
Abstract
Objective:
The development of biological valve prostheses with lifetime native-like performance and optimal host engraftment is an ultimate goal of heart valve tissue engineering. We describe a new concept for autologous graft coating based on a CD133+-stem-cells-plus-fibrin (SC+F) complex processed from bone marrow and peripheral blood of a single patient.
Methods:
CD133+-SC (1 × 106 cells/mL) from human bone marrow and autologous fibrin (20 mg/mL) were administered simultaneously via spray administration using the novel Vivostat Co-Delivery System. During static cultivation, SC+F performance was monitored for 20 days after delivery and compared with controls. For dynamic testing SC+F-composite was sprayed on a decellularized porcine pulmonary valve and transferred to a bioreactor under pulsatile flow conditions for 7 days.
Results:
Static cultivation of SC+F-composite induced significant improvements in stem cell proliferation as compared with controls. For dynamic testing, microscopic analyses on a smooth engineered heart valve surface detected homogenous distribution of stem cells. Ultrasonic analysis revealed native-like valve performance. Applied CD133+ stem cells differentiated into endothelial-like cells positive for CD31 and vascular endothelial growth factor receptor 2 and engrafted the valve. However, occasional delamination was observed.
Conclusion:
SC+F serves as an excellent autologous matrix for intraoperative tissue engineering of valve prostheses promising optimal in vivo integration. However, stability remains an issue.
Introduction
Completely tissue-engineered autologous heart valves maintaining native-like engraftment and long-term hemodynamic performance are not yet within reach. The considerable cost and time involved seem disproportionate with regard to their efficiency and possible clinical indications.8,9 However, encouraging results have been obtained with fibrin as an extracellular matrix with excellent characteristics for angiogenesis, tissue regeneration, and three-dimensional tissue engineering.8–11 Moreover, Syedain et al. demonstrated the adaptation of a growing fibrin-based tubular tissue construct to circumferential strain with an increase in tensile strength achieved by collagen deposition of interstitial cells within the fibrin. 12 Rüger and colleagues reported that mononuclear cells positive for CD133 (CD133+) derived from human bone marrow induced vascular morphogenesis within a three-dimensional avascular fibrin matrix. 13 Further, evidence suggests that pluripotent human CD133+ cells improve revascularization after myocardial injury and endothelialization of vascular grafts.14,15
In our novel concept we are combining the valuable properties of fibrin and human CD133+ stem cells. Both CD133+ cells and fibrin can easily be obtained from a single patient before a surgical heart valve replacement. Using simultaneous spray administration, homografts or xenografts can be coated with a completely autologous CD133+ stem cell-plus-fibrin (SC+F) composite that would definitely enhance biological acceptance. This biocompatible vital bioprosthesis might be able to integrate entirely in vivo, participate in remodeling processes, react to loading conditions, and possibly grow when implanted in children. Full immunological acceptance by the recipient could prevent accelerated degeneration 16 and calcification and minimize the elevated risk of endocarditis, infection, and thrombo-embolism. Further, direct intraoperative processing, that is, autologous biomaterial preparation, graft coating, and incorporation of tissue-engineered heart valves, could reduce the risk of contamination when biologic materials enter or leave the surgical theater. 17 It could increase ease of handling, improve safety, and minimize the cost of the final product. Thus, the aim of this study was to introduce and test a new approach to intraoperative autologous heart valve tissue engineering.
Methods
Cell isolation and labeling
All medical procedures dealing with human products were revised and approved by the independent institutional research ethics committee of the University of Rostock and all patients provided informed consent. For the separation of autologous stem cells in patients, 100 mL of bone marrow was obtained from the sternum before median sternotomy in patients undergoing cardiac surgery. Clotting of the bone marrow sample was prevented by the addition of heparin (5000 U; Ratiopharm GmbH). Then, autologous CD133+ stem cells were isolated using the CliniMACS cell separation unit (CliniMACS; Miltenyi Biotec) in combination with a mouse-anti-human CD133+ antibody (7.5 mL CD133 Reagent; Miltenyi Biotec). Isolated cells were fluorescently labeled with carboxyfluorescein succinimidyl ester (CFSE; CellTrace CFSE cell proliferation kit; Invitrogen) in accordance with the manufacturers protocol, enabling the monitoring of all living cells, including daughter cell generations after cell division. Then, cells were counted using fluorescent microscopy and kept in phosphate-buffered saline (University of Rostock, Rostock, Germany) at pH 7.0 for <10 min at a concentration of 1 × 106 cells/mL before spray administration. For microscopic analysis, the immunofluorescence signal was imaged using a Leica TCS SP2 confocal microscope (Leica).
Processing of autologous fibrin for spray administration
A peripheral blood sample of 120 mL was collected from each patient to process an autologous inactive fibrin at pH 4.0 using the Vivostat Co-Delivery System (Vivostat A/S). Four milliliters of inactive autologous liquid fibrin, 1 mL of an activating solution at pH 10.0, and 1 mL of CD133+ stem cell solution were then loaded into the three separate application channels of the Vivostat Co-Delivery system for simultaneous spray administration (Fig. 1A). This product was defined as the autologous SC+F composite.
