
Abstract
Attaining a well-qualified whole decellularized organ applicable for an enduring and successful transplantation, decellularization protocols should be organ specific in terms of decellularizing agents and time of tissue exposure. Since a bioscaffold resulting from a large solid organ should have the potential to preserve its three-dimensional architecture and consistency for at least several months in the site of transplantation, evaluating the mechanical properties of the bioscaffold is mandatory before transplantation. In the current study, we compared five different decellularization protocols and also two main decellularization techniques (perfusion vs. diffusion) to decellularize the sheep liver, which is similar to the human liver in terms of size and anatomy. Moreover, we assessed the retaining of vascular network by dye injection and angiography. We also determined the most proper sterilization method by comparing six different sterilization methods. The mechanical properties of the scaffolds were assessed by applying tensile strength, suture retention, and compressive strength tests. The perfusion technique showed better results compared to the diffusion technique. The protocol containing ammonium hydroxide and triton X-100 was the most proper decellularization protocol leading to completely decellularized livers along with intact vascular network. Furthermore, we noted that application of streptokinase in washing step facilitates decellularization. Our results also showed that a combination of two sterilization methods is necessary for complete sterilization of a sheep liver and peracetic acid or ethylene oxide+gamma irradiation was associated with the best outcome. Determining the most appropriate decellularization and sterilization method for each organ along with assessing the mechanical properties of the resulting bioscaffold are principal steps before fabricating efficient artificial organs in the foreseeable future.
Introduction
Baneful by-products released during degradation of synthetic bioscaffolds or the residual materials after fabrication techniques may have adverse effects on the host. They also tend to induce an inflammatory response and scar formation during the remodeling process. Moreover, they lack a system to deliver nutrients and oxygen to cells deep within the scaffolds; consequently, cells cannot migrate deep into and only survive near the surface. They should also be shaped into the desired configuration of the organ to fit into the body cavity. Shaping does not always result in a shape with the same size as the native in vivo organ. It may also have deleterious effects on the mechanical properties of the scaffold.5,8,9,11,14
Although much effort has been made to improve the mentioned drawbacks, yet not an ideal synthetic bioscaffold has been developed. Therefore, there is a strong desire for natural bioscaffolds due to characteristics, such as having the same size, shape, and composition as the main tissue, capability of neovascularization, rapid in vivo degradation, and the ability to induce efficient tissue reconstruction.1,11,14–16
Natural bioscaffolds are prepared by decellularizing tissues. The goal of decellularization is to remove a substantial amount of cellular and nuclear content (immunogenic materials) leaving behind the three-dimensional (3D) support system of the extracellular matrix (ECM) without significantly affecting the biological and mechanical properties; likewise, the biochemical composition of the remaining ECM. The ECM (the natural bioscaffold) can be safely used for transplantation because components of the resulting ECM are generally conserved in different species and are not immunogenic.
To optimally decellularize a tissue, it is crucial to consider that decellularization methods vary organ to organ and species to species.9,10,17,18
Due to abundant applications of biological scaffolds in regenerative medicine, efforts in developing the best decellularization protocol for each tissue are highly commendable. Following preparing the ECM from delicate tissues, regenerative medicine studies are going toward preparing the ECM of large solid organs, such as heart, lung, kidney, and liver.3,5,6,14,17,19–22
Up to now, different species of liver, mostly rats, have been decellularized by different methods for preparing the natural bioscaffolds.1,2,6,7,23,24 In these studies, mechanical values of the bioscaffolds have not been measured in vitro neither was available a long-term in vivo follow-up to evaluate the mechanical properties, which are critical parameters for a successful transplantation. Despite these studies having provided valuable clues to this field, still there is no promised established decellularization protocol available for whole organ decellularization, especially for human-sized liver tissue.
Animals raised for meat production like sheep are useful sources for isolating the liver organ. The organs of these animals are very similar to humans in terms of size and anatomy, thus having more potential applications for human usage. Here, we have compared different decellularization and final sterilization methods to find the optimal one for a human-sized liver tissue.
Materials and Methods
Twenty adult sheep were brought from a special farm in which the sheep were kept for research purposes in a sanitary and controlled environment. Before being used in our study, all the sheep were examined by a veterinarian to ensure good health.
All animals were cared in accordance with the guidelines for the care and use of laboratory animals prepared by the National Academy of Sciences.
Organ isolation
Each time an adult male sheep was euthanized following systemic heparinization (5000 IU bolus dose before surgery and 25 IU/kg/h IV infusion intraoperatively). The liver was removed surgically under sterile conditions using standard techniques for tissue removal. An attempt was made to accurately remove all major vessels of the liver without any rupture or injury. The livers were divided into five groups based on five different treatment protocols.1–5 Each group was divided into four subgroups, including perfusion with streptokinase (SK), perfusion without SK, diffusion with SK, and diffusion without SK. An intact sheep liver brought from the mentioned farm, served as the control group.
