
Abstract
Tissue-engineered composite skin is a promising therapy for the treatment of chronic and acute wounds, including burns. Providing the wound bed with a dermal scaffold populated by autologous dermal and epidermal cellular components can further entice host cell infiltration and vascularization to achieve permanent wound closure in a single stage. However, the high porosity and the lack of a supportive basement membrane in most commercially available dermal scaffolds hinders organized keratinocyte proliferation and stratification in vitro and may delay re-epithelization in vivo. The objective of this study was to develop a method to enable the in vitro production of a human skin equivalent (HSE) that included a porous scaffold and dermal and epidermal cells expanded ex vivo, with the potential to be used for definitive treatment of skin defects in a single procedure. A collagen–glycosaminoglycan dermal scaffold (Integra®) was populated with adult fibroblasts. A near-normal skin architecture was achieved by the addition of coagulated human plasma to the fibroblast-populated scaffold before seeding cultured keratinocytes. This resulted in reducing scaffold pore size and improving contact surfaces. Skin architecture and basement membrane formation was further improved by the addition of aprotinin (a serine protease inhibitor) to the culture media to inhibit premature clot digestion. Histological assessment of the novel HSE revealed expression of keratin 14 and keratin 10 similar to native skin, with a multilayered neoepidermis morphologically comparable to human skin. Furthermore, deposition of collagen IV and laminin-511 were detected by immunofluorescence, indicating the formation of a continuous basement membrane at the dermal–epidermal junction. The proposed method was efficient in producing an in vitro near native HSE using the chosen off-the-shelf porous scaffold (Integra). The same principles and promising outcomes should be applicable to other biodegradable porous scaffolds, combined with autologous cells, for use in wound treatment.
Introduction
T
Despite recent advancements in bioengineered therapies, treatment of wounds with a definitive skin substitute to replace both damaged dermis and epidermis in a single procedure still remains a challenge. Not surprisingly, human de-epidermized dermis (DED) has been proposed as an ideal dermal component with the advantageous retention of the basement membrane and consequent improved re-epidermization; however, restricted DED availability is a strong limitation for widespread clinical application.1,2 While crude collagen preparations or nonbiodegradable synthetic fibrous materials may be unsuitable for use as HSE dermal scaffolds due to uncontrollable degrees of absorption and integration to the wound bed,3–9 some tissue-engineered scaffolds widely used in clinical practice, such as Integra, may provide suitable off-the-shelf alternatives. These scaffolds are manufactured under approved safety and quality standards with demonstrated adequate porosity (20–125 μM) that allows for host cell infiltration and vascularization, while providing resistance to rapid degradation by wound collagenases in vivo. The pore configuration may significantly influence overlay graft take and skin regeneration.10,11 This is exemplified in various reports of application of Integra combined with a split-thickness skin graft or autologous cultured skin equivalents to provide permanent closure of chronic and acute wounds in two-stage procedures.12–15 However, normal epidermization and stratification in vitro before grafting is required to achieve wound closure upon grafting in a single procedure. Integra's degree of porosity (porosity within 70–200 μM) combined with the lack of a basement membrane equivalent, fails to provide an even surface that precludes efficient anchoring of keratinocytes and their harmonious proliferation and differentiation in vitro. Ultimately, effective neoepidermization is impaired and proliferating keratinocytes are seen to infiltrate the porous scaffolds, resulting in an irregular neoepidermis without proper basement membrane formation and wound closure. 16
One approach described has been to initially populate a dermal scaffold with neonatal fibroblasts for a long period of time (35 days) allowing deposition of neoformed extracellular components into the pores of the scaffold, providing an improved surface for a second-staged keratinocyte (neonatal) seeding on the surface. 8 However, the procedure is lengthy and the proposed use of neonatal cells does not provide for a consistent solution in definite wound closure as adult patients still require grafting of autologous keratinocytes.
Human plasma or fibrin (a key element in human plasma clot formation), has been used as a keratinocyte carrier in overlay grafting of previously incorporated allograft dermis, in a two-stage procedure.17–19 The fibrin is eventually digested by naturally occurring enzymes in the wound environment.
