
Abstract
Tissue engineering appears as a promising option to create new heart valve substitutes able to overcome the serious drawbacks encountered with mechanical substitutes or tissue valves. The objective of this article is to present the construction method of a new entirely biological stentless aortic valve using the self-assembly method and also a first assessment of its behavior in a bioreactor when exposed to a pulsatile flow. A thick tissue was created by stacking several fibroblast sheets produced with the self-assembly technique. Different sets of custom-made templates were designed to confer to the thick tissue a three-dimensional (3D) shape similar to that of a native aortic valve. The construction of the valve was divided in two sequential steps. The first step was the installation of the thick tissue in a flat preshaping template followed by a 4-week maturation period. The second step was the actual cylindrical 3D forming of the valve. The microscopic tissue structure was assessed using histological cross sections stained with Masson's Trichrome and Picrosirius Red. The thick tissue remained uniformly populated with cells throughout the construction steps and the dense extracellular matrix presented corrugated fibers of collagen. This first prototype of tissue-engineered heart valve was installed in a bioreactor to assess its capacity to sustain a light pulsatile flow at a frequency of 0.5 Hz. Under the light pulsed flow, it was observed that the leaflets opened and closed according to the flow variations. This study demonstrates that the self-assembly method is a viable option for the construction of complex 3D shapes, such as heart valves, with an entirely biological material.
Introduction
H
Mechanical or tissue valves are normally used to replace the entire aortic valve. Those types of substitutes have proven their effectiveness5,6 and the design and materials employed have greatly evolved during the past decades.3,7 However, they still represent foreign materials for the human body, which implies serious drawbacks, such as lifelong anticoagulant therapy to prevent thrombosis in the case of mechanical substitutes. On the other hand, patients who receive tissue valves are exposed to immune system reactions, accelerated calcification of the substitute, or even a potential rejection of the new valve.3,5,8,9 In both cases, the heart valve substitutes have a limited lifetime and will eventually have to be replaced. Further, the younger the patient, the more likely the degradation of the valve will be accelerated, which limits the expected lifetime of such a device. 3
Moreover, mechanical and tissue valves are unable to fully integrate into cardiovascular environment, to regenerate and to remodel depending on the physiological changes and signals sent by the body. This problem raises even more concerns when heart valves are replaced in infants, children, and young adults since many risky subsequent surgeries may be necessary. 8
An increasing number of studies have demonstrated that biological heart valve substitutes would represent a better option for the patients.10–13 Tissue engineering and regenerative medicine have strived for many years to develop new biological organs and tissues made with the patient's own cells. Heart valves designed using these principles could lead to new living replacement substitutes with the potential to grow and remodel with young patients, hence reducing and even eliminating many disadvantages of the traditional heart valve substitutes.14,15
Several options can be considered when developing a construction technique for a tissue-engineered heart valve (TEHV) substitute. The use of a porous scaffold made of biodegradable polymers and shaped into the three-dimensional (3D) structure of the aortic valve is one of the most popular techniques.8,16,17 Cells are subsequently seeded in the scaffold and allowed to proliferate while the polymer degrades, leaving more space for the cells to migrate and create their own extracellular matrix (ECM). However, even if those polymer scaffolds can easily be fabricated and their mechanical and chemical properties can be rigorously controlled, an incomplete degradation of the polymer may trigger a significant immune response. 18 Nevertheless, many studies have demonstrated the clinical potential of such techniques during in vivo experiments performed in large animal models19–21,23 and by producing, in a relatively short production time, viable biological substitutes. However, in many cases19–23 retraction of the leaflets and regurgitation were noted during in vitro and in vivo testing of the substitutes. In some studies, hypotheses pointed toward the contractile phenotype of the cells found inside the polymer scaffold.20,22–24
Decellularization of human or animal heart valves has also gained popularity.25–27 Since cells are known to contain the immunogenic materials of the tissues, 28 the main objective of those techniques is to remove all cells and to only keep the structure of the valve. Autologous or allogenic cells are sometimes reseeded to proliferate inside the acellular matrix.27,29–31 However, the decellularization process may damage the native ECM and the structure of the valve and thereby weaken their mechanical properties. 18 Moreover, the risks for an immunological response are still present even if the cells have been removed, mainly if a xenogeneic matrix is used.28,32,33 Although some research groups report successful human implantation of this type of valve substitute34–37 others rather describe a complete failure of the technique. 38
Recently, heart valve leaflets created with fibrin scaffolds 24 and whole TEHV made with synthetic polymer21,22 were decellularized. Those decellularized constructs did not exhibit the usual drawbacks encountered with decellularization of native valves, namely a decrease in the mechanical properties. Dijkman et al. 22 even reported that decellularized valves made with polymer scaffolds presented better performance than their cell-populated counterparts. Weber et al. 21 recently reported very promising results obtained with the implantation of this particular substitute in nonhuman primates.
