
Abstract
Tracheal reconstruction is indicated in cases of malignancy, traumatic injury, and subglottic or tracheal stenosis. Recent progress in airway transplantation has provided renewed optimism for potential solutions for defects involving more than half of the tracheal length in adults or one-third of the tracheal length in children. Biologic scaffolds derived from decellularized tissues and organs have shown great promise in tracheal allotransplantation, and cyclical decellularization techniques have been hypothesized as abrogating the need for immunosuppressive therapy. In this study, we performed a direct comparison of three decellularization protocols (Protocols A, B, and C) previously described in the literature, two of which were described in tracheal tissue (Protocols A and B). We concentrated on the immunogenicity within the epithelium and mucosa, quantified and qualified the extracellular matrix (ECM) components, and performed compliance measurements on large circumferential decellularized tracheal scaffolds following cyclical decellularization techniques using all three protocols. Quantitative measurements of glycosaminoglycans (GAGs) showed a significant decrease in the mucosal component following 17 cycles of all 3 protocols as well as a significant decrease of GAGs in the cartilaginous component following cycles 1, 9, and 17 of Protocol A and cycle 17 of Protocol C. Compliance measurements were also shown to be different between the protocols, with grafts becoming more compliant at physiologic pressures after cyclical decellularization with Protocols A and B and slightly less compliant but remaining similar to native trachea using Protocol C. Positive staining for anti-major histocompatibility complex Class I (anti-MHCI) and anti-MHCII remained within the submucosal glandular components despite multiple cycles of decellularization using all three protocols. This study illustrated that there are significant differences in ECM composition and resultant structural integrity of decellularized tracheal scaffolds depending on the decellularization protocol. Protocol B was shown to maintain the GAGs components despite an increase in tracheal compliance, while Protocol C decreases GAGs components following multiple cycles, despite showing a tracheal compliance resembling that of the native trachea at physiologic airway pressures.
Introduction
When end-to-end anastomosis cannot be performed, then tracheal replacement approaches have been attempted, including the single or combined use of autologous tissues, autografts, allografts, prosthetic materials, and tissue-engineered tracheae. Unfortunately, these approaches have been met with limited success. Autogenous tissues used experimentally, such as fascia lata, pericardium, tracheal wall, and buccal mucosa with auricular cartilage as well as those used in clinical practice, such as bronchial patches, dermal grafts, pericardium, and aortic grafts have all failed due to collapse in the long term. 4 While artificial materials have been added to these tissues in order to maintain rigidity and support, they have led to local infection, anastomotic dehiscence, vascular erosion and granulation tissue formation, and eventual stenosis. 2 Local, regional, and distant free flaps require lengthy, multistage procedures and are, therefore, not feasible in cancer treatment. 4
The goal of decellularization techniques is to remove cells and nuclear material from the organs and tissues and to keep the complex mixture of structural and functional proteins that constitute the extracellular matrix (ECM) intact. 3 Components of the ECM, such as collagens, laminins, and polysaccharides, are generally conserved among species and are thought to be well tolerated even by xenogeneic recipients. 1 Consequently, biologic scaffolds derived from decellularized tissues and organs have been used in various animal studies and clinical applications, as they are thought to stimulate tissue regeneration and regulate cell behavior without producing an inflammatory response. 3
The first clinical transplantation of a decellularized human trachea was performed in 2008. A donor trachea was initially decellularized using multiple cycles of a protocol involving a detergent-enzymatic reaction. 6 This group focused on the cartilaginous components and, despite the cells remaining within the cartilage of the donor trachea following multiple cycles of decellularization, the trachea was deemed nonimmunogenic using immunostaining for major histocompatibility complex (MHC) Class I and MHC Class II.
In this study, we focused on the epithelium and submucosal glands, as they are well known as dominant immunogenic components within the native trachea.7–9 More specifically, we examined the efficacy of cyclical decellularization methods in reducing the immune potential of decellularized tracheal scaffolds. We also aimed at examining other clinically relevant characteristics of tracheal function such as compliance and collapsibility, as very little is known about their preservation in bioengineered constructs and/or tracheal allografts. In addition, we qualified and quantified the ECM components within these decellularized tracheal scaffolds. Finally, we compared and evaluated three decellularization protocols, all of which differ in the nature of the chemicals used, their respective concentrations, and the total treatment duration, in order to elucidate which is the most appropriate for further evaluation in the transplantation of large circumferential tracheal segments.
Materials and Methods
Tracheal harvesting
Tracheae were harvested from male Yorkshire pigs (40–50 kg). All animals received humane care in compliance with the “Principles of Laboratory Animal Care” formulated by the National Society for Medical Research and the “Guide for the Care of Laboratory Animals” published by the National Institutes of Health. The Animal Care Committee of the Toronto General Research Institute approved all the studies. The tracheal grafts were randomly assigned to undergo decellularization using multiple cycles of one of the three different protocols. Tracheal grafts (n=15) measuring 9 cm in length were randomized to undergo compliance measurements before and after decellularization cycles. Tracheal grafts of variable lengths (n=15) were used for histology, immunohistochemistry, and biochemical assays. All grafts remained in tubular form during decellularization and were neither cut nor divided into smaller pieces.
Decellularization protocols
Three different protocols described in the literature were used for tissue decellularization. Two of the protocols (A and B) had been used for decellularization of tracheal tissue, and protocol C had been used for bladder tissue.
