
Abstract
Scaffolds seeded with multipotent precursor cells were hypothesized to heal critically sized bone defects. However, the success of this concept was limited by low cell survival after transplantation due to a lack of nutrients and oxygen. In vivo prevascularization of scaffolds before cell seeding may improve cell survival, yet the best seeding technique and time point of cell application remain elusive. Thus, the aim of this study was to compare different strategies. Demineralized bone matrix scaffolds were implanted around the saphenous arteriovenous (AV) bundle in nude mice. In vivo seeding was performed 0, 5, or 21 days after implantation using enhanced green fluorescent protein (eGFP)-expressing mesenchymal stem cells (MSCs). Cells were applied either by injection or the repetitive dripping technique. In vitro seeded and subcutaneously implanted scaffolds served as controls. Fourteen days after cell application, the fluorescence intensity of transplanted cells and the extent of newly formed vessels were quantified. We found that the AV flow through model as well as cell application increased vessel formation. In vitro seeding resulted in significantly higher cell numbers than in vivo seeding. With increasing time of prevascularization, the number of cells declined dramatically. In vivo seeding by cell injection was superior to the repetitive dripping protocol. On subcutaneously implanted scaffolds, significantly, more cells were found than on axially perfused scaffolds. We conclude that in vitro seeding is more efficient compared to the two novel in vivo seeding techniques of prevascularized scaffolds. With increasing time of prevascularization, the seeding efficiency for the in vivo methods further decreases, presumably due to the ingrowth of connective tissue. Even though, the presence of MSCs and the longer period of prevascularization enhances vessel formation, this conceivable advantage is limited supposedly by the inferior seeding efficiency.
Introduction
D
In the present study, we induced prevascularization using an AV flow through in a murine model. We compared two novel in vivo cell-seeding strategies at three time points: day 0, when no connective tissue had formed, but no vessels had yet grown into the scaffolds; day 5 after inducing vascularization, when little amount of connective tissue was present and only a small number of vessels had formed; and day 21, when more vessels had formed along with the presence of more connective tissue.
Materials and Methods
Cells, cell culture, and scaffolds
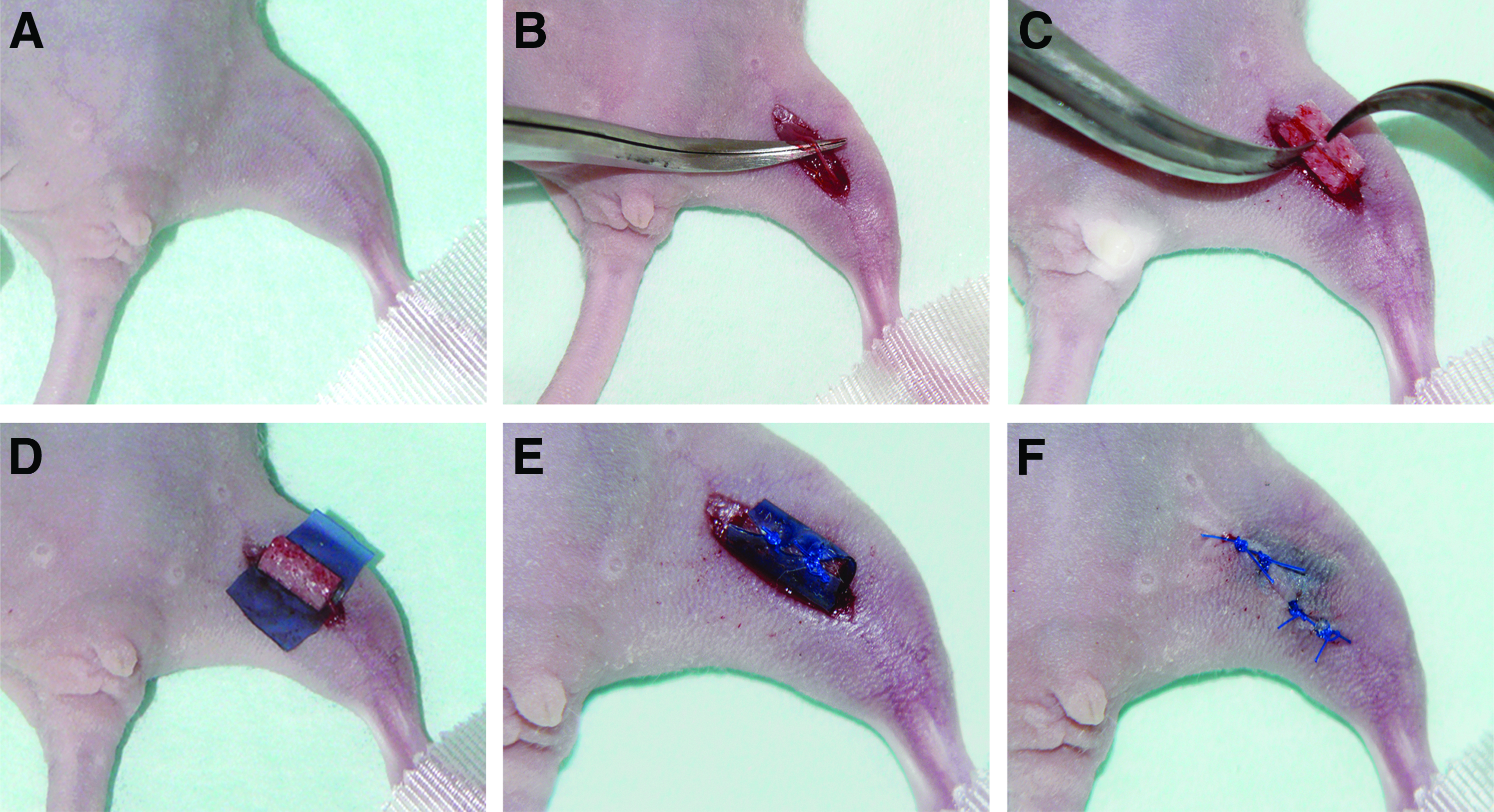
