
Abstract
This study describes a screening platform for a guided in situ vascular tissue engineering approach. Polymer rods were developed that upon 3 weeks of subcutaneous implantation evoke a controlled inflammatory response culminating in encapsulation by a tube-shaped autologous fibrocellular tissue capsule, which can form a basis for a tissue-engineered blood vessel. Rods of co-polymer were produced using different ratios of poly(ethylene oxide terephthalate) and poly(butylene terephthalate) to create a range of physicochemical properties. In addition, a set of different physical, chemical, and biological surface modifications were tested on their ability to actively steer this tissue capsule formation using a rat model as testing platform. Tissue capsules were mainly composed of circumferentially aligned collagen and myofibroblasts. Different implant material resulted in distinct differences in tissue capsule formation. Compared to its unmodified counterparts, all surface modifications resulted in increased wall thickness, collagen, and myofibroblasts. Oxygen plasma-treated rods resulted in loose tissue arrangement, collagen, and collagen/TGF-β-coated rods yielded thick, collagen-rich, densely packed tissue capsules, though with a random distribution of myofibroblasts. In contrast, chloroform-etched rods provided homogenous densely packed tissue capsules, completely populated by myofibroblasts. In conclusion, by varying the implant's surface characteristics, tissue capsule composition, cell distribution, and tissue arrangement could be tailored, enabling controlled guidance of the tissue response for in vivo vascular tissue engineering.
Introduction
T
Early tissue engineering approaches combining cell seeding with collagen scaffolds did not result in sufficient mechanical strength, 11 while the use of stronger nondegradable synthetic scaffolds do not overcome the initial drawbacks of using conventional vascular grafts. 12 Therefore, more recent approaches generally aim to ultimately fabricate a completely biological blood vessel, either via in vitro methods, 13 or with the use of a temporary scaffold that gradually degrades and is replaced by host cells and matrix.14,15
In contrast, an in vivo vascular tissue engineering approach using the subcutaneous space as bioreactor could rapidly generate a completely biological, autologous TEBV. This concept takes advantage of the foreign body response directed to a synthetic mold. Subcutaneous implantation of a cylindrical-shaped polymer rod will evoke an inflammatory response, culminating in the encapsulation of this rod by a fibrocellular tissue capsule. After removal of the rod, this tube-shaped tissue capsule forms a basis for a TEBV. Although the concept of in vivo tissue engineering is not new,16–18 no studies have been performed that systematically compare a set of different materials, surface modifications, and bioactive coatings on their ability to actively steer the tissue response for these vascular tissue engineering purposes. The chemical, physical, and morphological properties of the implant material's surface influence the cellular response upon implantation and thereby the tissue capsule formation.19–22 Polymer characteristics such as wettability influence protein adsorption and cell attachment 23 and the surface's topography and chemistry can largely affect cell morphology, function, and cytokine profile expressed.20–22 These variables were modulated by varying co-polymers ratio's and surface modifications. The use of the elastomeric co-polymer poly(ethylene oxide terephthalate)–poly(butylene terephthalate) (PEOT/PBT) enables tuning of surface wettability 24 and protein adsorption 25 by altering the ratio of the two polymers. Surface treatment may further enhance tissue formation. Solvent etching can both pattern the polymer surface and increase protein adsorption and cell attachment.26,27 In addition, gas plasma treatment may alter surface topography, chemical composition, cell attachment, and morphology.28–30 Next to a polymer-based approach, coating of the implant material with growth factors could promote cell differentiation and matrix synthesis.31,32 We therefore hypothesized that the tissue capsule formation around a subcutaneously implanted synthetic rod could be tailored by modulating the implant's surface characteristics. Rods of co-polymer were produced using various ratios of PEOT and PBT to create a range of physicochemical properties. We subsequently evaluated a set of physical, chemical, and biological surface modifications on their ability to steer fibrocellular tissue capsule formation for vascular tissue engineering purposes using a rat model as testing platform.
Materials and Methods
Fabrication of rods
All implant materials used are summarized in Table 1. Solid cylindrical-shaped rods composed of the elastomeric co-polymer PEOT/PBT (IsoTis Orthopedics S.A.) of 1.75±0.25 mm in diameter and 2 cm in length were fabricated with a rapid prototyping unit 33 (Envisiontec GmbH) used as melt extruder. Briefly, PEOT/PBT granules loaded into a syringe were heated to 180–200°C. Nitrogen gas of 4–5 bars was applied to extrude the melted polymer. Two different compositions of PEOT/PBT were used: a weight % of PEOT/PBT of 55/45 (Pa300) and 70/30 (Pa1000) with the molecular weight of the initial polyethylene glycol (PEG) used for the co-polymer reaction being respectively 300 and 1000 g/mol. As control, biocompatible poly-ɛ-caprolactone (PCL) rods of similar dimensions were fabricated using melt extrusion (Axon mini-extruder; Axon AB Plastmaskiner). PCL pellets (Purasorb PC 12; Purac Biomaterials) were heated up to 170°C and stirred (0.6 cc/revolution) until they were completely melted. Subsequently, PCL was extruded under a pressure of 25 bar through a capillary to fabricate cylindrical rods.
aPEOTbPBTc, with a the molecular weight of the initial PEG blocks used in the copolymerization, b and c resp. the weight ratios of PEOT and PBT used.
PBT, poly(butylene terephthalate); PEG, polyethylene glycol; PEOT, poly(ethylene oxide terephthalate).
