
Abstract
Tissue and organ dysfunction are major causes of worldwide morbidity and mortality with all medical specialties being impacted. Tissue engineering is an interdisciplinary field relying on the combination of scaffolds, cells, and biologically active molecules to restore form and function. However, clinical translation is still largely hampered by limitations in vascularization. Consequently, a thorough understanding of the microvasculature is warranted. This review provides an overview of (1) angiogenesis, including sprouting angiogenesis, intussusceptive angiogenesis, vascular remodeling, vascular co-option, and inosculation; (2) strategies for vascularized engineered tissue fabrication such as scaffold modulation, prevascularization, growth factor utilization, and cell-based approaches; (3) guided microvascular development via scaffold modulation with electromechanical cues, 3D bioprinting, and electrospinning; (4) surgical approaches to bridge the micro- and macrovasculatures in order to hasten perfusion; and (5) building specific vasculature in the context of tissue repair and organ transplantation, including skin, adipose, bone, liver, kidney, and lung. Our goal is to provide the reader with a translational overview that spans developmental biology, tissue engineering, and clinical surgery.
Impact Statement
This translational article provides a concise review of microvascular engineering efforts to date within the context of grafts, flaps, and entire organ replacement. Our article systematically and logically discusses current developments, challenges, and novel approaches in microvascular engineering. It provides a readable starting point for understanding various approaches and the implications of successful vascularization at the microvascular level as well as how surgical approaches can be used to facilitate connections to the recipient macrovasculature.
Introduction
Tissue and organ dysfunction are major causes of morbidity and mortality, impacting all medical specialties. For example, soft tissue loss that occurs following oncologic extirpation is broadly comparable with that affected by ischemic or infectious etiologies. In all scenarios, clinicians seek to restore function, form, or both, thereby preserving both quality and quantity of life. Unfortunately, this is not always achievable despite clinical advances. Reconstructive and transplant surgeons are tasked with replacing tissue and organs, respectively. Regrettably, replacement grafts, flaps, and organs are scarce and complication prone.
Grafts are pieces of tissue transferred to a remote anatomical site without intrinsic blood supply (Fig. 1A). 1 Skin grafts (SG) have become ubiquitous to treat small tissue defects, irrespective of etiology.2–9 Because SGs rely on diffusion from the recipient site for initial oxygen delivery, they need to be quite thin to limit necrosis. Thus, they are typically only suitable for the reconstruction of <2 mm thick defects. 10 Complete vascularization from the recipient takes several weeks.11,12 If the recipient site is suboptimal, as seen following irradiation, the graft may never vascularize. 13
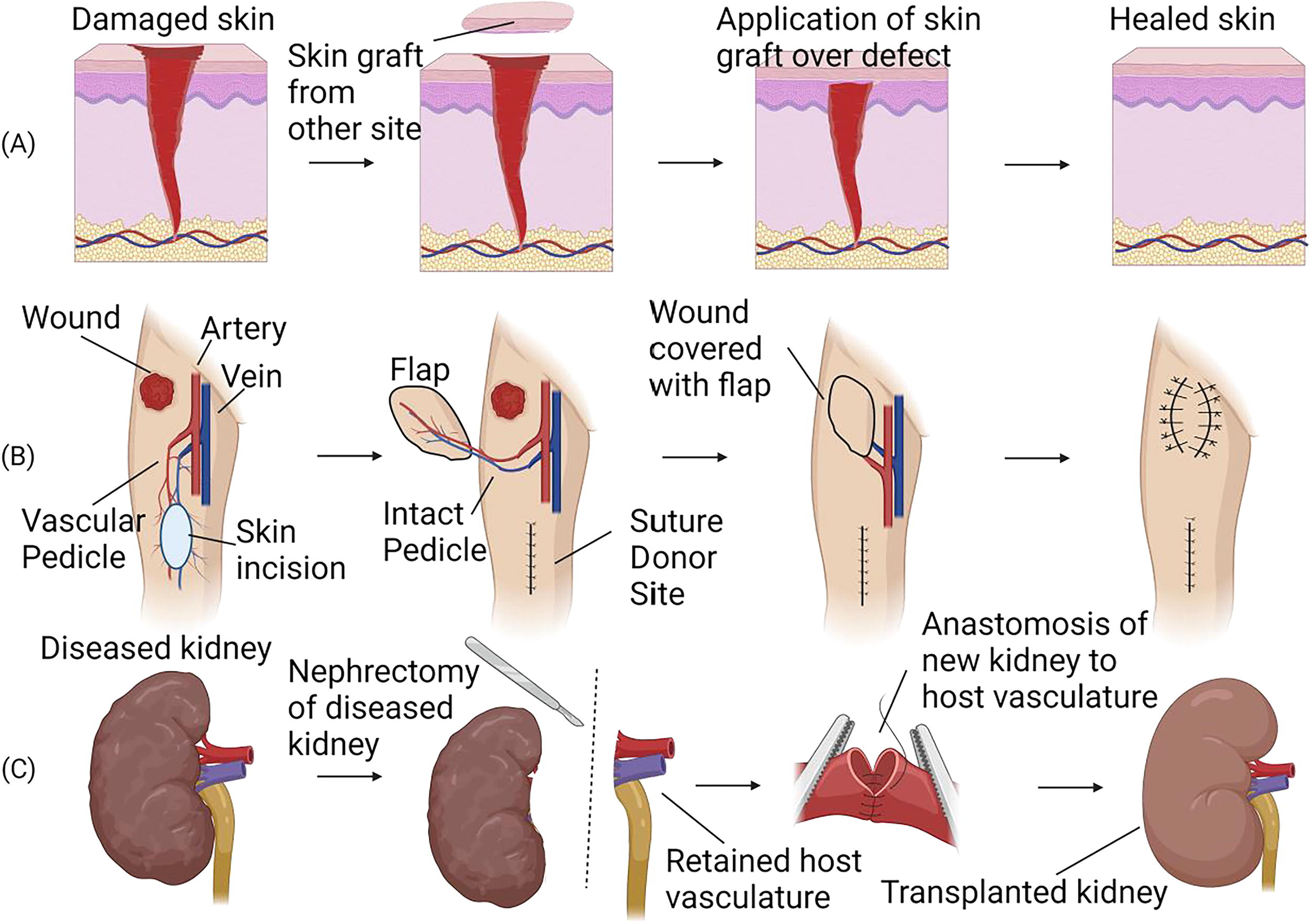
Diagram showing differences between graft, flap, and whole organ replacement.
In contrast, flap surgery is defined by the transfer of vascularized tissue (e.g., adipose, bone) with its feeding artery and draining vein (vascular pedicle [VP]) (Fig. 1B). Since flaps carry their own blood supply, they can be any thickness and are suitable for wound reconstruction of any depth. This autologous tissue transplantation has revolutionized reconstructive options across different anatomical sites.14–18 However, complications are common, 19 including flap loss secondary to thrombosis (up to 10%),20–22 and donor site morbidity with scarring, dehiscence, weakness, and paresthesia.23,24 Patients may have inadequate donor sites that preclude flap surgery.25,26
For entire organ replacement, the principles of vascular anastomosis allow for allogenic exchange (Fig. 1C). Notwithstanding donor scarcity, organ transplantation has specific challenges including immunosuppression and rejection risk. Despite a two-fold increase in transplants over the past 30 years, the number of waiting patients has increased six-fold. 27
The goal of tissue engineering (TE) is to create replacement tissues and organs. This interdisciplinary field relies on scaffolds, cells, and biological molecules to restore both form and function. Despite significant advances, clinical translation is limited largely by insufficient vascularization and slow perfusion upon implantation. This critical bottleneck limits implementation and the surgeon’s dream of being able to pull replacement parts “off the shelf.” Unfortunately, the ability to engineer a perfusable hierarchical microcirculation still precludes us. Here, we provide a microvascular overview and current surgical bioengineering attempts for graft, flap, and organ vascularization (Table 1).