All experiments were performed using an immortalized clonal expanded hMSC line, which is overexpressing human telomerase reverse transcriptase (hTERT) along with an enhanced green fluorescent protein (eGFP). An exact characterization of these cells has been published elsewhere. 12 In brief, single cell picked (SCP) cell clones of hMSCs were transduced with hTERT using lentiviral gene transfer. One clone (SCP-1) was selected and cultured. All cells used for this study were among passage 85–87. The SCP-1 cell line was additionally transduced with eGFP (SCP-1 eGFP). Cells were cultured in minimum essential media Alpha GlutaMAX™ culture media (Invitrogen, Darmstadt, Germany), supplemented with 10% fetal bovine serum (Sigma-Aldrich, St. Louis, MO) and 40 IU/mL penicillin/streptomycin (PAA Laboratories, Pasching, Austria) in a humidified incubator at 5% CO2 and 37°C in a T-225 flask (Nunc, Langenselbold, Germany). A confluency of 50% was never exceeded. Before in vivo seeding, cells were trypsinized using Trypsin (0.5 g/L) with EDTA-Na (0.2 g/L) dissolved in PBS (PAA Laboratories) and diluted in complete media to a final concentration of 6,250,000 cells/mL and stored in 15-mL tubes (Sarstedt, Nümbrecht, Germany) until the operation procedure. Cylindrical bovine demineralized bone matrix scaffolds (Tutogen, Neunkirchen, Germany) of 3 mm in diameter and 6 mm of height were used for all experiments. The scaffolds contained a central drill hole of 0.5 mm in diameter along the central axis of the cylinder and were slotted lengthwise (Fig. 1C), leaving a space for the saphenous vessel bundle in the center.
Surgical procedure for implantation of the scaffolds around the saphenous vessel bundle.
In vitro seeding
The in vitro seeding was performed according to a standard protocol. 13 In brief, 250,000 cells were suspended in 1 mL complete media together with the scaffold in a 1.5-mL eppendorf tube (Eppendorf, Hamburg, Germany). The tube was turned every 20 min for 3 h in total and placed in 96 wells with a fresh medium 24 h before operation.
Animals and experimental setup
All animal experiments were carried out in accordance with institutional and national guidelines for the care and use of experimental animals and with permission of the Animal Ethics Committee. Fifty four athymic nude mice (Harlan, Borchen, Germany) were divided into nine groups. A detailed description of the groups is shown in Table 1. Three time points after prevascularization were evaluated, namely, 0, 5, and 21 days. At each time point, cells were seeded either by injection of cells into scaffolds or by repetitive dripping of cells onto the scaffold. Each mouse received a control scaffold in a dorsal subcutaneous pocket, which was treated analogously to the scaffold that was placed around the vessels. At each time point, an empty scaffold group was included. On day 0, the in vitro-seeded scaffold group served as control.
In all animals, two scaffolds were implanted, one around the saphenous vessel bundle and one subcutaneously on the back. Both scaffolds were treated identically with respect to the seeding protocol and harvested 14 days after the seeding procedure.