The aim of this study is to present a new construction technique for aortic valve substitutes using a new entirely biological material. The proposed technique does not use any synthetic polymers or decellularization techniques to create a scaffold subsequently seeded with autologous cells. The material used is entirely biological and generated only with human cells. This approach has already been used with success for the reconstruction of other organs such as skin, 39 bladder, 40 blood vessels, 11 and cornea, 41 but it was never employed before for the complete construction of a 3D complex structure like the aortic valve without the use of an external permanent stent. This work hence reports the construction steps leading to a new entirely biological heart valve substitute and a first demonstration of its ability to present appropriate mechanical functions when submitted to a pulsating flow in a bioreactor.
Materials and Methods
Cell isolation and cell culture
Dermal fibroblasts were isolated from a skin biopsy obtained during a breast reductive surgery performed on a healthy 38-year-old patient. The use of these cells was approved by the Centre Hospitalier Affilié (CHA) Universitaire de Québec's Institutional Review Committee for the protection of human subjects. Tissues were obtained after informed consent was given by the patient. The large availability of dermal fibroblasts and the noninvasive nature of the biopsy motivated the choice of this cell type.
Dermis and epidermis were first separated as described previously 11 using a thermolysin solution (500 mg/mL; Sigma Aldrich, Oakville, ON, Canada) containing HEPES buffer (MD Biomedicals, Montréal, QC, Canada) for 2 h at 37°C. Fibroblasts were then isolated from the dermis using an enzymatic process using a collagenase H solution (0.125 U/mL; Roche, Laval, QC, Canada) for 20 h at 37°C.
Isolated fibroblasts were then seeded in 75 cm2 culture flasks (BD Biosciences, Mississauga, ON, Canada) and cultured in Dulbecco's Modified Eagle Medium (DMEM; Invitrogen, Burlington, ON, Canada) supplemented with 10% fetal calf serum (FCS; HyClone, Logan, UT) and antibiotics (Penicillin, 100 U/mL; Sigma Aldrich; Gentamicin, 25 μg/mL; Schering, Pointe-Claire, QC, Canada). Cells were cultured for 7 days and the culture medium was completely changed three times per week. Cells were maintained in a standard humidified incubator at 37°C with an 8% CO2 ratio.
The self-assembly method and the production of an engineered tissue
After the cell expansion period, fibroblasts were removed from the flasks' culture surfaces using an enzymatic process (0.05% Trypsin; Intergen, Purchase, NY; 0.01% EDTA; J.T. Baker, Montréal, QC, Canada). Cells were then seeded at a density of 7500 cells/cm2 in 500 cm2 petri dishes (Corning Incorporated, Corning, NY) and cultured with the same culture medium, supplemented with ascorbic acid (50 μg/mL sodium-L-ascorbate; Sigma Aldrich) to stimulate ECM synthesis. A cohesive tissue sheet was formed after 26 days of culture under these conditions and could easily be peeled off the culture surface of the petri dish.
Cell sheets were then superimposed using custom-made frames (73 mm×130 mm, internal dimensions) made of filter paper (BioRad, Mississauga, ON, Canada). Each frame was carefully placed on a fibroblast sheet and the excess parts of the tissue folded on the top of the frame. The frame and the cell sheet were carefully detached from the culture surface and placed on the next cell sheet for a total of four sheets. The cell sheets and frame were secured together using LigaClips (Ethicon Endo-Surgery, Cincinnati, OH). After three more weeks, two packs of four fused cell sheets were stacked to create a tissue made of eight cell sheets. The tissue was left for maturation for an extra 5 months. The culture medium was still changed three times per week.
Design and fabrication of the construction templates
The approach used in this study was to use several sets of templates to assist the valve's construction and provide adequate support to the flat tissues during the sequential steps conducting to their modeling into the required three-dimension shape of the aortic valve. Several construction templates were specially designed to create a 3D structure using the thick tissue obtained with the self-assembly method. Custom design and drawing of the templates were made using ProEngineer WildFire 4.0 (PTC, Needham, MA). Machining of all parts was performed at the workshop of Université Laval's Mechanical Engineering Department.
Templates were divided in two categories: flat templates and 3D templates. The form of both sets of templates was based on a 23 mm diameter aortic valve 42 and the shape of the leaflets was designed according to analytical equations proposed by Mackay et al. 43
The flat templates were composed of three parts: the bottom, middle, and upper parts (Fig. 1A). The bottom and middle parts were made of Delrin (McMaster-Carr, Aurora, OH), whereas the upper part was machined in transparent acrylic (Groupe Poly-Alto, Québec, QC, Canada) to allow visualization of the tissue during the maturation period. The 3D templates were composed of a stainless steel (Acier Loubier, Québec, QC, Canada) base and three Delrin inserts presenting the shape of deployed aortic valve leaflets (Fig. 1B).
