
Abstract
Bone defects because of age, trauma, and surgery, which are exacerbated by medication side effects and common diseases such as osteoporosis, diabetes, and rheumatoid arthritis, are a problem of epidemic scale. The present clinical standard for treating these defects includes autografts and allografts. Although both treatments can promote robust regenerative outcomes, they fail to strike a desirable balance of availability, side effect profile, consistent regenerative efficacy, and affordability. This difficulty has contributed to the rise of bone tissue engineering (BTE) as a potential avenue through which enhanced bone regeneration could be delivered. BTE is founded upon a paradigm of using biomaterials, bioactive factors, osteoblast lineage cells (ObLCs), and vascularization to cue deficient bone tissue into a state of regeneration. Despite promising preclinical results, BTE has had modest success in being translated into the clinical setting. One barrier has been the simplicity of its paradigm relative to the complexity of biological bone. Therefore, this paradigm must be critically examined and expanded to better account for this complexity. One potential avenue for this is a more detailed consideration of osteoclast lineage cells (OcLCs). Although these cells ostensibly oppose ObLCs and bone regeneration through their resorptive functions, a myriad of investigations have shed light on their potential to influence bone equilibrium in more complex ways through their interactions with both ObLCs and bone matrix. Most BTE research has not systematically evaluated their influence. Yet contrary to expectations associated with the paradigm, a selection of BTE investigations has demonstrated that this influence can enhance bone regeneration in certain contexts. In addition, much work has elucidated the role of many controllable scaffold parameters in both inhibiting and stimulating the activity of OcLCs in parallel to bone regeneration. Therefore, this review aims to detail and explore the implications of OcLCs in BTE and how they can be leveraged to improve upon the existing BTE paradigm.
Impact Statement
This review first examines the molecular groundwork of the influence of osteoclast lineage cells on bone regeneration and then transitions into empirical investigations on this influence in bone tissue engineering (BTE). The prevalence of bone loss coupled with inadequacies in the present standard of care make effective bone regeneration an enormous unmet need. BTE has had modest translational success up to the present, with a significant limitation being that it has a simple paradigm relative to the complexity of bone biology. This review intends to help BTE researchers expand this paradigm and ultimately expedite the advancement of this field into clinical applications.
Introduction
Bone defects because of age, trauma, and surgery, which are exacerbated by medication side effects and common diseases, such as osteoporosis, diabetes, and rheumatoid arthritis, are highly prevalent. The present clinical standard for treating bone defects includes autografts and allografts, and these treatments are faced with numerous limitations. 1 Autograft describes bone harvested from the recipient, while allograft describes bone harvested from a donor, with both intending to support therapeutic bone growth. While both options have distinct advantages, they also face considerable drawbacks. Autografts are highly effective because they promote osteoinduction and osteoconduction without the risk of immunological rejection. 2 However, they require a secondary harvesting procedure with a limited amount of bone that can safely be extracted. 3 They are also a costly treatment with many potential complications, including deformity, infection, and inflammation. 4 Some of these difficulties can be circumvented with the use of allografts. However, allografts have different drawbacks, including risk for immunological rejection, pathogen transmission, and dampened osteoinduction. 5 They are also costly because of low availability. 6 The two main treatments for bone defects ultimately fail to strike a desirable balance of availability, side effect profile, regenerative efficacy, and affordability. Therefore, bone tissue engineering (BTE) has become an attractive alternative.
BTE originated in the mid-1980s and has grown exponentially since. 7 It strives to use externally fabricated regenerative implants that avoid the aforementioned drawbacks associated with grafting procedures. 8 A paradigm has developed that describes how BTE researchers have widely approached this goal. There are four variables that are perceived as the main tools in the BTE toolbox: (1) biomaterials, (2) osteoblast lineage cells (ObLCs), (3) bioactive factors, and (4) vascularization. 8 These variables can theoretically work harmoniously within a defect site to stimulate net bone formation. However, in practice, few BTE approaches have found clinical success thus far. 9 A significant limitation that has been identified is the simplicity of this paradigm relative to the complexity of biological bone.
Osteoclast lineage cells (OcLCs), while ostensibly opposed to ObLCs through their major resorptive functions, are one of the most vital components of bone remodeling through their largely osteogenic signaling properties. 10 Contrary to the expectations associated with the BTE paradigm, not only has inhibition of OcLCs led to improved regeneration, but inclusion and stimulation have as well in certain contexts. Yet most BTE research has not systematically considered their influence up to the present. Therefore, this review aims to critically explore how consideration of OcLCs can be added to the current BTE paradigm for enhanced bone regeneration outcomes. It will start by establishing the molecular foundation of why this addition is appropriate. It will then transition into empirical evidence of how this addition has shown promise. This leads into the proceeding organization and discussion of existing BTE strategies that inhibit or stimulate OcLCs. While other investigators have thoroughly characterized the influence of OcLCs, the extensive literature search performed here has led to the conclusion that no other work mirrors the aim of this review. For instance, while Tsukasaki et al. characterized osteoclast biology in great amounts of detail, no emphasis was placed on the systematic modulation of their activity for BTE applications. 11 Similarly, Yahara et al. explored osteoclast origins and crosstalk with surrounding cells but did not extend this discussion into practical applications in BTE. 12 Interestingly, Kim et al. specifically detailed the crosstalk between osteoblasts and osteoclasts as it relates to bone homeostasis. 10 While relevant as a theoretical foundation, this does not venture into the territory of leveraging this communication for BTE applications. Altogether, this review aims to build on the foundations laid by pre-existing work to elucidate the potential role of OcLCs in the future of BTE.