Surgical procedure and histology
For all surgical procedures, mice were anesthetized by injecting a mixture of fentanyl (0.05 mg/kg), midazolam (5 mg/kg), and medetomidin (0.5 mg/kg) intraperitoneally. During the operation procedure, 100% of oxygen was provided and the operation site was disinfected. First, mice were placed in a prone position and an incision of 5 mm length was set medially on the back of the mice. A subcutaneous pouch was created to hold the scaffold. The scaffold was placed in this pouch and in contrast to the scaffolds implanted around the saphenous vessels, no silicone foil was placed around the scaffolds implanted on the back. Consecutively, the wound was closed using an interrupted, nonresorbable suture. Subsequently, mice were placed in a dorsal position and a 15-mm incision was set medially over the femur to expose the saphenous vessel bundle of the hind leg (Fig. 1A). The vessel bundle was dissected (Fig. 1B) and the scaffold was placed around the saphenous vessels (Fig. 1C). The construct was then wrapped in a silicone foil (Fig. 1D, E) and the wound was closed by an interrupted, nonresorbable suture (Fig. 1F). All operations and seeding procedures were performed by the same surgeon. All scaffolds were harvested 14 days after cell application. For in vivo seeding, the wound and the silicone foil were opened and 250,000 cells diluted in 40 μL media were applied by either repetitive dripping or injection using a 1-mL heparin syringe (BD, Basel, Switzerland). Two techniques for in vivo seeding were evaluated. The repetitive dripping seeding strategy was developed in analogy to the in vitro protocol. The cell solution was dripped onto the scaffold. The solution that was caught in the silicone foil was collected in a syringe and again dripped onto the scaffold until no more cell solution was remaining. For the injection method, four standardized injection sites were used. Subsequently, the silicone foil and the wound were closed using a suture as described previously. Scaffolds injected with cell-free media served as control groups. Fourteen days after the seeding procedure, a cardiac India ink injection was performed and scaffolds were harvested. To this end, a 15-mm thoracotomy was made and the heart was exposed. Forty microliters of heparin (Braun, Melsungen, Germany) followed by 0.5 mL of India ink (Sanford, Hamburg, Germany) was injected into the left ventricle to visualize the vessels in histology cuts. Explanted specimens were fixed in 4% paraformaldehyde for 12 h and afterward treated with a sucrose solution (3 h in 5% sucrose, 3 h in 10% sucrose, and 12 h in 20% sucrose). Specimens were frozen in tissue-freezing media (Jung, Nussloch, Germany). Serial cuts were prepared with a slice thickness of 16 μm. Ten sections were obtained from both ends and the middle portion of the scaffolds adding to 30 sections per scaffold. After acquisition of the fluorescence images, the same sections were stained with eosin according to a standard protocol for quantification of vessels.
Microscope and filters
For image acquisition, an Axiovert S100 (Zeiss, Jena, Germany) microscope equipped with a 75 W/2 xenon lamp and a Zeiss Fluar objective (10×/0.50; Zeiss) for fluorescence and an eosin image were used. For detection of the scaffolds' autofluorescence, a triple band filter set (F61-002; AHF, Tübingen, Germany) was used for the blue light spectrum. For detection of eGFP fluorescence, a small band filter set (excitation: 488/6 nm, dichroic mirror: 495 nm, emission: 510/10 nm; AHF) was used.
Image acquisition
Images were acquired using a Zeiss black and white digital camera (AxioCam MR; 1388×1040 pixels) and processed with the Zeiss AxioVision software (Release 4.8.2). The image size was reduced to a working resolution of 700×600 to reduce the illumination gradient within the image as described previously. 14 For large field microscopy, an automated microscope stage (SCAN IM 130×100-1 mm; Märtzhäuser-Wetzlar GmbH & Co. KG, Steindorf, Germany) was used. Three sections from both ends and the middle, adding to nine sections per scaffold, were selected from each scaffold according to their best histological appearance in terms of cutting artefacts. Each entire section was imaged using 7×8 FOVs to ensure a complete illustration of the section adding to a total area of 63.62 mm2 per scaffold. The exposure time for the fluorescent images was set to 250 ms according to preliminary experiments (data not shown). Eosin-stained sections were imaged by bright field microscopy. All images were exported as 16-bit gray value Tiff files.
Image analysis, algorithm tools, and quantification of vessels
The automated image analysis was performed using ImageJ (Version 1.43g). 15 The amount of cells being present was estimated by the mean relative fluorescence intensity (RFI) as described previously. 16 In brief, two images of the same region were acquired, one of the labeled cells and one of the scaffold (blue autofluorescence spectrum). A minimum image of both pictures was calculated using ImageJ and this newly created image was subsequently subtracted from the original image of the labeled cells. 16 For quantification of the vessel number, the same sections were stained using eosin. Each cross section was evaluated manually using standardized monitor settings and magnification by two independent and blinded observers. The number of lumina filled with India ink per cross section was counted, and mean values for both observers were calculated for each scaffold. If a vessel was cut tangentially, it was counted as one.