Initial preparation
In all subgroups, livers were rinsed in a sterile normal saline buffer to remove surface blood and excess tissues. The common hepatic artery and portal vein as afferents, and inferior vena cava as an efferent, were cannulated to provide an antegrade perfusion (artery to vein). All accessory vessels were ligated. The afferent cannulae were attached to a pump. One hour of phosphate-buffered saline (PBS) perfusion containing heparin (5000 IU per liter of PBS) was performed to wash out inside blood completely. In SK treating livers, the washing perfusion was done with PBS containing heparin and SK (5000 and 750,000 IU per liter of PBS, respectively). All decellularizing solutions were supplemented with 100 U/mL penicillin, 0.1 mg/mL streptomycin, and 0.25 μg/mL amphotericin B.
Decellularization
In perfusion subgroups, the decellularizing solutions were perfused via the cannulation into the liver tissue using the pump. In diffusion subgroups, the liver was separated into lobes and sliced into almost uniform pieces. The liver pieces were shaken using a refrigerated shaking incubator in the same solutions and temperature conditions for the same durations as the perfusion group all at speed of 100 rpm. A thorough description of applied decellularization protocols has been shown in Table 1.
Evaluation of the decellularized livers
Samples were prepared from the control and treated livers, paraffin embedded, stained with hematoxylin–eosin and studied under an optical microscope. For verification of decellularization, we calculated the cell survival rate defined as (the number of cells in treated tissue)/(the number of cells in untreated tissue)×100. The remaining cells were counted in eight random high-power fields (X400) and the averaged number was divided by the number of cells in the control sample, and then the result was multiplied by 100 and reported as the cell survival rate.25,264′, 6-diamidino-2-phenylindole (DAPI) staining was also performed to indicate any remained nuclear content and the slides were studied and imaged under a fluorescent microscope. Applying scanning electron microscopy (SEM), we also evaluated the decellularized livers' ultrastructure. Immunohistochemical (IHC) analysis using specific antibodies was performed to verify the retention of major liver ECM components, such as laminin, fibronectin, collagens I, and IV. The sections were incubated with primary antibodies, including sheep anticollagen I, antilaminin, antifibronectin, and anticollagen IV, followed by appropriate HRP-conjugated secondary antibodies.
The collagen and sulfated glycosaminoglycan (sGAG) content of the livers were quantified using the Sircol and Blyscan assay kits, respectively.
The mechanical properties of the treated livers were examined by performing three tests, including tensile strength, suture retention strength, and compressive strength, all with the rate of 0.5 mm/min using a dynamic testing machine.19,27,28
For the perfusion subgroup in which livers were completely decellularized with retained biomechanical properties, injection of the Allura Red AC dye through the afferent cannulae and also angiography were performed to show retaining of the vascular network.
Characterization of sterilization methods
Seven more livers were perfused with protocol 1 (Table 1) resulting in whole decellularized livers. Following decellularization, the control liver was sent to a microbiology laboratory for estimation of bioburden indicating the population of viable microorganisms in the tissue. Based on the estimated bioburden, the dose of 3 megarads (Mrad) of gamma irradiation (GIR) was recommended for the liver tissue.29,30 Sterilization was not performed in the control liver, while the remaining decellularized livers were sterilized with 6 different sterilization methods, including peracetic acid (PAA)+GIR, ethylene oxide gas (EOG)+GIR, freeze drying (FD)+GIR, EOG, GIR, and FD. In sterilization by GIR, the liver was irradiated with a minimum absorbed dose of 3 Mrad (with dose rate of 3.48 Gy/s) at dry ice temperature in a gamma irradiator (Gammacell 220; Nordion Co.). In sterilization by EOG, the liver was exposed to 100% EOG in an EOG sterilizer (MMM Münchener Medizin Mechanik GmbH) at 42°C with humidity of 40% for 8 h. For FD, the liver was freeze dried using a freeze dryer (Alpha 2–4, Chaist) at −80°C for 24 h. In sterilization with PAA+GIR, following decellularization PAA 0.1% was perfused via the cannulation into the liver tissue for 2 h at room temperature, and then the liver was irradiated as mentioned above. In all hybrid sterilization methods, GIR was performed as an adjunct method after applying the primary method. Following sterilization, a sample from the treated liver was sent for assessment of the mechanical properties.
Sterility is expressed in international standards as a sterility assurance level (SAL) of 10−6. SAL is defined as the probability of a viable microorganism being present on a tissue after sterilization. The most modern method of validation of sterility is using a biological indicator (BI) containing 106 viable microorganisms to ensure SAL of 10−6. 31 We utilized specific BIs for validation of sterilization by EOG and GIR. The BIs were placed inside the livers' packages before sterilization. Following sterilization, the BIs were removed aseptically and cultured in the appropriate culture medium. The culture medium changes colorimetrically from red to yellow if spores grow.
In addition, following all sterilization methods, the liver tissue was incubated in 3 different culture media, including the Tryptic Soy Broth, Thioglycolate Broth, and Sabouraud Dextrose Broth. Microbial growth was indicated by the presence of turbidity compared to an uninoculated control.