Surface modification of implant material
For chloroform etching, unmodified Pa300 rods were immersed in chloroform (Merck Millipore) and quickly air-dried to let the remaining chloroform evaporate. Rods were then washed in ultrapure water, sonicated twice for 15 min at 42 kHz to assure complete removal of the chloroform and air-dried. For oxygen gas plasma treatment, unmodified Pa300 rods were treated with 100 mTorr of oxygen gas at either 30 or 100 W for 5 min (reactive ion etching; Teske, University Twente, The Netherlands). All rods were sterilized by gamma-radiation (Synergy Health) with a dose of >25 kGy. In addition, sterile 100 W oxygen-treated Pa300 rods were dipped in a TGF-β3/collagen solution for 1 minute in a flow cabinet under sterile conditions. TGF-β3 solution consisted of activated TGF-β3 (R&D Systems) mixed in sterile rat tail collagen I (5 mg/mL; Culturex) resulting in a TGF-β concentration of 10 ng/mL. As control, similar oxygen-treated Pa300 rods were dip-coated in rat collagen I (5 mg/mL; Culturex) without TGF-β for 1 minute. Rods were air-dried and directly used for implantation.
Scanning electron microscopy analysis
Surface topography of all rods was verified using scanning electron microscopy (SEM). Rods were cut in pieces of 0.5–1 cm in length and gold sputter-coated. Several parts throughout the rods were evaluated. The effect of sterilization by gamma-radiation on all rods was evaluated on random samples using SEM.
In addition, SEM-images were used to quantify the surface roughness by measuring the mean gray value of the SEM-image using ImageJ. This results in a relative surface roughness value. Contrast and brightness were kept constant when all SEM-images were taken. In short, gray values of a surface of 100 μm2 were measured using ImageJ and plotted. The mean gray value was considered as baseline. All points projecting from baseline were totaled, thus accounting for both the height and frequency of the surface patterning, and divided by the amount of measurements. In total six measurements of three SEM-images were performed per type of rod. Values of all different types of rods were compared with each other.
Rat model
All experiments were approved by the Animal Care and Use Committee of the Leiden University Medical Center and were performed in accordance to Dutch legislation. Fifteen 13-week-old male Wistar rats (Charles Rivers) were housed in standard cages with ad libitum food and water intake. All operations were performed under isoflurane inhalation anesthesia. Per rat, four rods were implanted in the subcutaneous space of the abdominal area. Unmodified PCL rods serving as a control were implanted five times and all Pa300 and Pa1000 unmodified rods and all Pa300 modified and coated rods were implanted nine times. Following a small horizontal incision of ca. 1 cm, a longitudinal subcutaneous pocket was formed and the rods were inserted in this pocket. The incision was closed using 4-0 vicryl sutures (Johnson & Johnson). Rats directly received postoperational analgesia via per-operative injection of perfalgan (200 mg/kg). In addition, perfalgan (2.7 mg/mL) was added to the drinking water up to 1 day after surgery. After 3 weeks, rods with tissue capsules formed around it were harvested and the animals were sacrificed. Abdominal aortas of these rats were harvested and used to compare to the generated tissue capsules.
Analysis of tissue capsules
Tissue capsules containing rods were fixed in 4% paraformaldehyde. After extrusion of the rods tissue capsules were processed and embedded in paraffin. Serial cross sections of 5 μm of two parts of each tissue capsule were made for histological, immunohistochemical, and morphometrical analysis. All samples were routinely stained with hematoxylin-phloxine-saffron (HPS). To characterize the extracellular matrix, serial sections of each tissue capsule were stained with picrosirius red for collagen, alcian blue (pH 2.5) for glycosaminoglycans (GAGs), weighert's elastin for elastin, and alizarin red to assess potential calcification. Elastin was visualized using autofluorescence, excitated with blue light and unmixed with spectral microscopy (Nuance Fx). Picrosirius red-stained sections were analyzed using bright field microscopy and with polarized light. The tissue capsule sections were compared with similar sections of the medial layer of a rat aorta. Cellular composition of tissue capsules was characterized using immunohistochemistry, with antibodies against α-smooth muscle actin (α–SMA, 1:1000; Dako) for myofibroblasts, vimentin (1:300, heat-induced proteinase K antigen retrieval; Immunologic) for fibroblasts, desmin (1:250, heat-induced 0.1% trypsin antigen retrieval; Immunologic) for contractile smooth muscle cells, CD45 (1:50, heat-induced 0.1% trypsin antigen retrieval; Immunologic) for leukocytes, Von Willebrand factor (1:300, heat-induced 0.1% trypsin antigen retrieval; Dako) for endothelial cells, and Ki67 (1:20, heat-induced citrate antigen retrieval; BD Science) for proliferating cells and visualized with 3,3′-diaminobenzadine (DAB). Discrimination between fibroblasts, myofibroblasts, and contractile smooth muscle cells was made as described elsewhere. 34 In addition, a TUNEL-assay (Sigma Aldrich) was performed according to the manufacturer's instructions, fluorescently labeled with fluorescein isothiocyanate (FITC), and counterstained with 4′,6-diamidino-2-phenylindole (DAPI) to evaluate apoptotic cell death and, in combination with the Ki67 staining, cell turnover in the tissue capsule. Negative controls were obtained using an isotype antibody and in addition for all stainings a positive control was taken along. In addition, rods were stained with methylene blue after extrusion from the tissue capsule to determine whether any tissue adhered to the rod.
Statistical analysis
Data are presented as mean±standard error of the mean. All data were analyzed with a one-way ANOVA test using SPSS. Tukey post hoc analysis was performed to compare surface roughness gray values of all different rods and p-values of <0.05 were considered statistically significant.
Results
Implant material
SEM-images confirmed that all unmodified rods had a completely smooth surface (Fig. 1A–C), whereas surface modification by oxygen gas plasma treatment (Fig. 1D, E) and chloroform etching (Fig. 1F) indeed resulted in marked alterations in surface topography, creating distinct homogenously patterned surfaces. Chloroform etching resulted in formation of superficial pores ranging from 0.5 to 2.5 μm in diameter with some infrequent larger pores ranging from 10 to 20 μm in diameter (Fig. 1F), while oxygen treatment resulted in spiked peaks (Fig. 1D, E), with a larger depth for 100 W compared with 30 W oxygen gas plasma treatment. Image analysis revealed that all surface modifications resulted in increased surface roughness and significantly differed from one another (Fig. 2). Gamma-radiation did not affect the surface topography (data not shown).
