
Abstract
Periodontitis is an inflammatory disease affecting the support of the teeth, eventually leading to loosening and subsequent loss of teeth. Effective procedures for periodontal tissue engineering or regeneration require preclinical models before market introduction. Research has been performed in either small or large animals. Unfortunately, there is no intermediate-sized in vivo model available for periodontal regeneration studies, such as, for instance, rabbits. The objective of this study was to evaluate the rabbit as a new experimental model to study periodontal regeneration. In 12 rabbits, periodontal defects were created in a 4 × 6 mm bone window. The animals were sacrificed after 2, 4, 6, 8, 10, and 12 weeks. Up to 6 weeks, the fenestration defects healed partly by repair and partly by regeneration. After 6 weeks the root had erupted to such an extent that the original root defect shifted into the oral cavity. This signifies that the periodontal ligament (PDL) bordering the original bone defect site is newly formed during the natural eruption process and not locally regenerated. Apparently, the new PDL originates from mesenchymal cells that arise from the apical part (sheath of Hertwig) and subsequently developed into PDL fibroblasts. At 12 weeks, no signs of surgery were present anymore. On the basis of our observation that the defect of the PDL was replaced rather than restored, we conclude that the rabbit model has disadvantages and is less suitable for studies of regeneration of PDL.
Introduction

Lateral radiograph of the rabbit skull showing the bone and the roots of the two premolars and the three molars in the mandible. The lower half of the (black) circle is outlining the potential surgical site.
Therefore, the aim of this study was to evaluate rabbits as a potential animal model for studying periodontal regeneration.
Materials and Methods
Animals
Twelve healthy adult female New Zealand white rabbits, weighing about 3.2–3.8 kg, were used for this experiment. The ethics committee of Radboud Nijmegen University approved this study (approved project number RU-DEC 2007-045). All animals were handled in accordance with the national guidelines for the care and use of laboratory animals. All animals were screened for good physical condition and had a known specific pathogen-free status. The rabbits were allowed to accommodate to their new environment 2 weeks before surgery. Medium-hard food pellets and water were provided ad libitum, but was withheld overnight (14 h) preoperatively.
Surgical procedures
Surgery was performed under general inhalation anesthesia. The anesthesia was induced by an intravenous injection of Hypnomidate® (etomidate; Janssen-Cilag B.V., Tilburg, The Netherlands) and maintained by a mixture of nitrous oxide, isoflurane, and oxygen through a constant volume ventilator. The body temperature of the animals was maintained at 37°C using a heating pad. The rabbits were connected to a heart monitor. To minimize postoperative pain, Temgesic® (buprenorfine 0.05 mg/kg intramuscularly; Schering-Plough, Heist-op-den-Berg, Belgium) and Rimadyl® (carprofen 4 mg/kg subcutaneously; Pfizer, Capelle aan de IJssel, The Netherlands) were administrated preoperatively and continued for, respectively, 1 and 2 days postoperatively. To reduce perioperative infection risk, as an antibiotic prophylaxis Baytril® (enrofloxacin 5–10 mg/kg subcutaneously; Bayer HealthCare, Mijdrecht, The Netherlands) was given.
During anesthesia the rabbits were immobilized on their backs. In each animal, bilaterally periodontal defects were created. In advance, the perimandibular and cervical areas were shaved, washed, and disinfected with povidone-iodine. A 20 mm longitudinal extraoral (skin) incision was made along the inferior border of the mandible (Fig. 2A). Subsequently, a full-thickness flap was elevated to expose the lateral cortex of the mandible. Care was taken to respect the soft tissue, thereby preventing a communication to the intraoral environment. After elevating a full-thickness flap (Fig. 2B), fenestration defects were created by removing the cortical bone with the chisel-like tip (OP1) of an ultrasonic device (Piezosurgery®; Mectron, Carasco, Italy) using constant cooling with sterile saline. Thereafter, hand instruments (curettes) were used until the PDL was identified. The roots of the two most distal molars (which are one rooted) were carefully planed to ensure that the cementum, the PDL, and remnants of bone were completely removed. The dimensions of the noncritical-sized (bone) defects were approximately 4 × 6 mm (Fig. 2C) and left empty according to the study protocol, to study the defects in time. Subsequently, the soft tissue flaps were closed with resorbable sutures (4-0) in two separate layers (subcutis and cutis). At each time point, after 2, 4, 6, 8, 10, and 12 weeks, the animals were sacrificed in pairs by an overdose of Nembutal® intravenously (pentobarbital; CEVA Sante Animale BV, Libourne, France). Retrieved samples were processed for histology.