Protocol A
Protocol A had been initially described by Meezan et al. in 1975 for the isolation of morphologically and chemically pure basement membranes from several tissues. 10 It was later utilized by Macchiarini et al. for the first clinical tracheal transplantation. 6 Their animal work focused on the structural and morphologic evaluation of this tissue-engineered tracheal tubular matrix, which was decellularized using a detergent-enzymatic reaction. 11 They showed that 17 cycles of decellularization resulted in loss of MHCI and MHCII staining. The protocol originally described in their animal model involves rinsing circumferential tracheae for four times (for 4 h each) in phosphate-buffered saline (PBS containing 1% antibiotic and antimycotic solution). Tissue was then processed with multiple treatment cycles, including the following steps: Tissue was stored in Aqua milliQ for 48 h at 4°C and then incubated in 4% sodium deoxycholate (Sigma) for 4 h and 2000 KU of DNase-I (Sigma) in 1 M NaCl for 4 h. This process was repeated and performed for 17 cycles.
Protocol B
Protocol B had been used for xenogeneic tracheal reconstruction of a noncircumferential tracheal defect. 12 It was adapted from the original protocol 13 to a hydrated form, as it allowed for better re-epithelialization. Each circumferential trachea was subjected to 48 h immersion in 3% Triton X-100 solution at 4°C on a mechanical shaker, changing the solution after 24 h. After 48 h, a 0.1% peracetic acid, 4% ethanol, and 96% deionized water (diH2O) wash was administered for 2 h at 300 rpm on a mechanical shaker to decellularize and disinfect the tissue. The tracheae were then rinsed for 15 min in 0.9% NaCl and diH2O on a mechanical shaker to remove residual solutions. The published protocol involves only one cycle. For the purpose of assessing the effect of cyclical decellularization and to compare it with Protocol A, the process was repeated and performed for 17 cycles.
Protocol C
Protocol C had been used for acellular bladder matrix 14 and was later adapted by Brown et al. 15 Circumferential tracheae were washed separately in sterile phosphate-buffered solution (PBS) and then stirred on a mechanical shaker in a hypotonic solution of 10 mM Tris HCl, pH 8.0, 5 mM ethylenediaminetetraacetic acid (EDTA; Sigma), 1% Triton X-100 (Sigma), PefablocPlus™ (protease inhibitor; Sigma) 0.1 mg/mL, and antibiotics/antimycotic at 4°C for 24–48 h to lyse all cellular components. Tissue was placed in a hypertonic solution containing 10 mM Tris HCl, pH 8.0, 5 mM EDTA, 1% Triton X-100, and 1.5 M KCl and stirred for 24 h at 4°C to denature residual proteins. Tissue was then washed in Hank's Balanced Salt solution for 30 min on a shaker at room temperature four times before an overnight enzymatic digestion with 2 U/mL of benzonase (DNAse/RNAse; Sigma) at room temperature. A final 48 h extraction was performed at 4°C in 50 mM Tris HCl, pH 8.0, 0.25% CHAPS, 1% Triton X-100, and antibiotics/antimycotic with shaking. The tracheae were finally washed four times in sterile diH2O at 4°C. The published protocol involves only one cycle. For the purpose of assessing the effect of cyclical decellularization and to compare it with Protocol A, the process was repeated and performed for 17 cycles.
A single cycle of Protocol A or B lasts 48 h and, therefore, ∼35 days is required for 17 cycles. One cycle of Protocol C lasts about 5–7 days, and, therefore, more than 3 months is required for 17 cycles.
Histology and immunohistochemistry
Sections of native and decellularized (following cycles 1, 9, and 17) tracheae were fixed in 10% neutral buffered formalin and prepared for paraffin processing. Five micron sections were cut and stained with hematoxylin and eosin (H&E) to evaluate removal of cellular material. Elastin and collagen content in the native and decellularized grafts was qualified by using Verhoeff's elastin stain and Masson's trichome stain, respectively.
The presence of MHC markers was immunohistochemically evaluated using ABC elite (Vector Labs) detection kits for anti-rabbit MHCI (EP1395Y; Abcam) and anti-mouse MHCII (OX4; Abcam). Briefly, proteinase K (Roche) was used for antigen retrieval; nonspecific binding was blocked using goat serum, and the sections were incubated overnight at 4°C in the primary antibody at a dilution of 1:100. A nonspecific rabbit IgG (Vector Labs) and nonspecific mouse IgG (Vector Labs) at the same concentrations as the primary antibodies served as negative controls. A biotin-conjugated antibody at a dilution of 1:200 served as a secondary antibody and was applied for 1 h at room temperature. The Avidin-Biotin Complex was then applied for 30 min, and final staining was performed with dimanobenzidine as a chromogen for 10 min and counterstained with hematoxylin before serial alcohol and xylene dehydration and cover slipping.
Biochemical assays
The amount of glycosaminoglycans (GAGs) within native and decellularized tracheae was quantified using a Blyscan Sulfated Glycosaminoglycan assay kit (Biocolor; B1000) as per the manufacturer's instructions and as described in the literature. 12 Briefly, 50 mg samples of intact trachea, isolated tracheal mucosa, and isolated tracheal cartilage from both native and decellularized tracheae were obtained. Samples were incubated at 37°C on a rocker plate in 2.5 mL Pronase buffer (1.5 mg/mL Type XIV Protease, 0.1 M Tris [pH 7.5], and 10 mM CaCl2) for 48 h with vortexing after 12 h. The digested samples were then centrifuged at 1000 rpm for 10 min, and 25 μL of supernatant from each sample was aliquotted to 1.5 mL Eppendorf tubes, to which 75 μL diH2O was added. One milliliter Blyscan dye reagent was added to each tube, and the tubes were stirred at 300 rpm for 30 min at room temperature. The tubes were then centrifuged at 20,000 rpm at room temperature for 10 min, the supernatant was removed, and 1 mL of dissociation reagent was added to each tube. After vortexing, the tubes were left at room temperature to react for 15 min, vortexed again, and left to react for an additional 15 min. Three sets of 200 μL aliquots were placed into a transparent 96-well plate, the absorbance was measured at 656 nm, and the results were compared with the standard curve.
