
Abstract
Animal models for preclinical functionality assays lie midway between in vitro systems such as cell culture and actual clinical trials. We have developed a novel external fixation device for femoral critical size defect (CSD) in the femurs of immunodeficient mice as an experimental model for studying bone regeneration and bone tissue engineering. The external fixation device comprises four pointed rods and dental acrylic paste. A segmental bone defect (2 mm) was created in the midshaft of the mouse femur. The CSD in the femur of the mice were either left untreated or treated with a bone allograft, a cell-scaffold construct, or a scaffold-only construct. The repair and healing processes of the CSD were monitored by digital x-ray radiography, microcomputed tomography, and histology. Repair of the femoral CSD was achieved with the bone allografts, and partial repair of the femoral CSD was achieved with the cell scaffold and the scaffold-only constructs. No repair of the nongrafted femoral CSD was observed. Our results establish the feasibility of this new mouse femoral model for CSD repair of segmental bone using a simple stabilized external fixation device. The model should prove especially useful for in vivo preclinical proof-of-concept studies that involve cell therapy-based technologies for bone tissue engineering applications in humans.
Introduction
An optimal biomaterial should combine the essential characteristics of bone, namely osteoinductivity and osteoconductivity. Moreover, the scaffolds should be biocompatible, biodegradable, and have similar mechanical properties to that of bone.1–5 Scaffolds for bone repair have been fabricated using a wide range of biomaterials, such as synthetic polymers, native polymers (hydrogels), and their composites.6–9 Since the inorganic component of natural bone is composed of hydroxyapatite, ceramics such as calcium phosphate, calcium sulfate, and calcium carbonate (coral-based ceramics) have also been used as matrices for bone regeneration.3,10
Tissue engineering protocols that include integration of osteoprogenitor cells within scaffolds are a promising strategy for bone repair,11–16 and in recent years, considerable effort has been devoted to developing scaffolds that are impregnated with bone marrow-derived stromal cells (BMSCs). The results of both in vitro17–19 and in vivo20–23 mechanical tests on BMSC-impregnated scaffolds have shown that pressure, strain and fluid flow can influence the osteogenic differentiation of BMSCs in vitro as well as on bone regeneration in vivo. In addition, a perfusion culture of BMSCs showed more osteoblastic differentiation than that of static cultured constructs.17–19,24,25
With the development of cell-impregnated scaffolds, small immunodeficient experimental animals, such as athymic nude rats, have been found to be very suitable for studying the potential clinical utility and functionality of scaffolds that are impregnated with human cells, because they do not require immunosuppressive medication. Further, these animals enable xenogeneic cell transplantation without the risk of graft rejection.26,27
Preclinical bone tissue engineering assays are currently the only method for evaluating the functionality of cell-impregnated scaffolds and other bone substitutes that are intended for human use. The standard method for evaluating bone substitutes is creating a critical size defect (CSD) in the long bones of large experimental animals, such as sheep, to simulate the load-bearing condition. More recently, the laboratory rat with a CSD in the femur or tibia has replaced these large animals for evaluating bone substitutes. 28 However, models of orthotopic CSDs in laboratory rats are lacking standardization, and the size of CSD in the long bones of rats in most studies ranges between 2 and 10 mm. 29
Genetically engineered mice are currently being used to investigate human bone and skeletal disorders, and it is necessary that a valid and reproducible CSD model will be applied to mouse femur or tibia to cope with bone-tissue-related questions that require in vivo testing using a CSD.
Several reports have recently been published on fixation devices after CSD creation for use in mice and other small rodents. Femoral fixation after CSD creation can be done by either external or internal fixation. For external fixation, a polyethylene rod, for example, is attached to the fractured bone. For internal fixation, an orthopedic implant that is made from biocompatible stainless steels or synthetic materials is placed in the femoral shaft and fixed by insertion into the supracondylar metaphysic of the femur. Both fixation methods have advantages and disadvantages.26,30–38 Hence, most studies that assessed the functionality of cell-impregnated scaffolds and other bone substitute materials have been done on ectopic and cranial defect models in immunodeficient mice. 39 However, these defect models are unsuitable for studying the potential clinical utility of cell-impregnated scaffolds and other bone substitute materials for repairing load-bearing long bones, the primary target for future clinical applications.
