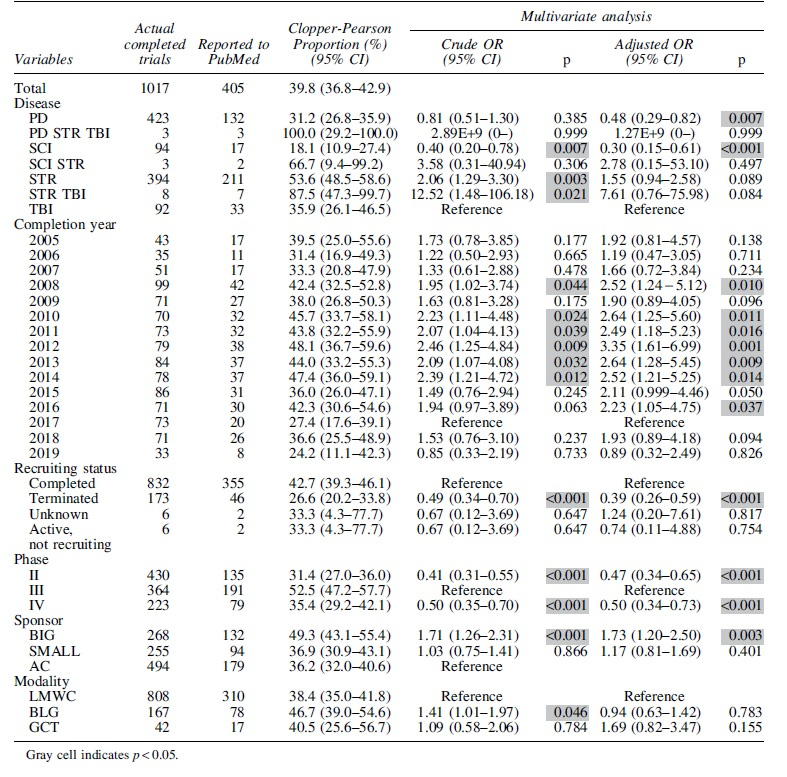
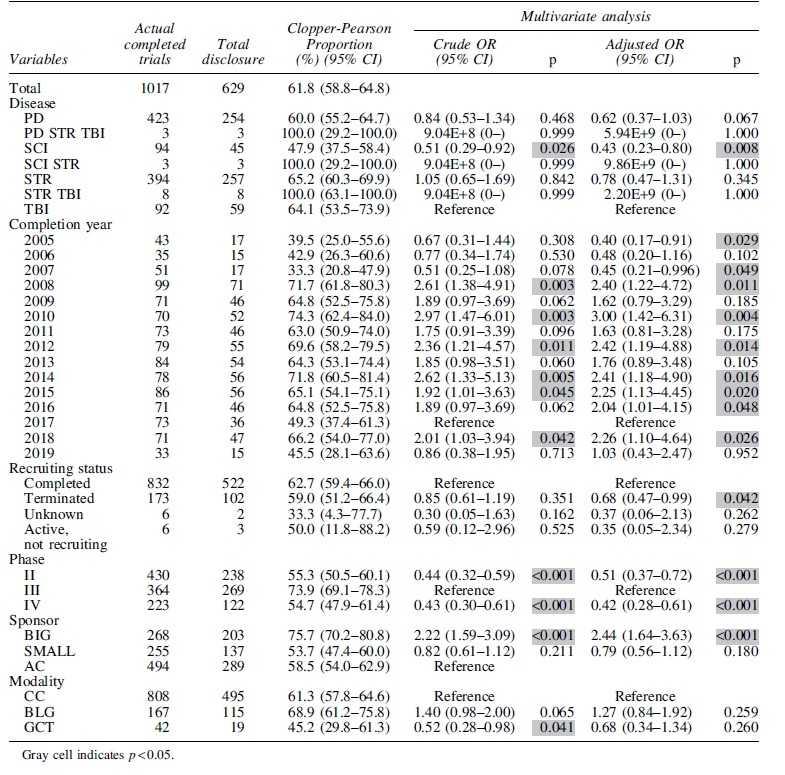
Tables 1 and 2 show the results of multivariate analysis regarding the result reporting rate of ClinicalTrials.gov and PubMed, respectively. Table 3 indicates the results of multivariate analysis on the total result disclosure rates (either ClinicalTrials.gov or PubMed or both).
