
Abstract
The development of in vitro culturing techniques for osteoblastic differentiation of human mesenchymal stem cells (hMSC) is important for cell biology research and the development of tissue-engineering applications. Dexamethasone (Dex) is a commonly used supplement, but the optimal use of Dex treatment is still unclear. By adjusting the timing of Dex supplementation, the negative effects of long-term Dex treatment could be overcome. Transient Dex treatment could contribute toward minimizing broad donor variation, which is a major challenge. We compared the two most widely used Dex concentrations of 10 and 100 nM as transient or continuous treatment and studied inter- and intraindividual variations in osteoblastic differentiation of hMSC. Characterized bone marrow-derived hMSC from 17 female donors of different age groups were used. During osteoblastic induction, the cells were treated with 10 or 100 nM Dex either transiently for different time periods or continuously. Differentiation was evaluated by measuring alkaline phosphatase (ALP) activity and staining for ALP, von Kossa, collagen type I, and osteocalcin. Cell proliferation, cell viability, and apoptosis were also monitored. The strongest osteoblastic differentiation was observed when 100 nM Dex was present for the first week. In terms of inter- and intraindividual coefficients of variations, transient treatment with 100 nM Dex was superior to the other culture conditions and showed the lowest variations in all age groups. This study demonstrates that the temporary presence of 100 nM Dex during the first week of induction culture promotes hMSC osteoblastic differentiation and reduces inter- and intraindividual variations. With this protocol, we can reproducibly produce functional osteoblasts in vitro from the hMSC of different donor populations.
Introduction
The differentiation of hMSC into functional osteoblasts in vitro requires suitable inductive factors at appropriate concentrations, time points, and durations.4,9 The basic protocol with organic phosphate and ascorbic acid is well established. A frequently used supplement is the synthetic glucocorticoid dexamethasone (Dex), which is known to regulate the osteogenesis of hMSCs and mineralization in vitro.10–15 The exact mechanisms of action of Dex are still poorly defined, but Dex seems essential for the full differentiation of hMSCs into mineral-producing osteoblasts.10–16 Dex mediates its effects not only by its specific influence on gene transcription,7,17–21 but also by interfering with other signaling pathways, indirectly affecting gene transcription. 10 Dex is also a stimulator of hMSC migration 22 and preserves the stemness of hMSCs during passaging. 23 A disadvantage of Dex is its inhibitory effect on cell proliferation and viability.11,13,15,18 The actions of Dex seem to be complex, and cell responses to Dex depend on the dose and duration of supplementation, differentiation stage of the human bone marrow-derived stem cells,4,7 and age of the hMSC donor.24,25
The effects of Dex on MSCs have been the focus of many research groups. Due to its negative effects, mainly on mature osteoblasts, 10 attempts are made to develop protocols where Dex is substituted.26–30 Commitment to an end-stage phenotype is determined at the beginning of differentiation culturing, 12 and previous reports have shown that short Dex treatment of hMSCs can stimulate osteogenesis at a later time point.7,11,31 The osteogenic effect of Dex on hMSCs persists for at least 5–7 days after withdrawal, and that mineralization requires only 7–10 days of treatment. 11
Our goal has been to minimize the inter- and intraindividual variations between donors in the osteoblastic differentiation of hMSC. We have investigated the benefits of limited supplementation with Dex in standard induction media for the osteogenic differentiation of hMSCs, by comparing transient and constant Dex treatment. We have compared the two most commonly used concentrations, 10 and 100 nM, in an attempt to see whether one is superior to the other. Based on the existing literature, we hypothesized that transient Dex treatment during the first week of the osteoblastic induction of hMSCs would provide the necessary stimulus for proper osteogenesis, while the negative effects of long-term Dex treatment could be overcome.