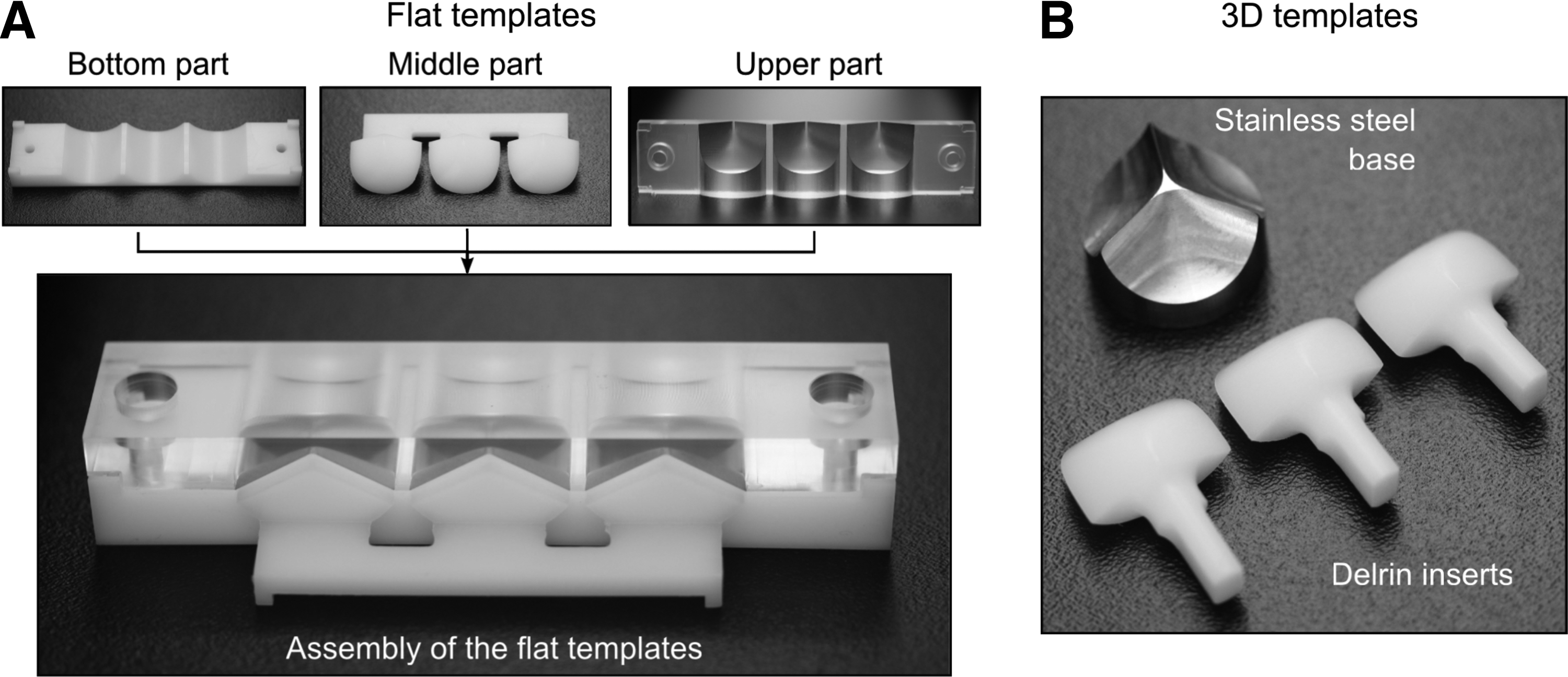
Custom-made templates designed to shape the tissue obtained with the self-assembly technique into a three-dimensional (3D) structure. The flat templates are composed of three parts used to preform the thick tissue to the shape of an unfolded valve. The three parts stack to ensure the proper positioning of the tissue
The following steps describe the construction of the first prototype using the proposed fabrication technique. A single sample was tested in the bioreactor.
Construction of the new valve substitute using the templates
The first steps of the construction technique used the flat templates to preform the thick tissue into the shape of an unfolded aortic valve (without Valsalva sinuses). Half of the tissue was placed over the bottom template and the middle part of the template was then positioned over the tissue. Tissue was then folded over the middle template (Fig. 2A) and the upper part of the template was finally added to secure the tissue in place (Fig. 2B). A slight pressure was exerted on the tissue by the upper part, which was precisely adjusted to fit the bottom part. The flat templates were designed in a way that the folded tissue was in contact at the commissures of the valve in order to promote a localized fusion of the tissue. Tissue and templates were completely submerged in the same culture medium used previously. The culture medium was changed three times per week for the rest of the construction steps.

