
Abstract
Severe skeletal muscle injuries involving substantial tissue loss can significantly impair muscle strength and functionality, reducing the quality of life for affected individuals. Such injuries, termed volumetric muscle loss, require extensive clinical intervention, as the body’s innate healing mechanisms are insufficient to regenerate functional muscle. The current standard of care primarily involves autologous muscle tissue transfer, with some consideration of acellular synthetic constructs. However, both approaches have limited therapeutic efficacy, presenting challenges such as donor-site morbidity, infection risks, and suboptimal functional recovery. Over the past decade, skeletal muscle tissue engineering (SMTE) has emerged as a promising strategy for regenerating functional muscle through bioengineered constructs. Advanced biofabrication techniques, including bioprinting, have further enabled the development of synthetic constructs that closely mimic native muscle architecture. Given these advancements, a critical review of recent therapeutic strategies, their achievements, and limitations is necessary. This review examines the spectrum of bioengineered constructs developed from various biomaterials and evaluates their therapeutic potential. Special emphasis is placed on 3D bioprinting strategies and their role in creating physiologically relevant constructs for functional muscle restoration. In addition, the integration of machine learning in optimizing construct design, predicting cellular behavior, and enhancing tissue integration is discussed. The review indicates that despite significant progress in SMTE, key challenges remain, including replicating the complex structural organization of muscle tissue, minimizing fibrosis, and achieving vascularization and innervation to regenerate functional, strengthened muscle. Future research should address these barriers while prioritizing the development of translational, clinically relevant regenerative constructs. In addition, efforts should focus on advancing scalable, construct-based regenerative treatments that are readily available at the point of care and easily managed in surgical settings.
Impact Statement
This review highlights key advancements in skeletal muscle tissue engineering (SMTE) for treating volumetric muscle loss (VML), a condition that severely impairs muscle function and quality of life. By exploring the advancements in bioengineered constructs and the role of 3D bioprinting, this review underscores innovative strategies that closely replicate native muscle tissue, offering new prospects for functional muscle regeneration. In addition, the review discusses machine learning integration in SMTE to optimize construct design and predict cellular behavior, presenting a promising avenue for developing constructs with high therapeutic value. This review also highlights essential insights into the existing limitations in constructs and proposes future directions that should be undertaken to advance construct-based regenerative medicine toward more effective and clinically viable solutions in VML therapy.
Keywords
Introduction
As per the Global Burden of Disease 2019 data, musculoskeletal conditions affect 1.71 billion people globally, almost 25% of the world’s population.1,2 These conditions lead to 17% of global disability-adjusted life years and cost $1 trillion annually in treatment. In the United States, musculoskeletal disabilities affect over 57 million people, making up 20% of all disability claims and resulting in an economic impact of over $213 billion annually. 3
Among the leading causes of musculoskeletal disabilities are injuries and trauma to skeletal muscle, particularly volumetric muscle loss (VML)—a condition characterized by significant loss of skeletal muscle tissue, resulting in severe functional impairment and disability. 4 VML commonly arises from high-impact trauma, including vehicular accidents, major falls, gunshot wounds, and explosive injuries, and is often associated with open fractures or compartment syndrome. 5 While VML is most prevalent in military personnel due to battlefield injuries, it also affects civilians through gunshot wounds, severe road accidents, major falls, or tumor ablation procedures.
Skeletal muscle is a highly organized and complex tissue composed of long, cylindrical myofibers bundled into fascicles (Fig. 1A). While minor muscle injuries can heal through endogenous repair mechanisms, VML disrupts these processes, preventing functional muscle regeneration. This failure is primarily due to the loss of satellite cells (SCs) and the extracellular matrix (ECM), both essential for tissue repair and structural organization. 6 In addition, the extensive loss of native muscle tissue eliminates critical regenerative cues needed to guide cellular responses during healing. 7 Some studies suggest that following VML, a prolonged presence of macrophages in an intermediate (M1-to-M2) phenotype leads to excessive ECM deposition rather than muscle fiber regeneration, resulting in scar formation.8,9 This scar/fibrotic tissue impedes SC migration and angiogenesis, compromising muscle repair. Moreover, scar tissue can obstruct the reformation of neuromuscular junctions (NMJs), which are often damaged in VML injuries10–15 (Fig. 1B). Since NMJs are essential for muscle function and development, their disruption further exacerbates impaired regeneration. VML also results in the loss of mitochondria-rich skeletal muscle cells, leading to a decline in oxidative metabolic activity and overall metabolic imbalance. Since mitochondria function as calcium sinks, an increase in cytosolic calcium levels can overwhelm mitochondrial calcium buffering capacity, disrupting mitochondrial function and compromising cell viability; this cascade further exacerbates muscle regeneration deficits. 16
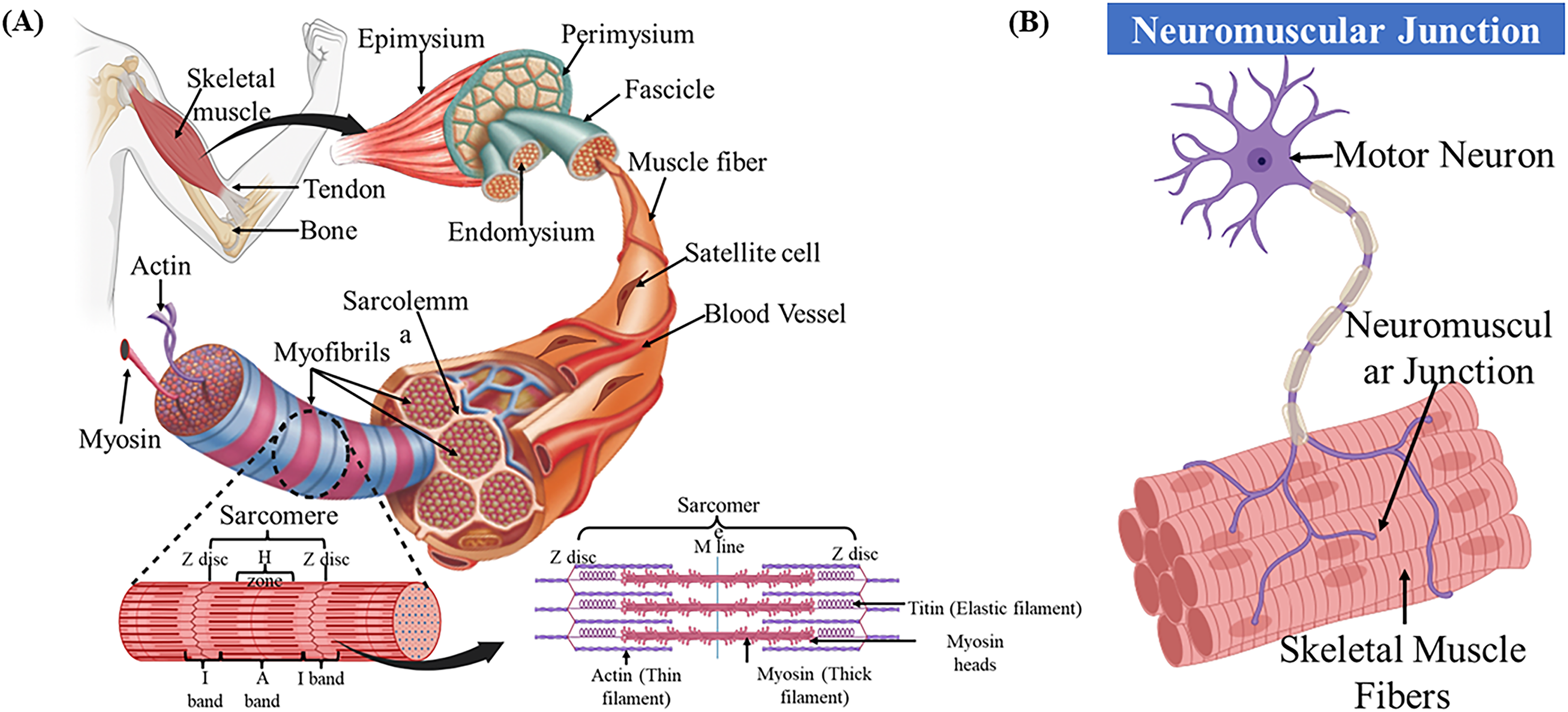
Schematics showing the
Consequently, the pathophysiological events following VML create a highly challenging environment for endogenous muscle repair, resulting in severe loss of muscle strength and functionality. In severe cases, these deficits can lead to long-term disability or even necessitate limb amputation.10–13
Treating VML injuries remains a significant challenge due to the complex biological processes involved in muscle regeneration. The current standard of care is autologous tissue transfer, or muscle grafting, which involves transplanting a muscle flap from a healthy donor site to the injured area.4,10 However, this approach has several limitations, including limited donor tissue availability, risk of graft infections, and potential transplanted tissue necrosis. 17 In addition, achieving full muscle restoration with adequate vascular integration and innervation remains difficult, often resulting in persistent functional deficits, reduced muscle strength, and impaired mobility.18,19
To assist patients with mobility, advanced bracing strategies have been developed. However, these devices become a permanent part of a patient’s life and are primarily designed for lower extremity VML injuries, making them less suitable for upper extremity impairments. Meanwhile, rehabilitation approaches, although beneficial, are largely ineffective as a stand-alone treatment and are most effective when combined with physical therapy regimens following muscle grafting surgeries to enhance muscle function and strength.