Statistical analysis
Statistical analysis was performed using SPSS (Statistical Package for the Social Sciences, version 12.0) software. Using the Kolmogorove–Smirnove (KS) test, we showed that our data has been distributed normally. Therefore, we used the t test to compare quantitative values between different groups. Two-tailed p values less than 0.05 were considered statistically significant.
Results
In each group, perfusion decellularization contributed to a better result compared to diffusion decellularization. Furthermore, application of SK resulted in more efficient decellularization in all subgroups except in perfusion subgroups of groups 1 and 5, in which tissues treated with SK and those that did not receive SK were both completely decellularized (Table 2).
For calculating the cell survival rate, the remaining cells were counted in eight random high-power fields (X 400), and the averaged number was divided by the number of cells in the control group, then the result was multiplied by 100 and reported as the cell survival rate.
Values are represented as mean±SD.
P, Perfusion; D, Diffusion; SK, streptokinase was added; WSK, without streptokinase, that is, SK was not added.
Group 1
The decellularization method applied in group 1 resulted in fully decellularized constructs in perfusion subgroups (Fig. 1A–D and Table 2). In these subgroups, SEM showed a honeycomb structure made of intact protein fibers with intact vessels and bile ducts in the absence of cells and nuclei (Fig. 1E–I).
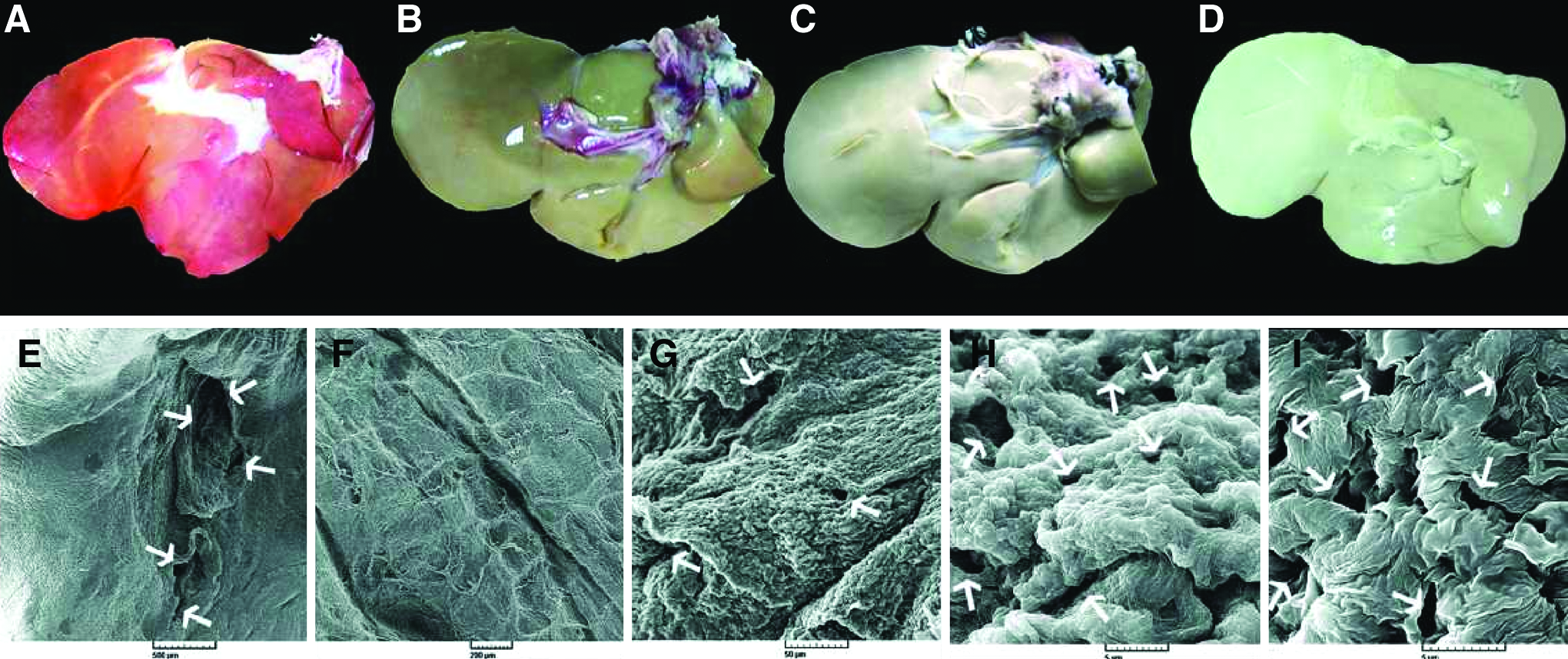
Preparation and ultrastructural analysis of the perfusion decellularized livers of group 1. Macroscopic view of the sheep liver decellularized by the protocol as described in Methods at 0, 16, 32, and 48 h of decellularization
IHC analysis of the treated livers in group 1 showed no reduction of ECM components compared with the control group (Fig. 2A, B). Total collagen and sGAG of all groups were quantified and expressed as μg/mg wet liver tissue (Table 3). Livers of group 1 showed a significantly higher collagen and sGAG compared to the control group possibly due to segregation of the cellular proteins during decellularization. Integrity of vascular network of the perfusion decellularized livers in group 1 was evaluated by the Allura Red AC dye and angiography. The injected dye flowed inside the vessels without any leakage, and angiography also confirmed the preservation of the vascular tree of the treated livers (Fig. 3A, B). In addition, DAPI staining revealed no remaining nucleus in perfusion subgroups (Fig. 3C–H). Decellularized livers in group1 exhibited higher mechanical properties especially in the tensile modulus, which represents elasticity of the material, compared to the control group (all p-values <0.001) (Fig. 4; Table 4).