(
Histological preparation
After euthanizing the animals, the mandibles were dissected and split in the middle. Subsequently, excess tissue was removed. The specimens were fixed in buffered formaldehyde (pH 7.4) 10% and dehydrated in a graded series of ethanol (70–100%). Thereafter, they were embedded (nondecalcified) in methylmethacrylate. After polymerization of the methylmethacrylate, sections (10–20 μm) were prepared using a diamond blade sawing microtome (Leica Microsystems SP 1600, Nussloch, Germany). 10 Sections were cut in a bucco-lingual direction and subsequently stained with basic fuchsin and methylene blue.
Histological and histomorphometrical evaluation
The histological evaluation was performed using a light microscope (Leica MZ12, Leica BV, Rijswijk, The Netherlands) and included a description of the observed tissue response. Additionally, microscopic images were projected on a color monitor using a CCD/RGB camera (Sony DXC151P, Wetzlar, Germany), and digital image analysis software (Leica Qwin Pro-image analysis system, Wetzlar, Germany) was used for the histomorphometrical evaluation. The following parameters (Fig. 3) were analyzed:
The size of the bony defect: the width of the bony defect as measured from the apical (lower) border to the coronal (upper) border. Eruption of the tooth: the middle of the bony defect was projected upon the root and subsequently compared to the middle of the root defect.
In each of the six groups, two animals were present in which bilateral defects were created, resulting in a total of four defects per group. Three separate histological sections were made per defect. Subsequently, each measurement was performed in threefold per section. The average of the three sections gave one value per defect.

Histomorphometrical measurements in an overview figure after 2 weeks. Original magnification, 1 ×. Bony defect: the width of the bony defect measured from the apical (lower) border to the coronal (upper) border (indicated by the green line in the lower right of the figure). Eruption of the tooth: the middle of the bony defect was projected upon the root compared to the middle of the root defect (indicated by the red line in the center of the figure). Color images available online at
Results
Experimental animals
All 12 rabbits in this experiment remained in good health and did not show any wound complication after surgery. In the first 2 postoperative days, three animals lost weight less than 3%. After feeding with extra grass hays, these animals increased in body weight compared to the preoperative levels. No visual signs of inflammatory or other adverse tissue reactions were observed.
Histological evaluation after 2 weeks
Macroscopically, the defects could be identified by an altered appearance of the bone texture, which was more porous and slightly darker in color. As depicted in Figure 3, microscopically the presurgical borders of the defect were clearly defined (indicated by green line on the lower right of the picture).
In contrast to regeneration, periodontal repair is the continuum of healing, during which disrupted (lost) tissues are restored by other than the original tissues and thereby do not replicate their original structure and function. Obviously, in this experiment a combination of repair and partial (bone) regeneration can be observed as indicated by the absence of a normal PDL. At the root surface bone apposition can be observed instead of a PDL and cementum. Angiogenesis was a distinct finding in all of the samples (Fig. 4). Complete bridging of the bony defect was not observed. Healing of the bone defect consisted of new woven bone, starting from the edges of the defect, while in the center still soft connective tissue was present. The new bone contained more and larger marrow spaces when compared to the surrounding original bone. At the root surface direct bone apposition onto the enamel surface was seen (Fig. 5); in contrast to the human situation, this does not cause ankylosis. It is considered to be bone because it can be distinguished from cementum by the presence of blood vessels, which are absent in cementum. Damage of the dentin layer caused by the tip of the ultrasonic device can be seen as well. In all specimens, surgery had removed not only soft tissue of the PDL but also a certain amount of root dentin; in two specimens even the root was fractured completely. In 2 weeks the root had erupted over a distance of 5.44 mm (Fig. 3, indicated by the red line). Therefore, the part of the root, which flanked the original defect, had already shifted upward. At the site of the original bone defect the PDL showed a normal aspect without any inflammatory reaction.