Our novel approach proposes the use of clotted human plasma to obstruct the excessive porosity and surface irregularity of a commercially available scaffold (Integra). In combination with preseeding of fibroblasts, the method shortens the preparation time of a composite HSE with a suitable architecture and substrate for keratinocyte attachment and efficient neoepidermization.
Materials and Methods
Access to human skin tissue and fresh frozen plasma
Skin tissue discarded during elective breast reduction or abdominoplasty surgery was obtained after informed consent, following research project approval by the Alfred Hospital and Monash University Human Research Committee, Melbourne, Australia. Donation of fresh frozen plasma was also approved by Red Cross and Monash University Ethics committees.
Isolation and expansion of primary adult keratinocytes and fibroblasts
Adult human keratinocytes were isolated and cultured according to modifications of the protocol previously described by Green et al., 20 as follows: a 4–8 cm2 piece of skin was digested in Dispase II (4 mg/mL; Roche) overnight at 4°C to separate the epidermis. Mechanically separated epidermal sheets were digested with trypsin (0.25%; Life technologies) at 37°C for 5–7 min to release the basal keratinocytes.
Keratinocytes were primarily cultured and expanded on gamma-irradiated (60 Gy) 3T3-J2 feeders (3:1 ratio) in DMEM: F12 media (Life Technologies) supplemented with
Adult fibroblasts were isolated and cultured from the donated dermis based on the protocol described by Gagantirkar et al. 7 with modifications as follows. Dermal skin samples were cut into smaller pieces and digested in dispase/collagenase I (4 and 3 mg/mL, respectively; Life Technologies) in 20% bovine calf serum (Thermo Fisher Scientific) and 5 mM CaCl2 (Sigma) for 2.5–3 h at 37°C. Isolated cells were seeded and expanded in DMEM with bovine calf serum (10%; Sigma) and gentamicin (50 μg/mL; Life Technologies).
Construction of control and novel HSE
Integra Dermal Regeneration Template Single Layer (Integra Life Sciences) was cut into 2×2 cm2 pieces and washed three times in phosphate-buffered saline (PBS) containing CaCl2/MgCl2 for 30 min each.
The scaffold pieces for construction of control HSE were placed into deep well inserts (In Vitro Technologies), seeded with human adult fibroblasts (passage 2–8, 8×104 cells per insert), and immersed in DMEM containing 10% bovine calf serum,
For generation of the architecturally improved novel HSE, Integra scaffolds containing human fibroblasts as previously described were soaked in human plasma (20–25 mg/mL) and CaCl2 (1%) for 30 min at 37°C. Excess human plasma was washed once in PBS. Keratinocytes were seeded and cultured in a similar manner to controls, but for the addition of aprotinin (150 KIU 2 /mL; Sigma) to media epidermization I and II, until HSE were elevated to an air/liquid interface. Novel HSEs were fixed and analyzed after 7–10 days.
Adult fibroblast viability assay
Adult fibroblast viability in HSE postplasma clotting was tested using flow cytometry. Control HSEs and architecturally improved novel HSEs were seeded with adult fibroblasts (2×105 cells per insert) and cultured as described above. Adult fibroblasts were recovered by trypsinization postplasma clotting and labeled with propidium iodide (6.7 μg/mL; Sigma). The proportion of dead cells was detected using a BD FACSCalibur and analyzed using FlowLogic software.
Immunostaining
Cryopreserved sections (10 μm) of HSE samples (control and novel) collected at day 7–10 at air/liquid culture conditions, were cut and labeled according to standard protocols as follows. For immunohistochemistry studies, slides were blocked with 1% bovine serum albumin (BSA)/1.5% horse serum (Sigma) for 30 min at room temperature, followed by overnight incubation at 4°C with mouse anti-human K14 (1:500; Thermo Scientific), K10 (1:500; DAKO), or Ki67 (1:100; DAKO). The antigens were detected using an anti-mouse ABC kit (Vector Laboratories) according to the manufacturer's instructions. Slides were counterstained with Hematoxylin and photographed using an Olympus CKX41 microscope and DP21 camera.
For immunofluorescence, slides were fixed in 2% neutral buffered formalin for 20 min before blocking nonspecific binding sites with 10% BSA/10% goat serum in PBS for 30 min. Slides were incubated in mouse anti-human collagen IV (1:500; Sigma) or mouse anti-human LMN-511 antibody (1:1000; MERCK) overnight at 4°C and detected using donkey anti-mouse Alexa Fluor 568 (1:500; Life Technologies). Images were collected using an Olympus BX61 microscope and FVII camera and analyzed using ImageJ software.
