
Abstract
Giant congenital melanocytic nevi are intractable lesions associated with a risk of melanoma. High hydrostatic pressure (HHP) technology is a safe physical method for producing decellularized tissues without chemicals. We have reported that HHP can inactivate cells present in various tissues without damaging the native extracellular matrix (ECM). The objectives of this study were to inactivate human nevus tissue using HHP and to explore the possibility of reconstructing skin using inactivated nevus in combination with cultured epidermis (CE). Human nevus specimens 8 mm in diameter were pressurized by HHP at 100, 200, 500, and 1000 MPa for 10 min. The viability of specimens just after HHP, outgrowth of cells, and viability after cultivation were evaluated to confirm the inactivation by HHP. Histological evaluation using hematoxylin–eosin staining and immunohistochemical staining for type IV collagen was performed to detect damage to the ECM of the nevus. The pressurized nevus was implanted into the subcutis of nude mice for 6 months to evaluate the retention of human cells. Then, human CE was applied on the pressurized nevus and implanted into the subcutis of nude mice. The viability of pressurized nevus was not detected just after HHP and after cultivation, and outgrowth of fibroblasts was not observed in the 200, 500, and 1000 MPa groups. Human cells were not observed after 6 months of implantation in these groups. No apparent damage to the ECM was detected in all groups; however, CE took on nevus in the 200 and 500 MPa groups, but not in the 1000 MPa group. These results indicate that human nevus tissue was inactivated by HHP at more than 200 MPa; however, HHP at 1000 MPa might cause damage that prevents the take of CE. In conclusion, all cells in nevus specimens were inactivated after HHP at more than 200 MPa and this inactivated nevus could be used as autologous dermis for covering full-thickness skin defects after nevus removal. HHP between 200 and 500 MPa will be optimal to reconstruct skin in combination with cultured epidermal autograft without damage to the ECM.
Introduction
C
The incidence of melanoma among GCMN patients has been reported to be from several percent to 10% or more; 70% of these cases arise by the age of 13 years.2–6 Therefore, surgical excision of all nevi in early childhood is usually recommended, although it is usually difficult to excise the nevus tissue completely because of the lack of autologous skin to cover the skin defects. To overcome this problem, we intended to prepare decellularized dermis from nevus tissue itself. 7 Decellularization techniques using chemicals such as surfactants, hypertonic or hypotonic solutions, and using physical methods such as freeze-drying have been reported.8,9
These methods require more than a few days for the process of tissue inactivation and several subsequent days or weeks for the debris of cells to be washed out. Sodium dodecyl sulfate (SDS) is the most effective among these methods and has already been used clinically.10,11 However, its cytotoxicity and the possibility of damaging the extracellular matrix (ECM) have been reported. 8 We prepared decellularized nevus using SDS and then attempted to reconstruct the skin in combination with cultured epidermis (CE); however, CE did not take on it because of residual SDS. 7
In general, decellularization treatment is composed of two steps: cell inactivation and cellular component removal, because of use in an allogeneic or xenogeneic system. To prepare transplantable autologous dermis from nevus tissue, only the cell inactivation process is indispensable because the residual autologous cellular components do not possess any immunogenicity. Therefore, we focused our attention on the inactivation technique using high hydrostatic pressure (HHP) technology.12–15 HHP technology at more than 600 MPa has been reported to inactivate cells and most pathogens present in heart valves, blood vessels, cornea, and bone/bone marrow, without damaging native ECM.16–20 In addition, we have reported that HHP at 200 MPa for 10 min was sufficient to induce the complete killing of mammalian cells and the complete inactivation of porcine skin without damaging the ECM.21,22
The objective of this study is to prepare inactivated nevus using HHP and explore the possibility of reconstructing skin defects after the removal of nevus using inactivated autologous nevus in combination with cultured epidermal autograft (CEA). The inactivated autologous nevus in this study refers to nevus tissue in which all cells, including nevus cells, fibroblasts, and keratinocytes, have been killed and the resulting debris has not yet been removed. We grafted CE on inactivated nevus and explored its take after implantation into nude mice.
