
Abstract
Alginate is a key hydrogel for cartilage tissue engineering. Here, we systematically evaluated four biomedical- and two nonbiomedical-grade alginates for their capacity to support the in vitro culture and in vivo transplantation of articular chondrocytes. Chondrocytes in all ultrapure alginates maintained high cell viability. Spheres composed of biomedical-grade, low-viscosity, high-mannuronic acid content alginate showed the lowest decrease in size over time. Biomedical-grade, low-viscosity, high-guluronic acid content alginate allowed for optimal cell proliferation. Biomedical-grade, medium-viscosity, high-mannuronic acid content alginate promoted the highest production of proteoglycans. When transplanted into osteochondral defects in the knee joint of sheep in vivo, empty spheres were progressively surrounded by a granulation tissue. In marked contrast with these observations, all alginate spheres carrying allogeneic chondrocytes were gradually invaded by a granulation tissue containing multinucleated giant cells, lymphocytes, and fibroblasts, regardless whether they were based on biomedical- or nonbiomedical-grade alginates. After 21 days in vivo, transplanted chondrocytes were either viable or underwent necrosis, and apoptosis played a minor role in their early fate. The individual characteristics of these alginates may be valuable to tailor specific experimental and clinical strategies for cartilage tissue engineering.
Introduction
Alginate is a long linear unbranched binary copolymer consisting of
The aim of this study was to systematically evaluate biomedical- and nonbiomedical-grade alginates for the purpose of articular chondrocyte transplantation in vitro and in vivo. We hypothesized that the composition (high mannuronic acid vs. high guluronic acid) and degree of purity of the alginates directly influence the morphology and size of the spheres and influence the viability, proliferation, and proteoglycan synthesis of encapsulated chondrocytes in vitro. Using a clinically relevant sheep model of an osteochondral defect, we also determined whether such differences may affect the response of the host to the transplanted alginates without or with encapsulated allogeneic articular chondrocytes in vivo.
Materials and Methods
Materials
All reagents were purchased from Invitrogen/Gibco unless otherwise indicated. L-cystein, Na2EDTA, calf thymus DNA and hemalaun were achieved from Sigma. Collagenase type-I (activity: 232 U/mg) was purchased from Biochrom. Dimethylmethylene blue was obtained from Serva. Chondroitin-6-sulfate from shark cartilage was purchased from Fluka. Plasticware was purchased from Falcon (Becton Dickinson). The anti-type-II collagen antibody (AF-5710) was obtained from Acris.
Alginates
Six types of alginates were used in this study (Table 1): a nonbiomedical-grade, low-viscosity, high-mannuronic acid content alginate (LVM) (Sigma), a nonbiomedical-grade, low-viscosity, high-guluronic acid content alginate (LVG) (Fluka), and four purified and biomedical-grade alginates (Novamatrix), including a low-viscosity, high-guluronic acid content alginate (BioLVG), a low-viscosity, high-mannuronic acid content alginate (BioLVM), a medium-viscosity, high-guluronic acid content alginate (BioMVG), and a medium-viscosity, high-mannuronic acid content alginate (BioMVM).
Data according to the manufacturer. 47
n.a., data not available.
Endotoxin assay
Endotoxin levels in the different alginates were determined by a commercial chromogenic Limulus lysate assay following the protocol of the ToxinSensor™ Chromogenic LAL Endotoxin Assay Kit (Genescript). Alginate solutions (1.2%) were diluted (1:100) with pyrogen-free water. Absorption was measured at 530 nm on a microplate reader (n=3) (GENios).
Isolation and cultivation of articular chondrocytes
Articular cartilage was harvested from the ankle joints of three 1-year-old female Merino sheep obtained from a local abattoir within 4 h of slaughter. Cartilage fragments (1 mm3) from the three donors were pooled and digested in spinner bottles containing Dulbecco's Modified Eagle Medium (DMEM), 600 U/mL penicillin G, 600 μL/mL streptomycin (basal medium), and 0.01% collagenase in a humidified atmosphere with 5% CO2 at 37°C for 16 h. 24 Isolated cells were filtered through a 100-μm mesh to remove the undigested matrix. Cell numbers and viability were determined by hemocytometry and trypan blue exclusion. Chondrocytes were placed in monolayer culture in basal medium containing 10% FBS (growth medium) and encapsulated in alginate spheres at passages 3–4.
Encapsulation of chondrocytes in alginate spheres
Cells were trypsinized, washed, and resuspended in sterile, filtered 1.2% alginate in 0.15 M NaCl at a density of 106 cells/mL. The cell suspension was extruded through a 21-gauge needle (Braun) into 102 mM CaCl2 under constant shaking and allowed to polymerize for 10 min. After one wash in phosphate buffered saline (PBS) and three washes in DMEM, the spheres were maintained at 37°C in a humidified atmosphere of 5% CO2 in growth medium, which was changed twice per week.
Microscopic evaluation of the alginate spheres
The morphology of the alginate spheres with and without articular chondrocytes prepared using each type of alginate was determined on days 3 and 21 postencapsulation using an inverted optical microscope (CKX-4; Olympus). The dimensions of the alginate spheres were measured using a computer-based image analysis (n=4).25,26 Briefly, low-magnification images of the whole sphere were acquired by a solid-state CC-12 digital camera (Soft Imaging System) mounted on an inverted microscope and analyzed with the analySIS® Five program (Soft Imaging System).
Cell proliferation and viability
At days 0, 1, 3, 7, 14, and 21 postencapsulation, individual spheres were dissolved in 50 μL of 55 mM sodium citrate and 90 mM NaCl (pH 6.8) for 20 min at 37°C. Chondrocytes were counted using a Neubauer chamber and cell viability was determined by trypan blue exclusion (n=6).
Total sulfated glycosaminoglycan contents of alginate spheres
Alginate spheres were dissolved as described earlier and the released chondrocytes were incubated overnight in 125 μg/mL papain in 1×PBE (100 mM sodium phosphate buffer and 10 mM Na2EDTA [pH 6.5]). Glycosaminoglycans were spectrophotometrically measured by binding to the dimethylmethylene blue dye using chondroitin-6-sulfate to generate a standard curve (n=6).27,28
In vivo transplantation of alginate spheres
Animal experiments were conducted in accordance with the German legislation on protection of animals (the NIH Guidelines for the Care and Use of Laboratory Animals; NIH Publication No. 85-23 Rev. 1985) and were approved by the local governmental animal care committee (No. 30/2008).
Three healthy, female, skeletally mature Merino ewes aged between 2 and 4 years were included in this investigation. They received water ad libitum and were fed a standard diet. Animals (mean weight: 70±20 kg) were sedated with 2% rompun (Bayer) at 0.05 mg/kg body weight and endotracheally intubated after intravenous administration of 20 mL of 2% propofol (AstraZeneca). Anesthesia was maintained by inhalation of 1.5% isoflurane (Baxter) and intravenous administration of propofol (6–12 mg/kg body weight/h). The knee joint was entered through a medial parapatellar approach. The patella was dislocated laterally and the knee flexed to 90°, exposing both the lateral and medial femoral condyles. Six cylindrical osteochondral cartilage defects (3.2 mm in diameter) of defined depth (4.0 mm) were created in the right and left lateral femoral condyles (n=36 defects) with a cannulated burr attached to a battery driven drill system (Synthes). Each defect was washed with saline and blotted dry. Alginate spheres (all of which were prepared 24 h prior to implantation and cultured in growth medium until implantation) were implanted press-fit without further fixation either as empty spheres (right lateral femoral condyles) or with encapsulated chondrocytes (left lateral femoral condyles) into the defects (one animal per time point), their final position being flush with the surrounding articular cartilage. The patella was reduced and the knee was put through a range of motion to assure the stability of the implants. The incisions were closed in layers. Postoperatively, amoxicillin clavulanate (Pfizer) was administered at a dosage of 30 mg/kg of body weight for 1 day. Caprofen (Pfizer) was used as a nonsteroidal anti-inflammatory drug at a concentration of 1.4 mg/kg body weight intramuscularly for 1 day postoperatively. No postoperative immobilization was used and the animals were allowed immediate full-weight bearing.