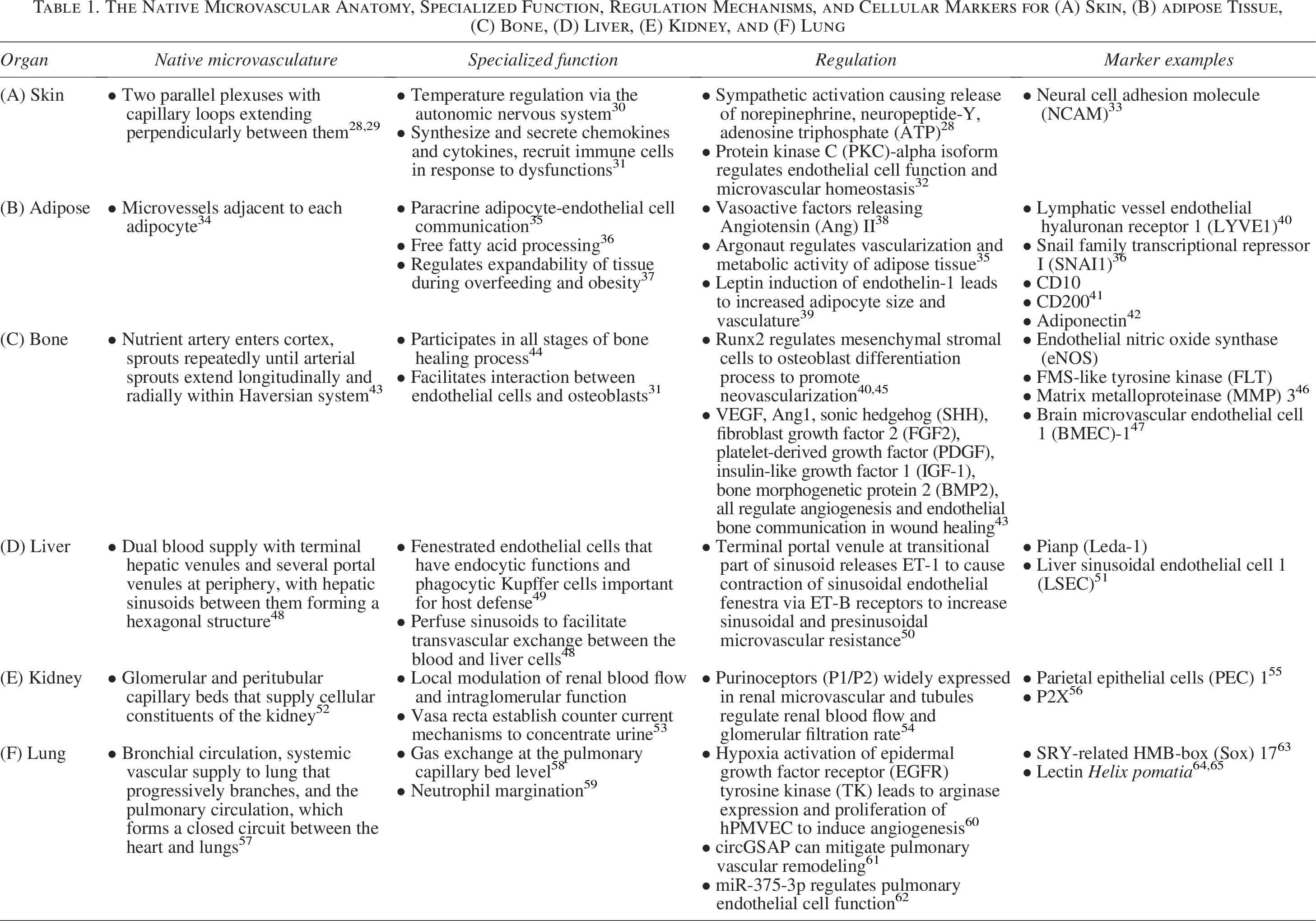
The Native Microvascular Anatomy, Specialized Function, Regulation Mechanisms, and Cellular Markers for (A) Skin, (B) adipose Tissue, (C) Bone, (D) Liver, (E) Kidney, and (F) Lung
The Microvasculature
The microvasculature is crucial to end-organ functionality. Native microvasculatures are characterized by organized tree-like branching of arterioles into progressively smaller vessels down to capillaries, converging into postcapillary venules. This permits blood flow regulation via arterioles, oxygen diffusion via capillaries, and immune cell modulation via venules.28–32 Thus, the potential of hierarchical microvascular replacement far exceeds just tissue reconstruction. The development of a rapidly perfused and tailored microvasculature would profoundly impact our ability to generate replacement tissue and treat microvascular dysfunction across all anatomical sites33–36 and redefine surgical treatments. 37 To develop the best engineering and surgical practices for microvascular creation, an understanding of native microvascular development is necessary.
Spouting angiogenesis
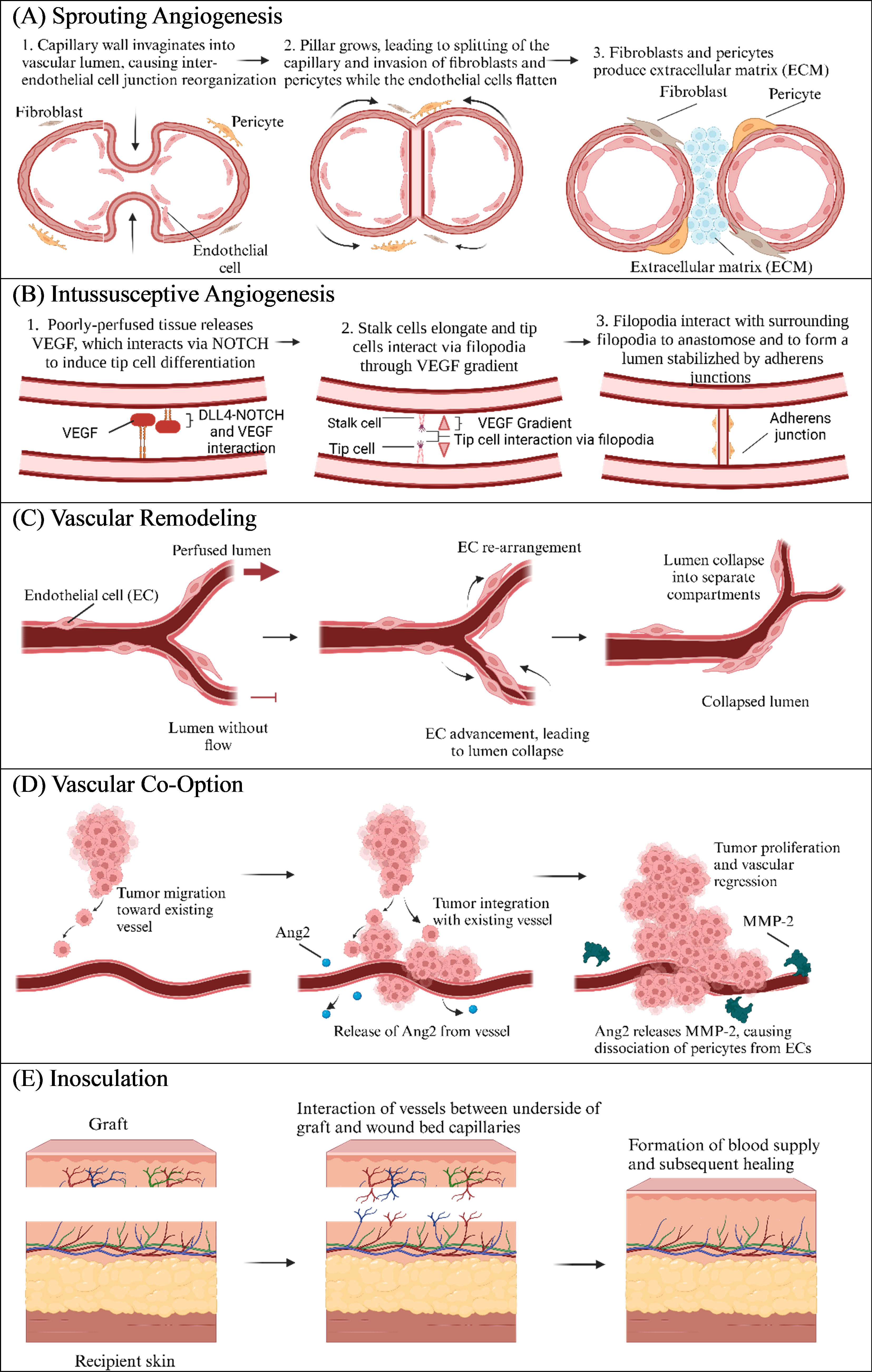
Sprouting angiogenesis (SA) (Table 2A), activated under ischemic conditions, releases proangiogenic factors like vascular endothelial growth factor (VEGF) to promote new vessel formation. 39 This process involves the tip cell, which migrates toward VEGF, and the stalk cell, which proliferates to extend the vessel (Fig. 2A).40,41 VEGF-Notch signaling impacts cellular regulation; Delta-like ligand 4 (DLL4)-Notch interaction influences endothelial cells (EC) fate toward stalk cells, and Notch signaling suppression enhances tip cell filopodia activity.42,43 VEGF gradients govern tip and stalk cell activities, causing sprout extension and luminal formation.45–49 The process is completed when EC migration stops and adherens junctions are established. 66
Detailing Specifics of (A) Sprouting Angiogenesis, (B) Intussusceptive Angiogenesis, (C) Vascular Remodeling, (D) Vascular Co-Option, and (E) Inosculation
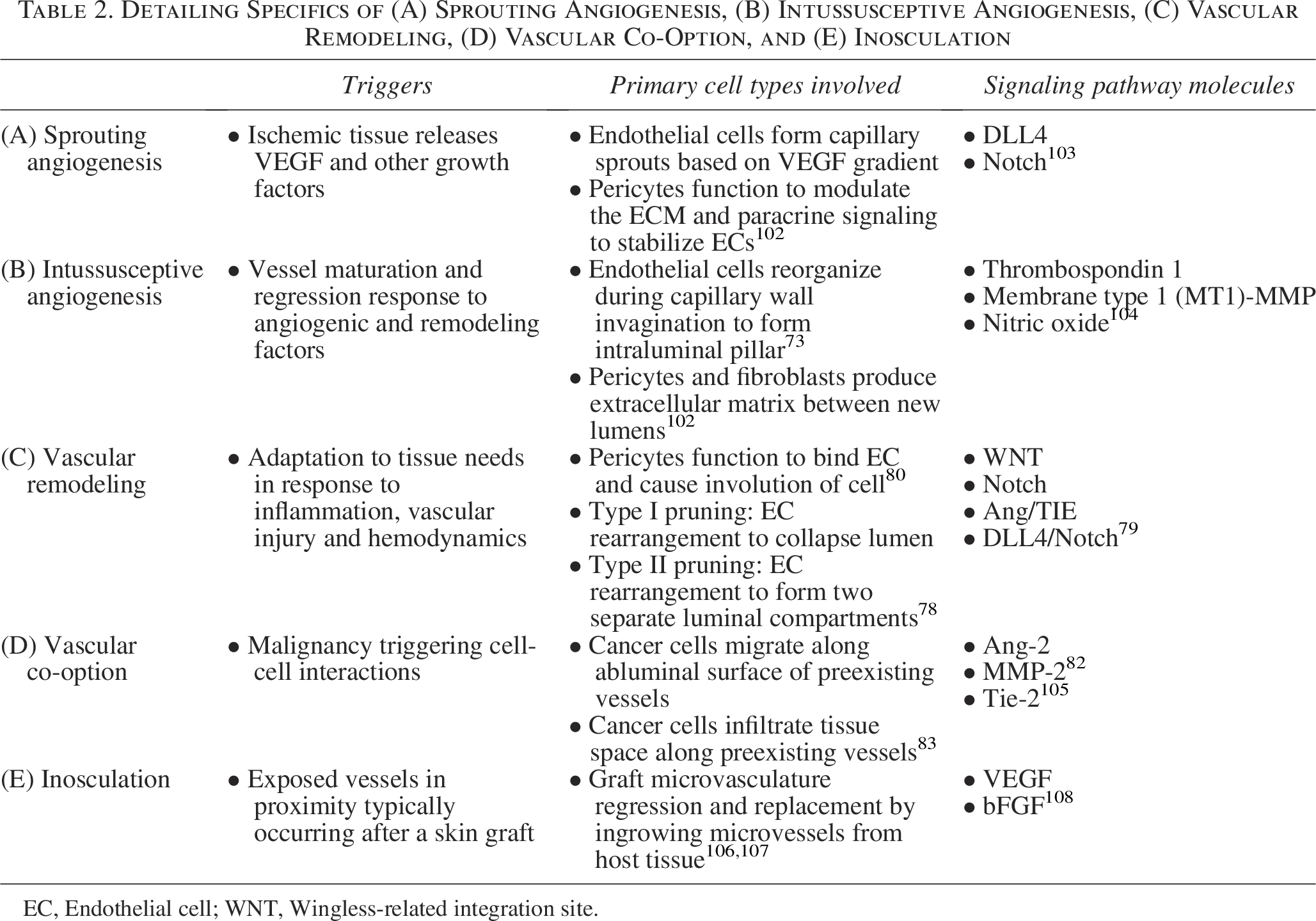
EC, Endothelial cell; WNT, Wingless-related integration site.
Pericytes, mesenchymal-origin cells associated with ECs, modulate vascular stability, and angiogenesis.51,52 Recruited by ECs through factors such as platelet-derived growth factor (PDGF)-B, they contribute to basement membrane (BM) formation and EC stabilization.54,55 Their density varies by tissue type, reflecting their function in regulating vascular permeability, integrity, and functionality.56–58 While VEGF remains the most studied angiogenic growth factor (GF), it is impacted by multiple GFs such as hepatocyte GF, which enhances VEGF; keratinocyte GF, which induces angiogenesis and stabilizes endothelial barriers; as well as angiogenic lymphokines (angiokines), which modulate capillary development.67–69 Multiple GFs, cytokines, lipids, and stimuli impact the regulation of junctional molecules and cell surface receptors. 70
Intussusceptive angiogenesis