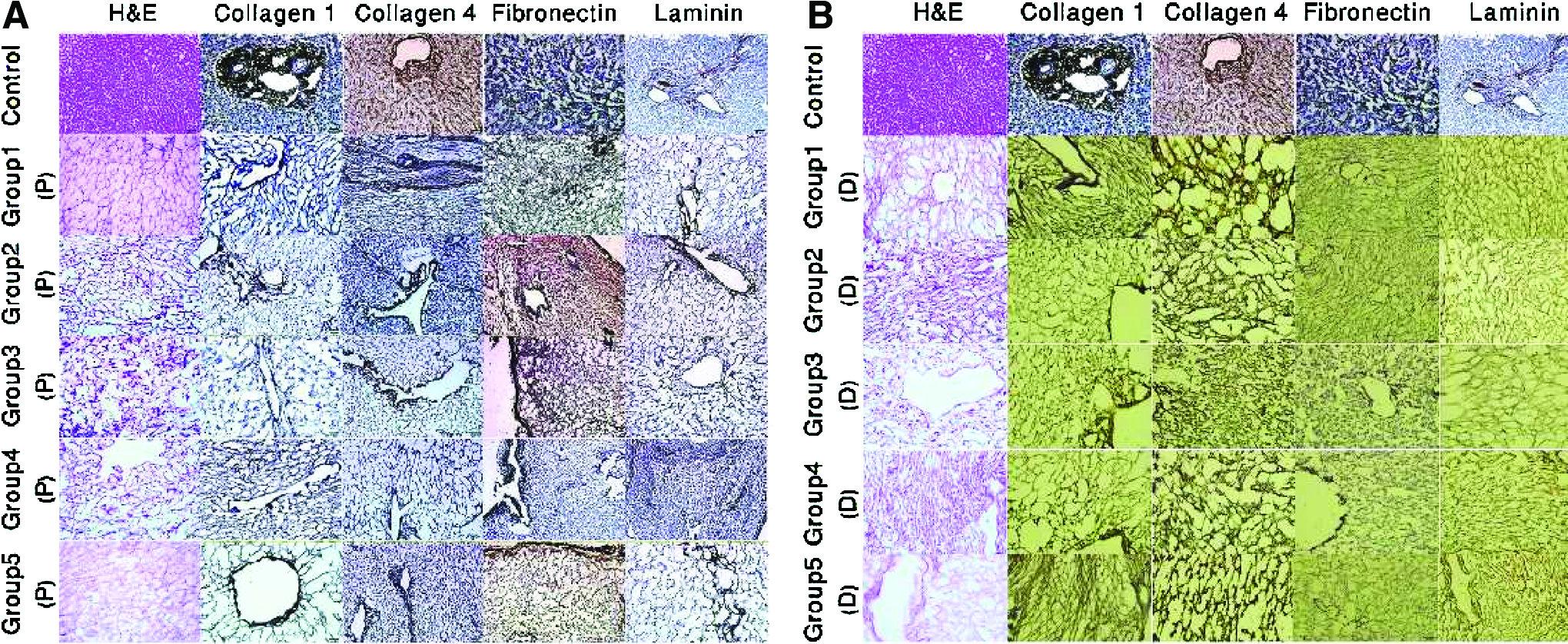
Comparison of histological structure and biochemical composition of the treated livers. Sections of control and treated livers were prepared for histological and biochemical analyses as described in Methods. H&E and immunohistochemistry (IHC) images of both perfused
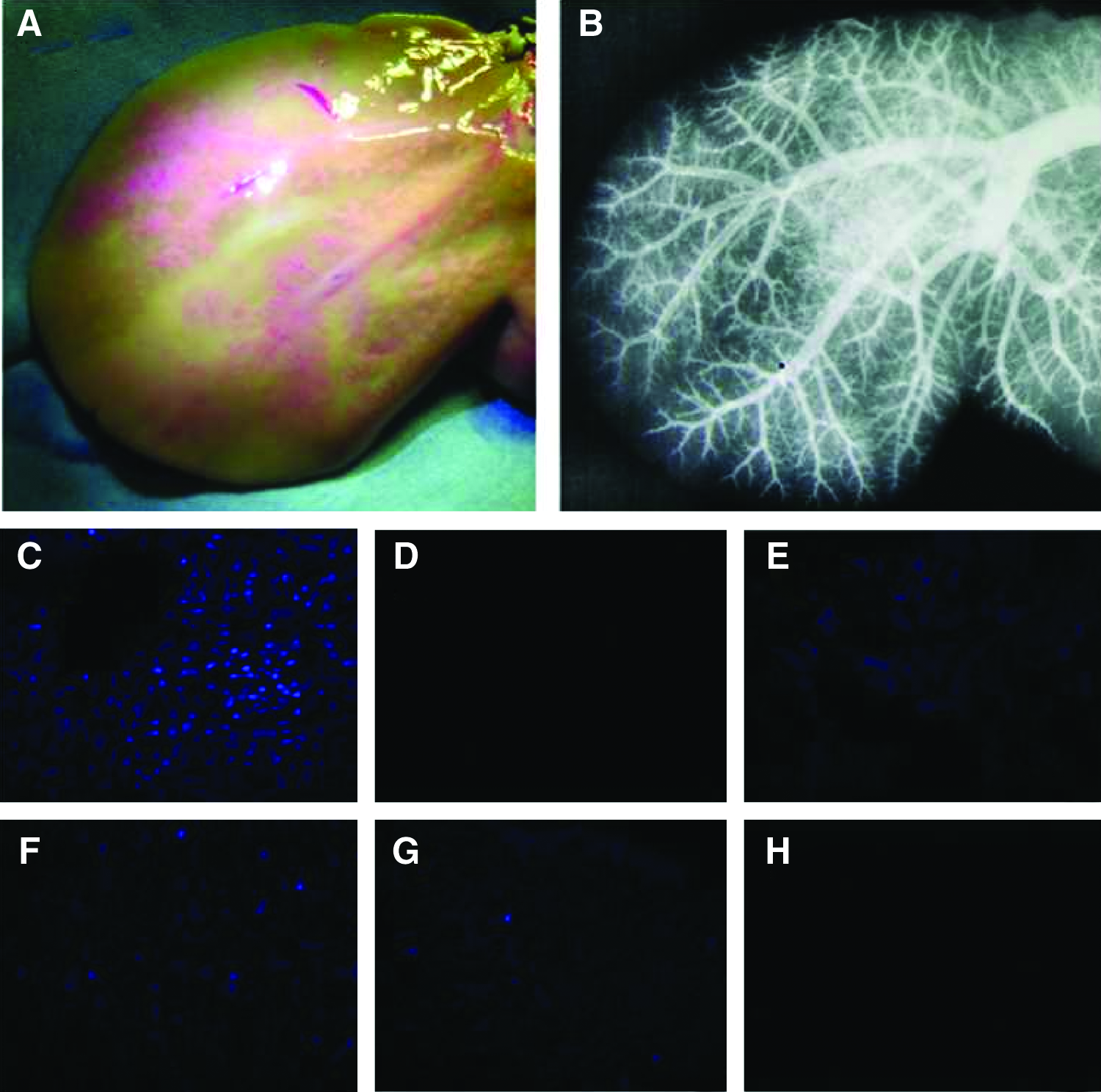
Characterization of vascular network and nuclear content of the treated livers. Allura Red AC dye was injected through the afferent cannulae of a perfusion decellularized liver in group 1 as described in Methods. The photograph shows the visible intact vascular network of the liver scaffold
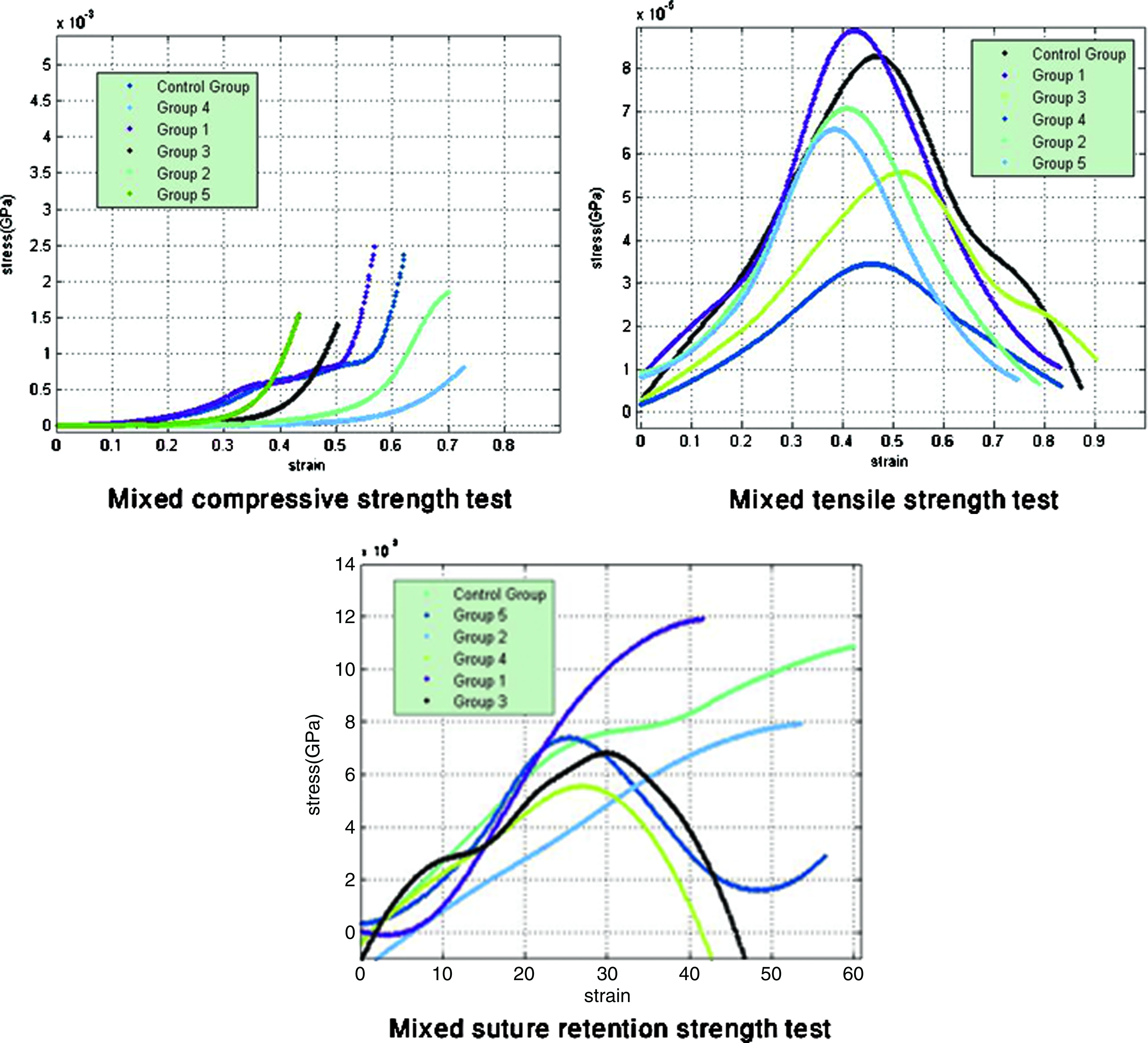
Mechanical properties' graphs of the treated livers. Mechanical properties of the treated livers were examined by performing tensile strength, suture retention strength, and compressive strength tests. Briefly, decellularized livers in group1 exhibited higher mechanical properties compared to the other groups (all p-values <0.001). Livers of group 2 showed decreased mechanical properties in all the tests compared to the control group. Mechanical properties of the livers in group 3 also decreased significantly and the mechanical tests' values in group 4 were the least among the all. In group 5, the mechanical properties showed significant decrease particularly in tensile strength test (p<0.001). Color images available online at