Compliance measurements
To assess tracheal structural integrity in the most physiologically relevant fashion, a novel assessment technique was developed. Tracheal segments were standardized at a length of 9 cm (n=15) and sealed at both ends (Fig. 6). One end was fixed (Fig. 6, green arrow) and the other was connected to plastic tubing, a three-way stop cock (Fig. 6, blue arrow), and a 60 cc syringe. A second set of plastic tubing (Fig. 6, orange arrow) was placed in a water bath, and each milliliter of volume extracted from the syringe correlated with the height of water displaced from the water bath to determine the pressure within the system. This device was placed in a micro-computed tomography (CT) scanner, and axial images showing the luminal area were taken at each negative pressure until complete tracheal collapse was achieved. Tracheae were also inflated with air at various positive pressures until bending of the trachea no longer permitted further inflation. Tracheal collapsibility and compliance were measured before and after decellularization using the three decellularization protocols. Pressure measurements were correlated with water displacement (cm H2O) within a water bath. Volume was measured by calculating the intraluminal area, using ImageJ, from axial images obtained using a micro-CT scanner over a 6 cm tracheal length. At each pressure measurement, the total intraluminal volume was calculated by adding serial volumes measured on the CT scans using the Image J program. Forty measurements at each 150 μm of tracheal length were taken beginning at the middle of the trachea and moving toward both ends. All measurements were added to account for the total intraluminal volume over a 6 cm tracheal length. Each trachea served as its own control, and measurements were performed on native tracheae and following cycles 1, 9, and 17 of decellularization using one of three protocols.
Scanning electron microscopy
Intact, isolated mucosa and isolated cartilage of both native and decellularized tracheal samples (following cycle 1) were fixed with 4% paraformaldehyde and 1% glutaraldehyde in 0.1 M phosphate-buffered solution (PBS) at a pH of 7.2 for 1 h. Samples were then washed with 0.1 M PBS at a pH of 7.2, thrice for 30 min per wash. Samples were then postfixed with 1% osmium tetraoxide buffered in 0.1 M PBS at pH 7.2 for 1 h. After postfixation, the samples were washed with distilled water, twice, for 30 min. The samples were dehydrated using serial ethanol dilutions of 25% twice for 15 min, 50% twice for 30 min, 70% twice for 30 min, 90% twice for 1 h, and 100% two times for 1 h and then left in 100% ethanol overnight at 4°C. They were then critical point dried (Tousimis Autosamdri 810) with a purge phase of 30 min. Tracheal samples were then mounted with carbon colloid paint on scanning electron microscope stubs, gold-palladium sputter coated for 2 min on a Polaron SC7640 Sputter Coater (Quorum Technologies), and then imaged at 5 kV on a Hitachi scanning electron microscope S-3400 (Hitachi High-Technologies Canada, Inc.).