Methods
The authors used PubMed to gather sources. To this end, six main searches were performed and included combinations of the following keywords: 3D bioprinting, bioprinting, coculture, extrusion, hybrid print, hydrogel, osteoblast, osteoclast, and tissue engineering. These searches were last performed on January 31, 2024. This generated 292 results that the authors selected from and categorized based on uniqueness, appropriateness to different parts of a preliminary outline, and overall relevance. Duplicates and works deemed irrelevant were eliminated. Furthermore, to uncover clinical aspects of the topic at hand, a search for clinical trials was performed on 6/6/2024 with the following keywords: bone tissue engineering and osteoclast. This generated four results and one was deemed relevant. All other citations were known to the authors or found in other literature reviews.
The Biology of Crosstalk and Relevance of OcLCs to BTE
The cells that have received the most attention within the present BTE paradigm are ObLCs and vascular cells. Many groups have thoroughly investigated how their activity can be stimulated to promote net bone formation. 13 Yet, the dynamic equilibrium that characterizes biological bone is remarkably complex, with myriad other essential cell types that contribute. One of the most noteworthy are OcLCs, known for their most immediately apparent function of resorbing bone. 10 However, several mechanisms exist where OcLCs both stimulate and inhibit ObLCs, and vice versa (Table 1). This enables a more complex influence of both cell types on bone equilibrium than their basic functions would imply. 14 First, many examples of communication from ObLCs to OcLCs exist, and these can be free or membrane-bound signals. Examples of free signals include stimulatory signals such as macrophage colony-stimulating factor,15–16 receptor activator of nuclear factor-kappa B ligand (RANKL),17–18 and WNT5A,19–20 as well as inhibitory signals such as osteoprotegerin (OPG)21–22 and WNT16. 23 Examples of membrane-bound signals include FAS ligand (FASL), 24 and semaphorin 3A,25–26 with both being inhibitory. OcLCs also send corresponding signals to ObLCs. Examples of free signals include stimulatory signals such as sphingosine 1 phosphate, 27 collagen triple helix repeat containing 1, 28 complement component 3 (C3), 29 WNT10B, 30 and bone morphogenetic protein 6 (BMP6), 31 as well as inhibitory signals like semaphorin 4D.32–33 An example of a membrane-bound signal is ephrin B2, 34 which is stimulatory. Lastly, osteoclastic resorption releases bioactive molecules from the bone matrix. Transforming growth factor β135–36 and insulin-like growth factor 137–38 both stimulate osteoblastogenesis of mesenchymal stem cells (MSCs) through this mechanism. The above crosstalk is far from a central focus of the current BTE paradigm. Yet its profound influence on bone remodeling establishes the molecular basis of OcLCs as an important consideration.
MSCs, mesenchymal stem cells.
Contrary to expectations associated with the ObLC-focused paradigm, the possibility for OcLCs to positively influence BTE outcomes has been empirically supported. Hayden et al. used osteoblasts, osteoclasts, or a coculture of the two on 8% silk films and evaluated for bone regeneration. 39 After an 8, 16, 24, and 32-week culture period, the coculture displayed greater indicators of bone formation than osteoblasts alone. Alternatively, Kay Sinclair et al. set out to investigate the ability of OcLCs to stimulate osteoblastic differentiation through the use of an analogous coculture construct involving RANKL-containing media, osteoclast precursor cells (RAW 264.7), and MSCs. 40 MSCs were added alone, simultaneously with RAW264.7 cells, or with RAW264.7 cells added 4 days before, to a clinically available β-tricalcium phosphate (β-TCP) ceramic bone graft substitute, chronOS (Synthes), and observed for 17 days. MSC proliferation and expression of markers for late-stage osteoblastogenesis were observed to be positively influenced by osteoclast presence. Similarly, Ruggiu et al. placed either osteoblasts cocultured with osteoclasts or osteoblasts alone, onto silicon-TCP-comprised Skelite™ bone graft scaffolds to create 3D cocultures. 41 After 8 weeks, both matrix deposition and scaffold biodegradation were enhanced in the coculture condition. Lastly, Dong et al. used a decalcified bone matrix scaffold seeded with a coculture of MSCs and osteoclast precursors, MSCs alone, or a cell-free control, and implanted into a femoral defect on rats. 42 They observed that the coculture demonstrated the greatest osteogenic potential in vivo and in vitro and experiments demonstrated that factors released from preosteoclasts were associated with increased MSC mobilization and osteoblastogenesis. Taken together, this literature indicates that the presence of OcLCs is associated with enhanced bone regeneration in certain BTE contexts. In tandem with the above communication mechanisms, this further establishes a need to expand beyond an ObLC-focused paradigm.
Another means through which resorbing cells can influence regeneration is resorption itself. Domaschke et al. demonstrated a mechanism of this nature within mineralized 30% collagen I and 70% hydroxyapatite (HA) scaffolds. 43 Osteoclasts successfully resorbed the scaffold, enabling new matrix deposition by osteoblasts. Scaffolds can also be designed to be highly specific to osteoclastic resorption. Hsu et al. capitalized on this strategy by developing poly(ethylene glycol) (PEG) diacrylate backbone hydrogels crosslinked by a peptide specific to cathepsin K cleavage. 44 They found that these hydrogels could not be degraded by plasmin, control buffers, or osteoblasts, but could be degraded by osteoclasts upon attachment. This could enable the release of regenerative compounds from these hydrogels. Lastly, Midha et al. fabricated a 70 mol% SiO2 and 30 mol% CaO bioactive glass scaffold in a coculture of macrophages and preosteoblasts. 45 The macrophages differentiated into mature osteoclasts, whereas the preosteoblasts took part in new matrix deposition on the biomaterial surface, which was enhanced by the release of osteogenic silica and calcium ions from the resorbed matrix. Overall, these works demonstrate how BTE constructs can be engineered to capitalize on osteoclastic resorption for bone regeneration. Moreover, they serve as a powerful example of how a paradigm focused on bone deposition can potentially be expanded for enhanced regenerative outcomes.