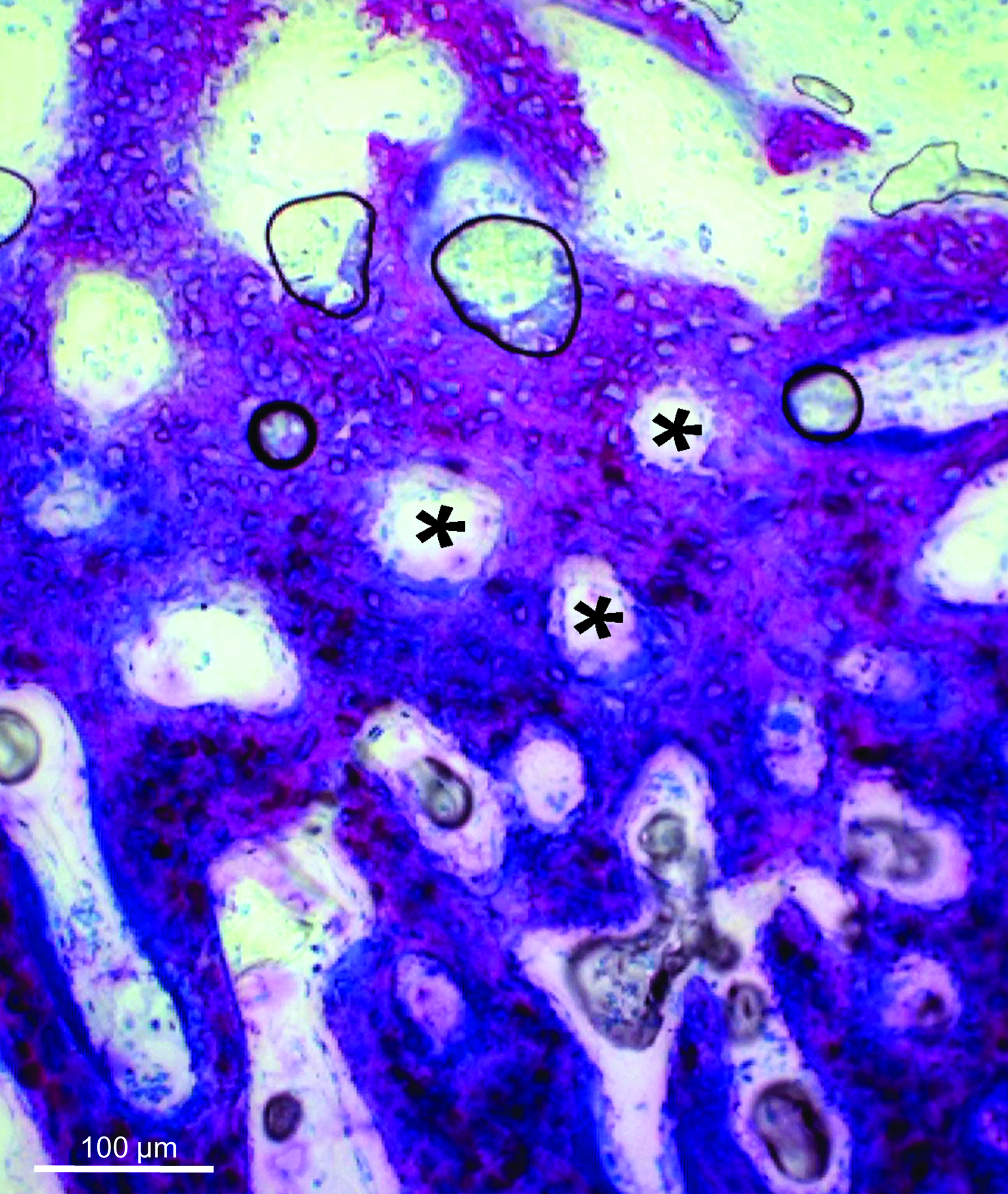
Angiogenesis in a 2-week sample (indicated by the symbol *). Original magnification, 20 ×. Color images available online at

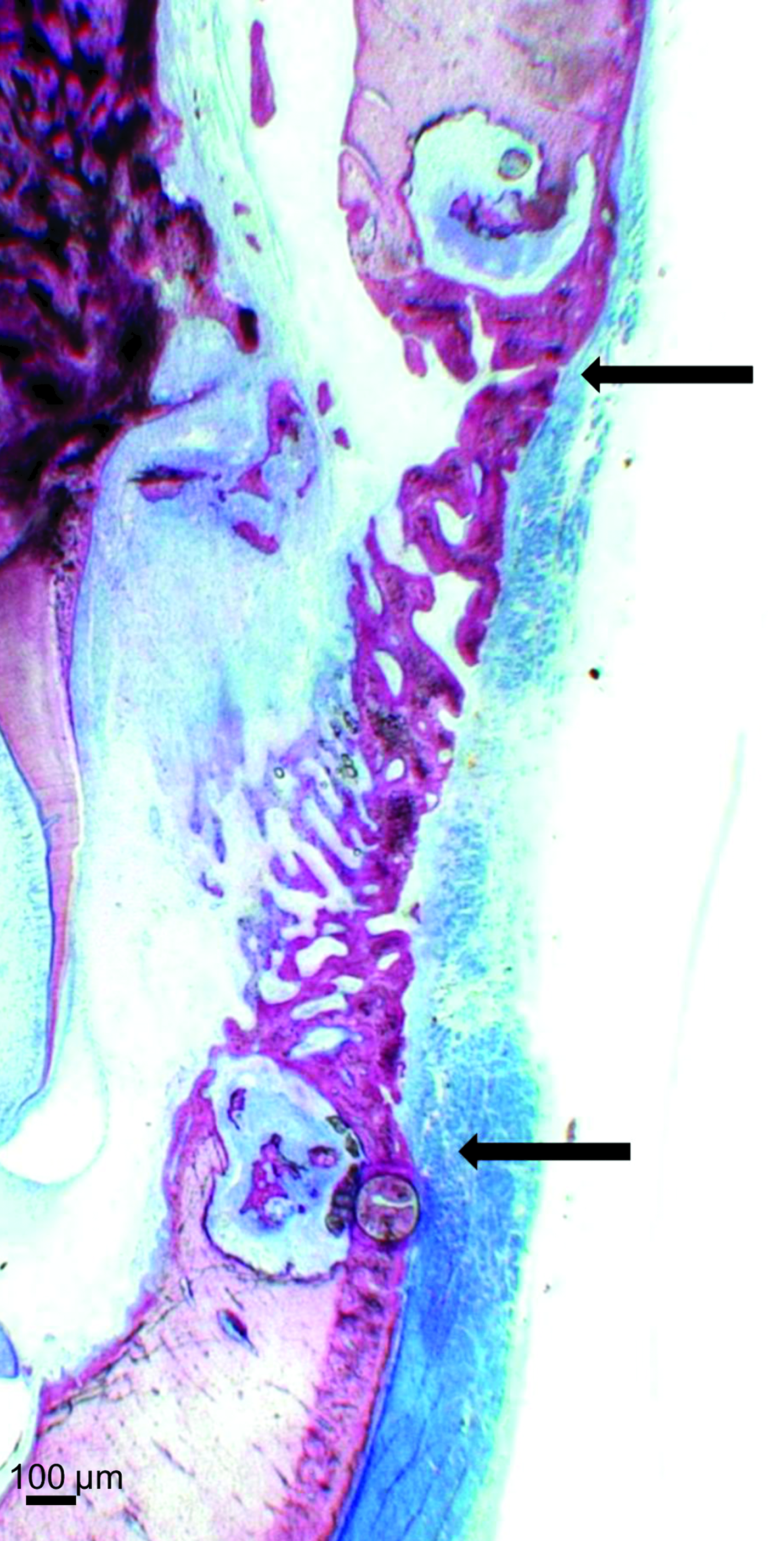
Direct bone apposition onto the enamel surface indicated by the two white arrows. Original magnification, 5 ×. Color images available online at
Histological evaluation after 4 weeks
Macroscopically, the defects could still be distinguished from the surrounding bone tissue, because of differences in color and morphology. Healing involved a combination of repair and regeneration. Woven bone had formed without clear orientation of the new cells, and contained larger and a great numbers of marrow spaces than the old bone. Compared to the 2-week results, the bone density/organization had increased, and the cortical layer was now intact and the defect closed (Fig. 6). Still difference in thickness between the newly formed cortical layer and the nonoperated can be noticed (Fig. 7). At the root surface the forming PDL seemed thicker, compared to the original width, as compared to the nonoperated side. More apical of the surgically created defect the PDL had a