To address these limitations, skeletal muscle tissue engineering (SMTE) has emerged over the past decade as a promising strategy. SMTE leverages bioengineered constructs to enhance muscle regeneration and restore function in VML injuries. 20 These constructs provide a three-dimensional (3D) support structure that mimics the native tissue microenvironment, promoting cell growth, differentiation, and functional integration. 21 SMTE integrates biomaterial science, cellular and molecular biology, and bioengineering to drive the development of advanced bioengineered constructs for de novo skeletal muscle regeneration. 22
Therapeutic strategies in SMTE are categorized into in situ, in vivo, and in vitro approaches 20 (Fig. 2). In situ tissue engineering involves implanting acellular constructs at the injury site to stimulate endogenous regenerative mechanisms. 23 In vivo approaches use cell-laden constructs implanted directly into the injury site, 24 while in vitro strategies involve developing, culturing, and maturing tissue-engineered muscle grafts (TEMGs) before implantation.20,23 In the past decade, notable developments have been made in all three strategies.25,26 Notably, the SMTE field has seen significant advancements in biofabrication strategies, with 3D bioprinting emerging as a powerful tool for developing constructs replicating complex muscle anatomy, aiding the restoration of functional neo-muscle.
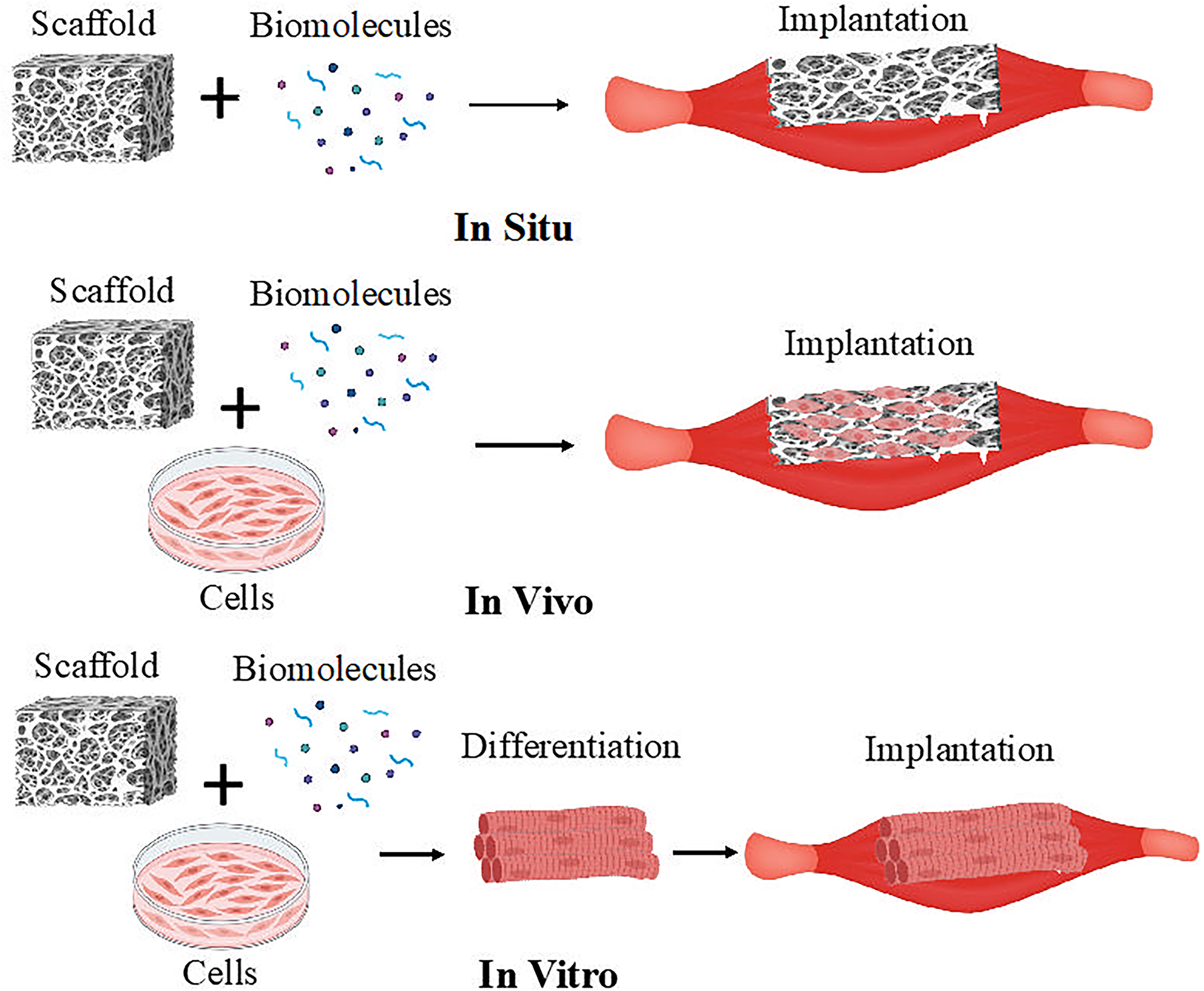
Schematic showing the strategies for skeletal muscle tissue engineering.
Given the substantial improvements in SMTE, this review provides a comprehensive overview of bioengineered constructs for VML. The discussion extends to the potential applications of artificial intelligence and machine learning (ML) in selecting biomaterials and optimizing construct manufacturing. Finally, the review highlights the current limitations, discusses the prospects within the SMTE field, and the essential advancements needed in regenerative medicine for VML injuries.
Regenerative Constructs in SMTE
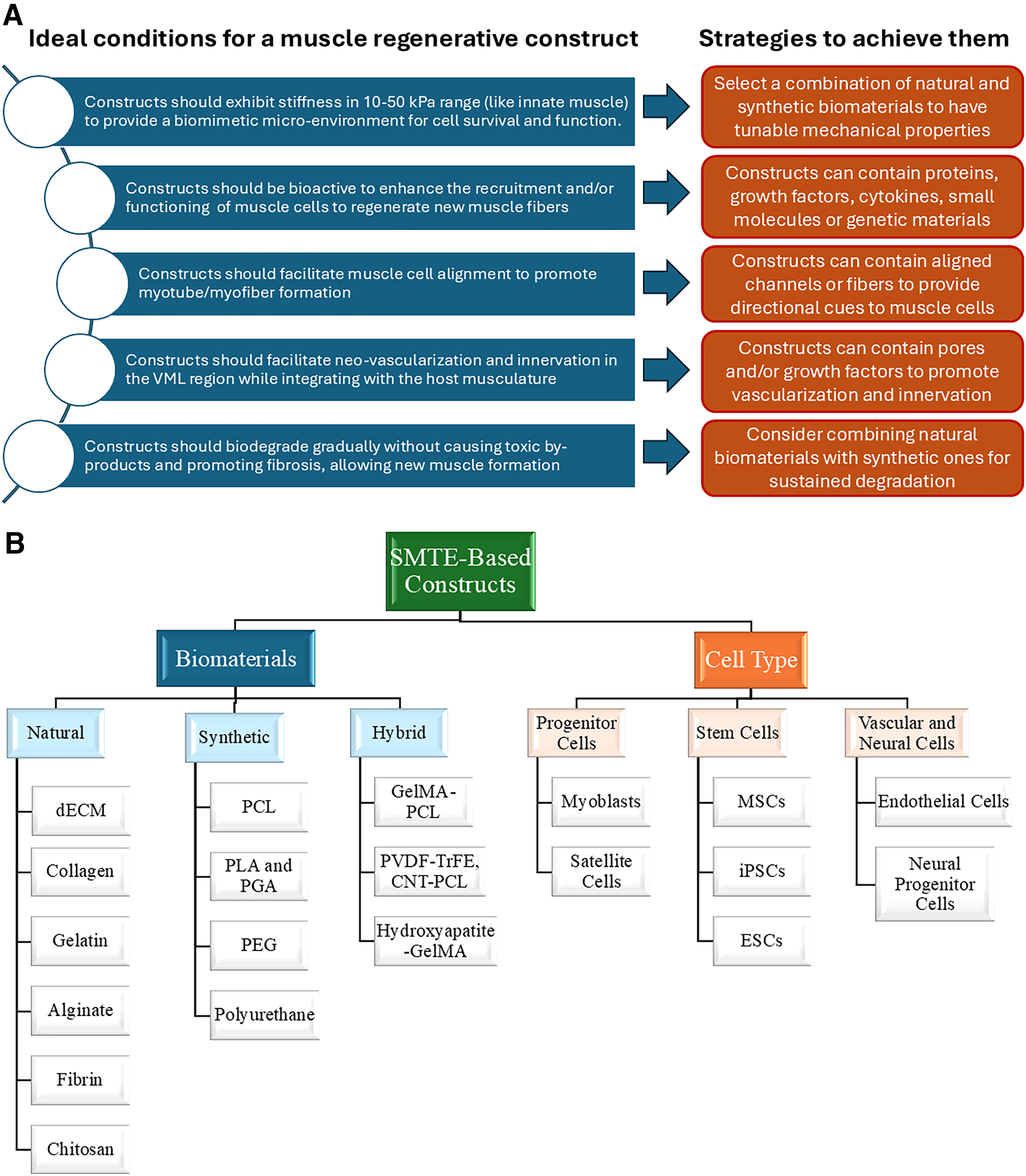
Regenerative constructs for VML aim to restore damaged or lost muscle tissue by promoting regeneration and tissue growth. These constructs typically incorporate biomaterial-based scaffolds, stem cells, growth factors, and gene therapies to activate the muscle cells’ natural repair mechanisms or enhance the regeneration cascade of the transplanted cells. By providing a supportive environment that mimics native muscle architecture and composition, constructs facilitate the regeneration of muscle fibers. The ideal design of a construct suitable for functional muscle regeneration and some strategies to achieve the design are illustrated in Figure 3A. Figure 3B summarizes the biomaterials and cell types commonly used in SMTE-based constructs. The following sections discuss in detail the three main categories of constructs that have been developed to regenerate skeletal muscle.
