
Abstract
The body contains a number of organs characterized by a tubular shape. In this study, we explored several methodologies for the construction of collagenous tubular scaffolds and films with defined (ultra)structure, length, diameter, orientation, and molecular composition. Standardization of molding, casting, freezing, and lyophilizing techniques using inexpensive materials and methods resulted in controllable fabrication of a wide variety of tubular and tissue-specific tubular scaffolds and films. Analysis included immunohistochemical and (ultra)structural examination. Handling and suturability were found adequate for tissue engineering applications.
Introduction
Multiple groups have applied porous collagenous scaffolds in the engineering of tissues.10–14 In general, the regeneration of tissues depends not only on cells, but also on a correct 3D architecture of the applied scaffold. 15 For instance, the pore size may influence cellular activity.16–18 Kroehne et al. demonstrated the potential of using collagen matrices with oriented pore structure for muscle cell differentiation. 13 The same may be true for tubular scaffolds. We previously showed that the 3D architecture of tendon, lung, and skin can be mimicked using flat type I collagen scaffolds. 15 Flat scaffolds may be sutured into tubes using a variety of techniques, 10 though the preparation of pretubularized collagen scaffolds may facilitate the surgical procedure. 19 Therefore, in this study, we extended our methodology by the preparation and characterization of tubular scaffolds.
Tubular scaffolding has been widely reported in literature for various applications.20–27 A number of construction methods use decellularization of tubular organs/tissues, 28 but this inevitably leads to batch-to-batch variations, whereas the precise composition and possible contaminants of the graft are generally unknown. In this study, we introduce new methods for graft construction from scratch. One major advantage of this bottom-up approach is the tenability of a number of parameters, thus facilitating tailor-made construction. In addition, the use of highly purified components will allow studies to the effect of a single component within the construct. In this study, we used highly purified type I collagen fibrils as the basic material. Collagen is the most abundant protein in the ECM of organs, and is the prime scaffolding material of the body, providing structural integrity and strength.29,30 Isolated collagen fibrils are highly biocompatible and have been amply used for tissue engineering purposes, including blood vessel,22,23,31 bladder, 32 urethra, 33 and cartilage. 34
Generally, tubular scaffolding can be achieved by introducing molding and casting techniques around a mandrel.35,36 Optimally, molding and casting techniques must allow the construction of tubular scaffolds corresponding to the organ under study, and it should allow in vivo implantation demands. In this respect the choice of the scaffold's diameter, length, lumen, internal 3D structure, and added biomolecules is essential for a tailor-made approach. In this study, we developed various tubular molding and casting methods, and characterized the resulting (composite) collagenous scaffolds/films. Analyses included macroscopic examination, scanning electron microscopy (SEM), immunohistology, and handling with respect to suturability.
Materials and Methods
Unless stated otherwise, all chemicals were purchased from Merck Chemicals.
Type I collagen fibrils
Insoluble type I collagen fibrils were purified from pulverized bovine Achilles tendon. 37 The purification consisted of biochemical washings with diluted acetic acid, aqueous NaCl solutions, urea, acetone, and demineralized water.
Elastin fibers
Elastin fibers were purified from pulverized equine ligamentum nuchae. 38 The purification consisted of several washings steps with 1 M NaCl, ethanol, chloroform/methanol, and ether, and 8% (w/v) CNBr in formic acid (under gaseous nitrogen conditions), demineralized water, urea, 2-mercaptoethanol, and a trypsin digestion.
Collagen suspension
A 0.8% (w/v) type I collagen suspension in 0.25 M acetic acid was prepared by swelling at 4°C for 16 h. The collagen suspension was homogenized with a Potter-Elvehjem device (Louwers Glass and Ceramic Technologies) with an intervening space of 0.35 mm on ice using ∼10 strokes. The suspension was deaerated by centrifugation at 250 g for 15 min.