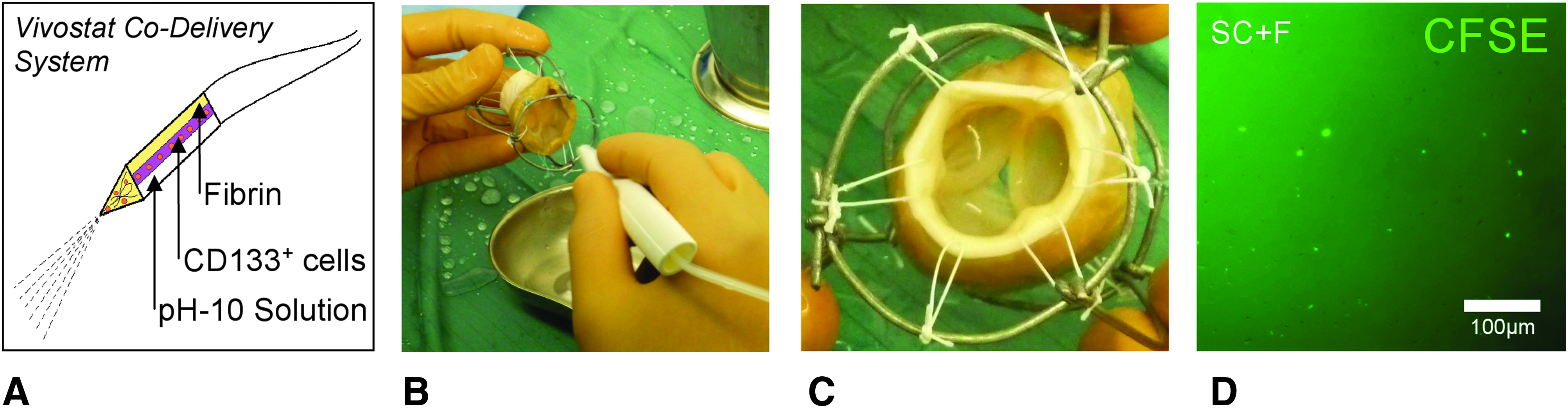
Representative images of autologous CD133+ SC+F heart valve coating.
For static in vitro analysis, 24-well plates were used and for dynamic in vitro analysis the pulmonary valve grafts were spray-coated with a film of SC+F composite.
Static in vitro conditioning
For static in vitro conditioning a 24-well plate was used for direct SC+F spray administration. Each well contained 500 μL of polymerized composite covered with 500 μL of StemSpan H3000 serum-free expansion medium (Stem Span H3000; StemCell Technologies). Six wells without fibrin served as controls for cultivation analysis. In the control wells, 83 μL of CD133+ stem cells/phosphate-buffered saline (concentration 1 × 106 cells/mL) was incubated with 917 μL StemSpan H3000 medium. The medium was supplemented with penicillin (100 IU/mL; Invitrogen), streptomycin (100 μg/mL; Invitrogen), and amphotericin (2.5 μg/mL; Sigma-Aldrich) and changed every day. The cultivation was monitored for 20 days.
Analysis of CD133+ cells throughout static in vitro conditioning
Cells were analyzed using fluorescence microscopy for cell number, cluster formation, colony formation, and cell shape at days 0, 1, 2, 3, 5, 8, 12, 16, and 20. Therefore, intracellular dye CFSE served as a stable indicator for cell identification and survival ensuring the CD133 origin. For the statistical analysis of cell numbers, 10 high-power fields (HPFs, 400-fold magnification) in each well were randomly selected and cell numbers were determined as cells per HPF. At the above described times, the composite was further examined for physical characteristics. For that purpose, the SC+F composite was classified as (1) solid, (2) structural breaks (=clot formation), or (3) complete destruction.
Quantitative analysis of the data is provided for the groups SC+F and control for the experimental group containing fibrin and the control group without fibrin, respectively. Static in vitro testing and all related evaluations were repeated and confirmed three times.
Modification of culture conditions for SC+F stabilization
To achieve greater fibrin stabilization, static SC+F cultivation was performed after the addition of trans-4-aminomethyl-cyclohexane-1-carboxylic acid (t-AMCA) (0.2 and 0.4 mg/mL) to the StemSpan H3000 (StemCell Technologies) medium. Quantitative analysis of the data is provided for the group SC+F+t-AMCA and analytic procedures were performed identically to those described in Analysis of CD133+ cells throughout static in vitro conditioning section.
Modification of culture conditions for in vitro differentiation of stem cells
To verify the angiogenetic differentiation potential of human autologous CD133+ stem cells, the nature of isolated stem cells was tested in vitro before and subsequently after an endothelial colony-forming assay (ECFA) using fluorescence-activated cell sorting (FACS) and immunohistochemical analyses. After the CD133+ cell isolation described above, the cells were directly incubated with fluorescent-labeled antibodies CD133/2-PE (Miltenyi Biotec), vascular endothelial growth factor receptor 2 (VEGFR2)-APC (Miltenyi Biotec), CD45-APC-Cy7 (BD Biosciences), and cell necrosis marker 7-AAD (BD Biosciences). Thereafter, FACS analysis was performed using the LSR II flow cytometer and FACS DIVA software (both BD Biosciences).
Human CD133+ cells that underwent the ECFA were plated in triplicate wells at a cell density of 3000 cells/dish (35 mm in diameter) in MethoCult SF H4236 medium (StemCell Technologies). The medium was supplemented with 33% fetal calf serum (Thermo Scientific), 2 IU/mL heparin (Ratiopharm), and growth factors (PAN Biotech) in a master mix containing fibroblast growth factor (50 ng/mL), interleukin-3 (20 ng/mL), VEGF (50 ng/mL), stem cell factor (SCF) (100 ng/mL), insulin-like growth factor (IGF-1) (50 ng/mL), and epidermal growth factor (EGF) (50 ng/mL) as described by Masuda et al. 18 After 25 days of incubation cells were transferred into Endothelial Growth Medium 2 (Lonza) and cultured on fibronectin-coated coverglasses (Thermo Scientific) in 24-well plates at a density of 150,000 cells/well. After 3 days cells were either analyzed using FACS as described above or fixed with 4% paraformaldehyde for immunohistochemical analysis.
