
Abstract
The present study was designed to investigate whether mechanical testing in conjunction with microcomputed tomography (μCT) analysis can be used to evaluate the quality of regenerated bone enhanced by the implantation of a composite composed of granular octacalcium phosphate and collagen (OCP/Col) matrix. Previous studies confirmed that the granules of OCP alone or OCP in Col matrix tend to mature into bone-like hydroxyapatite and enhance bone regeneration coupled with its own biodegradation, if implanted in various bony sites. OCP/Col was implanted in rat calvaria critical-sized bone defect for 4 to 12 weeks for microindentation, mechanical testing, μCT imaging, and histological examinations. The microindentation testing of the regenerated bone revealed a progressive increase of the Vickers hardness showing the highest value in 12 weeks. The Vickers hardness was in good agreement with both the parameters of μCT and the mechanical property; the quality of regenerated bone increased progressively with the implantation periods. The regenerated bone exhibited a mature bone-like matrix structure with osteocytes histologically. The quality of the regenerated bone was compatible to that of normal control calvaria bone regarding the mechanical properties. The results indicate that microindentation testing can be used to evaluate the quality of regenerated bone in the initial regeneration and the development of bone enhanced by OCP granules within Col matrix. It appears that the implantation of OCP/Col could be a model study to determine the quality of the regenerated bone.
Introduction
It would be valuable to learn whether tissue-engineered bone could acquire a quality equivalent to that of the normal bone, because the information allows us to comprehend whether the regenerated bone is functional. A few studies have applied the above-mentioned methods, including FTIR,13–15 to analyze cartilage or bone regenerated by tissue engineering measures. Bone regeneration by tissue engineering includes a variety of tissue alteration steps, from the initial bone apposition stage, including mineral deposition on scaffolds, to the remodeling stage in the regenerated bone with time. The quality of the regenerated bone is expected to depend highly on the engineering measures including the type of scaffold used. Nonresorbable scaffolds, such as sintered HA ceramic, 16 simply provide surfaces to which cells can attach, while biodegradable materials, such as β-tricalcium phosphate ceramic16,17 or hydrogels, 18 provide spaces after their own degradation to form new bone. There are some methods to fabricate scaffolds for regenerating bone such as direct precipitation19,20 of octacalcium phosphate (OCP) or hydrolysis 21 of α-tricalcium phosphate within organic matrices, and formation of fibrous HA 22 or granular HA. 23 It is highly likely that the pattern of bone regeneration is influenced by the chemical composition and the structure of these scaffolds due to their intrinsic osteoconductive characteristics. Therefore, the tissue-engineered bone could be a model to investigate the property in which the bone may exhibit variation in terms of quality depending on the scaffold used.
OCP has been proposed as a precursor of biological apatite crystals in bone and tooth.24–26 We previously found that OCP works as a locus to initiate bone apposition by osteoblasts, resulting in the enhancement of bone formation more than those by synthetic HA or Ca-deficient HA implantation.27,28 The subsequent studies disclosed that: (1) OCP tends to convert to HA if implanted in various tissue sites;27–30 (2) OCP biodegrades in vivo;31–34 and (3) OCP promotes osteoblastic cell differentiation in vitro.30,35–37 In addition, combining OCP with collagen further enhanced bone regeneration in rabbit bone marrow 38 or rat calvaria critical-sized defect39,40 with progressive biodegradation of this scaffold material.
In the present study, we focused our attention on the inorganic biodegradable OCP mineral in the granule form and analyzed the quality of the regenerated bone enhanced by the implantation of its composite with the atello-collagen matrix (referred to as OCP/Col hereafter). The purpose of the present study was to establish a method to estimate the bone quality and to determine when and how regenerated bone acquires characteristics that are compatible with those of the normal bone regarding the mechanical properties. Most studies about the bone quality have focused on the comparison of unhealthy and healthy bones regarding aging,41,42 disease development,43–45 and drug treatment.46–49 At present, little is known about the quality of the newly formed bone regenerated by tissue-engineered techniques. Microindentation by Vickers and ordinal mechanical testing were combined with the microcomputed tomography (μCT) imaging quantitative technique and histological examination of regenerated bone. The results confirmed that the microindentation correlates closely with the property of regenerated bone by OCP granules in Col matrix regarding maturation toward the quality of normal bone.
