
Abstract
Current treatment of traumatic craniofacial injuries often involves early free tissue transfer, even if the recipient site is contaminated or lacks soft tissue coverage. There are no current tissue engineering strategies to definitively regenerate tissues in such an environment at an early time point. For a tissue engineering approach to be employed in the treatment of such injuries, a two-stage approach could potentially be used. The present study describes methods for fabrication, characterization, and processing of porous polymethylmethacrylate (PMMA) space maintainers for temporary retention of space in bony craniofacial defects. Carboxymethylcellulose hydrogels were used as a porogen. Implants with controlled porosity and pore interconnectivity were fabricated by varying the ratio of hydrogel:polymer and the amount of carboxymethylcellulose within the hydrogel. The in vivo tissue response to the implants was observed by implanting solid, low-porosity, and high-porosity implants (n = 6) within a nonhealing rabbit mandibular defect that included an oral mucosal defect to allow open communication between the oral cavity and the mandibular defect. Oral mucosal wound healing was observed after 12 weeks and was complete in 3/6 defects filled with solid PMMA implants and 5/6 defects filled with either a low- or high-porosity PMMA implant. The tissue response around and within the pores of the two formulations of porous implants tested in vivo was characterized, with the low-porosity implants surrounded by a minimal but well-formed fibrous capsule in contrast to the high-porosity implants, which were surrounded and invaded by almost exclusively inflammatory tissue. On the basis of these results, PMMA implants with limited porosity hold promise for temporary implantation and space maintenance within clean/contaminated bone defects.
Introduction
Even in the civilian population, traumatic craniofacial bone injury is often accompanied by injury or loss of surrounding soft tissues. 4 One of the major difficulties reconstructive surgeons face when treating injuries involving significant bone loss is contracture and scarring of the overlying soft tissue envelope, which compromises facial projection and makes staged repair of bony structures difficult.5,6 Previously, definitive bone reconstruction was delayed until soft tissue coverage and a sterile wound environment were achieved.7,8 More recently, despite reports of local complications and wound infection rates as high as 100% in civilians suffering gunshot wounds to the face,9,10 early definitive repair of facial gunshot wounds via free tissue transfer has become common as the well-vascularized tissues that are transferred survive well in hostile wound environments.8,11
The field of regenerative medicine and the technologies borne from tissue engineering offer great hope toward providing an alternative and possibly better approach to regenerating injured or destroyed tissues. Most proposed tissue engineering strategies, however, currently require planning in the form of material fabrication, autologous cell harvest and expansion, and/or ex vivo tissue generation. Additionally, little to no evaluation of tissue engineering approaches is currently performed in wound environments involving infection, significant vascular injury, and large-scale tissue devitalization such as that encountered in a battlefield wound. Therefore, the successful use of a tissue engineering approach to provide immediate, definitive regeneration of tissues injured during craniofacial trauma such as those encountered during military service is unlikely using current approaches.
In the absence of immediate reconstruction, clinical management of facial bone loss can involve the placement of an alloplastic space maintainer to provide a template for future definitive reconstruction and prevent wound contracture into the space normally occupied by bone. 12 Polymethylmethacrylate (PMMA) is commonly used in such space maintenance applications12,13 and others within the craniofacial complex. 14 Although PMMA has many desirable characteristics for such applications (moldable, FDA-regulated, and familiar to surgeons), a number of problems exist with respect to wound healing around PMMA implants and other alloplastic craniofacial implants.15–17
For the purposes of facilitating a long-term tissue engineering approach to treating composite craniofacial defects, a temporary implant or space maintainer would allow time for a regenerative medicine approach to be used to definitively regenerate the injured or absent tissue. In addition to providing space maintenance, such a temporary implant could be used to prime the defect site, enabling better long-term success of the definitive regenerated tissue construct. Previous work has shown that recipient-site characteristics such as vascularity are important for the regeneration of new bone tissue and support of grafted tissue.18–20 For mandibular reconstruction, the defect site and surgical approach along with recipient-site complications such as infection, intraoral exposure, and prolonged antibiotic use have been significantly linked to graft failure.21,22 An ideal temporary space maintainer will therefore not only maintain the osseous void and prevent soft tissue collapse or contracture into the space, but also will allow or promote soft tissue coverage and healing without serving as a nidus for local infections.