Fixed cells were incubated with goat polyclonal anti-CD31 (Santa Cruz Biotechnology), mouse monoclonal anti-CD133 (Abcam), or rabbit polyclonal anti-VEGFR2 (Abcam) antibody. Instantaneously, cells were stained with anti-goat, anti-mouse or anti-rabbit Alexa Fluor 488–conjugated secondary antibody (Invitrogen) respectively. Thereafter, cells were imaged using the Leica TCS SP2 confocal microscope (Leica).
Dynamic in vitro conditioning
For proof-of-principle applicability and cell engraftment out of SC+F into tissue constructs, a decellularized cryopreserved stentless porcine pulmonary heart valve bioprosthesis (SynerGraft® Heart Valve, Model 700, 29 mm; CryoLife Inc.) was prepared for SC+F coating following the manufacturer's thawing and rinsing instructions.
The valve prosthesis was subsequently sutured to a sterilized metal bracket to stabilize its three-dimensional architecture for the SC+F coating procedure. Then heart valve coating with SC+F was performed in an airbrush-like fashion using the Vivostat Co-Delivery system (Vivostat A/S) to achieve a completely smooth and evenly covered surface (Fig. 1B–D). When coating was done, the prosthesis was sutured to a silicone cylinder to guarantee native-like valve anatomy for further analysis. All transfers for valve processing were arranged at a temperature of 4°C in Dulbecco's modified Eagle's medium (DMEM) standardized culture medium (Invitrogen) supplemented with penicillin (100 IU/mL; Invitrogen), streptomycin (100 μg/mL; Invitrogen), and amphotericin (2.5 μg/mL; Sigma-Aldrich). The bioprosthesis was transferred to a bioreactor provided by the Helmholtz Institute Aachen (Department of Applied Medical Engineering, RWTH Aachen University, Germany) for dynamic conditioning as previously described. 19 The medium, with a total volume of 500 mL, was not changed during dynamic conditioning for sterility reasons. In vivo physical charges of a pulmonary valve were mimicked using a valve opening frequency of 45 per min and a peak pressure exposure to the closed valve leaflets ranging between 22 and 27 mmHg.
Ultrasonic imaging
The valve performance was monitored every day for a follow-up period of 7 days by a transesophageal echocardiographic probe integrated into the bioreactor system. Both M-mode and two-dimensional images as well as movies were obtained. The degree of pulmonary regurgitation and pulmonary valve stenosis was scaled in four categories as grades I (minimal), II (mild), III (moderate), and IV (severe). In addition, the bioprosthesis and circulating medium were analyzed for structural changes and floating particles.
End-point analysis of dynamic, tissue-engineered valves conditioned in vitro
After 7 days the entire medium was centrifuged at 530 g for 10 min and the supernatant was withdrawn. The pellet was transferred to a culture flask containing DMEM and supplements (see above) and examined for CFSE-labeled cells and clots using fluorescence microcopy. The bioprosthesis was longitudinally divided into three parts, each of them containing one leaflet. The parts were temporarily kept in DMEM and checked for adherent CFSE-labeled cells using fluorescence microscopy at 400-fold magnification. For further analysis valve pieces were preserved in either liquid nitrogen or 4% formalin. In frozen transverse tissue sections (thickness: 5 μm), 4′-6-diamidino-2-phenylindole (DAPI)-stained, CFSE-labeled cells were analyzed for presence, localization of adherence, cluster or colony formation, and cell shape using fluorescence microscopy. To detect CD133+ cell differentiation, immunohistochemical stainings with either CD31 antibody (goat polyclonal IgG; Santa Cruz Biotechnology) followed by donkey anti-goat Alexa-Fluor 568–conjugated secondary antibody (Invitrogen) or VEGFR2 antibody (rabbit polyclonal IgG; Abcam) followed by goat anti-rabbit Alexa-Fluor 568–conjugated secondary antibody (Invitrogen) were performed. The sections were counterstained with TOPRO 3 and analyzed using confocal microscopy at 630-fold magnification.
CD133+ cells that did not undergo dynamic in vitro cultivation were observed as controls under static culture conditions.
All dynamic in vitro conditioning and analyses were performed in triplicate.
Statistical analysis
All data were stored and analyzed using the SPSS statistical package 17.0 (SPSS Inc.). Descriptive statistics were computed for continuous and categorical variables. The statistics computed included mean and standard deviations of continuous variables, frequencies, and relative frequencies of categorical factors. The results for continuous variables are presented as mean ± standard deviation. Because measurements were done several times on the same cell sample (well) within three independent groups, we applied the GLM Repeated Measures procedure for statistical analysis of the data to test null hypotheses about the effects of both the between-subject factor (group) and the within-subject factor (time).
With regard to endothelial differentiation, parameters during ECFA differences between the two time points days 0 and 28 were investigated using the paired t-test or Wilcoxon's rank test for paired data, as appropriate. Test selection was based on an evaluation of variables of differences for normal distribution using the Shapiro-Wilk test.
All p-values were obtained using two-sided statistical tests and values of p < 0.05 were considered to be statistically significant.
Results
SC+F application and fibrin degradation
The SC+F spray coating of surfaces turned out to be easy with excellent composite adhesion and homogenous cell distribution (Figs. 1D and 2). Immediately after application, fluorescence microscopy revealed air bubbles in the upper layer of the autologous CD133+ SC+F composite, which were no longer identifiable at any later point in time.