Results
Integra® supports keratinocyte proliferation, but fails to generate normal skin architecture in an adult HSE model
To generate an HSE deemed suitable for clinical application, adult fibroblasts were seeded into Integra and cultured for 4–7 days before addition of human adult keratinocytes (Fig. 1). Keratinocyte stratification and differentiation was induced by culturing the composite skin in high calcium and air/liquid interface conditions.

Schematic diagram of the Human Skin Equivalent (HSE). Adult fibroblasts and keratinocytes were isolated and expanded in vitro. In
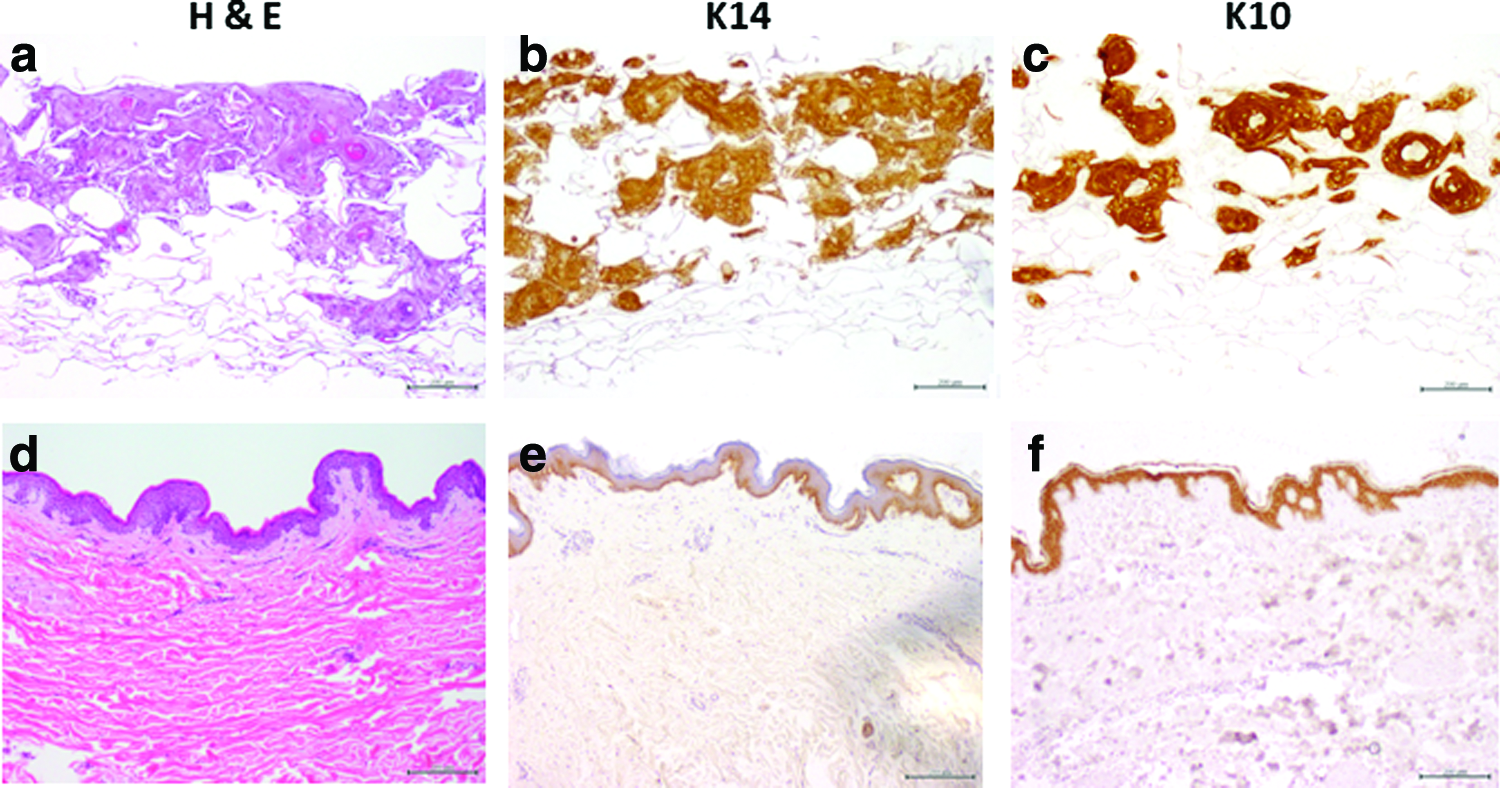
HSEs were fixed, sectioned, and stained for specific keratinocyte markers at the end of the culture period (Fig. 2a–c). H&E staining of HSEs confirm that Integra was able to support fibroblast survival and keratinocyte expansion. Nevertheless, in contrast to native multilayered epidermis (where Keratin 14 is expressed in basal layers and Keratin 10 is highly expressed in suprabasal layers, becoming reduced in the cornified upper layers), the neoepidermis formed in the HSE lacked normal stratification. Keratinocytes sunk into pores, often forming round cystic-like bodies with cell differentiation toward the centre as confirmed by K10 expression. Also, unlike in normal epidermis, Keratin 14 was expressed in the majority of keratinocytes.