In each treated group (1–5), samples were taken from 4 subgroups, including P-SK, P-WSK, D-SK, and D-WSK (n=4), and in the control group, samples were taken from 4 different locations of the liver. Collagen and sGAG content of the samples were quantified using the Sircol and Blyscan assay kits, respectively. The results were represented as mean±SD.
sGAG, sulfated glycosaminoglycan.
For evaluation of the mechanical properties, in each treated group (1–5), uniform rectangular pieces were cut from 4 subgroups, including P-SK, P-WSK, D-SK, and D-WSK (n=4), and in the control group, 4 same-sized pieces were cut from different locations of the liver. The mechanical properties of the samples were evaluated by performing three tests, including tensile strength, suture retention strength, and compressive strength, all with the rate of 0.5 mm/min using a dynamic testing machine. Tensile strength measures the force required to pull the material to the point where it breaks, the suture retention strength measures the maximum force required to pull a suture through the material tested and compressive strength measures the largest compression force the material can withstand. The results are presented as mean±SD.
Group 2
Applied protocol in group 2 failed to decellularize the livers completely (mean cell survival rate of 18.3%, Table 2). DAPI staining exhibited the remained nuclei (Fig. 3C–H). All ECM components were also slightly decreased (Fig. 2A, B). Decrease of the total collagen of the livers compared to the control group (0.882 vs. 1.89, p<0.001) suggests the deleterious effect of this protocol on the collagen content (Table 3). In this group, all the mechanical test values decreased compared to the control group (Fig. 4 and Table 4).
Group 3
Applied protocol in group 3 resulted in a significant amount of remaining cells and nuclei within the treated livers (mean cell survival rate of 33.75%, Table 2). The collagen, laminin, and fibronectin content of the ECM decreased significantly (Fig. 2A, B). Moreover, the collagen and sGAG content of this group were the least among the all (p<0.001) (Table 3). These data suggest the harmful effect of the protocol and/or the temperature condition of the procedure on the collagen and sGAG content of the ECM. The mechanical properties of the livers in this group also decreased significantly (Fig. 4 and Table 4).
Group 4
Applied protocol in group 4 was not successful to completely decellularize the livers (Table 2). Remaining nuclei are shown in DAPI staining images (Fig. 3C–H). IHC examination demonstrated reduced amounts of collagen I, collagen IV, laminin, and fibronectin compared to the control group (Fig. 2A, B). The collagen and sGAG content of the livers were almost similar to group 2 (Table 3). The mechanical tests' values were the least among the all (Fig. 4 and Table 4).