Despite the aforementioned shortcomings associated with solid PMMA implants, we hypothesized that an implant made of modified PMMA could fulfill many of these criteria. Previously, a number of groups have explored different methods for making porous PMMA.23–28 On the basis of this work, we hypothesized that porous PMMA implants with reproducibly tunable pore structure could be fabricated using a carboxymethylcellulose (CMC) hydrogel as an aqueous porogen. When tested in a clean/contaminated rabbit mandibular defect, we hypothesized that these implants would be able to maintain the defect space while promoting soft tissue coverage of the implant.
Materials and Methods
Experimental design
For the first part of this study, porous PMMA implants were synthesized and characterized using a CMC hydrogel as an aqueous phase to impart porosity on the implants. The percent of CMC in the aqueous phase and the ratio of aqueous phase:polymer phase were varied to control the bulk and surface characteristics. After characterization of the porous implants, two formulations, one with high bulk porosity and pore interconnectivity and one with lower porosity and less pore interconnectivity, were compared over 12 weeks in vivo to a solid PMMA implant within a modified rabbit mandibular defect.
Implant fabrication and characterization
Solid and porous PMMA implants were fabricated using a clinical-grade PMMA bone cement (SmartSet High Viscosity; DePuy Orthopaedics, Warsaw, IN) consisting of a powder of methylmethacrylate (MMA)/methyl acrylate copolymer, benzoyl peroxide, and zirconium dioxide and a liquid phase with MMA, N,N-dimethyl-p-toluidine, and hydroquinone. For the solid implants, the solid and powder phases were mixed according the manufacturer's specifications for approximately 90 s and, once they reached a dough-like consistency, packed into custom-fabricated 10-mm-diameter ×6-mm-height cylindrical Teflon® (DuPont, Wilmington, DE) molds. The solid implants were then allowed to harden at room temperature for 30 min before being removed from the molds and vacuum-dried overnight.
For porous implants, 7 and 9 wt% CMC hydrogels were prepared by dissolving the appropriate amount of United States Pharmacopeia–grade low-viscosity CMC (Spectrum Chemical Manufacturing Corp., Gardena, CA) in distilled water. The powder component of the PMMA cement was then mixed with the CMC hydrogel such that the powder was uniformly suspended within the aqueous phase. The liquid component of the PMMA cement was then added to the mixture of aqueous/powder phases. Aqueous-phase weight percentages of 30, 40, and 50 wt% were used to fabricate the implants, resulting in six experimental groups. The aqueous and polymer phases were then stirred by hand for approximately 90 s and packed into Teflon molds of the same size as the solid PMMA implants. The porous implants within molds were then allowed to harden for 30 min before being removed from the molds and placed within individual cassettes, and the aqueous phase was then leached from the implants in deionized, distilled water as previously described. 29 The porous PMMA implants were then vacuum-dried overnight in a laboratory freeze dryer (Lyph-Lock 4.5; Labconco Corp., Kansas City, MO).
Implant porosity and pore interconnectivity were analyzed using microcomputed tomography (μCT) as previously described. 30 Briefly, implants (n = 3) from all experimental groups were scanned using a SkyScan 1172 μCT imaging system (SkyScan, Aartselaar, Belgium). High-resolution 1280 × 1024 pixel images were created by scanning at an 8 μm/pixel resolution with no filter at voltage and current settings of 40 kV and 250 μA, respectively. Serial tomograms were reconstructed, resliced, and analyzed using NRecon and CTAn software packages provided by SkyScan. For porosity and pore interconnectivity analyses, the scanned object volumes were binarized using a global threshold of 60–255. Porosity and interconnectivity were determined using a 9-mm-diameter × 5-mm-height cylindrical volume of interest to eliminate edge effects. Pore interconnectivity was determined by repeatedly applying a shrink wrap algorithm with minimum interconnection sizes ranging from 40 to 320 μm. Interconnectivity is reported as the percentage of pore volume accessible from outside the volume of interest with pores considered accessible only if the interconnection to that pore allowed a sphere with diameter of the user defined minimum interconnection size to pass through.
Scanning electron microscopy was also used to examine the external surface of the implants. Implant surfaces were sputter-coated with gold for 40 s at 100 mA using a CrC-150 sputtering system (Torr International, New Windsor, NY) and observed at an accelerating voltage of 10 kV using an FEI Quanta 400 field emission scanning electron microscope (FEI company, Hillsboro, OR).
In vivo implant evaluation
Solid PMMA implants and porous implants (9 wt% CMC within the aqueous phase and both 30 and 40 wt% total aqueous phase in the implant) were evaluated in vivo using a modification of a nonhealing rabbit mandibular defect model. 31 All surgical procedures followed protocols approved by the Institutional Animal Care and Use Committees at both Rice University and the University of Texas Health Science Center at Houston. Eighteen healthy male adult New Zealand white rabbits (n = 6 per group) at least 6 months old and weighing 3.5–4 kg were purchased from Myrtle's Rabbitry (Thompson Station, TN). Before implantation, all implants were sterilized using ethylene oxide.
