
Abstract
Cartilage tissue engineering (CTE) has revolutionized the field of regenerative medicine, offering significant advancements in surgeries such as autologous chondrocyte transplantation. However, despite these advancements, infections associated with cartilage implants remain a persistent challenge, compromising the success of surgeries and patient recovery. To address these challenges, this review provides a comprehensive foundation for researchers interested in addressing infections in CTE. It begins by briefly outlining the major scaffolds currently used in CTE and distinguishing those with antimicrobial properties. Among the antimicrobial scaffolds identified, chitosan and chondroitin sulfate stand out for their promising compatibility and antibacterial properties. The review then explores additives that meet three essential criteria: compatibility with chondrocytes, suitability for use in CTE scaffolds, and antibacterial efficacy. Chitosan, zinc oxide, silver, and copper emerge as leading candidates due to their compatibility with chondrocytes and proven antibacterial capabilities. Importantly, the criteria used in this review were chosen to provide researchers with a practical and reliable starting point for immediate application. However, it is acknowledged that other promising antibacterial modifications such as fabrication processes and additives such as bioactive glass and graphene oxide, which may not fit these criteria, also hold potential for future research and innovation. This review underscores the need for further research and development to enhance infection control measures and improve patient outcomes.
Impact Statement
This review establishes a crucial foundation for in-depth research on infections in cartilage tissue engineering. Suggesting scaffolds with antimicrobial properties offers valuable insights and a significant starting point for researchers in this field.
Keywords
Introduction
Osteoarthritis (OA) causes the breakdown of cartilage in joint tissues, resulting in pain, swelling, and restrictions in joint mobility. 1 In cases of severe OA, surgical interventions may be needed. Various surgical strategies have been proposed over the years to treat defects by facilitating the regeneration of cartilage. Autologous chondrocyte transplantation (ACT) is one of the earliest chondrocyte implantation surgeries that has demonstrated promising outcomes in addressing osteochondral defects. Brittberg et al. described ACT as a two-step surgical process: (1) a biopsy of cartilage tissue is extracted from the patient and enzymatically digested to isolate the cells. These cells are then expanded in a laboratory until they reach a 10-fold increase before (2) a periosteal flap is harvested from the proximal medial tibia and sutured to the cartilage surface at the defect site, with a gap left for cell injection 2 (Fig. 1).
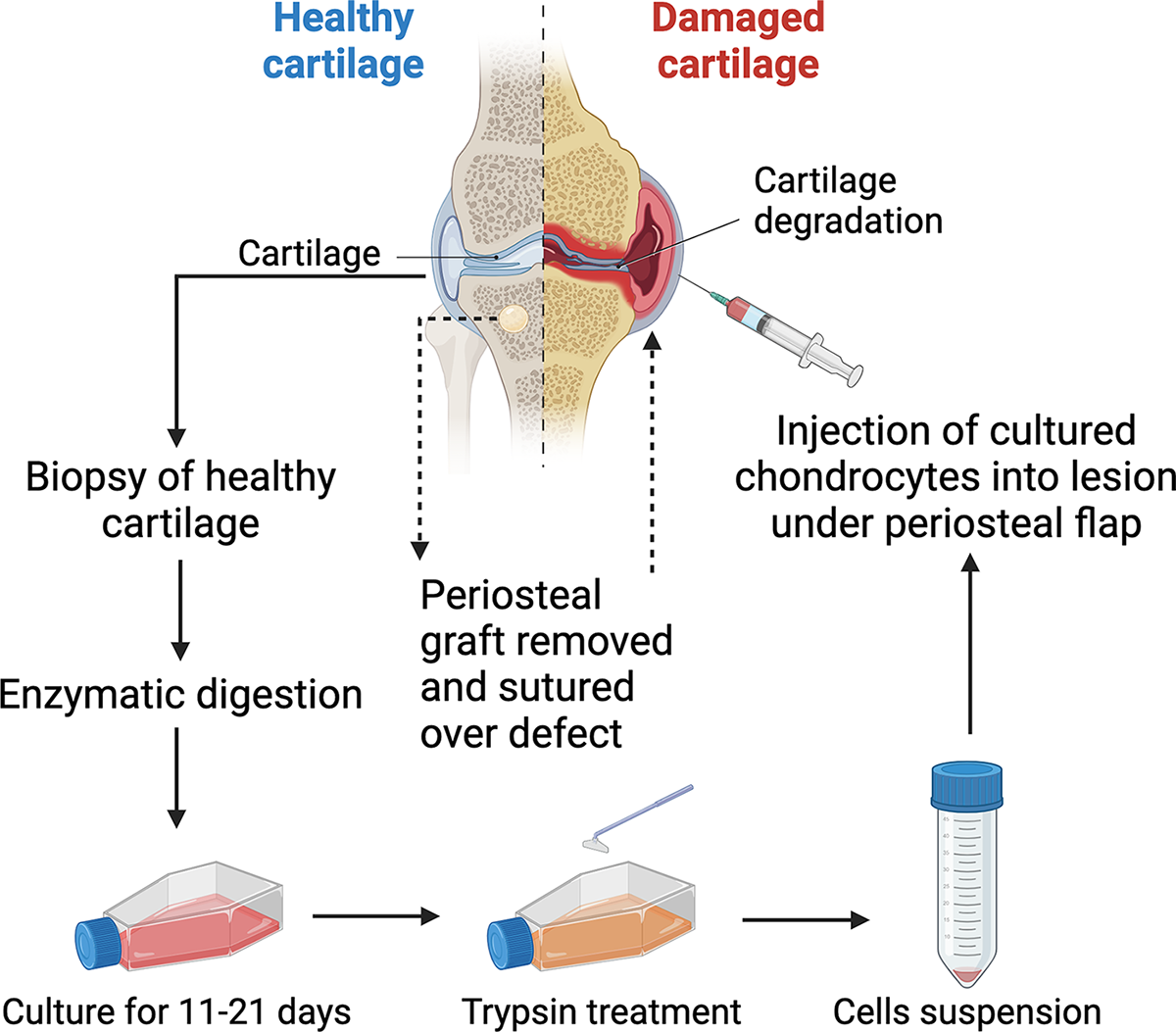
A schematic showing the two-step procedure in ACT. Chondrocytes from a biopsy of healthy cartilage tissue are expanded in the lab before being injected at the defect site under a periosteal flap. (Created with BioRender.com.) ACT, autologous chondrocyte transplantation.
A key limitation of ACT is the need for a second surgery, which has been addressed through modifications leading to matrix-associated ACT (MACT). However, both ACT and MACT face the challenge of chondrocyte dedifferentiation during expansion. 3 Therefore, research is primarily directed toward retaining the morphological properties of autologous chondrocytes during serial expansion.