Statistical analysis
Statistical analysis was performed using GraphPad Prism 5.0 statistical software (San Diego). Decellularized groups were compared with a native control using Dunnett's multiple comparison test analysis of variance. A p-value of <0.05 was considered significant.
Results
Histology and immunohistochemistry
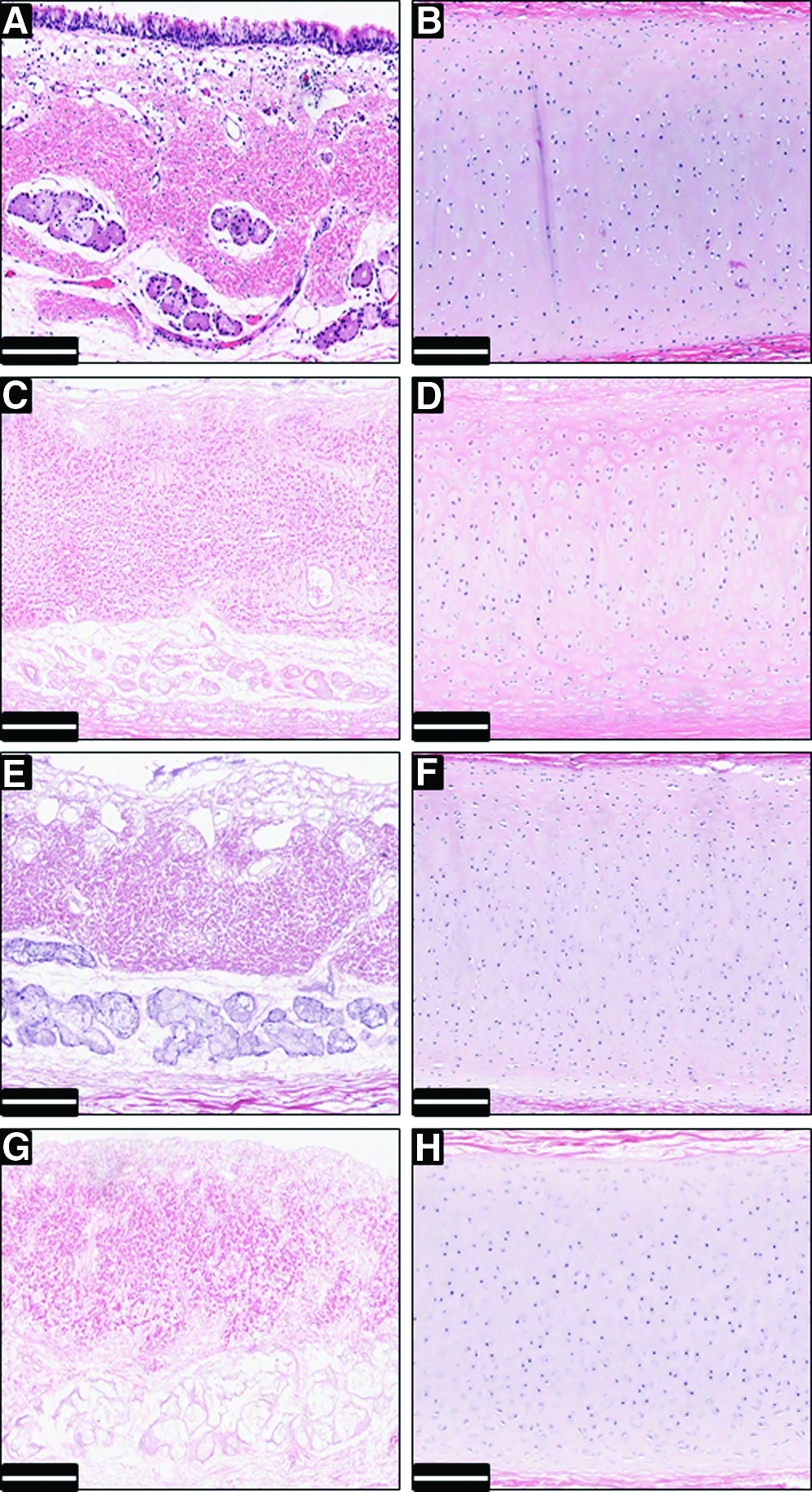
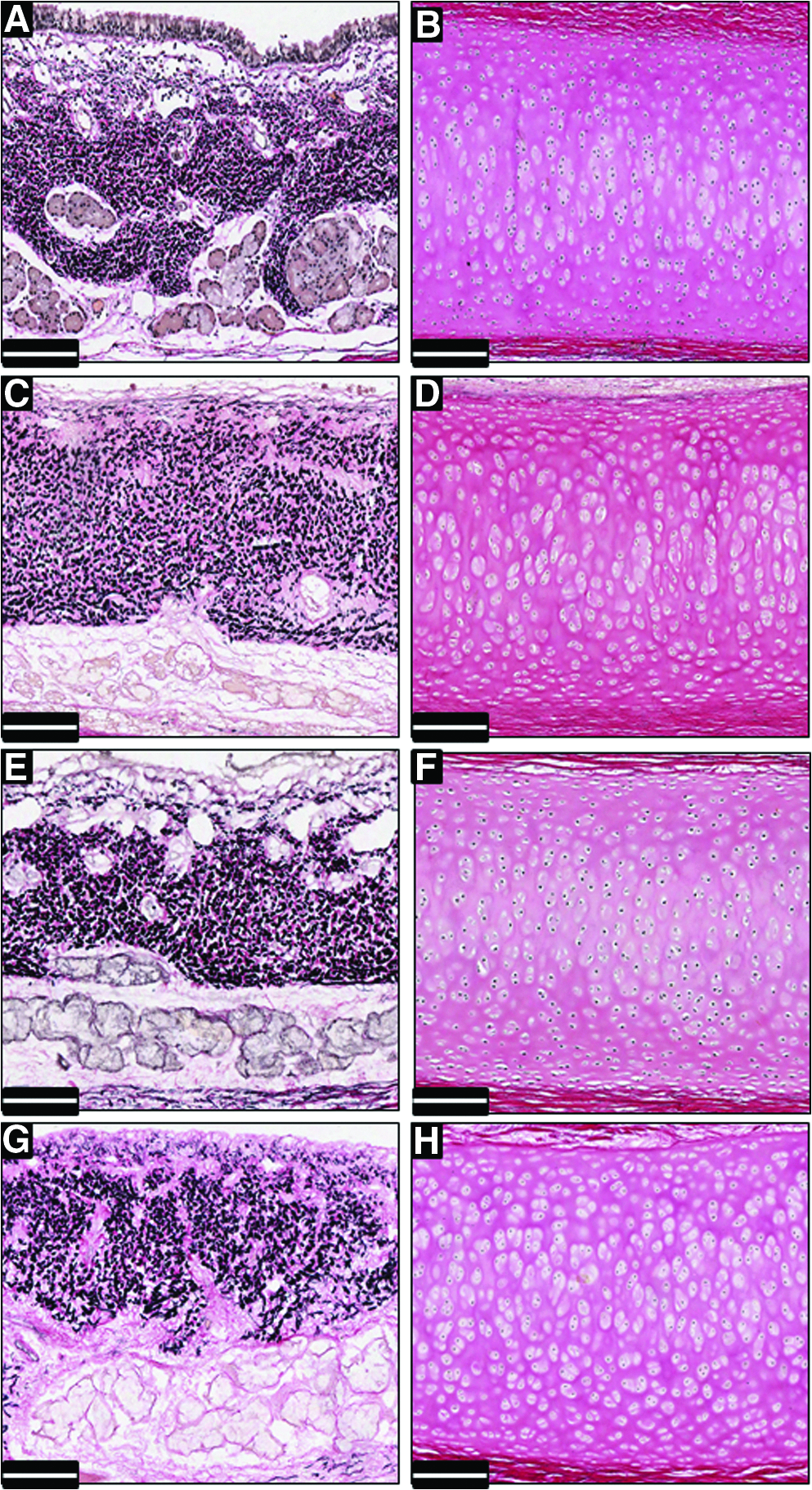
An ideal decellularization protocol removes all cellular and nuclear material while leaving the ECM components intact. The three decellularization protocols were compared by H&E to look at tracheal morphology as well as the presence or absence of nuclear material. Native pig tracheae displayed a pseudostratified ciliated epithelium, a submucosa containing mixed glands and smooth muscle (Fig. 1A), and hyaline cartilage (Fig. 1B). Sections that were decellularized using Protocol A, B, and C were assessed following 1, 9, and 17 cycles of decellularization. Following cycle 17 of decellularization, there is a loss of the epithelium as well as a loss of nuclear material from within the submucosa using Protocol A (Fig. 1C), Protocol B (Fig. 1E), and Protocol C (Fig. 1G). The nuclear material is not removed and remains within the hyaline cartilage following 17 cycles of decellularization using all 3 protocols (Fig. 1D, F, H). Qualitative assessment of collagen and elastin was performed using Masson's trichome stain and Verhoeff's elastin stain. Compared with native trachea (Figs. 2A, B and 3A, B), both collagen (blue staining) and elastin (punctate black staining) are maintained within the submucosa following 17 cycles of decellularization using all 3 protocols (Figs. 2C, E, G and 3C, E, G). Similar to native trachea (Figs. 2B and 3B), the cartilage also stains positive for Masson's trichrome following cyclical decellularization techniques (Fig. 2D, F, H) but not for elastin (Fig. 3D, F, H). The histology clearly shows that all protocols completely remove the epithelium and the nuclear material from the mucosa but are unable to penetrate the hyaline cartilage. Some of the ECM components, such as collagen and elastin, are not qualitatively affected by either of these protocols.
Hematoxylin and eosin staining of native trachea

Masson's trichrome staining of the native trachea
