
Abstract
In this study, the angiogenetic effect of sintered 45S5 Bioglass® was quantitatively assessed for the first time in the arteriovenous loop (AVL) model. An AVL was created by interposition of a venous graft from the contralateral side between the femoral artery and vein in the medial thigh of eight rats. The loop was placed in a Teflon isolation chamber and was embedded in a sintered 45S5 Bioglass® granula matrix filled with fibrin gel. Specimens were investigated 3 weeks postoperatively by means of microcomputed tomography, histological, and morphometrical techniques. All animals tolerated the operations well. At 3 weeks, both microcomputed tomography and histology demonstrated a dense network of newly formed vessels originating from the AVL. All constructs were filled with cell-rich, highly vascularized connective tissue around the vascular axis. Analysis of vessel diameter revealed constant small vessel diameters, indicating immature new vessel sprouts. This study shows for the first time axial vascularization of a sintered 45S5 Bioglass® granula matrix. After 3 weeks, the newly generated vascular network already interfused most parts of the scaffolds and showed signs of immaturity. The intrinsic type of vascularization allows transplantation of the entire construct using the AVL pedicle.
Introduction
One of the core limitations for transferring most of the bone tissue engineering concepts from in vitro into in vivo environments and clinical applications is the inadequate vascularization of tissue-engineered constructs. Therefore, induction of vascularization is a crucial part of any successful bone tissue-engineering model. Nowadays, the majority of tissue engineering approaches are based on the so-called extrinsic vascular pathway. 11 In this case, the construct is vascularized from the periphery; therefore, the implantation of specimens into a site of high vascularization potential is mandatory. 12 Large-bone defects in regions with comprised vascularization require a reconstruction using vascularized bone constructs, which will be transplanted into the recipient site using microsurgical techniques of vascular anastomoses. These bone constructs rely on the so-called intrinsic vascular pathway with a defined vascular axis. An novel animal model to generate axially vascularized tissue constructs was first introduced by Erol and Spira in 1979. 13 Recently, our group managed to vascularize different bone scaffolds using this arteriovenous loop (AVL) model.14,15 We also evaluated different angiogenic growth factors in this AVL model to enhance angiogenesis, and we were able to show an increased survival of osteoblasts in this model compared to extrinsic vascularized scaffolds.16–18 45S5 Bioglass® has been used to develop bone tissue scaffolds, and the effects of Bioglass® dissolution products to support angiogenesis by secretion of vascular endothelial growth factor (VEGF) have been reported. 19 However, the combination of 45S5 Bioglass® with the AVL model has not been described to date.
To create transplantable vascularized bone constructs, this study aims to investigate the axial vascularization of particulated 45S5 Bioglass using the AVL model in the rat.
Materials and Methods
Animals
Six male Lewis rats (Charles River Laboratories), each weighting 200–300 g, were used. All experiments were carried out in compliance with the animal care committee of the University of Erlangen-Nuremberg and the Government of Mittelfranken, Germany. All procedures were performed by the same microsurgeon (A. B.) under sterile conditions.
Operative procedures
Surgical procedures were performed under general anesthesia using Isoflurane (Baxter) using an operating microscope (Karl Zeiss). The AVL model has been described previously. 14
Briefly, the left femoral vessels were exposed in the medial thigh through an incision from the groin to the knee. After separation of the femoral vein and artery, a 2-cm-long femoral vein graft from the contralateral leg was interposed between the recipient left femoral vessels, creating an AVL. The microvascular anastomoses were performed using 11-0 sutures (Ethicon). The Teflon chamber was filled with the first half of the 45S5 Bioglass-based granula matrix and fibrin gel with a fibrinogen concentration of 10 mg/mL and a thrombin concentration of 2 I.U./mL. Afterward, the AVL was placed on the matrix, and the chamber was filled with the second half of the Bioglass®/fibrin gel matrix (Fig. 1). Finally, the lid was closed, and the chamber was sutured to the thigh musculature using 3-0 Prolene sutures (Ethicon).