Histology and immunohistochemistry
Spheres based on the different alginates with encapsulated articular chondrocytes were harvested after 21 days in vitro, fixed in 4% buffered formalin, dehydrated in graded alcohols, and embedded in paraffin. Expression of type-II collagen was detected by immunohistochemical analysis performed on paraffin-embedded histological sections (5 μm) using a specific primary antibody, a biotinylated secondary antibody (Vector Laboratories), and the ABC method (Vector Laboratories) using diaminobenzidine as the chromogen. To control for secondary immunoglobulins, samples were processed with omission of the primary antibody. Samples were examined under light microscopy (BX45; Olympus).
Three, 10, and 21 days after transplantation, the animals were sacrificed. The knee joints were exposed and grossly examined for synovitis, adhesions, or other adverse reactions from the implants. Distal femurs were retrieved, fixed in 4% phosphate-buffered formalin, trimmed, and decalcified. Paraffin-embedded frontal sections (10 μm) were stained with hematoxylin and eosin and safranin O according to routine protocols. 29 Representative sections were evaluated by a pathologist in a blinded fashion. For immunohistochemical detection of apoptotic cells in alginate spheres or in the surrounding granulation tissue, caspase-3 staining was performed using a polyclonal anticleaved caspase-3 antibody (1:100; New England Biolabs) and a goat secondary antibody (1:100; Dianova) linked to streptavidin-horseradish peroxidase and by treatment for 5 min with 3,3'-diaminobenzidine. As a negative control, slides were similarly treated by omitting the primary antibody. Sections were counterstained with hemalaun and examined by light microscopy (BX45; Olympus).
Statistical analysis
Data are given as mean±standard of the mean (SEM). One-way ANOVA was used in multiple comparisons. The Student's t-test or the Mann–Whitney rank sum test was used to detect significant differences when two groups were compared. p-Values of<0.05 were considered significant. Analyses were conducted using Origin 8 (OriginLab Corporation).
Results
Endotoxin content of biomedical- and nonbiomedical-grade alginates
All biomedical-grade alginates contained significantly less endotoxin when compared with nonbiomedical-grade alginates (∼60% and 80% less than LVM and LVG alginates, respectively; p<0.001) (Fig. 1). BioLVM alginate contained the lowest amount of endotoxin among all the purified alginates, that is, significantly lower than BioMVM (p<0.001). Maximal endotoxin contents were found in LVG alginate, significantly higher than in LVM and all purified alginates (p<0.001).
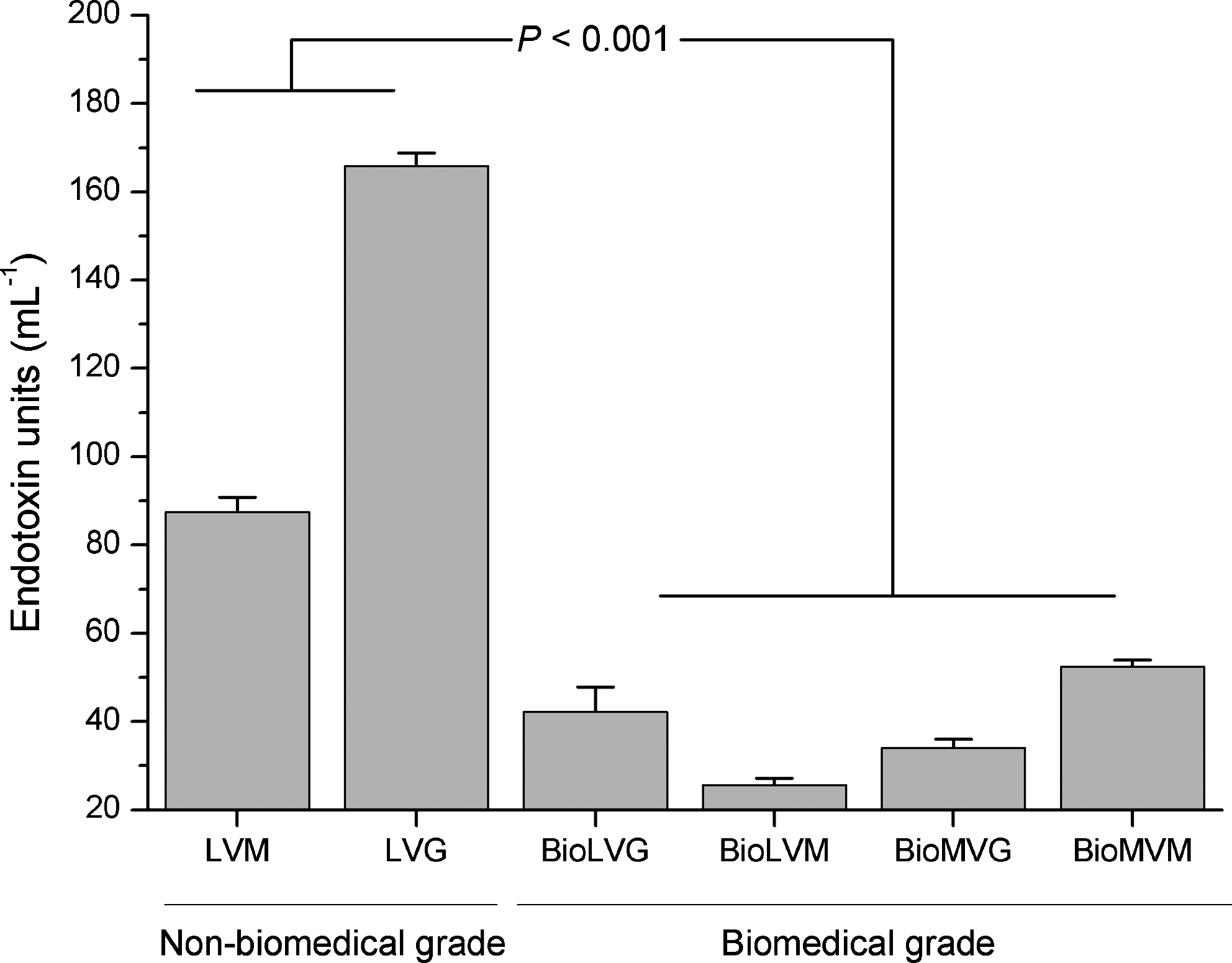
Endotoxin levels of nonbiomedical- and biomedical-grade alginates.
Morphological characterization of alginate spheres
In the absence of cells, spheres made of biomedical-grade alginates were spherically more uniform and could be prepared with a greater reproducibility than nonbiomedical-grade alginates (Fig. 2). Spheres based on LVM alginate showed surface irregularities and tails (Fig. 2A). LVM (2.81±0.04 mm) and BioLVM (2.81±0.09 mm) spheres had the smallest diameters, significantly different than those of spheres made of BioLVG (3.04±0.04 mm), BioMVG (3.06±0.04 mm), and BioMVM alginate (3.07±0.03 mm) (Fig. 3A).