Therefore, the aim of this study was to develop a mouse model in which a load-bearing long bone could be used for assessing the potential clinical utility of a cell-impregnated scaffold. This report describes the creation of a 2 mm CSD in the femur of immunodeficient mice and a method of external fixation, including the evaluation of the CSD, the bone allografts, and the cell-scaffold transplants in this mouse model. Since the usual size of a CSD in rat long bones is 6 mm29 and the length of the long bones of the rat is about thrice longer than those of the mouse, a 2 mm size CSD was created in this mouse model.
Materials and Methods
Surgical procedure
The design of an external fixation frame for the mouse femur with a CSD was based on that described by Ben-Ari et al. for repairing a rat's fractured tibia. 40 The method has been modified for application on segmental bone defect on rat tibiae and adapted for use in the mouse femur. The surgical protocols were approved according to institutional guidelines of the Animal Ethics Committee of the Technion–Israel Institute of Technology, Haifa, Israel. Athymic Nude-Foxn1nu mice, 8-week-old and weighing 25 g (Harlan Laboratories, Jerusalem, Israel) were used for the experiments.
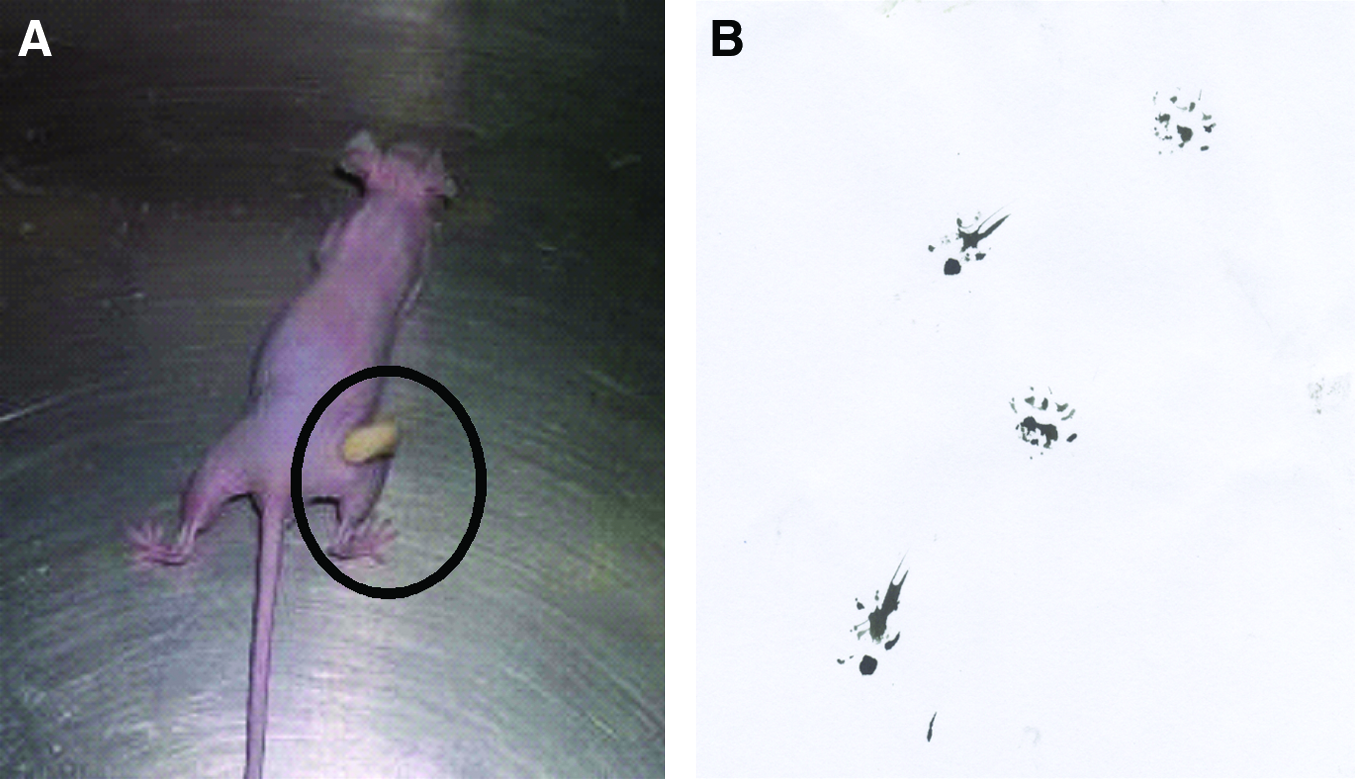
The mice were anesthetized with a 0.5 mL intraperitoneal injection of a 1:1 mixture of xylazine and ketamine. Under aseptic conditions, a longitudinal incision was made over the lateral aspect of the thigh, which was raised and fixed with silicon (Zetaplus, Shermack, Italy). Muscles were split at the linea alba to expose the femur proximally and distally to the medial aspect of the femoral condyle. Four holes (0.3 mm diameter), two holes in the distal region and two holes in the proximal region, were drilled in the midshaft of the femurs. Rods (27G, 0.4 mm) were inserted manually into the drilled holes by penetration through one lateral cortex to the opposite cortex and through the skin. The protruding ends of the rods on the lateral and medial sides were first bent and then connected with acrylic dental paste (Unifast Trad, GC America, Inc., Alsip, IL). Under saline irrigation, a bone defect of 2 mm between the rods was created in the cylindrical midshaft part of the femur (total length 8 mm) using a motorized mini-drill. The muscles were opposed over the bone defect, and the wound was closed with vicryl sutures (Fig. 1).

The external fixation frame weighed between 0.6 and 0.8 g. Approximately 1 h after surgery, the mice regained consciousness and started to move in the cage after a few hours. The mice were housed separately in plastic cages. All animals recovered well from the surgery with no visible restrictions in their movements. Animals were weighed before and at the end of the experiment, and no body weight loss was observed as a result of the surgery. Food and water were available ad libitum.