Ways to Modulate OcLC Activity in a BTE Context
Section 3 established a molecular and empirical foundation of how the consideration of OcLCs has the potential to improve BTE outcomes. 14 To build upon this, due to their prominent bidirectional role and osteogenic capacity in bone remodeling, modulating their activity may provide therapeutic strategies for treating different bone defects. As such, various soluble, environmental, and cellular cues have already been examined for successfully modulating OcLC behavior within a BTE context. The present BTE paradigm focuses on stimulation of ObLCs to maximize their bone deposition functions with comparatively little systematic evaluation of OcLCs. Contrary to expectations associated with this paradigm, both inhibition and stimulation of OcLCs have shown promise in promoting bone regeneration. These seemingly conflicting results create an unmet need for a thorough detailing of the circumstances surrounding OcLC inhibition and stimulation in a BTE context. Therefore, this section intends to organize and discuss these various inhibitory and stimulatory strategies to inform and expedite the development of regenerative technologies that aim to enhance the treatment of bone defects.
Inhibitory strategies
The present BTE paradigm is one of stimulating ObLCs to promote new bone deposition and ultimately promote bone regeneration. Bone resorption, the primary function of OcLCs, is the functional opposite of this and has therefore been targeted through OcLC inhibition. This approach has shown promise across different strategies, though with an interesting concentration of efficacy in the context of pharmaceutical components. This first subsection intends to detail this more paradigm-aligned approach to OcLC modulation in BTE.
Inhibitory soluble factors
BTE constructs can be loaded with soluble factors that can be released to surrounding tissue over a controllable time scale, where the released factor can focus its effect at the implantation site. Numerous studies have shown the possibility of inhibiting OcLCs with specifically drug-laden BTE constructs (Table 2). 46 Many of these drugs are indicated for osteoporosis and act to promote bone formation by inhibiting OcLCs. 47 For example, bisphosphonates such as alendronate are commonly prescribed medications for osteoporosis that inhibit osteoclastogenesis. 48 Zeng et al. capitalized on this by creating graphene oxide-related hydrogels and incorporating them into a Type 1 collagen sponge loaded with alendronate. 49 In vivo studies revealed that alendronate-containing sponges implanted into bony defects in a rat model were associated with a decreased osteoclast number and suppression of systemic bone loss as compared with alendronate-free sponges. Alternatively, Posadowska et al. developed an injectable system of alendronate-loaded nanoparticles separately suspended in a gellan gum (GG) hydrogel encapsulated in poly(lactide-coglycolide) (PLGA). 50 This system was associated with suppressed osteoclastogenesis of RAW264.7 cells, even despite RANKL administration. Yet they underwent robust osteoclastogenesis without the system. It is also noteworthy that this system was cytocompatible with osteoblast-like cells, suggesting potential for regenerative applications. Another notable bisphosphonate is clodronate. Hayden et al. compared the effect of alendronate to clodronate on osteoclasts, osteoblasts, and a coculture of the two over 12 weeks on a silk-HA film. 51 Both drugs could induce beyond a 90% reduction in osteoclast metabolic activity by the fifth day of culture. However, high doses of clodronate were observed to preserve the metabolic activity of osteoblasts when compared with alendronate, indicating potential utility in bone regeneration. Alongside well characterized effects, these works establish bisphosphonates as a potentially potent means of promoting bone regeneration partly through OcLC inhibition.52–53
Bold horizontal border separates components that inhibit OcLCs from components that stimulate OcLCs. BMSCs, bone marrow mesenchymal stem cells; GG, MSCs, mesenchymal stem cells; PCL, polycaprolactone; PEG, poly(ethylene glycol); PLGA, poly(lactide-coglycolide).
Other drugs outside the bisphosphonate class have been used to modulate OcLCs. Zhang et al. demonstrated a synergistic effect of resveratrol, a polyphenolic photoalexin derived from various plants, and strontium (Sr) ranelate, a medication for osteoporosis, on bone regeneration. 54 This involved 3D printing of scaffolds consisting of polycaprolactone (PCL), β-TCP, and a hydrogel-based bioink. The scaffolds were loaded with resveratrol, Sr ranelate, or both and evaluated for their influence on osteoclast activity. The group observed that the release of both components and Sr ranelate only decreased osteoclast size and tartrate-resistant acid phosphatase (TRAP) activity when compared with resveratrol only and a scaffold only control. They also observed that this dual delivery was associated with promotion of osteoblastogenesis and in vivo bone formation beyond scaffold only and defect only controls. Drugs with applications outside bone diseases have also been used. Petit et al. explored using thermosensitive chitosan hydrogels functionalized with D-α-tocopherol polyethylene glycol succinate-based nanoemulsions. 55 These hydrogels contained atorvastatin or lovastatin, common statins used to prevent cardiovascular disease and hyperlipidemia, to modulate bone cells pleiotropically. An in vitro experiment involved infection of TERT-2 OKF-6 human oral epithelial cells and human oral fibroblasts with Porphyromonas gingivalis to assess for inflammatory and osteoclastic markers. They observed that treatment with atorvastatin-loaded or lovastatin-loaded nanoemulsions led to reduced expression of RANKL as compared with the absence of statins. They also observed the nanoemulsions to be associated with increased expression of bone sialoprotein 2 (BSP2) in osteoblasts beyond untreated cells and systemic statin administration. Furthermore, in vivo experiments revealed that treatment of calvarial bone defects with these hydrogels was associated with increases in new bone formation as compared with untreated and statin-free hydrogel controls, as well as systemic statin administration. Interestingly, Pan et al. used cabozantinib, a cancer drug, in a hyaluronic acid-based hydrogel. 56 They assessed it in preosteoblasts and human bone-derived 786-O (Bo-786) renal cell carcinoma cell cultures and in a mouse model of renal cell carcinoma femoral bone metastasis. Cabozantinib led to a reduction in TRAP-positive multinuclear cells, hallmark features of mature osteoclasts, that formed in vitro, in comparison with a cabozantinib-free condition. It also was associated with enhanced preosteoblast differentiation despite the presence of Bo-786 cells, as evidenced by increases in alkaline phosphatase and osteocalcin expression beyond controls. Furthermore, the in vivo experiment demonstrated a reduced osteoclast number, increased osteoblast number, and increased bone volume in response to the hydrogel system when compared with controls. Gallium nitrate is another oncological drug used to treat hypercalcemia secondary to cancer through osteoclast inhibition. Ghanta et al. evaluated the ability of gallium acetylacetone (GaAcAc) released from methylcellulose-based hydrogels to suppress osteoclastogenesis of RAW264.7 or hematopoietic stem cells. 57 They observed greater efficacy of these hydrogels as compared with the GaAcAc solution in reducing the degree of bone resorption observed in ex vivo experiments. These findings further corroborate the observation that drugs investigated up to the present have largely inhibitory effects on OcLCs. However, further work is needed to verify the consistency of these findings, and more drugs ought to be explored.