Elastin staining of native trachea
Cyclical decellularization techniques have been hypothesized to reduce the immunogenic potential of decellularized grafts.6,11 We, therefore, performed immunohistochemistry looking at anti-MHCI and anti-MHCII staining following cycles 1, 9, and 17 of decellularization and compared it with the native trachea. Immunohistochemistry for anti-MHCI shows positive staining for all cells within the epithelium and the submucosal glands with very little staining within the cartilage (Fig. 4A). Immunohistochemistry for anti-MHCII shows positive staining for some cells within the epithelium and surrounding the submucosal glands with no positive staining within the cartilage (Fig. 4B). All isotype controls showed a lack of positive staining in the mucosa and the cartilage (figures not shown). Following 17 cycles of decellularization using Protocol A (Fig. 4C, D), Protocol B (Fig. 4E, F), and Protocol C (Fig. 4G, H), cells within the submucosal glands continue to stain positive for anti-MHCI and to a lesser degree for anti-MHCII, although the morphology of these glands appears to have changed, not resembling that of the native trachea. Higher cycles were also evaluated (over 17—figures not shown) and continued to show similar staining within the submucosal glands. Thus, despite the hypothesis that cyclical decellularization techniques have a potential to render tracheal scaffolds nonimmunogenic, we clearly show that at the protein level, there continues to be anti-MHCI and anti-MHCII staining within the glandular components.
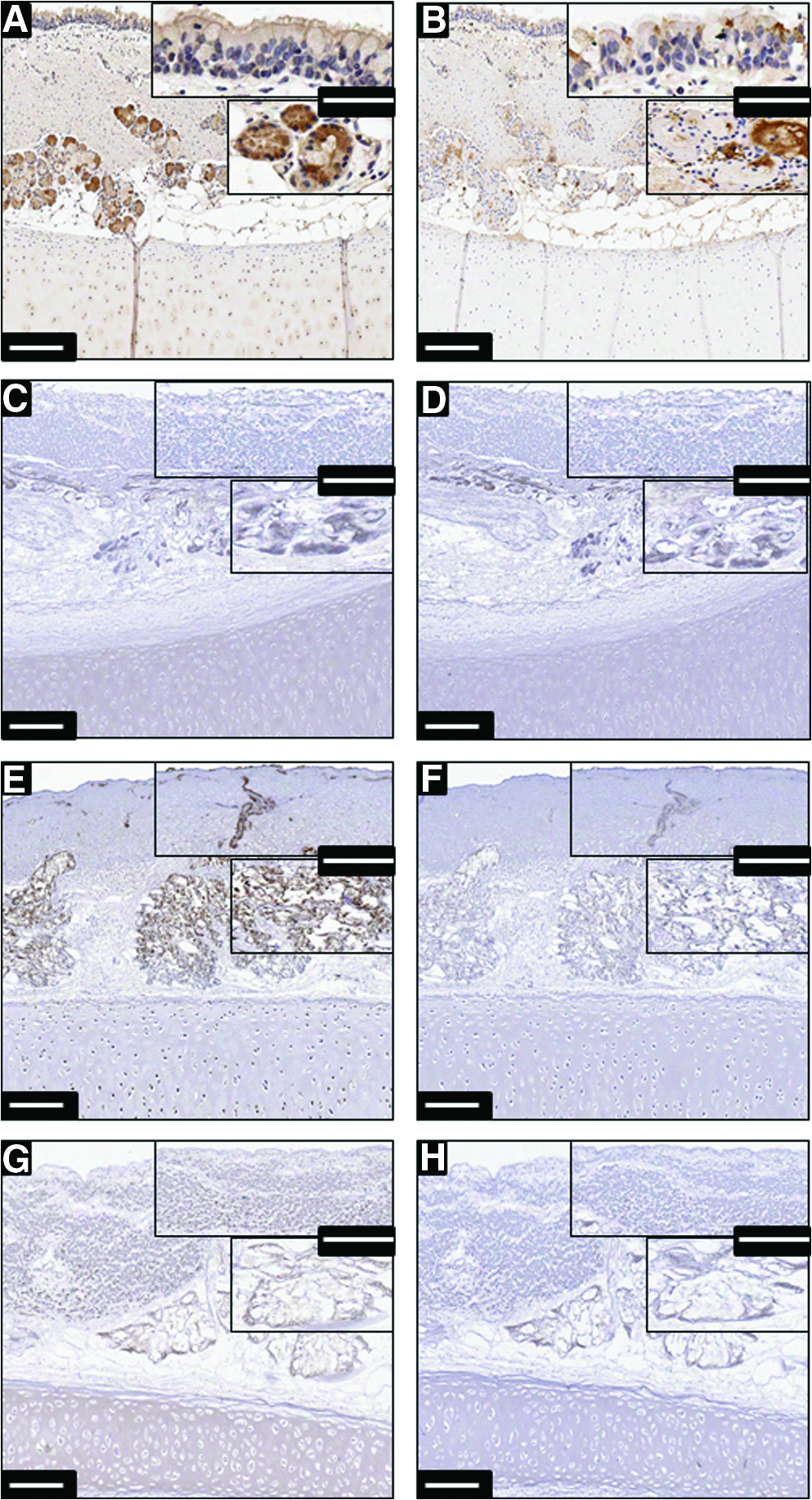
Immunohistochemistry of anti-major histocompatibility complex Class I (anti-MHCI)
Biochemical assays
GAGs, representing the largest component of the ECM, were quantified in both the mucosal (Fig. 5A) and cartilaginous (Fig. 5B) components of decellularized tracheal allografts following cycles 1, 9, and 17 using all three protocols. Compared with the native control, there was a significant loss of GAGs content within the mucosal components following 17 cycles of decellularization using all 3 protocols. Protocol B maintains GAGs within the cartilaginous component following cycles 1, 9, and 17. The GAGs content within the cartilage significantly decreases following cycles 1, 9, and 17 of Protocol A and cycle 17 of Protocol C when compared with the native control. Interestingly, this decrease in GAGs content has the potential to affect the function of tracheal scaffolds, which we proceeded to further evaluate.
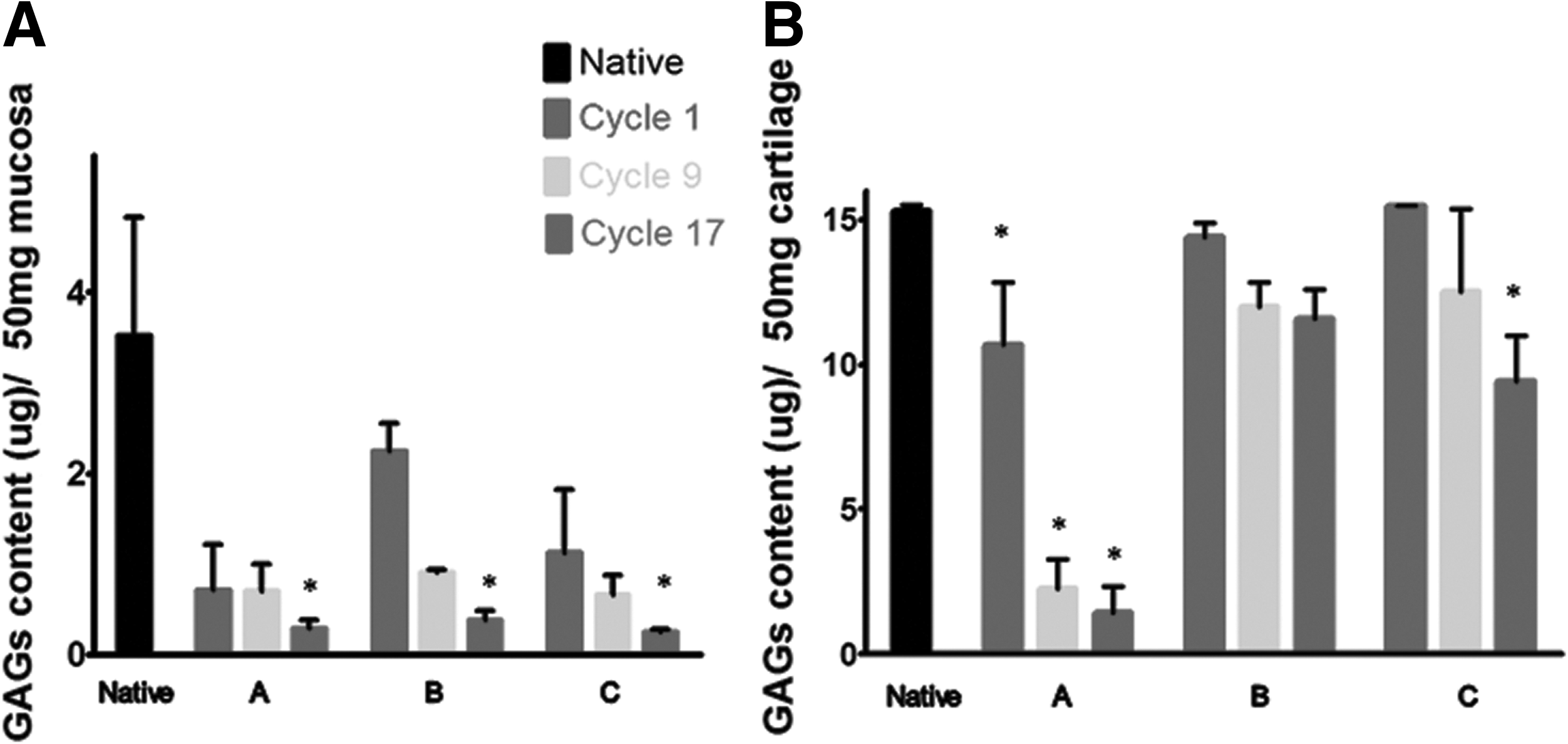
Glycosaminoglycans (GAGs) content was measured within the mucosal
Compliance measurements