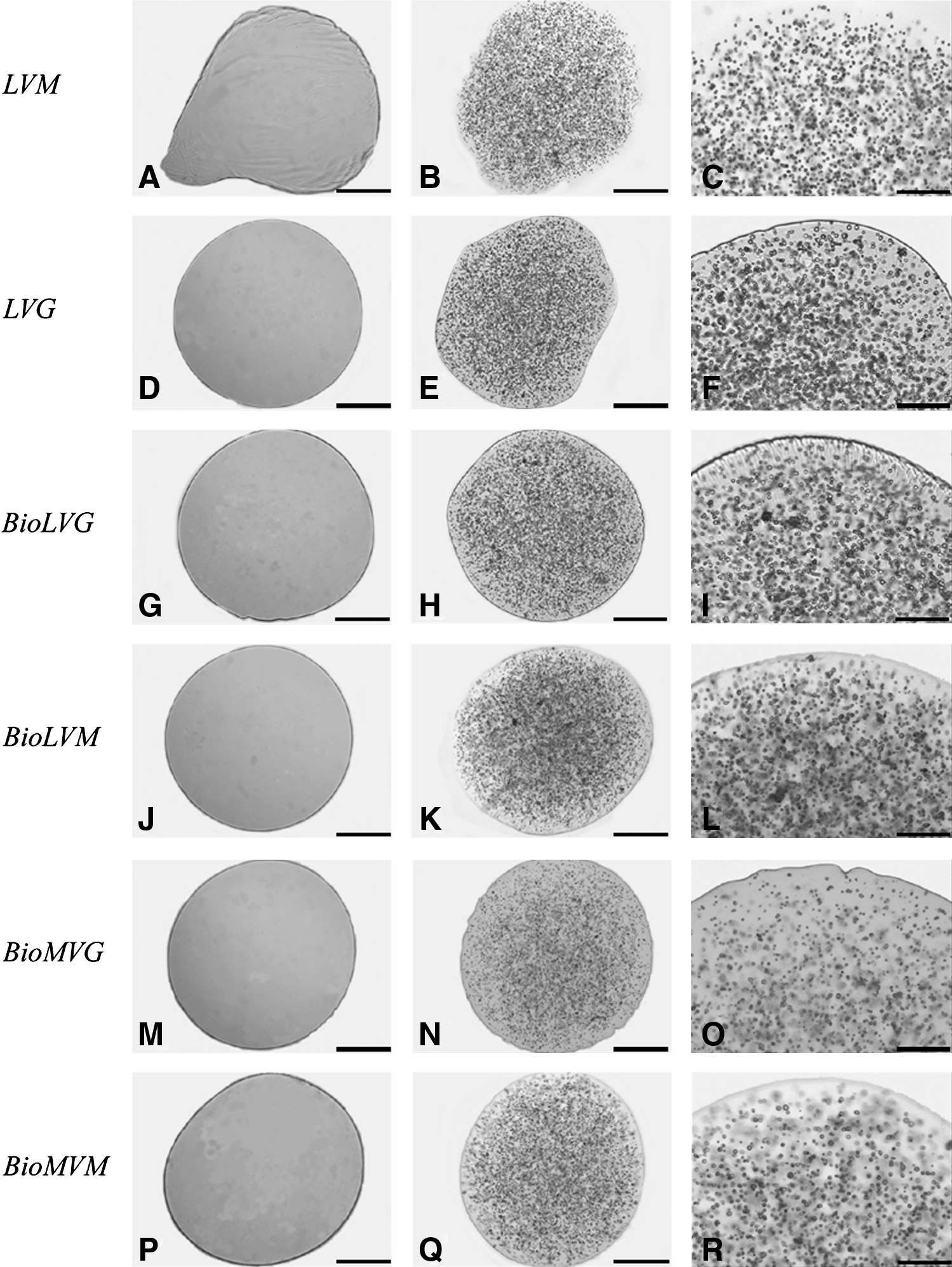
Photomicrographs of spheres obtained from the two nonbiomedical LVM
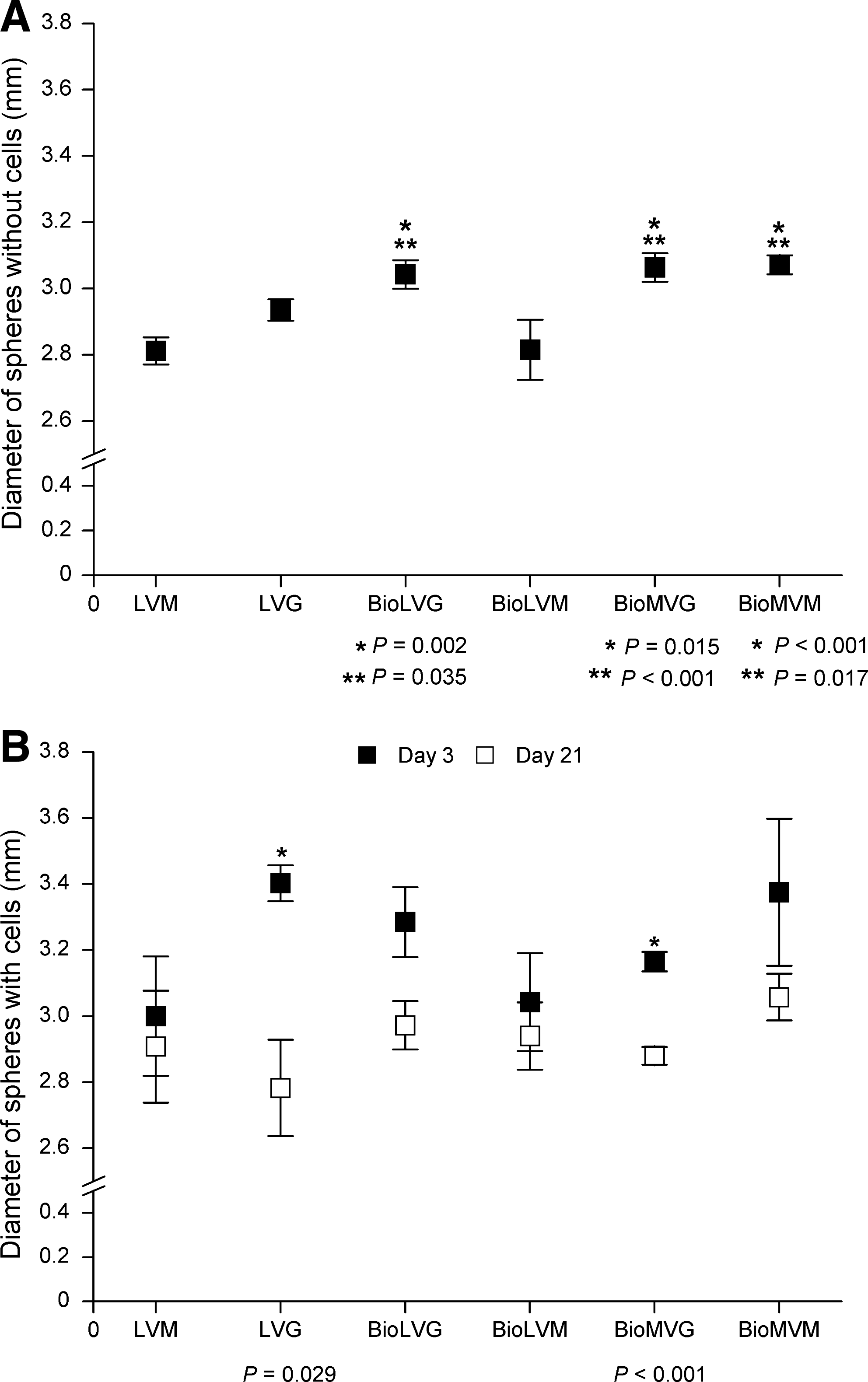
Diameter of alginate spheres without primary articular chondrocytes on day 0
When articular chondrocytes were encapsulated in the alginates (Fig. 2), the mean diameter of the spheres increased by 3.7% (BioMVG; p=0.024), 7.1% (LVM; p>0.05), 7.5% (BioLVG; p>0.05), 8.4% (BioLVM; p>0.05), 10.1% (BioMVM; p>0.05), and 16.1% (LVG; p<0.001), ranging between 3.00±0.18 mm (LVM), 3.04±0.23 mm (BioLVM), 3.17±0.05 mm (BioMVG), 3.29±0.11 mm (BioLVG), 3.37±0.22 mm (BioMVM), and 3.40±0.05 mm (LVG) (p>0.05). After 21 days in vitro, the diameter of all spheres decreased, with LVG (from 3.40 to 2.78 mm) and BioMVG (from 3.16 to 2.98 mm) spheres showing the most pronounced decrease of 20% and 6% (p=0.029 and p<0.001), respectively, whereas LVM and BioLVM spheres showed only minor changes (from 3.00 to 2.9 mm and 3.04 to 2.94 mm; p>0.05) (Fig. 3B).
Chondrocyte viability and proliferation in alginate spheres
At the time of encapsulation, cell viabilities were between 86% and 100% (p>0.05). At day 21, viability of chondrocytes encapsulated in ultrapure alginates was between 90% and 95%, compared with 80%–87% in nonpurified alginates (p>0.05, day 1 vs. day 21) (Fig. 4). All spheres contained a mean of 1.3±0.4×104 viable cells (1.6±0.5×104 total cells) at the time of encapsulation (p>0.05). On 21 days in vitro, the number of viable chondrocytes in the spheres increased 14% in LVG, 30% in BioLVM, 35% in BioMVG, 52% in LVM, and 92% in BioLVG alginate compared with the time of encapsulation (p>0.05). In contrast, the number of viable cells decreased 22% in BioMVM alginate spheres.