Various proteins and peptides have been observed to strongly influence the fate of OcLCs, as well as the broader bone remodeling system. 58 This has been leveraged in BTE constructs with modulatory potential. BMP-2, a well-known osteogenic factor, has shown pro-osteoclastogenic and regenerative properties in multiple studies. However, excessive use of BMP-2 can induce harmful side effects. 59 To address this, Arai et al. evaluated the supplemental local application of OP3-4 peptide, an analog of OPG, to promote bone formation in a murine tooth extraction model with a very low dose of BMP-2. 60 A gelatin hydrogel-containing BMP-2 with or without OP3-4 peptide was implanted within the socket of a mandibular incisor of mice. New bone formation was most enhanced, and osteoclast numbers were lowered in the socket loaded with BMP-2 and OP3-4. Similarly, Wang et al. loaded a thermosensitive hydrogel with both BMP-2 and OPG to be evaluated with bone marrow MSCs (BMSCs) in vitro and in a rabbit model. 61 They observed that hydrogels that included OPG could reduce the expression of RANKL beyond those without it. They also observed that the combination of both proteins promoted osteoblastogenesis and new bone growth beyond either protein alone or controls. Altogether, while findings discussed in 4.2.1 display a pro-osteoclast and regenerative effect of BMP-2, these investigations here suggest that if bone regeneration is augmented with OPG or OP3-4, the pro-osteoclast property of BMP-2 may be overridden. Nevertheless, OP3-4 has also been investigated for BTE in isolation. Luo et al. incorporated it into gelatin methacrylate and evaluated it in a rat model. 62 They similarly observed significantly reduced osteoclast numbers and increased expression of osteogenic proteins with OP3-4 when compared with a pure gelatin methacrylate control. Lastly, certain synthetic peptides outside the typical discussion of bone biology have also been explored. Hu et al. explored using chitosan methacryloyl hydrogels loaded with human beta-defensin 1 short motif Pep-B in periodontal pockets. 63 They observed that injection of this peptide-containing hydrogel significantly reduced osteoclast formation and alveolar bone loss. This further establishes the premise that certain proteins and peptides have demonstrated efficacy in inhibiting OcLCs as a mechanism of bone regeneration. However, more work is needed on what additional proteins and peptides can work through this mechanism outside of OPG and OP3-4 and how this can be applied in BTE.
Inhibitory environmental factors
Substantial work has revealed the potential of environmental factors to inhibit OcLCs in BTE, including ceramics, scaffold properties, plant-derived components, and nano-scale components (Table 3). Concerning ceramics, the bone matrix consists of organic components (collagen type I, proteoglycans, and glycoproteins) and inorganic components primarily in the form of HA. 64 The latter has been extensively investigated for OcLC inhibition. Although studies discussed in 4.2.2 suggest an almost exclusively pro-osteoclast effect of HA, select investigators have observed contrasting results. Hadi et al. explored the use of carbonated HA-chitosan (CHA-CS) hydrogel derived from blood cockle shells in orthodontic relapse within a rat model. 65 They observed a significant decrease in osteoclasts, increase in osteoblasts, and reduced relapse distance with CHA-CS when compared with controls. Furthermore, as discussed in 4.2.2, calcium-based ceramics in general exhibit largely pro-osteoclast and regenerative properties. However, certain noncalcium-based ceramic components have demonstrated the inverse effect on osteoclasts in direct comparisons with calcium-based ceramic components. Zhang et al. investigated the use of alginate microgels cross-linked with either Ca2+ or Sr2+ both in vitro and in a rat model. 66 The Ca2+ condition exhibited significantly greater markers of bone regeneration in vitro, which the authors attributed to the association of Sr2+ with osteoclast inhibition. However, it should be noted that bone healing within the rat model was comparable between the two conditions. Noncalcium-based ceramics have also been evaluated in association with calcium-based ceramics. Panzavolta et al. prepared gelatin scaffolds with Sr substituted HA, which were associated with inhibited osteoclastogenesis and stimulation of osteoblasts beyond pure-HA scaffolds. 67 While ceramics relevant to BTE tend to be osteoclastogenic, the former studies demonstrate interesting examples to the contrary. Further work is needed on alternative ways through which noncalcium-based ceramics like those involving strontium can support bone regeneration through this avenue. In addition, the unusual results with calcium-based ceramics seen with Hadi et al. warrant future exploration of the circumstances in which those results are probable and how this can be leveraged.
Bold horizontal border separates components that inhibit OcLCs from components that stimulate OcLCs. BMMs, bone marrow-derived macrophage; BMSCs, bone marrow mesenchymal stem cells; hiPSCs, MSCs, mesenchymal stem cell; OcLCs, osteoclast lineage cells; PCL, polycaprolactone; PLLA, poly(L-lactic acid; PLGA, poly(lactide-coglycolide).