Acellular constructs
Acellular constructs are developed using biomaterials designed to stimulate the endogenous repair mechanisms, forming new muscle fibers. 20 Specifically, these constructs are bioengineered with biophysical and/or biochemical cues to replicate the native ECM, creating a microenvironment that modulates host cell behavior and initiates the regeneration cascade. 27 One of the most significant advantages of this strategy is that the construct fabrication process is simple, eliminating the need to incorporate cells into the constructs, which leads to faster production, improved delivery, simplified storage, and reduced regulatory constraints compared with cell-laden constructs or TEMGs. 28
Selecting the right biomaterials is critical for developing effective regenerative acellular constructs. Biomaterials must possess specific mechanical, chemical, and biological properties that impact the strength, durability, degradation, and regenerative potential of the constructs. In SMTE, natural biomaterials such as collagen, fibrin, alginate, gelatin, chitosan, silk fibroin, hyaluronic acid (HA), laminin, agarose, and keratin are commonly used29–32 (Fig. 3B). Among these, decellularized ECM (dECM), sourced from the tissues such as small intestinal submucosa and urinary bladder matrix is a prominent choice in SMTE. Table 1 provides an overview of studies that have used dECM as the primary material for acellular constructs in muscle regeneration. The table also includes other natural biomaterials used to make acellular constructs. Overall, natural biomaterials are appealing due to their bioactive components that mimic the native ECM, fostering cell growth, differentiation, and maturation. 28 Moreover, they are biodegradable, with their degradation by-products typically not exhibiting cytotoxic effects. 45 However, sourcing and preparing natural biomaterials can result in batch-to-batch inconsistencies, potentially triggering immune reactions.46,47 In addition, natural constructs often suffer from low strength and durability, and they cannot be modified to enhance these properties. 48
Strategies for Developing Acellular Constructs for Skeletal Muscle Tissue Engineering

ECM, extracellular matrix; dECM, decellularized ECM; VML, volumetric muscle loss; SIS, small intestinal submucosa; UBM, urinary bladder matrix; SC, satellite cell; MHC, myosin heavy chain; TGF, transforming growth factor.
On the contrary, synthetic biomaterials offer tunable strength and durability, making them well-suited for SMTE applications. These materials can be engineered to achieve specific mechanical properties, such as stiffness, which can better mimic native skeletal muscle tissue. 49 Common synthetic biomaterials include poly lactic-coglycolic acid (PLGA), polyethylene glycol (PEG), polypropylene, poly lactic acid (PLA), polyglycolic acid (PGA), and polyurethane (PU) (Fig. 3B).50–53 Synthetic materials offer better batch consistency and greater control over mechanical properties, but they are typically bioinert, lacking the bioactive components necessary to modulate cell behavior. To address this, synthetic materials often require functionalization or modification to enhance properties such as cell adhesion, proliferation, and differentiation. In the past two decades, hybrid biomaterials combining natural and synthetic components have been developed, offering improved mechanical properties, bioactivity, and biocompatibility.
Although acellular constructs show promise, they often lead to fibrosis rather than the formation of functional muscle fibers. 54 This is partly due to a prolonged M1 macrophage response, as shown in Figure 4. Aurora et al. 40 indicated that the macrophage response transitioned to the M2 phenotype over time but did not yield substantial muscle repair. Similarly, Corona and Greising 55 highlighted that acellular scaffolds limit the migration of SCs, such as Pax7+ cells, which are essential for functional muscle regeneration. While some studies suggest that acellular scaffolds can promote neo-muscle formation, substantial evidence indicates that they are insufficient for regenerating fully functional muscle in VML injuries, mainly because they do not adequately support vascularization and NMJ formation due to excess fibrosis.10,55 Vascularization is crucial for supplying nutrients and oxygen to regenerating muscle tissue, ensuring the viability and function of newly formed muscle fibers. Muscle regeneration is limited without proper blood vessel formation, leading to impaired healing and reduced functional outcomes.56,57 Reinnervation is equally essential, as the formation of NMJs enables the muscle fibers to contract and function effectively. Muscle regeneration fails to integrate with the nervous system without functional innervation, impairing mobility and strength. 58 Vascularization and reinnervation are key to restoring the structural integrity of muscle tissue and its functionality, ensuring that newly formed muscle fibers can contract and contribute to movement. 59 Future research should focus on developing next-generation acellular constructs that enhance SC migration, vascularization, and NMJ formation at the injury site. In addition, constructs should biodegrade at a rate that supports muscle remodeling in the injured region.
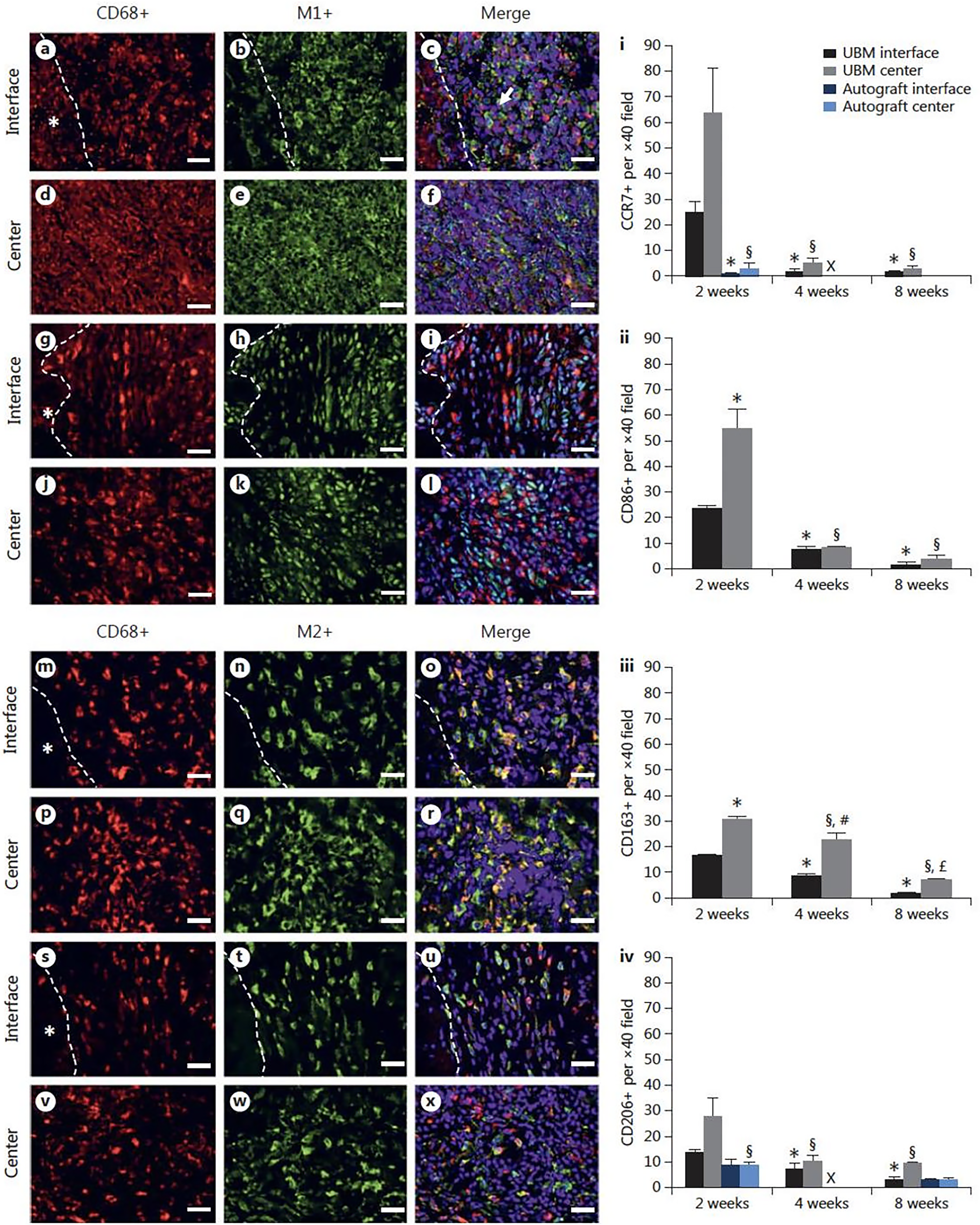
The porcine urinary bladder matrix (UBM) scaffold induced a prolonged proinflammatory (M1) macrophage response, as shown by immunohistological staining for pan macrophages (CD68+, red), M1 macrophages (CCR7+, CD86+, green), and M2 macrophages (CD163+, CD206+, green) in the tibialis anterior (TA) muscle defect repaired with the UBM scaffold. The interface and center of the repair were analyzed at the 2-week mark, revealing the scaffold exhibiting a dominant M1 response that persisted longer than expected, thereby hindering muscle regeneration. The defect was analyzed using immunohistological staining for pan macrophages (red) (CD68+), M1 macrophages (green) (CCR7+: a–f; CD86+: g–l), and M2 macrophages (green) (CD163+: m–r; CD206+: s–x). White dashed lines indicate the approximate interface along the remaining muscle mass (*) and the porcine UBM scaffold. Scale bars = 50 μm (magnification: 400×). Quantitative analyses of the spatiotemporal macrophage response are also shown (i–iv). Two regions were included in the analysis: the interface of the injured muscle and respective repair and the center of the respective repair. Means ± SEM. n = 3 muscles/group. *p < 0.05 versus UBM interface (2 weeks); §p < 0.05 UBM center (2 weeks); #p < 0.05 versus UBM interface (4 weeks); £p < 0.05 versus UBM interface (8 weeks). X indicates that no measurements were made for the autograft at the 4-week time point. Figure reprinted with permission from authors. 40
In summary, acellular constructs offer key advantages, including immune compatibility, off-the-shelf availability, and faster production due to their simple fabrication process. However, they lack the cellular components necessary for immediate regeneration, leading to slower integration and functional recovery. In addition, without bioactive modifications, these constructs are prone to scar tissue formation, hindering muscle regeneration.
Cell-laden constructs
Cell-laden constructs offer a promising approach to functional muscle restoration by introducing transplanted cells in the VML region. Given that VML injuries result in the loss of SCs in the surrounding tissue, incorporating exogenous cells into bioengineered constructs can facilitate tissue regeneration and remodeling.29,55 The transplanted cells compensate for the lost or damaged muscle cells and contribute to regeneration by modulating the microenvironment through paracrine signaling. This signaling helps recruit host cells, regulate immune responses, and promote myogenesis, thereby accelerating the formation of new muscle fibers.60,61 Furthermore, biomaterial-based delivery systems or constructs can influence cell fate by maintaining stemness and directing differentiation, ultimately aiding in the formation of functional skeletal muscle.