Mechanical testing
To analyze the mechanical properties of the externally fixated bone, the bending stiffness of mice bones was studied. A fixated femur was clamped at the femoral head. Vertical forces that ranged from 5 to 35 g were applied to the foot. The respective deflections of the femurs were measured with dial micrometers (1 mm accuracy) that were placed in front of and behind the fixators. The test was made with four different fixated or intact femurs. Detailed data regarding the mechanical testing are available in Supplementary Material (Supplementary Material and Data are available online at
CSD and bone allograft
The external fixation device provided a stable frame to tightly hold the bone before creating the CSD. Eight animals were used for each of the four groups (nongrafted CSD, bone allograft group, cell-scaffold group, and scaffold-only group).
To determine which defect size was critical in the femoral midshaft of mice, preliminary tests were conducted on creating a segmental defect of the following sizes: 2.0; 2.5; 3.0 mm. It was found that with defects of 2.0 mm the defect was maintained throughout the 8-week period. The larger CSD (2.5 mm and 3.0 mm) were found to interfere with the stability of the external fixation device (Supplementary Fig. S6). Consequently, a 2.0 mm gap was chosen as the optimal size of the CSD in this assay.
Bone allografts were obtained from bones of littermates of the experimental mice. The allografts were prepared by carefully removing all the attached muscles from the bones. The allograft was cut from the cleaned bones using a rotator drill and then fitted into femoral CSD.
Cell source and culture conditions
BMSCs were isolated from fresh human bone marrow of two male and two female Afro-American donors, aged 21–44 (Cambrex-Lonza Walkersville, Inc., Walkersville, MD) based on their”. The progenitor cells were cultured (37°C, 5% CO2, 1 week) in a standard culture medium (αMEM) that was supplemented with 10% fetal calf serum (FCS), 2 mM L-glutamine, 100 U/mL penicillin, and 100 μg/mL streptomycin (Biological Industries, Beit Haemek, Israel). At 70–80% confluence, the cells were trypsinized, counted, and passaged (P1) to induce osteogenic differentiation in culture; the P1 cultures were cultured in αMEM induction medium that contained 10% FCS, 2 mM L-glutamine, 100 U/mL penicillin, 100 μg/mL streptomycin, 100 μg/mL ascorbic acid, and 10−8M dexamethasone until confluence was achieved about 1 week later. The osteogenic potential of the cells in vitro is shown in Supplementary Fig. S5.