Intussusceptive angiogenesis (IA) (Table 2B) is the process by which new vessels are formed by dividing an existing vessel. 71 During capillary replication and remodeling, the capillary wall invaginates into the vascular lumen to form an intraluminal pillar (Fig. 2B). 71 The interendothelial junctions reorganize, forming a central perforation that is invaded by pericytes and myofibroblasts depositing ECM. 72 In contrast to SA, where pericytes participate in vessel development, stabilization, maturation, and regression; pericytes in IA help form the pillar interstitial core to allow pillar growth and splitting of the initial capillary.73,74 During this, the BM remains intact; ECs enlarge and flatten, resulting in a lower metabolic cost.75,76 IA is primarily regulated by hemodynamic forces but is also influenced by GFs. 76 However, unlike SA, VEGF is downregulated during IA. 77 Generally, the microvasculature is initiated through SA with IA playing a subsequent role. 71
Vascular remodeling
Vascular remodeling (Table 2C) involves growth, regression, and change in lumen size in response to tissue demands (Fig. 2C). 78 Pruning, microvessel regression, is influenced by blood flow, with nonperfused vessels prone to pruning.78,79 Two pruning types exist: type I occurs without flow and leads to endothelial advancement and lumen collapse, and type II begins in perfused vessels, with EC rearrangement maintaining the lumen before eventual collapse into separate compartments. 80 Signaling cascades such as Notch, Ang/TIE, and DLL4/Notch, facilitate balance between vessel formation and regression. 81 Pericytes, through interaction with EC C-X-C Motif Chemokine Receptor 3 receptors and activation of calpains, play a role in selective pruning. 82 Calpains, tightly regulated proteases, are involved in cell processes including proliferation, apoptosis, and differentiation. 83
Vascular co-option
Co-option (Table 2D) allows cancer cells to utilize preexisting vessels for tissue expansion independent of angiogenesis (Fig. 2D).84,85 This interaction complicates traditional therapeutic targets and 86 tumors grow until these vessels are fully integrated 87 ; Ang-2 then leads to endothelial detachment and vessel regression, promoting tumor advancement.84,88 After regression, both IA and SA occur. While associated with malignancy, similar mechanisms have been observed in wound healing. 89
Inosculation
Inosculation (Table 2E), critical for split-thickness skin graft (STSG) viability, involves forming a connection between the embedded graft microvasculature and recipient capillaries (Fig. 2E). 90 Although STSGs are ubiquitously used for skin repair, they are limited by availability, leading to the development of engineered substitutes such as decellularized dermal matrices.91,92 These matrices also utilize inosculation, but exhibit slower vascularization compared with autologous STSG. 93 Revascularization rate is influenced by thickness, with thinner grafts revascularizing faster. 94 While thicker grafts offer better coverage, diffusion challenges lead to higher failure rates.