We clinically analyzed relevant parameters and developed a novel device (Fig. 6A) that allows the measurements of tracheal collapsibility and compliance before and after decellularization. When compared with the native tracheae, which appear to be completely collapsed at pressures close to −100 cm H2O, tracheae decellularized using Protocol A collapse more readily between pressures of 0 and −50 cm H2O following cycles 1, 9, and 17 of decellularization (Fig. 6C). Tracheae decellularized using Protocol B collapse more readily between pressures of 0 and −50 cm H2O following cycles 1, 9, and 17 and expand more readily than native tracheae when positive pressure is exerted. Resting volume is also decreased following multiple cycles of decellularization (Fig. 6D). As for Protocol C, the intraluminal volume also decreases more readily following cycle 9 but not cycles 1 and 17 of decellularization. The tracheae, however, appear to completely collapse at pressures similar to those of native tracheae. When positive pressure is exerted, the tracheae also expand more readily than native tracheae following cycles 9 and 17 of decellularization (Fig. 6E). Compliance measurements show that at clinical ranges of tracheal pressures (−81.6 cm H2O to 13.6 cm H2O), Protocols A and B show a decrease in tracheal volume compared with native trachea. These measurements of tracheal collapsibility and compliance are clinically important and show that selecting an appropriate decellularization protocol is critical in preventing restenosis of the airway after transplantation.

A novel approach was used to measure tracheal compliance
Scanning electron microscopy
To further assess the morphology of decellularized tracheal allografts, scanning electron microscopy (SEM) was performed by comparing them with native trachea. Mounts of isolated native mucosa (Fig. 7A) show the presence of cells within the epithelium. Higher magnification of the cartilage shows the collagen bundles and other ECM components (Fig. 7B). Interestingly, following cycle 1 of decellularization, the luminal surface is shown to be very irregular and nonuniform with differences existing between all three protocols. The luminal surface following protocols A, B, and C (Fig. 7C, E, G) appears to be desquamated and depleted of epithelium. Collagenous and ECM bundles within the decellularized cartilage also appear to differ from native trachea (Fig. 7D, F, H). Protocol A appears to have a rough and irregular surface topography in comparison to the more uniform surface topography present in the native mucosal sample (Fig. 7C). The cartilage appears to have been denuded and appears to have lost the dense, tight, and cohesive ECM bundles characteristic of native cartilage (Fig. 