Tissue engineering is a rapidly advancing field within regenerative medicine, dedicated to refining culture techniques to mimic and regenerate biological tissues. It involves seeding cells into scaffolds, which are enhanced with specific signals. This innovative approach has demonstrated success in the regeneration of various tissues, 4 including cartilage. 5 Therefore, cartilage tissue engineering (CTE) focuses on creating functional cartilage by combining chondrocytes or other cell types with biocompatible scaffolds and signals to mimic the native cartilage environment. This approach aims to overcome the limitations of traditional methods, such as ACT.
Cartilage Implant-Associated Infection
Microbial contamination poses a significant risk in surgical procedures involving implanted materials, elevating the likelihood of infections, and compromising host defenses. A biofilm is a complex community of microorganisms that adhere to surfaces and form a protective matrix. Biofilms are composed of microorganisms embedded in an extracellular polymeric substance (EPS), which provides a favorable environment for bacterial growth and survival. Microorganisms like bacteria attach and multiply forming microcolonies, which then mature and disperse across the surface and into surrounding environments (Fig. 2). In the case of cartilage implants, biofilm formation occurs when bacteria attach themselves to the implant surface and the EPS acts as a shield against host defense and antibacterial agents. Due to that, implant-associated infections in ACT present heightened challenges, often necessitating surgical removal of implants, increasing morbidity. Wood et al. conducted a comprehensive examination of adverse events after ACT, reporting that 18 patients out of 497 experienced surgical site infections. 6 Another study documented a bacterial joint infection in one out of nine patients, leading to the removal of the implanted graft. 7 Additional studies, such as those by Hambly et al. and Day & Gillogly, support these findings, revealing joint sepsis and inflammatory arthritis or infection after ACT surgery.8,9 Although these studies report that infections in ACT are uncommon, they still cause substantial joint damage when they occur. Consequently, newly engineered cartilage constructs must incorporate antimicrobial properties into their scaffolds to prevent bacterial infection. However, while studies on adverse events in ACT exist, the exploration of infections in CTE remains limited. Existing literature reveals instances of infections in tissue-engineered implants, stressing the need for infection control measures. A study on degradable polyester tissue-engineered scaffold biomaterials in rabbit knee osteochondral defects reported infections in 10 out of 228 implanted scaffolds. 10 Therefore, due to the absence of extensive research on infections in CTE, this review seeks to establish an essential foundation for researchers interested in addressing infection control in CTE and ACT specifically. To the best of our knowledge, this is the first review dedicated specifically to this topic. Hence, it aims to provide researchers with a practical starting point by focusing on scaffolds that have already been successfully used in CTE and proven to exhibit antimicrobial properties. By identifying these scaffolds, which have demonstrated efficacy in prior applications, the review ensures that researchers can immediately build upon existing, validated materials without the uncertainty of untested approaches. Given the scarcity of antimicrobial scaffolds, we explored additives that enhance infection resistance, focusing on those that met three key criteria: (1) compatibility with chondrocytes, (2) prior successful integration with CTE scaffolds, and (3) demonstrated antibacterial efficacy. This criterion also ensures immediate applicability for researchers in the field. By identifying such scaffolds and modifications, the goal is to advance chondrocyte implantation surgeries and reduce the complications associated with infections in tissue-engineered constructs.