Integra is capable of supporting epidermization although disorganized keratinocyte-specific marker expression in the HSE in the absence of plasma/aprotinin
The coagulated human plasma allowed for improved keratinocyte anchorage and stratified neoepidermis with similar expression of a differentiation marker as in native adult skin
Human plasma was polymerized (clotted) into the scaffold before seeding human adult keratinocytes to create a supportive surface on Integra for epidermization in the novel HSE. This was achieved by incubating the fibroblast-populated scaffold with human plasma and CaCl2 at 37°C. Calcium triggers thrombin activation in plasma which in turn causes fibrinogen coagulation to produce a fibrin clot. Clot formation was evident by naked eye (Supplementary Fig. S1; Supplementary materials are available online at

Clotted human plasma plus aprotinin creates a smooth surface for epidermization in HSE. This novel HSE presents close to normal skin histology. Integra, populated with human adult fibroblasts, was incubated in clotted human plasma plus aprotinin
Expressions of Keratin 14 and of Keratin 10 were investigated in immunohistochemistry preparations as markers for basal and suprabasal layers, respectively. As in native human skin, Keratin 14 was expressed in almost all basal keratinocytes; however, extended expression was noted in the suprabasal layers of the HSE. Keratin 10, similar to native skin, was highly expressed in differentiating suprabasal layers. The capacity for long-term novel HSE cell renewal was indirectly assessed by the presence of Ki67-positive cells as a marker for cell proliferation status.
The morphological improvement of novel HSEs is associated with the observed continuous and linear deposition of normal basement membrane proteins
Deposition of a basement membrane was established by immunofluorescence using anti-human collagen IV and laminin-511 antibodies (Fig. 4). Addition of human plasma and aprotinin in the novel HSEs favored the continuous deposition of a thin layer of collagen IV and laminin-511 that mimicked the basement membrane observed in normal skin. When aprotinin was not added to the media culture, keratinocytes still deposited collagen IV and laminin-511; however, the protein deposition did not have a clear direction in migrating keratinocytes which infiltrated into the dermal component. Of note, laminin-511 was also detected at lower levels in the suprabasal layers of the HSE, unlike in normal skin. The neoformed basal membrane ensured a strong enough dermal–epidermal bond that withstood the rather harsh histological processing.