Materials and Methods
Isolation and primary culturing of hMSC
The study was approved by the ethics committee of the Hospital District of Southwest Finland, and all donors signed an informed written consent. Bone marrow aspirates (3–5 mL) were collected as previously described 32,33 from the posterior iliac crest of 17 female donors, ranging from young, healthy female trauma patients to middle-aged and elderly women with hip osteoarthritis but an otherwise unremarkable medical history. None of the donors had any medication affecting bone metabolism. Mononuclear cells (MNCs) were isolated by density gradient centrifugation (Ficoll-Paque™ PLUS; Amersham Biosciences) and seeded at 2×106 MNCs in 25-cm2 tissue culture flasks. The cells were cultured in alpha-minimum essential medium with L-glutamine, ribonucleosides, and deoxyribonucleosides, supplemented with 100 U/mL penicillin-streptomycin (Gibco Invitrogen) and 10% pretested fetal calf serum (FCS; Gibco, cat. no. 16000), further referred to as MSC medium. Nonadherent cells were discarded after 48 h. After 14–25 days, the cells were trypsinized and re-plated at 1000 cells/cm2 (passage 0). hMSC were characterized according to the position statement of the International Society for Cellular Therapy 3 as previously reported. 33 The basic medium for osteoblastic differentiation consisted of MSC medium supplemented with 10 mM sodium β-glycerophosphate (Merck) and 0.05 mM ascorbic acid-2-phosphate (Sigma-Aldrich) (OB medium). Passage 2–3 hMSC were plated at 2500 cells/cm,2 and half of the medium was changed twice weekly.
Timing of Dex supplementation
Cells from two donors (age 41 and 55) were cultured in OB medium supplemented with either 10 or 100 nM Dex for days 1–7, 15–28, 21–28, or 1–28. Cultures without Dex were used as controls. For each condition, eight parallel 48-plate wells were used for each donor. Osteoblastic differentiation and mineralization was evaluated after 28 days as described next.
Transient versus continuous Dex treatment
Based on the results from the Dex-timing experiment, transient treatment for the first week (days 1–7) and continuous treatment (days 1–35) were chosen for further investigation. The effects on proliferation, viability, and osteoblastic differentiation were investigated. Five conditions were compared: (1) OB medium, (2) OB medium supplemented with 10 nM Dex for the first week, (3) OB medium supplemented with 100 nM Dex for the first week, (4) OB medium continuously supplemented with 10 nM Dex, and (5) OB medium continuously supplemented with 100 nM Dex. MSC medium was used as a negative control.
Assessments of osteoblastic differentiation and mineralization
Osteoblastic differentiation was determined by spectrophotometric measurement of the cellular alkaline phosphatase (ALP) activity at 14, 21, and 28 days as previously described. 34 ALP activity is presented as units/μg protein. For ALP staining, the cells were fixed at 14, 21, 28, and 35 days, and for von Kossa staining of mineralization, the cells were fixed at 21, 28, and 35 days. The fixed cells were stained for ALP (Sigma Diagnostics) and deposited mineral (von Kossa), and the plates were scanned using a flatbed scanner with a transparency adaptor (HP ScanJet 5370C) at 600 dpi resolution and saved as 24-bit color images in TIF format. Transparency exposure adjustments were maintained constant to create images of equal intensity. ALP and von Kossa-positive areas were then histomorphometrically quantified from the images using an automated image analysis, 35 and the stained areas (cm2) were converted to a percentage of the total area.
Immunocytochemistry of collagen type I and osteocalcin
Terminal osteoblastic differentiation was demonstrated by immunostaining for collagen type I (COL1) and osteocalcin (OCN). hMSC from two donors were cultured in four-chamber slides (Nunc) in OB without Dex, with 100 nM Dex for 1 week, and 100 nM continuously for 14 and 28 days. Cells were fixed and stained with polyclonal primary antibodies against COL1 (1:100, rabbit anti human COL1; Fitzgerald Industries International cat. no. 70R-CR007) or OCN (1:60, rabbit anti human OCN; AbD Serotec cat. no. 70601515). Bound antibodies were detected with avidin-conjugated peroxidase and DAB (3,3′-diaminobenzidine, 3 min) (Vector Laboratories). The omission of primary antibodies was used as a negative control.
MTS cell proliferation assay
The effect of different Dex treatments on cell proliferation was assessed using a nonradioactive MTS colorimetric assay (CellTiter 96®; Promega Co.) as previously described. 36 hMSC were cultured at 1000 cells/well in 96-well plates, and cell proliferation was quantified at days 7, 14, and 21 following the manufacturer's protocol. The optical density at 490 nm (OD490) was measured and used as a cell proliferation index.