These processes are also driven by metabolic demand and hemodynamic cues 95 that complement GFs, such as blood flow shear forces and extracellular matrix (ECM) stiffness. 96 Metabolism influences GF activity 97 with capillary density being directly proportional depending on tissue type. 98 Organotypic vasculature is the principle that tissue-specific ECs have cellular and molecular heterogeneity 99 that modulate vascular differentiation and function. 100 Native angiogenic complexity 101 warrants multiple approaches to vascularized TE.
Strategies for Vascularized Engineered Tissue
Successful tissue replacement extends beyond simple vascularization, ideally requiring a microvasculature with a topology that supports rapid perfusion and functional demands. The interplay between microvascular and macrovascular systems is crucial for tissue function.109,110 For engineered tissues to survive, vascular networks are needed and a variety of approaches have been trialed. 111
Scaffolds
Vascularized tissue regeneration is facilitated by scaffolds.111,112 A diverse group of biomaterials exists including natural and synthetic. Aiming to mimic ECM, they provide structural support and mechanical stability.113–115 Additionally, scaffolds must exhibit biocompatibility to reduce immunogenic responses. 116 Scaffold modification, through prevascularization, GFs, and cell seeding offers therapeutic and unique advantages for microvascular engineering (Fig. 3).
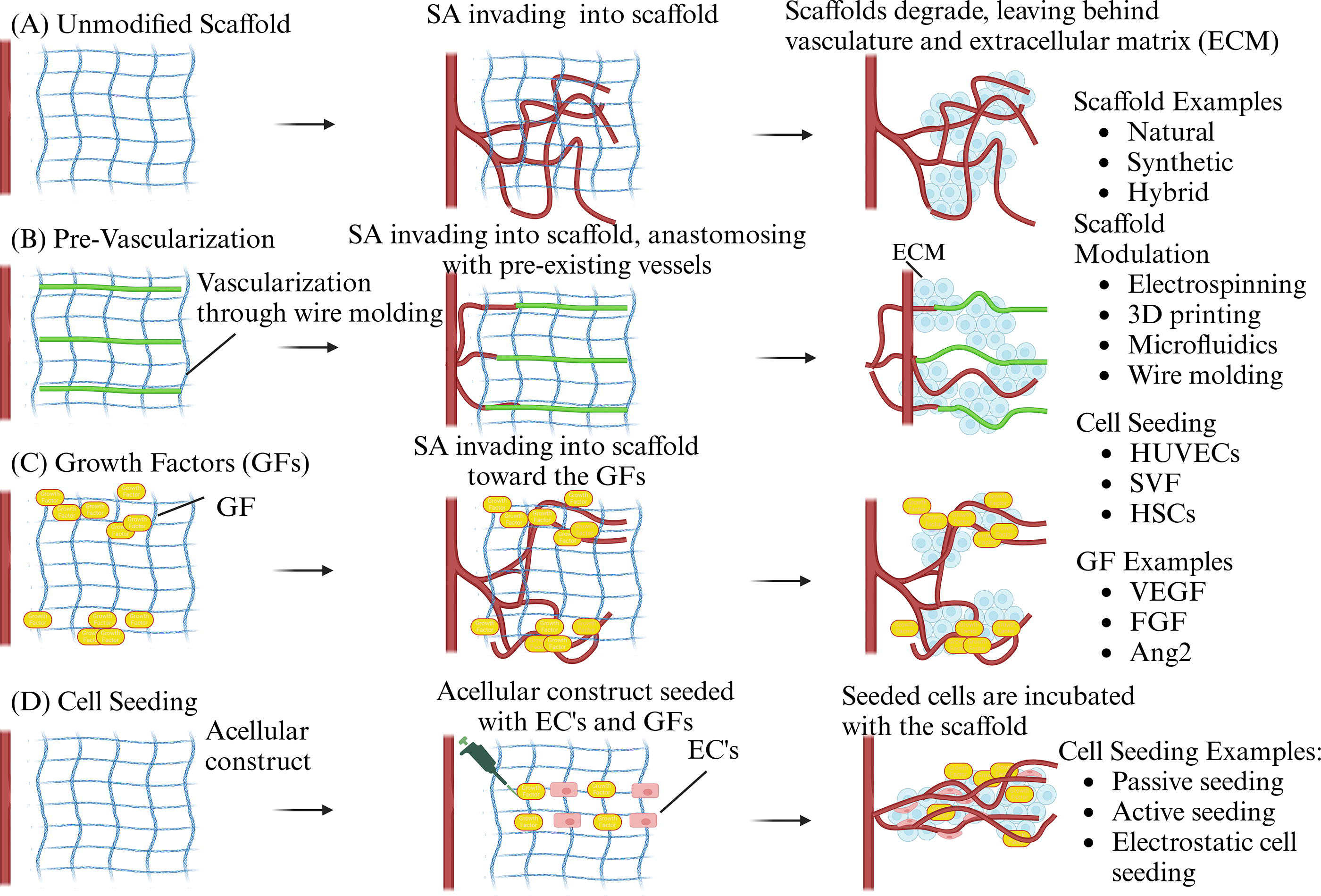
Diagram discussing current in vitro approaches for vascularizing engineered tissue.
Natural scaffolds (Figs. 3A and 4A), commonly collagen derived, are favorable due to biocompatibility and ECM similarity.139,140 Once implanted, ECs invade and remodel the biomaterial to establish vascularization.141,142 Collagen scaffolds can also be modified to promote intrinsic vascularization. 143 One study showed that hFGF incorporated into a collagen sponge was released with sponge biodegradation and exhibited dose-dependent angiogenesis. 144 Similar examples of natural scaffolds include gelatin and hyaluronic acid.145,146
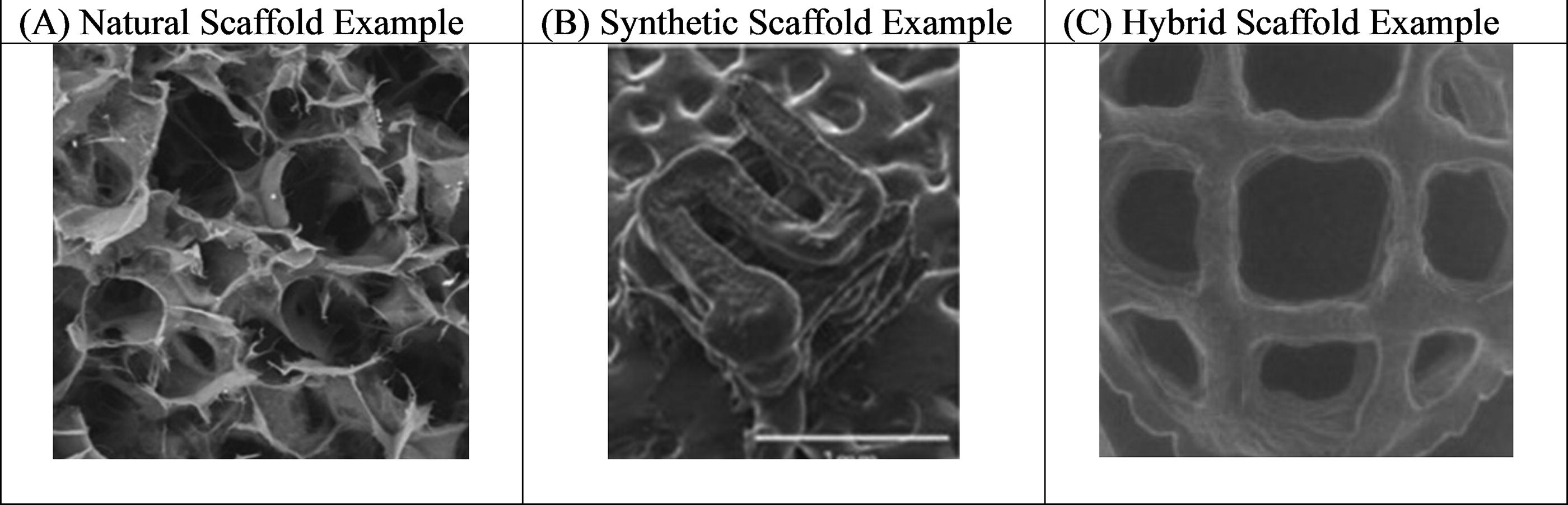
Synthetic scaffolds (Fig. 4B), such as poly(lactic-co-glycolic) acid (PLGA), polylactic acid (PLA), polycaprolactone, and polyglycolide, provide mechanical strength but are less favorable due to incompatibility.147–149 For example, PLA is more resistant to biodegradation, but its acidic byproducts adversely impact cell infiltration and vascularization. 150
Hybrid scaffolds (Fig. 4C), such as gelatin methacryloyl (GelMA), permit increased bioactivity with improved stability. 151 In one study, new vessel formation, collagen deposition, and re-epithelization were accelerated by cross-linking GelMA functionalized with endothelin-1 to promote wound healing. 152 These scaffolds have gained attention as they permit effective cell attachment and proliferation.153,154 A study by our groups showed that scaffolds made from microporous granular GelMA could control microvascular topology. 155
Vascularization adjuncts
Prevascularization (Fig. 3B) involves creating a scaffold microvasculature in vitro prior to implantation. Theoretically, this should expedite perfusion and reduce the metabolic effort needed for complete vascularization.175,176 Techniques for creating prevascularized tissues include bioprinting, microfluidics, wire molding, and microvascular fragments (MVF).131,177 While these channels are not a vessel, they mimic vessels but require cellularization prior to effectively conducting blood flow.