Group 5
Application of sodium dodecyl sulfate (SDS) in group 5 fully decellularized the livers of perfusion subgroups (Table 2). DAPI staining confirmed complete removal of nuclei in these subgroups (Fig. 3C–H), and the IHC study showed that the majority of ECM proteins remained almost unchanged (Fig. 2A, B). However, the collagen and sGAG quantity of the livers were significantly lower than those in the control group (Table 3) and the mechanical properties showed a significant decrease particularly in the tensile strength test (p<0.001) (Fig. 4 and Table 4).
Comparing different sterilization methods
In sterilization by either EOG or GIR as single methods, discoloration of the BI medium from red to yellow or turbidity of the tissue culture media indicated nonsterility. Following freeze drying as a single method, all culture media, including TSB, TGB, and SDB became turbid indicating nonsterility of the liver. In all hybrid sterilization methods (PAA+GIR, EOG+GIR, and FD+GIR), neither the color of the BIs changed from red nor any turbidity was observed in TSB, TGB, and SDB media after incubation, which confirmed the sterility of the livers. Among the sterilization methods, both EOG+GIR and PAA+GIR resulted in fully sterilized bioscaffolds along with preserved mechanical properties. FD+GIR completely sterilized the liver, but also reduced the mechanical properties (Table 5).
All hybrid sterilization methods resulted in complete sterilization, while single sterilization methods failed to sterilize the livers. The mechanical properties of the livers sterilized by PAA+GIR and EOG+GIR were comparable to the control group, while FD+GIR resulted in significant reduction of the mechanical properties.
PAA, peracetic acid; GIR, gamma irradiation; EOG, ethylene oxide gas; FD, freeze drying;+means completely sterilized;−means failed to completely sterilized.
indicates the sterilization was not performed in the control liver.
Discussion
Bioscaffolds prepared using the diffusion technique are available in a variety of forms with versatile applications. They have been used to induce the repair and replacement of damaged, defective, or missing tissue. For instance, they have been utilized in the treatment of dermal wounds, lower urinary tract, or musculoskeletal tissue reconstruction in both animal and human clinical studies.32–37 Although in the majority of literature available on decellularization, the natural bioscaffolds were prepared using the diffusion technique, modern tissue engineering and regenerative medicine moves toward creating whole organ transplants through the perfusion technique.3,6,21,22,24 The resulting ECM serves as a natural biological scaffold with the same architecture and vascular network as the native organ.7,9,10,15,38
Although the general components of an ECM are similar in various tissues, some characteristics are tissue specific, including biochemical compositions, quantity and distribution of the components, and ECM's 3D architecture.9,11,15,38–41 Due to subtle differences between the ECM of various organs, decellularizing agents, timing of tissue exposure, and terminal sterilization methods should be organ specific.
Applying a harsh decellularization method may have deleterious effects on tissue properties, whereas a mild one is not able to fully decellularize the tissue. Therefore, an appropriate decellularization protocol may be difficult to obtain. Incorrect decellularization and terminal sterilization can deleteriously affect the ultrastructure, biochemical, and mechanical properties of the remaining ECM resulting in an immunologic host response.9,17
A variety of ECM scaffolds have been successfully implanted in numerous animals and human patients.6,13,19,21–23,38,42–47 The way of host response to the implanted ECM pertains to a series of biological events taking place during the remodeling process. Several factors, including circulating progenitor cells, environmental stressors, oxygen, nutrition content, and pH of the surroundings, have been considered as factors that either participate or affect the remodeling process after implantation. However, the most important contributing factor is the processing protocol by which the ECM is prepared.11,15
To our knowledge, there has been no study in the literature to determine the most appropriate approach to decellularize a liver that is similar to the human liver in terms of size and anatomy.
We applied five different treatment protocols based on previously utilized decellularization treatments for harvesting the ECM of tissues and organs. We modified the concentration of the chemicals and time of tissue exposure based on what we thought to be most appropriate for a large solid organ like the sheep liver. Considering the potential applications for both a diffused and a perfused liver bioscaffold, we performed the decellularization protocols with both perfusion and diffusion techniques and compared their efficiency of cell removal.
We noted a better outcome with the perfusion technique, which can be explained by the efficient transportation of the nutrition and oxygen supply through the vascular network toward the constituted cells of the organs. In the diffusion technique, to completely decellularize a tissue, first, we must cut it into thin pieces; thus, it loses its 3D architecture and vascular network. Although these decellularized pieces have their own utilities, they cannot be used to produce artificial organs.
To our knowledge, use of SK before organ decellularization has not been reported in the literature. As our results support, we believe that application of SK before initiation of decellularization helps lysing the remaining blood clots and opening the path through which the decellularizing solution can simply move toward the cells.
However, decellularization in perfusion subgroups of groups 1 and 5 resulted in complete decellularization irrespective of receiving SK. Therefore, decellularization protocol (decellularizing agents) seems to be an integral part in cell removal and SK has an adjunctive role.