Live/dead cell viability assay
The effect of different Dex treatments on cell viability was evaluated using a LIVE/DEAD kit (Molecular Probes). Live and dead cells were quantified at days 7, 14, and 21 according to the manufacturer's protocol. The fluorescence counts at 530/642 nm (dead cells) and 485/535 nm (live cells) were measured with a micro-plate reader (Wallac 1420 Victor 2 ; PerkinElmer Life Sciences), and the level of dead cells was expressed as the percentage of the total cell count.
Apoptosis assay
Apoptosis were studied by a photometric ELISA (cell death detection ELISAPLUS; Roche Diagnostics). hMSC were plated in 24-well plates and cultured for 10, 14, or 21 days. Cells were lysed (200 μL lysis buffer/well), and lysates from triplicate wells were combined and measured in two replicates according to the manufacturer's instructions.
Statistical analysis
Results are presented as mean±standard deviation (SD). Differences between culture conditions were analyzed using mixed-models analysis of variances, with the culture medium as fixed factor and the donor as random factor to allow for multiple replicates from each donor. In all mixed-models analysis, Sidak's adjustment for multiple comparisons was used. The influence of donor age was analyzed using the mixed-models analyses with age and linear regression as cofactors. To investigate whether the same culture condition is optimal regardless of donor age, the donors were divided into three age groups based on the age periods of differing hMSC titers 37 and analyzed separately (Group I <30 years, Group II 30–60 years, Group III >60 years). To assess the magnitude of variation between donors and between parallel samples from the same donor, inter- and intraindividual coefficients of variation (CV%) were calculated. p-values lower than 0.05 were considered statistically significant, and all statistical analyses were performed using SPSS 19.0 for Windows.
Results
Transient 10 or 100 nM Dex treatment for the first week and continuous treatment with 10 nM Dex promote the strongest osteoblastic differentiation
hMSC were cultured for 28 days in osteoblastic induction (OB) media with or without 10 or 100 nM Dex for different transient time periods (days 1–7, 15–28, 22–28) or continuously (days 1–28) (Fig. 1). The strongest differentiation was observed when 10 or 100 nM Dex was present for the first week (days 1–7), or when 10 nM Dex was present continuously (days 1–28), showing a fourfold increase in ALP, when compared with the control (OB). In addition, mineralization was significantly higher in cultures treated for days 1–7 or continuously (days 1–28) with 10 or 100 nM Dex compared with all other treatments, where less than 5% of the areas stained positive for von Kossa (Fig. 1B). In cultures treated with 10 or 100 nM Dex for days 1–7, von Kossa-stained areas were increased more than 40-fold compared with the control, while the continuously treated cultures showed 13–28-fold increases compared with the control.
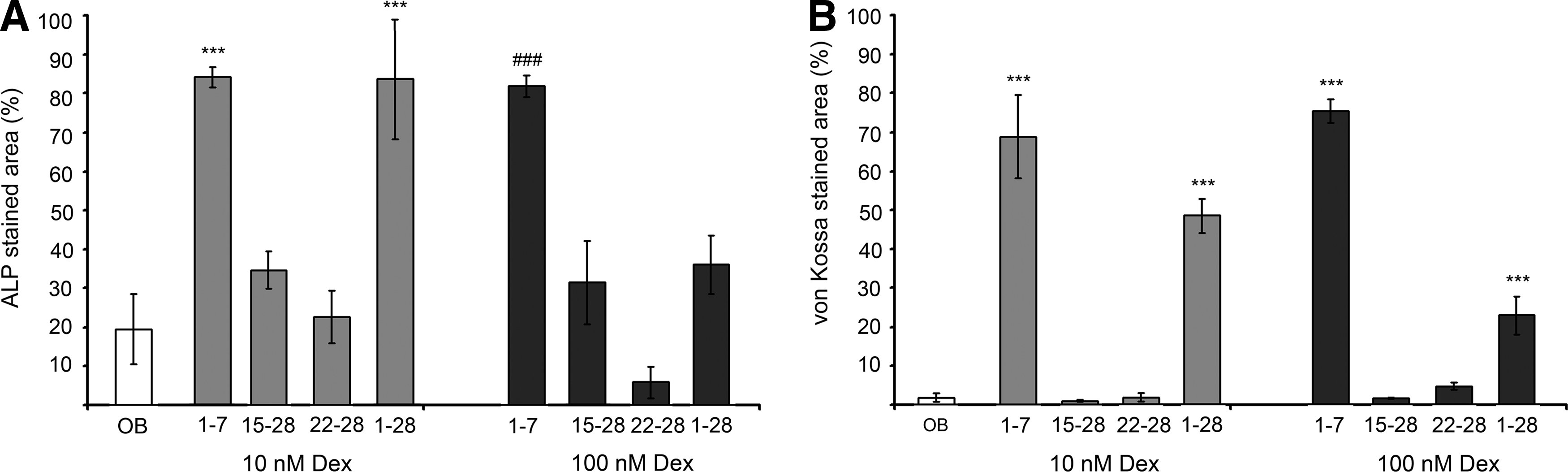