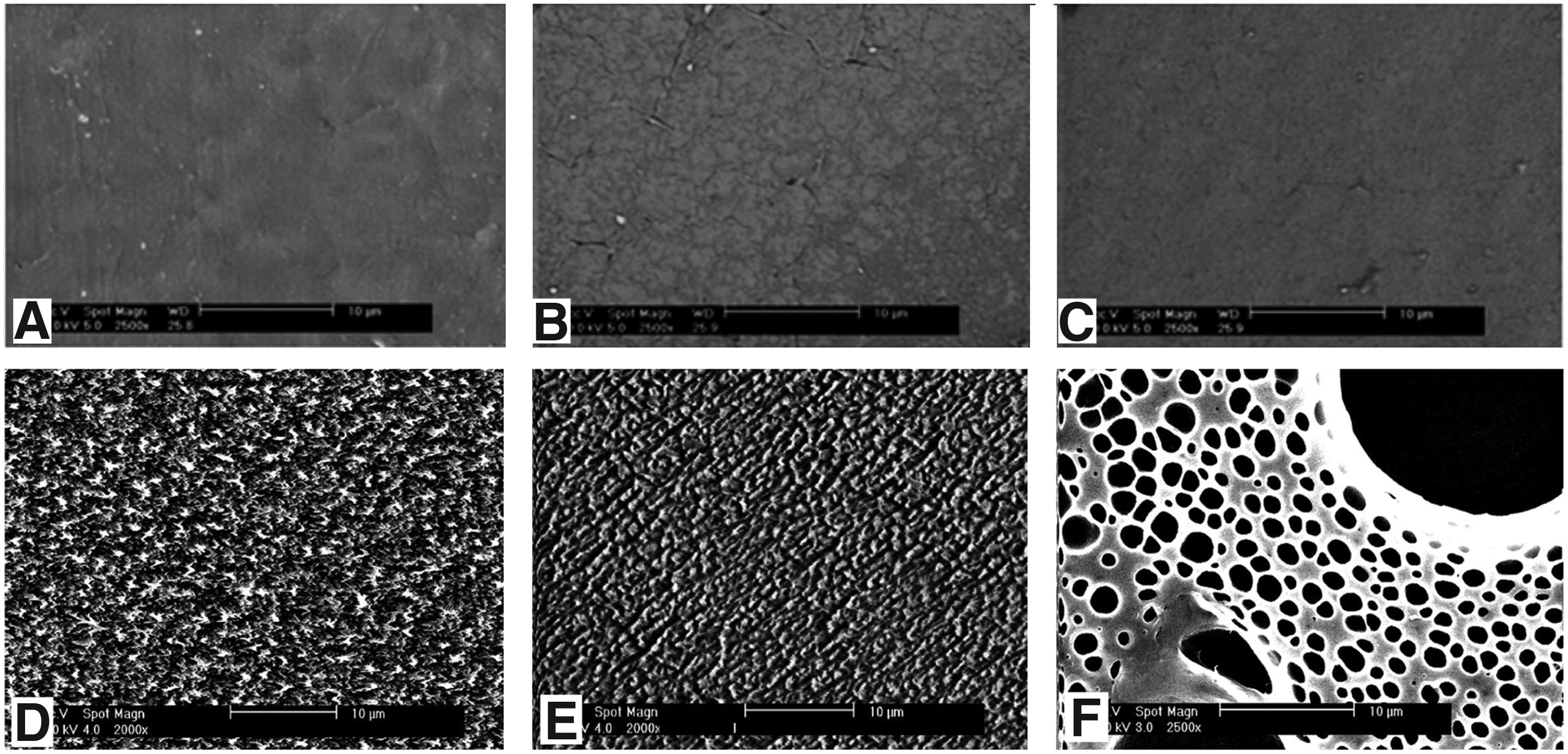
Scanning electron microscopy images of different types of unmodified and modified rods.
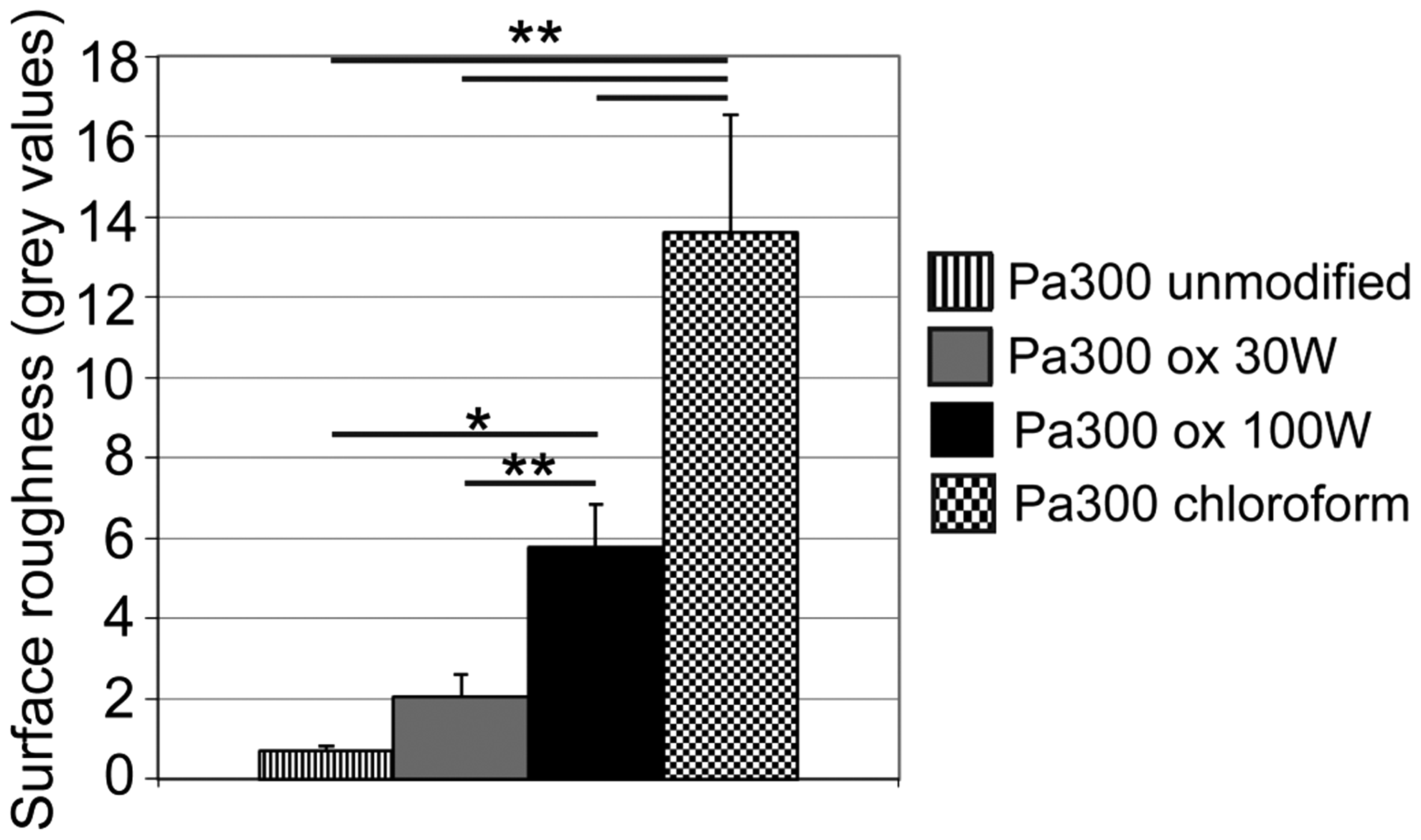
Gray value measurements indicating the surface roughness of unmodified and modified Pa300 rods. Pa300 oxygen 30 W-treated rods did not significantly differ in surface roughness compared to unmodified Pa300 rods. Apart from this, all types of rods were significantly different in surface roughness compared to each other. *p<0.05, **p<0.01.
General tissue capsule formation
One Pa1000 rod was not in situ any more at time of harvesting. Most likely, the rat bit through the sutures thereby opening the subcutaneous pocket. However, other reasons such as inflammatory mediated removal of the foreign body from the body cannot be fully excluded. In all other cases, rods were successfully harvested 3 weeks after implantation. Rods were completely encapsulated by a well-vascularised tissue capsule, with a more pronounced tissue response at the rims of the rods. Tissue capsules were attached to the surrounding subcutaneous tissue but could easily be harvested and subsequently smoothly extruded from the rod. Methylene blue staining of the rods after extrusion from the tissue capsule showed that hardly any tissue remained on the unmodified rods, and little tissue on the surface modified and coated rods (Supplementary Fig. S1; Supplementary Data are available online at
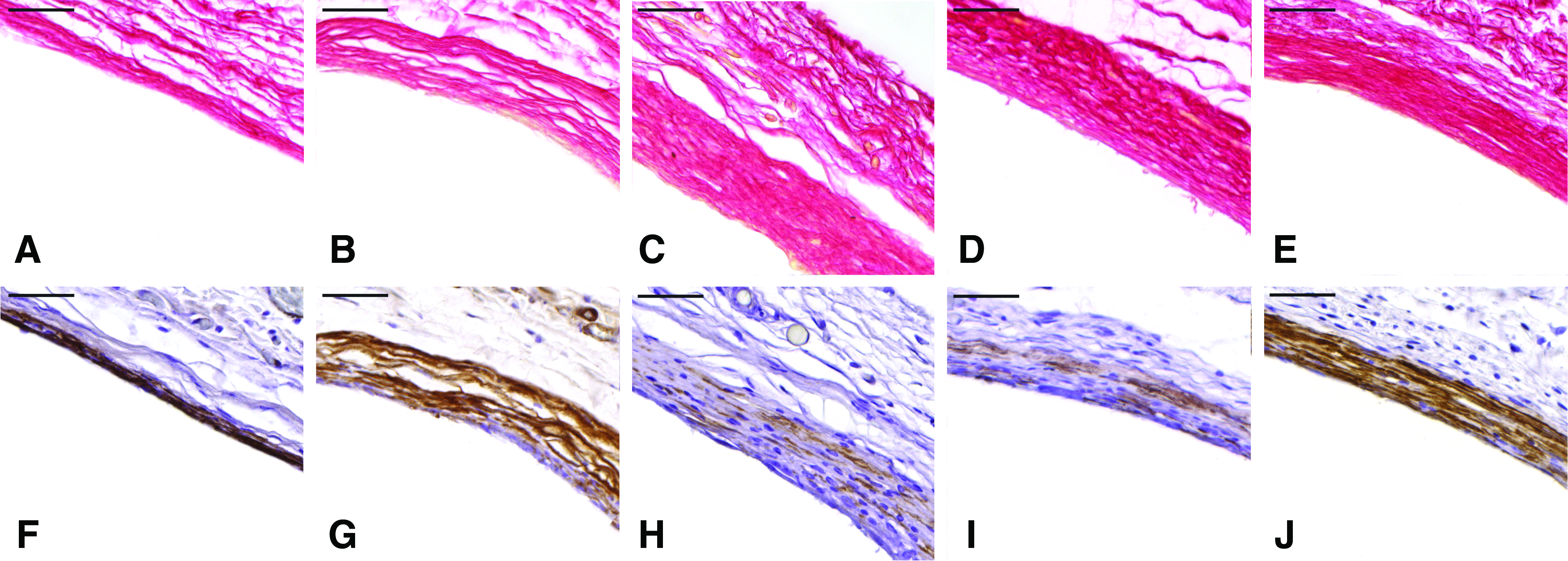