Polylactide-caprolactone
Synthetic polymer was synthesized by adding 90.0 g of L-lactide (Beuringer Ingelheim) and 10.0 g of e-caprolactone (Sigma-Aldrich) inside a glove box to a dried (180°C) 150 mL cylindrical stainless steel reactor equipped with an argon inlet. The reactor was sealed and brought outside the glove box to an oven set to 160°C. After 30 min, 0.3 mL tinoctanoate was added under Argon flow to the molten monomer. The reactor was then rotated in the oven at 130°C for an additional 24 h. The resulting white block of polymer was stored dry until further use. Polylactide
Tubular scaffolds
Tubular collagen scaffolds
The homogenized and deaerated collagen suspension was casted in a polystyrene mold with an inner diameter of 10, 13, or 22 mm after which a stainless steel mandrel with defined diameter was inserted (Table 1). A spacer was placed to keep the mandrel in place and the construct was frozen at either −20°C (freezer), −80°C (dry ice/ethanol), or −196°C (liquid nitrogen), and subsequently lyophilized (Zirbus) (Table 1) resulting into tubular collagen scaffolds (Fig. 1). From each diameter and for every freezing temperature, pores in the scaffolds were measured using scanning electron micrographs.
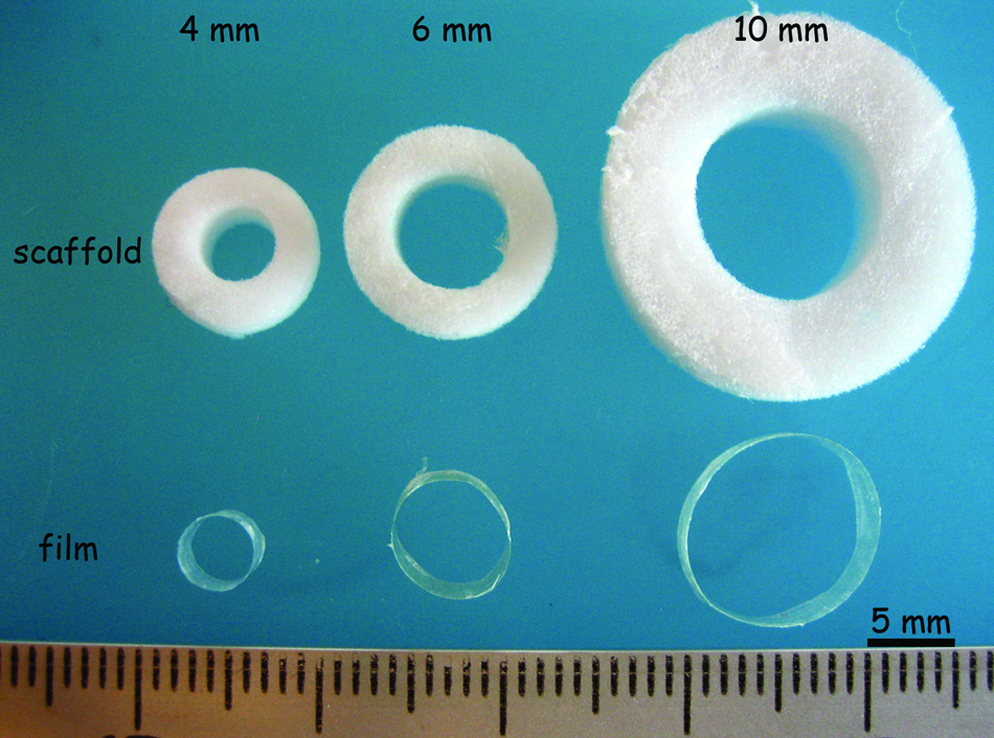
Macroscopic view of tubular collagenous scaffolds (−20°C freezing) and films (air-drying) with inner diameters of 4, 6, and 10 mm. Bar represents 5 mm. Color images available online at
Tubular films were prepared from −20°C tubular scaffolds only.
To obtain tubular scaffolds with inner circumferential orientation type I collagen fibrils were twirled upon the mandrel after inducing aggregation, and before freezing and freeze-drying.
To obtain scaffolds with inner radial orientation an inward out freezing gradient was established by placing liquid nitrogen (−196°C) inside a hollow 4-mm mandrel.
A two-segmented stainless steel mold was used to obtain long tubular scaffolds.
Long tubular collagen scaffolds
Typically, the prepared basic tubular scaffolds were up to 5 cm in length. Longer collagen scaffolds (11–12 cm) were made by preparing scaffolds in a custom-made two-segmented mold with an inner diameter of 14 mm (Fig. 2). One end of the mold was closed by a polystyrene cap with a centered hole, and a stainless steel mandrel (Ø 6 mm) was placed through the cap. The mold was filled with a homogenized and deaerated 0.8% (w/v) collagen suspension in 0.25 M acetic acid, after which the other end of the mold was closed, thus fixing the mandrel. The complete system was frozen at −20°C for 16 h. Subsequently, caps were removed and the frozen mold was lyophilized. Next, the two mold segments and mandrel were removed, resulting in a long tubular scaffold.

