
Abstract
Osseointegration of dental and orthopedic bone implants is the important process that leads to mechanical fixation of implants and warrants implant functionality. In view of increasing numbers of osteoporotic patients, bone implant surface optimization strategies with instructive and drug-loading ability have been heavily explored. However, few animal models are available to study the effect of novel implant surface modifications in osteoporotic conditions. Since laboratory rats comply with a number of practical advantages, including the reliability of several methods for rapid induction of osteoporotic conditions, the present work aimed to define the use of the femoral condyle in osteoporotic female and male rats as a suitable implantation model to study osseointegration of bone implants. The method describes the procedures for induction (by hypogonadism) and assessment (by in vivo micro-computed tomography [CT]) of osteoporotic conditions in both female and male rats. The implantation site architecture (femoral condyle bone properties and dimensions) was comparatively evaluated for female and male rats, and the implant installation procedures are described. Finally, the possible analytical techniques to evaluate bone responses via mechanical tests, ex vivo micro-CT, and histological methods are provided.
Introduction
T
Osseointegration of bone implants relates to the entire biological processes involved from implant placement to implant fixation within the bone tissue.4–7 Within that osseointegration process, bone regeneration is a consequence of complex events that involves the accumulation of osteoblast precursors, formation of bone matrix, and eventually mineralization.5,6 In view of osteoporosis, it is well established that an osteoporotic condition negatively affects the process of bone regeneration and hinders the normal activity of bone cells.6,7 Consequently, it is straightforward to assume that bone healing around dental and orthopedic implants placed in osteoporotic patients is negatively influenced and more prone to implant failure. 8 For such challenging situations, a possible improvement of bone-implant regeneration has been proposed via several strategies, which must be evaluated under in vivo conditions before clinical use. 7 In view of the need for translational models that address clinical relevance, few animal (in vivo) models have been designed to study bone-implant regeneration in osteoporotic conditions. 9 Although osteoporosis appears to be a human-specific disease and does not naturally occur in animals, the (characteristics of the) disease can be induced artificially in an animal with healthy bone condition. 10 Rodents, particularly rat models, have been used extensively in biomaterials research and much is known about their bone regeneration and remodeling.11,12 Laboratory rats comply with a number of practical advantages, including ethical and cost considerations, ease of handling and care, and the reliability of several methods for rapid induction of osteoporotic conditions.13,14 Therefore, ovariectomized rats have been accepted as the animal model to mimic osteoporosis in women. 15 Similar to female rats, hypogonadism in male rats is associated with an imbalance in bone resorption and bone formation, resulting in the development of an osteoporotic condition.16,17 To study the biological response at the bone-implant interface, the femoral condyle (i.e., distal part of femur located in the knee joint) implantation site, mainly the metaphyseal secondary spongiosa area, has been suggested. 18 The advantage of using the femoral condyle is that this location allows to evaluate the cancellous bone response, as well as mechanical properties of bone at the implant interface. 19
In view of this, the present work aimed to define the use of the femoral condyle in osteoporotic female and male rats as a suitable implantation model to evaluate the osseointegration of bone implants placed in an osteoporotic condition. To this end, the surgical procedures for induction of osteoporotic conditions in both female and male rats via the removal of gonadal tissues (hypogonadism) are described. Subsequently, the analytical method used to confirm the occurrence of an osteoporotic condition in the femoral condyle using in vivo microfocus X-ray computed tomography (in vivo micro-CT). Thereafter, femoral condyle size differences (width and height) between female and male rats and the implant installation procedures are described. Finally, the possible analytical techniques to evaluate osseointegration via mechanical tests, ex vivo micro-CT, and histological methods are provided.
Materials and Methods
Animal models
All animal experiments obeyed the guidelines (national and international) for animal care and the Dutch law concerning animal welfare. The in vivo studies were further approved by the Animal Ethical Committee of the Radboud University Nijmegen Medical Centre. To establish an osteoporotic condition, female and male Wistar rats (Charles River Laboratories International), aged 12 weeks old, and weighing of ∼250–350 g, were subjected to gonadal tissue removal (i.e., ovariectomy or orchidectomy).
Ovariectomy (OVX) procedures
Bilateral ovariectomy (or sham operation) was performed in female rats. Before the surgery, rat body weights were measured using a digital weighing apparatus. Thereafter, inhalational anesthesia was induced and maintained using 2% Isoflurane® by volume (Rhodia Organique Fine Ltd.). Following anesthesia, rats were placed in a left lateral position. Then, the dorsal part of the lumbar region was shaved and disinfected with 10% povidone iodine. The animal was placed on a heating blanket to prevent hypothermia. An incision was made on the dorsal side caudal to the posterior border of the ribs. The incision was ∼2 cm in length at the midpoint between the costal inferior border and the iliac crest, and a few millimeters lateral to the lateral margin of the lumbar muscle. Using blunt dissection, the muscles of the posterior abdominal wall were separated to enter the abdominal cavity. The ovary was located in a fat pad just beneath the muscles. The ovary and associated fat were exteriorized by gentle retraction using forceps. Then, a mosquito forceps was used to hold the fallopian tube and cranial-most part of the uterine horn distal to the ovary. A single ligature was placed around the blood vessel using absorbable surgical suture (Vicryl® 3.0; Ethicon Products). The ovary was disconnected by cutting above the clamped area and the uterine horn was returned into the abdomen. After confirming that no massive bleeding occurred, the abdominal wall (peritoneum and muscle layers) was closed with absorbable sutures (Vicryl 3.0) after which the skin was closed using metallic wound clips (Agraven®; InstruVet Bv). The procedure was repeated for the right ovary using the same incision design. Sham-operated animals followed the same surgical procedure, except for the removal of the ovaries. For pain control, Rimadyl® (5.0 mg/kg body weight) and Temgesic® (0.02 mg/kg body weight) were injected subcutaneously 15 min preoperation and every 12 h for 2 days after the surgery. Postoperatively, the animals were monitored for signs of pain, infection, and proper activity.
Orchidectomy (ORX) procedure
After inhalational anesthesia was induced and maintained by 2% Isoflurane by volume, the abdominal region was completely shaved and cleaned with 10% povidone iodine. The animal was placed in supine position on a heating blanket. A 1 cm midline skin incision was made between the ventromedial area and the umbilical area. Using blunt dissection, the muscles of the abdominal wall were separated to enter the abdominopelvic cavity. Then, the gonadal tissues were gently pulled through the incision including the testes, caudal epididymis, caput epididymis, vas deferens, and spermatic blood vessels. A mosquito forceps was used to hold the blood vessels and the vas deferens. A single ligature (Vicryl 3.0) was placed around the blood vessel, after which both testes were removed. After confirming that no massive bleeding was occurring, the abdominal muscle layers were closed with resorbable sutures (Vicryl 3.0) after which the skin was closed using metallic wound clips (Agraven). The sham operations were also performed following the same surgical procedure, except for the removal of testes. As pain control, Rimadyl (5.0 mg/kg) and Temgesic (0.02 mg/kg) were used subcutaneously every 12 h for 2 days after the surgery. The animals were monitored for signs of pain, infection, and proper activity.
Housing and food restriction
Before procedures of ovariectomy and orchidectomy, rats were acclimatized for 10 days, housed in sex-matched pairs using standard macrolon type III cages with sawdust as bedding material. The animals were fed standard rodent chow and bottled tap water ad libitum. The housing room was maintained under standard laboratory conditions (light–dark cycle: 12:12 h, temperature: 20–22°C, relative humidity: 45–55%). After OVX or ORX intervention, rats had free access to water and low-calcium pelleted chow (0.01% Ca and 0.77% P; ssniff Spezialdiäten GmbH). Sham-operated rats had unrestricted access to normal pelleted chow (1.17% Ca and 0.91% P).