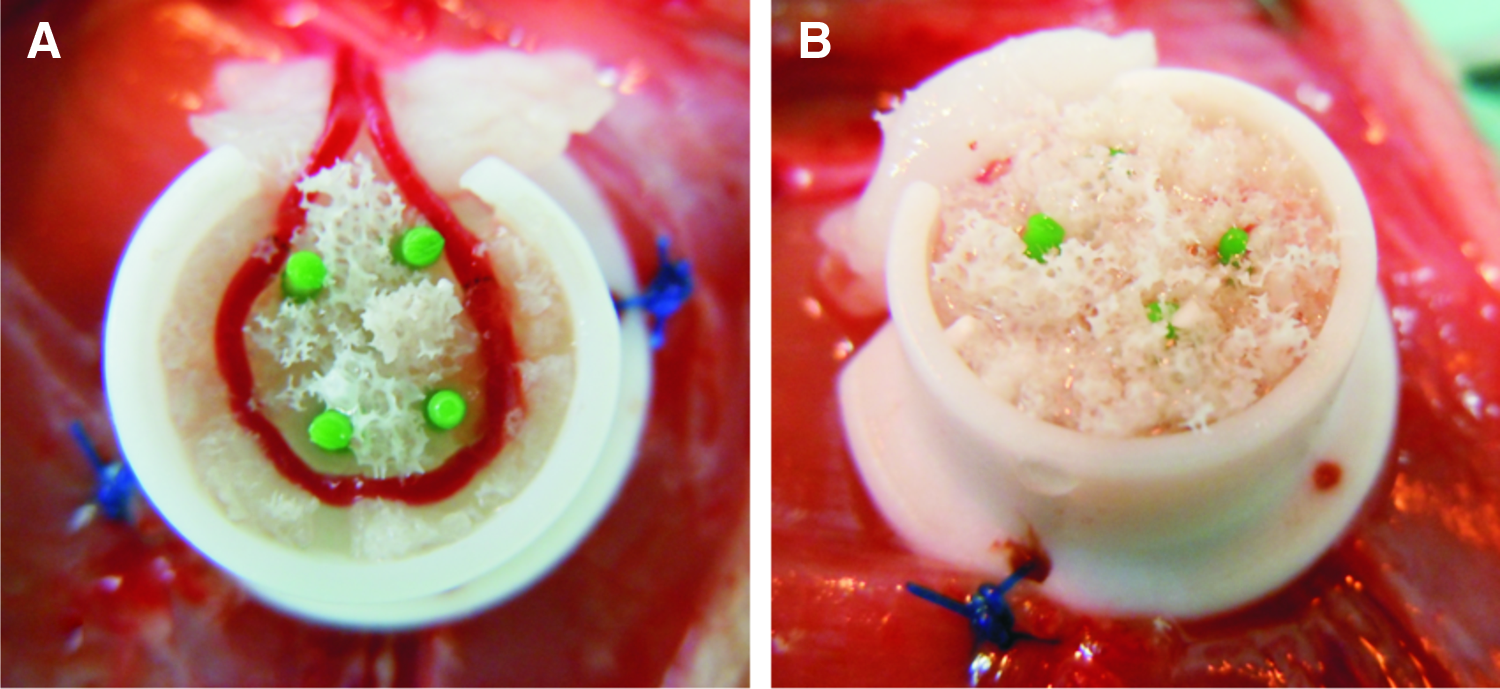
The arteriovenous loop was placed in the Teflon isolation chamber that was filled with the sintered 45S5 Bioglass®-granulated matrix and fibrin gel with a fibrinogen concentration of 10 mg/mL and a thrombin concentration of 2 I.U./mL.
The explantation interval was 3 weeks after the implantation procedure. All constructs were investigated by means of microcomputed tomography (μCT), histological, and morphometrical analysis.
Isolation chamber and composition of the matrix
The isolation chamber was made of heat-resistant medical-grade Teflon with an inner diameter of 10 mm and a height of 10 mm and a round lid. Inside the chamber, four plastic tubes were inserted to prevent a luxation of the AVL.
The matrix was comprised of 45S5 Bioglass® granules fabricated following the same procedure developed to make scaffolds, based on sintered Bioglass® powder. 19 In this process, melt-derived Bioglass® particles (mean size 5 μm) were used to fabricate scaffolds using the foam replica technique, as described elsewhere. 19 Briefly, a polyurethane foam (Recticel) was immersed in a Bioglass® containing slurry. After drying at 60°C for 24 h, the foams were sintered at 1050°C for 140 min. The densified scaffolds were then crushed to small prismatic pieces of size of 1–2 mm to obtain sintered Bioglass® granules. These granules exhibit a highly crystalline structure with Na2Ca2Si3O9 as main crystalline phase. 19
The fibrin gel (Tisseel VH S/D; Baxter Healthcare S.A.) had a final fibrinogen concentration of 10 mg/mL and a thrombin concentration of 2 I.U./mL. To delay fibrinolysis, aprotinin was added to the fibrin gel with a concentration of 1500 K.I.E./mL.