In vivo transplant, in vivo cell-scaffold transplant, and scaffold-only transplant
Confluent cultures (P2) were trypsinized, washed with phosphate buffered saline (PBS), and 1×106 cells were mixed with ProOsteon particles (Interpore Cross, Irvine, CA; particle size 0.5–1.0 mm, 20 μL volume). These calcium carbonate particles, which were covered with a 5 nm layer of hydroxyapatite (coral/hydroxyapatite scaffold), were rotated gently in an incubator at 37°C for 1 h. At the end of the incubation, the particles were collected by brief centrifugation. The particles were first mixed with mouse fibrinogen (15 μL; 3.2 mg/mL in PBS) and then mixed with mouse thrombin (15 μL; 25 U/mL in 2% CaCl2) to create fibrin clots. The fibrin clots were then transplanted into the CSD for 8 weeks. Control animals were similarly transplanted with scaffold only.
Postsurgery analysis
Digital x-ray, microcomputed tomography
Digital radiographs of mice femurs were taken on the day of the surgery, and then every 2 weeks for 8 weeks using an Oralix AC Densomat X-ray machine (Gendex Dental System, Milan, Italy) at the following operating conditions: 65 kV peak voltage, 7.5 mA anode current, and an exposure time of 0.26 s) that was operated by KODAK Dental Imaging Software version 6.5 (Kodak Dental Systems, GA).
After 8 weeks, the mice were euthanized and transplanted femurs were dissected, fixed in 10% neutral buffered formalin, and the metal rods of the fixation device were carefully removed before the bones were analyzed by microcomputed tomography (μCT) on a μCT 40 imaging system (Scanco Medical AG, Bassersdorf, Switzerland) providing an isotropic resolution of 20 μm. A constrained Gaussian filter was used to partly suppress the noise in the volumes. The mineralized bone tissue was differentially segmented from the nonmineralized tissues by using a global thresholding procedure. All samples were binarized using the same parameters for the filter width (1.2), the filter support (1) and the threshold (224; in permille of maximal image gray value).41,42
Histology and histomorphometry
After μCT imaging, the entire femur was decalcified with 10% ethylene diaminetetraacetic acid (EDTA). The orientation and alignment of the femoral bones were carefully taken into consideration during paraffin embedding to be able to view the defect. Longitudinal serial sections (6-μm thick) were stained with hematoxylin and eosin (H&E) for general histology and histomorphometry.
Using the Image Pro 6 image analysis software (Media Cybernetics, Silver Spring, MD), the area of newly formed bone in the CSD was measured on the H&E-stained sections, and the results were expressed as a proportion (percentage) of the area of the newly formed bone and the area of the original CSD. The results were determined from five H&E-stained sections of the femur of each mouse in the four experimental groups. The mean proportions of each experimental group were compared using an unpaired two-tailed Student's t-test, accepting p<0.05 as significant.
Results
Mechanical testing and analysis
The bending stiffness of intact bone was found experimentally to be
The maximal deviation of the bone with the fixator from the intact bone was found to be 1.5 micrometers. Therefore, we concluded that introducing the fixator does not dramatically affect the bending stiffness of the bone.
Postsurgery observations
Postsurgery rehabilitation and complete mobility that included load-bearing functionality were confirmed by analyzing ink-labeled foot-prints of the mice after surgery (Fig. 2). The mice fully recovered from the surgery and displayed a full range of hind leg movements when walking on a treadmill, as shown in a movie taken 10 days postsurgery (Supplementary Movie S1).