Statistical analysis
Statistical analysis was performed using GraphPad Prism 5 (GraphPad Software, La Jolla, CA). Different groups were compared to the in vitro seeding technique on day 0 with a one-way ANOVA test. Direct comparison for newly formed vessels within each day and the control group was performed with a Mann–Whitney-U test. Moreover, to calculate differences of vessel ingrowth within scaffolds around the femoral vessel bundle and subcutaneously implanted, a one-way ANOVA test was used. A value of p≤0.05 was considered significant.
Results
The murine model
The implantation procedure around the saphenous vessels required microsurgical instruments and magnification (Fig. 1). The operation itself lasted ∼15 min from cut to suture. There were no intraoperative complications, such as damage to the vessels. One animal died within 1 h after the operation due to complications of the anesthesia, all other animals survived well with full weight bearing, a regular gait pattern, and without a weight loss.
Qualitative manual histological analysis
The qualitative manual histological analysis of the scaffolds indicated that in vitro seeding did not only produce the highest cell numbers, but also accomplished the most homogeneous cell distribution throughout the scaffolds (Fig. 2A). In contrast, analysis of the cell injection group revealed a patchy cell distribution (Fig. 2B). The localization within the scaffold varied greatly. For all groups receiving cells by repetitive dripping, cells were mainly gathered in the outer region of the scaffolds and there were literally no cells in the inner regions of the scaffold (Fig. 2C). The longer the scaffolds remained implanted in vivo the more the amount of connective tissue within the scaffolds increased.

Representative fluorescence microscopy images of scaffolds seeded on day 0 and harvested 14 days after implantation.
Comparison of in vitro to in vivo seeding without prevascularization (day 0)
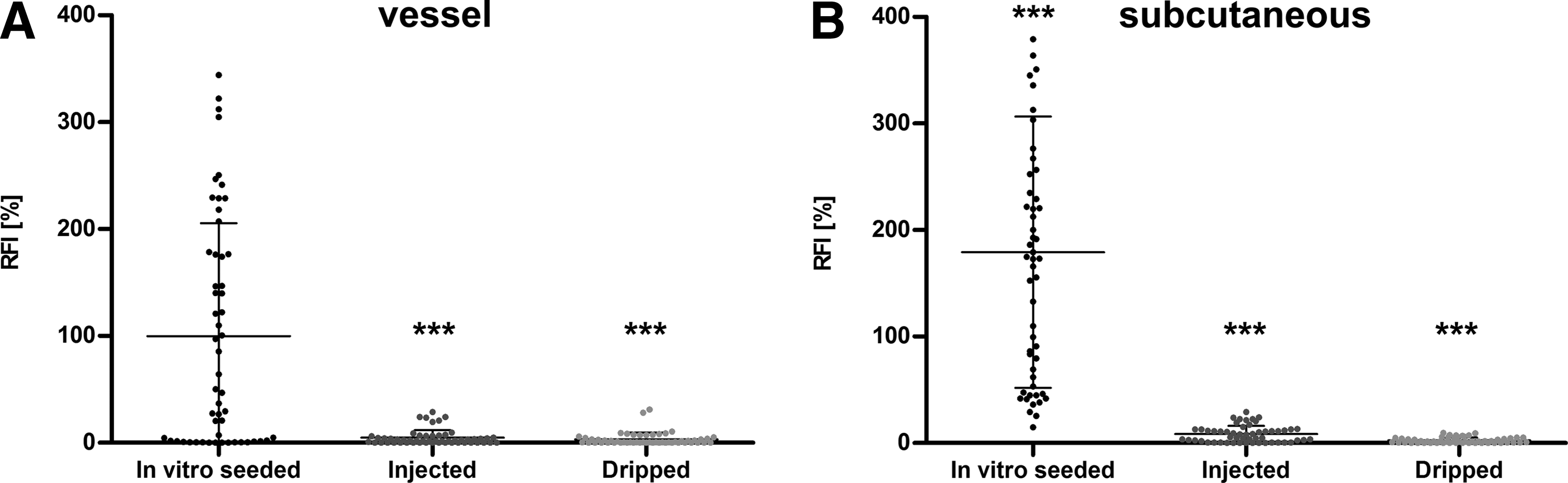
To evaluate the new in vivo seeding techniques, we first compared them to our standard in vitro seeding protocol. In this control group, cells were seeded on scaffolds 24 h before implantation. Alternatively, cells were seeded in vivo immediately after implantation of the scaffolds, either by the injection or the repetitive dripping method. All scaffolds were harvested after a 14-day period in vivo. The mean fluorescence intensity of in vitro seeded scaffolds around the saphenous vessel was considered 100%. For evaluation, a total of 3024 fields of view were analyzed per group. When cells were injected into the axially perfused scaffolds in vivo, after 14 days, the RFI was 4.8%±7.2% compared to the in vitro seeding group (p<0.0001, Fig. 3A). Repetitive dripping produced 3.3%±6.1% of RFI (p<0.0001; Fig. 3A). The subcutaneously implanted scaffolds that were seeded in vitro yielded an RFI of 179.2%±127.3% (Fig. 3B). Also here, injection and repetitive dripping produced significantly lower cell numbers with 4.1%±3.8% and 2.5%±2.6%, respectively, (p≤0.0001; Fig. 3B).