Macroscopically, no apparent differences were observed among tissue capsules formed around different types of rods. A macroscopic image of the tissue capsule is depicted in Figure 3A. Histology revealed that all tissue capsules were composed of collagen (Fig. 3B) and myofibroblasts as main cell type (Fig. 3C). Overall, the matrix of the tissue capsules was mainly composed of circumferentially orientated fibrillar collagen (Fig. 4B, C) and GAGs (Fig. 4E), in distribution comparable to a native artery (Fig. 4F–J). Surprisingly, there was some elastin present in the tissue capsules, though in contrast to native vessels only locally and in very little amounts (Fig. 4D, I). In terms of cellular composition, tissue capsules were dominated by circumferentially orientated α-SMA-positive, desmin-negative myofibroblasts (Fig. 5B, C). The remaining cells were mainly circumferentially orientated vimentin-positive, α-SMA-negative fibroblasts (Fig. 5A, B). In all cases, only few desmin-positive smooth muscle cells were present (Fig. 5C). CD45-positive leukocytes were only scarcely present (<1%) with minimal foreign body giant cell (FBGC) formation at the contact surface (Fig. 5D). Around the tissue capsule occasionally small polymer fragments were observed. These fragments did elicit a more pronounced inflammatory response at time of explantation of the tissue (Supplementary Fig. S2). HPS staining revealed cells with multiple nuclei in the cytoplasm suggestive for a FBGC (Supplementary Fig. 2A, B). In addition, some cells surrounding the polymer fragment were CD45 positive (Supplementary Fig. S2C). Alizarin red staining revealed no signs of calcification (Supplementary Fig. S3). The subcutaneous space generally has a low cell density and very loosely arranged, randomly distributed collagen, whereas the subcutaneous collagen neighboring the tissue capsule was in part deposited