Digital x-ray and μCT
The external fixation frame remained stable, and the edges of the original bone in the CSD were aligned parallel to each other throughout the 8-week study period, data for 0, 4, and 8 weeks are presented. No healing was observed in the empty nongrafted CSD (Fig. 3A–C). Cell-scaffold constructs and scaffold-only x-ray images throughout the experiments are shown in Figure 3D–F and G–I, respectively. Since the scaffold contained mineral (coral/hydroxyapatite), an opaque image was observed in x-ray images from the day of operation and continuously throughout the experiment. This opacity masked the defect site, and the digital x-ray technique was not informative regarding the healing process in these groups. Integration of the graft with the original bone was observed in the CSDs that were filled with the bone allograft (Fig. 3J–L).
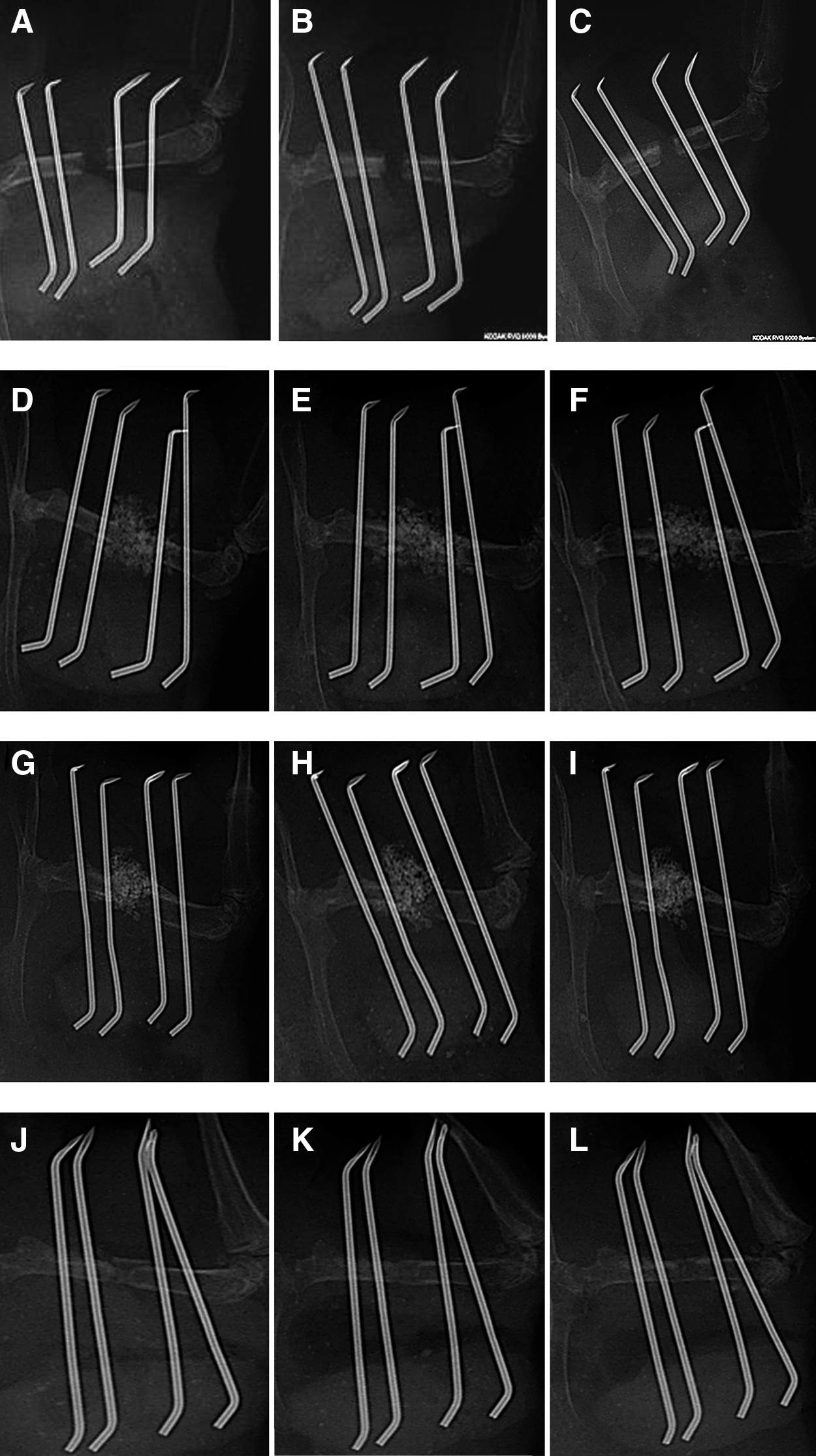
Digital radiographs of the femur with a nongrafted critical size defect (CSD) of an athymic nude mouse
Examination of the μCT images confirmed no closure of the CSD in the nongrafted CSD (Fig. 4A–C). Examination of the μCT images confirmed integration of the graft in the CSDs that were filled with the bone allograft (Fig. 4D–F); Bone trabeculae were observed between the two edges filling the gap of the original defect.