CD133+ stem cell proliferation in SC+F composites during 20 days of static cultivation. Representative images from fluorescence microscopy. Cells from human bone marrow are stained with CFSE. Magnification ×400. Images show equally homogenous distribution of stem cells within SC+F
During static in vitro testing, the SC+F composite remained physically solid until day 5. Then, continuous degradation started and numerous structural breaks were detected (mean destruction grade 2.25 ± 0.500 at day 7). By day 9, destruction of the SC+F composite was complete, exposing a gel-like solution with small clots of higher cell density (destruction grade 3.00 ± 0.000 on day 9).
After supplementation with t-AMCA (0.2 mg/mL) the autologous CD133+ SC+F composite was continuously solid until day 16 when the first structural breaks were detected (mean destruction grade 1.50 ± 0.577 on day 16). At the end of the follow-up period, the SC+F+t-AMCA composite destruction was nearly complete with a mean destruction grade 2.75 ± 0.500 on day 20. The extent of fibrin degradation is shown in Figure 3.

Quantitative analysis of fibrin degradation in CD133+ SC+F composites during 20 days of static cultivation. Square-marked line shows the degradation of unmodified SC+F. Triangle-marked line shows fibrin degradation after addition of 0.02 mg/mL tranexamic acid (SC+F+t-AMCA). Structural SC+F stability was assessed using light microscopy in 10 high-power fields (magnification ×100) of four representative wells per group. Classification for stability graduation was as follows: (grade 1) stable matrix, (grade 2) structural breaks, (grade 3) destroyed matrix. Values are given as mean ± standard deviation of mean. The data show improved SC+F physical stability with t-AMCA under static cell culture conditions. t-AMCA, trans-4-aminomethyl-cyclohexane-1-carboxylic acid.
Enhanced stem cell survival and proliferation during static in vitro cultivation
In vitro static cultivation revealed CD133+ stem cell survival within the autologous SC+F composite as detected by CFSE fluorescence throughout the entire follow-up period of 20 days. Continuous CD133+ cell proliferation inside the solid composite started on day 1 and was more prominent beginning from day 5 when compared with controls. Cell numbers on day 8 in the SC+F composite were 3.2 times higher compared with days 0 and 2.8 times higher compared with control wells (SC+F day 8: 16.7 ± 9.58 cells/HPF vs. SC+F day 0: 5.18 ± 2.55 cells/HPF and vs. control day 8: 6.25 ± 3.48 cells/HPF; Fig. 4). Moreover, on day 20 in SC+F the cell number rose 5-fold compared with day 0 and 6.5-fold compared with the control wells (SC+F day 20: 19.5 ± 24.1 cells/HPF vs. SC+F day 0: 5.18 ± 2.55 cells/HPF and vs. control day 20: 2.98 ± 2.03 cells/HPF; Fig. 4).
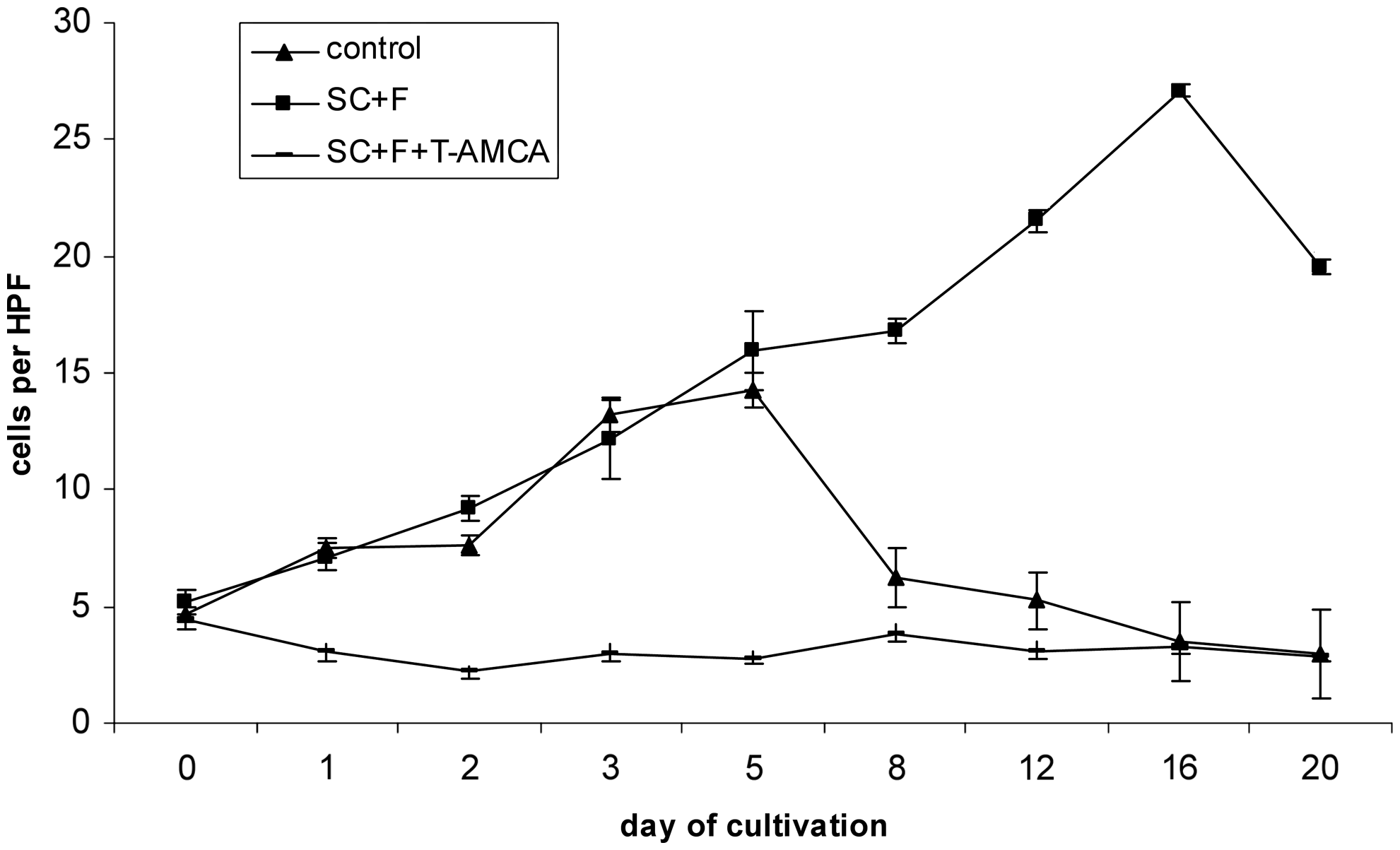
Quantitative analysis of CD133+ cell proliferation in SC+F composites during 20 days of static cultivation. Square-marked line shows unmodified SC+F in cultivation medium. Triangle-marked line shows cell proliferation in the medium alone (control). Stripe-marked line shows cell proliferation after the addition of tranexamic acid (t-AMCA, 0.2 mg/mL) to SC+F in the cell culture medium. The number of cells was assessed using fluorescence microscopy in 10 randomly analyzed high-power fields (magnification ×100) of four representative wells per group. Values are given as mean ± standard error of mean for days 0, 1, 2, 3, 5, 8, 12, 16, and 20 of observation. The data show continuous cell proliferation of CD133+ cells in the fibrin composite under static cell culture conditions. Post hoc tests after an overall F test revealed obviously different curves for SC+F and SC+F+t-AMCA for the whole period. The curves for control and SC+F+t-AMCA differed only up to and including day 5 and the curves for control and SC+F only from day 5 onward.
Within the SC+F composite, the formation of cell clusters and colonies was first observed on days 5 and 8, respectively. On day 16, in SC+F wells, 37% of observed fields were found to be positive for cell colony formation. This was clearly different from the controls and SC+F+t-AMCA, where no cell clusters or cell colonies were detected. After supplementation with t-AMCA, no cell proliferation in SC+F+t-AMCA was found, so that the number of cells in the composite remained lower compared with SC+F alone throughout the entire observation period (Fig. 4).