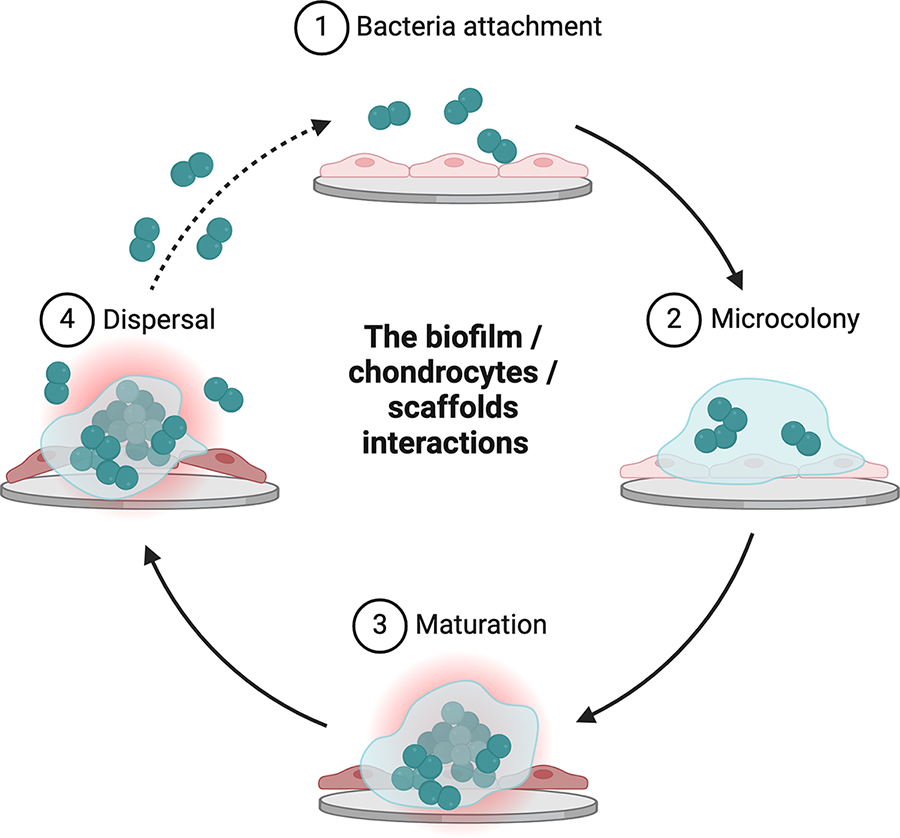
Process of biofilm formation and expansion on scaffolds in CTE. The four stages of biofilm formation on a scaffold containing chondrocytes. These stages include initial bacterial attachment, followed by microcolony formation, maturation, and eventual dispersion. (Created with BioRender.com.) CTE, cartilage tissue engineering.