Summary of Multivariate Analysis on the Result Reporting rate to ClinicalTrials.gov
Summary of Multivariate Analysis on the Result Reporting Rate to PubMed
Summary of Multivariate Analysis on the Total Result Disclosure Rate
Diseases
TBI was selected as a reference for multivariate analysis according to disease type. Table 3 shows SCI had significantly lower rates of total result disclosure with adjusted odds ratio (OR: 0.43 [95% confidence interval, CI: 0.23–0.80]; p = 0.008). Next, Table 2 shows low reporting rates from PubMed with adjusted OR (0.30 [0.15–0.61]; p < 0.001). Conversely, no difference was observed in that from ClinicalTrials.gov (Table 1).
The lower reporting rate of SCI to PubMed was interpreted as a cause of reduction in the total disclosure rate. In PD, no significance in the reporting rates was observed in total disclosure or ClinicalTrials.gov, but those in PubMed were slightly lower and more significant with an adjusted OR of 0.48 (0.29–0.82); p = 0.007. In STR, no difference in the reporting rate was observed in the total disclosure, but that in ClinicalTrials.gov was lower and more significant with an adjusted OR of 0.49 (0.26–0.76); p = 0.003. In contrast, the PubMed reporting rate was significantly higher only for the crude OR (2.06 [1.29–3.30]; p = 0.003).
Figure 2a shows the comparison of reporting rates by disease category. The reporting rate of STR trial results to ClinicalTrials.gov is the lowest among four neurological diseases, which are just <40%, whereas the other neurological diseases have also not reached 50% of the reporting rate. Nevertheless, the results of the STR trial were well published in journals, with a total disclosure rate exceeding 60%. The total result disclosure rate of PD and TBI also attained 60%. Conversely, the total disclosure rate of SCI trials was <50%.
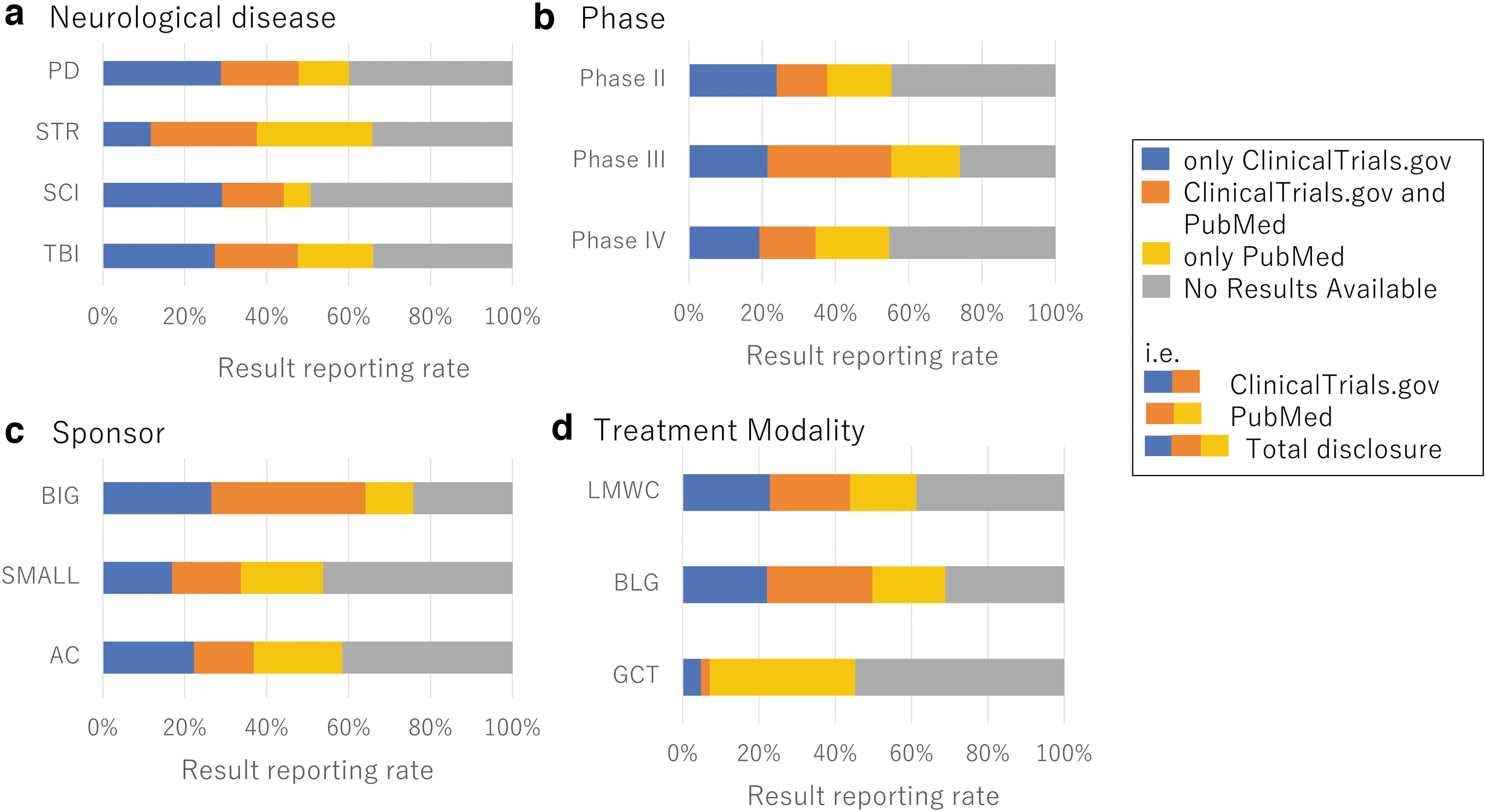