Construction steps using the flat and 3D templates. The thick tissue was placed over the bottom part of the template and then folded over the middle part that was carefully installed between the two layers of tissue
After 4 weeks of maturation in this configuration, the middle part of the flat template was removed and replaced by the three leaflets inserts. Assembly at the commissures was secured using LigaClips because of the fragile fusion between the folded tissues. The preformed tissue was then rolled over the stainless steel base to confer a cylindrical shape to the valve (Fig. 2C) and both sides were attached using LigaClips on the front and back of the junction line (Fig. 2D). The three inserts were joined together using a circular acrylic piece (not shown on Fig. 2), which included three holes, one for each insert. Finally, the 3D assembly was placed upside down (stainless steel base on the top, not shown on Fig. 2) in a custom-made 4 inches diameter polycarbonate (McMaster-Carr) petri dish and left for maturation for an extra 2 weeks. Enough culture medium was used to ensure that the whole assembly was completely submerged.
In summary, the construction of the valve using the self-assembly method involves several steps separated by different maturation times to promote fusion between the tissue layers.
• Step 1: cell expansion (7 days)
• Step 2: creation of fibroblast sheets (26 days)
• Step 3: stacking of the cell sheets in a four-layer configuration (3 weeks)
• Step 4: stacking of two 4-layer tissues in one 8-layer thick tissue (5 months)
• Step 5: installation of the thick tissue in the flat templates (4 weeks)
• Step 6: 3D assembly using the 3D templates (2 weeks)
Testing of the valve in a bioreactor
The valve (component 1 on Fig. 3) was placed in a new custom-built holder designed specifically for this application (Fig. 3). The holder ensures that the valve can securely be installed in a bioreactor. Some pieces of the templates were still in place at the beginning, but all parts of the templates were removed by the end of the installation process. The ventricular side of the valve was first installed around a mandrel (component 2 on Fig. 3) and secured with 4-0 Prolene suture (Ethicon Endo-Surgery) wrapped around a groove on the mandrel. A silicone o-ring (AS568-020; McMaster-Carr) was placed over the suture and compressed around the tissue with a polycarbonate ring (component 3 on Fig. 3). The valve and the mandrel were then inserted into a clear acrylic hub (component 4 on Fig. 3). Finally, to ensure that the tissue-engineered aortic trunk could not turn around because of the culture medium backflow, the upper part of the valve was held in place with three polycarbonate pieces (component 5 on Fig. 3) so that each secured approximately a 120-degree portion of the aortic trunk without touching the commissures of the valve.

Schematic representation of the TEHV installed in the custom-made valve holder. The main components of the valve holder are detailed as follows: tissue-engineered heart valve (1), mandrel (2), polycarbonate ring (3), acrylic hub (4), and polycarbonate inserts used to secure the upper part of the valve (5). TEHV, tissue-engineered heart valve.
The valve holder was placed in a custom-made bioreactor (Fig. 4, previously designed and presented by Ruel and Lachance 44 ) to evaluate the functionality and behavior of the new heart valve. The bioreactor is equipped with an air-driven ventricular pump (component 1 on Fig. 4) and a compliance chamber (component 2 on Fig. 4). The valve holder (component 3 on Fig. 4) was positioned directly at the exit of the ventricular pump. The bioreactor is controlled by a proportional servovalve (MPYE-5-1/8; Festo, Mississauga, ON, Canada) and a custom-made LabVIEW program (National Instrument, Austin, TX). It can produce a wide range of pulsed flow and pressure waveforms. Flow and pressure data were monitored using an ultrasonic flowmeter (component 4 on Fig. 4, Model H20XL; Transonics Systems, Inc., Ithaca, NY) and a pressure transducer (component 5 on Fig. 4, Model CDXpress; Argon Medical Devices, Athens, TX).

Custom-made bioreactor used to expose the TEHV to a light pulsed flow, composed of a ventricular pump (1), a compliance chamber (2), a valve holder with the TEHV installed inside (3), an ultrasonic flowmeter (4), a pressure sensor (5), and an elbow with a visualization window (6). Color images available online at
A visualization window was positioned on an acrylic elbow located over the valve holder (component 6 on Fig. 4). The aortic side of the valve could be seen through this window. To obtain clear images of the valve during the tests, culture medium without phenol red was used in the bioreactor (DMEM, High glucose, and HEPES, no Phenol Red; Invitrogen). A culture medium already supplemented in HEPES buffer was chosen since no gas exchange was possible with the air in the incubator. This culture medium was supplemented with 5% FCS, penicillin, gentamicin, and ascorbic acid. Images and videos of the valve in the bioreactor were taken at room temperature for easier access to the visualization window with the camera.
The command sent to the proportional valve was chosen to create a very low pulsed flow of 0.5 Hz through the valve. The system was not pressurized prior to the tests and the manually activated resistance (presented previously 44 ) was not included to the system to prevent the application of an important pressure gradient to the valve.