in semi-densely packed, organized layers with increasing cellularity, forming a transitional phase between the tissue capsule and the subcutaneous space. This area thus formed an adventitial-like layer with collagen (Fig. 4B), some fibroblasts (Fig. 5A), and small vessels (Fig. 5E).

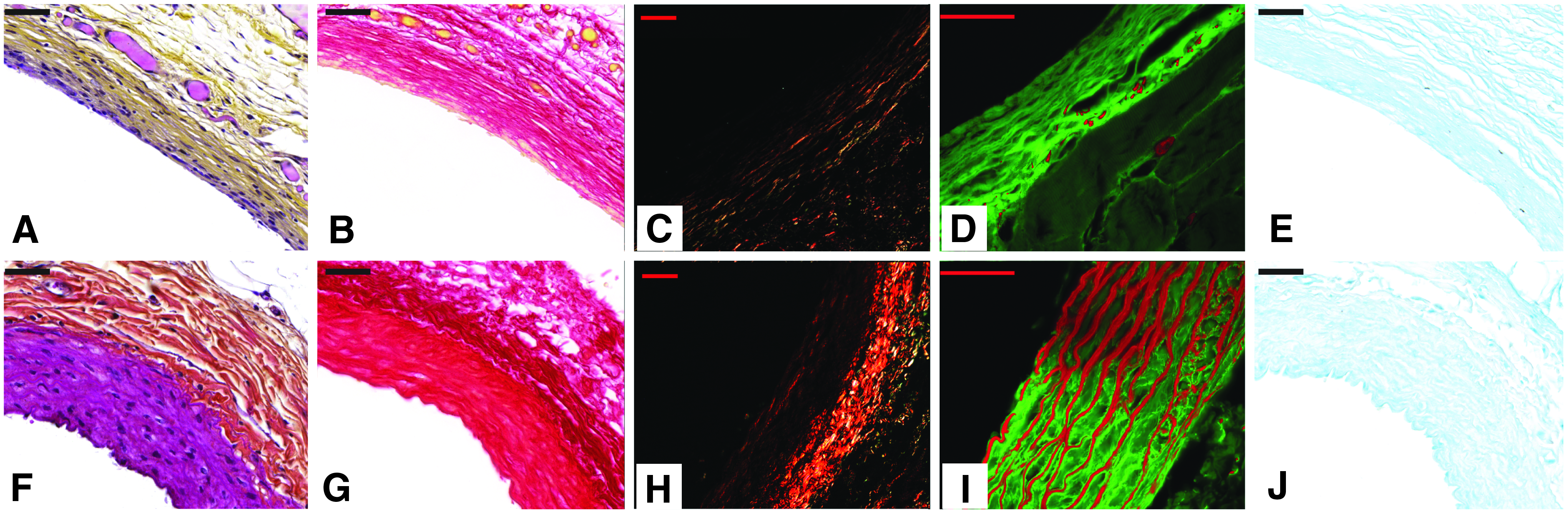
Detailed images of extracellular matrix composition of a tissue capsule formed around a Pa300 chloroform-treated rod (upper panel) compared to a rat aorta (lower panel).
Detailed pictures of cellular composition of serial sections of a tissue capsule formed around Pa300 chloroform-treated rod
Selection of implant material for surface modification
First, three types of unmodified rods were evaluated on their ability to influence the tissue response upon implantation. Although as described above the tissue capsules formed around all three rods had the same composition, they discernibly varied in relative proportion of especially collagen and myofibroblast content (Fig. 6). While the biocompatible PCL rods were encapsulated by a thin-walled, relatively acellular tissue capsule with few myofibroblasts (Fig. 6A, D), Pa1000 (Fig. 6B, E) and Pa300 rods (Fig. 6C, F) were encapsulated by a thicker, cell-rich tissue capsule mainly composed of myofibroblasts. There were no apparent differences between tissue capsules formed around Pa300 and Pa1000 in histology (Fig. 6B, C, E, F). However, in contrast to the other rods, Pa1000 rods became rather fragile during implantation, likely due to a faster degradation, and tended to break during harvesting with the risk of damaging the tissue capsules. Surface modifications were therefore performed on Pa300 rods.