Explantation procedures
Three weeks after the implantation of the AVL, animals were perfused using Microfil® MV-122 (Flowtech). Therefore, the aorta and caval vein were surgically exposed under general anesthesia, and the aorta was flushed with 150 mL heparin solution and subsequently with 20 mL yellow Microfil® (MV-122) containing 5% of MV Curing Agent. The rat was then placed in 4°C for 24 h, and the specimens were explanted, macroscopically inspected, and fixed in a 3.5% formalin solution for histological processing.
Microcomputed tomography
After fixation in formalin, all specimens were decalcified in ethylenediaminetetraacetic acid (EDTA) for 3 weeks. Afterward, the constructs were investigated using μCT.
To reveal the microstructure and vessel orientation, samples were examined with a high-resolution μCT analysis using a Skyscan 1172 (Skyscan B.V.) with an 11-MP detector. The tungsten tube was operated at a voltage of 80 kV and a current of 100 μA using no additional source filtering. The scan was performed with a rotation step of 0.4° over 180° with a resolution of 6.9 to 8 μm/voxel depending on the sample size.
Measured raw data sinograms were reconstructed with tomographic reconstruction software (NRecon Client and Server 1.6.4 with GPU support; Skyscan), which calculates the two-dimensional (2D) cross-sections after adjusting gray value levels. The three-dimensional (3D) visual images and STL-models were generated using imaging software (Amira 5.4.1; Visage Imaging) after labeling with a global threshold and using a 26-side growing algorithm on all layers. After binarization, additional skeletonization (Module autoskeleton Amira) using thinning algorithms was performed to determine the network structure of the vessels. The vessel network was divided into segments with individual length and mean diameter. Using a histogram class width of 1 μm, an accumulated vessel length was calculated for each vessel radius class.
Histological analysis
After μCT evaluation, all tissues were dehydrated in graded ethanol and embedded in paraffin. Cross sections (3 μm) were obtained from two planes perpendicular to the AVL axis using a Leica microtome (Leica Microsystems). Cross sections were stained with hematoxylin and eosin (H&E) and Masson's trichrome using standard protocols. Digital photographs of each H&E-stained cross section were obtained using a Leica Microscope (Carl Zeiss) and digital camera. Overviews of the whole specimens were acquired under 25× magnification with subsequent merging using Photoshop software (Adobe Systems Incorporated). Afterward, the cross-section area was measured using ImageJ (ImageJ, National Institutes of Health). To determine the vascularization of each construct, all cross sections were divided into 14 equal sectors, 6 at the periphery, 4 at the central part of the section, and each 2 at the artery and vein. Digital photos of each sector were taken under 200× magnification, and the number of blood vessels, standard deviation of blood vessel size, and average size of blood vessels were determined by bimodal rendering using a standardized threshold.
Immunohistochemistry: lectin BS-1, ED1, and alpha-smooth muscle actin
Cross sections of each specimen were immunochemically stained as described before. 17 Briefly, biotinylated lectin (BS-1; Sigma) was applied at 1:100 dilution, followed by the Streptavidin AB Complex/HRP detection system (Dako GmbH).
ED1 was stained as described elsewhere. 17 Primary anti-ED1 antibody (Serotec) was applied (1:300), followed by a goat anti-mouse secondary antibody (Dako GmbH) at 1:20 and APAAP complex (Dako GmbH) at 1:50.
For alpha-smooth muscle actin (ASMA) staining, a mouse anti-ASMA primary antibody (Dako GmbH) was applied at 1:300 dilution, followed by an anti-mouse anti-rabbit secondary antibody (Invitrogen) as described before. 17
Statistical analysis
Data were expressed as mean±standard deviation. Statistical analysis was performed using Excel Software (Microsoft Corporation)
Results
Matrix, surgery, and animals
No animal died during the operative and postoperative period of time. There were no major complications detectable such as hematomas, infections, or wound dehiscence. All of the implanted AVLs were patent at explantation.
Macroscopic appearance
At explantation, chambers were surrounded by fibrous tissue in all animals. Fibrin gel was partially replaced by vascularized connective tissue, whereas the Bioglass® granula showed no signs of degradation or resorption. Vascularization of matrices and patency of the AVLs were visible because of yellow filling of functional vessels with Microfil® (Fig. 2).