Investigations by in vivo micro-CT
In vivo micro-CT was used to assess trabecular bone morphological alterations in femoral condyles to confirm the presence of osteoporotic conditions in both female and male rats. The method involved certain steps to obtain a standard and reproducible assessment model. Considerations involved in setting up micro-CT scanning and guidelines for the process of assessment of bone morphology in rodent models have been described previously. 20
In vivo micro-CT scanning
At 4 and 6 weeks of hypogonadism, OVX and ORX rats and sham-operated rats (n=3 of each animal group) were scanned using a small animal in vivo micro-CT imaging system (Inveon; Siemens Medical Solutions). The animal was placed supine on the scan stage and was sedated under inhalational anesthesia (2% Isoflurane by volume) using a mask held over the rat's snout secured with a strap. The two hind limbs were bended and held in place with a strap. The distal femoral regions were manually located via the scout viewer (Inveon Acquisition Workplace software; Siemens Medical Solutions) as the region-of-interest for optimally focused scanning resolution. Then, CT images were acquired with the manufacturer recommended parameters: voltage 80 kV, anode current 500 μA, angular sampling 1° per projection for a full 360° scan, effective pixel size 30 μm, and exposure time of 1 s. The X-ray source-to-detector distance was 357.8 mm and source-to-object distance was 160.7 mm. Total procedure time was ∼30 min, including the preparation, sedation, and recovery of animal. Typical scan times were less than 10 min. Thereafter, all projection data were reconstructed using cone beam algorithm according to the manufacturer's default values.
Assessment of trabecular bone morphology
The scanned micro-CT data for right and left femoral condyles were imported into Inveon Research Workplace 3.0 software (Siemens Medical Solutions USA, Inc.). Trabecular bone was selected by the determination of a volume of interest (VOI) in the metaphyseal region. To obtain a standardized VOI selection, a reference point (i.e., the most proximal aspect of the epiphyseal growth plate) was first defined visually (Fig. 1). Then, after a fixed distance of 10 slices (=0.3 mm) corresponding to this landmark, a region-of-interest with a length of 2.1 mm (=70 slices) was chosen manually (excluding the cortical bone). The distance from the growth plate was applied to avoid metaphyseal primary spongiosa to be included in the trabecular VOI. Thereafter, the gray-value images were adjusted to remove noise and a fixed threshold was manually determined to extract trabecular bone and bone marrow separately. Using the Inveon Research Workplace 3.0 software, the following trabecular bone morphological parameters were automatically computed: (1) bone volume fraction (BV/TV, %), (2) trabecular thickness (Tb.Th, mm), (3) trabecular number (Tb.N, mm−1), and (4) trabecular separation (Tb.Sp, mm).

For selecting the region-of-interest, an anatomic landmark (red star) was defined using the growth plate. Corresponding to this landmark, a fixed region-of-interest (green area) was chosen manually 0.3 mm proximally in metaphyseal area (excluding the cortical bone).
Femoral condyle sizing (width and height)
To measure the size (width and height) of femoral condyles in female and male rats, anatomical reference points on the femoral condyle were defined using multiplanar reconstruction and three-dimensional (3D)-rendered images by Inveon Research Workplace 3.0. (A) On an axial (transverse) view, the width of the femoral condyle was measured between the most prominent points on the lateral and medial epicondyles, that is, transepicondylar distance (Fig. 2A). (B) On a lateral (sagittal) view, a height of the femoral condyle was measured between the most proximal point on the edge of the articular cartilage to the posterior border of the distal femur, that is, anteroposterior dimension (Fig. 2B). For accuracy, the measuring tool option was used to measure distances between the identical reference points on corresponding transverse and sagittal 3D images. All measurements were recorded in millimeters.
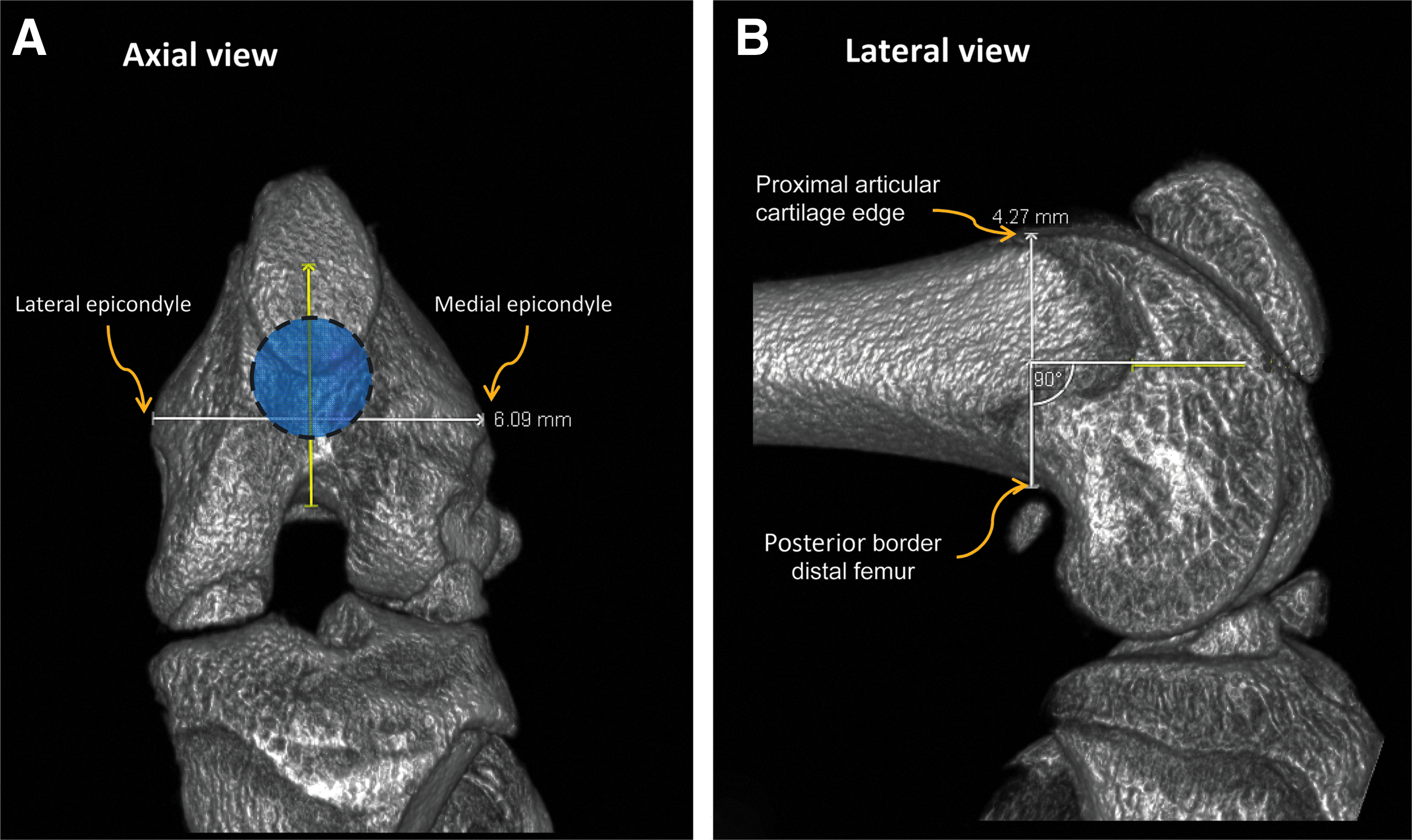
Method of femoral sizing on a three-dimensional (3D)-reconstruction computed tomography (CT) workstation. Morphological reference points defined on
Surgical procedures for implant installation
After confirmation of an osteoporotic condition, cylindrical titanium implants were installed in the femoral condyles. Under inhalation anesthesia (2% Isoflurane by volume), the animal was immobilized supine with the knee joint in a maximally flexed position and the hind limbs were shaved, washed, and disinfected with 10% povidone iodine. The knee joint capsule was incised longitudinally, and by lifting the patellar ligament gently and moving it laterally, the knee joint became fully exposed. This maneuver was facilitated by a slight extension of the knee. At the intercondylar notch, a cylindrical hole was prepared parallel to the long axis of the femur, using dental burs and surgical motor (Elcomed 100; W&H Dentalwerk Burmoos) with low-rotational drill speed (800 rpm) and continuous external cooling with saline. Then, implants were placed (press-fit) bilaterally into the predrilled holes, resulting in two implants per rat. After insertion of the implants, the soft tissue layers and skin were closed with resorbable sutures (Vicryl 4.0; Ethicon Products). To reduce postoperative pain, Rimadyl (5.0 mg/kg) and Temgesic (0.02 mg/kg) were used for 2 days. Animals were monitored on a daily basis for 1 week postsurgery to detect issues related to wound healing and mobility. After implantation procedures, all rats had free access to normal pellet food (1.17% Ca and 0.91% P) and water.