Detailed pictures of picrosirius red staining
Tissue capsule formation around surface-modified Pa300 rods
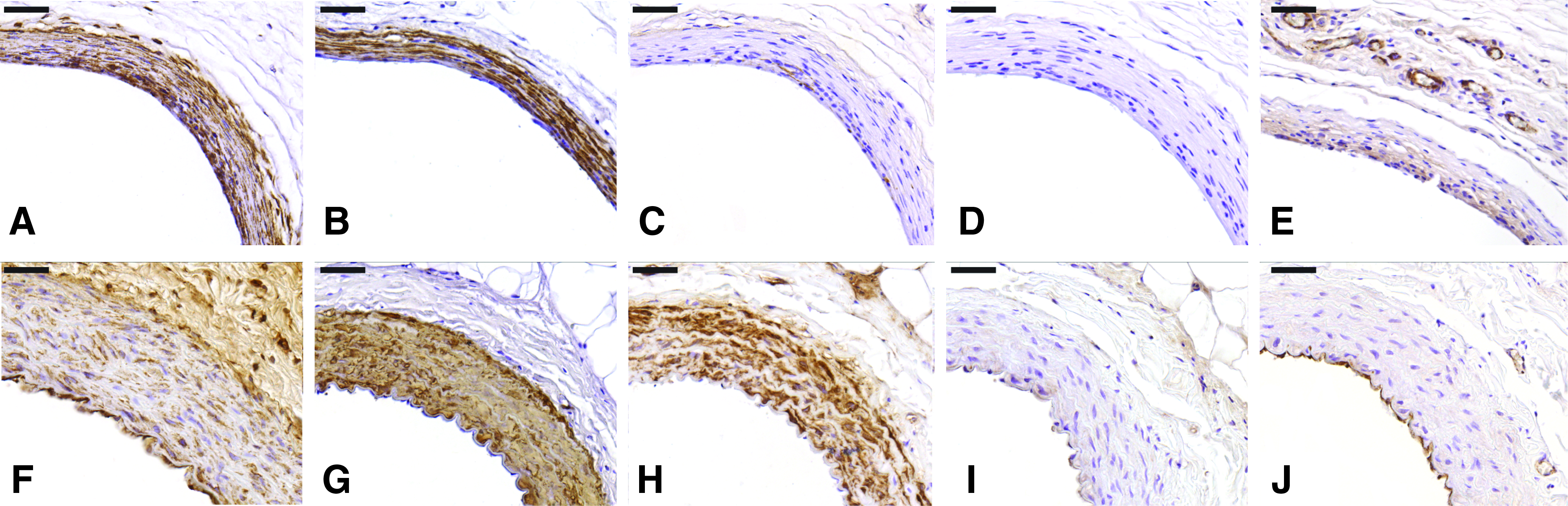
Similar to the unmodified rods (Fig. 6), the relative proportion of especially collagen and myofibroblasts largely varied between different types of modified rods (Fig. 7). Compared to unmodified rods, all modified rods had a larger wall thickness with consequently apparently more collagen and myofibroblasts (Fig. 7). In all tissue capsules some proliferating cells were present, mainly in the inner layers of the tissue capsule wall (Fig. 8A–E). No signs of apoptotic cell death were observed in any of the tissue capsules (Fig. 8F–J). Marked differences in morphology between different types of modified rods were observed (Fig. 7). Oxygen-treated rods yielded tissue capsules with a rather thick wall, yet very loosely arranged (Fig. 7B, G). Compared to unmodified, both oxygen-treated/collagen-coated rods (Fig. 7C) and oxygen-treated/TGF-β/collagen-coated rods (Fig. 7D) provided thick, densely packed tissue capsules. However, the relative proportion of myofibroblasts was lower compared to unmodified rods, with a relative random distribution of myofibroblasts throughout the tissue capsule wall (Fig. 7F, H, I). No apparent morphological differences between oxygen-treated/collagen-coated and oxygen-treated/TGF-β/collagen-coated rods were observed (Fig. 7C, D, H, I). Yet, chloroform-treated rods resulted in rather thick tissue capsules, with an evenly distributed wall thickness (Figs. 3 and 7E) and were almost completely composed of densely packed, homogeneously dispersed myofibroblasts (Figs. 3 and 7J).
Detailed pictures of picrosirius red staining
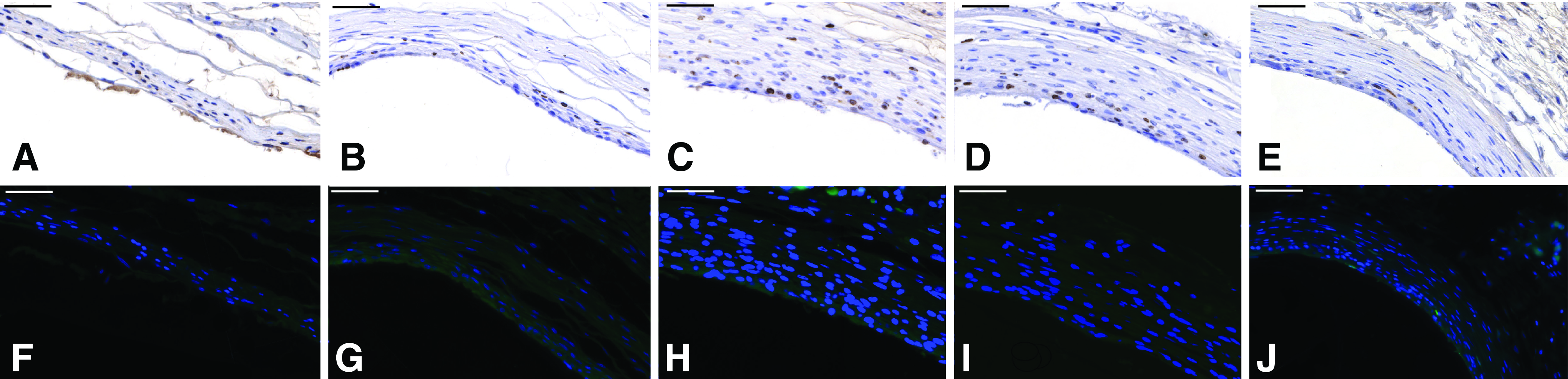
High magnification representative pictures of Ki67 proliferation staining (upper panel) and TUNEL staining (lower panel) of tissue capsule formed around
Discussion
In this study, a set of different physical, chemical, and biological surface modifications on the elastomeric co-polymer PEOT/PBT were evaluated on their ability to actively steer the tissue response for vascular tissue engineering purposes, using a rat model as testing platform. This study shows that by modulating these implant's surface characteristics, the tissue capsule formation can be tailored, mainly by affecting the amount and distribution of collagen and myofibroblasts in the tissue capsule wall.