Materials and Methods
Our protocol was approved by Kyoto University Graduate School and Faculty of Medicine Ethics Committee and the Ethics Committees of the National Cerebral and Cardiovascular Center Research Institute, Kansai Medical University, and Osaka Institute of Technology. The HHP procedure for human specimens was performed at the National Cerebral and Cardiovascular Center Research Institute and animal experiments were performed at Kyoto University. Our experimental protocol was approved by the Animal Research Committee, Kyoto University Graduate School of Medicine. The number of animals used in this study was kept to a minimum and all possible efforts were made to reduce their suffering in compliance with the protocols established by the Animal Research Committee.
Preparation of nevus tissue
Nevus tissues were obtained from seven patients (mean age: 4.6 years old, range: 7 months to 8 years old) who underwent surgery to remove nevi at Kyoto University Hospital. Subcutaneous adipose tissues were removed with scissors. Full-thickness nevus tissue samples of 8 mm in diameter were prepared using 8-mm biopsy punches (Kai Industries Co., Ltd.). In addition, 15-mm2 nevus specimens were prepared for an implantation experiment in nude mice. The prepared nevus specimens were preserved in Dulbecco's modified Eagle's medium (DMEM; Life Technologies Japan, Ltd.) at 4°C until the pressurization process.
Pressurization of nevus specimens by HHP
The nevus specimens of 8 mm in diameter were divided into five groups (n = 10 in each group): control, 100, 200, 500, and 1000 MPa groups. Specimens in the control group were removed from DMEM and preserved in a plastic bag filled with normal saline solution (NSS; Otsuka Pharmaceutical Co., Ltd.) without pressurization, instead of the pressurization process to which the other groups were exposed, at room temperature. The other specimens were packed in a plastic bag filled with NSS and each bag was immersed in transmission fluid in the chamber of a cold isostatic pressurization machine (Dr. CHEF, Kobe Steel, Ltd.). These specimens were pressurized at 100, 200, 500, or 1000 MPa for 10 min according to our previously reported procedure.16–22
The pressure inside the chamber was increased at a rate of 65.3 MPa/min until it reached the target pressure. The target pressure was maintained for 10 min and then decreased at a rate of 65.3 MPa/min to atmospheric pressure. After pressurization, nevus tissues were immersed in DMEM until the next experiment.
Assessment of the viability of the pressurized nevus tissue
Evaluation of the viability of the pressurized nevus tissue just after pressurization
The viability of the pressurized nevus tissue just after pressurization was evaluated using a WST-8 (4-[3-(2-methoxy-4-nitrophenyl)-2-[4-nitrophenyl]-2H-5-tetrazolio]-1,3-benzene disulfonate sodium salt) assay (Cell Count Reagent SF; Nacalai Tesque, Inc.). This assay is a modification of the MTT (3-[4,5-dimethylthiazol-2-yl]-2,5-diphenyltetrazolium bromide) assay and a colorimetric assay. 23 In this experiment, nevus specimens from four patients were used. After pressurization, two specimens measuring 3 mm in diameter (n = 80, n = 16 in each group) were punched out from the pressurized 8-mm samples (n = 40, n = 8 in each group) using 3-mm biopsy punches (Kai Industries Co., Ltd.). Each 3-mm specimen was placed into a well of a 96-well plate (Thermo Scientific Nunc A/S), and 100 μL of DMEM was added to each well and incubated for 15 min at 37°C. Then, 10 μL of the test reagent was added and incubated for 1 h. Next, the specimens were removed from wells and the absorbance of the medium was read using a microplate reader (model 680; Bio-Rad Laboratories, Inc.) at a test wavelength of 450 nm and a reference wavelength of 650 nm. The absorbance of DMEM was read to show the absorbance without cells as a control.
Outgrowth culture of pressurized nevus specimens
Nevus tissues from four patients were used in this experiment. Specifically, 3-mm samples (n = 80, n = 16 in each group) were punched out from 8-mm pressurized specimens (n = 40, n = 8 in each group). Each sample was placed in a well of a collagen type I-coated 24-well plate (AGC Techno Glass Co., Ltd.). A sterile small glass slide of 1 × 1 cm in size was put on each specimen to prevent it from floating. A total of 1 mL of high-glucose DMEM (Life Technologies Japan, Ltd.) supplemented with 10% fetal bovine serum (FBS; Life Technologies Japan, Ltd.) and with 100 units/mL penicillin, 100 μg/mL streptomycin, and 250 ng/mL amphotericin B (Life Technologies Japan, Ltd.) was added to each well and incubated at 37°C, 95% humidity, and 5% carbon dioxide. The medium was changed every 3 days.