Bioprinting (Table 3A) uses advanced manufacturing, such as extrusion and laser-based approaches, to create cell-laden 3D structures mimicking tissue, with microchannels that can be endothelialized for blood vessel simulation.117,122 This method allows for complex, signal-rich structures but faces challenges including bioink cytotoxicity.121,123
Detailing Techniques, Materials, Advantages, and Disadvantages of (A) Bioprinting, (B) Microfluidic Technology, (C) Wire Molding, (D) Microvascular Fragments

GelMA; gelatin methacryloyl; MWF, microvascular fragments; PDMS, Polydimethylsiloxane.
Microfluidic technology (Table 3B) leverages lithography to construct detailed microfluidic networks, facilitating precise geometrical control and influencing cell growth through fluid manipulation in micrometer-sized channels.178,179 This method mirrors natural vascular development but is generally confined to producing only thin tissues within the microfluidic setup, complicating implantation. 130 Given implantation difficulty, this technology remains largely restricted to simple in vitro microvascular testing.179–181
Wire molding (Table 3C) creates microchannels by molding polymers around suspended wires that are subsequently removed, leaving behind perfusable channels. These channels, once endothelialized, can function like natural vessels.129,182
Microvascular fragments (Table 3D) are functional vessel segments derived from adipose tissue that rapidly reassemble upon implantation. 183 Compared with SVF, they have increased levels of ECs and perivascular cells facilitating engraftment and vasculogenic efficiency. 184 MVF have been shown to inosculate with host vessels and accelerate scaffold perfusion, 134 irrespective of origin and degree of vessel specialization. 185
Growth factors
GFs (Fig. 3C), such as proteins and miRNA, are biologically active molecules that can affect cell growth and vascularization. 186
Proteins
Proteins (Table 4A), such as VEGF, enhance neovascularization through EC migration and vessel sprouting.187,188 Scaffolds with controlled GF gradients were found to increase vascularization, showing clinical promise.189–191 However, GF degradation by enzymes poses a challenge. 192 Timing of GF release affects vascular development; simultaneous application of proangiogenic and promaturation factors hinders angiogenesis, whereas sequential application enhances microvessel density. 193 Thus, temporal control of GF signaling appears crucial for therapeutic vascularization.
Substrate Examples Along with Advantages and Disadvantages for (A) Protein and (B) microRNA
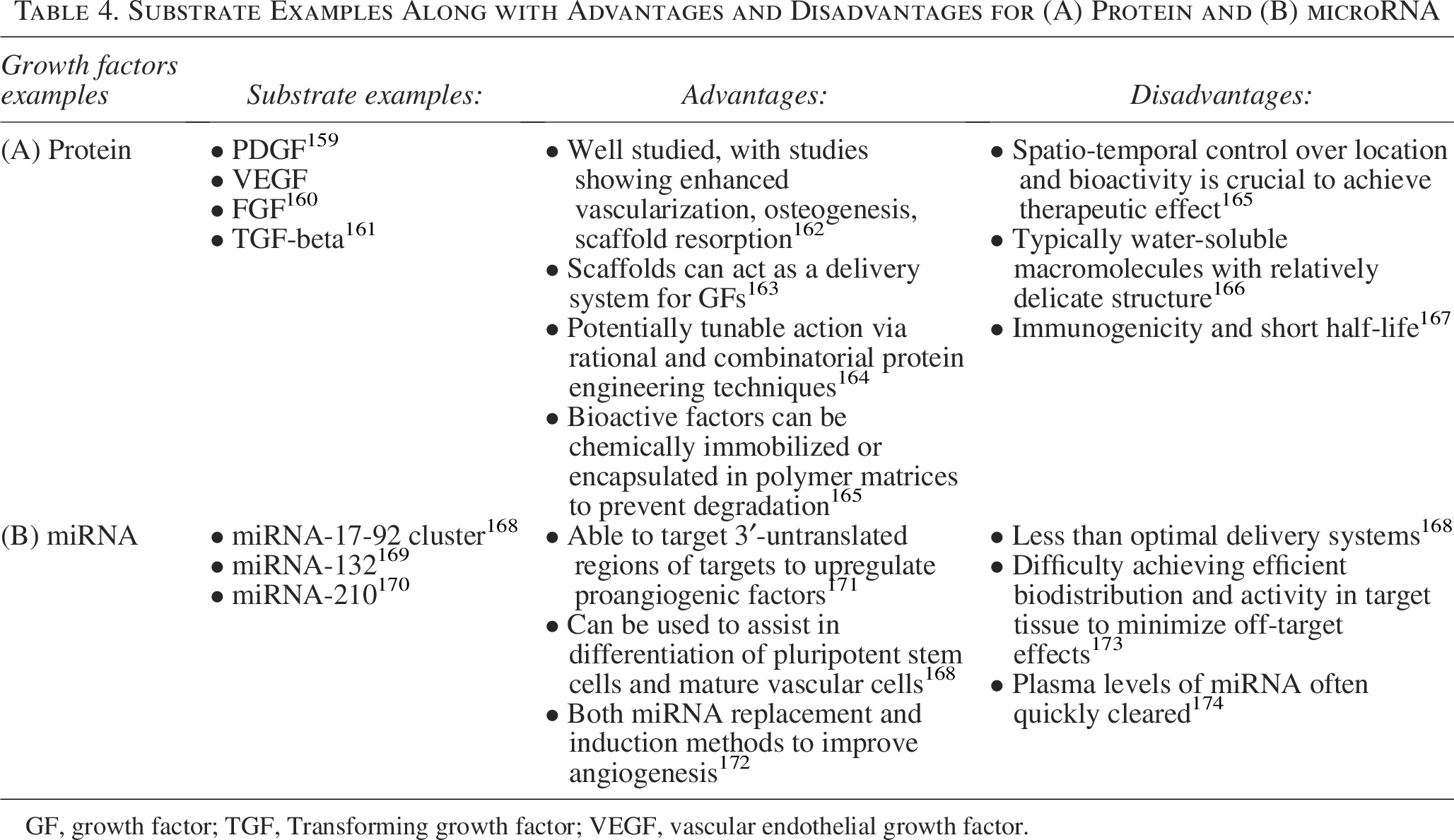
GF, growth factor; TGF, Transforming growth factor; VEGF, vascular endothelial growth factor.
miRNA
miRNA (Table 4B) plays a regulatory role in angiogenesis, influencing signaling pathways to encourage vascular growth. 194 For example, miRNA-503 overexpression in ECs enhances migration and proliferation by modulating cyclin E. 172 One study demonstrated how miRNAs regulate angiogenesis through NADPH oxidase-dependent mechanisms in ECs. 195
Cell-based approaches
Cell-based approaches, through cell seeding, coculturing, and cell-loaded micropatterning utilize cells to create functional constructs to aid in angiogenesis.