Much is known about cell–material interaction in vitro and the tissue response upon implantation in vivo. 35 However, most studies focused on different tissues such as bone or aimed to avoid encapsulation. 36 In contrast, our in situ tissue engineering method aims to deliberately evoke a pronounced tissue response, with specific requirements to cell type, matrix formation, alignment, and distribution of the generated tissue.
Using the foreign body response to generate tissue engineered vascular constructs
The generated tissue capsules were generally composed of GAGs, circumferentially aligned collagen, and myofibroblasts. Although the evoked response is essentially an inflammatory reaction, there were hardly any leukocytes or FBGCs present in the tissue capsules. Likely, this is dependent on the length of the implantation period. The foreign body response is dynamic, starting with an acute inflammatory phase dominated by neutrophils and macrophages that in weeks resolves in a more fibrotic response with influx of (myo)fibroblasts and matrix formation.31,35,37,38 In time, a rather acellular collagenous tissue capsule remains. 31 Our tissue capsules did not contain many leukocytes suggesting the inflammatory phase had largely resolved. The tissue capsules were still cell rich but showed only moderate proliferation with a negative TUNEL staining, suggesting mere proliferation instead of cell turn-over. This moderate proliferative activity suggests that the fibrotic phase of the foreign body response is still ongoing. Based on this, a 3-week implant period seems suitable for obtaining a matrix and cell-rich, noninflammatory tissue capsule.
Modulation of the foreign body response by altering implant material's surface characteristics
This study indicates that implant properties can favorably impact the tissue response in terms of morphology and composition. Compared to conventional PCL, tissue capsules formed around Pa300 and Pa1000 rods differed in wall thickness and composition. Indeed, PCL is more hydrophobic compared to Pa300 an Pa1000 39 and may therefore be less supportive for cell attachment. 23 Yet, more pronounced differences in both composition and morphology of the tissue were obtained by surface treatment and bioactive coating, in concordance with other studies22,40,41 underlining the impact of surface characteristics on the tissue response. We demonstrated that in comparison to its unmodified counterpart, chloroform etched and oxygen plasma-treated surfaces increased myofibroblast and collagen content of the tissue capsules. Plasma treatment is a well-known surface modification method that alters surface topography, roughness, and wettability, 42 thereby enhancing cell attachment, proliferation, and differentiation.28,29,43 Chloroform is conventionally used as a solvent for Pa300 44 and can therefore function as etching agent. Indeed, both oxygen gas plasma and chloroform treatment resulted in increased surface roughness, and enhanced tissue capsule thickness. While oxygen gas plasma treatment resulted in spiked structures on the surface, chloroform etching created a porous surface. The difference in surface texture may have dictated the tissue capsule morphology and explain the loose tissue arrangement around oxygen-treated rods compared to the densely packed tissue capsules formed around chloroform-etched rods. Indeed, the micropattern design of the surface has been shown to influence cell alignment and amount of tissue formation.45,46 Fibroblastic cells are particularly sensitive to these changes in surface patterns. 47 Interestingly, especially small pores of a few micrometer, such as the pores created with chloroform etching, promote fibroblast migration and proliferation. 46 Although oxygen-treated rods resulted in thick tissue capsules, the loose arrangement is not favorable for a vascular construct. In contrast, implantation of chloroform-etched rods favorably resulted in the most homogenous, collagen and myofibroblast-rich tissue capsule.
Modulation of the foreign body response by bioactive coating of the material
In addition to mere surface modification, the oxygen modified rods were coated with collagen and collagen/TGF-β. TGF-β induces fibroblasts to myofibroblasts differentiation and exerts pro-fibrotic effects. 32 Coating of the oxygen-treated rods with collagen alone and collagen/TGF-β apparently resulted in a large increase in collagen formation and wall thickness compared with unmodified rods. Yet, collagen/TGF-β coating of the oxygen-treated rods did not result in different tissue capsules compared to collagen coating of the oxygen-treated rods alone, suggesting that the result in the collagen/TGF-β coating is merely accredited to collagen. Collagen exhibits a wide range of biological functions. It supports integrin-mediated fibroblast binding and influences cell morphology, proliferation, and protein synthesis. 48 Indeed, collagen-coated materials have been shown to promote matrix formation in vivo 49 and fibroblast attachment in vitro 50 compared to its noncoated equivalents. As TGF-β is well known for its wound-healing activity, 51 the addition of TGF-β to collagen coating was hypothesized to further increase the (myo)fibroblast content and matrix formation and arrangement in the tissue capsules. Surprisingly, there were no significant differences in morphology of the tissue capsules compared to merely collagen-coated rods. The lack of accumulating effect of TGF-β might be attributed to the relatively short activity of the single dose-activated TGF-β that ranges depending on the application method from hours to several days. 52 In contrast, TGF-β levels in the foreign body response peak after 1 week and remain elevated for several weeks. 31 Moreover, fibroblasts participate in the foreign body response from 1 to 2 weeks after implantation onward.31,38 Thus, the largest effect of TGF-β might be induced especially after 1–3 weeks, 31 when sufficient fibroblasts are present.