Materials and Methods
Implantation procedure
Twelve weeks old male Wistar rats were used. The principles of laboratory animal care were followed, as were national laws in that respect. All procedures were approved by the Animal Research Committee of Tohoku University. A standardized critical-sized (9 mm in diameter) defect was made in the rat calvaria bone, and a composite consisting of synthetic OCP granules having 300 to 500 μm diameter and porcine OCP/Col disc was implanted into the defect. The created defects were filled with the same volume of implants. Experimental rats were fixed 4, 8, and 12 weeks after the implantation of OCP/Col disc. The detail of the preparation procedures of OCP and OCP/Col are as reported previously.27,39
Some of the rats were fixed with 4% paraformaldehyde in 0.1 M phosphate-buffered saline and decalcified with 10% ethylenediaminetetraacetic acid in 0.01 M phosphate-buffered saline or in a mixture of 10% of formic acid, 2.9% citric acid, and 1.8% of trisodium of citrate dihydrate. The specimens were embedded in paraffin, and the center of the defect was extracted and sectioned coronally. Each specimen was stained with hematoxylin and eosin. Quantitative histomorphological analysis has been described previously. 40 The percentage of newly formed bone in the defect (n-Bone%) was calculated as the area of newly formed bone/area of the defect originally created by trephination × 100. The percentage of the remaining implant in the defect (r-Imp%), in addition, was calculated as the area of remaining implants of area of the defect originally created by trephination × 100. n-Bone% and r-Imp% were quantified on a computer using Scion Image public domain software (Scion Corporation, Frederick, MD).
Measurements of mechanical properties
All calvaria other than those used for micrograph analysis were stored in a 70% ethanol solution for at least 4 weeks before testing to dehydrate. It has been demonstrated that this treatment has no significant effect on the elastic properties of bone. 50 The plane surface, revealing the calvaria bone, was polished with fine sandpaper before hardness testing. A multipoint fixture was used so that the specimen of complex shape could be flexibly mounted in the base. As a result, the specimens could be used without cutting.
The Vickers microhardness of individual bone was measured using a hardness tester (HM-102; Mitutoyo, Kanagawa, Japan). A pyramidal diamond indenter with 135-degree angles was applied to the bone surface (BS) under a load of 4.9 N for 25 s. The hardness was determined by measuring the length of the diagonals of the indentations left by the tetrahedral indenter into the surface of a calvaria bone. The Vickers hardness value is the ratio of the load applied to the indenter to the surface area of the indentation hardness value = 2Psin (θ/2)/D 2 , where P is the applied load in kilograms and D is the mean length of the diagonals in millimeters. The measurement point was selected from independent three arbitrary places in three portions of calvaria that were equally divided.
After Vickers hardness was measured, these samples were used for a compressive test. A compressive test was used to fracture the specimens at a cross-head speed of 0.5 mm/min on a computer-controlled universal testing machine (EZ-L-500N; Shimadzu, Kyoto, Japan). The load and displacement of the cross-head were recorded when the specimen failed. The apparent elastic modulus was calculated as the slope of the initial linear portion of the stress–strain curve. The area under the stress displacement curve from zero to the point where the final densification starts was defined as the toughness, which is the energy required to cause breaking of the calvaria bone.