Result reporting rate of clinical trials classified by categories.
Primary completion date (year)
For the analysis of the primary completion date, data for the year 2017 were used as reference. The total result disclosure rate was significantly lower with both crude and adjusted OR from 2005 to 2007, but was significantly higher with adjusted OR in 2008, 2010, 2012, 2014, 2015, 2016, and 2018. We also observed a significantly higher reporting rate to PubMed with adjusted ORs from 2008 and 2010 to 2016.
Recruitment status
To analyze the recruitment status, trials with the field of “Recruiting Status” described as “Completion” were used as reference. Regarding the field described as “Terminated,” the reporting rate to PubMed was significantly low with adjusted ORs (0.39 [0.26–0.59]; p < 0.001), whereas the total result disclosure rate was significantly low with adjusted OR of 0.68 (0.47–0.99); p = 0.042; however, the result reporting rate to ClinicalTrials.gov was significantly high with crude OR of 1.39 (1.00–1.94); p = 0.048.
Phases
In multivariate analysis, phase III was used as a reference, and both phases II and IV had significantly lower outcome reporting rates than phase III for any reporting destination (whether the results were posted to ClinicalTrials.gov or publication in a journal). In both phases II and IV, the reporting rate was significantly lower than that in phase III (whether the results were posted to ClinicalTrials.gov or publication in a journal).
Figure 2b shows the publication status of trial results classified by clinical phases. The total disclosure rate was highest for phase III trials and significantly lower for Phase II and IV trials.
Sponsor
The AC was set up as a reference. The big pharma (BIG) had significantly higher reporting rates in ClinicalTrials.gov and PubMed, whereas small pharma (SMALL) had a similar reporting rate to AC in all result reporting statuses.