Briefly, each animal was given preoperative intramuscular doses of buprenorphine hydrochloride (0.1 mg/kg body weight) for postoperative analgesia and 0.5 mL Durapen® (150,000 U/mL penicillin G benzathine and 150,000 U/mL penicillin G procaine) for perioperative antibiotic coverage. Before induction, ketamine hydrochloride (40 mg/kg body weight) and xylazine hydrochloride (7.5 mg/kg body weight) were given, after which rabbits were placed in a supine position, intubated, and placed under general anesthesia using an isoflurane–O2 mixture (2.5%–3% isoflurance for induction, 2% for maintenance) with constant cardiac and respiratory monitoring. The animals were then surgically prepped and draped, after which a 7-cm midline incision through the skin and superficial fascia was made beginning 0.5 cm posterior to the mentum. Using blunt dissection and electrocauterization, the left masseter was exposed and the soft tissue along the inferior border of the body of the left hemimandible was mobilized such that the periosteum covering the body of the mandible could be incised and elevated, exposing a 4 × 1.5 cm area on the lateral surface of the mandible. A 10-mm titanium trephine (Ace Surgical Supply, Inc., Brockton, MA) attached to a Stryker TPS® surgical handpiece (Stryker, Kalamazoo, MI) operating at 15,000 rpm with copious normal saline irrigation was used to create a bicortical defect through the exposed body of the left mandible. A 701 bur in combination with the surgical drilling unit was used to cut a 2–3-mm window through the alveolar ridge in the middle of the defect to provide access for removal of the crowns of the associated teeth and provide intraoral exposure of the defect. The defect site was thoroughly washed with normal saline, after which an implant was placed within the defect. The order of implant placement was randomized, and none of the surgical personnel, who were the same throughout the study, were aware of which implant was being used. Before closure, a titanium supporting plate (1.5-mm six-hole heavy-gauge titanium; Synthes, West Chester, PA) was secured in place to prevent iatrogenic fracture during the course of the study. The incision was then closed in three layers (muscle, fascia, and skin) using degradable sutures (Vicryl polyglactin sutures; Ethicon, Somerville, NJ). After wound closure, anesthesia was reversed, and the animals were extubated.
Postoperatively, the animals were given access to food and water ad libitum. Food was limited to a soft recovery diet (Critical Care for Herbivores; Oxbow Pet Products, Murdock, NE) and shredded or mashed fruits and vegetables to reduce stress on the mandible. All animals survived the 12-week postoperative period without complications.
Gross characterization
After 12 postoperative weeks, each rabbit was euthanized via intravenous injection of 1 mL Beuthanasia-D® (390 mg/mL pentobarbital sodium and 50 mg/mL phenytoin sodium). The left hemimandibles were then carefully dissected from the cranium with care taken to preserve the soft tissue surrounding the implant and within the oral cavity. The oral mucosa and dentition covering the alveolus of each specimen was examined to detect any areas of implant or bone exposure. Specimens were individually placed in 10% neutral buffered formalin and stored on a shaker table at 4°C for 72 h.
Histology
After fixation, samples were dehydrated, stored in 70% ethanol, and then embedded in MMA. After polymerization of the MMA, three coronally oriented 10-μM-thick sections through the center of each implant were cut using a modified diamond saw technique 32 and subsequently stained using methylene blue/basic fuchsin.
Each of the stained sections was analyzed using light microscopy (Zeiss Axio Imager Z1 and AxioCam MRc 5; Carl Zeiss AG, Oberkochen, Germany) by two blinded observers (S.Y. and F.K.K.). A quantitative scoring system (Table 1) was used to score the tissue response at the implant interface and within the pores of the porous implants.
Statistical analyses
Implant porosity data were analyzed using single-factor analyses of variance with post hoc pairwise comparisons made using Tukey's Honestly Significant Difference (HSD). Oral mucosal wound healing, as observed grossly and confirmed by microscopy, was analyzed using a Fisher–Freeman–Halton test. Histological scoring was analyzed using nonparametric statistics. The tissue response at the implant interface was analyzed using a Kruskal–Wallis one-way analysis of variance, with subsequent pairwise analyses made using the Dwass–Steel–Critchlow–Fligner test. A Mann–Whitney U-test was used to analyze the tissue response within the pores of the two porous implant types. The a priori level of significance for all analyses was chosen as α = 0.05. All analyses were performed using R version 2.10.0 (R Foundation for Statistical Computing, Vienna, Austria).