Comparison of three different methods of cell application for nonprevascularized scaffolds (day 0): Scaffolds were then placed around the saphenous AV bundle
Seeding efficiency after prevascularization: comparison of different seeding strategies
In this experiment, the fluorescence intensity of the group receiving cells by injection into the axially perfused scaffold on day 0 was considered 100% and the RFI was calculated for the 5- and the 21-day groups. Within the axially perfused scaffolds, the highest RFI resulted when scaffolds were seeded on day 0. The injection group yielded 100.0%±152.0% and the repetitive dripping group resulted in 70.0%±134.5% (p≤0.001; Fig. 4A). A highly significant reduction (p≤0.001) of the RFI was observed for injection and repetitive dripping of cells on day 5, respectively (9.3%±33.8% and 8.6%±26.6%; Fig. 4A). The RFI further decreased when seeded on day 21 for both, the injection (0.4%±0.8%) and repetitive dripping group (1.0%±4.0%) (Fig. 4A).
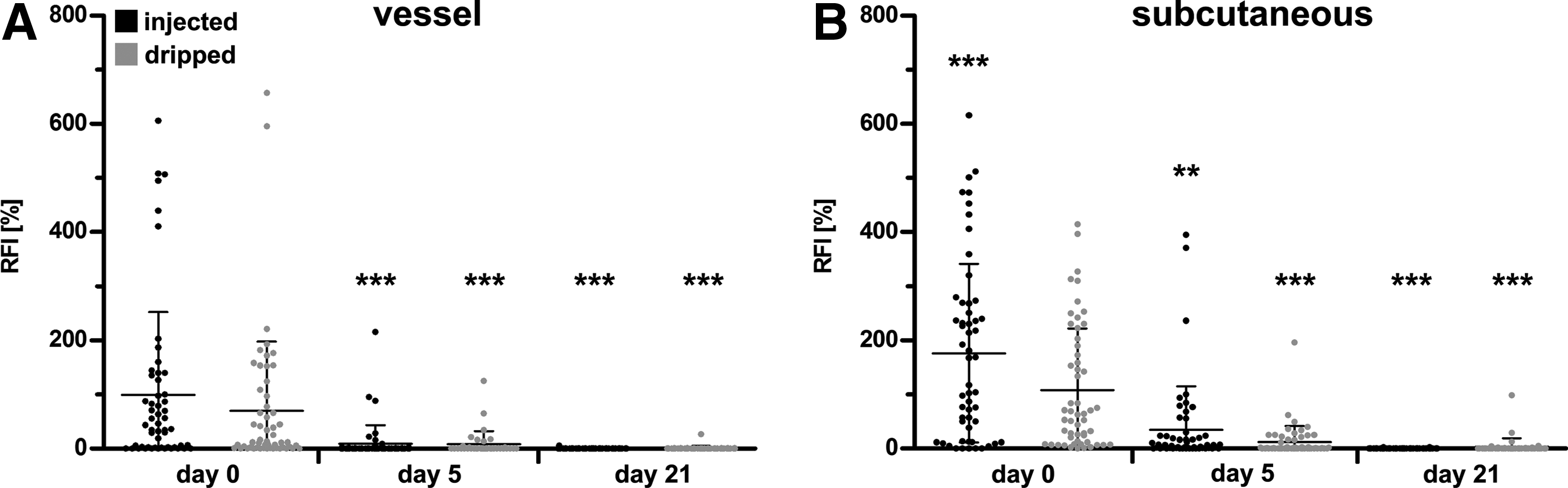
Comparison of different seeding time points. Cells were applied during implantation (day 0, no prevascularization), or 5, and 21 days after the implantation by either injection or repetitive dripping. The mean fluorescence intensity of scaffolds around the AV bundle with injected cells on day 0 was considered as 100%. Data are presented as a dot plot showing the mean RFI.
Similar results were observed within the subcutaneously implanted scaffolds. On day 0, the injection group resulted in an RFI of 176.1%±167.8% and the repetitive dripping group yielded 108.0%±122.8%, respectively (Fig. 4B). Also here, a significant reduction of RFI to 35.1%±86.3% (injection group) and 12.2%±32.0% (repetitive dripping group) was observed when seeding took place on day 5. After 21 days, cell numbers further decreased to 0.3%±0.5% within the injection group and to 3.6%±17.0% in the repetitive dripping group (Fig. 4B). In all of the control groups (media without cells), no fluorescence was observed (data not shown). Generally, the subcutaneously implanted scaffolds showed a distinctively higher RFI when compared to scaffolds placed around the AV bundle (Fig. 4).