Fluorochrome administration
Fluorochrome labels were administered to the rats to monitor new bone regeneration related to the implant surface. Four different fluorochromes were administered sequentially by subcutaneous injection (2-week intervals between each injection, starting 1 week postimplantation): calcein blue (M1255-10G; 30 mg/kg body weight), calcein green (C0875-10G; 10 mg/kg), alizarine complexone (A3882-1G; 30 mg/kg), and rolitetracycline (R2253-5G; 25 mg/kg). All fluorochromes were purchased from Sigma-Aldrich. For each fluorochrome label, a stock solution was prepared in 10 mL isotonic sodium bicarbonate solvent (2% NaHCO3) and filtered through a 0.22-sterile millipore filter. Finally, 100 μL fluorochrome solutions were prepared and stored sterile at 4°C ready for administration. More details on in vivo applications of fluorochrome labels have been published elsewhere. 21
Analytic methods of peri-implant bone regeneration
After rats were euthanized by CO2 suffocation, the femoral condyles were carefully dissected and cleaned from adhering tissues. Then, specimens were processed for evaluation of peri-implant bone regeneration:
Mechanical testing
Specimens were freshly retrieved and immediately transported on ice for subsequent mechanical testing (e.g., push-out test). To determine the strength of an implant fixation, a push out-test was performed using a mechanical testing bench (MTS 858 Mini Bionix II) as previously described. 22 In brief, specimen was grinded to expose both sides of implant, after which it was placed on a jig hole of 0.5 mm larger than the implant diameter (Fig. 3). The crosshead was moved as close to the specimen as possible without touching it with the push-out rod. Thereafter, a vertical force (parallel to a long-axis of implant) with a displacement speed of 0.5 mm/min was applied on the implant. The test was stopped when the peak force was reached (representing implant loosening) and was recorded in Newton (N).
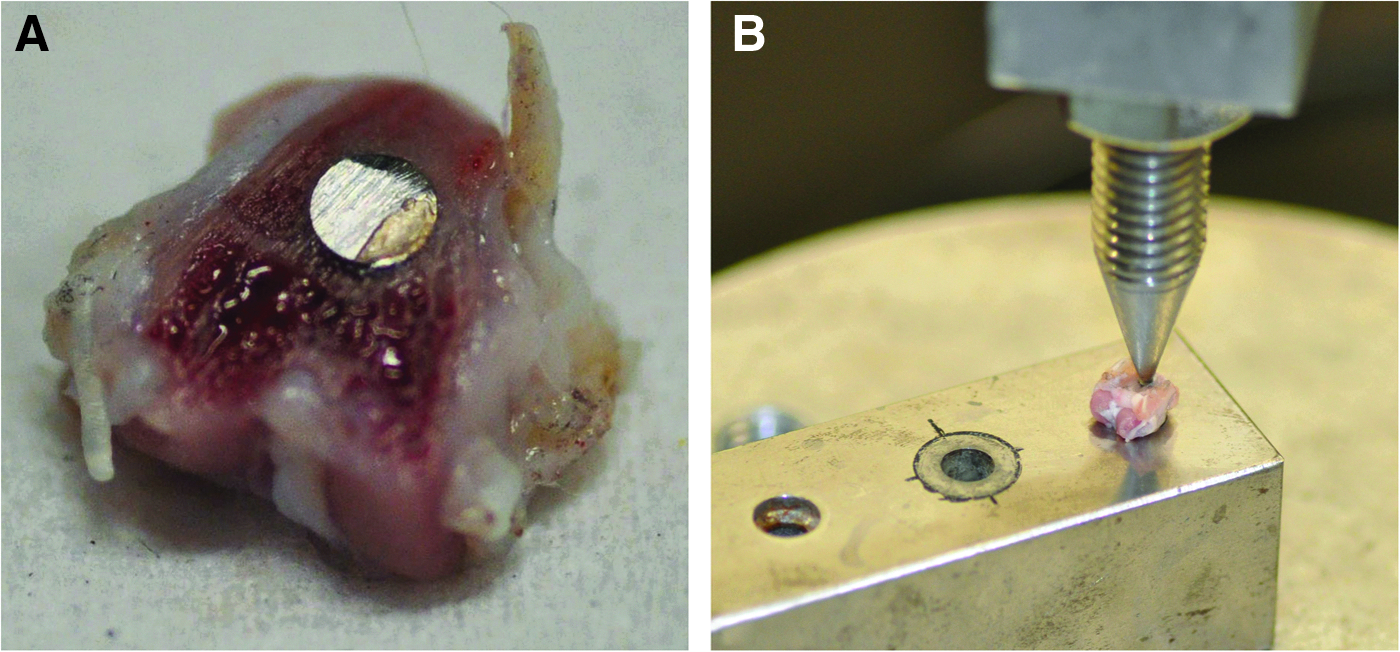
Photograph of mechanical test setup includes the specimen preparation
Ex vivo micro-CT examination
After implant removal (i.e., pushed-out with low force rate and a proper specimen alignment), bone tissues were scanned with a desktop X-ray microtomography system scanner (Skyscan® 1072). Before scanning, each specimen was wrapped in Parafilm® (SERVA Electrophoresis GmbH) to prevent drying during scanning and placed vertically onto the sample holder. Subsequently, a scan resolution of 11 μm was set for all the samples. Scans were recorded at 100 kV and 98 μA, with the use of a 1 mm thick aluminum filter to optimize the contrast, a 180o rotation, 5-frames averaging, a rotation step of 0.90° (206 images per scan), and exposure time of 3.8 s. After 3D reconstruction using NRecon v.1.4.4 (Skyscan), a constant VOI was chosen to include bone tissue surrounding the implant bed by using CT analyzer software (CTAn v.1.8; Skyscan). Thereafter, per sample, a fixed threshold was manually selected to segment peri-implant bone tissue and preserves its morphology. Finally, trabecular bone volume fraction was visualized and measured in a defined region-of-interest using a concentric radius ring larger than the used implant diameter and centered on the cylindrical implant bed.
Histological evaluation
After fixation in 10% formalin solution, specimens with implant in situ were dehydrated in ascending grades of alcohol from 70% to 100% and subsequently embedded into poly(methyl methacrylate) resin freshly prepared by mixing 600 mL of methyl methacrylate monomer (Acros Organics BVBA), 60 mL dibutyl phthalate (Merck KGaA), and 1.25 g perkadox (AkzoNobel). After polymerization, serial transversal sections (perpendicular to the long axis of the implant) were cut at a thickness of ∼10 μm, using a modified sawing microtome technique as described previously. 23 Longitudinal histological sections (parallel to the long axis of the implant) were also prepared with a thickness of ∼10 μm using same sawing technique. Then, sections were stained with methylene blue and basic fuchsin. Histological and histomorphometrical evaluations were carried out using a light microscope (Axio Imager Microscope Z1; Carl Zeiss Micro imaging GmbH) as described previously. 24
Fluorescence evaluation (bone dynamics)
Nondecalcified histological sections without staining were used to acquire fluorescent images using the Zeiss microscope (Carl Zeiss Micro imaging GmbH) with appropriate filters and pass excitations: (1) green fluorescence; filter No. 10 and excitation 450–490 nm, (2) red fluorescence; filter No. 00 and excitation 530–585 nm, (3) yellow fluorescence; filter No. 18 and excitation 390–420 nm. The dynamic of bone deposition at different time points were relatively qualified around implants based on observations of the intensity and area of fluorescent signals.