Cell seeding (Fig. 3D, Table 5A) of stem cells or ECs into scaffolds can promote vascularization following implantation.178,196,197 Scaffold porosity influences cell proliferation; larger pores aid vascularization but reduce mechanical strength.198–200 Seeding methods include: (1) passive, where cells are simply pipetted onto the scaffold, but unfortunately the yield is low (10–25%)201,202; (2) dynamic, using rotational or vacuum systems to enhance cell distribution coming at the expense of practicality and cell viability202–204 ; and (3) electrostatic, where cell adhesion is encouraged through surface charge but is cumbersome.202,205–207
Detailing Cell-Based Approach Examples, Cell Types, Advantages, and Disadvantages of Cell Seeding (A), Coculturing (B), and Cell-Loaded Micropatterning (C)

Coculturing (Table 5B) involves combining different cell types in vitro to mimic angiogenesis. Pericytes cocultured with ECs can induce BM development and recruit specific factors for capillary formation.208–210 Strategies also include preseeding scaffolds with cells and GFs, with some studies engineering cells to coexpress PDGF-BB and VEGF.211–213
Cell-loaded micropatterned (Table 5C) hydrogels represent an approach where elastomeric microdevices guide cells in building a microvasculature, offering the potential for creating tissue-specific microengineered vasculatures. 214
Guided Microvascular Development
Tissue vascularization is difficult to replicate in TE. 222 Postimplantation scaffold vascularization often lacks defined architecture, hindering tissue replacement. Creating patterned microvasculatures on scaffolds can support “like tissue with like tissue” replacement, crucial for scaling up TE. 223 Scaffold modulation with electromechanical cues and techniques like electrospinning and 3D printing help guide cells to replicate native tissues more accurately.224,225
Electromechanical cues
Electrical and mechanical stimulation plays a significant role in inducing hierarchical microvascular development (Fig. 5A).226–228 Scaffold modulation can mimic natural electromechanical cues and facilitate vascularization through methods such as cellular alignment, predefined vascular channels, and GF release.224,229–231

Guided microvascular development examples.
3D printing
3D printing allows for precise cell and biomaterial placement and has found utility in generating vasculatures with defined topology (Fig. 5B).231–233 Three basic requirements in microvascular bioprinting include: creation of hollow, endothelialized channels; biochemical and biophysical cues to induce endothelial sprouting; and flow-mediated conditioning for maturation. 191 Studies have demonstrated 3D-printed scaffolds seeded with stem cells can form new vascular networks that integrate with host tissue. 234
Electrospinning
Electrospinning employs electrostatic forces to generate fibrous scaffolds that aim to mimic native ECM and provide a conducive environment for vascular cell guidance (Fig. 5C). 235 Despite its precision, electrospinning has limitations with mechanical strength and cell density control compared with other techniques. 235 However, advancements have demonstrated its potential in vascular TE, such as electrospun vein grafts.236,237 Use of electrospinning in conjunction with cell seeding also has been shown to promote vascularization. 238 Unfortunately, with all these modalities, there exists difficulty in bridging the microvasculature to the macrovasculature.
Surgical Approaches to Bridge the Micro- and Macrovasculatures
Ideally, engineered tissue would be anastomosed directly to the recipient vasculature to restore perfusion. However, since this is not yet achievable, current attempts aim to create a proangiogenic environment at the recipient site and/or within the scaffold/graft/flap itself. 241 Until vascular ingrowth occurs (around 2 weeks), cellular hypoxia can be significant. 242 Consequentially, engineered tissues are limited in maximal achievable thickness by oxygen diffusion limitations (∼250 µm). 243 Many approaches and materials have attempted to integrate an anastomosable segment within a vascularized graft itself with varying degrees of success.244–246 Unfortunately, thrombosis is commonplace in small vessel replacements 247 requiring innovative microsurgical approaches to enhance connection between the micro- and macrovasculatures.
Arteriovenous loops
Surgical approaches to induce recipient capillary formation were first shown with arteriovenous loops (AVLs) (Fig. 6A). 248 AVLs utilize an expendable vein to connect the macrovascular arterial and venous systems. This deliberate fistula creates a unique microenvironment from which new capillaries can grow. It is believed that mechanical shear stress emanating from the AVL takes precedence in stimulating the neo-microvasculature,249,250 typically after 14 days. 251
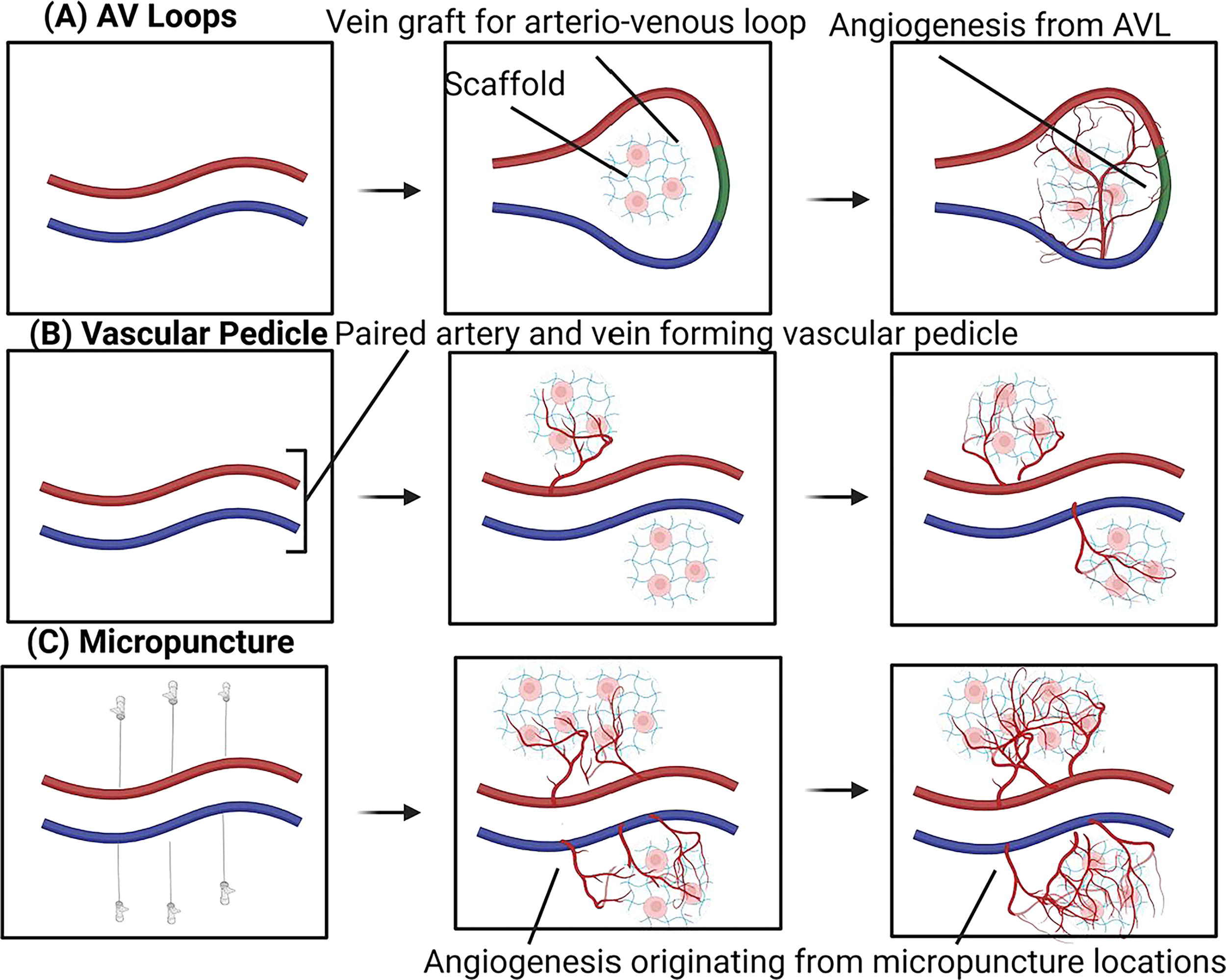
Surgical approaches to bridge the micro- and microvasculature. AVL
Plastic surgeons have historically used this approach to generate vascularized tissue in challenging clinical scenarios. 252 The thrombotic risk of traditional free-flaps using vein conduits was a significant impetus for AVL development. 253 When first used clinically, AVLs were characterized by a temporary end-to-side vein conduit that provided adequately mature vascular flow in preparation for flap transfer.254,255 Subsequently, the AVL was bisected and the surgeon was able to anastomose the flap outside of an ill-prepared recipient vasculature257,257 as seen in patients with trauma or atherosclerosis. 258 The risk-benefit profile of this approach has been thoroughly evaluated and deemed to be safe.259,260 Thus, it represents a verified microsurgical approach that can promote the vascularization of implanted biomaterials.