Despite the fact that collagen and collagen/TGF-β-coated oxygen-treated rods apparently resulted in the largest wall thickness, the lower relative proportion of myofibroblasts and their random distribution renders these coatings in our opinion less favorable as bioactive mold for vascular tissue engineering than, for example, chloroform-treated Pa300 rods that generated myofibroblast-rich, homogeneous distributed tissue capsules.
The concept of in situ vascular tissue engineering
Some studies using a similar in situ vascular tissue engineering technique have previously been performed. Sparks pioneered this method in the 70s of the 20th century, using a so-called Sparks mandril to generate a tissue capsule that was grown around a porous Dacron mesh.17,53 This mandril was implanted for several months, preferably in the muscle. Despite initial promising results as vascular graft in dogs and humans,53,54 grafts largely failed due to thrombosis and aneurysm formation.55–57 Likely, this was the result of a lengthy implant period rendering tissue capsules with relatively low cellularity, the continuous presence of synthetic material in the vascular graft and the relatively random choice of biomaterial. It was concluded that this concept should not be used anymore, until more was known about the foreign body response. 58 Currently, much more is known on the biological response to biomaterials, making it possible to optimize this ingenious concept.
Other groups have studied a similar in vivo tissue engineering approach, but using the peritoneum as bioreactor. 16 However, intraperitoneal implantation and especially subsequent harvesting of the rods is rather invasive and has the risk of adhesion formation, possibly hindering successful clinical implementation. Moreover, not all rods became encapsulated upon peritoneal implantation,16,59 creating the necessity to implant several devices. The use of the subcutaneous space as bioreactor may circumvent the drawbacks of using the peritoneal cavity, as it is easy accessible and even in some clinical settings, such as hemodialysis vascular access, it is the very location where the vascular graft is required. Indeed, others have successfully used the subcutaneous space as bioreactor for tissue engineering purposes.18,60 Importantly, most components desirable for a TEBV, such as collagen, elastin, fibroblasts, and a large vascular network, are present in the subcutis. 61
The tissue capsules generated by guided triggering of the foreign body response are collagen and myofibroblast rich. Myofibroblasts are plastic cells that possess a contractile apparatus and can synthesize and remodel extracellular matrix if stimulated 32 and therefore seem suitable cells for the basis of a tissue-engineered vascular construct. Importantly, flow and cyclic strain are potent stimuli for matrix synthesis62,63 and even myofibroblast to smooth muscle cell differentiation. 64 Prior studies showed that myofibroblast-rich tissue capsules can actually remodel to smooth muscle cell-rich constructs once placed in the vasculature. 16 Thus, upon grafting in the vasculature and exposure to high flow, myofibroblast-rich tissue capsules might in time differentiate and develop toward a more vessel-like phenotype. 16 Based on the present results, in future studies bioactive implants can be created to generate optimal tissue engineered grafts that should be further tested as vascular graft.
Our tissue capsule lacks an endothelial lining. Although the protective role of endothelium to prevent thrombosis is well established, the question whether endothelial cells are indispensible in TEBVs remains a matter of debate, especially in high flow situations such as hemodialysis vascular access. Moreover, the addition of an endothelial layer would require several laborious and costly in vitro steps that would partly defeat the strength of an in vivo vascular tissue engineering approach. Importantly, the endothelial layer of native vessels used as vascular graft is frequently denuded during vascular surgery,65,66 yet they show very little acute thrombosis. Indeed, if thrombosis occurs, this is mainly secondary due to intimal hyperplasia. 7 Recently, several studies implanted endothelial-deficient tissue-engineered conduits as vascular graft in various vascular settings with excellent patency,14,15,67 These studies also underlined that endothelium-deficient grafts may re-endothelialize in time once implanted in the vasculature, even in grafts of >10 cm in length. 14 Currently, a large clinical trial using tissue-engineered grafts without endothelial lining is being performed (clinicaltrial.gov, NCT01744418). Future studies where our tissue capsules are implanted in the vasculature should reveal if the patency is indeed adequate without endothelium and if spontaneous re-endothelialisation will occur.
A potential study limitation is the translation of the foreign body response from rats to humans. Indeed, it is not completely known how well the foreign body response in many laboratory animal species corresponds with the human response. However, biomaterials used for medical purposes are frequently screened on functionality and biocompatibility in rodent models using a subcutaneous or intramuscular implantation model.68–70 Such in vivo animal experiments are recommended in the ISO guidelines (ISO 10993: Biological of medical devices). In concurrence with our experiments, several groups using biodegradable synthetic scaffolds that are in vivo degraded as part of the foreign body response and replaced by host cells and matrix have been tested in rat models.15,67
Conclusions
This study illustrates that by exploiting the tissue response directed to a cylindrical polymer rod, a tube-shaped tissue capsule can be generated. By modifying the implant's surface characteristics, the tissue response can be tailored, mainly by affecting the amount, distribution, and organization of collagen and myofibroblasts. Based on these results, in future studies optimal bioactive molds can be fabricated to develop and evaluate tissue capsules as vascular graft.
Footnotes
Acknowledgments
T.C.R., J.I.R., F.F.R.D., L.M., and T.L. are supported by the research program of the BioMedical Materials institute (P3.03 DialysisXS), co-funded by the Dutch Ministry of Economic Affairs, Agriculture and Innovation. This study was supported by a grant by the Dutch Kidney Foundation. M.J. Goumans is gratefully acknowledged for supplying TGF-β.
Disclosure Statement
All the authors declare no competing financial interests.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.