normal appearance. In some specimens remnants of bone chips and/or root dentin were seen even within the PDL. Probably, these bone chips were left because of the piezo-electric surgery and thereafter encapsulated within the PDL. At the location of the already upward-shifted defect, the PDL had regained its normal anatomical appearance. However, in the region of the original bone defect, there was no clear orientation of the PDL cells.
Intact cortical bone layer, containing larger and greater number of marrow spaces. Two black arrows indicating the defect 4 weeks postoperatively. Original magnification, 1 ×. Color images available online at
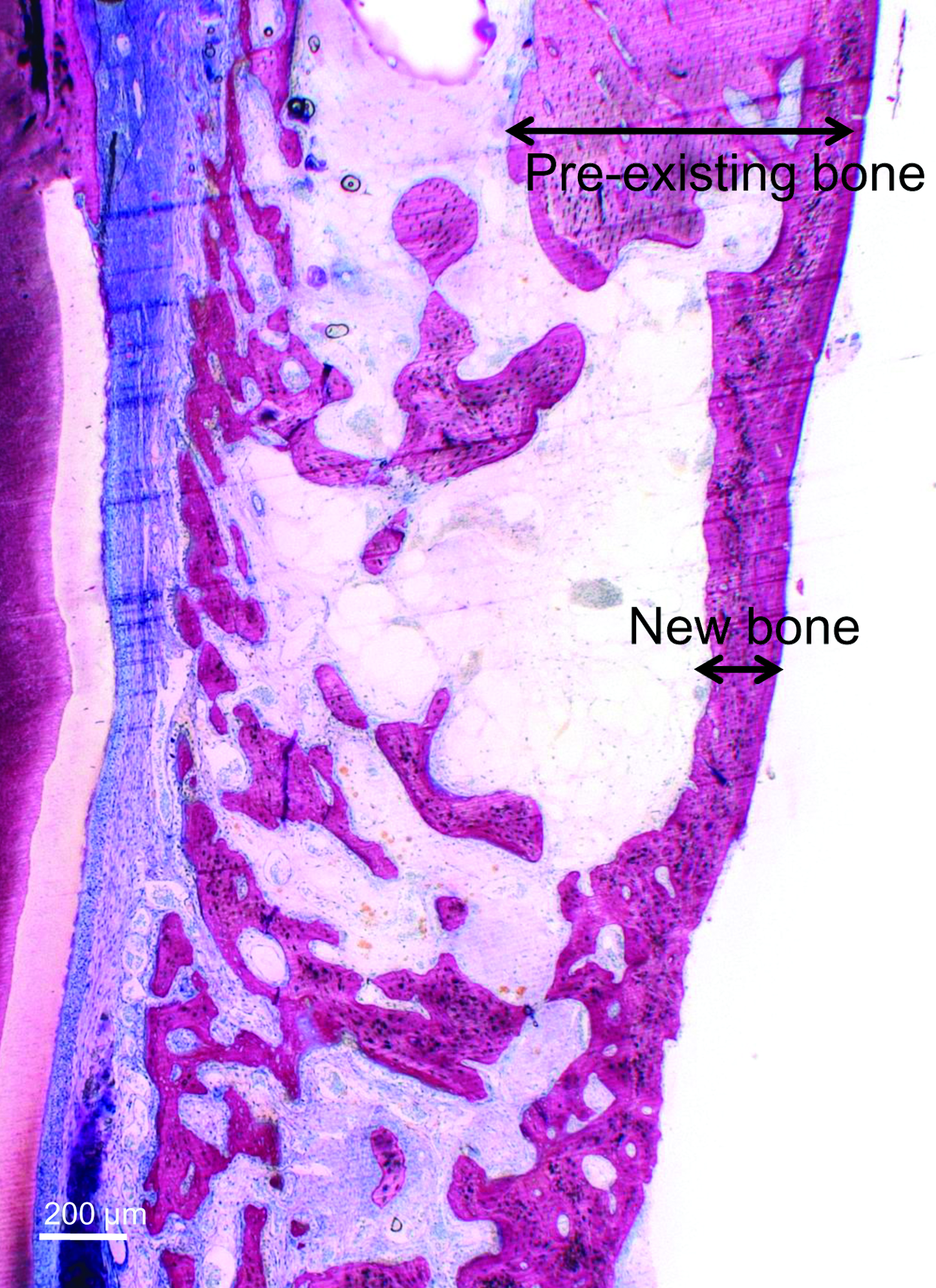
Difference in thickness between the preexisting bone and the newly formed bone indicated by the two black arrows. Original magnification, 2.5 ×. Color images available online at
Histological evaluation after 6 weeks
Visual inspection showed no clear distinction between the defects and surrounding bone tissue. A maturing bone defect with stretching of the osteocytes was observed; the cortical bone over the defect was thicker, but still less than the original bone. PDL looked normal