7D). Protocol B gives rise to rounded surface topographical markers with pronounced areas where fibrous components of ECM are visible (Fig. 7E). The collagenous bundles and ECM appear to have been eroded in comparison with protocols A and C as seen in the lack of ECM bundles. The uniformity of the surface topography also appears to have changed (Fig. 7F). Protocol C is different from other protocols in that the luminal surface appears much smoother and rounded in terms of surface topographical features and is uniform in height (Fig. 7G). The cartilage of Protocol C has large bundles of collagen, some of which appear to have the wave like characteristics of native trachea; however, the smaller collection of ECM fibers that aggregate together have been destroyed, and only large bundles of ECM seem to have remained following the decellularization process (Fig. 7H).

Scanning electron microscopy of native
Discussion
The literature dealing with the concept of tissue decellularization implies that maintaining the native three-dimensional architecture of the ECM is essential in maintaining the function of the organ, but that full decellularization is necessary to prevent immune and inflammatory reactions. As such, the most robust and effective decellularization protocols include a combination of physical, chemical, and enzymatic approaches. The efficiency of a given decellularization method or protocol is, however, dependent on the tissue of interest. 3
The three decellularization protocols used in this article differ in the properties of their components. Protocol A, used in the first clinical transplantation of a decellularized airway, uses an ionic detergent in combination with an enzymatic reaction and a hypertonic solution. Previous publications regarding this protocol have reported the use of multiple cycles (17 cycles) for decellularization. Protocol B, used for xenogeneic patch tracheoplasty, combines a nonionic detergent with an acid and a hypertonic solution that removes the remaining cellular debris. Protocol C, used for generating acellular bladder matrices, employs a nonionic detergent, at a lower concentration than Protocol B, in combination with enzymes, hypotonic and hypertonic solutions, and chelating agents that penetrate and solubilize the cellular contents, thereby decellularizing the tissue. Both Protocols B and C were published as 1 cycle of decellularization; however, for the purpose of comparison, the scaffolds were evaluated up to 17 cycles. Knowing that these three protocols differ profoundly in their composition, it is not surprising that our hypothesis was supported, and differences were found in tracheal scaffolds following these protocols.