Statistical analysis of the data showed that the hypothesis that for the whole data set of the three groups the cell number values at all nine time points are equal was rejected (GLM Repeated Measures Analysis, F test: p = 0.005). Further, the time–group interaction was significant as well (p < 0.001). This means that the hypothesis that the deviations from equality over the nine time points are the same for the three groups was also rejected. Consequently, there was an independent influence of the group on the course over time.
Additionally, we compared one level of time to the subsequent level, and tested two hypotheses: first, averaged over the three groups, the mean of the specified contrast is 0, and second, the means of the specified contrast are the same for the three groups. For the first test, we found a significant increase only for the first contrast of the difference between days 0 and 1 (p = 0.031). Hypotheses that the means of a specified contrast were the same for the three groups were rejected for the differences days 0–1 (p = 0.048), days 1–2 (p = 0.041), days 5–8 (p = 0.002), and days 8–12 (p < 0.001). Illustrating the first difference (days 0–1), we found an increase both for the control group and SC+F and a decrease for SC+F+t-AMCA. The same situation was reflected by the difference for days 1–2. On the other hand, between days 5 and 8 there was an extreme decrease for the control group, but for the other two groups there were increases. Finally, between days 8 and 12 there were small decreases for control and SC+F+t-AMCA, but a considerable increase for SC+F (Fig. 4).
Additionally, comparisons among the three groups were carried out. As the F test offered significant differences between the three groups (p < 0.001), we performed post hoc tests to evaluate differences among specific means of two groups at a time. It was no surprise that all three post hoc tests gave significant results (p < 0.001). Although the curves of SC+F and SC+F+t-AMCA were obviously different for the whole period, the curves of the control group and SC+F+t-AMCA differed only up to and including day 5, and the curves of the control group and SC+F differed from day 5.
Microscopic cell shape analyses revealed no differences in phenotypic CD133+ cell structure among all groups. Most of the cells were round, with a few cells having a spindle shape or branched morphology as of day 2 in the SC+F group. These cells appeared earlier and at a higher frequency than in SC+F+t-AMCA (semiquantitative assessment, data not shown).
Endothelial precursor cell nature of human CD133+ stem cells
A FACS analysis before ECFA showed that 93.7% ± 2.03% of isolated viable human cells were positive for the CD133 stem cell surface marker. In addition, FACS proved that the CD133+ stem cells were negative for endothelial cell marker VEGFR2. After 28 days of ECFA conditioning, FACS and immunohistochemistry revealed significant differences in cell shape and surface marker expression. Cells had lost their CD133 positivity (day 0: 93.7% ± 2.03% vs. day 28: 0.620% ± 0.333%; p < 0.001; paired t-test; Fig. 5A1 and A2) and had significantly generated the endothelial surface marker VEGFR2 (day 0: 1.94% ± 0.920% vs. day 28: 11.8% ± 0.700%, p < 0.001; paired t-test). Confocal imaging revealed the spindle-shaped morphology of CD31+ and VEGFR2+ adherent cells (Fig. 5B1, B2, and C). With regard to leukocyte surface marker CD45, FACS uncovered no difference in the number of CD45+ cells before and after ECFA (day 0: 98.7% ± 1.13% vs. day 28: 98.7% ± 0.145%; p = 1.000; paired t-test). However, FACS analyses revealed a transition from a CD45low population before ECFA to a CD45low and a CD45high population after ECFA (Fig. 5D). Further, FACS after ECFA revealed that VEGFR2+ cells were found exclusively inside the CD45high population and could even be enriched within this population by further sorting for cell size and complexity. Accordingly, CD31+ cells after ECFA were more numerous within the CD45high population than in CD45low population (data not shown). As a result, freshly isolated human bone marrow CD133+VEGFR2− cells partially adopted endothelial-like cell morphology, adhesion, and surface marker expression after stimulation via an ECFA.