Most recently, AVLs have been explored for TE.250,261 For example, AVL placed within a polycarbonate chamber filled with fibrin showed enhanced angiogenesis. 262 AVLs placed within cross-linked collagen/glycosaminoglycan chambers resulted in a heavily vascularized tissue chamber with the formation of alpha-Smooth muscle actin (SMA)-positive arterioles. 263 This suggests the versatility of AVLs to induce vascularization in diverse biomaterials even within poorly vascularized native recipient tissues. 264 The success of AVLs with TE in the research arena has now been clinically translated for large bone defect reconstruction where AVLs were combined with cancellous bone grafts and fibrin scaffolds. 265
Unfortunately, some shortcomings exist with AVLs including the prolonged time (up to 12 weeks) required for a new and complete capillary network to develop,250,264,266 potential unwanted systemic hemodynamic manifestations of this deliberate fistula, and requisite microsurgical expertise to execute them.266,269,270
Vascular pedicles
Unmodified scaffolds are often difficult to vascularize secondary to limited GF supply (Fig. 6B). 271 To mitigate this, VPs have been utilized. In this approach, a large surface area of recipient macrovasculature (artery and/or vein) is placed in direct contact with the graft/flap/biomaterial that needs to be vascularized. While eliciting less vascularization than AVLs, 272 VP provides a technically simple proangiogenic surgical platform to build upon and is especially useful to those lacking microsurgical expertise. 273 Similar to AVLs, they can also be used alongside other engineered approaches, such as scaffold microchannels 273 and ASC seeding 274 with the pedicle facilitating voluminous vascularization 275 depending on the exact configuration.
Flow-through or ligated VPs were analyzed for their proangiogeneic potential in a murine model, and it was shown that flow-through VPs were associated with improved patency, angiogenesis, and tissue production. 276 Similar results were seen when VP was used to vascularize a collagen-chitosan scaffold to promote vascularized adipose formation. 277
Like AVLs, VPs have also been translated into clinical care already in a variety of settings for both simple wound repair 278 and more complex reconstructive approaches. 3D-printed biodegradable scaffolds were used in combination with corticoperiosteal flaps (CPF) for critical bone defect regeneration. In this study, a patient with a 36-cm tibial defect underwent intramedullary nail fixation and scaffold implantation, after which a flow-through CPF was placed within the scaffold. VP provided the impetus for scaffold vascularization that resulted in limb-salvage and functional restoration. Subsequently, Scanning electron microscopy confirmed the presence of vascularized bone. 279
The advantages of VP included relatively easy surgical execution, no systemic hemodynamic alterations, and verified clinical translation already. However, like AVLs, they suffer from deferred angiogenesis 280 and the inability to achieve/restore prompt blood flow to the adjacent implant. This has led to newer microsurgical approaches being developed in an attempt to promote rapid angiogenesis.
Micropuncture
With both AVLs and VPs there exists an angiogenic delay, likely because of time-limited BM breakdown of the vessel wall that is necessary prior to EC sprouting and new luminal formation (Fig. 6C). We recently hypothesized that this enzymatic degradation process could be mechanically expedited by puncturing the targeted macrovasculature. In micropuncture (MP), we use 30–100 μm diameter needles to generate precise microperforations in the recipient vascular segment just prior to collagen scaffold implantation. These MP “mother” vessels permit immediate cellular extravasation and microvascular outgrowth without themselves suffering thrombosis or significant hemorrhage. 281 When combined with modified scaffolds, microvascular development can be further controlled through this unique surgical bioengineering approach. 155
The MP technique has not been applied clinically as we just recently described the approach. However, the potential limitations include bleeding and thrombotic risk to the underlying vasculature. Bleeding would be more of an issue with arterial MP while thrombotic risk would likely be more troublesome with venous MP. Larger animal studies are needed to see how this could be scaled up from murine models to patients. As currently performed, MPs are placed within a VP to allow for adjacent graft/scaffold vascularization. It will be interesting to see if MPs within AVLs would have a synergistic effect on promoting scaffold vascularization and studies are ongoing.
All three surgical approaches demonstrate the possibility of modulating angiogenesis through a combination of microhemodynamic alterations and/or inflammation. Both processes have been described in the past as critical to new capillary growth. Because the surgical approaches described are highly modifiable; they may find a niche not just for reconstructive surgery and tissue engineering but also for the entire gamut of ischemic disease.
Building Tissue-Specific Vasculature
Tissue and organ regeneration have significant unmet needs. While advancements have been made, the goal to build rapidly perfusable tissues or organs to aid in reconstruction is still limited. Here, we provide a brief overview of the impact and residual challenges microvascular bioengineering has for tissue and organ replacement.
Reconstructive surgery
Skin
Limitations in skin graft availability and donor site morbidity have led to engineered substitutes ranging from acellularized biomatrices to synthesized materials. Unfortunately, these substitutes still cannot recreate the native skin microvasculature thereby limiting true skin functionality (Fig. 7A).283,284 Achieving organized vascularization in skin substitutes remains challenging (Fig. 7B).285–288
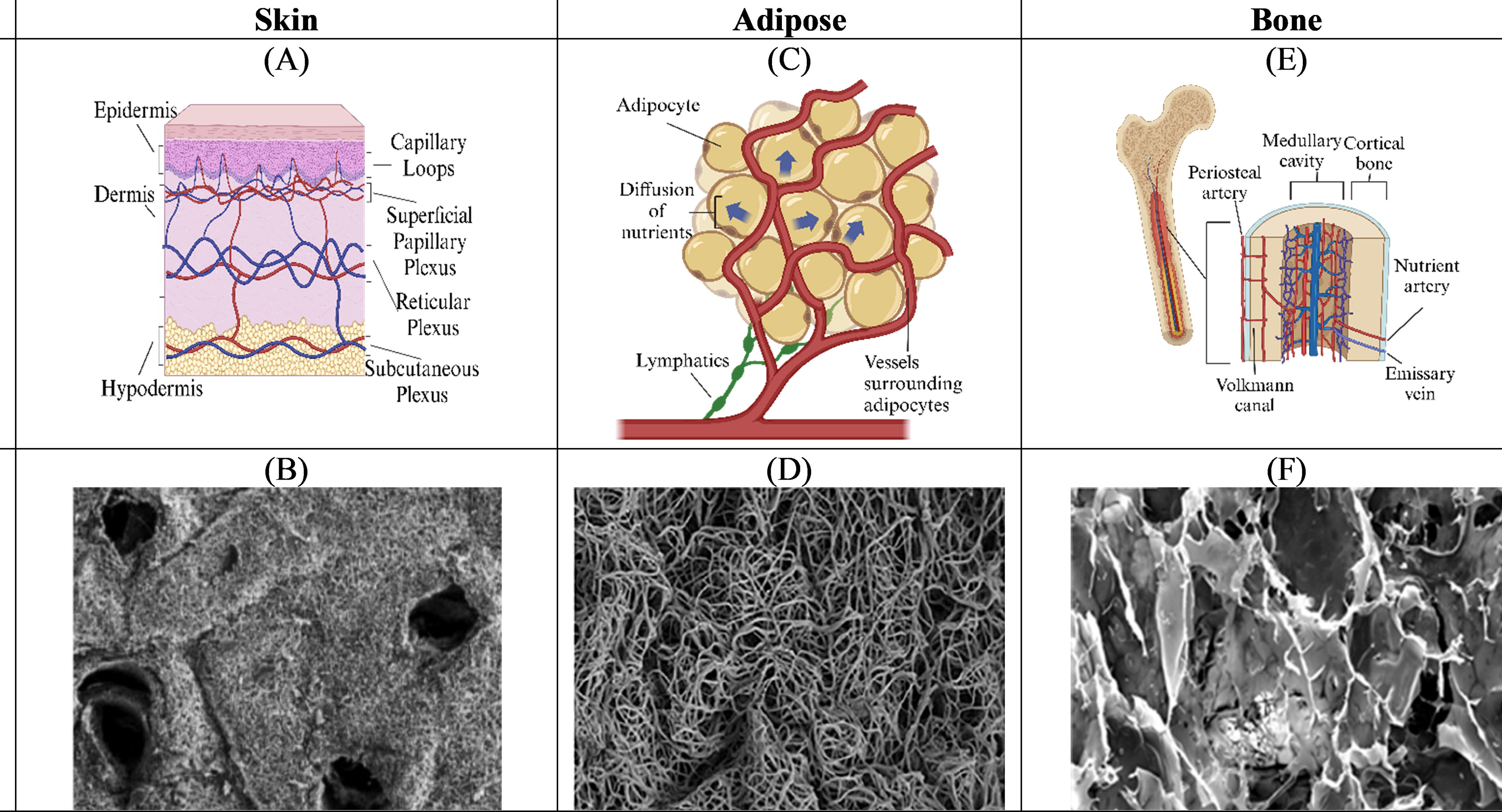
Skin native vasculature
Adipose
The role of fat grafting is well established. However, voluminous reconstruction is still precluded by poor vascularization.288–290 As native adipocytes develop in parallel to vascular networks (Fig. 7C), emerging approaches in vascularized adipose engineering employ synthetic, natural, and ECM-based scaffolds (Fig. 7D).291–294 Vascularized adipose TE has had varying success in concurrently promoting angiogenesis and tissue regeneration295–302 ; however, challenges still persist.303–305
Bone
Successful bone reconstruction depends on effective vascularization and the nutrient artery is vital (Fig. 7E).43,306,307 Diversity in bone structure and tensile force requirements present additional challenges in bone TE. 3D-printed scaffolds and cell seeding have demonstrated variable effectiveness in concurrently promoting microvascular formation and osteogenic differentiation.308–310 Despite advancements, clinical translation remains challenging (Fig. 7F).