Scaffolds
To regenerate healthy cartilage tissue, scaffolds must meet specific requirements: (1) suitable structure, which includes the right porosity, pore size, and interconnections to support cell movements, growth, and change, as well as to enable the exchange of oxygen, nutrients, and waste; (2) mechanical characteristics that are like the original cartilage tissue; (3) biocompatible, meaning they do not cause toxicity, cellular stress, immune reactions, or scarring; and (4) biodegradable, meaning they break down at a rate that matches the formation of new tissue.11–13 The characteristics of scaffolds are tailored to the specific cells being used; for instance, macro-pores suited for articular chondrocytes are >250 µm in size (Fig. 3) as correct pore sizes facilitate cell growth, maintenance of a suitable phenotype, and chondrogenic differentiation. 14 Additionally, chondrocytes grown on flat surfaces lose their capacity to generate certain proteins essential for hyaline cartilage formation. 14 Instead, a three-dimensional design for scaffolds is used to combat the dedifferentiation of chondrocytes into fibroblast-like cells. 14

The difference in scaffold properties tailored to articular chondrocytes (ACs) versus mesenchymal stem cells (MSCs). Articular chondrocytes require low oxygen tension and macro-pores >250 µm in size. (Created with BioRender.com.)
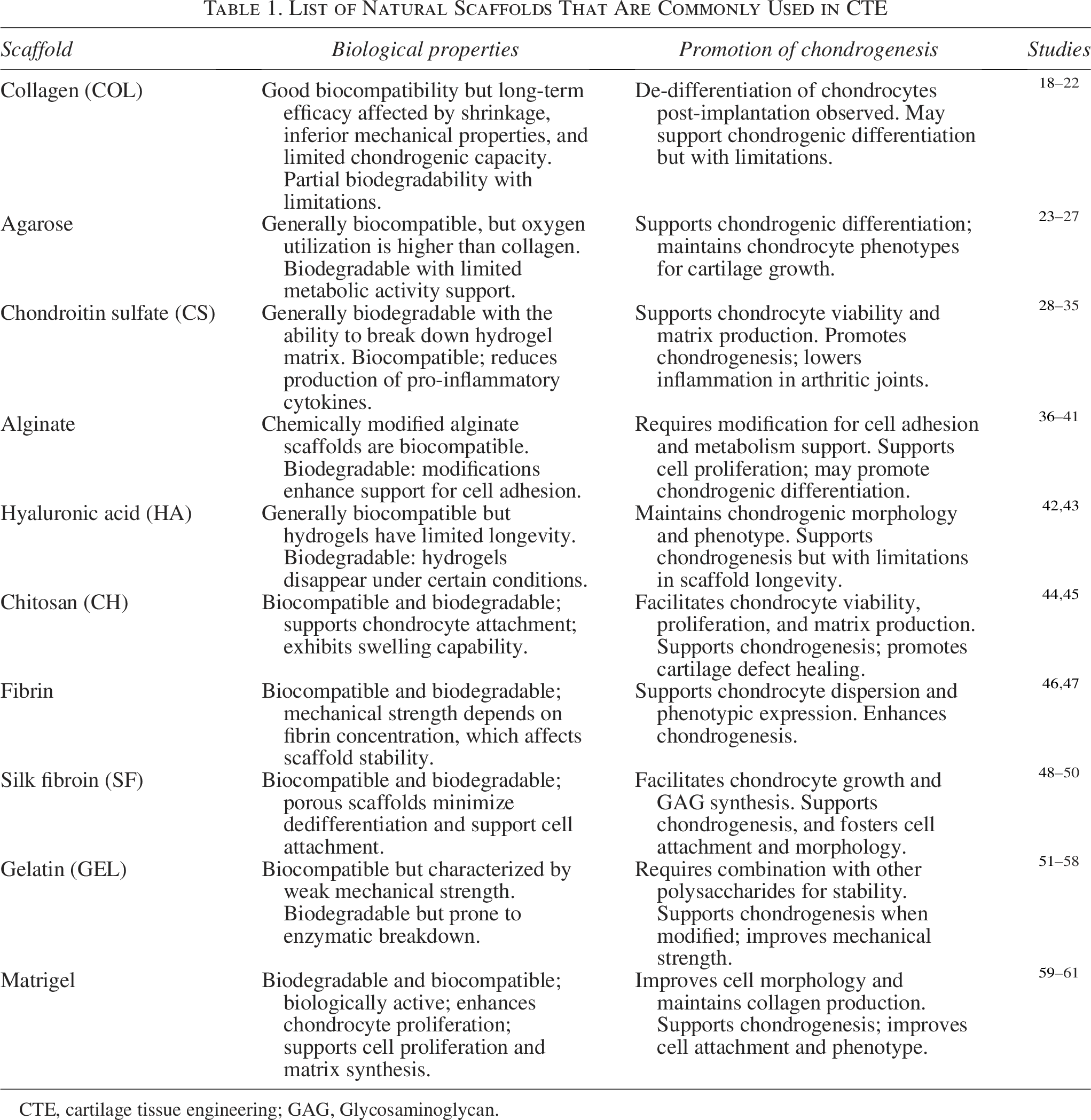
Materials used in scaffolds for CTE applications encompass a broad spectrum of natural and synthetic polymers. Hybrid scaffolds combining natural and synthetic polymers at different concentrations are also used to obtain the right biochemical and biomechanical properties for engineering applications. 12 Natural, synthetic, and hybrid scaffolds have been extensively reviewed in the literature.14–17 To avoid redundancy, we have summarized the key findings and studies in tables (Tables 1–3), providing an accessible overview for those new to this field. For a more comprehensive analysis, the referenced articles offer detailed reviews.14–17
List of Natural Scaffolds That Are Commonly Used in CTE
CTE, cartilage tissue engineering; GAG, Glycosaminoglycan.