Assessment of bone microstructure
The calvaria bone was analyzed using a Microfocus X-Ray CT System (SMX-90CT; Shimadzu). The bone specimens were scanned continuously with increments of 20 μm thickness for 512 slices with a tube voltage of 90 kV and a tube current of 0.1 mA. The voxel size was 20 × 20 × 20 μm3. After the scanning, the image data were transferred to a workstation, and the structural indices and the mineralization of bone were calculated using a three-dimensional (3D) image analysis system (TRI/3D-Bon; Ratoc System Engineering, Tokyo, Japan). TRI/3D-BON builds 3D models from serial tomographic datasets for observation and morphometric analysis. The 3D images were segmented into voxels identified as bone and marrow. The gray-scale images were segmented using a strict filter to remove noise and a fixed threshold to extract the mineralized bone phase. The isolated small particles in marrow space and the isolated small holes in bone were removed using a cluster-labeling algorithm. The BS area was calculated using surface triangulation of the binary data based on the marching cubes method. The bone volume (BV) was calculated using tetrahedrons corresponding to the enclosed volume of the triangulated surface. The total tissue volume (TV) was the entire volume of the analysis. The normalized index, the bone surface to volume ratio (BS/BV), and the bone volume fraction (BV/TV) were then calculated from these values. In addition to bone structure, we also quantified the bone mineral density (BMD) at the level of calcified bone tissue. In advance, cylindrical phantoms containing a HA slurry including solid and the solution with various concentrations were imaged, and the linear relationship between the HA concentrations (0.3–0.7 g/cm3) and absorption was verified. The BMD was calibrated using this relationship.
Statistical analysis
Descriptive values of the data were represented as means ± standard error (SE). One-way analysis of variance was used to compare the means among groups. Probability values of p < 0.05 were considered to indicate statistical significance.
Results
The sample in the present study was divided into the decalcification group and undecalcification group. The decalcification group and undecalcification group were three samples (three rats) and five samples (five rats) per the implantation periods. Each mechanical test was performed by four samples; another one sample was used for the bone microstructure analysis in the undecalcification group.
Histological examination