Results
Implant fabrication and characterization
Porous PMMA/CMC implants were reproducibly fabricated as described in the Materials and Methods section. μCT analyses showed that porosity increased as expected with increasing incorporation of the aqueous phase (Fig. 1). Significant differences in implant porosity were observed between all groups as the aqueous phase incorporation increased. Varying the amount of CMC within the aqueous phase did not significantly alter the implant porosity.

Porosity values as calculated by microcomputed tomography (μCT). Samples were scanned and the resultant scans were reconstructed, reoriented, and binarized. Implant porosity was determined using a cylindrical (9 mm diameter ×5 mm height) volume of interest slightly smaller than the implant dimensions to eliminate edge effects. Data are reported as means ± standard deviation (n = 3). The asterisk over a bar denotes a statistically significant difference (p < 0.05) as detected using analysis of variance and Tukey's post hoc tests between the group marked and the group with the same % carboxymethylcellulose (CMC) but lower aqueous phase in relation to polymer phase. No statistically significant differences in porosity were found as a result of changing the % carboxymethylcellulose from 7% to 9%.
Pore interconnectivity also increased with increasing aqueous phase incorporation (Fig. 2). Interconnectivity appeared to be affected by the percentage of CMC in the aqueous phase; the more negative slope observed for implants with 9% CMC within the aqueous phase indicates that more of the interconnections in these implants were smaller than for those implants fabricated with 7% CMC in the aqueous phase.

Implant interconnectivity percentages as a function of the minimum interconnection size. Samples were scanned and processed as reported in the Materials and Methods section, and a built-in software package was used to determine the percentage of the implant porosity that was accessible from outside the volume of interest. Data are reported as means ± standard deviation (n = 3).
Scanning electron microscopy images and μCT reconstructions also showed differences in the porosity and surfaces of the fabricated implants (Fig. 3). The porosity increases with increasing aqueous phase incorporation quantitatively detected with μCT are seen in cross sections and surface images of the implants. Further, the pore size appears more consistent within implants fabricated using 9% CMC in the aqueous phase, likely resulting in the relative abundance of smaller pore interconnections within these implants compared to those fabricated using 7% CMC.

Representative images of implant cross sections and surfaces. Cylindrical implants (10 mm diameter × 6 mm height) from each experimental group were scanned by μCT or scanning electron microscopy (SEM). Virtual μCT cross sections of the implants were made by slicing through the center of the axially oriented implant. For electron micrographs, the scale bars represent 500 μm.
In vivo implant evaluation
On the basis of the implant characterization, solid PMMA implants, 9% CMC 30 wt% implants (16.9 ± 4.1% porosity, 39.7 ± 9.4% interconnectivity at a 40 μm minimum connection size), and 9% CMC 40 wt% implants (44.6 ± 2.1% porosity, 81.2 ± 1.0% interconnectivity at a 40 μm minimum connection size) were chosen for implantation in the in vivo phase of the study. All animals survived the surgery and postoperative period without complications. No changes in eating habits or activity were noted by the investigators, husbandry staff, or veterinary staff.
Gross characterization
At the time of animal euthanasia and implant/hemimandible harvest, no signs of mobility or infection were noted in any of the animals or visible tissues after harvest. Wound healing (closure) of the oral mucosa over the alveolar ridge at the site of the intraoral communication was assessed grossly (Fig. 4) and correlated to histological results (Table 2) to confirm the gross observations. Wound healing was considered incomplete when any exposed bone or implant could be grossly observed and histology also indicated a failure of soft tissue coverage over the implant or within the defect. The increase in oral mucosal wound healing observed in defects filled with both low- and high-porosity implants (83% of defects healed in each group) versus nonporous PMMA implants (50% healed) was not statistically significant (p > 0.08).

Representative gross views of harvested tissue covering the alveolus and implant. (
Histology
Histology and histological scoring were performed to assess the ability of the implants to maintain space within the surgically created osseous void and to view and quantify the soft tissue response around and within the implants. At low magnifications allowing coronal views of the entire implant and defect in cross section, all implants successfully maintained the defect space within the hemimandible. This space maintenance was confirmed by the lack of tissue collapse or contracture into the space occupied by the implants with the exception of tissue invading the pores of the porous implants (Fig. 5).