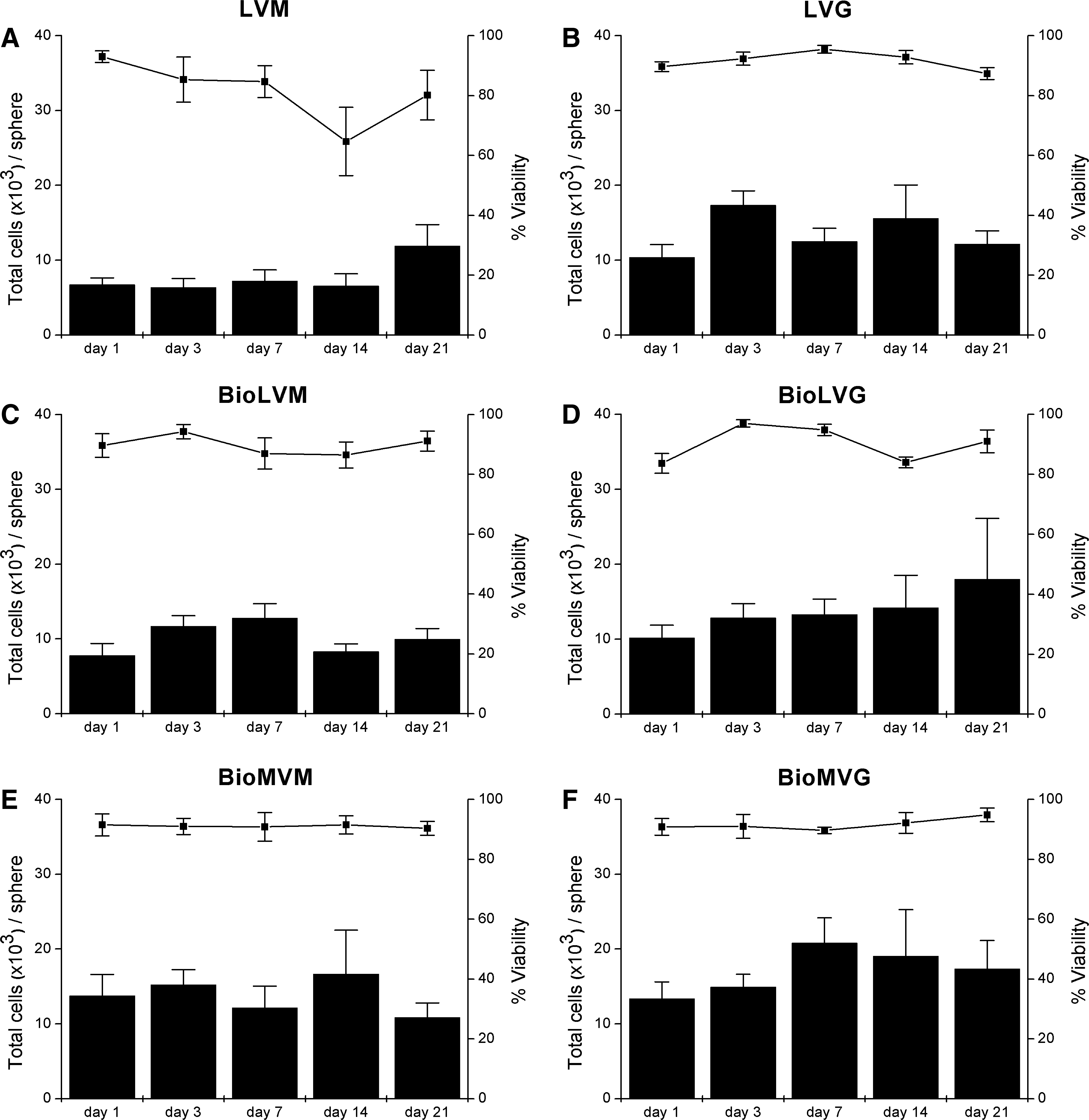
Time course of cell number (columns) and viability (line) of primary articular chondrocytes encapsulated in LVM
Immunohistochemical analysis of type-II collagen expression in articular chondrocytes encapsulated in alginate spheres
Immunohistochemical analysis of type-II collagen expression after 21 days in vitro revealed positively stained articular chondrocytes with their cell-associated matrix, with no apparent differences between the biomedical- or nonbiomedical-grade alginates (Fig. 5).
Immunocytochemical analysis of type-II collagen expression in articular chondrocytes with their cell-associated matrix encapsulated in spheres composed of
Sulfated glycosaminoglycan content of alginate spheres containing articular chondrocytes
On day 3 after encapsulation, spheres based on LVM alginate contained 7.2-fold more proteoglycans than all other alginates (p<0.002) (Fig. 6). After 21 days, chondrocytes in LVG (p<0.001, 5.2-fold), BioMVG (p=0.035, 2.3-fold), and BioMVM (p=0.014, 3.6-fold) alginates produced significantly more proteoglycans than on day 3, whereas the proteoglycan content in LVM alginate decreased 2.6-fold (p=0.624).
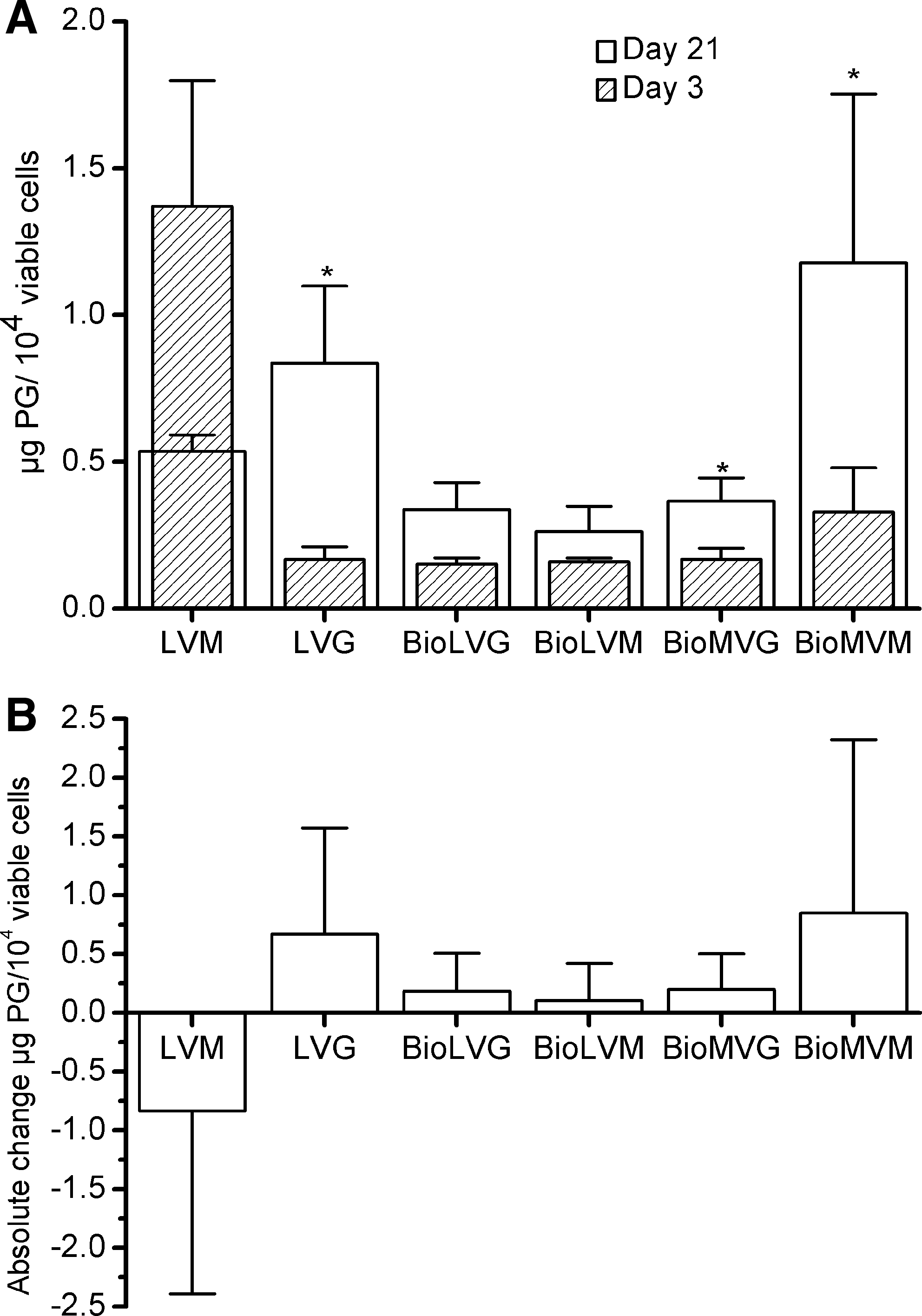
Proteoglycan (PG) contents of articular chondrocytes encapsulated in the six different types of alginate on days 3 and 21.