List of Synthetic Scaffolds That Are Commonly Used in CTE

FDA, U.S. Food and Drug Administration.
List of Hybrid Scaffolds That Are Commonly Used in CTE

ECM, extracellular matrix
Natural scaffolds
Made from natural materials, natural scaffolds are highly bioactive and biocompatible and break down into nontoxic substances while being similar in composition to native tissues, making them an ideal microenvironment for cells. 14 As these scaffolds resemble cartilage’s extracellular matrix (ECM), they facilitate chondrogenesis and sustain the cellular phenotypes of chondrocytes, influencing cell adhesion and proliferation. Unfortunately, natural scaffolds rapidly lose their structure, are sensitive to water where they convert into gel-like substances, and lack the mechanical robustness required to support cells and the regenerated tissue. They usually form fibrous cartilage, which is susceptible to future damage compared to healthy hyaline cartilage. 14 These natural scaffolds are listed in Table 1, which summarizes the key findings and studies related to each scaffold material’s properties and use in CTE.18–61
Synthetic scaffolds
Synthetic polymers generally offer more controlled physiochemical and mechanical properties than natural materials and are frequently utilized in biomedical applications due to their biocompatibility and biodegradability as they may be broken down by hydrolysis of their ester bonds, requiring no enzymatic activity at all and releasing only nontoxic products eliminated as regular waste; however, they are also more prone to immune reactions postimplantation such as inflammation and tissue formation. 12 Synthetic scaffolds used for CTE are summarized in Table 2.62–74
Hybrid scaffolds
Hybrid scaffolds can be made by combining two or more natural and synthetic materials into a single membrane or hydrogel. Choosing compatible materials that complement each other’s weaknesses allows for a scaffold with improved mechanical properties while still mimicking the natural microenvironment needed for successful cartilage tissue reconstruction. Most hybrid scaffolds described in the literature for CTE use natural molecules such as those described in Table 1 to make the scaffold more closely mimic the native cartilage environment, supporting cell attachment, growth, and proliferation while maintaining the cartilage phenotype during passaging to achieve cell numbers necessary for ACT and MACT procedures. Synthetic polymers like those in Table 2 are added to enhance mechanical strength, thermal properties, and structural framework. Table 3 lists the hybrid scaffolds that are commonly used in CTE studies with animal models and articular chondrocytes.75–83
Antimicrobial Scaffolds and Additives
Using porous scaffolds as a framework for guiding new tissue development involves the risk of implant-associated infections due to the challenge of ensuring sterile biomaterials for safe therapeutic application both in vitro and in vivo as well as the possibility of infection during chondrocyte passaging in culture.84,85 Though investigation into the formation of biofilms and associated infections on scaffolds used in CTE has not been extensively explored, the risk still exists, and preventative measures must be taken. As such, this section first explores which of the CTE scaffolds, summarized in Tables 1–3, alone exhibit antimicrobial properties. Then, the section delves into antimicrobial additives that satisfy three criteria: (1) the additives must have demonstrated compatibility with chondrocytes in previous research, (2) the additives must have been used on a CTE scaffold covered in this review (regardless of the type of cells used), and (3) the additives must have rendered the scaffold antibacterial. Therefore, we propose that the scaffolds and additives discussed below and summarized in Table 4 are compatible with chondrocytes, antibacterial on CTE scaffolds, and should be investigated against infections in ACT.