Statistical analysis
GraphPad InStat® (GraphPad Software) was used. Differences in bone morphological values between the two medical conditions of rats were calculated using Student's unpaired t-test. Similarly, differences in size of femoral condyle between female and male rats were statistically tested using Student's unpaired t-test and considered to be significant at p<0.05. Values are presented as absolute mean and standard deviations (SDs).
Results
Results of in vivo micro-CT
Trabecular bone morphometrical analysis
For both female and male rats, μCT slices revealed that rats after hypogonadism had less trabecular bone at the femoral condyle (metaphyseal region), disorganized trabecular architecture, and expanded marrow cavities compared to the sham-operated animals (Fig. 4). In contrast to trabecular bone in female rats with healthy conditions, significant changes in bone structures characterized by a decrease in bone volume fraction (Fig. 5A), trabecular thickness (Fig. 5B), and trabecular number (Fig. 5C) as well as an increase in trabecular separation (Fig. 5D) were observed after 4 and 6 weeks follow-up in female rats with osteoporotic conditions (p<0.05). In addition, the results of the bone volume fraction (58.8% vs. 74.3%) and trabecular thickness (0.13 mm vs. 0.19 mm) showed a gradual increase with increasing follow-up periods (4 vs. 6 weeks) after sham-operation procedures, respectively (p<0.05; Fig. 5A, B). The quantitative measurements in male rats with osteoporotic conditions also displayed a significant decrease in bone volume fraction (Fig. 6A), trabecular thickness (Fig. 6B), trabecular number (Fig. 6C), and an increase in trabecular separation (Fig. 6D) after 6-weeks follow-up (p<0.05).
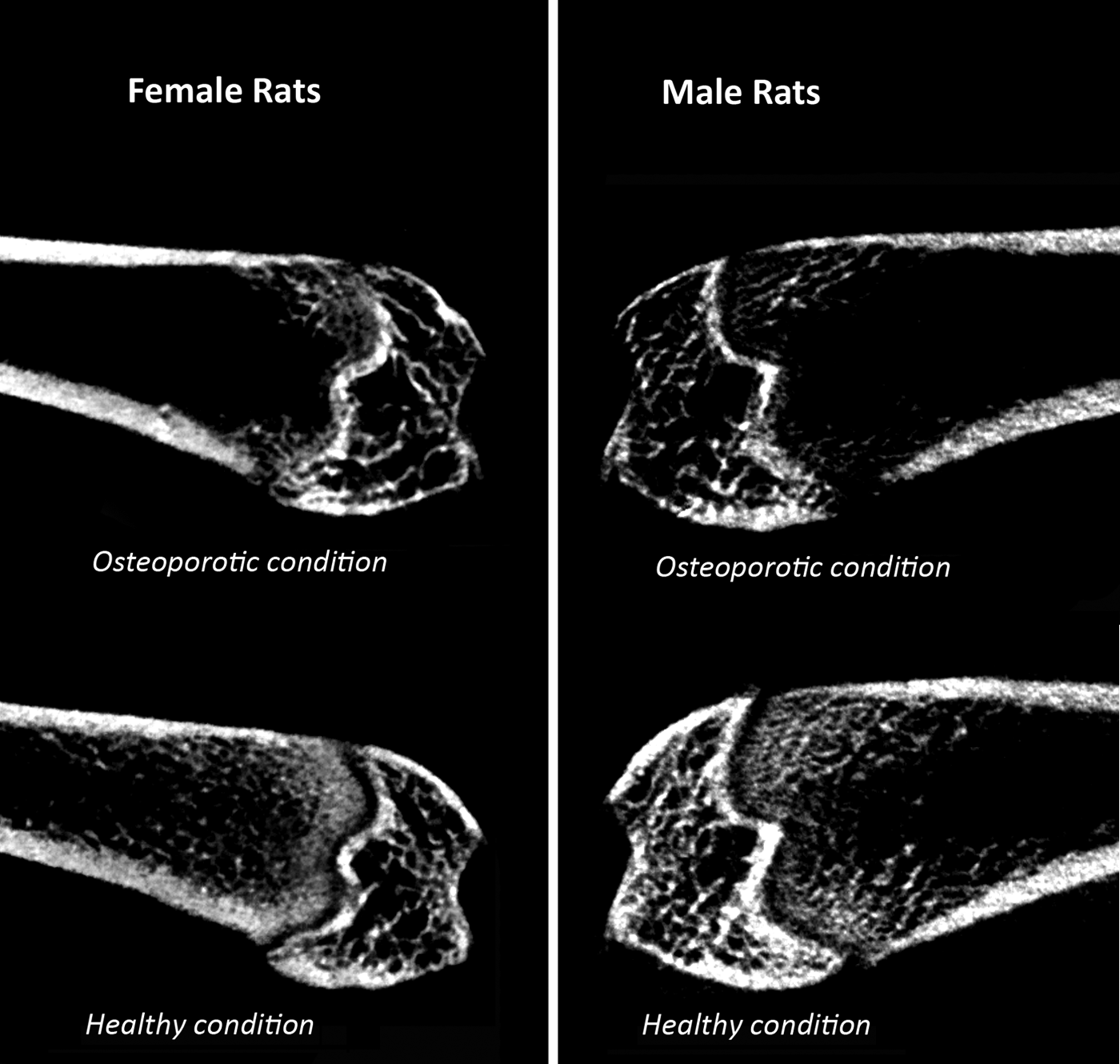
Representative two-dimensional (2D) slices obtained by in vivo micro-CT (30-μm pixel size) from female and male rats with osteoporotic and healthy conditions. The representative 2D images were selected from the middle (coronal) portion of femoral condyles in the mean animals based on the mean bone volume fraction (BV/TV).