in most regions, while in other areas layers of bone had been deposited directly onto the dentine/enamel surface. In most specimens the defect in the root could not be identified, indicating that, because of the continuous eruption, the root dentin with defect had already shifted into the oral cavity and was lost by occlusal wear.
Histological evaluation after 8 and 10 weeks
For the histological outcome after 8 and 10 weeks, no major differences were observed between these time points. Maturation of the surgically created fenestration defect progressed, indicated by a further increase in cortical thickness and organization of both the cortical and trabecular bone. In some specimens the alternating pattern of enamel and dentin, as typical for the rabbit root, could be clearly seen (Fig. 8). Also, a normal thickness and organization of the PDL was observed in the region of the original bone defect.

The alternating pattern of enamel and dentin. E depicts enamel surfaces; D depicts dentin surfaces; alveolar bone can also observed. Original magnification, 2.5 ×. Color images available online at
Histological evaluation after 12 weeks
Macroscopically, the defect could not be distinguished from the surrounding tissues anymore. Complete regrowth of the tooth and its periodontium was observed (Fig. 9). It must be emphasized that although the area of the surgery was completely regenerated showing a natural functional anatomy, regeneration was induced only partly from the original defect. Especially, the PDL was rather being replaced than regenerated as a consequence of the continuous eruption. With respect to bone thickness, PDL, and the orientation of the bone cells, no differences compared to the nonoperated areas were observed.

Histological overview after 12 weeks; the original defect site is depicted by the symbol *. Original magnification, 1 ×. Color images available online at
Histomorphometrical evaluation
Only at the 2-week time point the eruption could actually be measured. At the other time points this was impossible either because of the progressed eruption or because of the pronounced root curvature. The mean bony defect was 4.4 ± 0.5 mm (mean ± standard deviation) in height and 5.5 ± 0.5 (mean ± standard deviation) in length. After 2 weeks the length of eruption was 5.4 mm (average of 2.7 mm/week).