Construction of long tubular scaffolds (∼10 cm) using a two-segmented stainless steel mold, showing a macroscopical view without
Tubular collagen scaffold with internal radial orientation
A hollow mandrel (outer diameter Ø 4 mm, brass) was inserted in a tubular polystyrene mold (diameter 27 mm) with a centered hole. The hollow mandrel was closed at one end with a brass plug. The 0.8% (w/v) collagen suspension was placed in the mold and the hollow mandrel was filled with liquid nitrogen. This caused the suspension to freeze from the lumen outward (inward out). After 2 h (to ensure complete freezing), the construct was lyophilized.
Tubular collagen scaffold with internal circumferential orientation
A homogenized collagen suspension was made as described, using 12.5 mM acetic acid instead of 0.25 M to enable collagen fibril aggregation. A polystyrene mold was filled for one quarter with 0.1 M phosphate buffer (pH 7.4). The collagen suspension was put on top filling the tube for three quarters. Another quarter of 0.1 M phosphate buffer (pH 7.4) was put on top of the collagen suspension to achieve slow homogenous aggregation. Next, a stainless steel mandrel (Ø 4 mm) was placed and the aggregating collagen fibrils were manually twirled around it. Then, the mandrel with the circumferentially oriented collagen fibrils was removed from the mold, frozen at −20°C, and lyophilized.
Tubular films
Tubular collagen films
Films were produced originating from scaffolds. It was not possible to make tubular film from collagen suspensions directly, since collagen suspensions were not viscous enough to remain fully attached to the mandrel. Tubular collagen scaffolds prepared at −20°C were wetted in demineralized water around poly-ether-ether-ketone (PEEK) mandrels (diameter 4, 6, and 10 mm). For this, tubular scaffolds were fixed at the PEEK mandrel's ends with suturing thread (3-0 Vicryl; Ethicon, Johnson & Johnson) and deaerated in demineralized water under vacuum for 5 min in a desiccator. The fixed and wetted tubular scaffolds were dried standing around their mandrels at 21°C for 16 h. PEEK was used for its high inertness, so films could be removed from the mandrel after drying (see Results and Discussion sections).
Composite tubular scaffolds/films
Tubular collagen scaffold with abluminal polymer film
For improving tubular collagen scaffold's strength, an abluminal synthetic polymer film was applied. PLCL was homogeneously dissolved in chloroform to a final concentration of 20% (w/v). Tubular collagen scaffolds (Ø 4 mm, −20°C) with mandrel (Ø 4 mm) were dipped into the polymer solution for 3 s and the scaffold was left standing at 21°C to dry on the stainless steel mandrel. Burst pressure and ultimate tensile strength (UTS) were measured as described previously. 39 Briefly, 1.5–2 cm tubular scaffolds (with abluminal film, n = 6) were placed around a hollow mandrel. After clamping at both ends, ∼0.01% (w/v) bromephenol blue in water (Biorad) was pumped into the scaffold's lumen. Burst pressures were measured in mm Hg by a pressure transducer connected to a computer. For UTS measurements, tubular scaffolds were cut open longitudinally and fixed between polystyrene clamps. Specimen strips (n = 6) were pulled until rupture, reflecting the UTS.
Tubular collagen film with elastin fibers and luminal type IV collagen
A type I collagen fibril/elastin fiber 1.6% (w/v) suspension (collagen:elastin = 1:1) in 0.25 M acetic acid was prepared similarly to a basic collagen suspension. The suspension was casted in a tubular polystyrene mold with mandrel (PEEK, Ø 4 mm), frozen (−20°C), and freeze-dried. A film was made from the scaffold by air-drying the wetted scaffold at 21°C (as described in the Materials and Methods section “tubular collagen film”), followed by removal from the mandrel (pieces of up to 1 cm). A 0.1% (w/v) type IV collagen (Fluka) suspension in 0.25 M acetic acid was luminally coated; the tubular collagen/elastin film was pinned on a 25G needle and vertically fixed on styrofoam. The lumen of the tubular film was filled with the type IV collagen suspension, which was collected at the bottom. This procedure was repeated at least four times, followed by air drying at 21°C.