Several studies have demonstrated the superior regenerative potential of cell-laden constructs compared with acellular scaffolds. For instance, Conconi et al. 62 engineered constructs seeded with autologous myoblasts and compared their efficacy against acellular scaffolds in a rodent model. Over 30 days, the myoblast-seeded constructs exhibited substantial vascularization and retained structural and functional integrity for an additional month, whereas the acellular constructs were encapsulated by fibrotic tissue. In another study, Qiu et al. 63 investigated using porcine heart ECM combined with human umbilical cord mesenchymal stem cells (MSCs) for treating tibialis anterior muscle defects in rodents. Constructs seeded with MSCs exhibited superior functional recovery, as evidenced by increased isometric torque measurements at 4 and 8 weeks postimplantation compared with MSCs or ECM alone. The MSC-seeded constructs also facilitated macrophage polarization toward the M2 phenotype, activated SCs, and promoted robust myofiber formation. After 8 weeks, the ECM+MSC-treated group demonstrated complete muscle regeneration with restored muscle architecture (Fig. 5B–D), whereas treatments with only MSCs or ECM resulted in only partial mitigation of muscle atrophy. In addition, mechanical function recovery was significantly enhanced in the ECM+MSC-treated group, as shown by improved force generation at 1 month (Fig. 5E) and 2 months (Fig. 5F) postimplantation.
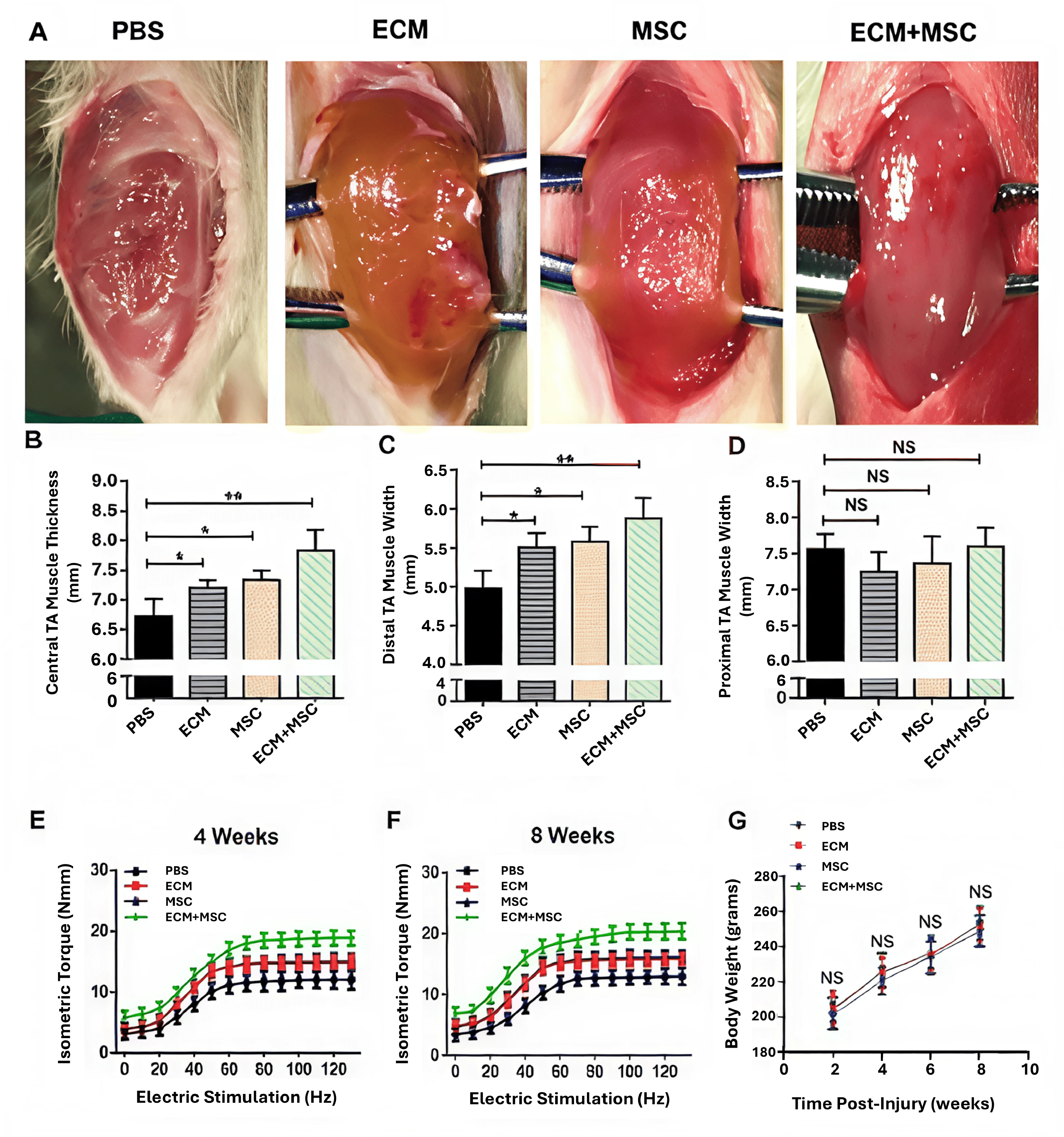
Gross morphology and functional evaluation of TA muscle after volumetric muscle loss (VML) injury and repair.
Cell-laden constructs also actively support revascularization and immunomodulation in addition to forming new muscle fibers. This can be achieved by incorporating multiple cell types in the constructs and transplanting them to the injury site. For instance, various cell types, including C2C12 muscle cells, skeletal myoblasts, adipose-derived stem cells, MSCs, endothelial cells (ECs), and regulatory T cells, have been incorporated into constructs to enhance neovascularization, promote functional integration, and improve regenerative outcomes.64–66 However, very few studies focus on reestablishing the NMJs with cell-laden constructs, critical for improving functional recovery in the newly formed muscles. Table 2 summarizes key studies that have utilized cell-containing constructs for VML treatment.
Cell-Laden Construct Strategies for Volumetric Muscle Loss Treatment
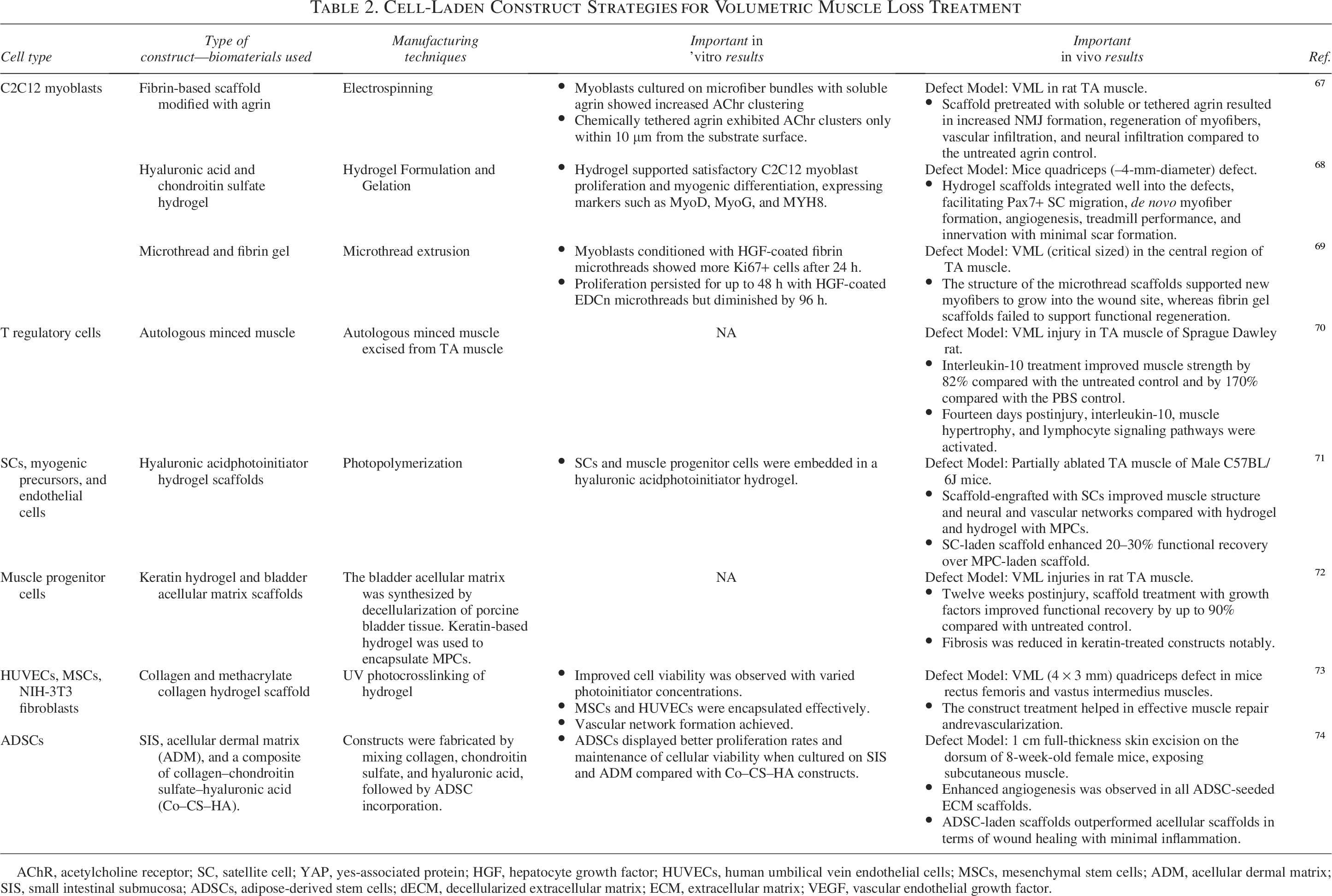
AChR, acetylcholine receptor; SC, satellite cell; YAP, yes-associated protein; HGF, hepatocyte growth factor; HUVECs, human umbilical vein endothelial cells; MSCs, mesenchymal stem cells; ADM, acellular dermal matrix; SIS, small intestinal submucosa; ADSCs, adipose-derived stem cells; dECM, decellularized extracellular matrix; ECM, extracellular matrix; VEGF, vascular endothelial growth factor.