List of Antimicrobial Scaffolds That Have Been Used in CTE

AECMs, artificial extracellular matrices; MSC, mesenchymal stem cell; S-GAG, Sulfated Glycosaminoglycan.
Antimicrobial scaffolds
Chitosan
Few of the scaffold materials used in CTE have been shown to possess antimicrobial properties in existing literature. Among these, chitosan (CH) extracted from Mealworm Beetle (Tenebrio molitor, Zophobas morio) and Rhinoceros Beetle (Allomyrina dichotoma) has exhibited inhibitory activity against Gram-negative and Gram-positive bacteria such as Escherichia coli, Staphylococcus aureus, Pseudomonas aeruginosa, Bacillus cereus, and Listeria monocytogenes.86–88 CH has thus been used in hybrid scaffolds with several other natural and synthetic materials such as poly-caprolactone (PCL), hyaluronic acid (HA), poly (ethylene glycol), and poly (lactic-co-glycolic acid) (PLGA), inducing significant antimicrobial effects.89–91
Chondroitin sulfate
Chondroitin sulfate (CS) extracted from Scophthalmus maximus, Holothuria scabra, Eupentacta fraudatrix, Massinium magnum, and Holothuria mexicana has been reported for both articular cartilage repair and antibacterial effects. 92 CS and CH have been combined to create artificial extracellular matrices (AECMs) through interpolyelectrolyte complexation and lyophilization as well as crosslinking with glutaraldehyde, calcium ions (Ca2+), N,N-(3-dimethyl aminopropyl)-N′-ethyl carbodiimide, and N-hydroxysuccinimide. 93 The CH-CS composite AECMs demonstrated superior antibacterial effectiveness against E. coli compared with controls. 93
Sharma et al. investigated the combined antibacterial and anti-inflammatory capabilities of a CH-CS polyelectrolyte complexation (CH-CS PEC) scaffold; in vivo, tests revealed that CH-CS PEC facilitated faster showed more significant bacterial cell death compared with either CH or CS alone, which they attributed to a synergistic effect of both CH and CS. 94 Nonetheless, research into antimicrobial scaffolds in CTE is limited, so additional methods of creating antibiotic scaffolds for tissue engineering are necessary. Various methods are employed to create antibacterial scaffolds, including the integration of antibiotics 95 or drug-loaded nanoparticles (NPs), as well as structural modifications to inhibit bacterial growth.
Antimicrobial additives
Among the diverse approaches to scaffold modification, three notable additives—silver, zinc oxide, and copper—have been identified. These additives have been applied to chondrocytes, demonstrated usage and compatibility on CTE scaffolds, and exhibited antimicrobial properties.
Silver
Silver (Ag) is widely used in medicine for its extensive antimicrobial properties, and Ag NPs are commonly added to scaffolds as antibacterial agents in tissue engineering because they do not significantly alter scaffold physiochemical properties. Alarcon et al. examined the safety and effectiveness of incorporating Ag NPs coated with collagen into collagen hydrogels and found that, at Ag NP concentrations below 0.4 μM, the scaffolds maintained their mechanical properties and biocompatibility with primary human skin fibroblasts and keratinocytes, similar to pure collagen hydrogels. 96 Additionally, the scaffolds significantly inhibited several bacterial strains including Staphylococcus epidermidis, S. aureus, E. coli, and P. aeruginosa, at much lower concentrations than the Ag nitrate used as a control. Moreover, when scaffold materials were subcutaneously implanted in mice, there was a noticeable decrease in interleukin-6, an inflammatory marker characteristic of arthritis. 96 Ag NPs have been incorporated into natural, synthetic, and hybrid scaffolds where they were found to induce wound healing while reducing bacterial infection significantly.97–102 Research investigating the effect of Ag on chondrocytes when used for CTE specifically is unavailable in the literature; however, He et al. studied the effect of Ag NPs on chondrogenic differentiation of human bone marrow-derived mesenchymal stem cells (hMSCs). 103 Their results found that 30 nm Ag NPs influence chondrogenesis by enhancing the expression of chondrogenic markers (increased SRY-Box Transcription Factor 9, Cartilage Oligomeric Matrix Protein, and GAG) while simultaneously decreasing hypertrophy (reduced expression of type X collagen, a hypertrophic chondrocyte marker) in hMSCs. 103