Select investigators have explored the manipulation of scaffold properties. For instance, Halai et al. explored micropatterning of a ceramic implant material in an MSC and bone marrow-derived hematopoietic cell coculture. 68 Thirty micrometer diameter pits were associated with enhanced osteogenesis, reduced osteoclastogenesis, and a lower osteoclastic cell number than planar controls. This lends important insights into scaffold surface design considerations that ought to be further explored as a variable distinct from composition. Some groups have also explored plant-derived compounds, such as Bose et al., who investigated the effect of garlic extract within human MSC-monocyte cocultures seeded on calcium phosphate scaffolds. 69 The extract was observed to reduce osteoclast resorption potential after 21 days and to increase the osteoblastic markers of osteocalcin by 1.6-fold and alkaline phosphatase by threefold after 14 days as compared with the control. It was also observed to enhance collagen formation within a rat model. Interestingly, Yao et al. examined the effect of traditional Chinese medicines, including Eucommia Oliv., Dipsacus asper Wall., Loranthus parasiticus Merr., Achyranthes bidentata Bl., and Cuscuta chinensis Lam. 70 They incorporated them into gelatin and TCP-based composites that were placed in the parietal bone of neonatal rat calvarias organs. They observed that C. chinensis Lam. was associated with stimulation of osteoblastogenesis and decreased osteoclastogenesis when compared with Chinese medicine-free controls. While these works show a compelling outlook for plant-derived compounds as OcLC inhibitors in BTE, future studies should focus on further categorizing them in a way that enables better functional predictions.
A few groups have explored nano-scale inhibitory components. Shan et al. developed a hyaluronic acid-based hydrogel loaded with tobacco mosaic virus (TMV) nanoparticles and assessed their influence on osteoclastogenesis. 71 These TMVs were associated with reduced expression of osteoclastogenic genes when compared with a TMV-free control in vitro. They were also associated with enhanced bone mass when compared with pure hydrogel and a treatment-free control within a mouse tibial defect model. In the same study, this group also evaluated an RGD1 mutant variation TMV that displayed even greater potential in osteoclastogenesis inhibition. Moreover, Byun et al. infused tannic acid-mineral nanoparticles into a gelatin-based cryogel to evaluate their bone-forming potential. 72 After seeding RAW264.7 cells, nanoparticle-containing gels displayed lower levels of osteoclastogenic markers than controls. Furthermore, in vivo studies demonstrated that these gels were associated with new bone of higher quantity and quality than controls. Lastly, Li et al. evaluated zinc oxide and minocycline serum albumin nanoparticles for treating peri-implantitis. 73 Compared with untreated and pure minocycline controls, hydrogels containing zinc oxide were observed to reduce osteoclast number and maintain supporting bone tissue within a murine disease model. This helps establish nano-scale components as an effective way to inhibit OcLCs in BTE, but more work is needed in characterizing their varying effects.
Inhibitory cellular factors
Another approach to OcLC inhibition is capitalizing on cell–cell interactions, such as signaling from MSCs (Table 4). 74 For instance, Tcacencu et al. implanted a MSC-laden hydrogel into a bony defect within the mandible of a rat model and observed significant increases in bone volume at 1 week and reduced osteoclast number at 1 and 4 weeks as compared with cell-free controls. 75 These results indicate MSCs may have efficacy in supporting bone regeneration through OcLC inhibition, but further investigation is needed to determine the consistency in which this holds true across different contexts. Nonbone cells have also demonstrated inhibitory potential. To investigate the effect of adipocytes, Han et al. cotransplanted adipocytes and osteoblasts into a mouse model and observed that adipocytes could promote enhanced osteogenesis and reduced osteoclast density as opposed to osteoblasts alone. 76 Furthermore, cellular components and secretions have also been investigated. Zheng et al. developed an injectable methylcellulose hydrogel-containing osteocyte lysate. 77 The presence of osteocyte lysate was associated with a reduction in TRAP-positive cells within coculture and mouse defect models when compared with controls. It was also associated with significant elevation in new bone formation within the defect models relative to controls. Alternatively, Liu et al. incorporated BMSC-derived extracellular vesicles into a gelatin-based hydrogel to treat periodontitis in rats. 78 This system was associated with less TRAP-positive cells and less overall bone loss than a vesicle-free PBS-hydrogel control within the disease model. These findings suggest that future work is needed on the ways through which different cellular factors influence OcLCs in relation to regenerative outcomes. This could enable the isolation and leveraging of specific cellular components for BTE.
Bold horizontal border separates components that inhibit OcLCs from components that stimulate OcLCs. BMSCs, bone marrow mesenchymal stem cells; CAPCs, cultured autogenous periosteal cells; MSCs, mesenchymal stem cells; OcLCs, osteoclast lineage cells.
Stimulatory strategies
Contrary to expectations associated with the BTE paradigm, many investigations have uncovered situations in which stimulation of OcLCs has been associated with effective bone regeneration. Intriguingly, this is particularly true with incidental and naturally occurring strategies that were not designed for this application. This second subsection intends to amalgamate this exciting assortment of literature to help expedite and advance the development of new BTE technologies.
Stimulatory soluble factors
Although pharmaceutical-based BTE strategies chiefly exhibit antiosteoclastic properties, there do exist interesting counterexamples (Table 2). For instance, a more complex effect of bisphosphonates on OcLC differentiation has been observed. Li et al. demonstrated this by developing hyaluronic acid-based hydrogels loaded with a bisphosphonate called pamidronic acid. 79 The authors’ in vitro studies demonstrated that these hydrogels could support early differentiation of macrophages into preosteoclasts while inhibiting late-stage differentiation into mature osteoclasts as compared with a bisphosphonate-free control. The in vivo studies demonstrated that these hydrogels could enhance bone regeneration compared with both a bisphosphonate-free and a hydrogel-free control. This reveals how bisphosphonates applied in BTE can exert different effects at different stages of OcLC differentiation despite consistent inhibition of osteoclastogenesis. Therefore, an important area for future work will be on the potentially complex ways through which different drugs influence OcLCs within a BTE context.