Endothelial differentiation potential of CD133+ stem cells during static in vitro ECFA. Images from confocal microscopy after ECFA show spindle-shaped endothelial-like cells negative for CD133
Coating of decellularized heart valves and dynamic in vitro testing
With simple handling and processing the spray procedure was also suitable for precise application of SC+F on three-dimensional tissue engineering constructs such as decellularized heart valves (Fig. 1). Immediately after SC+F application, no valvular leaflet adherence or other structural/functional impairment of the coated valve was noted in direct visual observation during echocardiography. During the follow-up observation in the bioreactor, echocardiography revealed native-like performance of the SC+F tissue-engineered pulmonary valve up to day 3. The solid but seemingly elastic composite had no negative effects on the leaflet movements even though all leaflets were coated with a 1 mm layer of SC+F on both sides. Minimal nonprogressive pulmonary valve reflux (below regurgitation grade I) was observed in one engineered heart valve during the entire experiment.
From day 4 of dynamic in vitro cultivation, echocardiography first revealed floating composite clots at the inner surface of the valve and at the leaflets (Fig. 6A). After the termination of bioreactor testing, microscopic analysis of the medium showed SC+F clots of different size as well as numerous single CFSE-labeled cells, which were observed via fluorescence microcopy (Fig. 6B).
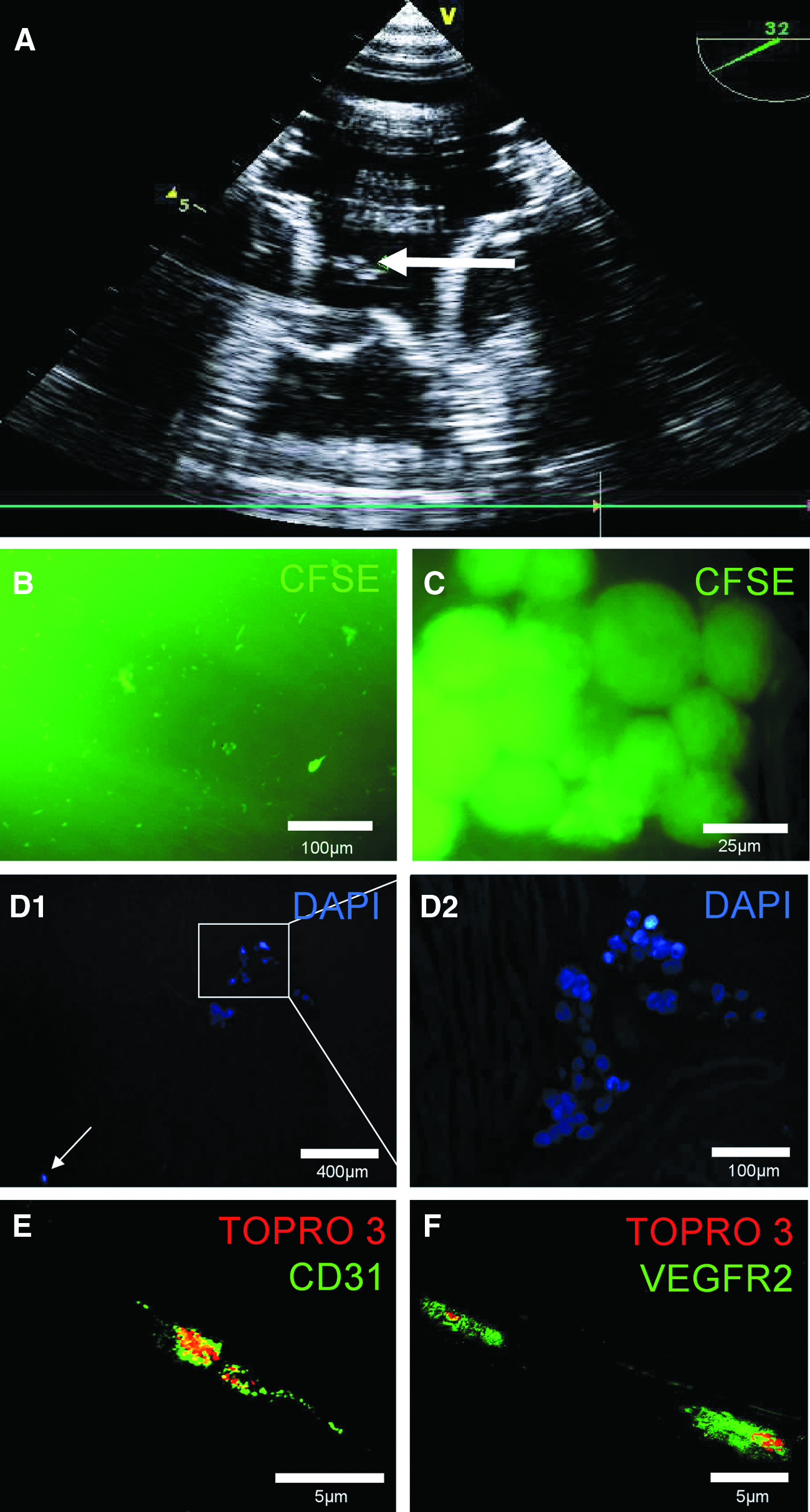
Monitoring SC+F-engineered heart valves during 7 days of dynamic in vitro cultivation.