Representative light micrographs (25 × magnification) of coronally sectioned tissue samples through the center of the (
At higher magnification, the tissue response at the implant–tissue interface and within the implant pores could be observed (Fig. 6). At the implant–tissue interface, both the low-porosity and solid implants were in many cases surrounded by a thin, well-organized fibrous capsule. The low-porosity implants were also in direct contact in many areas with any newly formed bone observed at the implant interface. The high-porosity implants were primarily surrounded by an abundance of inflammatory plasma cells at the implant interface, and a similar inflammatory cell population was observed within the pores of the highly porous implants. When a quantitative scoring system was applied, the interfacial tissue response for the highly porous implants was statistically significantly different from the response observed around both the solid and low-porosity implants (Fig. 7, p < 0.05). Similarly, the difference in tissue response within the pores of the low- and high-porosity implants was statistically significant (Fig. 7, p < 0.05).
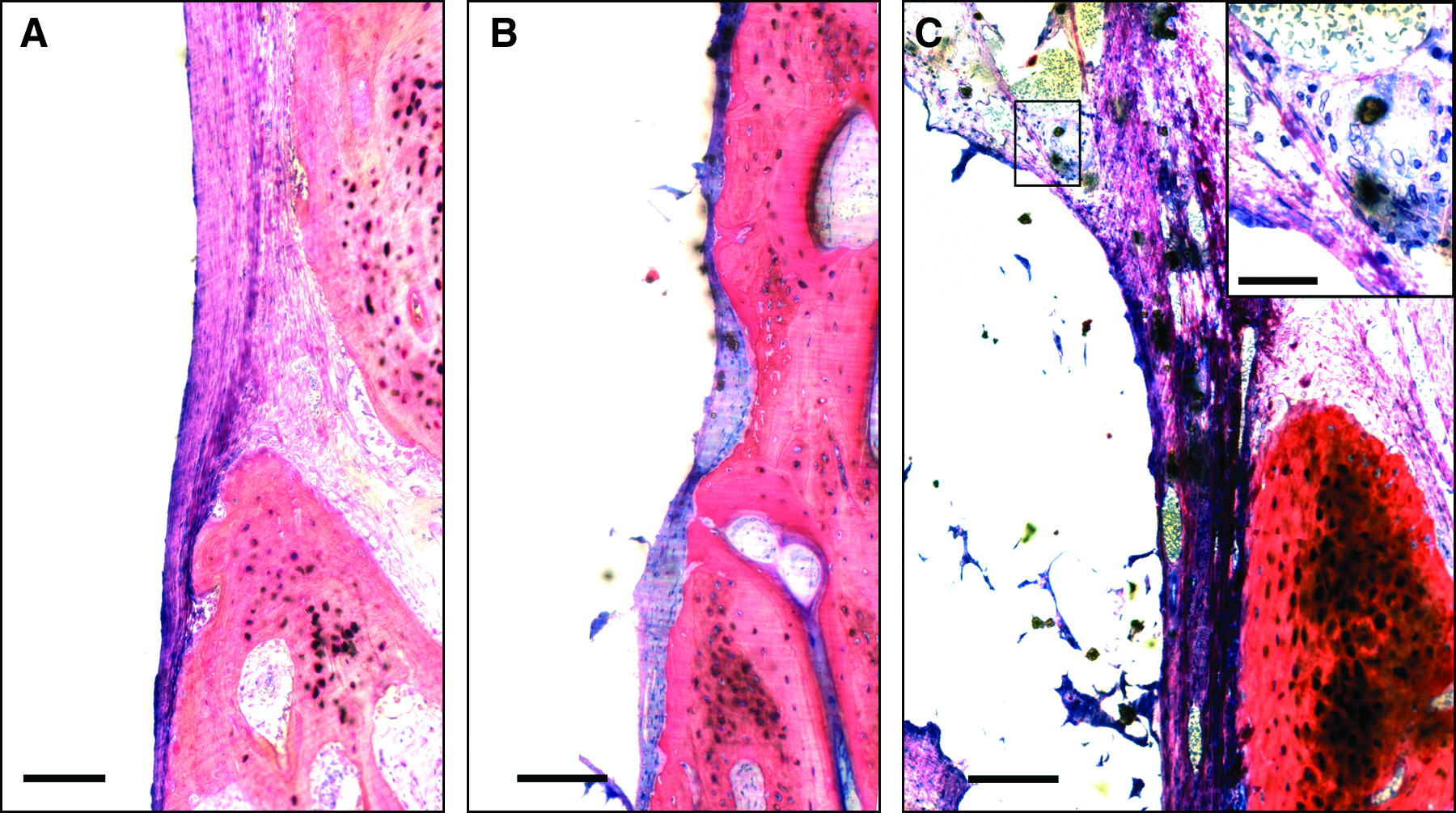
Representative light micrographs (200 × magnification) of the lingual surface of coronally sectioned tissue samples through the center of the implanted (
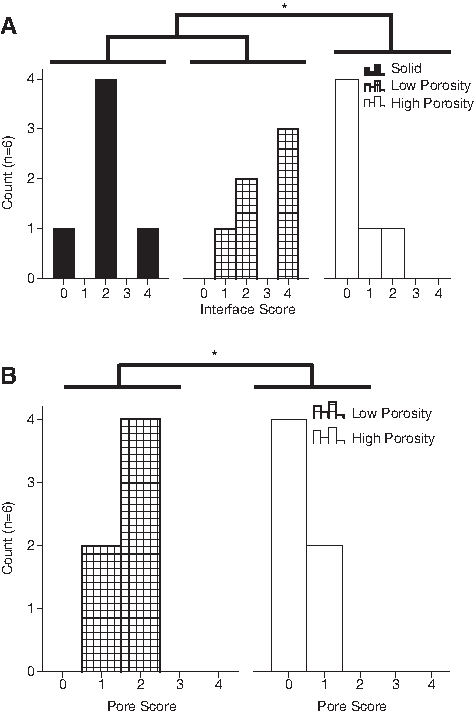
Score distributions for the graded (
Discussion
Temporary space maintainers have historically been used clinically to prevent soft tissue collapse into bony defects and provide a template for delayed bone healing or grafting.12,33 Recently, however, space maintenance has been used infrequently, particularly in the staged repair of traumatic injuries, as immediate free tissue transfer has eliminated the need for space maintenance and staged repair. Additionally, problems with existing biomaterials such as problems with healing of surrounding tissues, implant extrusion, or bacterial colonization have further limited the use of space maintainers, particularly in applications where soft tissue healing or infection may be a concern.34,35 Unfortunately, due to limitations in current tissue engineering technology, injuries involving lacking or devitalized soft tissues or the possibility of infection are precisely the type a staged repair using temporary space maintenance might allow a regenerative medicine approach to be undertaken.