Zinc oxide
Zinc ions have been reported for their antibacterial properties against bacteria such as E. coli and are incorporated into tissue engineering as NPs or coatings to confer this antimicrobial property onto PLGA, PCL, gelatin, and CH among other scaffolds.104–106 Zinc deficiency is known to be associated with diseases affecting cartilage, so research has been conducted investigating the effect of ZnO on chondrogenic differentiation as well as chondrocyte growth and matrix synthesis.107,108 Fibrous zinc oxide (ZnO) composite scaffolds with ZnO concentrations ranging from 1 to 10 wt.% have been assessed for their ability to direct human mesenchymal stem cell (MSC) differentiation toward chondrocyte and osteoblast lineages. 108 Scaffolds with lower ZnO percentages were found to enhance MSC chondrogenic differentiation, as evidenced by increased collagen type 2 (COLII) production and higher expression of cartilage-specific genes, while scaffolds with higher ZnO percentages were more effective in promoting osteogenic differentiation, as shown by elevated alkaline phosphatase activity, enhanced collagen production, and greater expression of bone-specific genes. Mirza et al. observed that the combination of low oxygen levels and 1% ZnO NPs significantly increases chondrocyte proliferation and sulfated glycosaminoglycan production while enhancing the expression of anabolic genes (COLII, aggrecan) and reducing the expression of the catabolic gene Matrix Metalloproteinase-13. 107 They concluded that 1% ZnO NPs contribute to maintaining the balance in cartilage’s hypoxic environment. Furthermore, the production of the transcription factor hypoxia-inducible factor 1A, which is crucial for chondrocyte survival under low oxygen conditions, remained unaffected by the presence of 1% ZnO NPs. 107
Copper
Copper (Cu) ions have also been identified for their antimicrobial effects and explored as therapeutic agents in the medical field because they do not present the risk of bacterial resistance.109–111 Copper is also a good choice for MACT because it exists naturally in the human body, unlike Ag for example. 112 Cu has been incorporated into tissue engineering scaffolds such as CH, polylactic acid, and polyethylene oxide where it was found to prevent biofilm formation by inhibiting Staphylococcus carnosus, E. coli, and S. aureus growth.112–114
Significant for the context of this review, Cu has been incorporated into hydrogel scaffolds to stimulate the formation of connective tissue. 115 Recently, Madzovska-Malagurski et al. investigated Cu as a versatile agent in tissue engineering approaches, examining its dual role in providing antimicrobial effects and facilitating chondrogenesis. 116 Their research centered on the concentration of Cu in alginate microbeads, considering it a critical factor in controlling the properties and functionality of the hydrogel, so Cu-alginate hydrogels were formed into microbeads with varying concentrations of Cu ions, Cu (II), ranging from 13.5 to 270 mM. They found that microbeads with a higher Cu (II) concentration of ∼100 μmol g−1 demonstrated immediate bactericidal effects against E. coli and S. aureus, while microbeads with a Cu (II) content of ∼60 μmol g−1 released Cu ions more slowly and significantly promoted chondrogenic phenotype of bovine calf chondrocytes in a 3D culture. 116
Promising Additives and Approaches for Future Exploration
As one of the pioneering efforts to explore the infection control in CTE, this review aims to provide a practical, near-term guide for researchers and clinicians seeking immediate application. Therefore, the decision to focus on scaffolds already used in CTE having antimicrobial properties as well as antimicrobial additives that meet the defined criteria of compatibility with chondrocytes, prior use on CTE scaffolds, and proven antibacterial efficacy ensures the review is practical and relevant. This approach highlights materials directly applicable to CTE, avoiding speculative solutions and grounding the findings in established research. However, these strict criteria narrow the scope by excluding innovative additives not yet tested with chondrocytes or applied to CTE. Thus, this section briefly explores promising additives and innovative strategies that may not fit the established criteria but hold significant potential for future exploration.