Scaffold characterization
Scanning electron microscopy
SEM was used to analyze the morphology and structure of the tubular scaffolds/films. Samples were fixed on a stub with double-sided carbon tape, and sputtered with an ultrathin gold layer in a Polaron E5100 Coating System. Examination was done in a JEOL SEM 6310 apparatus (JEOL Ltd.) at an accelerating voltage of 15 kV.
Suturability
Basic tubular collagen scaffolds (4 mm, −20°C) were crosslinked and tested for suturability. Tubular collagen scaffolds were crosslinked by means of 1-ethyl-3-dimethyl aminopropyl carbodiimide (EDC; Fluka) and N-hydroxysuccinimide (NHS; Fluka). Briefly, scaffolds with mandrels were preincubated in 50 mM morpholinoethane sulfonic acid (USB Corporation) (pH 5.0) containing 40% (v/v) ethanol (0.4 mg collagen/mL) for 5 min under vacuum. Next, wetted scaffolds were crosslinked in 33 mM EDC and 6 mM NHS in 50 mM morpholinoethane sulfonic acid buffer (pH 5.0) containing 40% (v/v) ethanol for 4 h. The mandrels were removed after 2 h of crosslinking. Scaffolds were washed with 0.1 M Na2HPO4, 1 and 2 M of NaCl, and demineralized water. 37 Scaffolds were then sutured (end-to-end) by four point sutures to a porcine femoral artery and between the urethra and the bladder of a rabbit. General suturability, or “surgeon-friendliness,” was evaluated by an experienced surgeon and by evaluation of leakage at the site of sutures/anastomosis using flushing of the tubular scaffolds with buffered saline. Suture retention was measured using the same mechanical setup for testing UTS. 39 Square knotted 5-0 Vicryl sutures (Ethicon) were placed ∼2 mm at one end of crosslinked collagen tubular scaffolds (∼2 cm in length, n = 6) leaving 5 cm extra suture thread. The other (free) end of the tubular scaffold was clamped and the suture thread was fixed. The thread was pulled (2.9 mm/min) until rupture through the scaffold.
Immunohistochemistry
Immunofluorescence microscopy was used to study the presence and location of the different components in the composite collagen film (containing type I collagen, elastin fibers, and type IV collagen) as described. 40 In brief, samples were snap-frozen in liquid-nitrogen-cooled isopentane. Rehydrated cryosections (5 μm) were blocked with 1% (w/v) bovine serum albumin (USB Corporation) in phosphate-buffered saline (pH 7.4) and incubated with polyclonal rabbit antibovine type I collagen (1:100; Chemicon), polyclonal goat anti-human type IV collagen (1:50; Southern Biotechnologies), and monoclonal mouse antibovine elastin IgG (1:1000; Sigma). Bound primary antibodies were observed with appropriate secondary Alexa488 fluorochrome–conjugated antibodies (1:200; Molecular Probes). Omission of the first antibody was taken as a control. Sections were fixed in 100% ethanol, air-dried, and embedded in mowiol.
Results and Discussion
Tubular scaffolds
Tubular collagen scaffolds
A standardized method was used to obtain tubular type I collagen scaffolds with inexpensive materials and methods, including polystyrene tubes, stainless steel mandrels, freezing, and lyophilizing. Tubular scaffolds were made with inner diameters ranging from 4 to 10 mm (Fig. 1), by selecting specified mandrels and molds (Table 1). Scaffolds were generally about 5 cm in length. The pore sizes could be influenced by the freezing temperature (Fig. 3). A low freezing temperature resulted into smaller pores than a higher one; freezing at −20°C gave pore sizes of about 150 μm, in contrast to ∼10 μm pores in the case of −196°C freezing. In the latter procedure, however, macroscopical cracks in the scaffolds were observed due to the rapid freezing. Freezing at −80°C by means of dry ice and ethanol gave a heterogeneously dispersed lamellar structure with lamellae about 60 μm apart.