The results of histological overview of the implants are shown in Figure 1a. The created defects were occupied by the forming tissue and the remnants of OCP/Col implanted at each time. After 4 weeks of the implantation, bone matrix was formed within the reticulum of OCP/Col. The newly formed bone seemed to increase with time. In 12 weeks, the newly formed bone matured and significantly increased. Osteoblasts were aligned around the surface of the OCP granules. New bone was directly formed adjacent to the OCP granules (Fig. 1b). On the other hand, multinucleated osteoclast-like cells were also attached to the surface of the OCP granules, suggesting that OCP biodegrades through cellular-mediated resorption process (Fig. 1c).
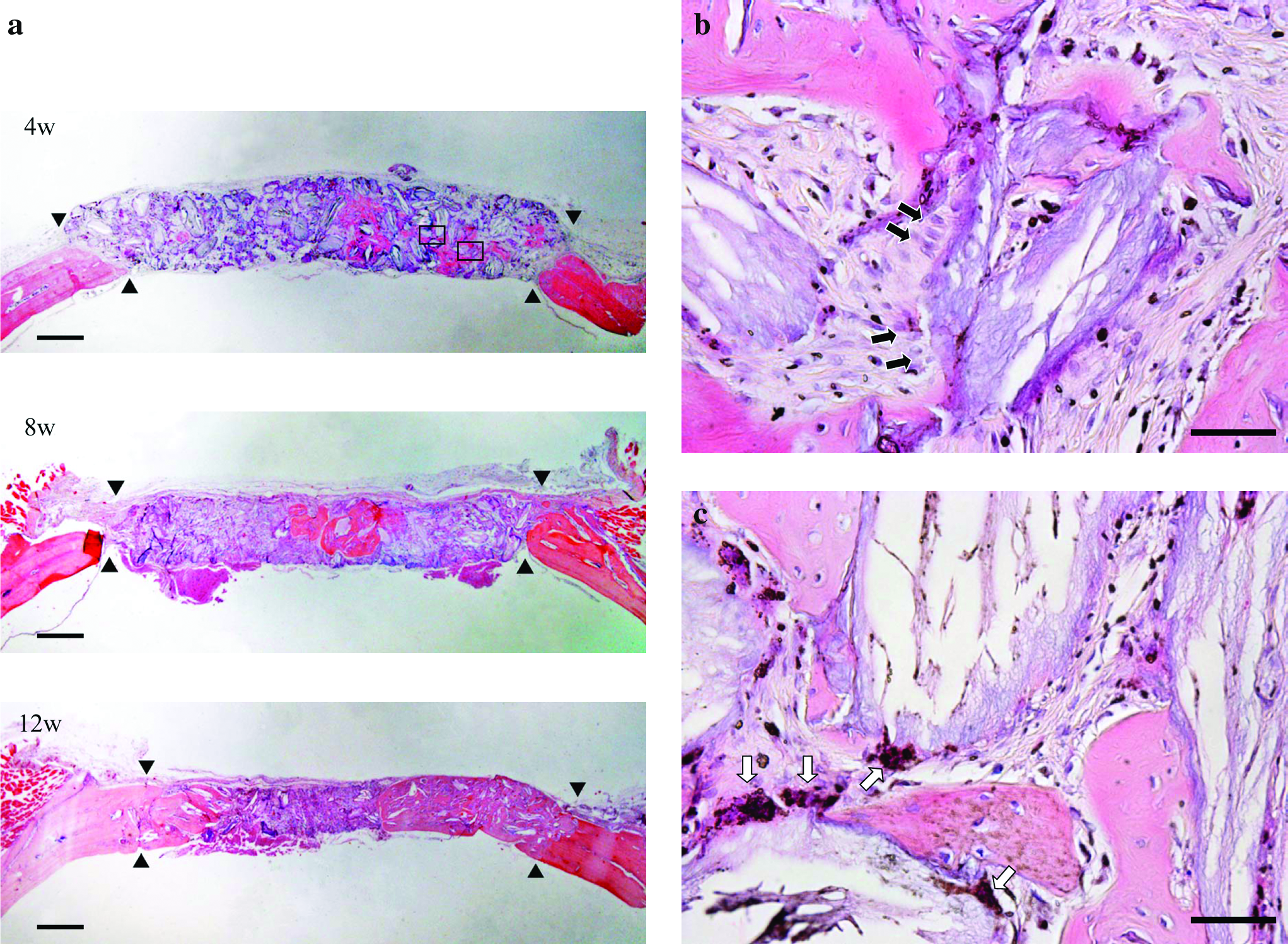
Histological and histomorphometrical analysis of OCP/Col implantation. (
Histomorphometrical findings regarding n-Bone% and r-Imp% are shown in Figure 1d. Mean n-Bone% ± SE in 4, 8, and 12 weeks was 23.03 ± 0.55, 39.95 ± 2.59, and 52.71 ± 1.71, respectively. n-Bone% was seen significantly to increase with implantation time. Mean n-Imp% ± SE in 4, 8, and 12 weeks was 16.88 ± 2.19, 14.70 ± 1.42, and 7.78 ± 1.00, respectively. No significant difference was seen between 4 and 8 weeks. By 12 weeks, resorption of the OCP granules was noted, coupled with the enhancement of new bone formation.
Mechanical evaluation
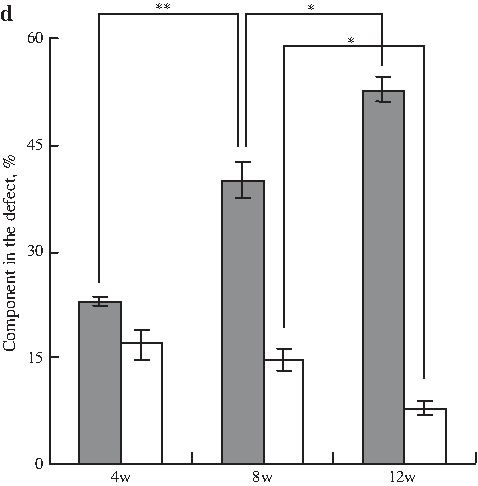
Microindentation is conventionally used for testing the hardness of synthetic materials or tissues. However, the precision and accuracy in testing tissues need further validation and exploration. Therefore, our experimental study was designed to test the differences in hardness from the immature tissue in the initial regeneration to the maturation stage with time. In the present study, the specimens were fixed using a special self-designed multipoint fixture. Nevertheless, all indentation marks were identifiable for defining the diagonals for measurement. In the microindentation testing, Figure 2a displays the Vickers hardness of various bone samples in rat calvaria for 4, 8, and 12 weeks and that in the untreated control. Each datum is the mean value of measurements (n = 36), with the error bar indicating the SE. The hardness could be expressed by the mean value, including that of the newly formed bone, the soft tissue, and the OCP granules dispersed in the Col matrix. With prolongation of the implantation time, the tissue hardness of the OCP/Col implanted group gradually increased and reached the value beyond that of the control (untreated without implantation).