While cell-seeded constructs significantly enhance muscle recovery by improving cell engraftment and stimulating regeneration post-VML injury, several challenges remain. A primary limitation is maintaining long-term cell viability and function within the implanted construct. In addition, achieving a balance between multiple incorporated cell types—such as myogenic, endothelial, and neural cells—is complex yet necessary for promoting angiogenesis, myofiber maturation, and NMJ formation. Future research should focus on developing biomaterials capable of sustaining cell encapsulation while guiding cellular behavior toward the rapid restoration of vascularized and innervated muscle.
Overall, cell-laden constructs represent a transformative approach to skeletal muscle regeneration, offering active SCs that support myogenesis, angiogenesis, and faster integration with host tissue. These constructs better mimic native skeletal muscle architecture and can be customized for VML injuries. However, challenges such as limited cell viability, potential immune rejection, and the complexities of biomanufacturing and storage must be addressed to maximize their clinical potential. Future advancements should prioritize scalable, biocompatible, and functionalized constructs that ensure long-term cell survival and orchestrate a regenerative response.
Prematured tissue constructs/TEMGs
In this strategy, synthetic muscle grafts are developed in vitro and then implanted into the defects. This process begins with incorporating cells into 3D constructs, supplemented with relevant growth factors and cultured under controlled conditions to promote cellular expansion and differentiation. 75 Through a combination of biochemical and biophysical stimuli, these cells are guided to mature into myotubes or myofibers, forming TEMGs capable of integrating with host tissue postimplantation. 76 Table 3 highlights key studies that have developed TEMGs for SMTE.
Tissue-Engineered Muscle Graft Strategies for Volumetric Muscle Loss Treatment
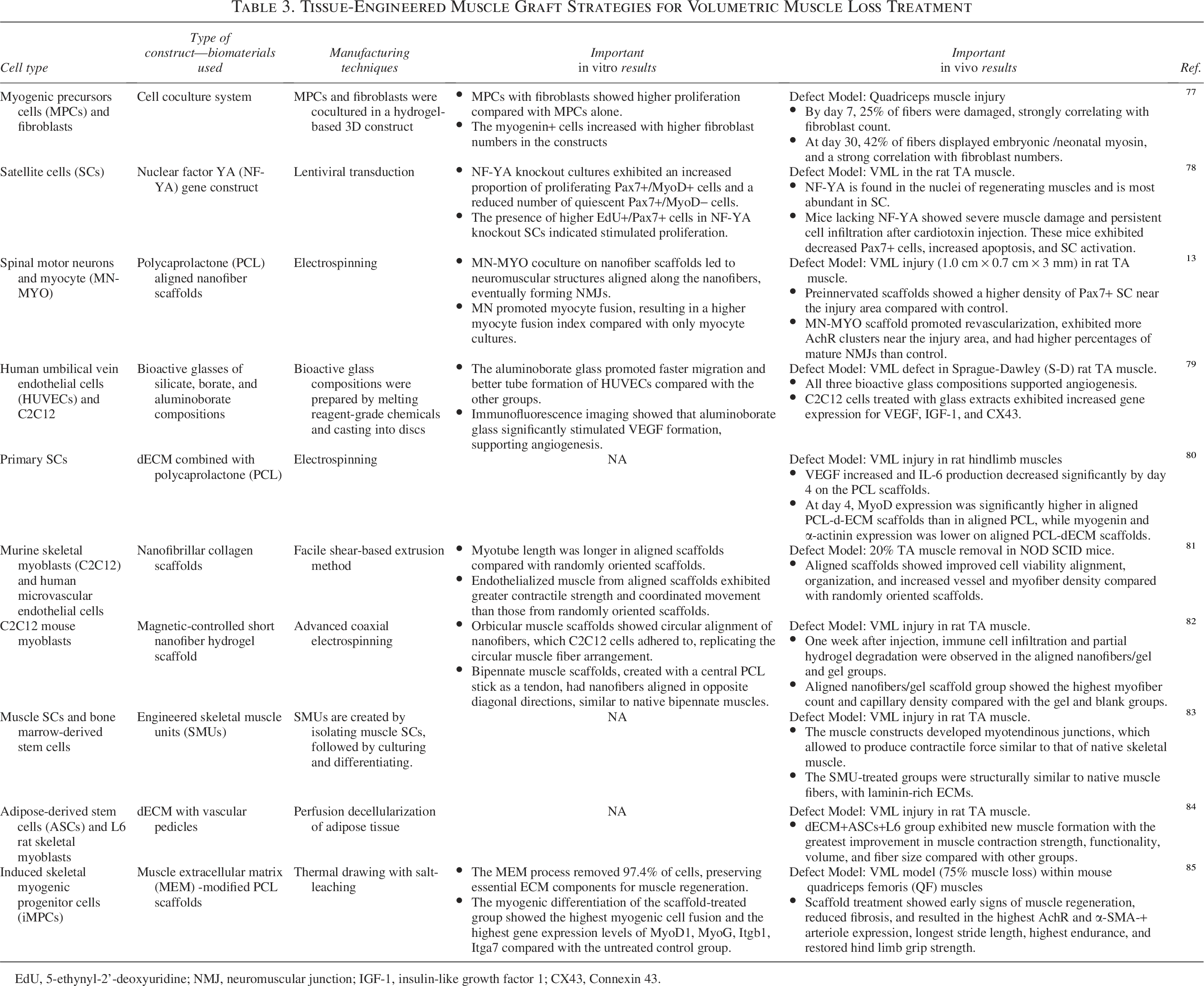
EdU, 5-ethynyl-2’-deoxyuridine; NMJ, neuromuscular junction; IGF-1, insulin-like growth factor 1; CX43, Connexin 43.
The scaffold or construct within TEMGs is crucial in establishing a microenvironment conducive to cell survival, differentiation, and functional tissue regeneration. Ideally, these constructs should be biodegradable, allowing progressive cellular remodeling into mature muscle fibers—a fundamental requirement for effective muscle regeneration.86–90 Natural biomaterials, particularly dECM, are promising candidates for TEMGs due to their ability to retain native biochemical and structural cues, which support cellular attachment, differentiation, and tissue organization.91–93 Specifically, dECM preserves essential bioactive components and ECM architecture, making it an ideal choice for engineering complex tissue constructs requiring high bioactivity. 94
Alternatively, synthetic polymers such as polycaprolactone (PCL), PLA, PGA, PLGA, and PEG are widely utilized due to their tunable mechanical properties and controlled degradation rates. 95 Composite materials that integrate natural and synthetic biomaterials are increasingly used to enhance the mechanical integrity and bioactivity of TEMGs. For example, alginate-PEG and gelatin-PCL composites have demonstrated favorable mechanical and biological properties, making them promising candidates for TEMGs.96,97
Recent advancements in TEMGs have focused on integrating vascular and neural components to improve muscle functionality. Prevascularized and preinnervated TEMGs have demonstrated superior regenerative potential by enhancing vascular integration and NMJ. Das et al. 13 utilized an in vitro coculture strategy by combining spinal motor neurons with skeletal myocytes on aligned nanofibrous scaffolds to develop innervated TEMGs. These preinnervated constructs successfully formed aligned neuromuscular bundles, promoting myocyte fusion and maturation. Within just 7 days of coculture, functional NMJs were observed on muscle fibers (Fig. 6A–a′), and the presence of motor neurons significantly increased the myocyte fusion index compared with constructs containing only myocytes (Fig. 6B, C). Upon implantation in a rat VML model, these preinnervated TEMGs facilitated muscle SC migration, enhanced microvascularization, and promoted NMJ formation near the injury site, leading to improved functional recovery. As innervation is a critical factor in skeletal muscle development, maturation, and functional control, TEMGs should either be preinnervated during fabrication or possess the capacity to support effective neural integration postimplantation.58,98

Innervation of myocytes and the impact of motor neurons on myocyte maturation in vitro.
Despite their high regenerative potential, TEMGs face several limitations. While they can generate contractile force, the magnitude is typically lower than that of native muscle tissue. 20 One of the significant barriers to TEMG efficacy is the lack of a vascular network, which restricts oxygen and nutrient diffusion, particularly in densely packed, metabolically active muscle cells. Since TEMGs often exceed the diffusion limit, developing a vascular network is essential to sustain cell viability. 98 In addition, the prolonged in vitro culture required for TEMG maturation presents challenges in clinical scalability, cost-effectiveness, off-the-shelf availability, and regulatory compliance. 99
The variability in biomaterials, cell types, culture conditions, construct dimensions, stimulation protocols, bioreactors, and preclinical models also contributes to inconsistent outcomes in TEMG-based skeletal muscle regeneration. 58 For effective VML repair, engineered constructs must incorporate both vascularization and innervation to support cell survival, metabolic activity, and functional contractility. Prevascularization strategies, such as EC coculture and the delivery of angiogenic growth factors, vascular endothelial growth factor (VEGF), fibroblast growth factor, platelet-derived growth factor, have enhanced capillary formation and vascular integration. 100 On the contrary, innervation strategies, including motor neuron coculture, electrical stimulation (E-Stim), topographical guidance cues, and neurotrophic factor delivery (BDNF, NGF), facilitate NMJ formation and enhance functional recovery. 101
By integrating vascular and neural components into engineered muscle grafts, TEMGs can more effectively restore muscle function following VML. Future research should prioritize scalable, biomimetic strategies that ensure long-term cell survival, enhance functional integration, and accelerate clinical translation.