Histology and thickness measurement of the tissue
Biopsies of the tissue were taken at each important step of the construction technique: before the use of any templates, before the 3D assembly, and after the tests in the bioreactor. Biopsies were fixed for 24 h in a 3.7% formaldehyde solution (VWR, Montréal, QC, Canada) and embedded in paraffin. Tissues were then cut in 5 μm-thick cross sections with a microtome and either stained with Masson's trichrome45,46 using Weigert's hematoxylin, fuchsin-ponceau, and aniline blue colorations or with Picrosirius Red47–49 using Direct-Red 80 (Sigma Aldrich). Samples were observed afterward using a microscope (Imager M2; Carl Zeiss, Toronto, ON, Canada) under visible light or through a Circular polarizer D (Carl Zeiss). The thickness of the tissues was evaluated using AxioVision software (Carl Zeiss). Three biopsies were taken at different locations on the tissue and several measurements of the thickness were taken on each histological cross section of the biopsies. A mean thickness was calculated using all measurements. Thickness was evaluated on samples taken on the tissue before it was installed in the flat template since it was more uniform at this step.
Results
Macroscopic structure of the valve and installation in the valve holder
The valve holder was designed to provide an adequate support to the tissue-engineered valve while permitting free movement of the leaflets. Parts of the valve holder (components 3 and 5 on Fig. 3) helped to keep the cylindrical portion of the valve opened, but the three deployed leaflets kept their characteristic shape without the help of any external support.
The top view of the tissue-engineered valve installed in the valve holder (Fig. 5A) illustrates the leaflets in a closed position. The free edges of the valve close at the line of coaptation and form an almost symmetrical shape similar to a native valve. The bottom of the valve (Fig. 5B) also presents the same characteristic shape of a native heart valve with the three leaflets touching each other and creating a tight and continuous surface.

Macroscopic view of the TEHV installed in the valve holder and observation of its behavior in the bioreactor through the visualization window for a complete cycle. Top
Study of the tissue-engineered valve behavior in the bioreactor
The main objective of testing the valve in a bioreactor was to confirm the ability of this heart valve model to properly function under a mechanical stimulation. The goal was not to demonstrate the ability of the valve to resist physiological flow and pressure but to confirm the capacity of the valve architecture to open and close properly under a light flow. This first test in a bioreactor hence aimed to demonstrate the potential of this new construction technique to produce a functional heart valve substitute that can eventually normally function under in vitro physiological conditions.
When placed in the bioreactor under a light pulsed flow, the tissue-engineered valve exhibited a behavior similar to that of a native heart valve, as illustrated on Figure 5C to G. The three leaflets opened during the first phase of the flow wave (Fig. 5C, D) and closed (Fig. 5F, G) to prevent a backflow toward the ventricle. The mean positive flow measured in the system while operating under light pulsed flow was 336 mL/min.
Due to the mildness of the flow, the three leaflets did not completely open during the systole. The maximum opening of the valve is presented on Figure 5E and the flow area covers only a small portion of the available flow area. Also, the opening, and the closing of the leaflets did not appear to be completely symmetrical.
Even if the free edges were well adjusted to each other when the valve was initially installed in the valve holder (Fig. 5A, B), it was observed that the closing was not complete under the pulsed flow. A mild regurgitation of ∼5.8 mL/beat was observed after the closing of the leaflets. A small triangular opening can be observed in the middle of the valve when the leaflets are closed (Fig. 5G) and backflow might have occurred through this orifice and caused minor regurgitation of the valve.
Histological staining and thickness measurements of the tissue
Masson's trichrome and Picrosirius Red stainings were used to observe the cells and the content of the ECM (Fig. 6). Histological cross sections of the TEHV stained with Masson's Trichrome presented a uniform distribution of the cells throughout the ECM. This uniform distribution of the cells suggests the ability of the tissue to remodel during the fusion of the fibroblast cell sheets. Plus, the initial eight-layer sheets used to create the thick tissue cannot be distinguished from one another, which is also a good indication of the mobility of the cells within the tissue and the possible remodeling of the ECM during the static maturation. The uniform distribution of the cells inside the ECM could be observed at each step of the construction technique and after the tests in the bioreactor (Fig. 6A–D). The tissue presented a mean thickness of 356 μm before its installation in the template.