Biomechanical parameters of the implanted OCP/Col in rat calvaria versus implantation periods. (
In the compressive testing, elastic modulus and toughness of each bone sample are shown in Figure 2b and 2c, respectively. Elastic modulus was significantly lower in the implanted group than in the control group. The toughness of the regenerated bone by OCP/Col was comparable to that by bone in the control group, although the elastic modulus was lower than the control value.
μCT evaluation
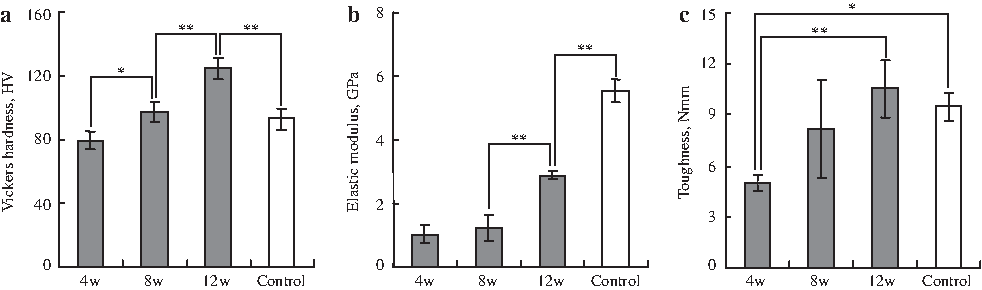
The 3D reconstruction of the bone structures in the rat calvaria by μCT is shown in Figure 3. In the implanted group, X-ray absorbance was scattered throughout the defect within 4 weeks and amalgamated in 12 weeks to a large area of the defect. The increase of radiopacity in the protuberance shows the formation of the new bone with increasing the calcification in relation to the implant. It seems likely that the newly formed bone was captured among the isolated OCP granules. Table 1 shows the quantification of the bone microstructure for 4, 8, and 12 weeks and that in the untreated control. Radiomorphometric data (BS/BV and BV/TV) in the control groups were different compared to those of the implanted groups. With the prolongation of the implantation time, the BS/BV gradually decreased. In contrast, BV/TV in bone formation increased to approximately 50% of the defect for 12 weeks. Likewise, the BMD appeared to increase with time.
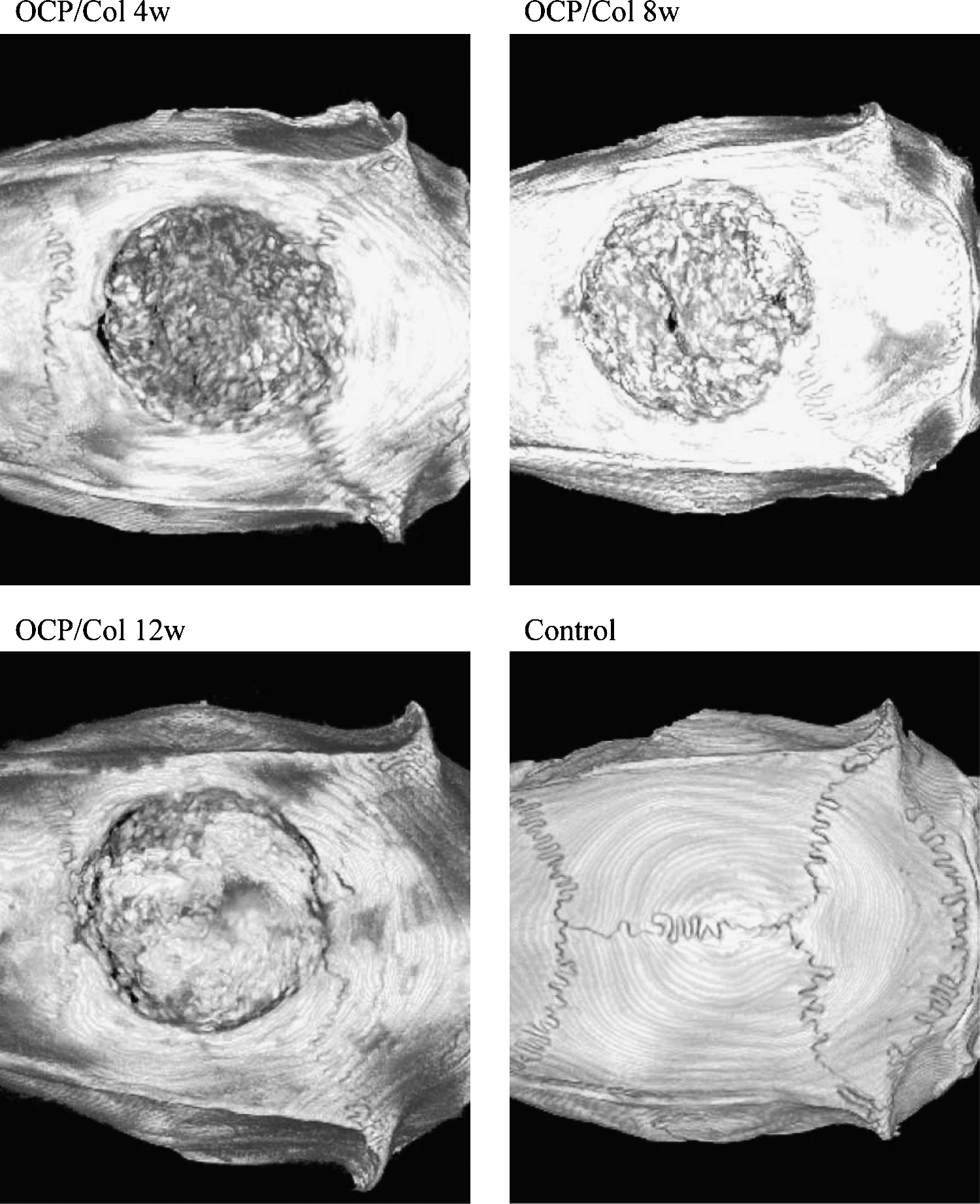
Three-dimensional microcomputed tomography images showing the implanted OCP/Col in the critical-sized defect of rat calvaria and the control (without implantation). The increase of radiopacity in the protuberance shows the formation of new bone along with time.
Each value was expressed as mean. The errors were calculated from the maximum error margin of the gray-level histograms in microcomputed tomography.
OCP/Col, octacalcium phosphate and collagen; TV, tissue volume; BV, bone volume; BS, bone surface; BMD, bone mineral density.
Discussion