Macroscopic findings following in vivo transplantation
One day after preparation of the spheres using the six different alginates (without or with allogeneic articular chondrocytes), the resulting implants were press-fit into osteochondral defects in the knee joints of adult sheep. After 3, 10, and 21 days in vivo, no joint effusion, osteophytes, or adhesions were observed. Macroscopically, there were no descriptive differences between defects receiving biomedical- or nonbiomedical-grade alginates, without or with cells, at either time point.
Histological evaluation of the transplanted alginate spheres without articular chondrocytes
Over the time of observation, no histological sign of articular cartilage regeneration was discernible within the defects. At 21 days, the articular cartilage defects were filled with a fibrous repair tissue containing fibroblast-like spindle-shaped cells. The extracellular matrix of the repair tissue did not stain positive for safranin O. There was also no sign of a reconstruction of the subchondral bone. Transplanted alginate spheres containing allogeneic articular chondrocytes were mostly fragmented and rarely spherically intact, with no detectable differences. Implanted alginates without chondrocytes either remained spherically intact or were fragmented without differences between groups throughout the entire observation period. After 3 days of transplanting empty alginate spheres in vivo, erythrocytes surrounded all implants without any granulation tissue, inflammatory reaction, or invasion of capillary vessels from the bone marrow. After 10 days, erythrocytes were present and a granulation tissue was forming. After 21 days, this granulation tissue was more developed compared with day 10 and completely encircled the alginate spheres. It mainly contained eosinophils, fibroblasts, and multinucleated giant cells, with some capillaries and very few lymphocytes. In the depth of the defect, active osteoblasts synthesized woven bone. There was no evidence of an invasion of the spheres by cells from the host in all of the spheres at any of the time points examined (Fig. 7). No differences in the formation of the granulation tissue between groups and spherically intact versus fragmented spheres were seen (Fig. 8).

Histological analysis of representative sections (hematoxylin and eosin [H&E] staining) of an osteochondral defect at day 3
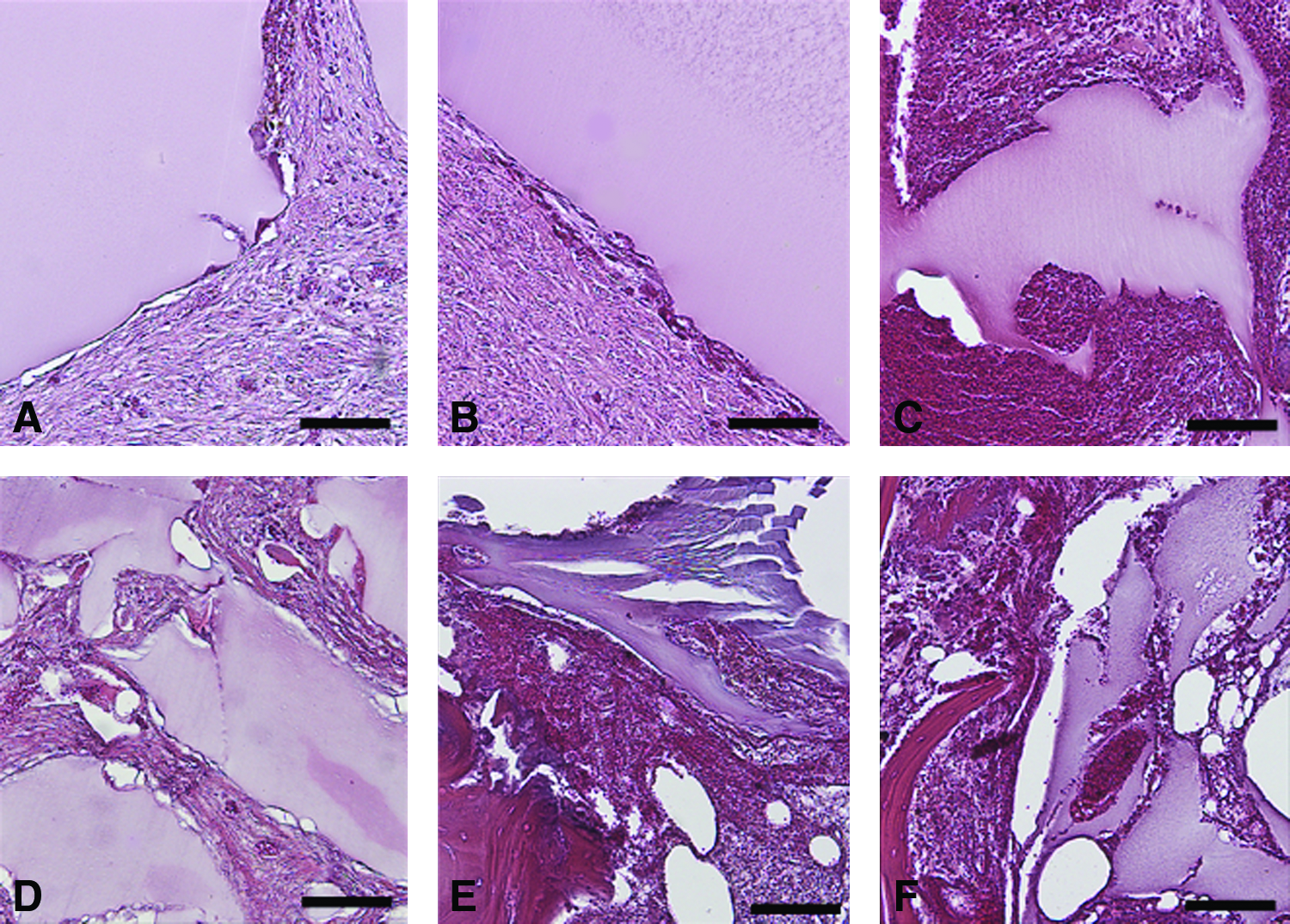
Histological analysis of the host tissue (H&E staining) surrounding the implanted alginate spheres without cells composed of
Histological evaluation of the transplanted alginate spheres with articular chondrocytes
There were no histological signs of articular cartilage regeneration in the osteochondral defects over the entire observation period. At 21 days, the articular cartilage defects were filled with a fibrous repair tissue composed of fibroblast-like spindle-shaped cells. Repair tissue contained no safranin O-positive extracellular matrix. There was also no evidence of a reconstruction of the subchondral bone. Transplanted alginate spheres containing allogeneic articular chondrocytes were mostly fragmented and rarely spherically intact, with no detectable differences between groups at the three different time points evaluated. At 3 days in vivo, all alginate implants were surrounded by erythrocytes, a granulation tissue was not yet formed, and there was no inflammatory reaction or capillary invasion. Chondrocytes within the transplanted alginates were mainly viable. At 10 days in vivo, a granulation tissue containing lymphocytes had formed around the periphery of all alginate spheres and begun to invade them. Erythrocytes were present, although to a lesser extent compared with day 3. Most of the chondrocytes within the transplanted alginates were viable and some of them necrotic, without detectable differences between groups. After 21 days in vivo, the granulation tissue enclosed all spheres composed of the six different alginates. It was comprised of multinucleated giant cells, lymphocytes, eosinophils, fibroblasts, and some erythrocytes, consistent with a chronic resorptive process. Capillary vessels from the bone marrow began to penetrate the granulation tissue without reaching the margins of the implant.