Scanning electron microscopy micrographs of cross sections of tubular collagen scaffolds (4 mm), frozen at different temperatures: −20°C (freezer)
Long tubular collagen scaffolds
A two-segmented mold was made to obtain longer tubular scaffolds. The length of the mold was limited because the frozen collagen suspension could only be freeze-dried from the top in the tubes used. Use of the designed two-segmented stainless steel mold resulted in tubular collagen scaffolds of 11–12 cm in length. SEM analyses displayed a highly porous ultrastructure similar to basic tubular scaffolding (Figs. 2C and 3A). Longer segments of scaffolds may be needed in tissue engineering of ureter and blood vessel. In the latter case, longer scaffolds can especially be useful in bypasses by end-to-side vascular grafting. If desired, longer scaffolds may be dried into tubular films.
Tubular collagen scaffold with internal radial orientation
Radial orientation was achieved through the creation of a temperature gradient across the mold's radius by placing liquid nitrogen into a hollow mandrel that was surrounded by collagen suspension. Radial orientation consisted of parallel collagen lamellae with spaces ranging from 80 to 100 μm interconnected by struts (Fig. 4B, inset). Radial orientation may be useful to achieve deeper cell penetration into scaffolds, as cells may migrate along the radial orientation deep into the scaffold. 24 Further, radial orientation mimics the architecture of the ECM of a number of organs, including some skeletal muscle (e.g., of the diaphragm) and secretory organs. It may also be useful for tissue engineering of peripheral nerve. 24

Scanning electron microscopy micrographs of tubular collagen scaffolds, displaying circumferential orientation
Tubular collagen scaffold with internal circumferential orientation
Circumferential orientation of the collagen was achieved by twirling aggregated type I collagen fibrils on a mandrel, followed by freezing and freeze-drying. SEM showed that circumferential sheets of aggregated collagen were ∼50–100 μm apart (Fig. 4A). A circumferential orientation is generally found in layers of smooth muscles in the wall of tubular organs, for example, the vascular tunica media. In such organs smooth muscle cells are positioned within circumferentially aligned ECM molecules. 41 The procedure allows smooth muscle cells to be incorporated into the tubular scaffolds by twirling the cells in between the collagen fibrils.
Suturability
The suturability of crosslinked basic tubular collagen scaffolds was assessed as surgeon-friendly, as evaluated by interposing tubular scaffolds into a porcine femoral artery and between a rabbit urethra and bladder (Fig. 5). Four-point sutures were used for placement to the femoral artery. After suturing, the scaffold was flushed with saline, resulting in some perfusion through the scaffold's wall, but none at the anastomotic side of the artery. In case of interposing tubular scaffolds between rabbit urethra and bladder, also four-point sutures were used. None of the sutures were pulled through the scaffold's wall. Suture retention of wet tubular collagen scaffolds was quantified as 0.1 ± 0.02 N. Thus, suturability was considered satisfactory with regard to in vivo implantation studies. The concentration used of the crosslinker EDC was 33 mM, which is relatively high though. This concentration was found optimal with respect to the immobilization of glycosaminoglycans, the increase of the denaturation temperature, and the decreases the free amino group content of collagen scaffolds. 42

Demonstration of suturability by ex vivo placement of a collagen tubular scaffold (−20°C, inner diameter 4 mm) end-to-end to a porcine femoral artery
Tubular films
Tubular collagen films
Tubular type I collagen films were made by air-drying wetted tubular scaffolds around mandrels. Film thicknesses were ∼30, 40, and 70 μm for the inner diameters of 4, 6, and 10 mm, respectively (with matching molds shown in Table 1) (Figs. 1 and 3D for 4 mm mandrels). Dried scaffolds on stainless steel mandrels were difficult to remove. In the case of PEEK mandrels, films could be easily removed due to the high inertness of PEEK. However, tubular films exceeding about 1 cm in length were difficult to remove. Larger film may be removed entirely from the mandrel if thicker films are prepared by an increased type I collagen concentration in the casting suspension.
Composite tubular scaffolds/films
Tubular collagen scaffold with polymer film
A porous PLCL film was abluminally applied to 4 mm tubular scaffolds and was firmly attached to the collagen scaffold. The addition of an outer synthetic porous polymer film created hybrid scaffolds and prevented the collapse of the scaffold. Basic tubular scaffolds, regardless of diameter, tend to collapse when wetted and placed on a flat surface, but the PLCL coating prohibited this (Fig. 6A). The burst pressure of tubular collagen scaffolds with abluminal polymer film was 102 ± 35 mm Hg, whereas tubular collagen scaffolds without polymer had no significant pressure build up. 39 UTS was 343 ± 76 versus 93 ± 21 kPa for tubular collagen scaffolds with and without abluminal polymer film, respectively. The thickness of the outer polymeric film was ∼50 μm. The film contained pores of about 5–10 μm in diameter (Fig. 6B), possibly caused by air bubbles escaping from the collagen scaffold during preparation. Such pores may facilitate nutrient exchange and cellular influx and/or adhesion.