Engraftment of CD133+ cells into decellularized heart valves in vitro
After explantation of the valve prosthesis from the bioreactor, fluorescence microscopy showed adherent CFSE-labeled cells, cell clusters engrafted into the outer layers of valve matrix, and single cell attachment at the inner surface of the valve (Fig. 6C, D1, and D2). Moreover, in uninterrupted dynamic in vitro conditioning CD133+ stem cells proved their capacity for differentiation into endothelial-like cells when spindle-shaped cells positive for endothelial cell lineage markers CD31 and VEGFR2 were found attached and incorporated at the inner layer of the valve (Fig. 6E and F).
Discussion
The results of our in vitro study present a possible concept for intraoperative autologous tissue engineering of heart valve bioprostheses using CD133+ stem cells embedded in a fibrin matrix.
Our findings apparently demonstrate a homogenous CD133+ stem cell distribution after sprayed cell seeding within the SC+F group that was comparable to controls. However, the increased proliferation and survival of CD133+ stem cells within the SC+F compared with controls remain a subject for debate. We used CFSE fluorescence as a convenient indicator for survival and CD133+ origin in dividing cells, knowing that CFSE itself might impair cellular activity and viability. 20 Although cell death under control conditions could not be prevented, static in vitro cultivation of SC+F revealed CD133+ stem cell survival throughout the entire follow-up period. Since a matrix-free control was used, the experiment lacks an immaculate control. Hence, it cannot be excluded that certain matrix-dependent fibrin-independent properties are responsible. Cells were cultivated three-dimensionally with extracellular stiffness within SC+F and cell-to-cell interaction; oxygen as well as nutrient diffusion capacities are most likely different among the groups compared. 21 However, the results also document that CD133+ stem cells undergoing a two-dimensional matrix-free ECFA do survive and differentiate. Their proliferation rate was high (data not shown). For ECFA cultivation serum and growth factors were added to the medium. SC+F generated by the Vivostat Co-Delivery device contains a certain amount of serum proteins and growth factors secreted by platelets whose concentration is highly dependent on the individual patient. Thus, our results confirm the processed autologous fibrin as a possible matrix for the survival and development of CD133+ cells compared with a noncomposite control. The role of fibrin itself, its biological properties, growth factors, and serum proteins must be further identified.
In our novel concept, the firm and flexible adhesion of fibrin on mobile three-dimensional tissue constructs was highly appreciated. By adding CFSE-labeled CD133+ stem cells to the fibrin we were able to prove successful SC+F coverage of a complex pulmonary heart valve bioprosthesis. However, incomplete coverage cannot be excluded to date. The sprayed cell seeding approach definitely requires compliance with technical rules, a certain learning curve must be expected, and embolus formation by a preformed, detachable fibrin clot must be considered. Concerning the latter, ultrasonic imaging did not reveal any clot detachment or embolus formation during the first 3 days of dynamic conditioning. SC+F-coated bioprostheses performed like original human valves without any valvular leaflet adherence or other structural impairment. However, direct cell coverage of the graft's inner surface was limited owing to fibrin decomposition and subsequent SC+F detachment starting around day 4 during dynamic conditioning. Further bioreactor testing is required to create more stable SC+F-coated bioprostheses and to analyze the extent of shear stress tolerance before SC+F failure.
The endothelial border of cardiovascular grafts is crucial to its host acceptance and engraftment. 22 We chose autologous CD133+ stem cells from human bone marrow since this cell type constitutes a source of endothelial progenitors which possess high plasticity and the ability to differentiate into mature, functional endothelial cells especially in ischemic heart disease. 23 Fibrin was recently described as a perfect matrix for cell development in cardiovascular tissue engineering in vitro by Jockenhoevel et al. 24 and in vivo by Grant et al.8,25 Numerous studies document the pivotal role of fibrin for the so-called endothelial lining, sprouting, and tubule formation in angiogenesis in vitro.26–28 Syedain et al. even demonstrated strength adaptation of a growing fibrin-based tubular tissue construct to circumferential strain. 12 To the best of our knowledge, our results for the first time present endothelial-like cells that partially engrafted the flow side of a cardiovascular graft after a single simultaneous spray application of a patient's CD133+ endothelial precursor cells and fibrin. Although endothelial-like cell coverage of the inner surface was limited, by optimizing SC+F stability and cell attachment to the graft our novel approach at least in part could make a positive contribution to graft integration, host recellularization, and endothelialization in vivo.15,29 Moreover, intraoperatively processed autologous SC+F tissue-engineered heart valves might have the potential to grow, to react to loading conditions, and to prevent well-known complications after conventional heart valve replacement.2–5 Finally, it probably reduces the risk of contamination and increases the ease of handling compared with other tissue engineering approaches. 17