Figure 2c illustrates the result reporting rate classified by the sponsor. Regarding the disclosure of trial results to ClinicalTrials.gov, SMALL and AC were reportedly low at 35%, whereas BIG was reportedly high at >60%. Furthermore, the reporting rate of BIG was high in PubMed and ClinicalTrials.gov.
Treatment modality
LMWC was set up as a reference for treatment modality. For BLG, no difference was confirmed in any resultant reporting rates in ClinicalTrials.gov and total disclosure, but the reporting rate was slightly higher than that in PubMed with a significant crude OR. The reporting rate for both ClinicalTrials.gov and PubMed in GCT was significantly lower with a crude OR (0.52 [0.28–0.98]; p = 0.041); however, no significant difference was observed with the adjusted OR, and the reporting rate to PubMed was not significant either. Conversely, the reporting rate to ClinicalTrials.gov was revealed to be significantly lower adjusted OR (0.10 [0.03–0.35]; p < 0.001). Therefore, trials that evaluated the targeted treatment modality, that is, GCT, contributed somehow to be one of the factors that reduce the reporting rate of study results to ClinicalTrials.gov.
Figure 2d illustrates how the treatment modality affects the disclosure of trial results. The BLG trial had the highest rate of reporting trial results, followed by the LMWC. The GCT trial had a low reporting rate of trial results. The reporting rate for GCT results to ClinicalTrials.gov was remarkably low, although there was no significant difference observed in PubMed. Consequently, the total disclosure rate was reduced correspondingly. Next, we examined the time required from study completion to result in reporting by treatment modality.
Figure 3 shows the decrement in the unreported rate of results using the Kaplan–Meier method over time from the primary completion date of trials to the disclosure on ClinicalTrials.gov, PubMed, or both. In all cases, the unreported rate decreased over time, but to various degrees. For example, when comparing the unreported rate at 60 months in both databases, the GCT group had more unreported results (56%) than the BLG (34%) and LMWC (43%) groups, a ranking that remained unchanged throughout the study period.
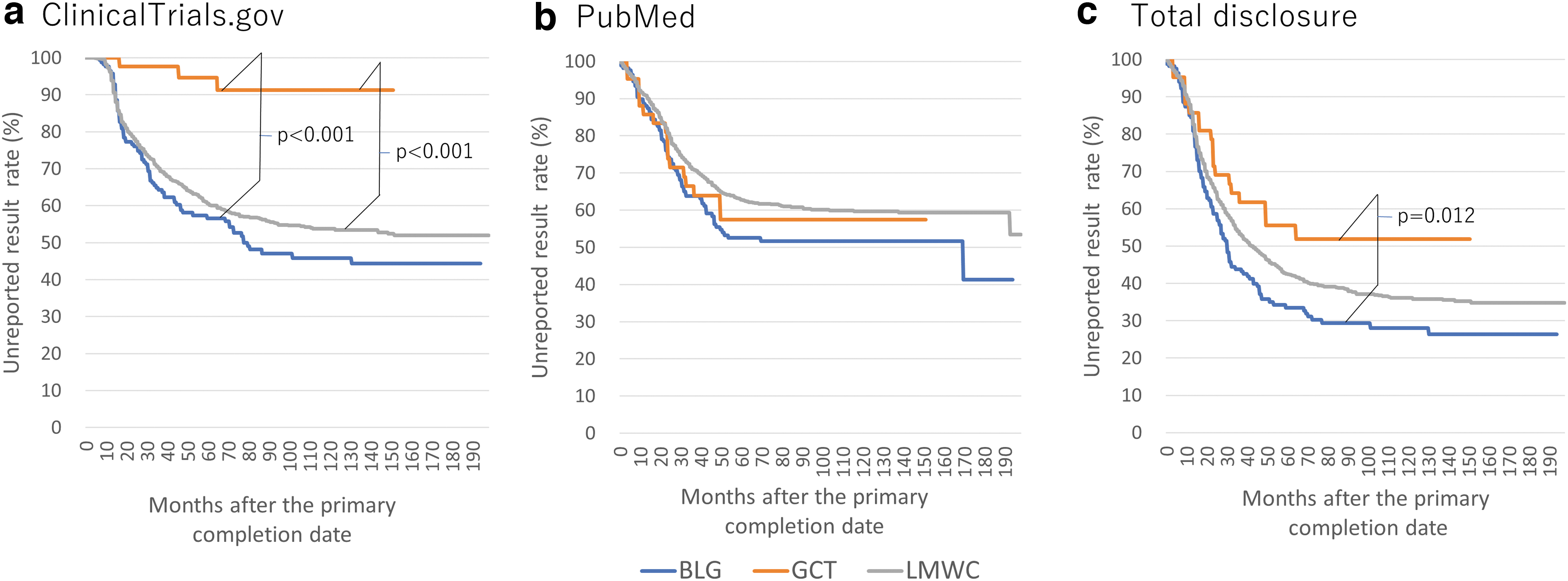
The decrement curve in the unreported result rate by the Kaplan–Meier method trucked by modality.