Dexamethasone (Dex)-timing. Osteoblastic differentiation cultures of human mesenchymal stem cell (hMSC) treated with 10 and 100 nM Dex during different time periods (days indicated at x-axis) and compared with the control without Dex (OB).
The only difference between 10 and 100 nM Dex was seen with continuous treatment, where 10 nM yielded two-fold higher osteoblastic differentiation and mineralization than 100 nM (Fig. 1A, B, respectively).
Transient treatment with 100 nM Dex promotes high ALP activity and mineralization
Under qualitative microscopic evaluation, hMSC cultured in OB without Dex or transiently treated with 10 and 100 nM Dex for the first week reached confluence by day 14. By day 21, ALP-positive cells were evenly spread throughout the culture plate surface of the control and transiently Dex-treated cultures, whereas in the continuously Dex-treated cultures, the staining was sparser.
ALP activity assay and histomorphometry of ALP-stained areas confirmed these observations. At all time points, the cells transiently treated with 100 nM Dex showed the highest ALP activity (20%–330% higher compared with other OB treatments) and largest ALP-stained areas (1–23 times larger ALP-stained areas compared with other OB treatments), while transient treatment with 10 nM Dex was less effective (1–13 times larger ALP-stained areas compared with other OB treatments) (Table 1). Transiently 10 and 100 nM Dex-treated cultures showed higher mineralization than other cultures based on the measurements of von Kossa-stained areas (Table 1). Transient treatment with 100 nM Dex induced the highest degree of mineralization at 28 and 35 days (1.7–6.4 times larger von Kossa-stained areas compared with other OB treatments), and transient 10 nM Dex was nearly as effective (1.4–5.7 times larger von Kossa-stained areas compared with other OB treatments).
Comparison of the six different culture conditions at each time point (mixed-models analysis of variance, p-values<0.05–0.001):
Lower compared with others.
Higher than MSC medium, OB medium, 1-week continuous 10 nM Dex treatment, and continuous 100 nM Dex treatment.
Higher than MSC medium, OB medium, and continuous100 nM Dex treatment.
Higher than all others.
Higher than MSC medium, OB medium, 1-week 10 nM, and continuous 100 nM Dex treatment.
MSC, mesenchymal stem cell; Dex, dexamethasone; ALP, alkaline phosphatase.
In MSC medium, ALP activity was low at all time points, and positive ALP staining was negligible throughout the experiment (Table 1). No positive von Kossa staining was detected with MSC medium.
Transient 100 nM Dex treatment promotes COL1 and OCN expression
In control (OB) and transiently 100 nM Dex-treated cultures, a clear and widespread COL1 staining was observed at day 14 (Fig. 2A, B). OCN expression, a late marker of bone formation and a sign of more mature osteoblastic phenotypes, was not detected in control cultures, while transiently and constantly 100 nM Dex-treated cultures were positive for OCN at 28 days (Fig. 2D–F). The degree of mineralization at 28 days was visualized by von Kossa staining (Fig. 2G–I), and the differences between the cultures were quantified (Table 1).