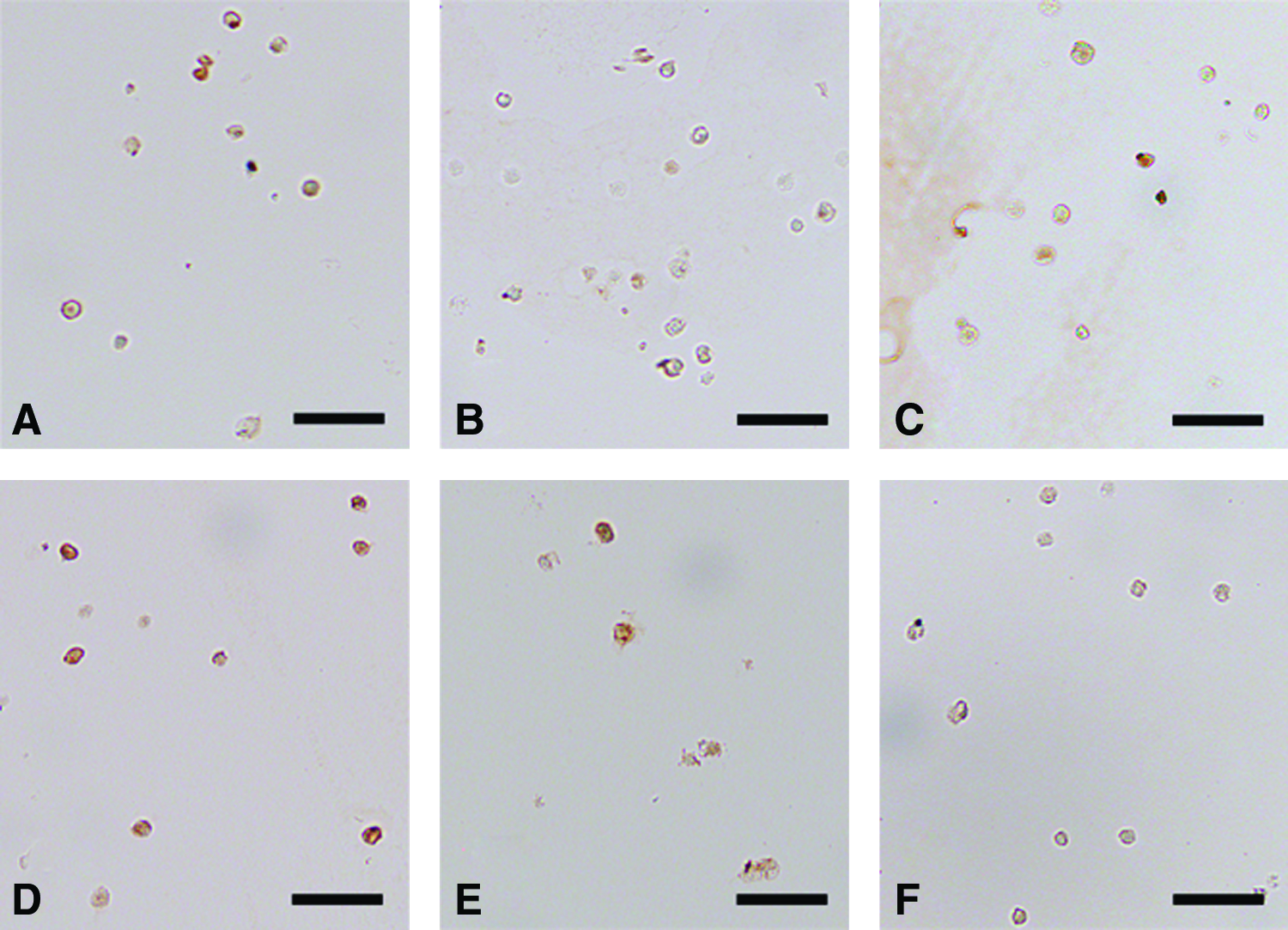
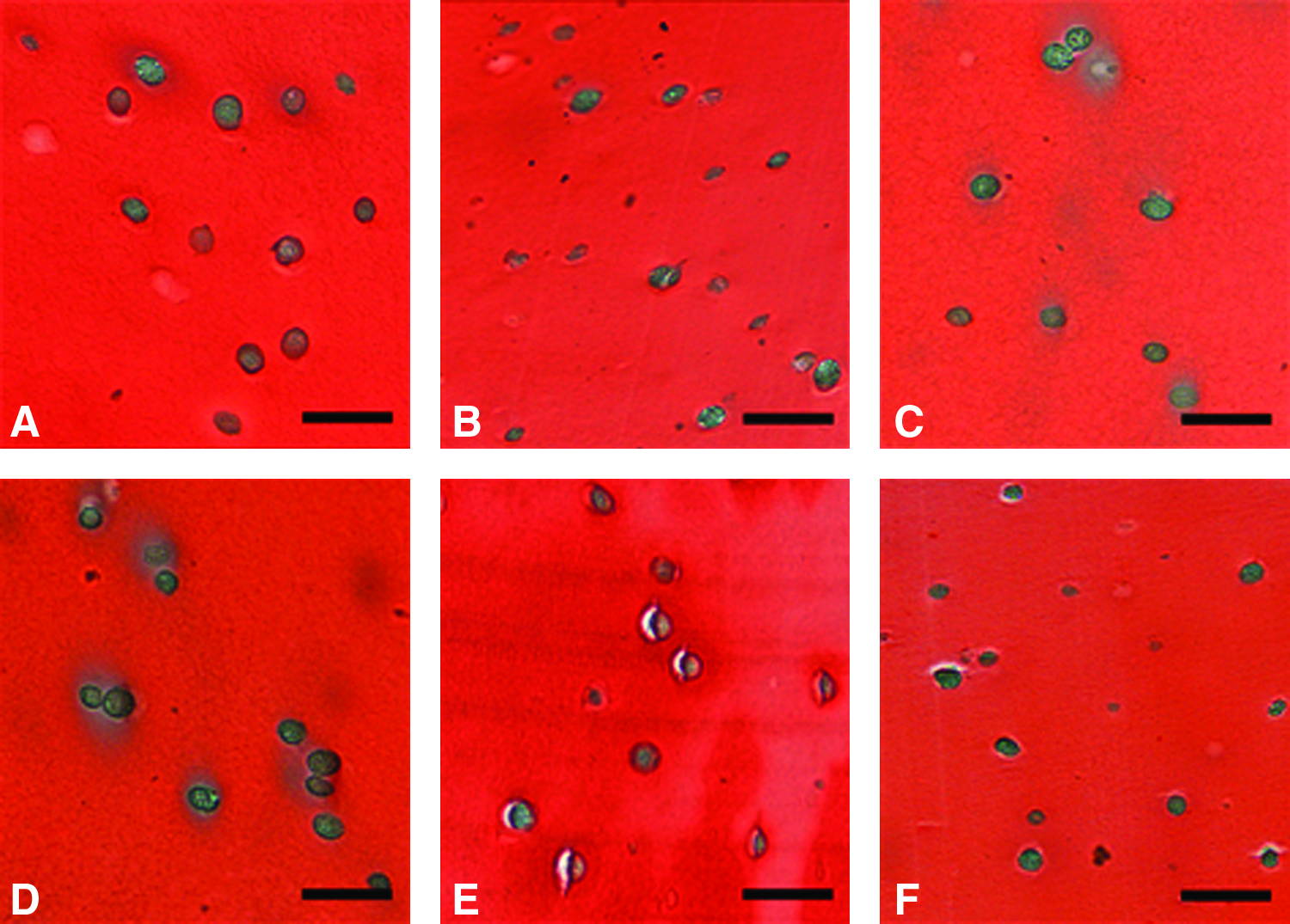
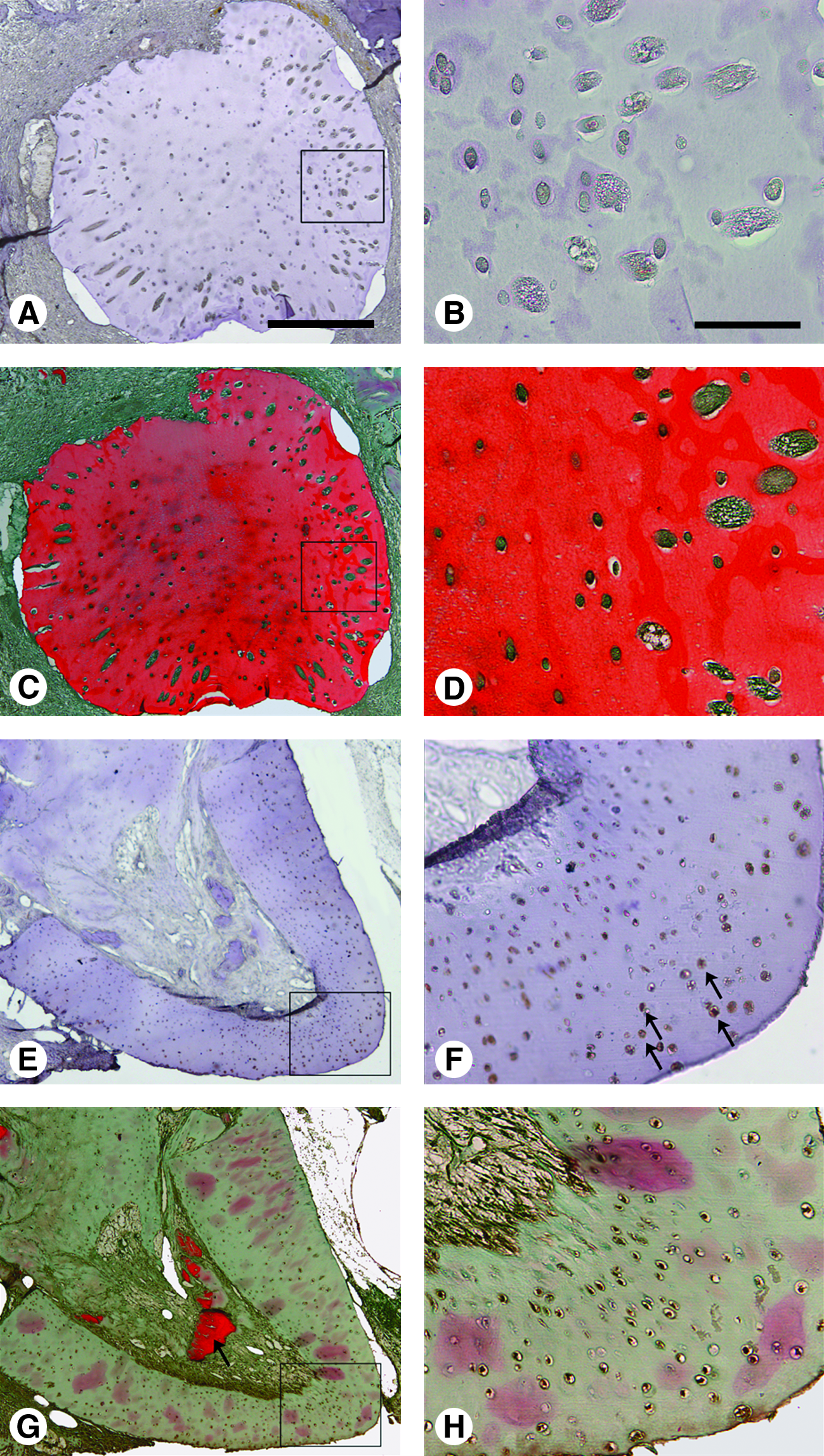
Importantly, all alginates were extensively invaded from their periphery by branches of a granulation tissue containing multinucleated giant cells, lymphocytes, and fibroblasts (Fig. 9), in marked contrast with the observations noted using empty alginate spheres (Fig. 8). There were no detectable differences at either time point between groups or between spherically intact and fragmented spheres. The bone marrow at the base of the defect contained active osteoblasts synthesizing new bone. Transplanted chondrocytes within the alginates were either viable or necrotic, without detectable differences between groups. Both the newly formed cartilage matrix and the alginate stained with safranin O, without detectable differences between groups (Figs. 10 and 11C, D). To study the survival of chondrocytes within alginate, we next examined the activity of caspase-3, a key enzyme activated in cells undergoing apoptosis. Interestingly, there was a high number of brown-colored apoptotic cells present in a safranin O-negative articular cartilage fragment that had been sheared off during implantation of the sphere, which serves as a positive control for activated caspase-3 (Fig. 11E, F). However, nearly all chondrocytes in all alginates were negative for activated caspase-3 after 3 weeks, suggesting that apoptosis played a minor role in the fate of the transplanted allogeneic chondrocytes at this time point (Fig. 11A, B).