3D Bioprinted Constructs in SMTE
Despite advancements in conventional manufacturing techniques, replicating the structural and compositional complexity of the ECM remains a significant challenge. In addition, precisely arranging cells within a 3D construct to promote myofiber alignment, neo-vascularization, and innervation is complex using traditional fabrication approaches. Bioprinting, an advanced form of 3D printing that integrates living cells within biomaterial-based inks, enables the precise deposition of cells and ECM components in spatially defined regions. This technique facilitates the rapid fabrication of complex, tissue-mimetic structures, closely replicating the in vivo microenvironment of skeletal muscle.102,103 Bioprinting methods are classified into inkjet-based, extrusion-based, and laser-assisted techniques, each offering distinct advantages and limitations. 104 Among these, extrusion-based bioprinting (EBB) is the most widely used in SMTE due to its ability to develop anisotropic, multicellular 3D constructs that mimic the architecture of native muscle tissue.
Hydrogels and their role in bioprinting for SMTE
Hydrogels play a critical role in bioprinting by serving as bioinks that encapsulate cells and provide a supportive microenvironment for their survival and differentiation. In SMTE, commonly used hydrogel materials include alginate, gelatin, fibrin, collagen, and dECM, selected for their biocompatibility, biodegradability, and ability to mimic the native ECM. 105 One of the most critical factors governing hydrogel performance in bioprinting is viscosity, which determines the structural integrity and printability of the constructs. EBB, for instance, requires higher viscosity hydrogels to ensure the stability of printed structures while maintaining optimal cell viability.106,107 Carefully selecting hydrogel properties is crucial to achieving high-resolution constructs with appropriate mechanical support and bioactivity.
Bioprinting for cellular alignment and functional muscle regeneration
Beyond material selection, topographical and biophysical cues introduced during bioprinting significantly influence cellular behavior, alignment, and differentiation. By guiding cell orientation and fiber formation, bioprinting enables the fabrication of highly organized, anisotropic muscle constructs that closely resemble native skeletal muscle architecture. 108 It can also help fabricate constructs with spatial and temporal gradients of growth factors, such as VEGF, for enhanced vascularization and repair. 109 Table 4 overviews various cell-alignment techniques, emphasizing strategies to enhance muscle regeneration through controlled cellular organization.
Various Cell-Alignment Techniques for the Engineered Construct for Volumetric Muscle Loss Treatment

Several innovative bioprinting techniques have also been developed to enhance structural integrity and functional integration within engineered skeletal muscle constructs, as mentioned below.
Multimaterial printing
Figure 7A shows this approach combines sacrificial and supportive biomaterials, such as PCL pillars coprinted with gelatin-based sacrificial materials, to create spatially controlled architectures.
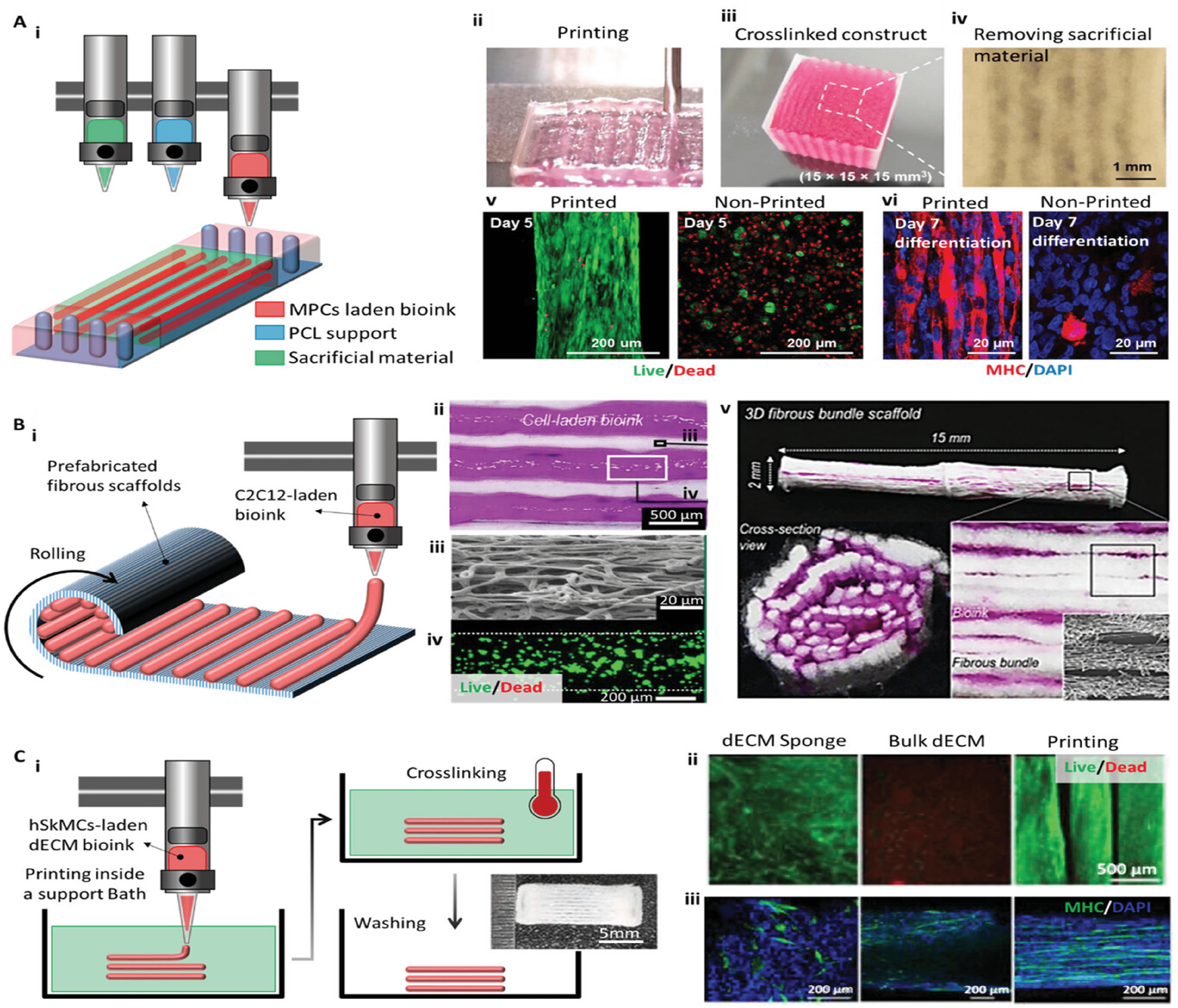
Extrusion-based 3D bioprinting for SMTE with enhanced structural stability.
Layered scaffold fabrication
Figure 7B shows that a combination of 3D printing and electrospinning is used to create PCL-based scaffolds, followed by the extrusion of a cell-laden bioink, which is then rolled into a tubular construct for mechanical reinforcement and muscle fiber alignment.
Embedded bioprinting
Figure 7C shows that freeform reversible embedding of suspended hydrogels (FRESH) involves bioprinting within a gelatin microgel support bath, which preserves ECM bioink integrity during crosslinking. This method enhances fiber-rich constructs, improving cell viability, nutrient diffusion, and myogenic differentiation. 106
State-of-the-art bioprinted constructs
Bioprinting offers unparalleled control over the tissue microenvironment, enabling the precise integration of multiple cell types, including myogenic progenitors, fibroblasts, and ECs, within a single construct. 106 This multicellular approach, explored in the last few years, is crucial for regenerating functional skeletal muscle, ensuring cell–cell interactions, vascularization, and ECM remodeling. By recapitulating the biochemical and mechanical properties of native muscle tissue, bioprinted constructs significantly improve cell viability, structural organization, and functional restoration, making bioprinting an indispensable tool for SMTE. 117 Table 5 highlights key studies using EBB to develop constructs for VML treatment.
Studies That Used Extrusion-Based 3D Bioprinting to Develop Therapeutics for Skeletal Muscle Tissue Engineering
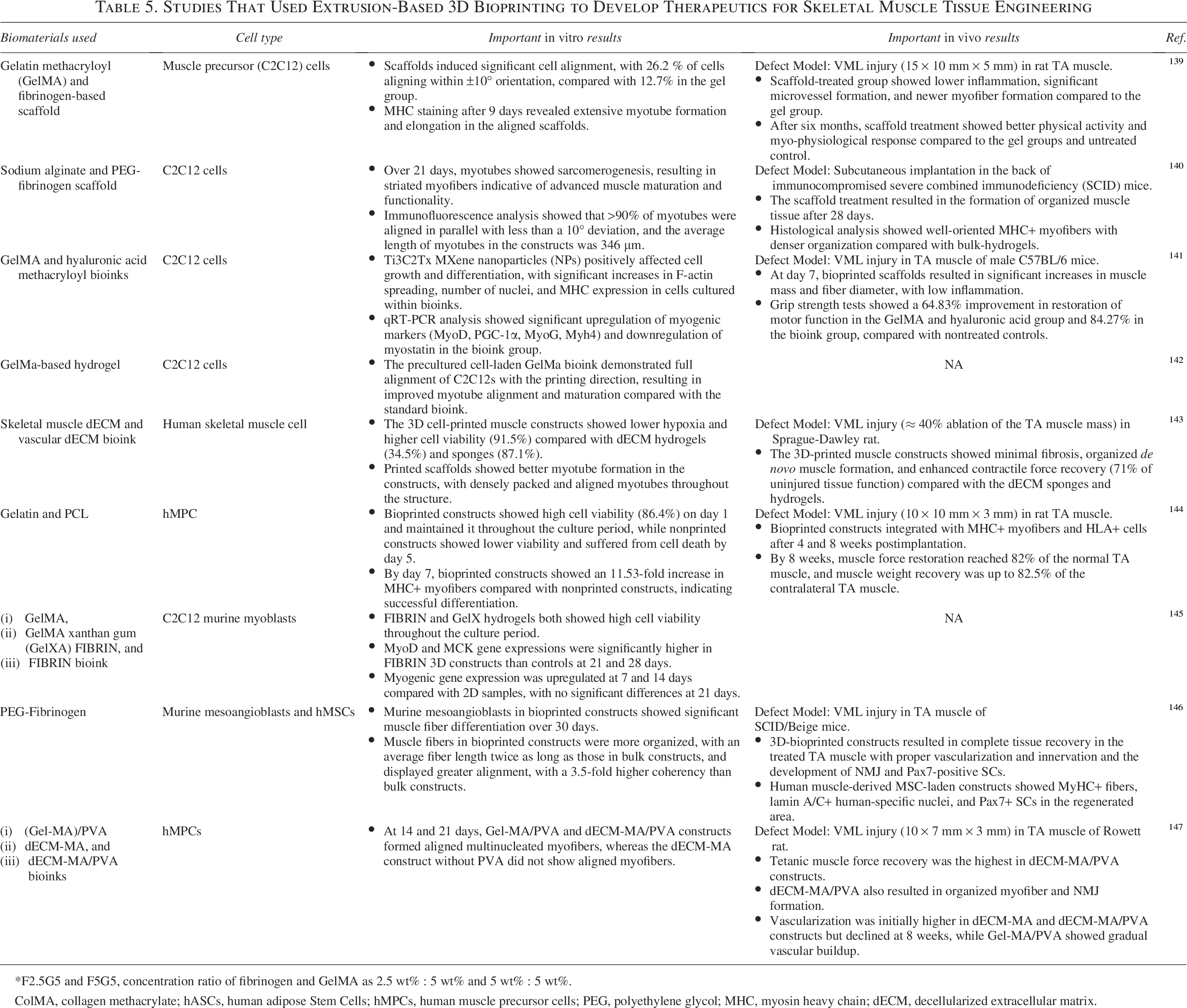
*F2.5G5 and F5G5, concentration ratio of fibrinogen and GelMA as 2.5 wt% : 5 wt% and 5 wt% : 5 wt%.