Macroscopic appearance upon explantation: After removing the Teflon isolation chamber, Bioglass® granules showed no signs of degradation or resorption. Vascularization of matrices and patency of the arteriovenous loops were visible because of yellow filling of functional vessels with Microfil®. Color images available online at
Histological evaluation
Abundant connective tissue was generated in all animals at the explantation time point. The newly formed tissue was localized around the vascular pedicle without predominance in the venous or arterial part of the AVL (Fig. 3). Functional vessels were observed by black filling of lumina with Microfil® in the connective tissue. Vessels originating from the vascular axis were found in all animals, penetrating the construct without reaching the central part of the specimens at this time point. The connective tissue was filled with immature vascular sprouts and a variety of different cells such as neutrophils and fibroblasts. Macrophages could be detected using ED1 staining without showing multinucleated giant cells (Fig. 4). Newly formed vessels could be also verified using Lectin and ASMA immunohistochemical stainings, which showed endothelial cells and smooth muscle cells inside the vessel walls. In the center and the periphery of the specimens, the fibrin gel matrix was apparent in all animals with a marked absence of vascularized connective tissue compared to the area around the vascular pedicle. The 45S5 Bioglass® granula matrix was still apparent and evenly distributed in all constructs. Masson's trichrome staining failed to detect newly formed bone in all animals.
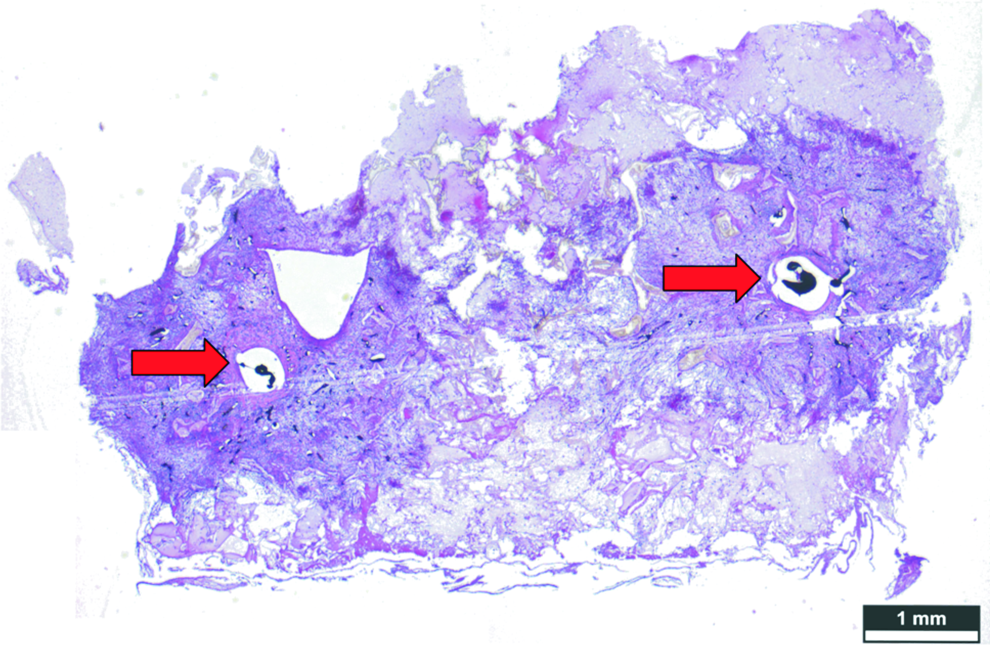