After 2 weeks, specimens were removed from the wells and migrated fibroblasts were observed using an optical microscope (TS1F-APH; NIKON Co., Ltd.) at 200 × magnification. Then, the viability of specimens was evaluated using WST-8 assay. Each specimen was placed in a well of another 96-well plate and 100 μL of DMEM was added to each well and incubated for 15 min. Then, 10 μL of the test reagent was added and incubated for 1 h. Next, specimens were removed and the absorbance was read at a test wavelength of 450 nm and a reference wavelength of 650 nm. The absorbance of DMEM was read to show the absorbance without cells as a control.
Histological and immunohistochemical assessment of the pressurized nevus specimen
Here, 8-mm pressurized specimens were fixed with 10% neutral-buffered formalin solution and embedded in paraffin blocks. Sections of 5-μm thickness from the central area of each sample were stained with hematoxylin and eosin (H&E). Other sections were used for immunohistochemical staining of type IV collagen for the basal lamina of epidermis and capillaries. After deparaffinization and rehydration, the sections were immersed in 0.1% trypsin in phosphate-buffered saline (PBS; Dako Japan Co., Ltd.) for 15 min at room temperature. The sections were then rinsed twice in PBS (Life Technologies Japan, Ltd.) and immersed in 130 mL of 3% hydrogen peroxide (H2O2; Wako Pure Chemical Industries, Ltd.) for 15 min to block the endogenous peroxidase activity. After the sections had been rinsed three times in PBS, a protein blocking agent (PBA; Nacalai Tesque, Inc.) was applied for 10 min to block nonspecific protein binding. Next, the sections were incubated with rabbit polyclonal anti-type IV collagen antibodies (dilution 1:500; Abcam®, Abcam plc.) as primary antibodies overnight at 4°C. After the sections had been rinsed three times in PBS, the peroxidase-labeled secondary antibody, MAX PO (multi; Nichirei Biosciences, Inc.), was applied and incubated for 30 min. The sections were then rinsed three times in PBS, exposed to DAB (3-3′-diaminobenzidine tetrahydrochloride; Dako Japan Co., Ltd.), and counterstained with hematoxylin. Microphotographs were taken using a fluorescent microscope (Biorevo BZ-9000; Keyence, Co.) at 200 × magnification.
Implantation of nevus specimens into the subcutis of nude mice
Seven-week-old male BALB/c nude mice (n = 15; Shimizu Laboratory Supply) were used. The mice were anesthetized by inhalation of 2% isoflurane (Wako Pure Chemical Industries, Ltd.). Then, 15-mm2 nevus specimens (n = 3 in each group) were implanted into the subcutis of the nude mice. The mice were sacrificed by carbon dioxide inhalation 6 months after implantation, specimens were excised, and pictures were taken to compare the gross appearance. The cranial half of each specimen was fixed with 10% neutral-buffered formalin solution and embedded in paraffin blocks. Next, 5-μm sections of each sample were stained with H&E and used for immunohistochemical staining of vimentin for the confirmation of residual human cells including nevus cells and fibroblasts. The conventional (avidin-biotin complex-alkaline phosphatase [ABC-AP]) method was used in the immunohistochemical staining 23 as follows.
After deparaffinization and antigen retrieval as mentioned above, endogenous peroxidase activity was blocked using 0.3% H2O2 in methyl alcohol for 30 min. The slides were washed in PBS six times and mounted using PBS with 1% goat normal serum for 30 min. Subsequently, antivimentin antibody (SP20; Abcam, Abcam plc.) was applied overnight at 4°C. The slides were then incubated with biotinylated goat antirabbit IgG (Vector Laboratories, Inc.) as a secondary antibody diluted to 1:300 in PBS for 40 min, and washed in PBS six times. ABC-AP (Vector Laboratories, Inc.) at a dilution of 1:100 in bovine serum albumin (BSA; MP Biomedicals, LLC) was applied for 50 min. After washing in Tris-buffered saline (TBS, Trizma® Pre-set crystals; Sigma-Aldrich Japan Co. Ltd.) six times, coloring reaction was carried out with fast red (Histofine®; Nichirei Biosciences Co., Ltd.) and nuclei were counterstained with hematoxylin. Microphotographs were taken using a fluorescent microscope at 200× magnification.