Recent advancements in scaffold design have introduced a variety of techniques to enhance antimicrobial properties, creating new possibilities for applications in CTE. For example, the incorporation of antimicrobial agents, such as antimicrobial peptides, into scaffolds has demonstrated effective bacterial inhibition within various fields of tissue engineering. 117 Moreover, graphene oxide, widely recognized for its exceptional properties, has been extensively incorporated into scaffolds for antibacterial research. Scaffolds with graphene oxide show inhibition of bacterial growth and improved biocompatibility.118,119 Furthermore, graphene oxide has been successfully combined with various NPs to enhance its antimicrobial efficacy and broaden its functionality in scaffold design, 120 making it a potential candidate for CTE applications. Bioactive glass has also garnered attention for its antibacterial properties and is particularly recognized for its compatibility with osteocytes, which are mesenchymal-derived cells. 121 Advanced fabrication techniques, such as electrospinning, also offer promising tools for infection control in CTE. Electrospinning has enabled the creation of electrospun nanofibers infused with Ag NPs, producing scaffolds with a large surface area that is highly effective for antibacterial action. 122 Finally, emerging technologies include smart scaffolds that release antimicrobial agents in response to environmental triggers such as pH or bacterial presence as reviewed by Skwarczynski et al. 123 These smart scaffolds provide targeted action and reduce unnecessary exposure to antimicrobials, making them another potential candidate for CTE applications. The field of antimicrobial scaffolds is diverse, with numerous innovations that hold significant potential for future exploration in CTE. A more detailed analysis of this topic can be found in the review by Serrano-Aroca et al. 124
In addition to diverse scaffolds, chemical signals such as growth factors are used extensively in CTE. Growth factors promote tissue regeneration and exhibit antimicrobial properties through derived peptides, which disrupt microbial membranes, enabling both infection control and repair.125,126 Additionally, growth factors like Insulin-Like Growth Factor 1 and Transforming Growth Factor Alpha have been explored to enhance antimicrobial peptide expression. 127 Thus, using growth factors as signals with antimicrobial scaffolds, such as those previously discussed, illustrates a promising synergy to enhance tissue regeneration while simultaneously addressing microbial challenges in ACT through CTE.
Conclusions
The field of CTE holds great promise for addressing the challenges of OA and cartilage regeneration. While advancements have been made in the field, research on infections in ACT and the attention given to infection control measures in chondrocyte implantation surgeries are notably scarce. Therefore, this review seeks to examine which of the major scaffolds used in CTE demonstrate antimicrobial properties. Our research highlights the antimicrobial properties of CH and CS, making them suitable candidates for infection prevention in cartilage implants. In addition, we propose an alternative avenue for addressing infections by incorporating additives such as ZnO, Ag, or Cu into any of the mentioned scaffolds used in CTE. This innovative approach aims to create antibacterial constructs, reducing bacterial infections, and rendering these scaffolds suitable for chondrocyte implantation surgeries. Finally, this paper highlights promising additives and fabrication processes that are increasingly recognized in the field of infection control within tissue engineering, offering potential applicability to CTE. This review serves as a critical foundation, laying the groundwork for comprehensive research on infections in CTE.
It is important to note that significant gaps and limited research in CTE remain. Therefore, to initiate research in this underexplored field, we recommend a stepwise approach beginning with foundational in vitro studies. Researchers should first focus on testing antimicrobial scaffolds and additives in controlled environments to establish baseline efficacy and compatibility. The simplest and most accessible starting point is culturing chondrocytes alongside bacteria on CH scaffolds, as CH has well-documented antimicrobial properties supported by numerous studies. Alternatively, researchers could test the addition of antimicrobial agents such as Ag, ZnO, or Cu to any existing CTE scaffold. These additives have demonstrated compatibility with chondrocytes and antibacterial efficacy, making them suitable candidates for preliminary studies. Once these initial experiments validate the antimicrobial potential of scaffolds and additives, further research should mimic real-world conditions. This includes evaluating scaffold performance under dynamic, physiological load conditions, hypoxic environments, and in the presence of growth factors to simulate joint mechanics. Such advanced in vitro studies will provide insights into how these materials behave in more complex and realistic scenarios. Finally, exploring alternative materials not yet tested with chondrocytes, such as bioactive glasses, graphene derivatives, and smart scaffolds, could uncover new antimicrobial and regenerative options. These innovative materials hold promise for expanding the scope of infection control strategies in CTE. By systematically progressing from simple in vitro setups to more complex, physiologically relevant models, researchers can build a robust foundation for tackling the pressing challenge of infections in ACT using specific CTE scaffolds and additives.
Authors’ Contributions
L.A.D. and R.M. proposed the idea, N.N. and R.R. contributed equally to the preparation of this review, and all authors read and approved the article.
Footnotes
Funding Information
The authors extend their appreciation to the King Salman Center for Disability Research for funding this work through Research Group no KSRG-2023-062.
Disclosure Statement
The authors declare that they have no conflict of interest.