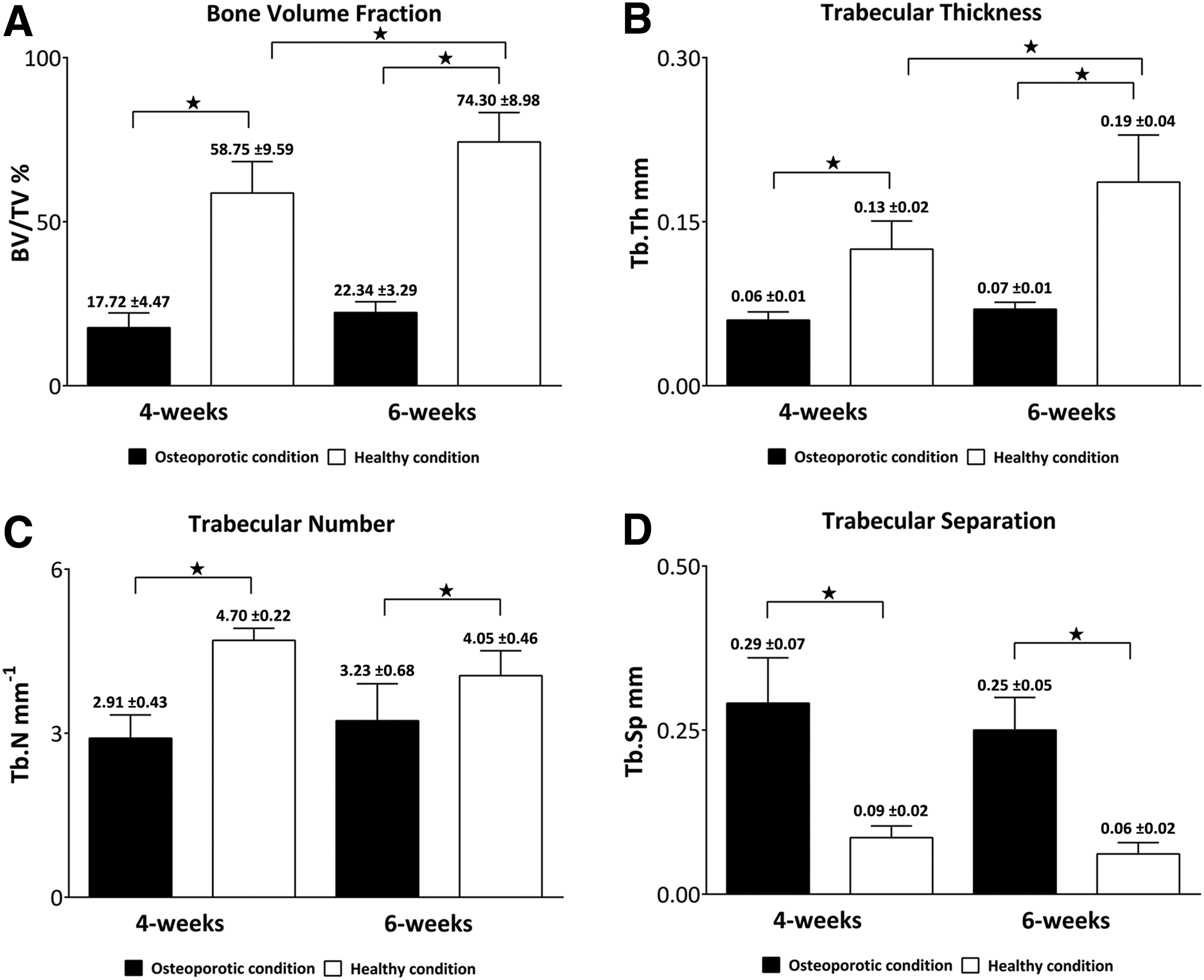
Graphs of in vivo micro-CT structural parameters

Graphs of in vivo micro-CT structural parameters
Gender-specific changes in trabecular bone morphology
At 6-weeks follow-up, osteoporotic conditions were more pronounced in female than in male rats compared to gender-equivalent healthy rats. Osteoporotic female rats had 3.3-fold lower bone volume fraction, 2.7-fold thinner trabeculae, and 4.0-fold higher trabecular separation compared to the healthy rats (p<0.05; Fig. 5A, B, D). In male rats, osteoporotic conditions demonstrated to induce a 2.3-fold lower bone volume fraction, 1.3-fold thinner trabeculae, and 2.2-fold higher trabecular separation compared to healthy conditions (p<0.05; Fig. 6A, B, D). Finally, bone volume fraction and trabecular thickness parameters in healthy female rats were significantly higher compared to male rats with osteoporotic and healthy conditions (p<0.05; Fig. 7A, B).

Differences in
Gender-related differences in femoral condyle sizing
The mean width of the femoral condyle in male rats (6.90±0.09 mm) was significantly higher compared to female rats (6.03±0.08 mm; p<0.05; Fig. 8A). Furthermore, the values for femoral condylar height in male rats (5.10±0.06 mm) were significantly higher than in female rats (4.34±0.05 mm; p<0.05; Fig. 8B).

Results of femoral condyle sizing for
Observations of bone-implant interface analytical methods
Mechanical test (e.g., push-out method)
The femoral condyle implantation model allows mechanical tests in a standard mechanical setup under controlled circumstances and provides a direct quantitative outcome. For example, the mechanical performance (e.g., push-out values) of implants placed in the femoral condyle was affected by osteoporotic versus healthy bone conditions, indicated by the increased push-out force related to different experimental implant groups as previously published. 25
Ex vivo micro-CT
Images obtained from bone specimens without implants (i.e., after mechanical test) by high-resolution ex vivo micro-CT showed the feasibility to visualize obvious structural details of trabecular bone in the proximity of the implant bed. In both two-dimensional (2D) and 3D images (Fig. 9A, C), trabecular bone around the implant bed in osteoporotic condition oriented irregularly with more spaces and disruption structure network, whereas it showed a well-defined and dense trabecular structure around the implant bed in healthy conditions (Fig. 9B, D).
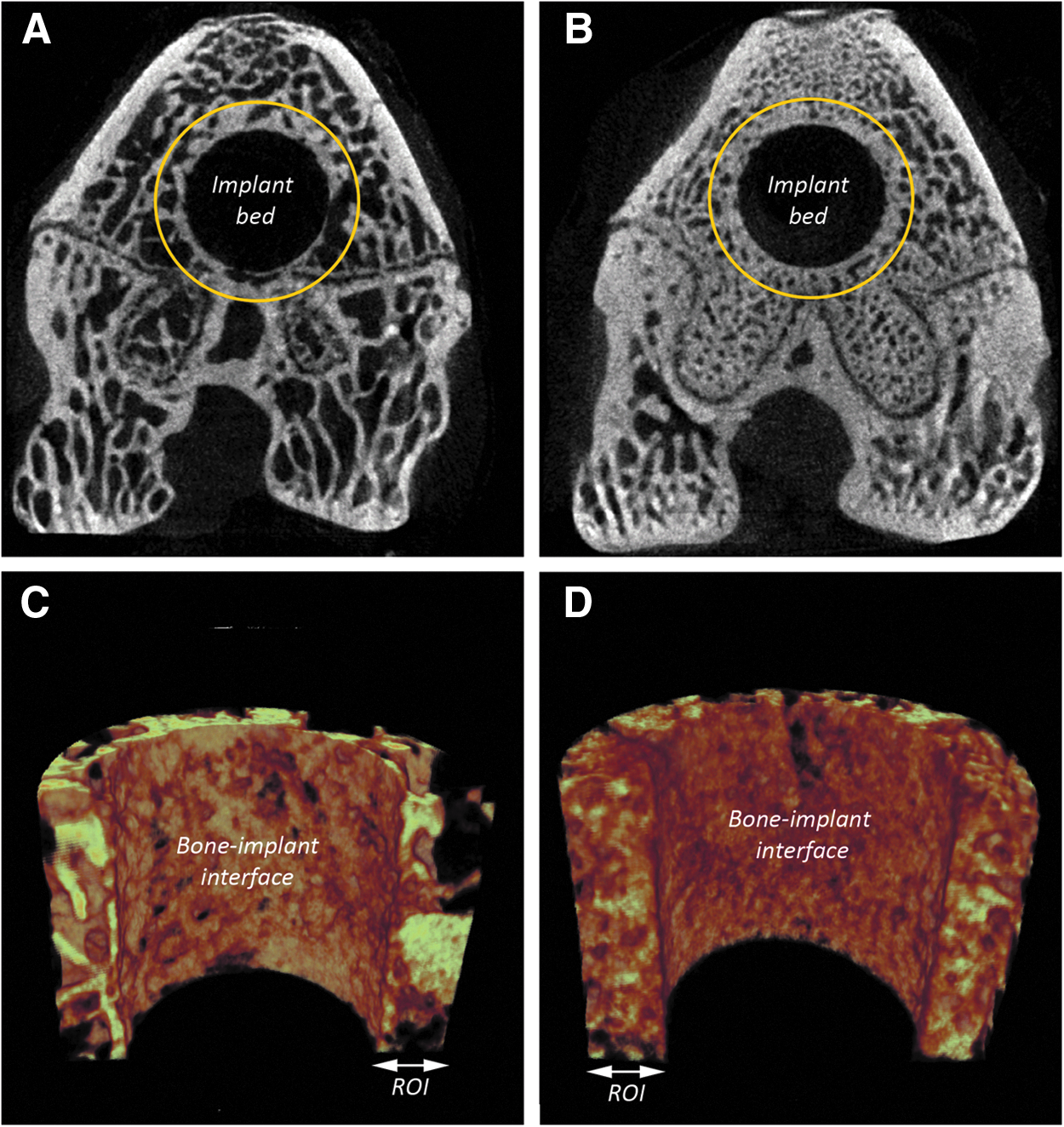
Representative 2D ex vivo micro-CT images after implant removal using mechanical tests for
Descriptive histological evaluation
In transverse histological images, trabecular bone reduction around implants appeared characteristically greater in osteoporotic compared to healthy conditions in both female (Fig. 10A, B) and male rats (Fig. 10C, D). The trabeculae were sparse, irregular, and discontinuous. In contrast, the femoral condyle trabeculae in healthy rats were dense and arranged regularly in the proximal area around the implants. Longitudinal histological sections (Fig. 11) further showed the possibility to evaluate the bone in the close vicinity of the entire implant placed in osteoporotic condition.