Implantation of pressurized nevus tissue with CE into the subcutis in nude mice
Human CE using keratinocytes cultured from human neonatal foreskin using Green's method was prepared by Japan Tissue Engineering Co., Ltd. (J-TEC). The epidermis of nevus in control and 100 MPa groups was intact and that of pressurized nevus in 200, 500, and 1000 MPa groups was removed during the pressurization process, so specimens in the 200, 500, and 1000 MPa groups were used in this experiment. CE of 1 × 1 cm in size was placed on 8-mm pressurized nevus of the 200, 500, and 1000 MPa groups (n = 12; n = 4 in each group) and implanted into the subcutis on both sides in nude mice (n = 6; two grafts per mouse). The mice were sacrificed by carbon dioxide inhalation and specimens were taken 14 days after implantation. Half of the cranium was fixed with 10% formalin and embedded in paraffin blocks. Then, 5-μm paraffin sections were stained with H&E and subjected to immunohistochemical staining of type IV collagen, cytokeratin 14, and anti-involucrin.
Anti-type IV collagen staining was performed as mentioned above. Anticytokeratin 14 staining was carried out by the following procedure. After deparaffinization and rehydration, the sections were immersed in a preheated staining dish containing ethylenediaminetetraacetic acid (EDTA; Nichirei Bioscience, Inc.) and incubated for 20 min at 95°C. After being cooled to room temperature, the sections were rinsed twice in distilled water (DW; Life Technologies Japan, Ltd.) and immersed in 3% H2O2 for 10 min. After being rinsed in DW and TBST (Tris-buffered saline with 0.05% Tween® 20 [polyoxyethylene sorbitan monolaurate; Nacalai Tesque, Inc.] and 0.15 M NaCl [Sigma-Aldrich Japan Co., Ltd.]), PBA (Dako Japan Co., Ltd.) was applied for 5 min to block nonspecific protein binding. Next, the sections were incubated with rabbit polyclonal anti-type cytokeratin 14 antibodies (dilution 1:10,000; Abcam, Abcam plc.) for 1 h at room temperature. After being rinsed in TBST, EnVision + System HRP Labeled Polymer Anti-Rabbit (Dako Japan Co., Ltd.) was applied for 30 min at room temperature. The sections were rinsed in TBST, exposed to DAB, and counterstained with hematoxylin.
For anti-involucrin staining, after deparaffinization and rehydration, antigen retrieval processing was performed using proteinase K in TBS (PK, dilution 1:3; Dako Japan Co., Ltd.) for 5 min at room temperature. The sections were rinsed twice in DW and immersed in 3% H2O2 for 10 min. After being rinsed in DW and TBST, the protein blocking reagent A (Histofine mousestain kit; Nichirei Bioscience, Inc.) was applied for 60 min. After being rinsed in TBST, the sections were applied with mouse monoclonal anti-type involucrin antibodies (dilution 1:100; Abcam, Abcam plc.) for 1 h at room temperature. After being rinsed in TBST, protein blocking reagent B (Histofine mousestain kit; Nichirei Bioscience, Inc.) was applied for 10 min. Furthermore, after the sections had been rinsed in TBST, simple stain mouse MAX PO (M) (Histofine mousestain kit; Nichirei Bioscience, Inc.) was applied for 20 min. The sections were then rinsed with TBST, exposed to DAB, and counterstained with hematoxylin. Microphotographs were taken using a fluorescent microscope at 200× magnification.
Statistical analysis
Statistical significance was assessed using Tukey–Kramer multiple comparisons test. All data are expressed as the mean ± standard error. Values of p < 0.05 were accepted as statistically significant.
Results
Viability of the pressurized nevus tissue
The results of quantitative evaluation of the viability of the pressurized skin are shown in Figure 1. The absorbance level was significantly higher in the control and 100 MPa groups than in the 200 and 500 MPa groups. The level in the 200 and 500 MPa groups was zero and indicated that the viability of specimens had been completely removed. The absorbance level at 1000 MPa was slightly positive; we will discuss the viability associated with this in the Discussion section below.