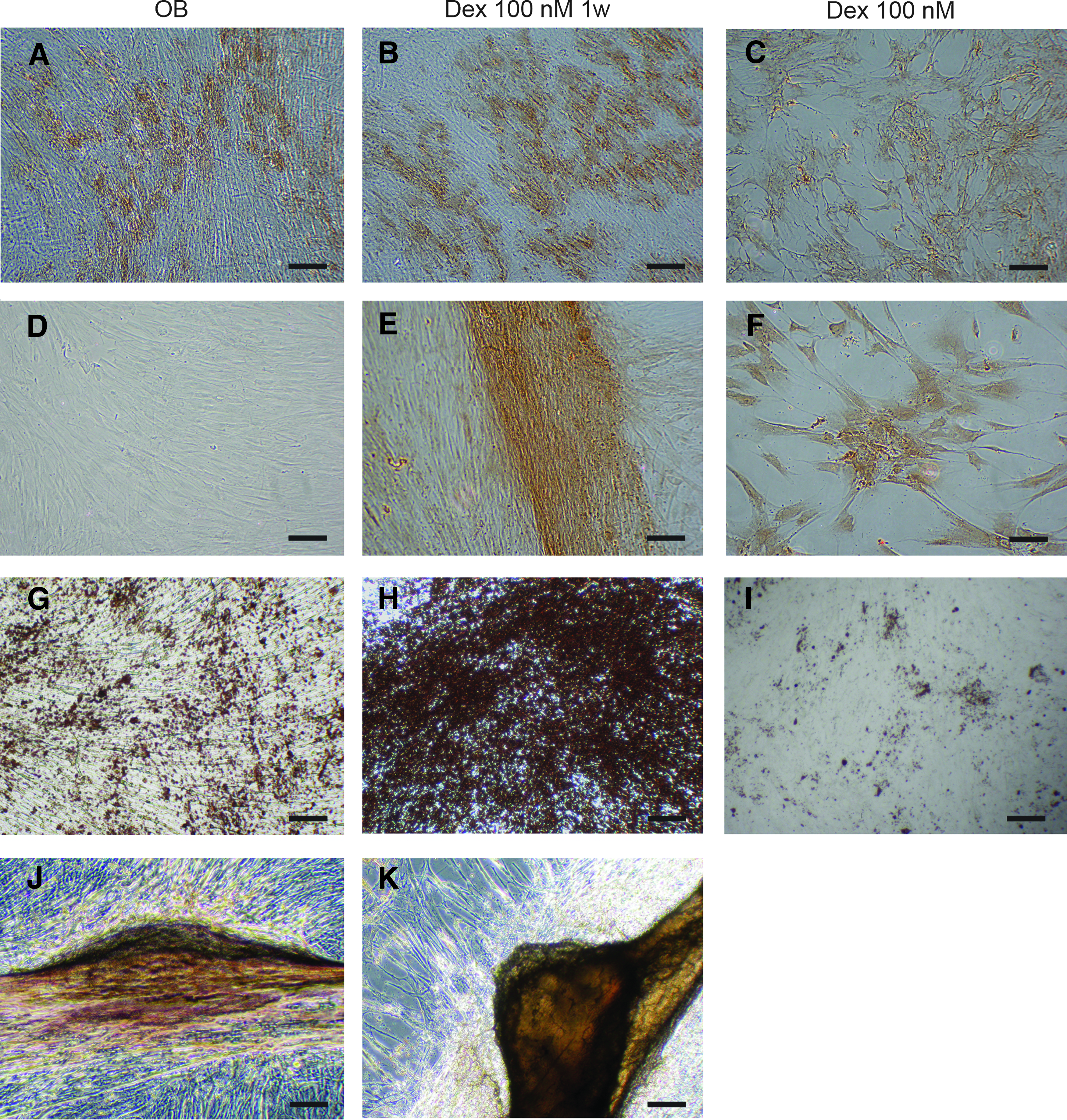
Osteoblastic differentiation. Terminal osteoblastic differentiation demonstrated by immunostaining for collagen type I at 14 days
The morphological features were different with different Dex treatments. At 14 days, transiently Dex-treated cultures and control cultures were already confluent (Fig. 2A, B), while constantly treated cultures were only about 40% confluent with a monolayer of larger cells with membrane extensions (Fig. 2C). At 28 and 35 days, 3D formations associated with in vitro bone formation were visible, with a different structure and morphology in the different treatments (Fig. 2G–K). Typical bone nodule formation was only rarely observed. Transiently Dex-treated cultures showed areas of multilayered cells forming 3D strand-like formations that stained positively for both OCN (Fig. 2E) and von Kossa (Fig. 2K). A similar formation was also detected in some of the control cultures (Fig. 2J). No 3D formations were seen with continuous 100 nM Dex treatment.