ColMA, collagen methacrylate; hASCs, human adipose Stem Cells; hMPCs, human muscle precursor cells; PEG, polyethylene glycol; MHC, myosin heavy chain; dECM, decellularized extracellular matrix.
ML in SMTE
SMTE often faces challenges in developing constructs or TEMGs that closely mimic the innate muscle anatomy. ML addresses these challenges by automating data analysis and predictive modeling to optimize construct design and tissue regeneration. 118 ML includes supervised, unsupervised, and deep learning (DL) approaches. 119
Supervised learning involves training models using labeled data to make predictions, while unsupervised learning identifies patterns in unlabeled data. 120 DL is a subset of ML that utilizes neural networks with multiple layers. 121 DL models include artificial neural networks (ANNs) and convolutional neural networks (CNNs), commonly used for image recognition and understanding natural language tasks. 122 In SMTE, ML has influenced the optimization of bioprinting. By analyzing mechanical testing data, ML models can recommend optimal combinations of bioinks to replicate the ECM of muscle tissue. ML also aids in optimizing culture conditions for cell differentiation and proliferation and enhances bioactive piezoelectric constructs by predicting the effects of electrical and mechanical cues.123–125 ML can help design constructs that accurately replicate mechanical properties such as stiffness, ensuring a better microenvironment for cell maturation. 126
Furthermore, ML algorithms can be used for in-process quality control in bioprinting. These processes often rely on data from integrated cameras or sensors within bioprinters. For instance, Jin et al. 127 used a pneumatic extrusion bioprinter to create two-layer structures and used a CNN to classify prints as “good” or “error” with high accuracy (Fig. 8A). 129 In another study, Gerdes et al. 129 incorporated infrared thermocouples to measure extrusion temperatures and trained ML models to predict print flaws and parameters such as line width (Fig. 8B). Similarly, Bonatti et al. 130 used CNNs for real-time monitoring of 3D printing with varying parameters. The prints were classified as “ok,” underextruded, or overextruded, and the CNN accurately identified defects, allowing for early termination of faulty prints and optimization of printing parameters (Fig. 8B). Sun et al. 131 proposed a novel system for real-time monitoring of the Taylor cone and jet formation in electrospinning. An optical microscope was integrated into the setup to capture images during the printing process. These were then classified into eight categories, including one for successful deposition and seven for different types of errors. Using a CNN with majority voting on image sequences, the system effectively identified and corrected deposition issues in real-time (Fig. 8C). In another study, Ruberu et al. 132 collected 177 samples to reproducibly form constructs using Bayesian optimization.
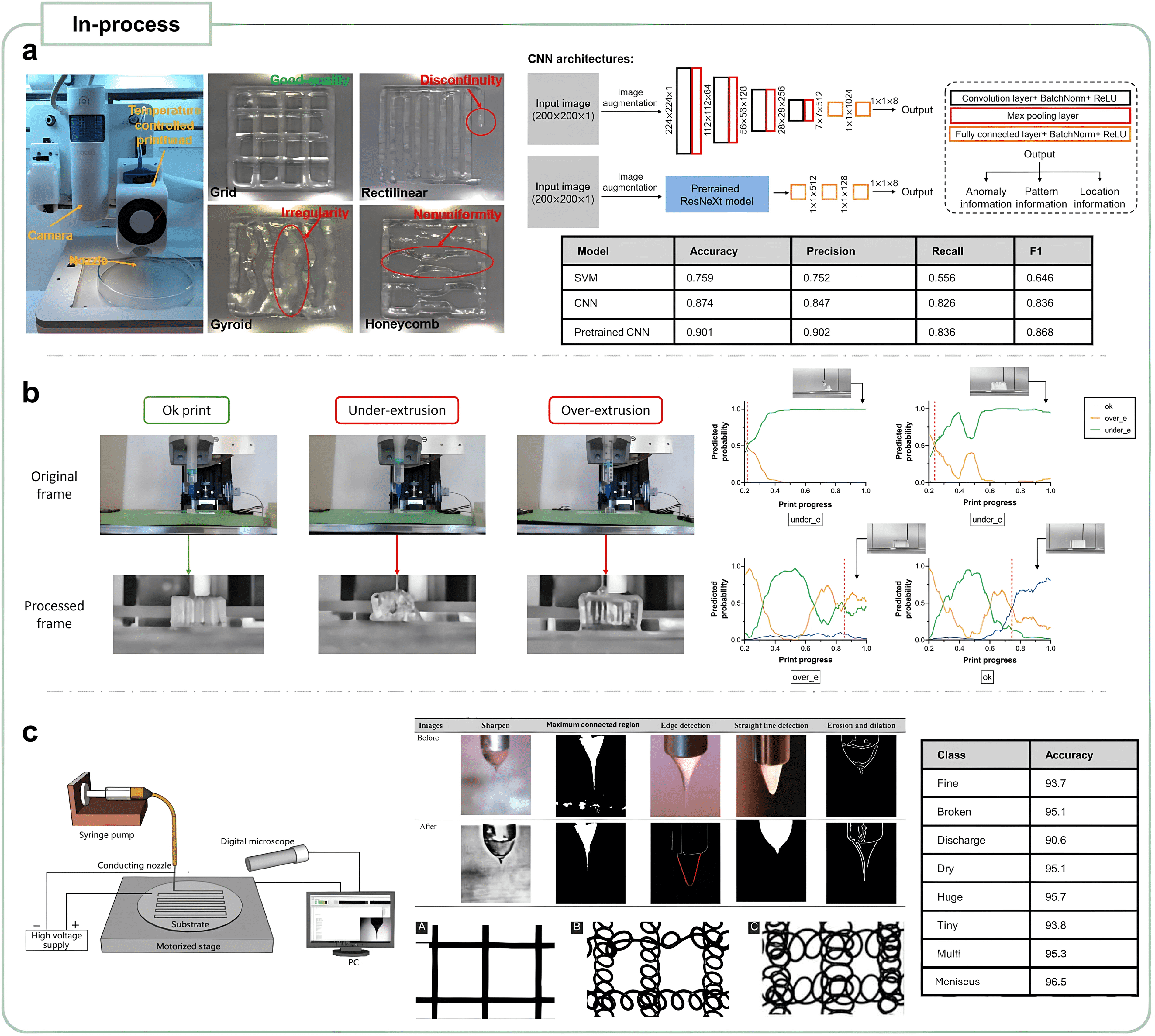
Machine learning (ML) application in in-process quality control (QC) for 3D bioprinting.
ML can also help design constructs replicating mechanical properties such as stiffness, ensuring a better microenvironment for cell maturation. 126 For instance, predictive modeling can recommend the best combination of alginate, gelatin, and chitosan bioinks used in bioprinting to create constructs that closely mimic muscle tissue’s natural ECM.125,133 Moreover, ML can predict how engineered tissues respond to mechanical stimuli such as stretch or compression and help design constructs that provide appropriate mechanical cues.
In terms of cell culture and tissue development, ML can aid in optimizing culture conditions for cell differentiation and proliferation.123–125 ML can improve muscle models for in vitro and in vivo studies. By analyzing data from in vitro experiments, such as cell viability assays and mechanical testing, ML can predict the long-term behavior of engineered constructs in vivo. For instance, Sujeeun L.Y. et al. 134 used ML to predict the performance of electrospun polymeric constructs for skin tissue engineering. They trained six supervised learning algorithms to correlate properties with cell viability and achieved the highest accuracy with random forest regression. Lim J Y et al. 135 studied skeletal muscle gauge (SMG) as an imaging marker for sarcopenia. They developed an ML algorithm to predict SMG using clinical and inflammatory markers in colorectal cancer patients. The study of 1094 patients showed low SMG in 21.6% and 20.5% of patients in training and test sets, respectively. The LP-SMG model was an independent predictor of low SMG and outperformed individual clinical variables. It can be an effective tool for detecting sarcopenia without relying on CT scans during treatment.
Figure 9 summarizes the current and potential applications of ML in SMTE. ML can help predict cellular responses to constructs, design personalized constructs, and automate constructs’ quality control during fabrication. ML can uncover patterns that improve muscle regeneration understanding by analyzing large datasets. In the next few years, ML can advance therapeutics for VML, enhancing efficiency and therapeutic efficacy while reducing development timelines.