Quantification of vessels after prevascularization
To assess the amount of newly formed vessels in the different groups, eosin counterstained cryocuts of all scaffolds were evaluated after India ink injection (Fig. 5). Within each treatment group, 3024 FOV were evaluated by two independent observers. Implantation around the AV bundle (Fig. 5, black dots) resulted in significantly more vessels inside the scaffolds compared to implantation subcutaneously at all time points (p≤0.01). This difference further increased on day 5 (Fig. 5, gray dots; p=0.03) to day 21 (p<0.0001). With increasing time of prevascularization, the number of vessels also significantly increased for both groups, the subcutaneous as well as the AV bundle group (p≤0.01). All the scaffolds that received cells contained a significantly higher number of vessels compared to media control (Fig. 5, control; p≤0.01). Accordingly, the maximum vessel number was detected after 21 days of prevascularization by implantation around the AV bundle before cell seeding.
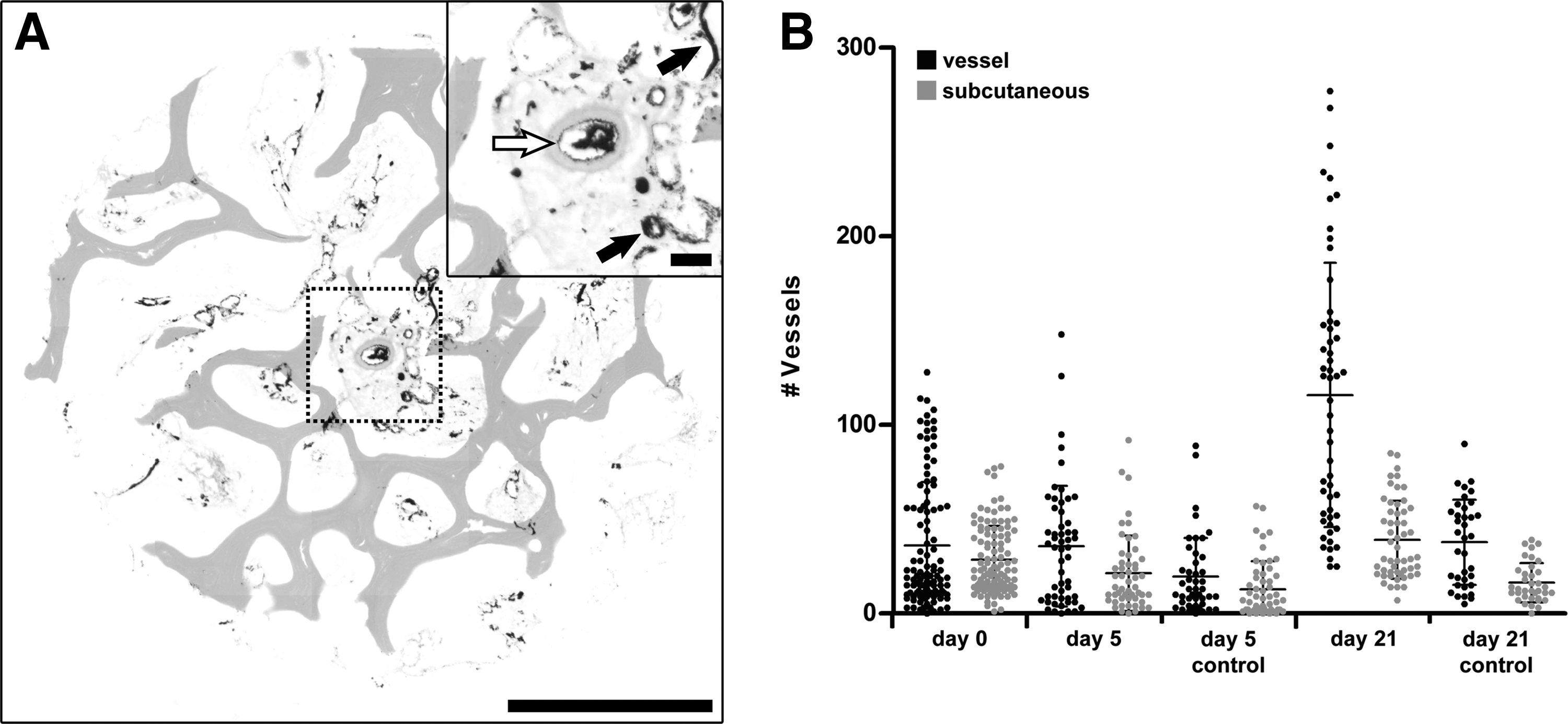
Quantification of vessel numbers using India ink injection in eosin counterstained cryocuts.