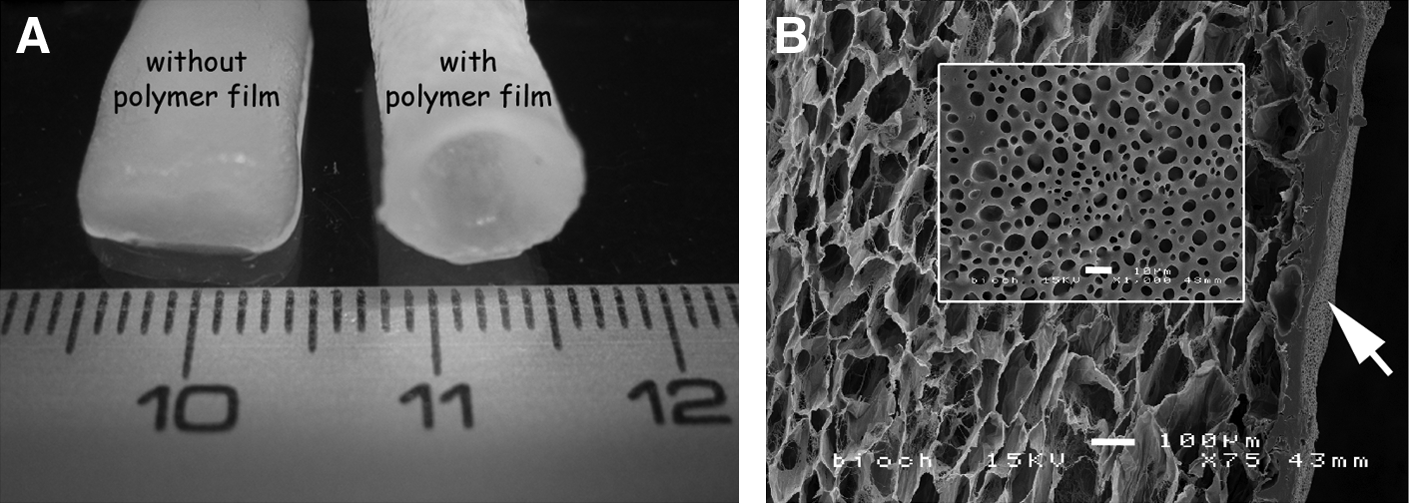
Reinforcement of tubular scaffolds by synthetic polymer films. Prewetted collagenous tubular scaffolds without a polymeric film tend to collapse, but remain open after supplementation with a polymeric film
Tubular collagen film with elastin fibers and type IV collagen
A tubular collagen film was constructed harboring elastin fibers and a luminally deposited type IV collagen layer. This was performed to illustrate the potential of tailor-made scaffolds in mimicking both composition and architecture of the ECM. Elastin fibers were added to the collagen suspension. Elastin fibers were found in clusters throughout the type I collagen film (Fig. 7). The resulting film had a thickness of ∼100 μm. Type IV collagen was luminally coated, and had a thickness of ∼4 μm.