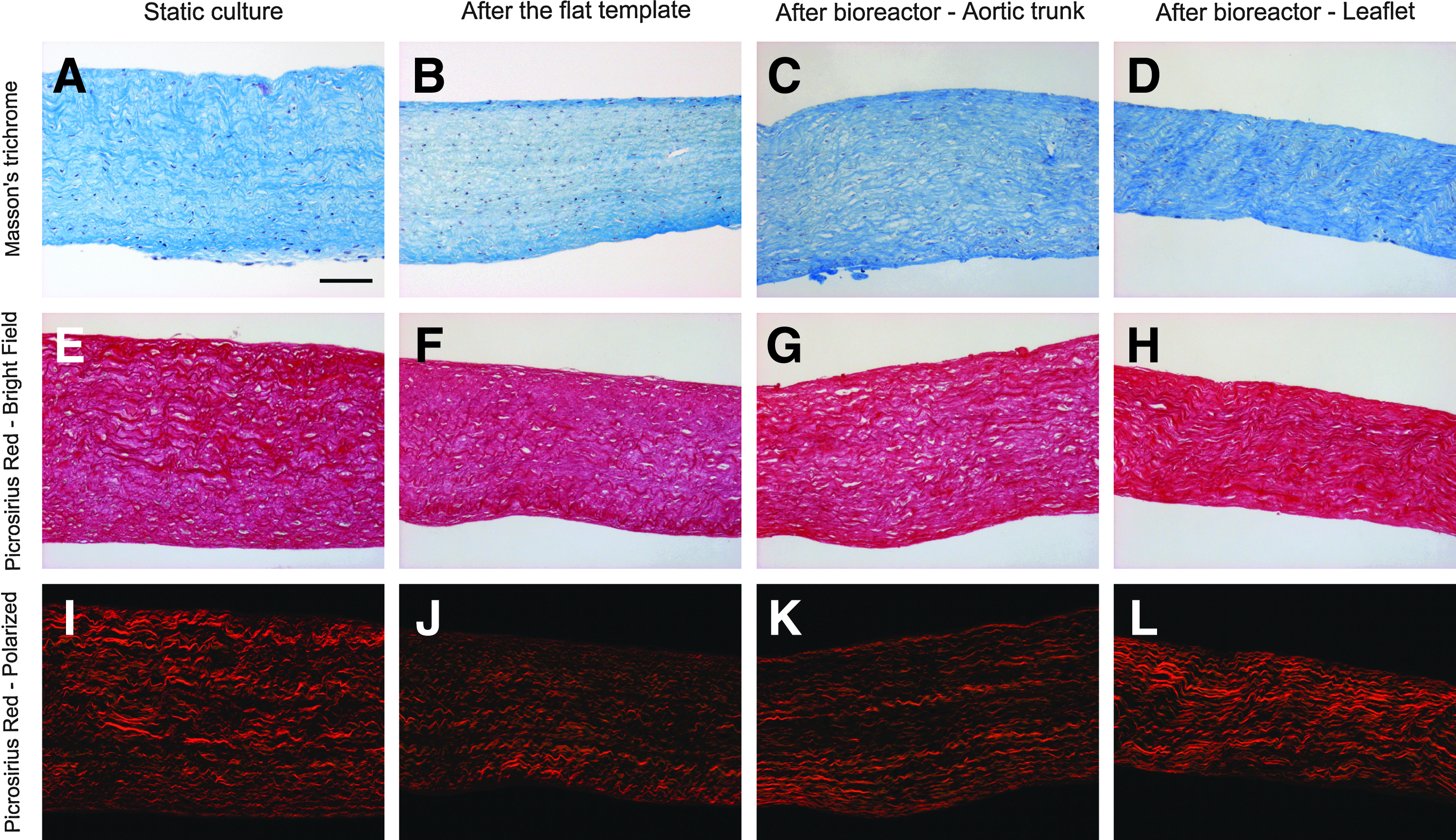
Histological staining of the tissue-engineered valve at different stages of the construction: after static culture
The thick tissue displayed a dense ECM mainly composed of collagen. Masson's trichrome and Picrosirius Red staining of the initial plane tissue (Fig. 6A, E, I) showed a corrugated structure of the collagen and this wavy structure of the fibrils is preserved through the different construction steps. However, the tissues that composed the leaflets of the valve seem to have experienced longitudinal strain after the tests in the bioreactor, while still presenting small corrugations of the fibers. Accordingly, the ECM also appears denser on the leaflets side after bioreactor simulation (Fig. 6D, H, L).
The use of polarized light (Fig. 6I–L) on Picrosirius Red stained cross sections allows the visualization of different maturation levels of the collagen fibers. 1 An orange coloration indicates larger fibers, whereas a green coloration reveals thinner collagen fibers. Both types of collagen are present in the tissue at each of the construction steps. Orange collagen fibers appear to become more predominant after the maturation in the bioreactor, especially on the leaflets of the valve, indicating more mature collagen fibers.
Discussion
This study presented a new construction technique for aortic valve substitutes and reported the initial steps achieved toward the development of an entirely biological heart valve substitute using the self-assembly method. This article highlights the potential of the self-assembly method for the production of more complex structures such as the aortic valve's leaflets and trunk. It also presented the design of the modeling templates enabling and guiding tissue proliferation into a viable and appropriate 3D shape, and the first demonstration of the valve's potential to respond to mechanical stimuli.