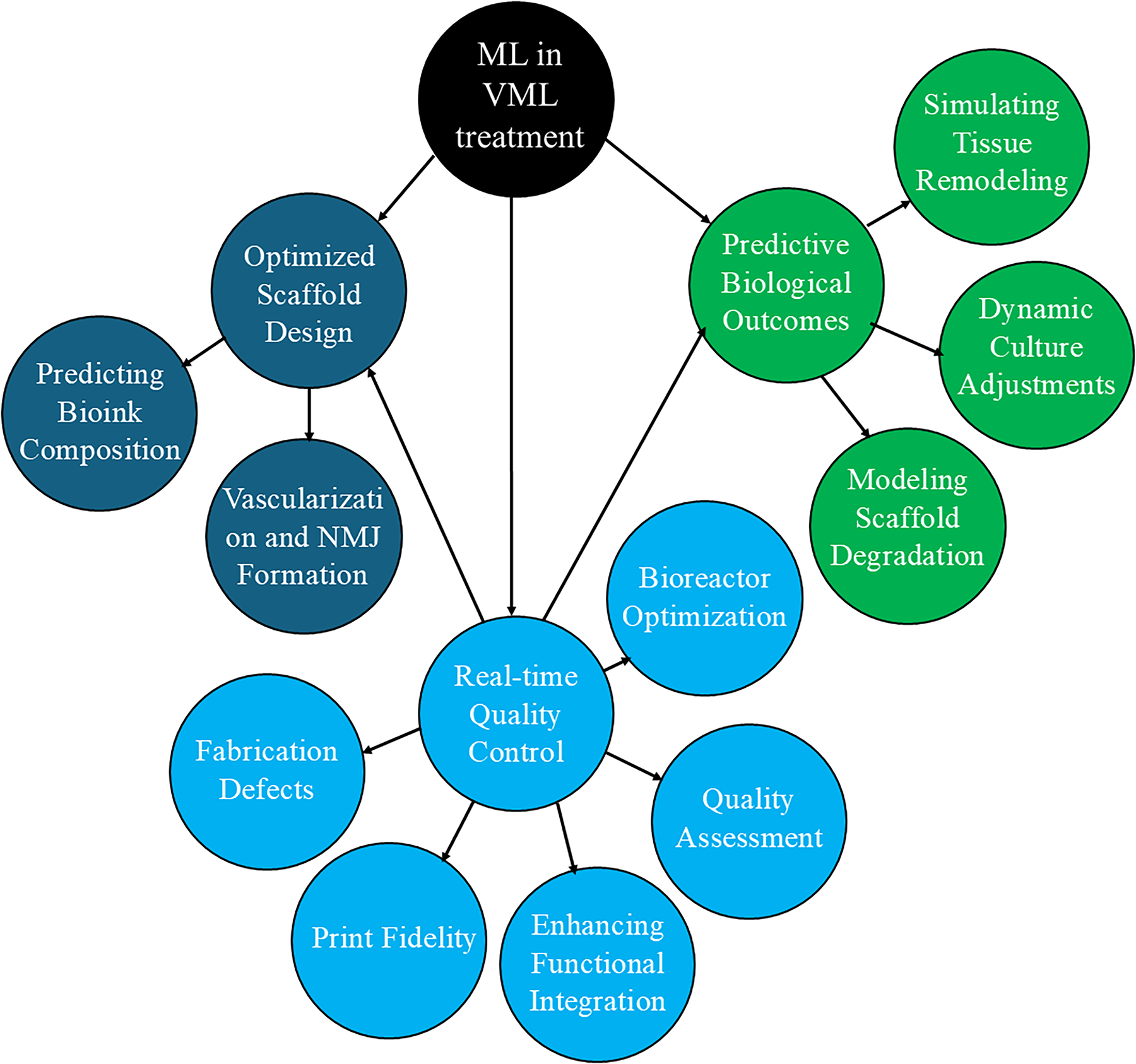
Chart showing the existing and potential applications of ML for the construct design for VML treatment.
Research Gap and Prospects for the Future
Despite significant progress in biomaterials, biofabrication, and cell-based therapies, SMTE faces significant challenges that hinder the clinical translation of therapies and promote functional muscle regeneration. Addressing these gaps is essential for developing scalable, biofunctional, and physiologically relevant muscle constructs capable of restoring vascular, neuromuscular, and mechanical integrity in VML injuries.
Enhancing NMJ formation and functional integration
One of the most significant obstacles in SMTE is achieving functional integration between newly formed muscle and host tissue. Specifically, reinnervation, essential for restoring NMJs, remains particularly difficult, resulting in newly formed muscle with low functional recovery and limited force generation. Current strategies to promote NMJ formation include coculturing myogenic and neural progenitors, delivering neurotrophic factors (e.g., brain-derived neurotrophic factor, nerve growth factor), and applying E-Stim to guide synaptogenesis. Future research should integrate ML-driven predictive modeling to optimize scaffold architectures and biochemical cues that facilitate NMJ formation, nerve infiltration, and functional recovery. Moreover, stand-alone “smart” (responsive) constructs that can guide reinnervation in vivo without added E-Stim protocols should also be explored.
Addressing fibrosis and immune modulation in SMTE
Fibrosis is a major obstacle in VML treatment, often leading to scar tissue formation, impaired regeneration, and loss of function. To mitigate fibrosis, researchers have explored antifibrotic agent delivery, immune-responsive biomaterials that balance proinflammatory and anti-inflammatory macrophage activity, and controlled release of bioactive factors to fine-tune the inflammatory response and prevent excessive scar tissue formation. Despite promising findings, comprehensive studies evaluating the clinical translatability of these approaches are still lacking. Future research should focus on developing immunomodulatory scaffolds that actively regulate inflammation while promoting vascularization, myogenesis, and functional muscle regeneration and minimizing scar tissue formation.
Overcoming limitations in vascularization and oxygen transport
Inadequate vascularization remains a critical bottleneck in engineered muscle constructs, leading to ischemia, inadequate oxygen diffusion, and limited construct survival postimplantation. Although strategies such as prevascularization, angiogenic growth factor delivery, and coculturing ECs have improved capillary formation, sustaining long-term vascular integration remains challenging. Future research should focus on (1) developing hybrid bioprinting techniques incorporating vascularized cell-laden bioinks to create hierarchically structured capillary networks, (2) utilizing ML-driven optimization to predict optimal multicell ratios, scaffold properties, and spatial gradients of angiogenic cues for enhanced vascular integration, and (3) designing bioactive materials that release proangiogenic factors in a spatiotemporally controlled manner to promote sustained capillary formation.
Leveraging ML for SMTE optimization
ML offers immense potential in tissue engineering, but its applications in SMTE remain underdeveloped due to limited high-quality datasets. Many ML models are trained on small, nongeneralizable datasets, leading to overfitting and poor real-world applicability.128,136 To harness ML effectively in the future, researchers must (1) develop standardized, publicly accessible large datasets to improve model reliability, (2) use feature selection techniques to identify key biomaterial–cell interactions that enhance myogenic differentiation and functional integration, and (3) integrate ML with bioprinting to optimize scaffold architectures, predict mechanical and biochemical properties, and enable real-time adaptive printing for reproducible construct fabrication.
Advancing biofabrication for complex muscle architectures
Although bioprinting and electrospinning have significantly improved the fabrication of anisotropic, hierarchical muscle structures, challenges remain in recapitulating the multiscale organization of native muscle. Future directions should include 4D bioprinting, allowing constructs to dynamically adapt to external stimuli for enhanced tissue remodeling. In this regard, electroactive biomaterials such as polyaniline, polypyrrole, polythiophene, graphene, and metallic nanoparticles can be explored to promote electromechanical stimulation, facilitating myotube formation, NMJ development, and contractile function. Moreover, hybrid biomaterials integrating conductive nanocomposites, bioactive factors, and mechanical cues can also be explored to create stimuli-responsive constructs for personalized and effective regenerative therapies. 137
Understanding cell–material interactions
A limited understanding of how cell types (myoblasts, mesoangioblasts, stem cells) interact with various biomaterials hinders construct optimization. 138 Although natural and synthetic biomaterials have been widely explored, the precise mechanisms by which scaffold physicochemical properties influence cell behavior remain unclear. Further research is needed to elucidate (1) the impact of electrical and mechanical stimulation on muscle regeneration and functional recovery and (2) optimal biomaterial compositions that support cell adhesion, proliferation, and long-term construct stability.
Bridging the gap between preclinical research and clinical translation
Although several constructs have been developed over the past two decades, almost none is available in the clinics. Translating SMTE technologies into clinically viable therapies requires addressing scalability, standardization, and regulatory approval challenges. Many engineered constructs fail to restore function due to inadequate vascularization, reinnervation, and mechanical integration. Future efforts should focus on the following: (1) Developing scalable manufacturing processes to produce off-the-shelf, patient-specific muscle grafts. (2) Strengthening collaborations among bioengineers, clinicians, regulatory officials, and insurance companies to facilitate the translation of clinically relevant constructs that align with surgical implantation techniques and postoperative rehabilitation protocols. (3) Establishing preclinical models that are similar to or close to human VML models to assess the long-term safety, efficacy, and functional restoration of engineered constructs.
By addressing these research gaps, SMTE has the potential to transform muscle regenerative medicine, offering clinically viable bioengineered solutions for VML and musculoskeletal disorders in the upcoming decade. The combined efforts in biomaterial innovation, bioprinting technology, computational modeling, and regulatory science will pave the way for personalized, scalable, and effective therapies to restore skeletal muscle function.
Authors’ Contributions
S.Y.S.: Reviewed all the studies and prepared the original draft of the article. P.S.: Contributed to editing, preparing the final draft, and overseeing project administration. Both authors reviewed and approved the final version of the article.
Footnotes
Author Disclosure Statement
The authors have nothing to disclose.
Funding Information
This work was supported by R03 Grant No. 1R03EB036096-01 and R01 Grant No. 1R01AR083865-01A1.