The log-rank method showed a significant difference between BLG and GCT (p = 0.012); however, when the reporting destination was limited to PubMed, these differences were reduced and reversed to 53% for BLG, 63% for LMWC, and 57% for GCT, without significant differences among them. Conversely, when only trials that reported results to the ClinicalTrials.gov registry were included, and trials that reported results to PubMed were not counted, the difference significantly increased in reporting rates. The unreported rate for both BLG and LMWC was 57% and 61%, respectively, at 60 months after the primary completion date, whereas 95% of GCTs were unreported, a tendency that remained unchanged throughout the study period. The results of the log-lank method showed significant differences (p < 0.001) between BLG and GCT and between LMWC and GCT.
Discussion
During our analysis of trends in clinical trials of regenerative medicine for STR, 10 we suspected whether the results of gene and cell therapy trials are poorly reported. This observation motivated us to expand the analysis to four neurological diseases and examined factors affecting the result reporting rate using multivariate analysis. In this analysis, to the best of our knowledge, the different effects in modality were considered a factor affecting the result reporting rate, in addition to the sponsor and phase, which have been previously reported.
We previously attempted to combine ClinicalTrials.gov and ICTRP to investigate trends in regenerative medicine. 10 However, using multiple registry databases can be burdensome because of the need to extract duplicate trial data and then eliminate them. Moreover, the ICTRP does not require the inclusion of an estimated “trial completion date” on the registration of individual clinical trials. Therefore, we decided that using the ICTRP database is unsuitable for this analysis; instead, we exclusively applied the ClinicalTrials.gov registry. The database of journal articles used in this analysis was limited to the articles only from PubMed, carrying out a hands-on approach.
The impetus for this study was our suspicion that only a few reports of regenerative medicine results for STR were identified in our previous analysis of clinical trials on this topic. In this study, the reporting rate of results to ClinicalTrials.gov was one of the independent factors, as a significant difference in the adjusted OR was observed for STR. Our research found that the reporting rate for STR results to ClinicalTrials.gov was the lowest among the four neurological diseases at <40%, whereas the reporting rate to ClinicalTrials.gov did not reach 50% for the remaining diseases.
Although result reporting to PubMed was significantly different only in crude ORs, not in adjusted ORs, STR results were frequently reported in journal publications. Therefore, the combined reporting rate to ClinicalTrials.gov and PubMed exceeded 60%. The result reporting rates of PD and TBI reached 60% when ClinicalTrials.gov and PubMed results were combined, whereas that for ClinicalTrials.gov and PubMed of SCI remained <50% and <20%, respectively. These outcomes were significant in the adjusted ORs. Our findings indicate that some degree of bias may occur in favor of either ClinicalTrials.gov or PubMed in terms of result reporting, depending on the disease type because of various clinical trial characteristics. The cause of this bias remains unknown. Nevertheless, these reporting rates are broadly similar to those previously reported by Zwierzyna et al. 4 (overall, neurology had a 40% reporting rate on ClinicalTrials.gov and <60% for both ClinicalTrials.gov and PubMed).