Immunohistochemical images of cross-sectioned tubular film with type I collagen fibrils and elastin fibers, with a luminal type IV collagen layer. Staining for
The tubular scaffolds and films with different diameters prepared in this study are applicable for tissue engineering of various tubular organs in the human body. Tubular scaffolds are the materials of choice when replacing tubular structures in the body. Small-diameter tubes are necessary for replacement of, for example, urethra and blood vessel (∼641 and ≤6 mm43 in humans, respectively), whereas larger diameter tubes are required to repair defects in for instance the trachea and esophagus (inner diameters of 1.241 and 1.5–2 cm, 44 respectively). Small-diameter blood vessels, for instance, are defined as having diameters equal or <6 mm. The human ureter has an average diameter of 3 mm or less, but may range from 1 to 6 mm. 45 The human urethra has a diameter of 6 mm (male or female), 41 but is not equal in diameter along its entire length, and may range from 6 to 8 mm.46,47 In a rabbit model, 3–4-mm tubular scaffolds are more appropriate for urethra. Nuininga et al. 33 sutured flat collagen scaffolds into a tubular shape for urethra tissue engineering. The use of tubular scaffolds from scratch can prevent unnecessary seams in the scaffold. Tissue engineering of large-diameter organs would require larger scaffolds with diameters over 10 mm, namely, up to 2.5 cm for esophagus (or higher 48 ) and trachea (1.4–2.7 cm49) in humans. Longer scaffolds were also constructed, which may especially be useful for tissue engineering of organs, like the ureter, which is generally 25–30 cm in length, or esophagus which is 25 cm long. 48
It was also possible to create tubular scaffolding with different pore sizes ranging from 10 to 150 μm. Differences in 3D organization of a biomaterial, like pore size and porosity, have been shown to influence cellular behavior. 15 Lower porosities may limit cellular ingrowth, especially when the pore size is smaller than the cell's diameter. Cells would not be able to reach the center of the scaffold limiting nutrient diffusion and waste product removal. Too large pores would provide a too small specific surface area, limiting cell attachment. 18 O'Brien et al. 50 showed a linear and strong correlation between scaffold-specific surface area, cell attachment (3T3 cells), and viability for pore sizes of 96–150 μm, which are comparable to basic −20°C tubular scaffolds in this study.
Mechanical properties of scaffolds are important criteria in scaffold analysis. For some applications in regenerative medicine, collagen tubes may have insufficient strength. Therefore, several alterations to the collagen tube were investigated in this article, such as the abluminal application of a polymer PLCL film. PLCL has been proposed as a biomaterial in tissue engineering applications, for example, blood vessels.51–53 The degradation time of the polymer may be up to a few years, depending on the size and implantation site. The degradation products are expected to be nontoxic and to be incorporated in the natural metabolism. In theory, the concentration of degradation products in the body may be low as a result of the slow degradation process, thus limiting major pH changes in comparison to fast degrading materials such as poly glycolic acid (PGA). However, (in vivo) follow-up studies regarding the biocompatibility and biodegradability of the polymer are required. Burst pressure of tubular scaffolds with an abluminal polymer film were up to 100 mm Hg, and UTS was ∼3.5 times higher compared with basic tubular collagen scaffolds. Such strengths would be sufficient for regenerative medicine applications in, for instance, ureter or urethra.
The drying of wetted −20°C tubular scaffolds around their mandrels resulted in tubular collagen films. Composite tubular films could be prepared comprised of an outer layer of type I collagen and elastin, and a luminal layer of type IV collagen. Type IV collagen is a typical basement membrane component on which endothelial and epithelial cells may proliferate and differentiate. The method described holds promise to prepare tubular constructs with tissue-specific basement membranes, capable of directing cellular proliferation and differentiation. The basement membrane equivalent may be further optimized by the introduction of other basement membrane components such as heparan sulfates by crosslinking, for example, by EDC/NHS.42,54 The tubular structures harboring a specific basement membrane analog may then be evaluated, for example, as blood vessel intima equivalents or as esophagus constructs.
Conclusion
A number of methodologies, based on casting, molding, freezing, and lyophilization is described to construct tubular collagenous scaffolds and films. The technology allows for large flexibility and tunability with respect to dimensions (diameter, size, wall thickness, and length), inner structure (e.g., pore size and inner morphology), and composition (blends with other components and specific inner/outer layers). The technology enables the construction of tailor-made tubular scaffolds and films based on biomolecules and may serve regenerative medicine applications.
Footnotes
Acknowledgments
Henny Giesbers from instrumental services (RUNMC) is acknowledged for his assistance in obtaining mandrels and custom-made molds. Kees Jansen from the Department of Urology is thanked for his help in the handling/suturability experiments. Roger Lomme from the Department of Surgery (RUNMC) is acknowledged for his assistance in biomechanical analysis. The microscopical imaging center (NCMLS, RUNMC) is acknowledged for facilitating electron microscopy services. This study was financially supported by the Dutch Program for Tissue Engineering (DPTE 6735) and by the EU-FP6 project EuroSTEC (contract: LSHB-CT-2006-037409).
Disclosure Statement
No competing financial interests exist.