Transient Dex treatment stimulates proliferation and viability, and inhibits apoptosis
Transient treatment with 10 or 100 nM Dex stimulated cell proliferation compared with continuous treatments. This started to appear at day 14 and was even more pronounced at 21 days (Fig. 3A). There were no statistically significant differences in proliferation between transient 10 or 100 nM Dex treatments and control (OB) cultures.

Cell proliferation
The levels of dead cells were low at all time points (Fig. 3B). The number of dead cells was temporarily elevated at 14 days in cultures with MSC medium and in cultures continuously treated with 10 or 100 nM Dex.
Apoptosis rates were low in all culture conditions at days 10 and 14 (Fig. 3C). At day 21, control cultures (OB) showed 2–7-fold higher apoptosis levels, and cultures transiently treated with 10 nM Dex showed 5–16-fold higher apoptosis levels compared with all other treatments.
Low inter- and intraindividual variations in transient treatment with 100 nM Dex
In terms of inter- and intraindividual CV%, transient treatment with 100 nM Dex was superior to the other culture conditions. Transiently 100 nM Dex-treated MSC cultures of different donors (n=17) showed lowest interindividual CV% in all osteoblastic differentiation assays (ALP activity, ALP- and von Kossa staining) (Fig. 4A). Transient 100 nM Dex treatment also resulted in lowest intraindividual variations in the three differentiation assays (Fig. 4B).
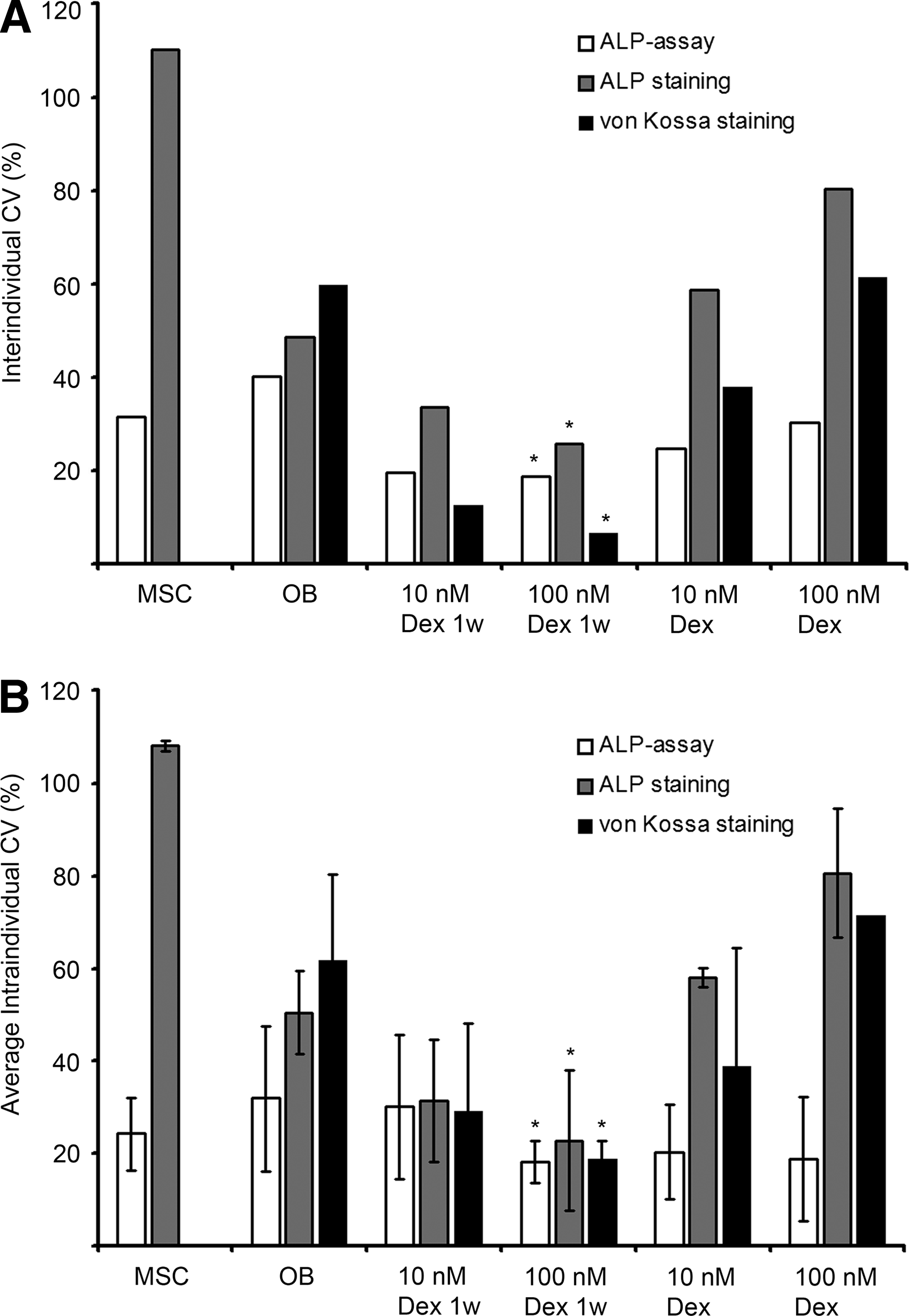
Coefficients of variation (CV%).
Transient treatment with 100 nM Dex is optimal regardless of donor age
Based on the mixed-models analyses, osteoblastic differentiation was strongest with transient treatment with 100 nM Dex, independent of donor age. This was further confirmed by dividing donors into three age groups: Group I (median 23, range 19–26 years, n=4), Group II (median 55, range 38–60 years, n=6, 4 postmenopausal), and Group III (median 69, range 65–75 years, n=7). In all age groups, the highest ALP and mineralization was seen with transient treatment with 100 nM Dex (Supplementary Table S1; Supplementary Data are available online at

CV% in age groups. Variations between donors in
Discussion