Discussion
In this study fenestration defects in rabbits were evaluated as a potential new model for evaluating periodontal regeneration strategies in tissue engineering. Compared to the small models, such as mouse or rat, or the large models, like dogs or nonhuman primates, the rabbit serves as an intermediate model, in size, handling, and in costs.11,12 Before actually evaluating regenerative constructs in a rabbit, it is essential to collect data on its regular healing pattern in time to determine the optimal healing time for potential further studies. Therefore, in an attempt to design a new model to study periodontal regeneration, obviously one has to be aware of the anatomy and periodontal wound healing after creation of a defect.
During the surgical approach, it is essential to bypass the facial artery, to prevent severe bleeding. By initially making a superficial incision, this vessel can be easily identified, and to preserve its integrity, subsequently freed from the surrounding tissues. A commercially available piezoelectric device (Piezosurgery®Mectro, Carasco, Italy) was used to create the fenestration defects. This device, characterized by piezoelectric ultrasonic vibrations only results in an effective reduction of the hard tissues, such as bone and dentin. If contact with the soft tissues occurs, these will remain undamaged. 13 Histological evaluation elucidated that in some specimens, specifically because of the limited dentin bulk at the open apex, the apical part of the root fractured. To avoid this complication, a more coronal positioned defect can be created. Histological observation led to the impression that the more severely the root was damaged, the less fast the root erupted.
Healing of the fenestration defect followed a pattern of initial repair and spontaneous regeneration. Synchronically to the eruption process, new PDL was formed, together with a layer of (acellular) cementum. Initiated by local cells, also the alveolar defect was restored; from all edges of the defect, bone was formed to bridge the defect in time. This bone healing process seemed to progress without specific relation to the PDL healing. Both these processes can therefore be seen as two separate entities. Already, after 6 weeks, the original defects were hard to discern. Additionally, because of the eruption, the root defect already was shifted upward and could not be observed anymore. This experiment corroborates the literature stating that for rabbit molars the average eruption speed is 2–3 mm per week.14,15 Continuous tooth eruption has also been described for incisors in rats. Surprisingly, in contrast to rabbits, rat molars show this continuous eruption feature to a much lesser extent.
In contrast to periodontal bone loss as a consequence of periodontitis (ligature-induced model), in this study surgically created defects were made via an extraoral approach. As an advantage, such defects can be prepared in a reproducible manner, thereby allowing various treatment modalities to be compared. Moreover, the operator has a good view at his operation field. However, as a drawback, surgically created defects show more spontaneous regeneration. Although others have induced periodontitis in the rabbit successfully by means of ligatures, 16 they did not aim to regenerate such defects.
In our opinion this specific model is not appropriate because of the irreproducibility of the induced baseline defects. Another drawback is that these intraoral defects are limited in size and accessibility. Moreover, as a parallel to our study, probably because of the fast eruption the intrabony defects in the rabbit will be, at least partly, spontaneously regenerated during the eruption process after ligature removal, which is, of course, in contrast to the human situation. For initial testing of a tissue-engineered material, it is preferable to test the material without the risk of contamination with the intraoral environment. Therefore, other than intraoral approaches have been advocated like the subcutaneous pouch model. 17 However, this pouch model is no equivalent of the periodontal environment, as is the present model.
In conclusion, in rabbits, artificially created periodontal defects cannot sufficiently be evaluated because of the high eruption speed of the teeth. The presented rabbit model is therefore less suitable for studies in periodontal regeneration due to the observation that in rabbits the PDL is not restored but rather replaced.
Footnotes
Acknowledgments
The Dutch Technology Foundation STW (project no. NKG.6099) financially supported this study. The authors would like to thank N. van Dijk for preparation of the histological samples and V. Cuijpers for his help with the figures. The authors would like to thank R. van Dijk (Robouw, the Netherlands) for given us the opportunity to work with the Piezosurgery®. The authors would especially like to thank J. Maltha and V. Everts for their advice concerning animal models.
Disclosure Statement
No competing financial interests exist.