The present study aimed to evaluate methods to reproducibly fabricate and characterize porous PMMA implants using a CMC porogen and to then develop an animal model to test selected formulations in a nonhealing bone defect that approximated a more toxic wound environment than most traditional animal models. In the first part of the study, porous PMMA implants were fabricated in a one-step process by incorporating a CMC hydrogel that could be leached away rapidly in vitro or in vivo. Varying both the amount of CMC within the aqueous phase and the relative amount of aqueous phase to polymer phase allowed for well-controlled porosity and pore interconnectivity. As expected, higher percentages of porogen resulted in greater implant porosity, while increasing the viscosity of the aqueous phase porogen by incorporating of greater amounts of CMC within the hydrogel led to a more consistent pore size and higher pore interconnectivity when the minimum interconnection size was decreased.
In the second part of the study, two formulations of porous PMMA implants and solid PMMA implants were implanted into nonhealing rabbit mandibular defects that had been contaminated through an open communication with the oral cavity. Porous PMMA formulations were selected such that both a highly porous, highly interconnected implant (9% CMC 40 wt%) and an implant of lower porosity and lower interconnectivity could be compared (9% CMC 30 wt%). Healing of the communication into the oral cavity was assessed as well as the tissue response both around and within the implants. All formulations successfully maintained space within the defect. Soft tissue was only observed within the defect when it was penetrating the pore network in the two formulations of porous implant. The oral mucosal defects created to allow communication into the bone defect healed in more cases (5/6 healed for both low- and high-porosity implants) when the bony defects were filled with porous implants than when filled with solid implants (3/6 healed), although the differences between groups were not statistically significant.
Although the gross mucosal defect closure over the high- and low-porosity implants was equivalent, microscopically, the tissue response around and within the pores of the low-porosity implants was more favorable. At the implant–tissue interface, a small, well-formed capsule or direct tissue–implant contact was typically observed around the low-porosity implants. Immature fibrous tissue with few inflammatory elements was generally seen within the filled pores of the low-porosity implants. Contrastingly, the tissue surrounding and within the pores of the highly porous implants was almost exclusively inflammatory, consisting mostly of plasma cells. Thus, the low-porosity and solid implants elicited a more favorable soft tissue response than the highly porous implants, while the porous implants may have provided a template for improved wound healing in comparison to the solid implants.