The present study provides evidence that the regeneration of the newly formed bone by the implantation of OCP/Col up to 12 weeks in rat calvaria can be expressed by the increase of the hardness estimated by the microindentation technique. The increase of bone regeneration estimated by μCT and histological examination was identical to that of the increase of the hardness of the regenerated bone by the microindentation test. The results suggest that the present method used could be applied to the estimation of newly formed bone, especially to that of the tissue actively formed with time, stimulated by the implantation of osteoconductive biomaterials, such as biodegradable bone substitute material.
μCT analysis disclosed the characteristics of the 3D bone structure in rat calvaria regenerated by OCP/Col implantation with time. BMD has been suggested to be associated with the degree of mineralization and the architecture of bone, 51 although its accuracy could be affected by the geometric variations. 52 We hypothesized that the pattern of bone regeneration simulated by OCP granules within Col matrix and the structure could be reflected in the numerical value of BMD. In fact, it was apparent that the BMD and the BV/TV increased, while the BS/BV decreased with implantation period. The results show potentially the actual bone regeneration while TV and BV not always indicate definitive tendencies (Table 1), which could be overestimated or underestimated by the inaccuracy of the defect margin in size, resulting in affecting the radiomorphometric values. It is conceivable that the difference between BV/TV and BS/BV is reflecting the fact that the new bone formation was initiated from the surface of the OCP granules within the Col matrix, resulting in the individual OCP granules being surrounded by newly formed bone material at least in the early stage of bone regeneration. The hypothesis could be supported by the previous observation that the newly formed bone around the OCP granules alone33,34 or OCP granules within the collagen matrix39,40 became to agglomerate with time.