Transplant surgery
Liver
End-stage liver disease causes two million deaths annually 314 with transplantation being the primary treatment. Organ scarcity mandates TE solutions.314,315 Liver engineering is particularly challenging because of its unique vascular and sinusoidal network, crucial for filtration and metabolism (Fig. 8A). Techniques such as decellularization and recellularization (Fig. 8B) have shown promise, but are limited by thrombosis and immune reactions. Bioprinting and other methods are also currently being explored to create functional hepatic microvasculature.316–319
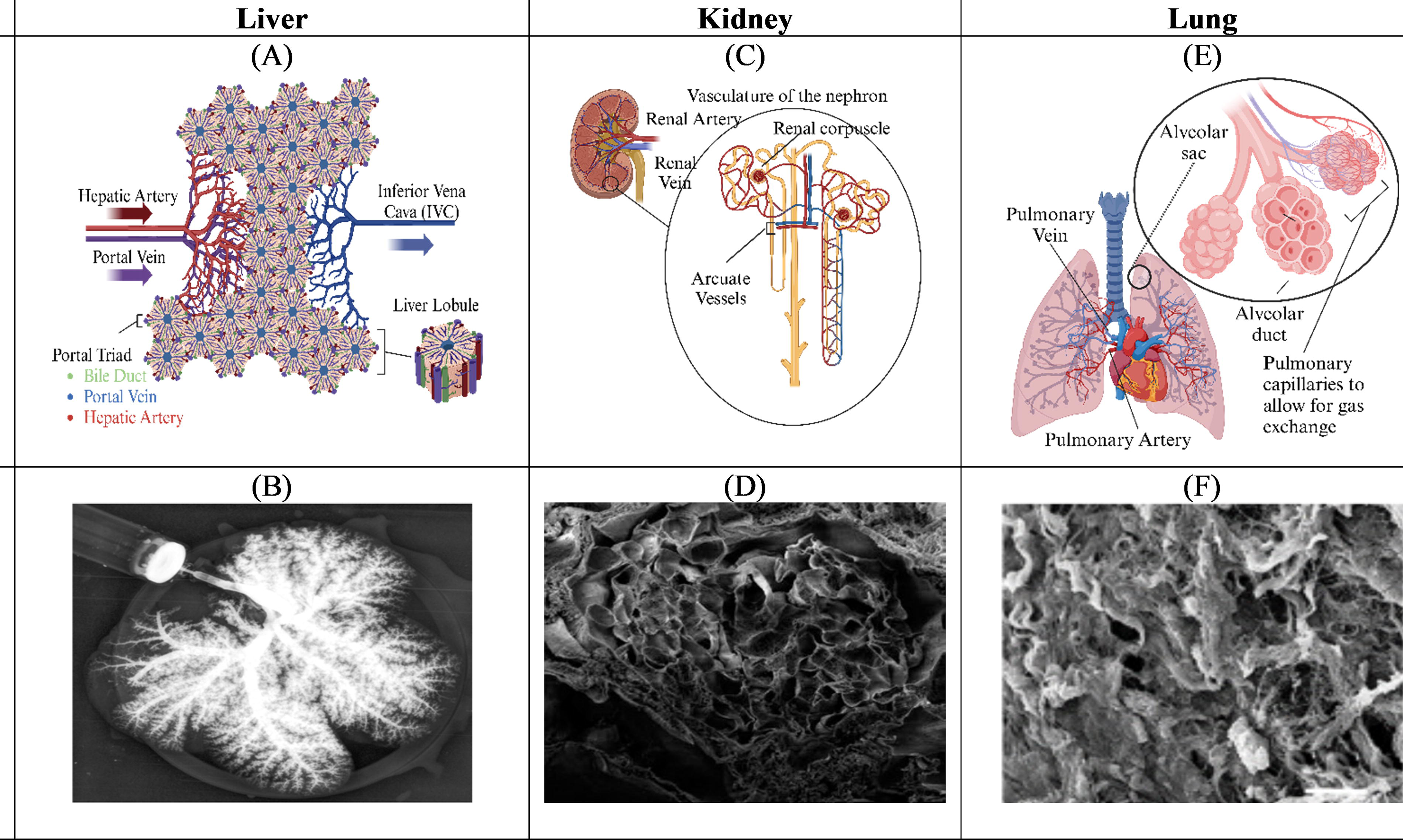
Liver native vasculature
Kidney
Kidney transplants are a solution for end-stage renal disease but also suffer from donor scarcity. The dense and complex renal microvascular network (Fig. 8C) poses unique TE challenges as the resultant vasculature needs to not only accommodate 20% of cardiac output but also mitigate renin release and filter blood.53,320 Despite promising advances (Fig. 8D), long-term functionality and thrombosis remain significant obstacles.53,320–334
Lung
Lung engineering is complicated by the need to replicate a dual circulatory system for effective gas exchange (Fig. 8E). Decellularized scaffolds have been a primary focus, with experiments demonstrating the potential for gas exchange in recellularized lungs (Fig. 8F). However, challenges such as recreation of a functional alveolar-capillary barrier persist, underscoring the need for continued research.57,59,335–347
Conclusion and Future Directions
Despite significant advances in TE, vascularization remains an obstacle in creating truly functional tissue. Because of tissue and organ-specific nuances at the microvascular level, customization is warranted depending on tissue type. Innovative combinatorial engineering and surgical approaches may hold promise in solving the challenges intrinsic to tissue and organ microvascular fabrication.
Authors’ Contributions
D.J.R. conceived the research topic and oversaw the direction, planning, writing, and editing. K.S. performed the literature review and was the primary writer. K.S., M.A., D.A.F.-A., J.C.E.-M., O.W., J.D., S.A., and M.E.L.: all provided critical feedback and editing.
Footnotes
Funding Information
NIH-1R56HL157190-01 (D.J.R.), Dorothy Foehr Huck and J. Lloyd Huck Endowed Chair of the Pennsylvania State University (D.J.R.), Comprehensive Health Studies Collaborative Program Award of the Penn State College of Medicine (D.J.R.).
Disclosure Statement
Authors have no conflict of interest to disclose.