Regarding the primary completion date (year), the result reporting rates to ClinicalTrials.gov were low in 2005–2007 because Section 801 of the Food and Drug Administration Amendments Act became effective in 2007. 11 Furthermore, PubMed had significantly higher reporting rates from 2008 and 2010 to 2014 and 2016; however, its cause needs to be examined in more detail.
Regarding the field of “recruitment status,” a few errors were found, which may have been due to data entry errors by the primary investigator, such as “unknown status” or “active, not recruiting,” despite entering specific dates in the field of “Actual primary completion date.” We considered those trials were the mistake of not updating recruiting status, in fact, as we confirmed that some trials contain study results.
We conducted a sensitivity analysis with 1005 trials, which excluded “active, not recruiting” and “Unknown” trials and obtained almost the same findings (Supplementary Tables S1–S3). “Terminated,” in which the trial was terminated before the estimated patient recruitment was completed for various reasons, was identified as a factor that decreases the result reporting rate in PubMed. The reason for “Terminated” may be related to the efficacy or safety issues of the study drug. In such cases, the results should be reported ethically. The results of this analysis show that the reporting result rate to ClinicalTrials.gov did not differ based on the number of completed trials, but the number of reports on publication in journals was lower. A more detailed analysis is needed for further discussion.
The reporting rate of clinical phases to ClinicalTrials.gov and PubMed was significantly lower for Phase II and IV trials when phase III trials were considered reference. Phase III trials are high because the efficacy of the drug has been confirmed to some extent at an earlier phase, and thus, the result at the subsequent regulatory application is essential. Biases that appear positive may also be present in the reporting and can appear at any phase. 12
Conversely, the reason for the low reporting rate of Phase II trials may be partly because the efficacy and safety are not yet sufficiently clear, and researchers tend to hesitate to report “unfavorable” results. A similar negative bias may occur for phase IV trials. Goldacre et al. 5 reported a similar trend of significantly higher reporting rates for phase III and lower reporting rates for phases II and IV using crude ORs, although the trend was not statistically significant using adjusted ORs. Remarkably, similar trends were obtained, despite the different enrollment databases and scope of data collection.
Regarding the result reporting, findings of lower reporting rates for SMALL and AC are consistent with the previous report by Zwierzyna et al. 4 Notably, Goldacre et al., 5 who used the EUCTR as the registry database, also reported a trend of higher result reporting rates from big industries and lower from universities (ACs). DeVito et al. 13 showed that industry groups were more likely to comply with regulations if sponsors who initiated the development were industry groups compared to nonindustry or non-U.S. government sponsors.
Conversely, Goldacre et al. 5 showed that nonmajor sponsors are more likely to be unaware of the reporting obligations or may lack the administrative procedures to point out violations and help researchers comply with the regulations. Mayo-Wilson et al. 14 noted that, while big companies work to improve result reporting rates by assigning dedicated personnel to internal administrative departments for procedures such as registration and reporting, implementing such measures is not financially achievable for most nonmajor pharmaceutical institutions. These factors imply that clinical trial sponsors could affect the reporting of clinical trial results.
Finally, multivariate analysis of modalities showed that GCT contributed as one of the factors that could reduce the rate of reporting trial results to ClinicalTrials.gov. The decrement curve of the unreported result rate over time by the Kaplan–Meier method (Fig. 3) significantly illustrates the pronounced influence of the modality and dispels the concern that only GCTs might have a shorter duration after primary completion compared to LMWC and BLG. Overall, our multivariate analysis showed that STR as a disease and GCT as a modality were contributing factors to the lower reporting rate to ClinicalTrials.gov. The answer to our initial question was considered to be an additive effect of STR as a disease and GCT as a modality. In STR, the reporting rate to ClinicalTrials.gov was low, but was relatively high to PubMed (significant only in crude ORs), indicating that result disclosure in a journal publication was more preferred.