As discussed in 4.1.1, BMP-2 has shown pro-osteoclastogenic and regenerative properties in multiple BTE studies. Ning et al. developed an injectable composite hydrogel by modifying low-acyl gelatin gum hydrogels with hemicellulose polysaccharide microfibers to treat medication-related osteonecrosis of the jaw (MRONJ). 80 The hydrogel was laden with adipose tissue-derived stem cells and BMP-2 and transplanted into MRONJ sockets of rats. These hydrogels stimulated bone formation and osteoclastogenesis relative to those without BMP-2. Interestingly, Brierly et al. evaluated a star-shaped PEG and maleimide functionalized heparin hydrogel (starPEG-heparin) for delivery of BMP-2 in a rat model of MRONJ. 81 The hydrogel was modified through the functionalization of arginylglycylaspartic acid (RGD) to create starPEG-RGD-heparin hydrogels with BMP-2. The authors observed that hydrogels laden with BMP-2 increased bone formation relative to the absence of BMP-2 and osteoclast number relative to an empty defect. Taken together, these studies show pro-osteoclast and regenerative properties of BMP-2. However, the findings in 4.1.1 demonstrated that the former property can be overridden with additional components like OPG or OP3-4. Therefore, future work ought to uncover the properties and utility of BMP-2 across a greater breadth of BTE contexts.
Multiple groups have also investigated parathyroid hormone (PTH). Yi et al. created a PEG-PCL-PEG (PECE) copolymer hydrogel loaded for continuous PTH (cPTH) or intermittent PTH (iPTH) release and injected it into the midpalatal suture of rats. 82 The cPTH hydrogels were associated with increased RANKL expression and inhibited OPG expression when compared with the control and pure maxillary expansion groups. Furthermore, significant increases in bone volume fraction were observed with both cPTH and iPTH release relative to the pure expansion group. Lu et al. also explored local and continuous application of PTH, as well as PTH-related protein (PTHrP). 83 Temperature-sensitive PECE hydrogels carrying PTH and PTHrP were implanted into the maxillary first molars of rats. They found a significant increase in markers of osteoclastogenesis, including osteoclast number and RANKL to OPG ratio, as well as an increase in expression of osteogenic markers such as osteocalcin, RUNX2 and alkaline phosphatase relative to PTH-free and PTHrP-free controls. Alternatively, Hayden et al. developed a culture system with a silk fibroin sponge or film. 84 MSCs alone or with osteoclasts derived from THP-1, a specific human leukemia monocytic cell line, were seeded along with tethered PTH or glucose-dependent insulinotropic peptide. Overall, the most notable finding was that incorporating PTH increased calcium deposition and remodeling-induced surface roughness under coculture conditions relative to a green florescent protein control. These findings establish PTH as both stimulatory to OcLCs and effective for bone regeneration. However, more work is needed on the differences between cPTH and iPTH as well as how PTH can be applied to BTE.
Stimulatory environmental factors
As discussed in 4.1.2, ceramics have been extensively investigated in BTE research and frequently are associated with both OcLC stimulation and bone regeneration (Table 3). The most common category would be calcium-based ceramics, which have a particular tendency toward this combination of properties when incorporated in a BTE scaffold. For instance, Jeon et al. investigated the differentiation of osteoblasts and osteoclasts from human-induced pluripotent stem cell-derived MSCs and macrophages on HA-coated PLGA/poly(L-lactic acid) (HA–PLGA/PLLA) scaffolds. 85 The group found that the HA-PLGA/PLLA scaffolds with 5.0% HA led to the greatest osteoblast and osteoclast formation in vitro as opposed to 0% or 1% and promoted new bone formation in a murine model. Capitalizing on another calcium-based ceramic, Trojani et al. fabricated a self-hardening Si-hydroxypropylmethylcellulose hydrogel-containing biphasic (40% TCP and 60% HA) calcium phosphate particles. 86 It was laden with MSCs and injected into a mouse model. At 4 and 8 weeks, TRAP-positive osteoclastic cells were observed at the injection site attached to the particles with mineralized bone formed in the surrounding area. However, no evidence of bone formation was demonstrated by cell-free and particle-free controls. Considering other material classes, Ji et al. compared 3D scaffolds comprised of gelatin-methacryloyl, PCL, and β-TCP in vitro and within a critical-sized bone defect of rats. 87 They observed that the β-TCP scaffold specifically could increase osteoclastogenesis and expression of relevant genes. It was also capable of promoting bone regeneration beyond the control condition. These findings support the notion that calcium-based ceramics are largely stimulatory to OcLCs and conducive to bone regeneration. Further investigations should attend to whether this consistently holds true across various BTE contexts.
Calcium-based ceramics have also been explored in comparison with combined and noncalcium-based ceramics. The work of Borciani et al. exemplifies the former. 88 They developed a collagen-based scaffold, hybridized with either HA nanoparticles or strontium-enriched bioactive glasses and evaluated its effect on bone formation in a 2–3-week coculture of osteoblasts and osteoclast precursors. While both scaffolds were observed to promote the development of TRAP-positive cells, the effect was stronger for those containing HA nanoparticles. Both scaffolds could also promote an increase in osteoblast viability over time. In addition, Douglas et al. developed an alkaline phosphatase-loaded GG hydrogel placed in media containing varying ratios of calcium glycerophosphate and magnesium glycerophosphate. 89 The resulting mineralized hydrogels’ influence on osteoblast or osteoclast precursors was then investigated. Samples containing proportionally more calcium glycerophosphate led to more osteoclastogenesis, whereas the more magnesium-dosed counterpart promoted more osteoblast activity. However, both calcium- and magnesium-containing samples underwent effective mineralization. Taken together, these results suggest that calcium-based ceramics are an effective means of stimulating OcLCs in a BTE context when compared with alternative ceramics that have been investigated up to the present.