The current study has a number of strengths. First, although porous PMMA has been well studied,24,27,36–39 including porous PMMA fabricated using an aqueous phase consisting of a CMC hydrogel as a porogen,25,40 the present study is one of the first systematic studies of fabrication methods to quantitatively examine the effect of both the ratio of aqueous phase to polymer phase but also the effect of the aqueous phase viscosity as done by varying the amount of CMC within the aqueous phase. Increasing the viscosity of the aqueous phase by using a 9 wt% CMC hydrogel, as opposed to a 7 wt% CMC gel as has been previously used, 41 resulted in a more consistent pore architecture with smaller, more consistently sized pore interconnections. Because of this, both porous implant formulations chosen for the in vivo study were fabricated with 9 wt% CMC hydrogels. An additional benefit of the chosen materials is that both PMMA and CMC are FDA regulated for craniofacial applications, and the fabrication of the implants can be done in a standard operating room with only minor alterations in the manufacturer-recommended preparation of PMMA.
A strength of the in vivo portion of the study was the development of a more clinically relevant animal model that may better simulate the type of clinical situation in which the technology investigated may be used. The animal model was based on a previously developed rabbit mandibular defect 42 that was modified to allow contamination of the wound through an opening into the oral cavity. This conferred several advantages. First, mucosal wound healing within the rabbit oral cavity is a well-established method for evaluating wound healing,43–47 particularly when evaluating biomaterial-guided wound healing.48–53 Second, in the clinical setting, the presence of intraoral communication is significantly correlated to decreased bone graft survival time, 22 and thus an implant evaluation strategy that focuses on the closure of these communications is relevant for a situation where definitive repair will be performed using a standard or tissue-engineered bone graft. With relation to the presence of these intraoral communications, infection is a major concern when dealing with any implantable biomaterial, 54 particularly PMMA,55,56 and thus evaluating the tissue response to the implant in an environment where it will most likely be exposed to bacteria strengthens any conclusions drawn with respect to optimal material formulations. Finally, although the observed differences in oral mucosal wound healing do not allow one to draw any definitive conclusions about how the presence of porosity affected the oral mucosal wound healing, this study establishes the statistical parameters necessary to determine the statistical power needed to achieve significance in future studies using this model. While a difference in healing clearly existed between both the high- and low-porosity implants and the solid PMMA implants, the difference was not significant. Somewhat surprisingly, the difference in tissue response to the porous implants based on histological scoring was significant and may be an important parameter not only for initial wound healing but also for subsequent bone regeneration.57–59
This study is not, however, without weaknesses. First, an ideal tissue engineering solution to the problem of complicated craniofacial bone defects would not involve multiple interventions and delayed reconstruction. An ideal solution would use a degradable material 60 that could address the issues of soft tissue coverage, infection, and bone regeneration concurrently, thus eliminating the need for and risks associated with repeated operations. At present, such a solution does not exist nor does there appear to be any such solution developed for use in the near future. While the animal model developed is viewed by the authors as one of the strengths of this method of material evaluation, the complexity of the model may also be viewed as a weakness. Not only is the tooth-bearing segment of the mandible more complicated in structure than many craniofacial bones, it is also exposed to very different mechanical stresses than other bones. 61 Further, the method of wound contamination was poorly controlled. Oral flora of the rabbits and the amount of flora that passed through the communication was likely variable between animals.
Limited research is available investigating PMMA strictly for use as a space maintainer; however, PMMA has a long track record of use in craniofacial applications. In an early study using PMMA to repair canine mandibular defects, Worley reported that repair failed in 7 of 11 dogs due to wound dehiscence over solid PMMA implants. 62 Kangur et al. reported similar problems with mucosal dehiscence over solid PMMA used to fix canine mandibular fractures and attributed the presence of an acute inflammatory tissue response to the PMMA to this oral communication. 63 Despite these findings, a number of studies exist that report no complications with solid PMMA use in craniofacial applications.12,35,64,65
Porous PMMA, as previously mentioned, has also been investigated in animal studies and limited clinical use. In a long-term study in guinea pigs comparing porous and solid PMMA implanted in the hypodermis, van Mullem et al. reported implant extrusion occurred in 4/36 solid implants and none of the porous implants. 26 Similar to the present study, the same study noted that foci of inflammatory cells were found more frequently around and within the porous PMMA implants (1:1 aqueous phase:polymer phase) than the solid implants. Clinically, the porous PMMA seems to have been used successfully with little note of complications, 66 and, although reports of long-term results are rarely found, the current study differs from those previously published as the intent is for the porous implants to only be used as temporary implants.