Several promising hMSC applications would benefit from an in vitro protocol ensuing terminal osteoblastic differentiation, independently of donor-related varieties. The development of such a protocol was the aim of this study. We found enhanced differentiation and mineralization using transient treatment with 100 nM Dex during the first week of induction culture. This treatment decreased the variability in osteoblastic characteristics between hMSC from different individuals. Transient treatment with 10 nM Dex was not as effective as 100 nM.
Our initial experiments using Dex treatments for different time periods showed that the presence of Dex during the first week of induction is critical for proper osteoblastic differentiation. This is reasonable, as phenotype commitment seems to be determined early in the culture period, 12 and an early report suggested that 7 days of supplementation with Dex is enough for terminal osteoblastic differentiation. 11
Previous studies support our results on the long-term stimulatory effects of transient Dex treatment on osteogenesis. In two studies, the primary cultures of hMSCs were first treated with 10 nM Dex for the first 48 h, which then stimulated later cell proliferation and ALP expression7,31 and mineralization. 31 In a third study, using a protocol similar to ours, 7 days of treatment with 100 nM Dex resulted in the same level of ALP and mineralization as continuous Dex treatment. 11 Song et al. 38 reported increased ALP activity with increased treatment time using 100 nM Dex, but it is unclear whether their study was performed on primary or passaged cells. This is of importance, as the response to Dex is different in primary and passaged cells.7,10,17,18,23,31,39
Controversies regarding the use of Dex for the in vitro differentiation of hMSCs are often based on the adverse effects of long-term in vivo use of glucocorticoids.10,40 In vitro Dex is known to inhibit cell proliferation.11,13,15,18 We also found significantly delayed proliferation with continuous Dex treatments, but in contrast, transiently treated cultures showed a proliferation equal to control cultures. Our results of transient Dex treatment are in agreement with previous studies12,26 but in conflict with those by Cheng et al., 11 who found that both transient and continuous Dex treatment inhibit proliferation.