This first prototype, built using the self-assembly technique, presented a 3D structure similar to the shape of a native aortic valve. To support the three leaflets, a part of the aortic trunk was included but the presence of the Valsalva sinuses was intentionally omitted to keep the first design of the modeling templates as simple as possible. However, even if the shape of a substitute should be as exact as possible to reproduce the same hemodynamic behavior as a native heart valve, it may still present adequate functionality without a perfect reproduction of the 3D architecture. For example, White et al. 50 presented a heart valve substitute developed with decellularized porcine intestinal submucosa where the shape was similar but not identical to a native pulmonary valve. Their results showed a good functionality of the valve when implanted in sheeps even if there were some shape differences with respect to a native valve. The use of decellularized native valves would allow a better shape reproduction compared with the use of scaffold or plane tissues. However, Gilbert et al. 51 exposed, in a detailed review on decellularization protocols, that any process intended to remove cells in a native tissue will modify the architecture of the ECM, which may result in loss of mechanical properties and changes in biological properties.
This study used dermal fibroblasts to produce cell sheets that were used to create the TEHV. Syedain et al. 23 reported leaflet contraction problems with the use of this cell type in fibrin scaffolds. Flanagan et al. 20 also observed the same problem while working with mixed fibroblasts and smooth muscle cell population. In this study, we neither observed this phenomenon during the construction process of the valve, nor during our short-term bioreactor simulation. The plane thick tissue was allowed to freely contract when detached from its anchoring frame prior to its installation in the templates. This may explain the lack of extra contraction during the subsequent construction steps. However, particular attention will be dedicated to this specific subject for the long-term in vitro tests since it was demonstrated that tissue contraction may be an issue.
The in vitro testing of a TEHV is a crucial step to evaluate the mechanical function of the substitute. Many specialists agree that the use of a bioreactor, such as the one used in this study represents an adequate tool to evaluate the behavior of tissue- engineered cardiovascular substitutes such as valves or arteries.52–55 Bioreactors can be very useful to evaluate the mechanical behavior of the constructs but they can also be used to modify biological and mechanical properties of those constructs. The first tests presented in this article focus on the study of the mechanical flow regulation function of the valve, whereas the enhancement of the biological and mechanical properties of the substitute will be addressed in subsequent steps of the project. This study did not feature in vivo assessment of the TEHV, which may limit the complete understanding of its behavior. However, thorough in vitro experiments in bioreactors are essential steps before translating the tests to animal models.
Since the goal of those tests in the bioreactor was a first assessment of the valve's ability to properly function, that is, open and close under a pulsating fluid flow, the magnitude was limited compared with actual aortic flow rates to maintain the structural integrity of the tissue. The TEHV responded very well to the light flow and the leaflets exhibited an appropriate motion similar to that of a native aortic valve. It was, however, noted that the flow area was smaller than the flow area of a native heart valve56,57 but since the mean positive flow in the bioreactor (336 mL/min) was very small compared to a normal physiological flow through the aortic valve of 5.6 L/min, 58 the resulting fluid forces may not have been large enough on the leaflets for them to open completely. This light flow may also have contributed to the regurgitation of the valve since the back pressure applied to the leaflets was also limited (39 mmHg).
However, despite the fact that the frequency of the pulsation, the flow rate, and pressure conditions used in the bioreactor did not reflect the in vivo conditions encountered at the aortic valve, it was powerful enough to produce the movement of the leaflets while preserving the integrity of the construct. It enabled the visualization of the valve behavior and validated the ability of the self-assembly method to produce a complex 3D structure using plane tissue and custom-designed templates. The number of valves presented (one tested prototype) obviously limits the conclusions that can be drawn from this study. However, the results are very promising and still present the self-assembly method as a viable option for the construction of TEHV, even if optimization is still necessary for the next steps.
The production time of one substitute may also raise concern for the use of the valve in a clinical context. The time frame presented in this paper corresponds exactly to the real time frame of the experiment, but the maturation period of a certain number of steps, the eight-layer maturation or the maturation in the templates for example, may be further optimized in order to reduce production time. The achievement of this goal will place self-assembled heart valves in a more favorable position for a clinical translation, along with other construction techniques, such as decellularization and polymer scaffolds, which can already produce biological substitutes in a shorter production time.
While there are obvious modifications of the ECM caused by the maturation in the templates and the testing of the valve in the bioreactor, namely the longitudinal stains of the collagen fibers and the compaction of the ECM, the tissue preserved its integrity during the whole process. Qualitative analysis of the histological staining seems to indicate densification of the tissue and modification of the collagen fibers. However, further investigations will be necessary to address the underlying cause of those changes.