Using the presented methods for fabrication and evaluation, the porous PMMA implants appeared to promote or allow wound healing of the oral mucosa better than the solid implants, although not significantly so. Significant differences in the tissue response to the two formulations of porous implants were also observed. A number of possible explanations exist for these two findings. The trend of improved wound healing with use of the porous implants may best be explained by increased tissue integration within the pores of the implants. This may have limited implant micromovement and improved the rate at which new tissue formed across the implant to close the communication. Similar improvements in wound healing and implant retention have been found when using porous polyethylene for the fixation of bone-anchored hearing aids.67,68
The inflammatory tissue response around and within the highly porous implants was likely caused by increased bacterial seeding of these implants. The increased porosity and interconnectivity of these implants compared to those of the low-porosity and lower interconnectivity group likely led to bacterial accumulation deeper within the implant in areas where the bacteria could not effectively be cleared. Kiechel et al. compared infection control within porous and nonporous PMMA seeded with Staphylococcus aureus and implanted in the paravertebral fascia of rabbits and found increased infections occurred in animals implanted with porous PMMA implants. 69 Sclafani et al. found that increased porosity increased the resistance to infection in implants inoculated 14 days after implantation but not if the implants were inoculated at the time of implantation. 70 Thus, in applications and models where contamination or infection exists at the time of implant placement, an appropriate balance with respect to porosity is needed to allow tissue ingrowth and implant integration but not bacterial seeding deep within the implant. If contamination is not present at the time of implantation, fibrovascular ingrowth has been shown to occur rapidly and thus a more porous implant may be acceptable. 71 Additionally, studies of induced membranes or capsules around PMMA implants suggest that the formation of a well-formed capsule around the implant, as seen more frequently around the low-porosity implants in this study, may facilitate greater success of later efforts aimed at definitive bone regeneration, provided that the capsule is not destroyed during implant removal and any necessary debridement.57–59 Finally, it is important to note that the method of fabrication of the porous PMMA implants may lead to particulate PMMA release, 72 which could account for the inflammatory response elicited by the highly porous implants. 73
On the basis of the results of the present study, the low-porosity space maintainers appear to be a promising alternative to solid PMMA for temporary implantation as part of a regenerative medicine approach to treating traumatic craniofacial injuries. Future work in this area should focus on tissue regeneration within the maintained space as well as release of any bioactive factors from the space maintainer such as antibiotics or growth factors that may better ensure success of later stage tissue engineering efforts. The characterized implants may provide a critical step in allowing the use of regenerative medicine approaches as an alternative to traditional approaches in treating contaminated or open traumatic defects. The methods described for the fabrication of these implants may be applicable to a wide variety of different materials, and the animal model described may provide a more useful analog to clinical situations where tissue engineering strategies may need to be used in possibly contaminated environments.
Conclusions
Methods were developed allowing porous PMMA space maintainers to be reproducibly fabricated using a CMC hydrogel as an aqueous phase porogen. Porosity and pore interconnectivity can be controlled by varying the ratio of the aqueous phase to polymer phase and the concentration of CMC within the hydrogel, respectively. In vivo, porous space maintainers potentially improve oral mucosal healing over a clean/contaminated bone defect created in the rabbit mandible. The tissue response to a porous implant of low-porosity and pore interconnectivity was more favorable than the response to a more porous and interconnected implant. This low-porosity implant may be ideal for temporary space maintenance within craniofacial defects. The described methods may be applicable in a variety of tissue engineering applications and may allow broader application of current tissue engineering approaches that may not be suitable for use in more harsh wound environments.
Footnotes
Acknowledgments
This work was supported by a grant from the Armed Forces Institute of Regenerative Medicine (W81XWH-08-2-0032). The authors would like to thank Ms. Natasja van Dijk and Mr. Vincent M. Cuijpers for their technical expertise and assistance. J.D.K. acknowledges support from the Baylor College of Medicine Medical Scientist Training Program (NIH T32 GM07330), Rice Institute of Biosciences and Bioengineering's Biotechnology Training Grant (NIH T32 GM008362), and a training fellowship from the Keck Center Nanobiology Training Program of the Gulf Coast Consortia (NIH Grant No. 5 T90 DK070121-04). P.P.S. acknowledges support from the Robert and Janice McNair Foundation.
Disclosure Statement
No competing financial interests exist.