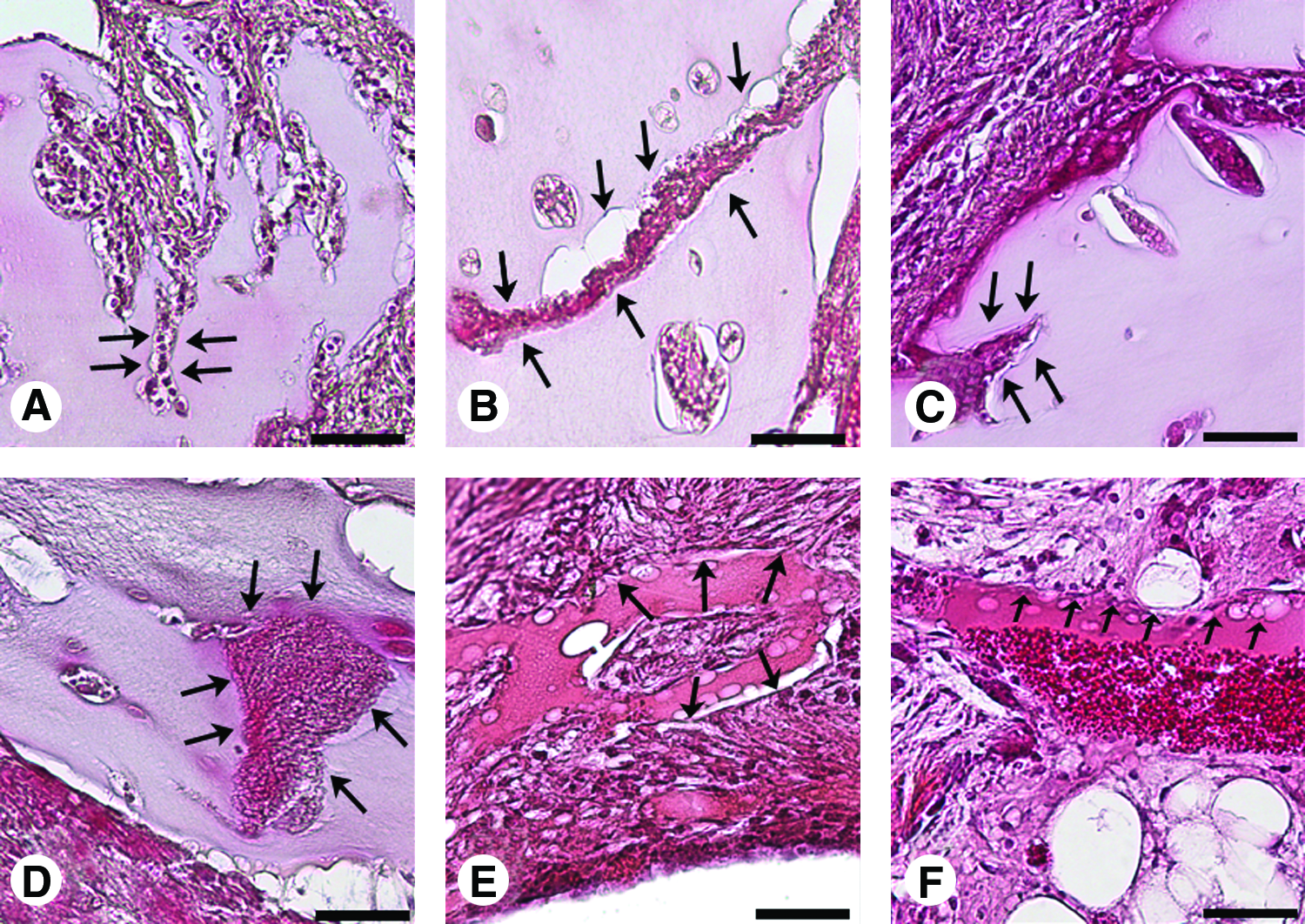
Histological analysis of representative sections (H&E staining) of the invading host tissue after 21 days in vivo following transplantation of alginate spheres with alginate-encapsulated allogeneic articular chondrocytes composed of
Histological analysis (safranin O) of representative sections of spheres composed of
Histological sections of an alginate sphere (BioMVG) with encapsulated articular chondrocytes stained with a polyclonal anti-caspase-3 IgG that detects activated caspase-3
Discussion
The rationale of this study was to systematically characterize different nonbiomedical- and biomedical-grade alginates for their capacity to support the in vitro culture and in vivo transplantation of articular chondrocytes. The most important findings are that biomedical-grade alginates contain less endotoxin and have a more regular shape, that the composition and the properties of the alginates influence cell proliferation, viability, and proteoglycan production, and that following transplantation in osteochondral defects in vivo all alginates are invaded by multinucleated giant cells and lymphocytes when carrying allogeneic articular chondrocytes.