X-ray images of the cell-scaffold construct and the scaffold only (Fig. 5A, D) revealed the scaffold that contained mineral (coral/hydroxyapatite). The opaque material was also seen in μCT images from both groups (Fig. 5B, E) that were taken at the end of the 8-week study period. To distinguish between the mineral content of the scaffold and the newly formed bone, samples were demineralized and then histologically evaluated.

Histology
Examination of the histology sections of the femurs in which no graft was placed in the CSD confirmed no repair of the CSD with newly formed bone after 8 weeks, the CSD contained connective and adipose tissue (Fig. 4C).
Examination of the histology sections of the femurs in which a bone allograft was placed in the CSD confirmed integration of the graft with the original bone and repair of the CSD with newly formed bone after 8 weeks (Fig. 4F). Examination of the histology sections of the femurs transplanted with cell-scaffold constructs (Fig. 5F) revealed the creation of a bone bridge (in six out of eight animals) in the middle of the bone defect as shown by histology. Higher magnification showed numerous osteoblasts and osteocytes that reside in the newly formed bone (Fig. 5G). In scaffold-only transplants no bone was observed, apart from a few bone fragments (Fig. 5C).
Histomorphometry of the newly formed bone in the CSD area revealed maximal bone formation in the bone allograft (95%), whereas minimal bone formation (10%) was observed in the nongrafted CSD that may be attributed to limited outgrowth from the bone stubs. Histomorphometry of the CSDs that were transplanted with the cell-scaffold construct revealed a substantial amount of newly formed bone (65%) in all CSDs, and a bony bridge was present in six of the eight CSDs, 8 weeks after surgery. Histomorphometry of the CSDs that were transplanted with the noncellular scaffold construct revealed a modest amount of newly formed bone (20%) and no bony bridges in the CSDs (Fig. 6).