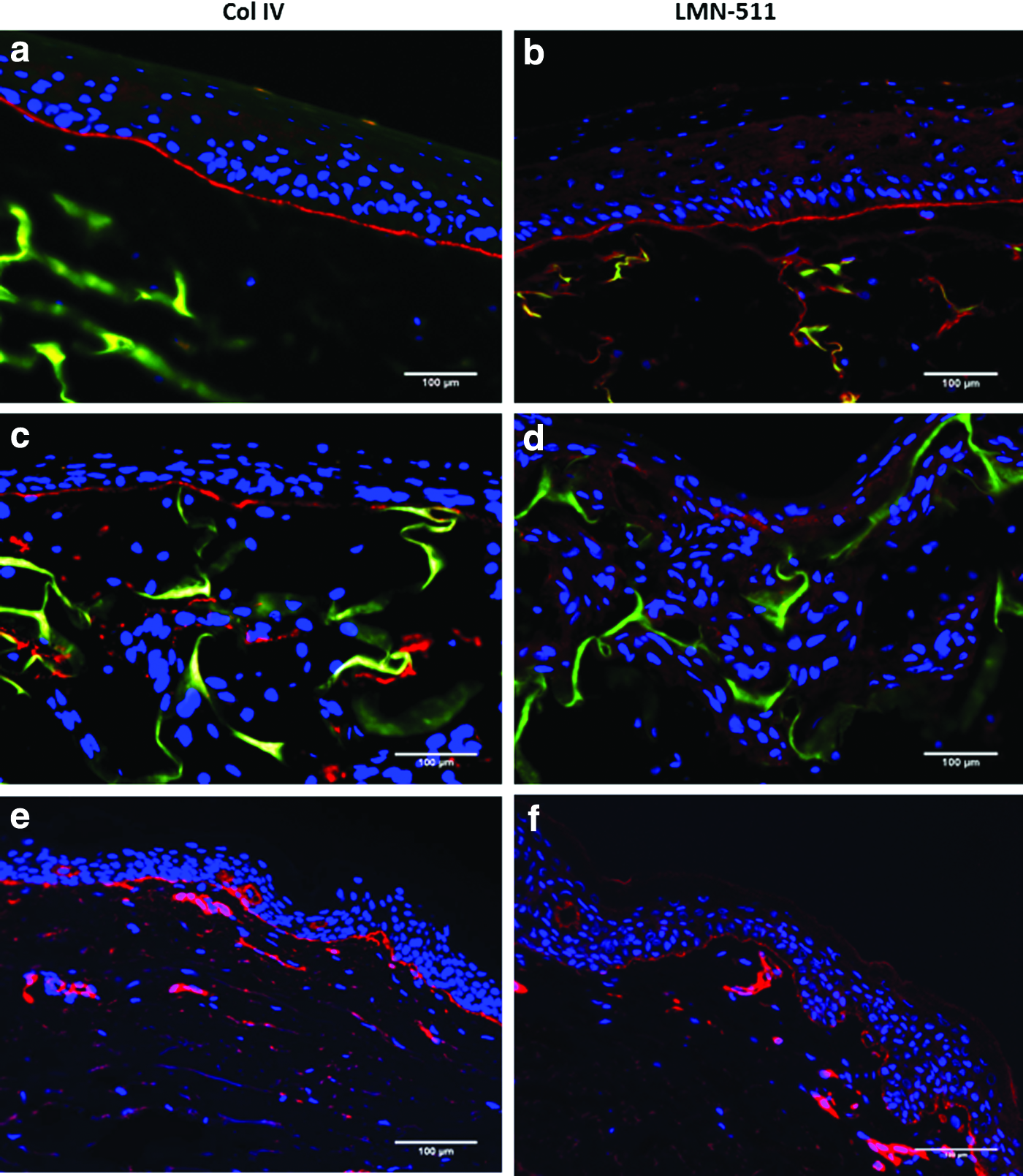
A continuous linear basement membrane is formed when both clotted plasma and aprotinin are added to HSE. Expression of basement membrane markers in this novel HSE in the presence
Discussion
This work describes an effective method for tissue engineering of composite skin that has potential application as a single-stage treatment of skin defects such as burns, chronic leg ulcers, and diabetic ulcers. There are a number of bilayer tissue-engineered skin products such as Apligraf®, Orcel®, and StrataGraft® available in the US or Europe, all of which carry allogeneic neonatal fibroblasts and keratinocytes and are therefore not suitable for permanent closure of a wound. Instead, they are used for the treatment of ulcers and/or burns as a temporary coverage or dressing.22,23 In this study, we have described in vitro methods for tissue engineering a skin substitute that can carry autologous adult keratinocytes on a clinically proven dermal substitute and therefore can potentially provide a permanent skin substitute for wound closure. Animal models are required for testing this product.