The components of the ECM, the interstitial matrix, and the basement membrane provide structural support to organs and tissues. They also play important roles in the support and anchorage of cells, segregating tissues, regulating intercellular communication, sequestering growth factors, and are essential for tissue growth, wound healing, and fibrosis. 16 In this article, we qualitatively assessed the presence of several ECM components such as collagen and elastin and found them to be maintained even after 17 cycles of decellularization using all 3 protocols. However, when we measured GAGs, which are bound to proteoglycans using a biochemical assay, there was a significant decrease in the mucosal GAGs content using all 3 protocols following 17 cycles. Compared with the native trachea, there was also a significant decrease in the GAGs within the cartilage even after a single cycle of decellularization using Protocol A. Interestingly, Protocol B maintained GAGs within the cartilage despite cyclical decellularization, while Protocol C showed a significant decrease only after 17 cycles.
All three protocols adequately removed the epithelium and the nuclear material from within the mucosa following cycles 1, 9, and 17 of decellularization. Similar to previously described literature, nuclear material remained within the cartilage.6,12 The clinical relevance of this would appear to be minimal, as cartilage is thought to lack MHC complexes. 17 However, the extent of the inflammatory response to the remaining nuclear material within the cartilage has yet to be established in vivo. As described in the literature, we showed that native trachea stains positively for MHCI and MHCII in the epithelium and submucosal glands.18,19 Previous reports have shown that anti-MHCII staining is lost following 17 cycles of decellularization but concentrated mainly on the cartilaginous components of the trachea. 6 Decellularized tracheal scaffolds were shown to stain positively for both MHCI and MHCII in the submucosal glandular components even following multiple cycles of decellularization and using all three protocols. This suggests that these tissue-engineered scaffolds may not be entirely nonimmunogenic, and recipients should be carefully monitored for rejection.
Due to the shape of the trachea and, more specifically, the incomplete cartilaginous rings, the trachea is an asymmetric and anisotropic structure with nonlinear mechanical properties. Previous studies have assumed a linear elastic material and have treated the trachea as a symmetric structure. Studies evaluating these nonlinear mechanical properties of the trachea have found that treating it as a linear material can cause large deviations in predicting the compliance.20,21 Although these mechanical parameters were measured in native and immature airways using different devices, very little is known about the preservation of these characteristics in bioengineered constructs and tracheal allografts. Therefore, we looked at assessing tracheal collapsibility using a novel device measuring tracheal volume and pressure. At pressures simulating physiologic breathing, we found that compliance increases using Protocols A and B but decreases slightly using Protocol C. It is clinically important to evaluate these parameters and the differences between protocols, as they will likely affect the behavior of decellularized tracheal allografts after implantation. Tracheae with a higher compliance will likely be at a higher risk for tracheomalacia and potentially even postoperative stenosis. Tracheae with significantly lower compliance are stiffer and might lead to granulation tissue due to lack of flexibility at the anastomosis.
We found no clear relationship between loss of GAGs and changes in structural integrity, with Protocol A showing a significant decrease in GAGs within the cartilage and an increase in compliance, while Protocol B showed an increase in compliance despite maintaining the GAGs content. The biomechanical properties of cartilage are considered to result from its structure as a fiber-reinforced composite in which collagen fibers provide tensile stiffness and entrap large aggregates of hydrophilic proteoglycans. 22 We speculate that the mechanical integrity and tracheal compliance is likely not solely due to the loss of GAGs within the cartilage but possibly due to a disturbance in the protein-protein interactions affected by decellularization. As such, the reagents used in Protocols A and B are likely to impact both the GAGs (chondroitin-sulfate) and Type II collagen within the hyaline cartilage, and this has a direct effect on tracheal compliance. The detergent used in Protocol A (sodium deoxycholate) is more potent in its ability to also remove the GAGs content. We also speculate that the combination of different reagents and enzymes used in Protocol C, which increases the packing density of the detergents, has the ability to preserve these interactions, the three-dimensional structure, and, therefore, maintain tracheal compliance.
Furthermore, little work has been done that rigorously characterizes and analyzes the micro- and nano-topography of the tracheal matrix. Scanning electron micrographs revealed dramatic differences between the morphology and topography of native trachea compared with decellularized scaffolds. When comparing different decellularization protocols, differences in roughness, roundness, and density of the ECM and uniformity of surface topography were also found. Conconi et al. 23 described dual-decellularization techniques of tracheal matrices. Similarities were found in their detergent-enzymatic method and our Protocol A in terms of roughness of the ECM and pot-hole marked topography after 48 h of treatment. Comparisons to their second method, the Herberhold method, reveal that our three methods do less damage, demonstrated by the relative smoothness and lack of discernible surface features in some parts of the matrix. In comparison to cartilage matrix in articular cartilage, it appears that porcine tracheal cartilage has a similar arrangement to human cartilage.24,25 The porcine tracheal cartilage as shown in our SEM images lacks the defined and repeatable groove formations seen in rabbit, sheep, and rat articular cartilage.
In conclusion, this article confirms that all three protocols maintain collagen and elastin. One of the major differences between the protocols lies in the maintenance of the GAGs components with Protocol A causing the most significant decrease in both the mucosal and cartilaginous components. The second major difference lies in the ability to maintain the functional integrity of these grafts—both Protocols A and B cause an increase in compliance, while Protocol C, despite causing a slight decrease in compliance, appears to be more comparable to the native trachea. Identification of the ideal decellularization protocol, where there is minimal tracheomalacia and no undue rigidity, remains an important challenge in the field. Positive staining for MHCI and MHCII, which remained specifically in the submucosal gland compartment following 17 cycles, using all 3 protocols allows us to conclude that cyclical decellularization is not yet complete for removing the immune potential of large circumferential tracheal scaffolds. We would also recommend that future work particularly addresses the submucosal gland compartment.
Footnotes
Disclosure Statement
No competing financial interests exist.