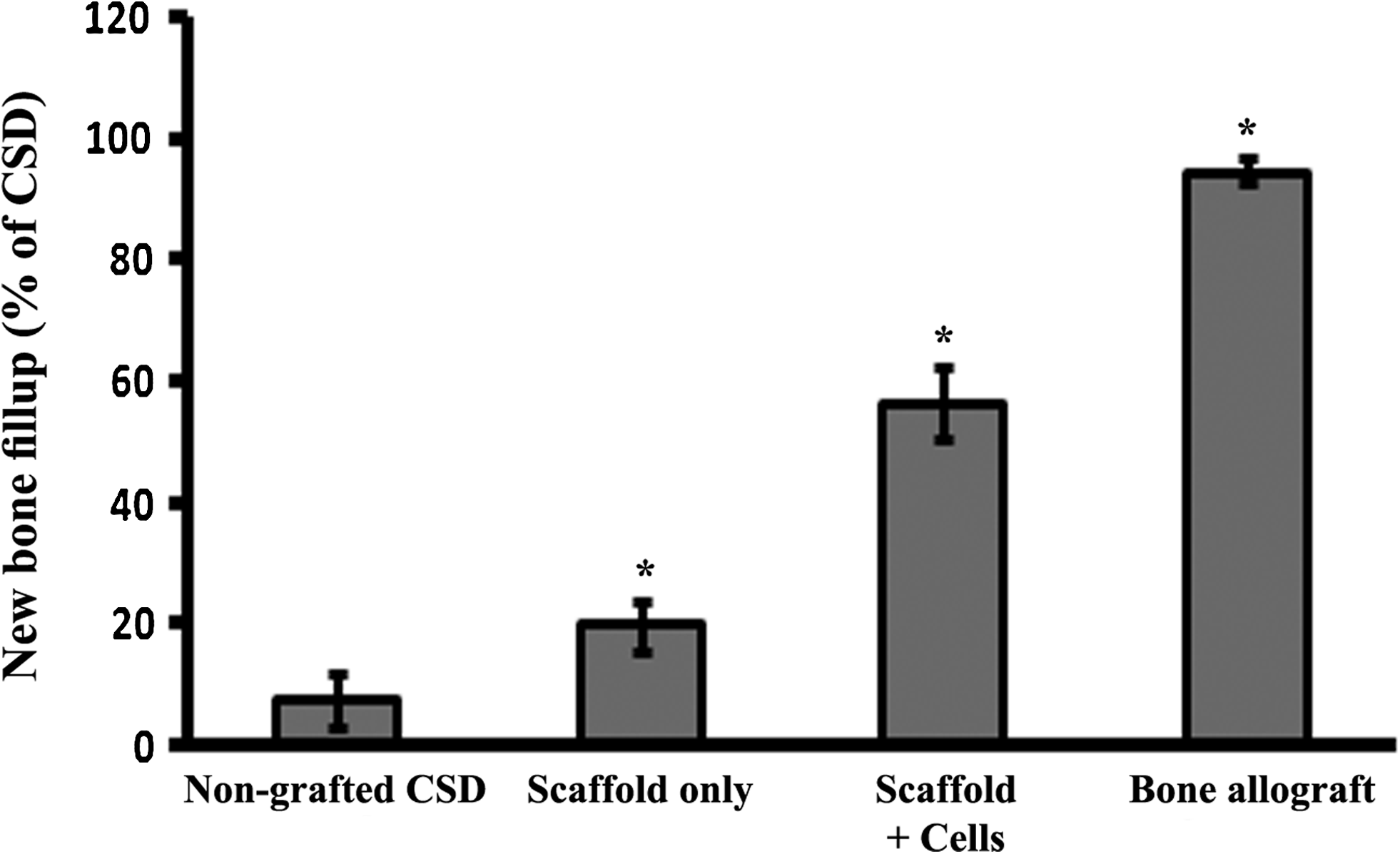
Quantitative analysis of the area of new bone formation in the CSD of athymic nude mice, 8 weeks after surgery. The data are expressed as the mean±standard deviation of the area of the newly formed bone, in proportion to the total defect area, in the CSD of eight athymic nude mice of each experimental group. *p<0.05, and is the significance of the difference to that of the nongrafted CSD.
Discussion
Various approaches have been used for treating large bone defects 28 in the field of tissue engineering. There are several established and acceptable animal models, such as rabbits,43–46 sheep,28,47–49 and dogs,14,50 which have been used for assessing the efficacy of cell therapy based on BMSCs to repair long bone defects. However, these animal models are not available in most research laboratories. In the last few years, CSD models in laboratory rodents became popular for determining the potential of different biomaterials or approaches for bone tissue engineering. The main small animal model in existence, relevant to this type of study, is the immunodeficient rat,14,27,51 whereas the only available strain is the athymic rat, which is not fully immunocompetent as compared with immunodeficient mice strains available for human cell studies.
Cheung et al. have developed a custom-made external fixation method for repairing femoral fractures in the mouse. 52 This application was specifically designed for repairing bone fracture and not for creating a segmental bone defect, because the distance between the rods did not allow the creation of a 2–3 mm defect. In addition, its utility was limited because of the need to fabricate a customized bone fixation device.
Several mouse CSD models with internal fixation of the long bone have recently been published.26,38 In these models, the femur was fixed using a pin that was inserted through the knee, passed through the medulla of the bone, and then fixed by insertion into the supracondylar metaphysic part of the bone.