The ammonium hydroxide solution containing Triton X-100 and gradually increasing concentration of the SDS solution, both resulted in fully decellularized constructs in perfusion subgroups, but the latter caused a significant loss of mechanical properties of the remaining ECM. Potent ionic detergents like SDS tend to disrupt the 3-D ultrastructure of the ECM, decrease the GAG content, intercept protein–protein interactions and impair the collagen integrity, which leads to reduction of mechanical properties. 17 Although several studies have applied SDS to decellularize different tissues, the mechanical properties has been assessed in limited number of studies.6,21 Recently, Uygun et al. decellularized a rat liver with SDS applying the perfusion technique. Although they reported 100% retention of collagens quantitatively, no assessment of the mechanical properties was performed and the graft function was followed for just 8 h in vivo and 24 h in an ex vivo blood perfusion system. 6
Our results show that 0.05% ammonium hydroxide containing 0.5% triton X-100 with duration of 48 h is proper for decellularizing the sheep liver tissue. In a recent study by Baptista et al., livers of different animal species were decellularized all with the same protocol, which was mainly 1% Triton-X 100 with 0.1% Ammonium Hydroxide with different tissue exposure timing. They transplanted the seeded scaffolds into the abdominal cavity of adult rats. However, they did not measure the mechanical properties of the resulting ECM in vitro nor did give any data regarding the long-term follow-up of the transplanted ECM. 22
The final mechanical properties of the scaffolds before transplantation are of crucial importance. In vivo application of SIS-ECM showed that more than 50% of the scaffold is degraded by 28 days and is completely replaced within 60 days after implantation. 10 For multilayer forms of the ECM, it takes 90–120 days for complete degradation. 11 These findings suggest that a large solid organ-derived ECM would require several months to be completely degraded and replaced by the host tissue cells. After transplantation, a liver-derived ECM to be gradually degraded, neovascularized, send signals to intended host cells, and finally completely be replaced by the host tissue, should maintain its 3D architecture and consistency for several days to months. Therefore, a sufficient mechanical property of the ECM is quite imperative.
In this study, the poorest mechanical properties were noted in group 4. The livers in this group were treated with a protocol consisting of a hypotonic and hypertonic treatment combining with Triton X-100 and SDS. Similarly, in a previous study, arteries subjected to Triton X-100 and hypotonic/hypertonic solutions showed significantly decreased mechanical properties. 48 Unexpectedly, protocol 1 resulted in higher mechanical properties compared to the control group. This can be possibly due to the lower total water content of the decellularized liver than the fresh tissue, while the ECM components especially in terms of quantity and integrity of collagens (which are the main determinants of mechanical properties) remained intact. Moreover, the collagen and sGAG content of the livers in group 1 were higher compared with the control group similar to the study by Baptista et al. A plausible explanation to this finding can be the removal of cellular components, such as cellular proteins, during decellularization. 22
The poor mechanical properties of treated livers in groups 2 and 3 are likely due to disruptive effects of Trypsin/EDTA. Trypsin/EDTA tends to decrease the elastin content and tensile strength of up to 50%. In addition, the collagen content in group 3 decreased significantly. In group 5, the reduced mechanical property of the treated livers was probably due to both loss of collagen integrity and decreased collagen quantity.
The sterility of a bioscaffold before implantation is also crucial; nevertheless, sterilization can negatively affect the mechanical properties. Thus, a proper sterilization method defines as the method that can completely sterilize the scaffold, while preserving its mechanical properties. In our study, EOG as a single method failed to sterilize the whole liver tissue. EOG has been shown to insufficiently penetrate tissue, which may be the reason for its failure to sterilize the liver. 49 Although freezing and drying both can remove a number of microorganisms, FD fails to eliminate all microorganisms especially spores and viruses. Hence, it is considered a method of preserving rather than sterilizing. The sterilization dose of 3 Mrad was unsuccessful in sterilizing the human-sized liver tissue. On the other hand, studies have shown that high dose GIR (≥4 Mrad) may cause loss of mechanical strength of the material. 50 Hence, the best measure seems to be the use of hybrid sterilization methods to both sterilize the tissue and preserve its mechanical properties. However, among hybrid sterilization methods in our study, FD+GIR reduced the mechanical strength of the liver significantly. Similarly, Haut and Powlison found significant reduction in the modulus and strength of the human patellar tendon freeze dried before irradiation. 51 In our study, PAA+GIR and EOG+GIR were noted to be the best sterilization methods.
In conclusion, based on our results, the perfusion technique was more efficient in decellularization compared to the diffusion technique. Moreover, SK was shown to have an adjunctive role in decellularization. Among decellularization protocols, protocol 1 with the perfusion technique resulted in fully decellularized livers with preserved mechanical properties. The hybrid sterilization methods of PAA+GIR and EOG+GIR were considered the best for the sheep liver. Further studies with a larger sample size are warranted to confirm these findings.
Footnotes
Acknowledgments
We would like to profoundly thank Dr. Erfan Amini and Mr. Majid Kajbafzadeh for their critical review of the manuscript. We would also like to thank Mr. Vadood Baghaei for assistance with preparation of the figures.
Disclosure Statement
No competing financial interests exist.