Hematoxylin and eosin stainings: The newly formed tissue was localized around the vascular pedicle (arrows) with a reduction in the central part and the periphery of the arteriovenous loop. Functional vessels were observed by black filling of lumina with Microfil in the connective tissue. Magnification ×25. Color images available online at
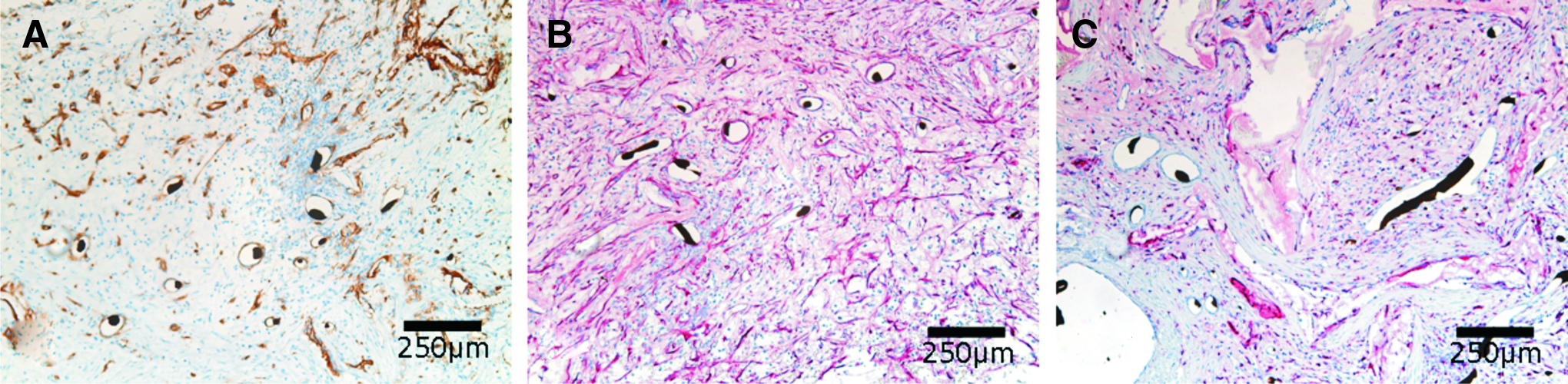
Immunhistochemical stainings: Endothelial cells could be detected using Lectin stainings
Microcomputed tomography
MicroCT evaluation showed patent AVLs in all animals. Capillary sprouts originating from the vascular axis were visible in all constructs penetrating the matrix, whereas a reduced vascularization was evident in the center and the periphery of the specimens (Fig. 5). After decalcification, some 45S5 Bioglass® granules were still apparent in the images obtained by μCT.

MicroCT analysis strategy of accumulated vessel length with regard to vessel diameter: Measured raw data sinograms
Morphometrical analysis
Histology
At the explantation time point, the cross-section area averaged 29±6 mm2. Quantitative analysis of blood vessel distribution revealed an equal number of blood vessels in the arterial and venous parts of the constructs (43±61 vessels/cross section (CS) vs. 43±23 vessels/CS) with a decrease in the central part of the specimen (27±24 vessels/CS) (Fig. 6). The average vessel area was determined at 658±195 μm2.
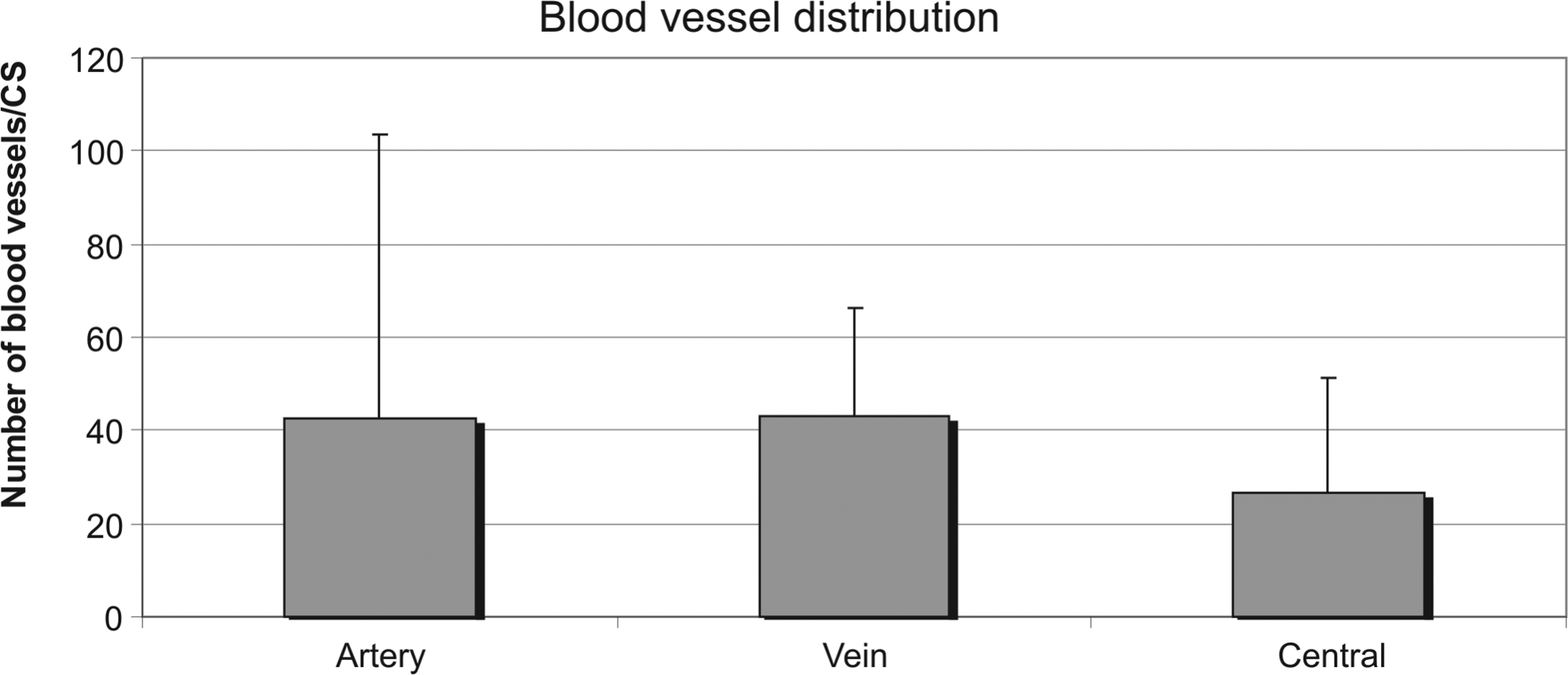
Morphometrical analysis of blood vessel distribution of cross sections. At 3-week explantation time point, there was an equal number of blood vessels in the arterial and venous parts of the constructs with a decrease in the central part of the specimens detectable.