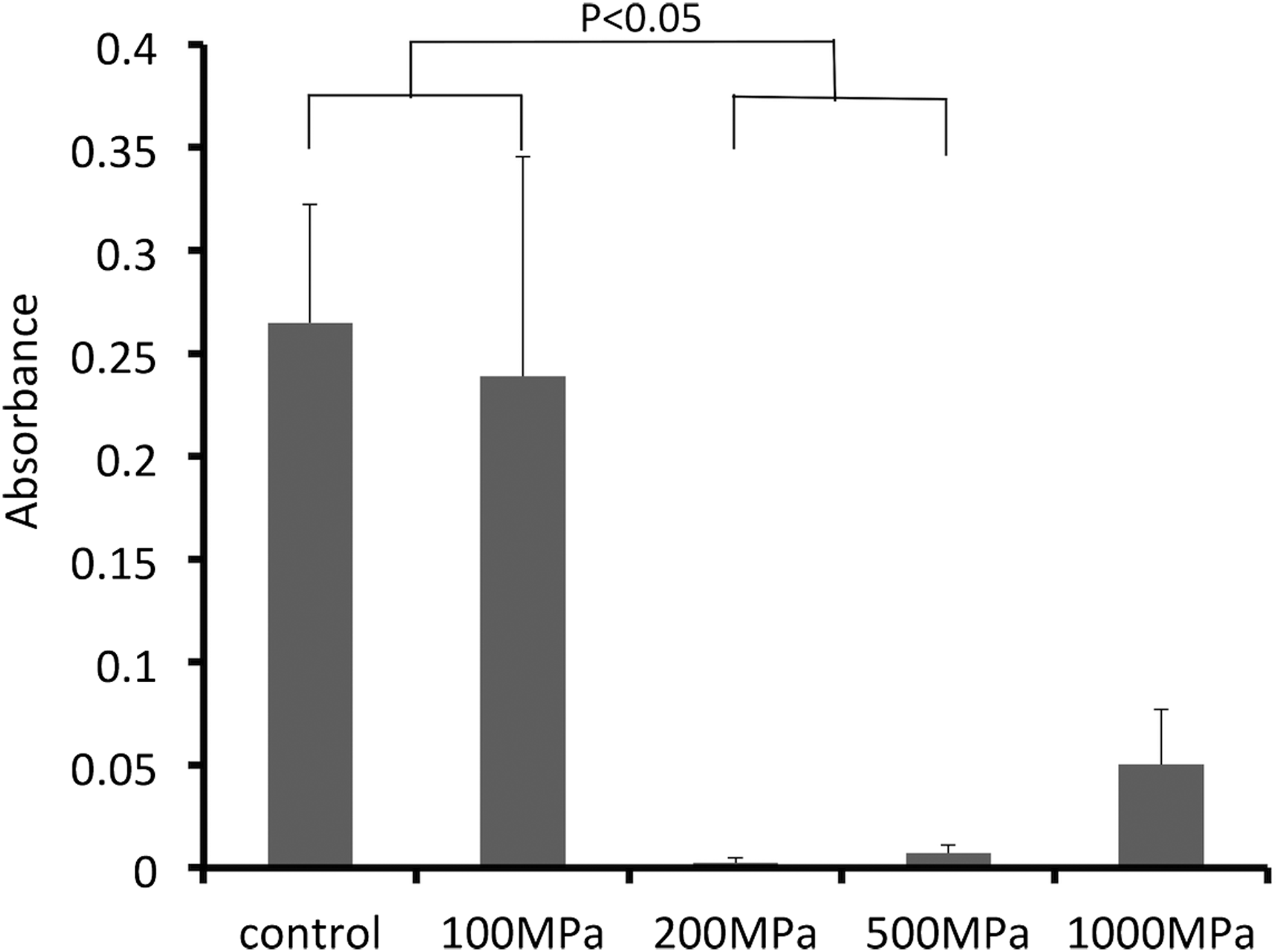
Comparison of the viability of pressurized nevus specimens. The mean absorbance level of Dulbecco's modified Eagle's medium was used as an arbitrary zero point. The absorbance level was significantly higher in the control and 100 MPa groups than in the 200 and 500 MPa groups (p < 0.05).
Outgrowth fibroblasts and viability of the pressurized nevus after cultivation
Figure 2 shows outgrowth fibroblasts after 14 days of cultivation. Fibroblasts were observed in the control and 100 MPa groups, whereas no fibroblasts were observed in the other groups. A quantitative comparison of the viability of pressurized nevus tissue after cultivation is shown in Figure 3. The levels in the control and 100 MPa groups were significantly higher than those in the other three groups with no viability (p < 0.01).