The reconstructed tissues do not exhibit a three-layer composition, unlike the native valve, which presents a ventricularis, spongiosa, and fibrosa. 9 Considering that no factor in an in vitro culture can trigger the differentiation of layers, it was expected to find such a uniform microscopic structure in the valve. However, based on previous results presented in the literature,8,17,27,59,60 it is believed that once the tissues will be exposed to long-term dynamic conditions, the ECM might be able to remodel and create a three-layer structure properly responding to mechanical constraints exposed on the leaflets in a physiological-like environment. Moreover, Gauvin et al. 61 have recently shown that a cell sheet created with the self-assembly method had the ability to change its mechanical properties and microscopic internal structure as a result of dynamic conditioning. These results suggest that a reconstructed heart valve leaflets made of self-assembled tissue sheets could reorganize and eventually feature a characteristic three-layer structure when exposed to a proper dynamic stimulus in vitro and in a living host.
Few data reporting the physiological thickness of fresh aortic valve leaflets are found in the literature. However, Stradins et al. 62 conducted a study to evaluate the biomechanical properties of pathologically unchanged human aortic and pulmonary heart valves. Their experiment protocol included the thickness measurement of 44 leaflets using a cathetometer. They obtained a mean thickness of 0.605±0.196 mm for the aortic leaflets and 0.397±0.114 mm for the pulmonary leaflets. The thick tissue produced in the present study was thinner than these measured aortic leaflet thicknesses but in the range of the pulmonary leaflets.
Interestingly, Stradins et al., 62 Vesely et al. 63 and Leeson-Dietrich et al. 64 also demonstrated that the mechanical properties of aortic and pulmonary heart valve are nearly the same, despite their difference in thickness. Also, the successful implantation of pulmonary valve in the aortic position achieved during a Ross procedure65–68 confirms the ability of a valve with thinner leaflets to sustain the severe mechanical constraints found at the exit of the left ventricle, as long as the valve present appropriate mechanical properties. It is thus believed that the biomechanical characterization of the tissue developed with the self-assembly method will help to determine whether the tissue is thick enough and presents the proper mechanical properties to be able to replace an aortic valve or if the development of a thicker tissue is necessary. If a thicker tissue is needed, a greater number of tissue sheets could be stacked to obtain the desired thickness. Mechanical characterization of the tissue to evaluate its biomechanical behavior represents one of the upcoming steps of the project.
The proposed construction technique described in this article is presented as an alternative technique toward the achievement of the same goal pursued by other techniques. This pilot study on the construction of complex 3D shapes using the self-assembly method has obviously a limited impact compared with in vivo implantation of other TEHV performed by other groups.19–21,23,36,37 However, this study presented a unique construction technique that can create a complex 3D heart valve structure solely using a fully biological plane tissue to begin with.
Finally, aside from the biomechanical characterization of the tissue, future work will feature additional tests in the bioreactor to assess the behavior of the tissue-engineered valve when exposed to more demanding flow and pressure, closer or equal to physiological values. Other sets of experiments will also address the enhancement of the valve's mechanical and biological properties using dynamic conditioning in the bioreactor. In-depth in vitro characterization of the TEHV will give a better understanding of the valve's behavior and will enable us to do a precise optimization of the construction technique to rapidly move toward in vivo assessment of the substitute.
Conclusion
This study presented the first attempt in the development of an entirely biological stentless heart valve substitute using the self-assembly method. The construction technique is based on different sets of custom-designed templates leading to the achievement of a 3D aortic valve structure from a thick plane tissue. The first actual valve prototype exhibits a similar behavior to that of a native heart valve when placed in a bioreactor under a light pulsed flow. The tissue's dense ECM was mainly composed of corrugated collagen fibers and contained uniformly spread cells. Based on the observation of this first prototype, this new construction technique appears promising for the development of new heart valve substitutes
Footnotes
Acknowledgments
This work was supported by the Fonds de recherche du Québec—Nature et technologies (FRQNT), the Fonds de recherche du Québec—Santé (FRQS), the Canadian Institutes for Health Research (CIHR), and the FRQS TheCell network. C.T. is recipient of a scholarship from the Natural Sciences and Engineering Research Council of Canada (NSERC) and J.-M.B. is recipient of a Frederick Banting and Charles Best Canada Graduate Scholarships from the CIHR. V.L. receives a scholarship from the FRQNT and M.Y.T. from the FRQS. The authors would also like to thanks Pierre Carrier, Marc-André Plourde-Campagna, Jean-Claude Gariépy, Cindy Perron, and Jahdonna Isaac for their technical assistance. We also thank Dr. Patrick Mathieu, Dr. Philippe Pibarot, and Dr. Yvan Maciel for insightful discussions on this project.
Disclosure Statement
No competing financial interests exist.