Microcomputed tomography
Evaluation of accumulated vessel lengths in relation to the vessel radius displayed a significant increase of the vessel length of small sprouts compared to larger vessels. Most sprouts showed a vessel radius of around 10 μm, indicating a very immature vascular network (Fig. 7).
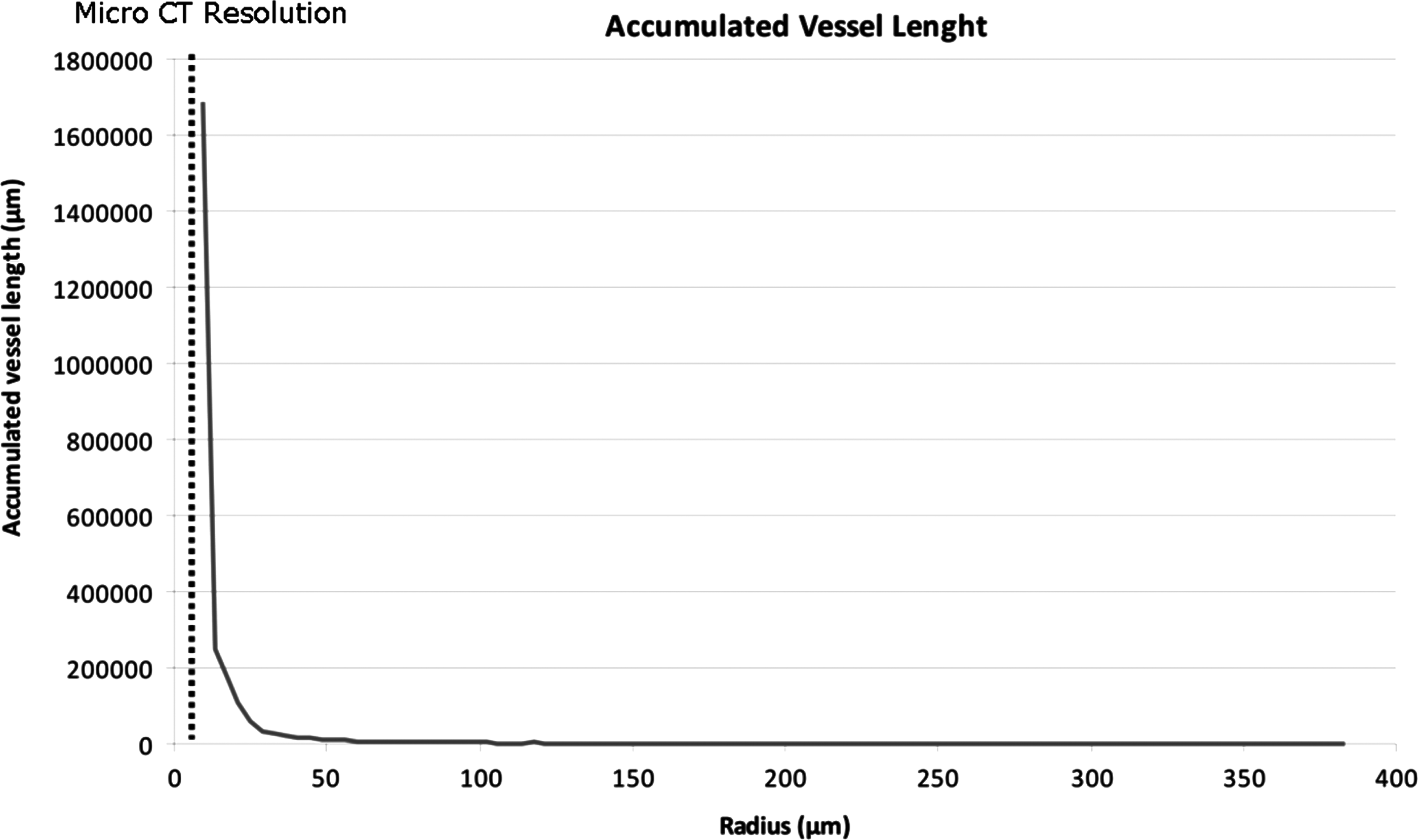
Microcomputed tomography (μCT) analysis of accumulated vessel length with regard to the vessel radius. The histogram displays a peak at a vessel radius of 10 μm with a rapid decrease in the vessel length in larger vessels. The μCT had a resolution of 6.9 to 8 μm/voxel.