The present findings suggest that the purification process of alginate results in a substantial decrease of the endotoxin contents. These data are in good agreement with those reported by Ponce et al. 30 and support the concept of using highly purified alginates for biomedical applications. The considerable difference in the endotoxin contents of the nonpurified alginates is probably a result of the use of different species of raw algae for isolation or of different production and purification processes. As endotoxins suppress cell proliferation, downregulate the synthesis of extracellular cartilage matrix molecules, and stimulate proteoglycan degradation,31,32 purified alginates might be more beneficial, especially for clinical applications of articular cartilage repair.
Spheres composed of purified alginates were spherically more uniform and could be prepared with a greater reproducibility than those made of nonpurified alginates. A uniform shape of the spheres, without irregularities at the surface is advantageous. 33 Under stress, for example, following transplantation into a cartilage defect, imperfections of the surface may lead to implant rupture and to the subsequent destruction of the encapsulated chondrocytes. In this respect, further studies are needed to determine the biomechanical properties of the implants. BioMVG alginate generated spheres with a defined and highly reproducible size. The diameters of all spheres increased when chondrocytes were encapsulated and ranged from 3.0 (LVM) to 3.4 mm (LVG) with the procedure employed in the present study, 34 although measuring the diameter of asymmetric spheres may result in potential inaccuracies. In comparison, microdroplets for pancreatic islet graft immunoisolation to treat diabetes are 10-fold smaller (0.3–0.8 mm). 35 For experimental cartilage repair, the size of the articular cartilage defect in the given animal model dictates the diameter of the alginate spheres. 36 Therefore, a decrease in the diameter of the implant—as observed for LVG alginate—has to be taken into account to prevent its loss. Because the size of the spheres is a critical parameter, it will be necessary to establish a routine production procedure for spheres, for example, using a microencapsulation apparatus that fulfills the needs of a quality control for clinical applications in articular cartilage repair. Moreover, to optimize the filling of the volume of a defect according to its geometry, it may be preferable to use several microspheres instead of one large sphere or to produce an alginate–chondrocyte compound directly in the desired defect shape.
The proliferation and viability of encapsulated chondrocytes over 21 days in vitro did not correlate with the type of alginate employed. Interestingly, viabilities of chondrocytes encapsulated in the biomedical-grade alginates always exceeded 90% after 3 weeks in vitro, in contrast with the declining viability of chondrocytes in nonbiomedical-grade alginates. These increased numbers of viable chondrocytes in purified alginates are higher compared with previous studies reporting viabilities between 60% and 80%37,38 and may be attributable to the lower endotoxin content. 31 Here, we encapsulated chondrocytes at a density of 106 cells/mL, approaching the mean cell density in adult human femoral (14×103 cells/mm3)39,40 and sheep articular cartilage (53×103 cells/mm3).39,40
The chondrocytes not or only slightly proliferated at this cell density in the different alginates. This is consistent with previous results and supports experimental gene transfer strategies to produce therapeutic proteins within a cartilage defect, as resting chondrocytes are capable of expressing transgenes for several weeks.41–43
Maximal proteoglycan contents on day 3 were found in LVM alginate spheres. Over the course of 21 days, only chondrocytes encapsulated in BioMVG, BioMVM, and LVG alginates produced and retained significant amounts of sulfated proteoglycans. However, a proportion of the newly synthesized proteoglycans may have been also released into the growth medium.44,45 These data suggest that LVM alginate is beneficial for short-term (3 days) proteoglycan production of articular chondrocytes, whereas LVG and BioMVM might be better suited for mid-term (3 weeks) deposition of proteoglycans. It also implies that neither the purification grade, composition, nor the viscosity plays a critical role in cell viability and matrix production of encapsulated chondrocytes.
Immunohistochemical analysis revealed that type-II collagen was expressed in vitro in encapsulated articular chondrocytes and mainly found in the cell-associated matrix, regardless whether biomedical- or nonbiomedical-grade alginates were employed. This is consistent with data from other studies and confirms that the three-dimensional alginate system supports the expression, production, and deposition of type-II collagen by articular chondrocytes.46–49 Moreover, both biomedical- or nonbiomedical-grade alginates allowed for the redifferentiation of the chondrocytes used in the present study, which had a dedifferentiated phenotype at passages 3–4 used for the experiments. Chondrocytes cultivated in monolayer rapidly lose their differentiated phenotype, which can be restored in three-dimensional alginate cultures.50,51 Such redifferentiation of articular chondrocytes is characterized by decreased cellular proliferation. 52
A major problem for the clinical use of alginate for articular chondrocyte transplantation is the reaction of the host immune system against the biomaterial and/or encapsulated allogeneic cells.
6
To our best knowledge, the biocompatibility of nonbiomedical- and biomedical-grade alginates for articular chondrocyte transplantation has not been systematically investigated to date. Previously, inflammatory reactions were noted after intraperitoneal injection of nonbiomedical-grade poly-
Most importantly, when alginate spheres contained allogeneic chondrocytes, they were invaded by multinucleated giant cells, lymphocytes, and fibroblasts, a finding in marked contrast to empty spheres, which were not subjected to such cellular invasion at any time point. This considerable difference between the invasion of spheres containing allogeneic cells and the empty spheres may be explained by the presence of necrotic cells and the absence of capillaries in the close periphery of the implants at 21 days, suggesting a suboptimal nutrition situation of the transplanted chondrocytes that might have stimulated the invasion of the granulation tissue. It is also possible that the divergences of maturity between cartilage source and implantation site might have influenced the results.59,60 Whether the invasion of the granulation tissue aims to remove the necrotic articular chondrocytes within the alginate or results from the in vitro cultivation in xenogeneic serum or their allogeneic nature remains to be determined.
Taken together, biomedical alginates contain less endotoxins, are spherically more uniform, and support the three-dimensional culture of articular chondrocytes in vitro. Spheres composed of biomedical-grade, low-viscosity, high-mannuronic acid content (BioLVM) alginate showed the smallest decrease in size over time. Biomedical-grade, low-viscosity, high-guluronic acid content (BioLVG) alginate allowed for optimal cell proliferation. Articular chondrocytes in all ultrapure alginates maintained high cell viability. Biomedical-grade, medium-viscosity, high-mannuronic acid content (BioMVM) alginate promoted the highest production of proteoglycans. Following transplantation in osteochondral defects, both biomedical- and nonbiomedical-grade alginates were surrounded by a granulation tissue. When containing allogeneic articular chondrocytes, host cells including multinucleated giant cells and lymphocytes invaded the transplanted spheres at 3 weeks in vivo, in contrast to empty spheres. Biomedical-grade, low-viscosity, high-guluronic acid content (BioLVG) alginate may be therefore applied in conditions wherein high cell numbers are needed, for example, to repopulate an articular cartilage defect. Biomedical-grade, medium-viscosity, high-mannuronic acid content (BioMVM) alginate might be used in instances wherein matrix production by encapsulated chondrocytes is of key importance. These individual characteristics of the different alginates evaluated in the present study may be valuable to tailor specific experimental and clinical strategies for cartilage tissue engineering.
Footnotes
Acknowledgments
The authors are grateful for the excellent technical assistance of Janine Becker. This study was supported by a grant from Deutsche Forschungsgemeinschaft (DFG MA 2363/1–3).
Disclosure Statement
No competing financial interests exist.
This investigation was performed at the Department of Experimental Orthopaedics and Osteoarthritis Research, Saarland University, Homburg, Germany.