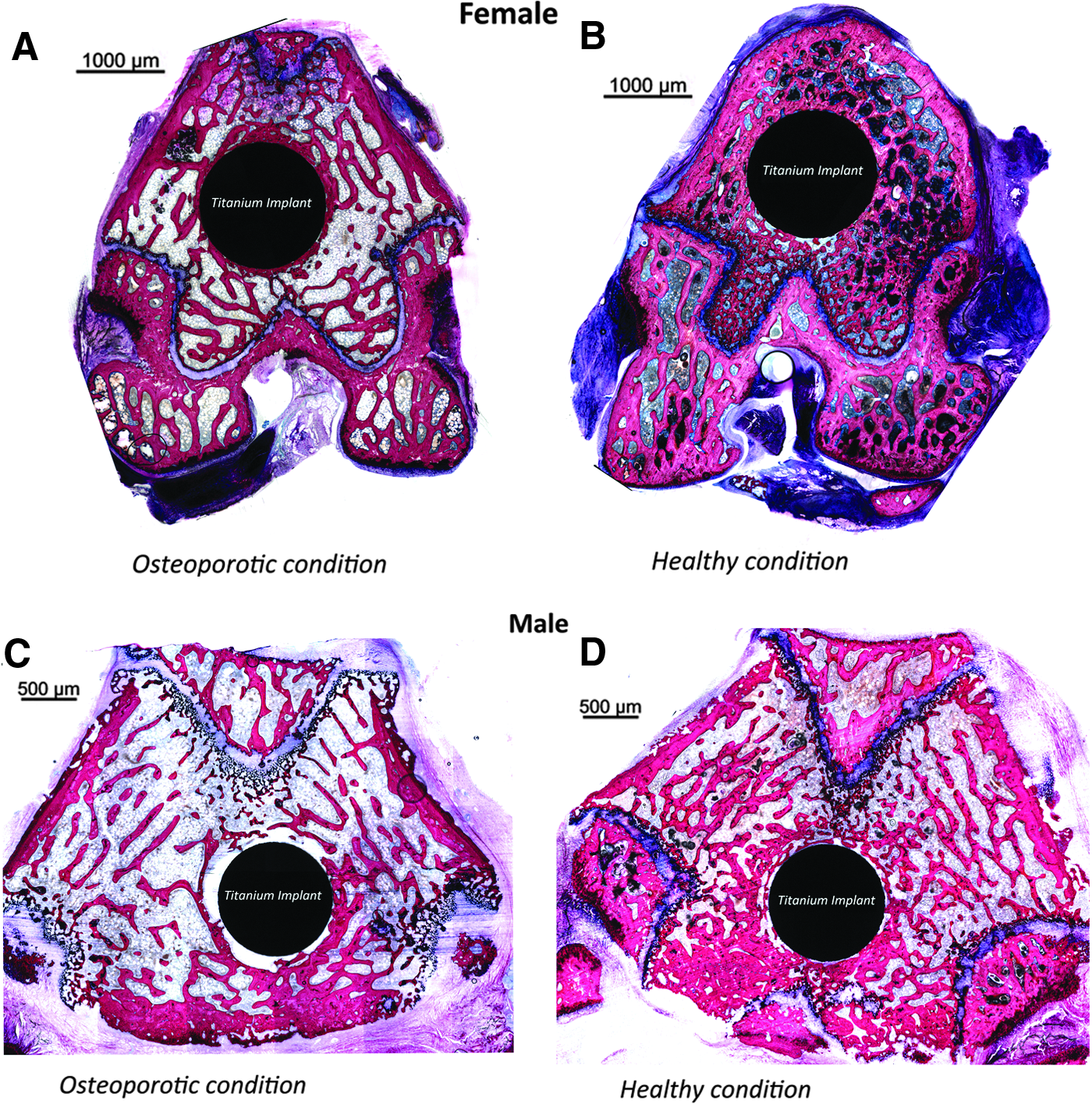
Panorama view of cross-sectioned histological images for femoral condyles in female and male rats with
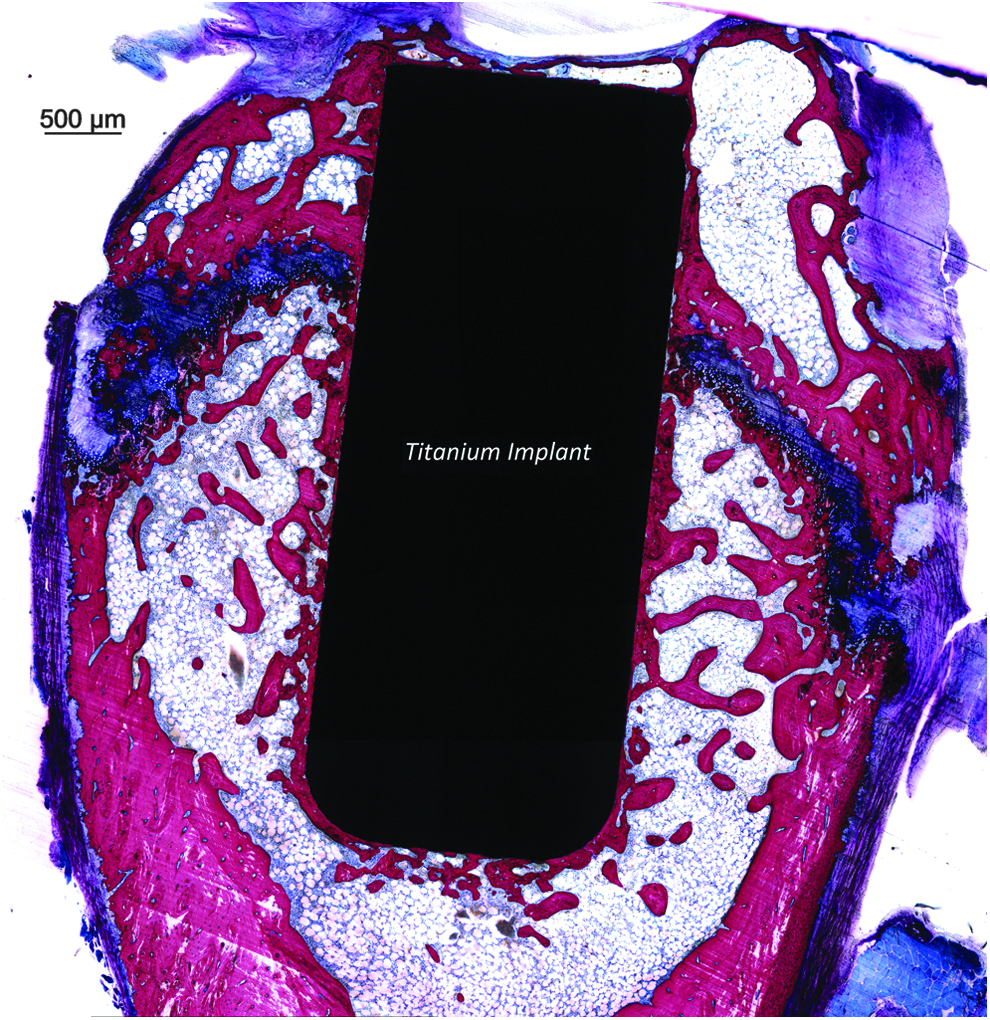
Longitudinal histological section image obtained at×100 magnification showing the entire interface of bone with implant surface.