Discussion
Large-bone defects still represent a major challenge for orthopedic and plastic surgeons. Vascularized autologous bone grafts are still the gold standard for the treatment of large osseous defects with exposed structures such as nerves, vessels, or tendons, especially in the regions of compromised perfusion after trauma or irradiation. Major disadvantages are the sometime-significant donor-site morbidity and the limitations regarding shape and quantity. 20 Therefore, researchers place a great deal of hope and expectation in bone tissue engineering to overcome these problems. 21
Prevascularization strategies are well known in plastic surgery for decades, and the technique was first applied in a clinical setting by Shen in 1982. 22 It is based on a simple principle: After vascularization of a tissue volume by a defined vascular axis, which is introduced into the construct at a site of good perfusion, the tissue volume can be transferred into the recipient site using microsurgical techniques. From the reconstructive surgeon's point of view, the creation of the AVL is associated with a minimal donor-site morbidity compared to vascularized autologous bone grafts such as fibula, scapula, or iliac crest.
The AVL model represents a model for tissue prefabrication because of its defined vascular axis leading to intrinsically vascularized tissue constructs. The model is based on an AVL created in the medial thigh of the rat with an interposed vein graft from the contralateral leg. After its first introduction in 1979, the AVL model became one of the most promising tools to analyze angiogenesis arising from a defined vascular axis. It has been shown that the arterovenous loop enhanced neovascularization in a higher degree than an arteriovenous shunt. 23 The Teflon isolation chamber prevents the scaffolds from extrinsic vascularization from the surrounding tissue. 24 Therefore, the constructs are exclusively vascularized from the vascular axis. The reason for the arising angiogenesis from the large femoral vessels in this model has not been completely determined. The initial surgical trauma as well as the hypoxic tissue volume and maybe the imposed pulsatile shear stress within the AVL could be responsible for the vivid vascular sprouting.
Using the AVL model in combination with the Teflon isolation chamber, we were able to show for the first time axial vascularization of 45S5 Bioglass granules made by the same procedure used for Bioglass-based scaffolds. 19 We used an explantation time point of 3 weeks because of previous studies of our group showing direct luminal sprouting in the AVL model between days 10 and 14. 25 It has been observed that using a plain fibrin gel matrix in the AVL model with or without adding angiogenic growth factors, after 1 week, no luminal sprouting occurs. 17 Moreover, recent studies have demonstrated axially vascularization of different bone scaffolds such as custom-made processed bovine cancellous bone matrix, particulated porous hydroxyapatite, and beta-tricalcium phosphate matrix using the AVL model.14,15 It is known that the venous and the graft segments of the AVL are responsible for early angiogenesis up to day 14. 25 The thick tunica media of the artery was thought to avoid vascular sprouting at early stages after AVL construction. In this study, there was no detectable difference between the arterial and venous parts of the AVL in the histological evaluation. This might be due to the explantation time point of 3 weeks. In previous studies using a particulated porous hydroxyapatite and beta-tricalcium phosphate matrix, a predominance of neocapillaries arising from the venous part of the AVL was found at 2 weeks, whereas no further difference was detected at the 4-week explantation time point between the arterial and venous AVL segments. 15
We determined the vascular network both histologically and by microcomputed tomography. Histology can evaluate a limited number of 2D cross sections and therefore yields a 2D approximation, while μCT offers the opportunity to reconstruct and morphometrically evaluate the vascular network of the entire specimen. In this study, the 3D evaluation by μCT displayed a dense network of neocapillaries originating from the AVL. Morphometrical evaluation revealed a uniform shape and size of the sprouts, indicating that the maturation process has not yet occurred. The limited variability in the diameter of capillary lumina shows that the vascular network is in the early stages of remodeling. This is in agreement with previous corrosion cast studies where neocapillaries displayed a diameter between 10 and 15 μm. 25 The μCT evaluation possesses a resolution of 6.9 to 8 μm/voxel depending on sample size; therefore, vessels with a minimum radius of 9.6 μm were detected in comparison with scanning electron microscopy of corrosion casts in the previous study. In this study, histological and μCT findings could be positively correlated, showing an average vessel size of 658±195 μm2 in the histological evaluation and a maximum in the accumulated vessel length at a vessel radius of 10 μm in the μCT investigation.