Furthermore, the rate of reporting results in PubMed for GCT was not different from that for control LMWC, indicating that reporting results of GCT to ClinicalTrials.gov tended not to be favored, whereas journal publication was more preferred. In general, trial result reporting to ClinicalTrials.gov is considered to comply with higher standards and be more complete than publication in journals.15,16 This may raise another ethical issue if more investigators avoid reporting results to ClinicalTrials.gov in favor of publishing results in journals, which is an easier option. If negative safety and efficacy issues occur during clinical trials and those are not disclosed, researchers may carry out unnecessarily duplicate human clinical trials in the future, which may raise another ethical issue. Therefore, we believe that some systematic approach is needed to further encourage reporting trial results not only to ClinicalTrials.gov but also to global registries.
The areas for improvement that emerged from this analysis are the poor reporting of GCTs to ClinicalTrials.gov and the poor reporting from SMALL and AC. Focusing on these improvements, academia would need to begin by recognizing the contributions of researchers who posted trial results to the Clinical Trials Registry, as one of the recommendations put forward by Liu et al. 17 This could be taken a step further, and recognizing the contribution of reporting results in a clinical trial registry as an achievement equivalent to publishing an article would encourage a public funding agency, such as Japan Agency for Medical Research and Development (AMED), to evaluate it as an achievement equivalent to a researcher's publication and use it as an indicator to influence the subsequent research funding selection. This is used as an indicator that influences the selection of subsequent research funds.
Such a policy could be used to raise the reporting rate. In this study, from the perspective of mid-level regenerative medicine researchers who are not particularly experts, we applied solely ClinicalTrials.gov as a registry and searched for four neurological diseases relying on the ClinicalTrials.gov thesaurus followed by searching PubMed for article reports as we used a manual method of searching by NCT number and manually classifying the modalities to be examined. We are aware of the possibility of underestimates in journal publications due to this research method; however, we believe our pilot research remains significant.
Preliminarily, we attempted to find more journal articles corresponding to trials with unknown publication of results, using acronyms of clinical trials obtained from ClinicalTrials.gov database in stead of NCT numbers. Resultant newly identified 52 clinical trials were merged to the original data and we conducted another multivariate analysis as a sensitivity analysis. As a result, we observed slightly different findings from the original findings in completion year (2015 and 2016 of PubMed, and 2006 and 2016 of total disclosure); however, we observed the similar findings with the original in disease area, status, phase, sponsor, and treatment modality as our main subject of this pilot study (Supplementary Tables S4–S6). Although it is challenging and have high expectations to apply practical use of new modalities such as GCT, we need to be cautious about the risks ahead.
Disclosure of trial results could be an indicator of keeping transparency and safety issues; therefore, those involved in research should clarify the status of trial result reporting to meet their ethical obligations. If the disclosure rate of trial results remains poor, discussion should be simulated to solve and determine the cause and take effective countermeasures. In particular, the field of hematologic oncology, which has rapidly advanced in practical usage in the past decade, evolves on a different scale than the field of neurological diseases; therefore, simple analogies cannot be made based on this study. A separate analysis will be needed. To address these issues, we would further expand the scope of our study to tackle the result reporting issues by disease areas and modalities.
Footnotes
Acknowledgment
The authors express their appreciation to Ms Midori Maehata for excellent assistance in this research work.
Authors' Contributions
T.N., H.O., and A.M. conceived the work. T.N., S.H., T.A., and H.O. processed and analyzed the data. T.N., S.H., T.A., H.O., and A.M. wrote the article. All authors contributed to article editing.
Data Availability
Data that support the study findings are available from the corresponding author upon reasonable request.
Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported by the Highway Program for Realization of Regenerative Medicine of The Japan Agency for Medical Research and Development (AMED) under the Grant Number JP22bm0904001.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.