Discussion
In vivo cellular nutrition by diffusion is limited to a distance of ∼200 μm. 17 Therefore, a lack of vascularity of cellularized scaffolds is believed to reduce cell survival after implantation. Prevascularization of scaffolds in vivo was hypothesized to improve cell survival by providing a pre-established vascular network within the scaffold before cell seeding. The aim of this study was to compare different seeding strategies after prevascularization in a murine model.
The murine model
To use the well-established eGFP-labeled hMSC line for cell detection, athymic nude mice were employed. Previously, we demonstrated that eGFP labeling is currently the most reliable technique to track cells in vivo. 16 To induce a microvascular network within scaffolds, three different approaches are available: the AV loop model, which requires an AV microanastomosis; the AV ligated bundle model with distal ligation of both vessels; the AV flow through model, where the scaffold is placed around the vascular bundle without further intervention.18–22 Tanaka et al., demonstrated that the AV loop model produced more vessels compared to the flow through models. Nevertheless, the flow through models also had vigorous potential for angiogenesis and tissue generation without the necessity of microvascular anastomosis. 18 We therefore developed a new mouse model for prevascularization of 3D scaffolds by AV flow through, choosing the saphenous artery and vein, which are easily accessible at the superficial medial aspect of the upper hind limb. A scaffold, with an axial channel, was placed around the AV bundle. Of importance for our model, was that the scaffold upon contact with any liquid obtained a sponge-like consistency. This allowed placement of the slotted scaffold around the AV bundle entirely encircling the vessels (Fig. 1C). After a short learning curve, the procedure proved to be simple and reproducible. Due to its simplicity, this model may serve as a screening tool for in vivo prevascularization studies.
Comparison of different strategies for in vivo seeding
To utilize the potential of prevascularization, cells have to be seeded on scaffolds in vivo. Up to now, there has been no established protocol available for in vivo seeding. Furthermore, no study has compared the efficiency of different seeding strategies. The key problem is, with the ingrowth of vessels, connective tissue fills the scaffold's voids. Thereby, cell application is hampered. The standard method of in vitro seeding is repetitive dripping of cells onto the scaffold, which results in a homogenous cell distribution and in high efficiency. 3 Therefore, in vitro seeded scaffolds served as a control. In the present study, the first in vivo seeding strategy was developed according to the in vitro protocol. Cells were repetitively dripped onto the scaffold after implantation. In an attempt to seed even highly tissue-filled scaffolds, we developed a second seeding strategy. Cells were injected in a small volume at multiple, defined sites of the scaffold. The first point of issue was to evaluate the efficiency of these three different strategies without prevascularizing the scaffolds (day 0). As expected, the in vitro seeded scaffolds produced a higher RFI than both in vivo seeding techniques. This finding may be partially explained by the fact that the in vitro seeded scaffolds were kept in the incubator for 24 h after the seeding procedure to give the cells time to adhere properly. Due to this approach, the cells began to proliferate, resulting in higher cell numbers on the day of application. Second, we compared the two in vivo seeding techniques applied on days 0, 5, and 21 after prevascularization. With the dripping technique, the cells were located mainly at the outer regions of the scaffolds. On the other hand, with injection, cells were found predominantly in central regions, showing a slightly higher RFI comparatively to the dripping protocol. With both techniques, however, the RFI decreased significantly with increasing time of prevascularization. This is in contrast to findings of Arkudas et al. who concluded that the longer the scaffolds were prevascularized, the more cells survived. 8 In that study, a cell containing gel was applied into preformed holes within the scaffold. During prevascularization, these voids were kept open using plastic spacers, which were removed on the day of cell application. By this means, the problem of connective tissue filling the voids of the scaffolds was successfully circumvented. However, two aspects have to be taken into account. First of all, in the study performed by Arkudas et al., cells applied into prevascularized scaffolds were within a gel, inhibiting cell adhesion. Furthermore, CFDA labeling was used to identify viable cells ignoring the fact that this dye can also be detected in apoptotic cells and macrophages. The number of viable cells might thereby be overestimated.16,23 While Arkudas et al. concluded that prevascularization may improve cell survival, our findings indicate that connective tissue ingrowth inhibits efficient cell seeding in vivo, thus reducing the hypothesized benefits of in vivo prevascularization. Consequently, it is of paramount importance to develop and evaluate new techniques to increase the efficiency of in vivo seeding. Future studies must address this urgent issue.