Sintered Bioglass® is a slowly biodegradable material in body fluid, because its crystalline phase can transform into an amorphous calcium phosphate. 4 In this study, we were not able to show degradation or resorption of the Bioglass® matrix. This might be due to the short explantation time point and/or because of the limited vascularization of the matrices, especially in the beginning of the study. As expected, we were also unable to detect newly formed bone in the explanted specimens, although Bioglass® is known to be osteoconductive and to enhance bone generation.4,5 This could be explained by the absence of osteogenic growth factors and/or osteogenic cells in this study, the relatively short explanation time point of 3 weeks as well as by a lack of biomechanical stimulation in the isolation chamber.
In this study, we used fibrin gel as a binding agent of the particulated matrix. Fibrin gel has also the ability to act as a possible release system for growth factors such as angiogenic or bone morphogenic growth factors.26,27 Previous studies have shown that fibrinogen concentration mainly determines the degradation of the fibrin gel part of the matrix and also affects the replacement with vascularized connective tissue. 28 We used a low, but well-studied, fibrinogen concentration of 10 mL/mg in this study to achieve a fast vascularization of the scaffolds. The polymerization time of the fibrin gel highly depends on the thrombin concentration. Therefore, we used a low thrombin concentration of 2 I.E./mL to obtain an evenly distributed fibrin gel matrix between the Bioglass® granula. We also used aprotinin in a concentration of 1500 I.U./mL to preserve the fibrin matrix in the first days after AVL implantation due to its known ability to slow down fibrinolysis via inhibiting plasmin. 29
Recently, we were able to show an increased neovascularization in the AVL model by the use of fibrin gel-immobilized VEGF165 and basic fibroblast growth factor (bFGF).15,17 The incorporation of 45S5 Bioglass® should lead to increased secretion of VEGF in vitro and increased neovascularization in vivo, as documented in the literature. 30 In a recent investigation, we were able to prove the possible combination of the intrinsic AVL model with an extrinsic vascular pathway using a newly developed porous titanium chamber to allow additional extrinsic vascularization of scaffolds via incorporated pores in the chamber design. 31 Further studies should combine 45S5 Bioglass® scaffolds with angiogenic growth factor and/or porous chambers to accelerate vascularization of matrices. Also, the use of other bioactive glass compositions containing specific metallic ions with angiogenic effect (e.g., Co 32 and Cu 33 ) will be considered, based on the body of evidence available 34 about the cellular response to specific metallic ions released from bioactive glasses.
Conclusions
This study shows for the first time axial vascularization of a particulated sintered 45S5 Bioglass® matrix using the AVL model of the rat. After 3 weeks, the newly generated vascular network already interfused most parts of the scaffolds and showed signs of immaturity. The intrinsic type of vascularization allows transplantation of the entire construct using the AVL pedicle. In the future, a combination of 45S5 Bioglass® scaffolds with angiogenic growth factors and/or porous chambers might accelerate the vascularization of matrices for bone tissue engineering.
Footnotes
Acknowledgments
This study was supported by research grants from Xue-Hong and Hans Georg Geis, Baxter Healthcare Corporation, Deutsche Forschungsgemeinschaft DFG (KN 578/2-1), as well as the University of Erlangen-Nuremberg (ELAN Program) and the “Emerging Fields Initiative” of the University of Erlangen-Nuremberg. The authors thank Mr. Peter Reinhardt for production of the Teflon chambers. This work contains parts of Phillipa Newby's doctoral thesis.
Disclosure Statement
No competing financial interests exist.