The nature of the human CD133+ cell is still a subject for debate. Originally, it was classified as a marker for primitive hematopoietic and neural stem cells. On the one hand, studies established CD133 as a marker for human allogenic transplantation of hematopoietic stem cells. On the other hand, recent reports presented that CD133 is also expressed by cancer stem cells. 30 Still, other advanced studies show that CD133+ cells from human bone marrow serve as an adequate source of early endothelial progenitor cells. 31 Our results confirmed the endothelial precursor cell nature of applied CD133+ stem cells. Although losing CD133 surface marker expression under in vitro static ECFA cultivation, cells partially developed VEGFR2 surface marker expression in adherent spindle-shaped endothelial-like cells. Cell surface marker CD31, frequently used for quantitative capillary density assessment, 32 was also found to be positive after ECFA. Despite the well-known lack of CD31 expression specificity, CD31 serves as an adequate marker in endothelial cell identification when cell shape, behavior, and other more specific markers are reviewed. With regard to the CD45 expression of applied cells after ECFA, both VEGFR2 and CD31 expressions were more pronounced in the more differentiated CD45high population than in the CD45low population (data not shown). However, the role of CD31 expression as well as its regulation in endothelial differentiation of endothelial precursors must be further identified. Accordingly, we also found spindle-shaped endothelial-like cells partially positive for VEGFR2 and CD31 adhering to the flow side of the grafts that were tested in a bioreactor. In this case, shear stress during dynamic in vitro conditioning might have activated intrinsic vasculogenic activities, promoting endothelial-like cell formation and valve cell engraftment. 33
The partial degradation of fibrin in the SC+F beginning around days 4–5 in both static and dynamic in vitro settings was in accordance with the data of Buchta et al. 34 and points out the challenge of this new approach in the search for in vivo advances. Cell proliferation within SC+F rose and colony formation became apparent with the increasing level of fibrin destruction. Neither phenomenon was observed when fibrin degradation had been inhibited by t-AMCA, which made us aware of the crucial role of fibrin decomposition. Elevated cell proliferation in SC+F could be caused by the increase in cell-to-cell contacts offered during fibrin matrix degradation. Hence, the risks and or benefits of strengthening mechanisms for the intravascular application of SC+F remain unclear. The outcome after cardiac surgery is heavily influenced by the biological balance of platelet/fibrin clot formation and degradation with embolization. 35 When advancing to in vivo trials, it may be possible to stabilize SC+F using host recellularization or the initiation of coagulation. However, we recommend that testing our model in vivo should be restricted to the implantation of SC+F-coated grafts into the venous system and pulmonary valve position in preclinical animal experiment settings. Within these advances the progress of SC+F must be continuously monitored.
The inhibition of fibrin destruction by tranexamic acid led to reduced cell proliferation within the composite even when degradation of the SC+F scaffold began on day 16 of in vitro static conditioning. Apart from reduced cell-to-cell contacts, a possible slight cytotoxicity of t-AMCA may have impaired cell proliferation.36,37 However, the level of applied t-AMCA concentrations for sufficient SC+F stabilization was between the concentrations previously described for systemic 38 and local antifibrinolysis in vivo. 39 With regard to possible in vivo trials using the approach described in this article, antifibrinolytic agents such as tranexamic acid could also impair graft recellularization and in vivo stabilization of the SC+F coating. Endothelial sprouting in fibrin is most likely fibrinolysis dependent and the reduction of fibrinolysis could cause thrombus and embolus formation in vivo. 40 Hence, in our initial application of our new approach, bioreactor examinations mimicking flow conditions at pulmonary valve site were performed exclusively for autologous SC+F-coated pulmonary heart valves without the addition of any antifibrinolytic agents. However, there are numerous conceivable improvements for the introduced approach. These include chemical stabilization of SC+F using tranexamic acid, aprotinin, or plasminogen-activator inhibitor 1. The impacts of cell density within SC+F, a multiple layer application technique, and platelet concentration need to be investigated. Modulation of the thrombin/factor XIII concentration ratio could also be useful.36,37 Further, other mature cell types such as endothelial cells, smooth muscle cells, pericytes, and fibroblasts are probably of primary importance in graft integration and host recellularization in vivo.26–28 However, their autologous isolation might be difficult and technologically limited. Instead, other adult angiogenetic stem cell types could be applied for sufficient graft endothelialization. 41
In conclusion, the feasibility of the intraoperative autologous SC+F-based heart valve tissue engineering concept is very promising with excellent results for spray applicability, composite surface structure, graft coating, and native-like valve performance. For the first time, our results document homogenous stem cell distribution by a single simultaneous spray application of a patient's CD133+ endothelial precursor cells and fibrin on a cardiovascular tissue construct. Moreover, CD133+ stem cell proliferation and differentiation into endothelial-like cells that engrafted the heart valve bioprosthesis were identified under in vitro static and dynamic conditioning, respectively. When aiming for in vivo advances, our approach as described in this article could be beneficial for graft integration, acceptance, recellularization, growth, and charge adaptation, preventing well-known complications after conventional heart valve replacement. In addition, it probably reduces the risk of contamination compared with other tissue engineering concepts. However, SC+F stability remains an issue. The degradation of SC+F through the dissociation of fibrin with a subsequent decrease in stability and cell coverage of the graft under shear stress must be addressed. Whether endovascular application of SC+F is protective or harmful must be tested in further experimental in vivo studies.
Footnotes
Acknowledgments
We thank Ms. Margit Fritsche for excellent technical assistance. We are grateful to Probicon GmbH for proofreading the article. This work was supported by the German Ministry of Education (BMBF; Germany, Berlin; funding indicator 0312138 A), the Ministry of Economy (Mecklenburg-West Pommerania, Schwerin; funding indicator RTC V220-630-08-TFMV-F/S-035), and the German Research Foundation (DFG; Germany, Berlin; funding indicator SFB TR37, TPA4).
Disclosure Statement
No competing financial interests exist.