Noncalcium-based ceramics have also been evaluated in association with calcium-based ceramics in the context of OcLC stimulation. For instance, Kowal et al. developed amorphous multiporous scaffold consisting of 70 mol% SiO2 and 30 mol% CaO laden with osteoblasts and osteoclast precursors. 90 The authors observed the promotion of osteoclastogenesis that was absent in controls alongside support of osteoblastogenesis. In conjunction with Panzavolta et al., this indicates that different combination strategies can impact OcLCs in stimulatory or inhibitory directions. 67 Lastly, some groups have evaluated noncalcium-based ceramics on their own. Laurenti et al. developed 2D magnesium phosphate nanosheets, designed to be an injectable hydrogel system. In in vivo experiments, it was associated with both enhanced osteoclast and osteoblast number, as well as improved bone defect healing, when compared with a control condition. 91 These interesting results establish the need for future investigations on OcLC-stimulating noncalcium-based ceramics applied to BTE.
As discussed in 4.1.2, BTE researchers have explored the manipulation of scaffold properties as a BTE strategy through which OcLCs can be modulated. Interestingly, strategies of this nature have also demonstrated stimulatory effects in certain contexts. Exemplifying this, Jones et al. examined different degradable scaffold biomaterials in single or coculture. 92 They seeded both osteoblasts and osteoclasts in monoculture or coculture onto scaffolds comprised of vapor-stabilized fibroin, methanol-stabilized fibroin, chitosan, or PLLA. Vapor-stabilized fibroin, methanol-stabilized fibroin, and chitosan were associated with increased osteoclast and osteoblast growth in both monoculture and coculture, whereas PLLA was only conducive to increased osteoblast activity. An interesting avenue for future work is whether this holds true with other synthetic polymers. Alternatively, Wang et al. explored the influence of matrix stiffness on OC activity. 93 The authors observed hydrogel stiffness to be positively correlated with osteoclast formation. They also observed that moderate stiffness was conducive to preosteoclast-dependent osteogenesis and bone regeneration. The efforts of these groups illustrate a need for future investigations to thoroughly explore the influence of mechanical and surface properties on OcLCs in relation to BTE.
Certain nano-scale components have also shown potential in stimulating OcLCs and enhancing bone regeneration. For instance, Croes et al. investigated silver (Ag) nanoparticles as part of a chitosan coating for titanium implants designed to prevent implant infection. 94 When incorporated into the tibia of rats, the proinflammatory activity of Ag nanoparticles led to increased osteoclast number and improved peri-implant bone volume relative to a pure chitosan coating. This helps establish nano-scale components as an effective way to stimulate OcLCs in BTE, but more work is needed in characterizing their varying effects.
Stimulatory cellular factors
Myriad investigations have shed light on the potential of cell-based BTE strategies to stimulate OcLCs (Table 4). One area of investigation has been in the use of ObLCs, such as with Zehnder et al., who bioprinted a scaffold with an alginate and gelatin-based hydrogel containing osteoblast and osteoclast progenitors. 95 These scaffolds exhibited greater TRAP activity and matrix protein concentration than scaffolds with osteoclast progenitors alone. Alternatively, Chen et al. directly compared an osteoblast-to-osteocyte transition cell line, IDG-SW3, with MSCs in coculture with osteoclast precursors on a 3D collagen hydrogel. 96 They found that IDG-SW3 was associated with superior osteoclast activation and a higher quality of matrix deposition in vitro. They also observed an enhanced bone healing when IDG-SW3 was incorporated in vivo. Altogether, the former studies lend support to the potentially OcLC-stimulating and regenerative properties of ObLCs. However, further work is needed on the conditions in which this trend applies across different BTE contexts.
Certain alternative cell types have also demonstrated both stimulatory and regenerative potential. Interested in cancer cells, Quent et al. used tissue-engineered bone constructs with a PEG-based hydrogel containing MDA-MB-231, MDA-MB-231BO, and SUM1315 human breast cancer cells. 97 These cells were associated with increased osteoclast number in comparison with the scaffold alone in in vivo studies. In addition, new bone formation occurred around the constructs, indicating compatibility between these cells and bone regeneration. Interestingly, Nagata et al. performed a clinical trial investigating the application of cultured autogenous periosteal cells (CAPCs) in promoting alveolar bone regeneration. 98 These CAPCs were implanted after being mixed with autogeneous bone and platelet-rich plasma across 33 sites in 25 cases. This treatment was associated with effective osteoblast and osteoclast recruitment, as seen by elevations in alkaline phosphatase and TRAP activity within regenerated bone tissue with respect to CAPC-free controls. While this clinical trial stands as one of the only of its kind, these results demonstrate a potentially promising future for OcLC-stimulating cell-based constructs. Overall, these studies reveal an intriguing influence of certain alternative cell types on OcLCs and bone regeneration that warrants more thorough future investigation.
Conclusions
BTE offers a compelling future alternative for bone regeneration. Yet the slow translational results warrant critical examination. OcLCs are inextricably linked to BTE outcomes. The realities of their connection to ObLCs in the process of bone formation, as well as their influence on scaffold properties and empirical results, support this conclusion. These cells can also be inhibited and stimulated with various controllable parameters in parallel to bone regeneration. Therefore, these cells constitute an additional variable on which thorough consideration is warranted in the endeavor of developing bone regeneration technologies. However, knowledge gaps do exist that create a need for future work.