The microindentation testing of the regenerated bone revealed a progressive increase of the Vickers hardness showing the highest value in 12 weeks. This result suggests that the hardness of the bone increases with time, although OCP granules remained entirely unresorbed. It has been considered that bone strength depends on a variety of structural and material properties,53–55 including the amount of calcified bone tissue and the advancement of the organization of the tissue. The implantation experiment by OCP or OCP/Col may involve two aspects regarding the possible increase of the hardness: (1) OCP is converted to HA by itself27,28,30,56 and (2) OCP promotes apatite deposition around OCP particles.20,56 In the microindentation test, it seems likely that the new bone around the OCP granules within Col matrix became resistant to the Vickers indentation by their agglomeration. It is possible that such processes could raise the hardness of the new bone formed around the OCP granules. Some studies have reported that biological apatite crystals exist in intimate association with bone that retains its mechanical strength.12–15 Boskey confirmed that trabecular or cortical bone shows an increase in the mineral content, crystallinity, carbonate/phosphate ratio, and collagen maturity with age. 6 The intermolecular cross linking of bone collagen is attributed to the acquiring of the mechanical properties, such as tensile strength and viscoelasticity in the fibrillar matrices. In a microbeam X-ray diffraction (XRD) study, it was reported that a newly formed bone matrix with a less anisotropic microstructure decreases its elastic modulus with age. 12 In this study, it was also verified that the biological apatite crystals display mechanical anisotropy along their c-axis.11,12 It is still undetermined whether HA crystals converted from the OCP can indicate such an orientation in the implantation site, although the OCP can be converted into HA topotaxially without changing its original plate-like c-axis elongated morphology both in vitro 57 and in vivo. 56
The present mechanical testing demonstrated that elastic modulus increased modestly, whereas the toughness increased markedly although its level was compatible to that of the control calvaria bone. This might be happened by the specific pattern of bone regeneration by the OCP granules that the bone matrices are primary formed around the OCP granules dispersed within Col matrix in the initial stage, then the formed bones are agglomerated with the implantation period. The fact that the elastic modulus of the implanted group was significantly lower in the control group could be explained by the assumption that the bone regeneration is still under a developmental stage at least regarding the elastic modulus. In mechanical testing, since the loading rate of the external stress exceeds the interior assigning rate, the OCP granules, which could be brittle inorganic material, may be fractured abruptly. There seems to be still a discrepancy that the increase of the hardness did not follow the tendency of the increase of elastic modulus (modest increase) but, rather, that of the toughness (increase up to that of the control). Although the histological analysis using undecalcified specimens is required to clarify the quality of the newly formed bone matrix, these parameters may be related to the extent of mineralization in osteoid tissue formed around the OCP granules in the Col matrix. The proteinacious tissue, rather than the inorganic mineral, could improve the toughness of the tissue.
We analyzed the mechanical properties of the regenerated bone by the implantation of OCP/Col. The bone microstructure and the mineralization in the matrix are considered to be the factors to control the quality and the strength. The relationship between the quality and the strength in bone has usually been studied using the tissues suffering from bone diseases, such as osteoporosis, in which the bone mass or density decreases. Multipronged approaches have been required to analyze the quality because the bone is a complex tissue. It seems likely that the material characteristics, including the shape or biological responses, may be critically important in analyzing the tissue regeneration enhanced by the implantation of scaffold materials, such as biodegradable OCP material. The present findings may provide a method for the evaluation of the newly formed bone created with biodegradable materials.
Footnotes
Acknowledgments
This study was supported in part by Grants-in-Aid (17076001, 18800007, 19390490, 19700399, and 20659304) from the Ministry of Education, Science, Sports, and Culture of Japan.
Disclosure Statement
No competing financial interests exist.