A defect whose size did not exceed 5 mm was then created in the bone. These models have several limitations, as the insertion of the pin removes a large part of the bone marrow. The surgical procedure involves the fixation of the whole leg and can affect the mobility of the mouse. The method of fixation can affect the weight-bearing aspect of this model Moreover, the inserted pin needs to be completely removed before the mechanical testing, and this removal can cause deformation to the bone that can affect the results of the mechanical tests.
Another CSD model that is sometimes used is the mouse ulnar defect model, where the radius serves as a fixator53,54 and no external fixation device is used. Despite the simplicity of this model, it has some limitations. First, the model does not truly mimic the human situation of load-bearing. Second, the diameter of the mouse radius is less than 1 mm, and this small size is restrictive, because it does not allow scaffold constructs to be assayed. Third, any repair may be due to a contribution from the adjacent radius.
The external fixation device, which is described in this article, provides a rigid frame for creating a CSD in mice. Our results clearly show that no repair was observed in the untreated femoral CSD, 8 weeks after its creation, and this finding suggests that this CSD is a genuine femoral CSD.55–57
The CSD model fixated using the external fixation device described in this article mimics the true load-bearing situation needed for clinical bone repair that is crucial for osteogenesis.19,23 Mechanical testing of the described external fixation device shows that the bending stiffness of the fixated femur is similar to that of an intact femur. Combined with the fact that the overall weight of the device is less than 4% of the mouse body weight, we conclude that this device does not interfere with mobilization after surgery, as seen using the footprints labeling technique and treadmill. Moreover, based on mechanical testing performed on several fixated legs, the model proves to be highly reproducible. It thus provides a reliable load-bearing model in an orthotopic site such as the femur.
It is now more than a decade since the demonstration of ectopic bone formation and subsequent new bone formation using a ceramic scaffold that was loaded with xenogeneic cells in an immunodeficient mouse.39,58 The new external fixation device, which is described in this article, will allow for the in vivo testing of bone substitute materials impregnated with xenogeneic cells after creating a femoral CSD to be more feasible and accessible to researchers studying bone tissue engineering. The advantages of the model are (1) the fixator is not custom made, and researchers can fabricate and apply it in their laboratories, (2) the volume of the induced femoral CSD is about 15mm3, and this volume should allow investigation of osteoinductivity and osteoconductivity of different BMSC-impregnated scaffolds, and (3) mechanical testing is made feasible, because there is no need to remove the rods that hold the two parts of the femur.
As just described, the femur of nude mice is very small, typically under 15 mm length and 3 mm in diameter. We have, nevertheless, succeeded in demonstrating that it is possible to apply a simple external fixation device to the mouse femur. In the present study, a cell-scaffold construct was used for testing the repair of a femoral CSD in mice. Our results show that 65% of the defect gap volume was filled with newly formed bone in femoral CSD that was transplanted with a cell-scaffold construct. In six out of the eight animals of this experimental group, a bony bridge was observed in the femoral CSD, 8 weeks after surgery, whereas no bony bridge was observed and only 20% of the gap was filled in transplants containing scaffold only. This result indicates the need for osteoconductive biomaterial combined with cells for substantial in vivo bone formation.59,60 Biocompatible scaffolds are crucial for the in vivo testing of implanted cell-scaffold constructs, because they provide the necessary support for cell proliferation and differentiation. 8 The results of the present study show that this model can be used for screening of a variety of combinations of cell-based transplant materials, which include various cell types and three-dimensional biomaterials. Such combinations can be screened using this model to optimize protocols for successful in vivo assays. Using this model could be useful for predicting the outcome of testing in larger animals and influence the choice of an experimental protocol in a human clinical study.
In conclusion, the model was shown to be easy and convenient to apply, reproducible, mechanically stable, and light weight. In addition, the model can be used in numerous research settings, such as bone tissue engineering and for studying bone healing in wild-type, immunodeficient, and genetically engineered mice.
Footnotes
Acknowledgments
The authors wish to acknowledge EU grant GENOSTEM (LSH-2003-503161) for supporting this research. The excellent technical assistance of Janette Zavin and Pessia Shenzer is also acknowledged.
Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.