To qualitatively evaluate the maturation stage of osteoblast cultures, we used immunostaining for COL1 and OCN. Dex is suggested to inhibit 41 or postpone 7 COL1 and reduce OCN production.26,41 We found positive COL1 staining already at 14 days with transient Dex treatment. In contrast to earlier proposals,26,41 OCN was not detected in cultures without Dex, while transiently Dex-treated cultures showed uniform and widespread OCN staining, and also continuously treated cultures were positive for OCN. This is in line with previous reports, where transient Dex treatment enhanced OCN expression to levels higher than controls without Dex, 11 and 10 nM Dex increased the OCN expression compared with OB medium without Dex. 42 The methods applied in our study did not allow the assessment of the amount and distribution of the collagenous matrix in different culture conditions. It is likely that the different morphologies seen with different Dex treatments influence the distribution of the collagen matrix, and, subsequently, the 3D structure of the mineralized matrix. We did not perform an analysis of the mRNA expression levels of matrix components. Such an mRNA analysis would have provided quantitative data on the effects of transient and constant Dex treatment on COL1 and OCN. However, expression at the transcriptional level does not always correspond to the actual protein level due to post-translational regulation.
Broad variations between donors8,11,15,23,28,42,43 and variations between different experiments with cells from the same donor are common problems associated with hMSC research,2,6,9,42 especially regarding osteoblastic differentiation.8,11,12,15,43 Both donor characteristics and the stage of the hMSC are known to affect the response to Dex.4,6,7,23,24,39 If culture conditions are suboptimal, then variations might be greater due to differences in responsiveness among heterogenic donor populations. As an important advantage, our results demonstrated smaller inter- and intraindividual variations with transient Dex treatment. Eleven of our 17 donors suffered from hip osteoarthritis, which may affect MSC functions.6,44 Despite this heterogeneity, transient Dex treatment showed only minor individual variations, whereas continuous or no Dex treatment resulted in higher variations. Supporting our findings, lower variations with Dex treatment have been previously demonstrated. 11
The impact of donor age on hMSC performance is another essential issue. We have previously reported an age-related decline in growth characteristics and the osteoblastic differentiation potential in hMSC from younger and also very old patients. 33 In the present study, despite age-related differences in the level of osteoblastic differentiation, transient treatment with 100 nM Dex provided the best outcome in all age groups.
The potency of hMSC might also be gender related. 6 In that respect, our study is limited, as all donors were women. However, the effect of gender on the responsiveness of hMSC to osteoblastic induction and Dex seems secondary to age and other demographic factors.6,43 In previous studies on Dex and hMSC, gender of the donors and/or possible gender-related differences in the Dex response have not been specified. A few studies addressing the issue have all reported no gender-related differences in the Dex response.15,43,45,46 Therefore, it is reasonable to assume that transient 100 nM Dex treatment would provide a high degree of differentiation and low variations also with hMSC from male donors.
In conclusion, transient 1-week treatment with 100 nM Dex seems to reduce donor variability in the osteoblastic differentiation of hMSC. The timing of Dex treatment seems to be an important parameter for controlling and adjusting in vitro hMSC bone formation, which is relevant for basic hMSC research and tissue-engineering applications.
Footnotes
Acknowledgments
Tero Vahlberg, M.Sc., at the Department of Biostatistics, University of Turku, is acknowledged for statistical consultation. The study was financially supported by The Finnish Funding Agency for Technology and Innovation, Turku University Central Hospital (EVO grant), Päivikki and Sakari Sohlberg Foundation, Einar and Karin Stroems Foundation, Orion–Farmos Research Foundation, and The Swedish Cultural Foundation in Finland. J.J.A. is a supported Ph.D. student of the National Doctoral Program of Musculoskeletal Disorders and Biomaterials (TBDP). The funding sources had no involvement in the study.
Disclosure Statement
No competing financial interests exist for any of the authors.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.