An important question is when inhibition or stimulation of OcLCs is advantageous. While certain patterns could be detected in section 4, future investigators need to thoroughly document the details of both scenarios, including biomaterials, cells, bioactive factors, and microenvironments. This could enhance the ability to predict which modulatory components will yield the best regeneration in different physiological and clinical contexts. Another question is the difference in seeding OcLCs directly onto a scaffold as compared with capitalizing on those in native tissue. Seeding ObLCs directly onto a scaffold has shown merit, 7 yet it is inconclusive whether this would be true for OcLCs. Furthermore, while a criticism of the BTE paradigm is a near-exclusive stimulatory focus on bone forming and vascular cells, OcLCs are not the only relevant additional consideration. Examples include the interface between bone and the nervous system, 99 or cells of the immune system. 100 Lastly, the searches performed for this review revealed a notable dearth of clinical investigations on the consideration of OcLCs in BTE. For the myriad of preclinical investigations within this area to improve patient outcomes, BTE must increasingly consider translational avenues. Overall, future work must build upon the BTE paradigm to account for more of the complexity of bone biology. With this trajectory, BTE could improve upon the present standard of care and help regenerate bone for the millions afflicted with bone defects.
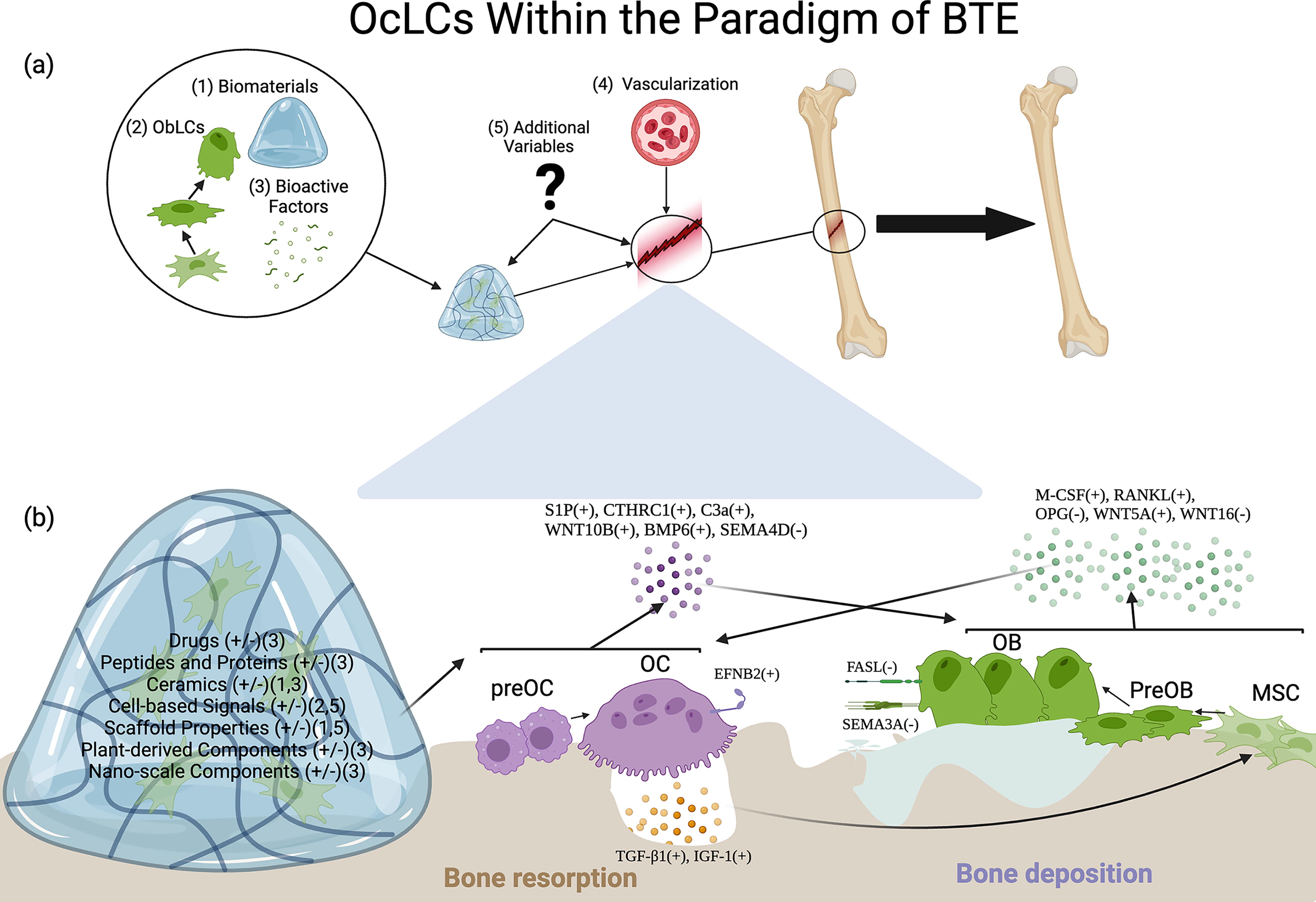
Visual depiction of where consideration of OcLCs fits within the paradigm of BTE.
Footnotes
Acknowledgments
Authors’ Contributions
E.J.D.: Completed initial 2021 literature review and half of 2024 literature review, designed figure, developed tables, wrote abstract, impact statement, and sections 1 through 7; E.J.: Completed half of 2024 literature review, helped write section 1, completed multiple rounds of edits and reviews for all sections; G.K.: Reviewed literature from 2021 literature review and added methodological details to papers cited in sections 3 and 4; R.H.C.: Oversaw concept, offered guidance to authors, completed multiple rounds of edits, and reviews for successive drafts; J.P.F.: Oversaw concept, directed structure, and article review.
Disclosure Statement
No competing financial or personal interests exist for any of the authors.
Funding Information
No funding was received for this article.