In subcutaneously implanted scaffolds, we detected twice the RFI for both seeding techniques at all time points. One possible explanation therefore could be that, during implantation, a small pocket is created. During seeding, the excess of cell suspension probably remains within this pocket, and therefore is kept in direct contact with the scaffold. This prolongs the time for cells to adhere. In contrast, when implanted around the AV bundle, the scaffold is entirely exposed (Fig. 1) during the seeding procedure, which inevitably results in the drainage and loss of excess cell suspension. While these findings may suggest at first that subcutaneous implantation is superior to seeding prevascularized scaffolds, we believe that we are not yet able to reap from the benefits of this concept. Placement of the prevascularized scaffold in a specific chamber might enhance cell seeding by combining the benefits of the two strategies.
Another important aspect when determining the seeding time point is its effect on cell differentiation. Shortly after implantation, before vessel ingrowth takes place, there is low oxygen tension within the scaffold. Oxygen is a key regulatory signaling molecule in tissue development. 24 In hypoxic conditions, MSCs maintain their undifferentiated characteristics 25 and hypoxia-inducible factor 1-alpha (HIF-1α) accumulates. Together with vascular endothelial growth factor (VEGF), which is a downstream target of the HIF-1α pathway, this promotes vessel ingrowth. Therefore, with increasing time, the vessel will invade the scaffold and the oxygen level will increase. Both, HIF-1α and VEGF, are also key factors in regulation of osteogenic differentiation. 24 Vessel ingrowth and osteogenic differentiation go hand in hand, as specific differentiation into osteoblasts requires increasing oxygen levels. 25 Hence, key markers of osteogenic differentiation cumulate with increasing time. 26 Consequently, the time point of in vivo seeding will have a great impact on the cell function.
Cell application promotes vessel formation
Significantly, more vessels were formed in scaffolds placed around the AV bundle compared to those implanted subcutaneously. This was the case, even though the scaffolds around the AV bundle were wrapped with a silicone foil, to prevent neovascularization from the surrounding tissue. In contrast, the subcutaneously implanted scaffolds were in direct contact to the surrounding tissue. This is conclusive with previous studies, which demonstrated robust neovascularization upon the use of the AV flow through model.8,9,11,27 Interestingly, scaffolds seeded with hMSCs contained a significantly higher number of vessels compared to the media control, independent of whether they were implanted subcutaneously or around the AV bundle. This effect was much more pronounced with increasing time. Meaning, the difference of the vessel numbers between the control group and the hMSC-seeded group was significantly increased for the time point of 21 days, when compared to day 5. This effect is presumably even less distinct on day 0; however, we did not include this additional control group. The increase in vessel formation in the presence of hMSCs may be due to the angiogenetic cytokines released by the transplanted, hypoxic hMSC. Laschke et al. indicated that precultivation in an angiogenic extracellular matrix also accelerates vessel formation. 7 By combining these in vitro and in vivo techniques, ingrowth of connective tissue could possibly be limited in relation to vessel growth. Furthermore, it would be of great interest to evaluate whether the presence of hMSCs, also influence other cell types of the host organism, such as fibroblasts, osteoblasts, and others. This would be an important step in further understanding the effects of stem cell therapy.
Conclusion
We conclude that the new AV flow through model induces ample vascularization of scaffolds. The application of hMSCs further enhances these results. However, prevascularized scaffolds are rapidly filled with connective tissue, hampering secondary cell seeding. In vivo seeding by cell injection is superior to the repetitive dripping protocol. Nonetheless, more efficient strategies for application of vital cells to prevascularized scaffolds should be evolved. Alternatively, when pursuing the more efficient in vitro seeding technique, cells should be prepared to withstand the oncoming hypoxic insult until new vessels have formed.
Footnotes
Acknowledgments
Hans Polzer was supported by the Friedrich-Baur-Foundation, LMU Munich (project 0018/2008), the scientific publisher council of MMW, Munich and by the Faculty of Medicine, LMU Munich (FöFoLe, project 704). Florian Haasters acknowledges the support of the Friedrich-Baur-Foundation, LMU Munich (project 0019/2008) and the Faculty of Medicine, LMU Munich (FöFoLe, project 660). Wolf Christian Prall and Elias Volkmer were supported by the Faculty of Medicine, LMU Munich (FöFoLe, project 565 and 642). We acknowledge the support of Tutogen Medical GmbH. Tutogen provided the scaffolds (Tutobone, Bovine Demineralized Bone Matrix).
Disclosure Statement
No competing financial interests exist. Tutogen provided the scaffolds (Tutobone, Bovine Demineralized Bone Matrix) with regular charges of 20 € per scaffold, adding up to 2160 € in total. This support does not result in a conflict of interest, as scaffolds were not the matter of analysis. Any comparable scaffold from another company would have served similarly. The scaffolds simply served as a cell carrier and are approved for patient application. The company did not take any influence on the study design, data analysis, and manuscript preparation.