Descriptive bone dynamic evaluation
Fluorochrome labeling provided a simple and distinct tool for evaluating dynamics of bone regeneration around femoral condyle implants. The fluorochrome images (Fig. 12A) consistently showed various stages of new bone regeneration, indicated by different intensity of fluorescent signals surrounding the implants. For example, calcein green (at 3 weeks; Fig. 12B) indicated more new bone formation (i.e., more intense areas of green signal) occurred primarily following the placement of implants with modified (calcium phosphate-coated) surfaces in osteoporotic and healthy conditions as previously published. 25 While less bone formation (i.e., less fluorescent signals) occurred at the stage of 5 weeks (red, alizarin complexone; Fig. 12C) and 7 weeks (yellow, rolitetracycline; Fig. 12D).
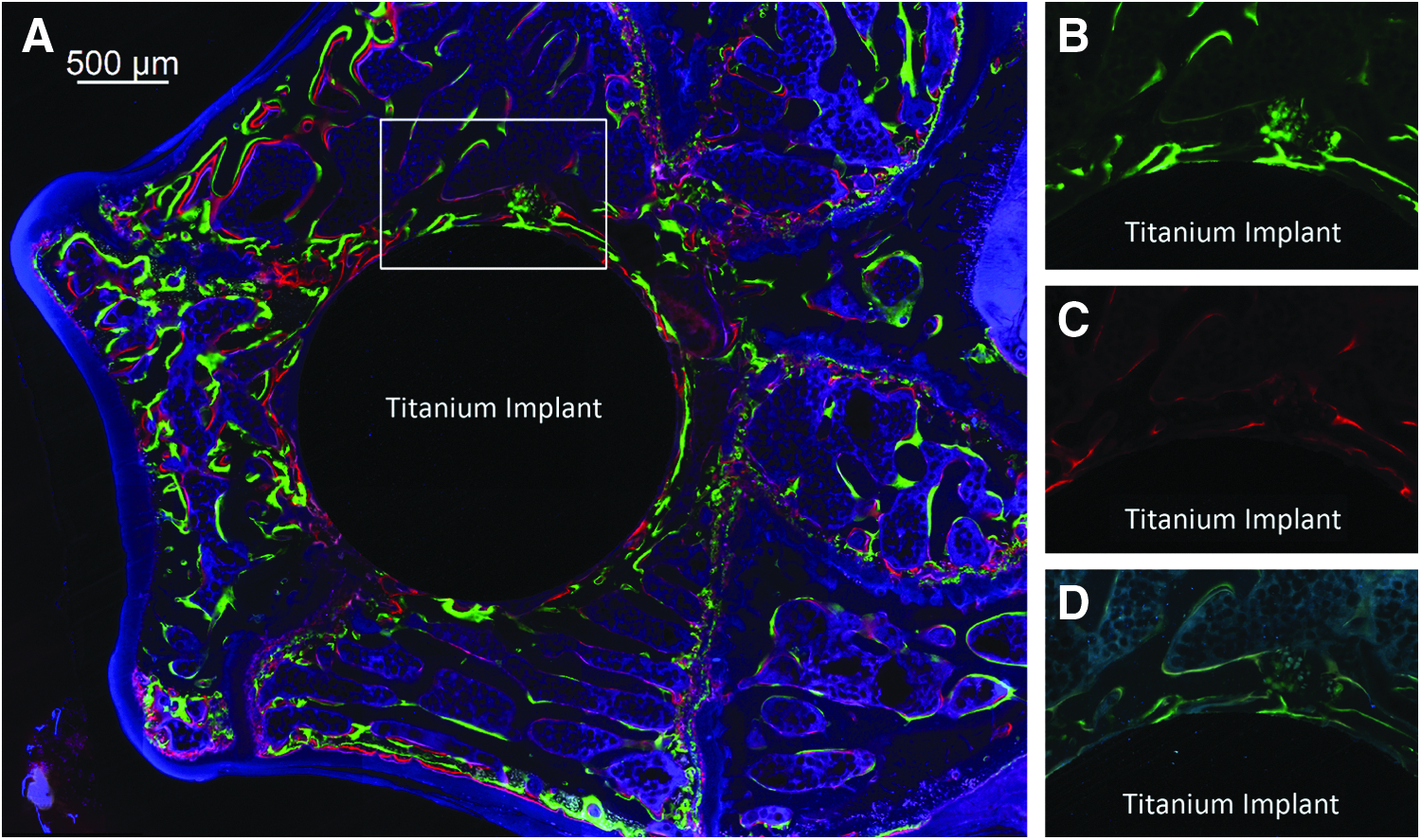
Fluorochrome image
Discussion
This work aimed to describe the methods of inducing osteoporotic conditions in female and male rats by the removal of gonadal tissue (hypogonadism). The presence of osteoporotic conditions was confirmed based on the assessment of the trabecular bone morphology in femoral condyles using in vivo micro-CT method. After hypogonadism, female rats were significantly more susceptible to bone loss than male rats compared to gender-equivalent healthy animals. The size of the femoral condyle in male rats appeared substantially larger than in female rats (i.e., gender-related differences). Furthermore, the femoral condyle demonstrated to be a suitable implantation site that allows for consistent in vivo evaluation methods of bone regeneration related to titanium implants placed in compromised conditions (i.e., osteoporotic bone).
Osteoporotic female and male rat models
Rat models are commonly used for conducting basic research for bone regeneration in healthy conditions. 12 However, there is no ideal animal model for studying bone regeneration to implants in more challenged (osteoporotic) conditions. 13 This is because osteoporotic disorders occur naturally in humans and can be only experimentally induced in animals. 26 For instance, an ovariectomized (female) rat is studied heavily for effects of osteoporotic conditions and has been recommended by Food and Drug Administration (FDA) as the preclinical animal model for testing osteoporotic medications. 13 In the present work, it was also proven that the removal of ovaries (i.e., estrogen deficiency) causes a rapid reduction (after 4–6 weeks) in trabecular bone structures in the (metaphysis) femoral condyle. We also combined the effect of calcium-restricted diet that only contains 0.01% calcium and 0.77% phosphorus in the current osteoporotic rat model, as it was previously shown that a diet with normal calcium content reduces the rate of bone loss due to sex hormone deficiency in female rats. 27 In the literature, Saville 28 has initiated the attempt to characterize the ovariectomized rat model for postmenopausal osteoporotic conditions. Thereafter, several studies extensively used the ovariectomized rat model in osteoporotic bone research.10,27,29–31 In addition, several studies used the ovariectomized rat model to understand and improve bone-implant interfaces in osteoporotic conditions.32–34 The mechanism of bone loss after ovariectomy is suggested to be caused by the fact that bone resorption exceeds bone formation. 27 It has been found that estrogen inhibits bone resorption by controlling the activity and the number of osteoclastic cells by, for example, the upregulation of the Fas Ligand (FasL) gene in osteoclasts. 35 In addition, decreasing levels of estrogen were found to upregulate the expression of RANKL-stimulating cytokines include interleukin-1 (IL-1), tumor necrosis factor (TNF-α), and IL-6, which are known to stimulate bone resorption.36,37 On the other hand, it has been found that the activation of estrogen receptor-α (ERα) in osteoblasts stimulates their anabolic (osteogenesis) abilities. 38 Consequently, a lowering effect on osteoblastic cell activity in osteoporosis is assumed to be correlated with estrogen deficiency, which causes a reduction of mesenchymal stem cells becoming committed to osteoblastogenesis.39–41
In the present work, we have found that hypogonadism in male rats was also associated with significant morphological alterations in the trabecular bone in femoral condyles. This is in agreement with previous studies that attempted to characterize the male rat model (orchidectomized) for osteoporotic conditions in men.16,17,42 The etiology of bone loss associated with an androgen-deficiency is less clear. However, it has been reported that osteoblastic cells also possess androgen receptors, which stimulate their bone-forming activity. 43 Consequently, androgen deficiency might be an important reason for an impaired bone formation in orchidectomized rats. 44 Furthermore, evidence suggests that estrogen hormone also has an important role in male bone homeostasis similar as in female bone.45,46 More specifically, low gene expression of ERα in osteoblasts was reported in male rats after gonadal tissue removal and was correlated with increased bone loss.45,47
Clinically, monitoring bone mineral density (BMD) by dual-energy X-ray absorptiometry (DXA) is most commonly used to diagnose an osteoporotic condition. 48 The estimation of BMD by DXA is known as the T-score (the number of SDs from the healthy young adults BMD mean) of the same sex and ethnicity as the patient. 49 According to guidelines from the WHO, osteopenia (mild-to-moderate bone loss) is defined by a T-score between −1 and −2.4. Osteoporosis (sever bone loss; pathological level) is established when a T-score of BMD is ≤−2.5 SD. 50 However, the estimated BMD by DXA does not provide information of bone morphology (3D structural assessment). Additionally, for small animal bones, BMD and tissue mineral density (TMD) measurements are not appropriate for small trabecular metaphyseal region (i.e., a significant error can occur in BMD and TMD calculations). However, BMD and TMD measurements may be possible for trabecular bone if the resolution is sufficient and larger animal or human specimens are used. 20 Trabecular bone morphology contributes substantially to bone quality and its evaluation seems a feasible and efficient index to detect the early progression of osteoporotic lesions.51,52 In the present work, in vivo microCT has been used primarily to generate information about mean bone volume fraction (BV/TV), mean trabecular thickness (Tb.Th), mean trabecular separation (Tb.Sp), and mean trabecular number (Tb.N). These parameters are commonly used to characterize the trabecular bone morphology in rodents. 20 Based on that, we were able to detect early (i.e., 4–6 weeks after hypogonadism) bone morphology changes in osteoporotic animals as confirmed by a significant decrease in trabecular bone volume fraction, thickness, and number and increase in trabecular bone separation compared to healthy conditions. These findings of rapid bone morphological alterations assessed by in vivo micro-CT within the first 2 months in rats with sex-hormone deficiency were also demonstrated previously.53–55 An important issue that should be considered when assessing bone morphology in long bones (e.g., distal femur) of small animals like rats is that not all trabecular bone sites show equally rapid alterations in bone structures after hypogonadism. 26 For instance, epiphyseal bone has shown to be hardly susceptible to estrogen deficiency-related bone loss. 56 However, differences in trabecular bone morphological parameters have demonstrated to be more pronounced in the metaphyseal area postovariectomy.24,25,56 In view of this, trabecular bone structures were presently analyzed in a well-defined region-of-interest that only includes metaphyseal secondary spongiosa of the distal femur.