Similar to previously described outcomes,16,24,25 Integra, clinically proven to perform as an efficient dermal scaffold template, was able to support keratinocyte expansion in vitro. However, the resulting neoepidermis lacked normal structure. Obstructing the scaffold porosity optimized the conditions for Integra to sustain cellular components on its surface. A resulting novel HSE with at least three recognizable epidermal layers (stratum basal, spinosum, and corneum) was consistently achieved. The novel HSE neoepidermis differentiated in a similar pattern to native adult human skin (marked with expression of Keratin 10), and the presence of ki67-positive cells assured continued proliferation potential. Evidence of formation of the neobasement membrane was also observed using collagen IV and laminin-511 as markers.
Although essential for postgrafting cell influx and reduced wound contraction, 26 excessive scaffold porosity may be a hindrance for organized neoepithelialization. This was evident in the control HSE constructs; the lack of a smooth surface resembling a basement membrane for keratinocytes to anchor combined with the rugged topography promoted irregular neoepidermization.
Human plasma has previously been described in tissue engineering as a carrier for keratinocytes. It is rich in cytokines and growth factors and may also improve healing upon grafting.18,19 This work harnessed the plastic properties of a fibrin clot to introduce a novel improvement to existing models using porous scaffolds. Soaking the fibroblast-populated dermal substitute (Integra) in human plasma and calcium until its clotting, successfully reduced the pore size and created a smooth surface, which benefitted keratinocyte adhesion and establishment of a neoformed basement membrane, in a relatively short time interval.
Aprotinin, a serine protease inhibitor, was added to the novel HSE culture media to inhibit fibrinolysis and clot dissolution triggered by the keratinocytes. Plasminogen activators on the keratinocytes' cell membranes can activate plasmin (a serine protease) resulting in fibrin degradation. 27 This supports the observation that in the absence of added aprotinin, keratinocytes infiltrated the whole dermal component resulting in a disorganized keratinocyte proliferation. Once keratinocytes had proliferated past confluency for 4 days, aprotinin could be withdrawn from the culture media. Possibly at this stage, confluent keratinocytes form tight junctions and may have started to deposit basement membrane proteins and, therefore, are not as mobile and vulnerable to topographical irregularities as subconfluent keratinocytes.
Fibroblasts were incorporated to both control and novel HSE as a source of growth factors, such as KGF, that stimulate keratinocytes growth in a paracrine manner. Beyond important epidermal interaction during in vitro culture, fibroblast presence may be beneficial postengrafting in vivo where an HSE epidermis must rely on autocrine and paracrine growth factors for survival until effects of angiogenesis takes place. The graftability and timely vascularization of the proposed novel HSE construct is yet to be confirmed in animal studies.
A similar strategy presented here can be applied to other bioengineered scaffolds such as single-layer Pelnac® (porcine collagen crosslinked with glutaraldehyde) or MatriDerm® (bovine noncrosslinked lyophilized matrix coated with α-elastin hydrolysate). Pelnac, however, is not designed for in vitro culture and demonstrates major contraction and degradation during the culture period. MatriDerm, behaves similarly to Integra during the culture period and has been successfully used in single procedures in combination with split-thickness skin graft in replacing full-thickness burns. 28 Our novel strategy in constructing a composite skin in culture reduces the need for donor skin and ensures that cultured epidermis has formed a strong dermal–epidermal junction with the scaffold and can potentially sustain shear force postgrafting. This strategy requires further testing in animal models. It would be interesting to compare the graftability and vascularization of our novel composite skin using MatriDerm or Integra in vivo.
Permanent and rapid wound closure is essential for retention of moisture, electrolytes, and thermoregulation. Some commercially available scaffolds have proven their capacity to become permanently engrafted in the wound bed providing for a dermal scaffold. However, the required porosity for revascularization of these scaffolds may be the main deterrent for wound epithelialization and rapid wound closure. Enabling improved keratinocyte proliferation, effective neoepidermal and basement membrane formation in bioengineered HSE is a major development toward single-stage procedures. The conceptual use of clotted plasma as an agent to ameliorate surface conditions and cell adhesion could be extended to other nontoxic and biodegradable porous scaffolds for in vitro or in vivo permanent skin substitute development.
Footnotes
Acknowledgments
The authors like to acknowledge LEW Carty Charitable and Alfred Foundation for funding this project and Professor Stephen M. Jane and Dr. Stephen Goldie for critical evaluation of the article. The authors also thank Monash Micro Imaging for their assistance with microscopy.
Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.