Following hypogonadism, the magnitude of bone loss, in particular bone volume fraction, trabecular thickness, and trabecular separation, was gender-specific (i.e., greater in female than in male rats). The authors assume that this relates to female rats having naturally larger trabecular bone network than male rats. 57 In addition, male rats exhibited a slightly slower rate of bone loss relative to female rats after removing gonadal tissues, suggesting that bone tissue in male rats might be less sensitive to sex hormone deficiency compared to female rats of similar age. 58 Sham-operated animals served as baseline controls in the present work to be certain that the bone loss due to hypogonadism represents true bone loss. However, the authors noticed that trabecular bone volume and thickness for female rats in healthy conditions were gradually increased at 6-week compared to 4-week follow-up after sham operations. The authors presume that exposing rats to a sham surgical procedure might slightly cause trauma to the gonadal tissues, which causes temporary bone loss.
Bone implant placement options and analytic methods
Currently, few implantation models are available to characterize the bone-implant integration in compromised bone conditions like osteoporosis. 9 Since osteoporotic conditions occur significantly most in trabecular bone, the femoral condyle, rich in trabecular bone, is suggested as a suitable location for studying bone-implant interfaces in an osteoporotic condition. 19 Considering the present model, the femoral condyle is confirmed to be an appropriate site to install implants and investigate their biological and mechanical performance. Furthermore, an appropriate implant size minimizes unexpected surgical complications of the implantation site (e.g., fracture of femoral condyle) and makes a selected implant precisely fit and surrounded by sufficient trabecular bone tissue. 59 In the present work, the authors found that the size of the femoral condyle in male rats is substantially larger than in female rats and allows for installing of implants with 2–3 mm in diameter. Using custom-made implants with a simple cylindrical shape and proper size (2 mm in diameter), retrieved specimens showed the possibility for standardized and reproducible mechanical (push-out) testing. Such mechanical tests are commonly used to predict the fixation strength related to integration between the bone and implant surface. 60 A quantitative evaluation of bone-implant integration depends on obtaining adequate histological sections. 61 In the present work, femoral condyle specimens showed the possibility for preparing multiple thin (∼10 μm) nondecalcified histological sections with the implant remaining in situ. The advantage of retaining the implant in the histological sections is that this allows the evaluation of the intimate contact of trabecular bone at the implant surface at higher magnification and on both directions of histological sectioning, that is, transverse and longitudinal.61,62 However, a disadvantage of histological examination is that it only provides a 2D information of a 3D structure. 63 High-resolution 3D methods via the ex vivo micro-CT can give further insight into the trabecular bone structure around implants.64,65 However, it has to be emphasized that metallic scattering artifacts of X-rays prevents an accurate evaluation of trabecular bone in the close vicinity to the implant surface. 65 As an alternative, it was possible with the present model to visualize peri-implant bone tissues after pushing out an implant using a proper specimen alignment and slow pushing force rates. There was no obvious disruption of peri-implant tissues after the implant was removed and did not compromise the qualitative and quantitative evaluations on micro-CT images.
In the current work, multiple fluorochrome administration (bone labeling) facilitated several analytic time points during the study without an increase in the number of animals being used. The fluorochromes form chelate complexes with apatite via iminodiacetic acid groups, which are primarily used for labeling of bone formation in vivo and enhance the information contained in bone specimens. 21 Bone seeking fluorochromes (i.e., calcium-binding fluorochromes) provide a useful tool for analyzing the availability of bone formation sites, time, and amount of bone deposition. More importantly, the administration of several fluorochrome colors provides spatiotemporal information on the dynamics of bone regeneration in the vicinity of an implant surface over single labels. Considering the fact that crucial processes in bone-implant interactions take place within the first few weeks, a shorter period between the administrations of fluorochrome markers is recommended. However, because conventional methodology of fluorescence analysis does not allow visual discrimination of overlapping fluorescent colors (especially red and yellow spectra), it is necessary to keep certain time intervals between the administration of the fluorochrome markers (normally 1 or 2 weeks). In addition, we found that it is not advisable to wait too long (maximum 5–6 weeks) before retrieving specimens after injecting the first fluorochrome label. Second, using appropriate software, a superior morphometric quantification of the labeled bone area can be performed. Finally, much thinner bone sections (∼10 μm thick) gave sufficient fluorescent signal even after 8 weeks postimplantation, which lead to more detailed analysis on the dynamics of bone formation.
Conclusion
This work describes methods to establish a hypogonadism-induced osteoporotic condition in female and male rats, for which rapid bone morphological alterations can be determined via in vivo micro-CT within the first 2 months. The magnitude of bone loss was demonstrated to be gender-specific (i.e., greater in female than in male rats). The size of the femoral condyle in male rats is substantially larger than in female rats, for which the options for instalment of bone implants with larger dimensions or altered geometry become wider. This animal model provides a suitable means for the evaluation of bone responses to bone implants using an appropriate implantation site (femoral condyle) and allowing multiple analytical techniques to address peri-implant bone regeneration both qualitatively and quantitatively in a controlled in vivo compromised (osteoporotic) condition in a cost-effective and rapid manner.
Footnotes
Acknowledgments
The authors acknowledge Vincent Cuijpers for his assistance on micro-CT imaging, and Natasja van Dijk for assistance with histological preparation. This study was supported by Saudi Arabia scholarship (No. R0000747), Ministry of Higher Education, King Saud University, Riyadh.
Disclosure Statement
No competing financial interests exist.