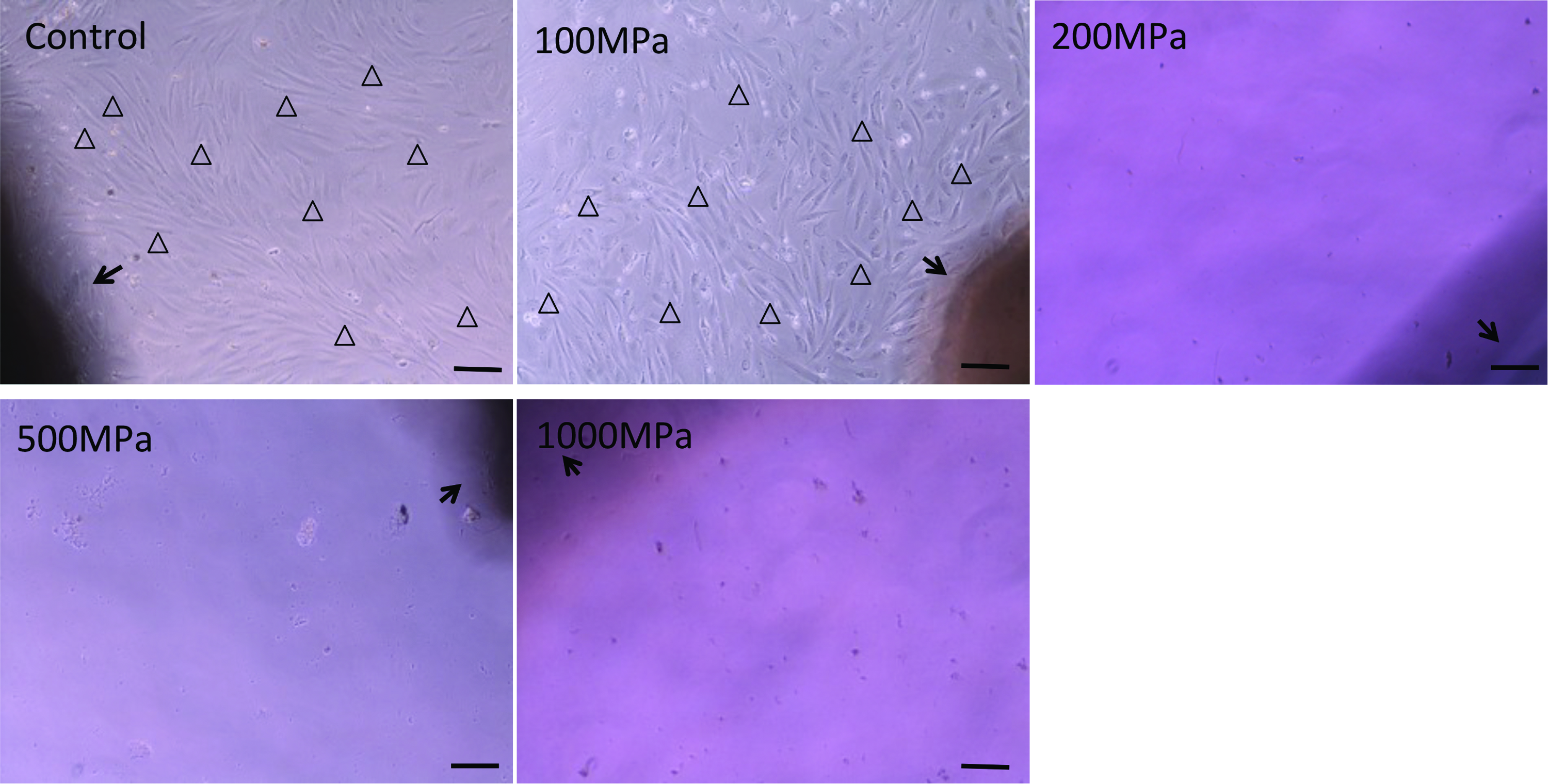
Micrographs of cultured fibroblasts on day 14. Fibroblasts were observed in the control and 100 MPa groups, whereas no fibroblasts were observed in the 200, 500, and 1000 MPa groups. Black arrows indicate pressurized nevus. Open arrowheads indicate fibroblasts. Scale bar: 50 μm. Color images available online at
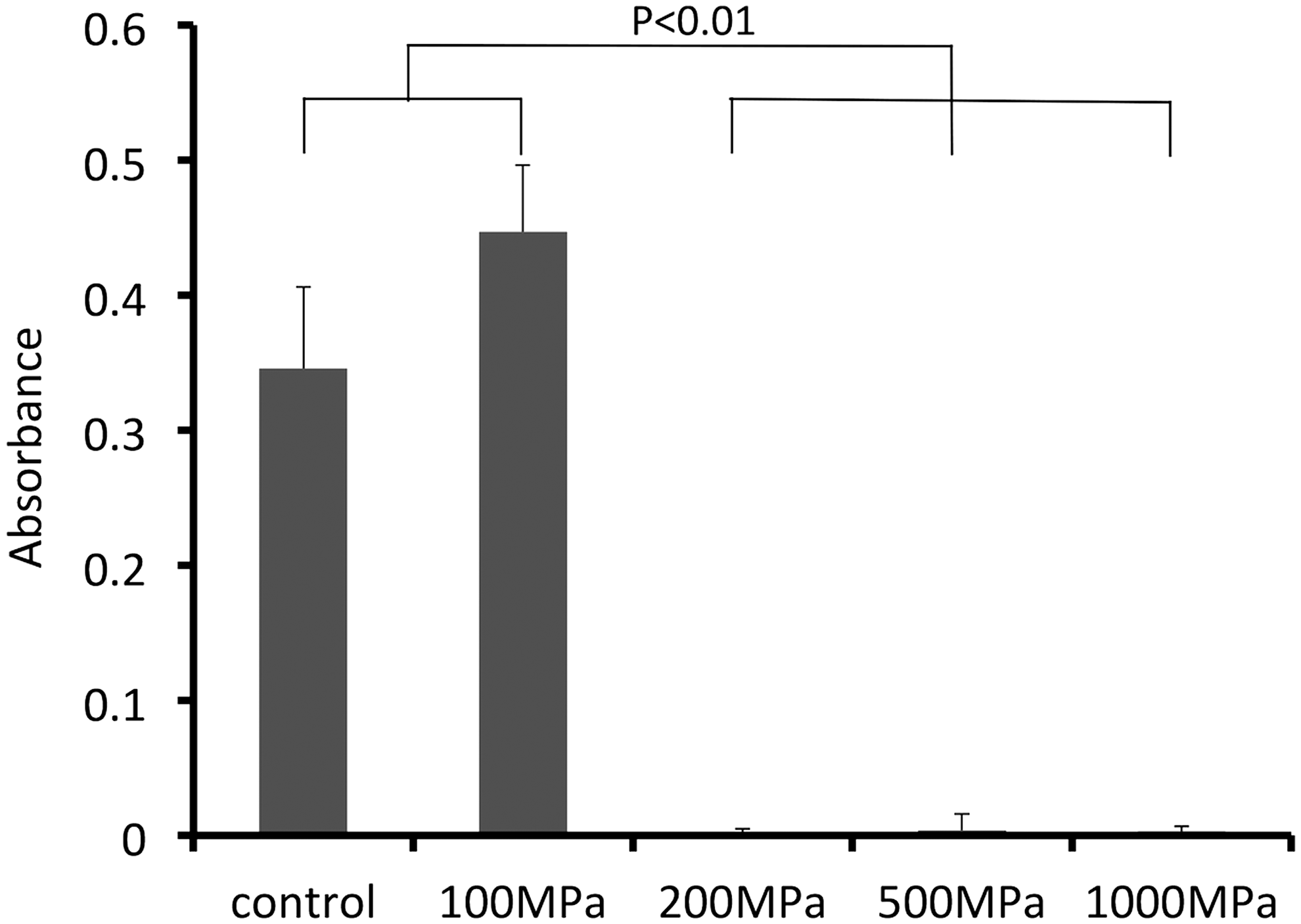
Comparison of the viability of nevus specimens after cultivation. The absorbance levels in the control and 100 MPa groups were significantly higher than those in the 200, 500, and 1000 MPa groups (p < 0.01).
Histological evaluation of the pressurized nevus
Figure 4 shows H&E sections of pressurized nevus specimens. The epidermis remained intact in the control and 100 MPa groups, whereas it was separated and removed in the other three groups. Immunohistochemical staining of type IV collagen showed that the basal lamina of the epidermis and capillaries in the dermis remained intact in all specimens regardless of the existence of epidermis, as shown in Figure 5. Immunohistochemical staining of collagen type I of the pressurized nevus specimens showed the arrangement of collagen fiber of the dermis was regular and denaturation of collagen was not observed in all specimens (S2A).

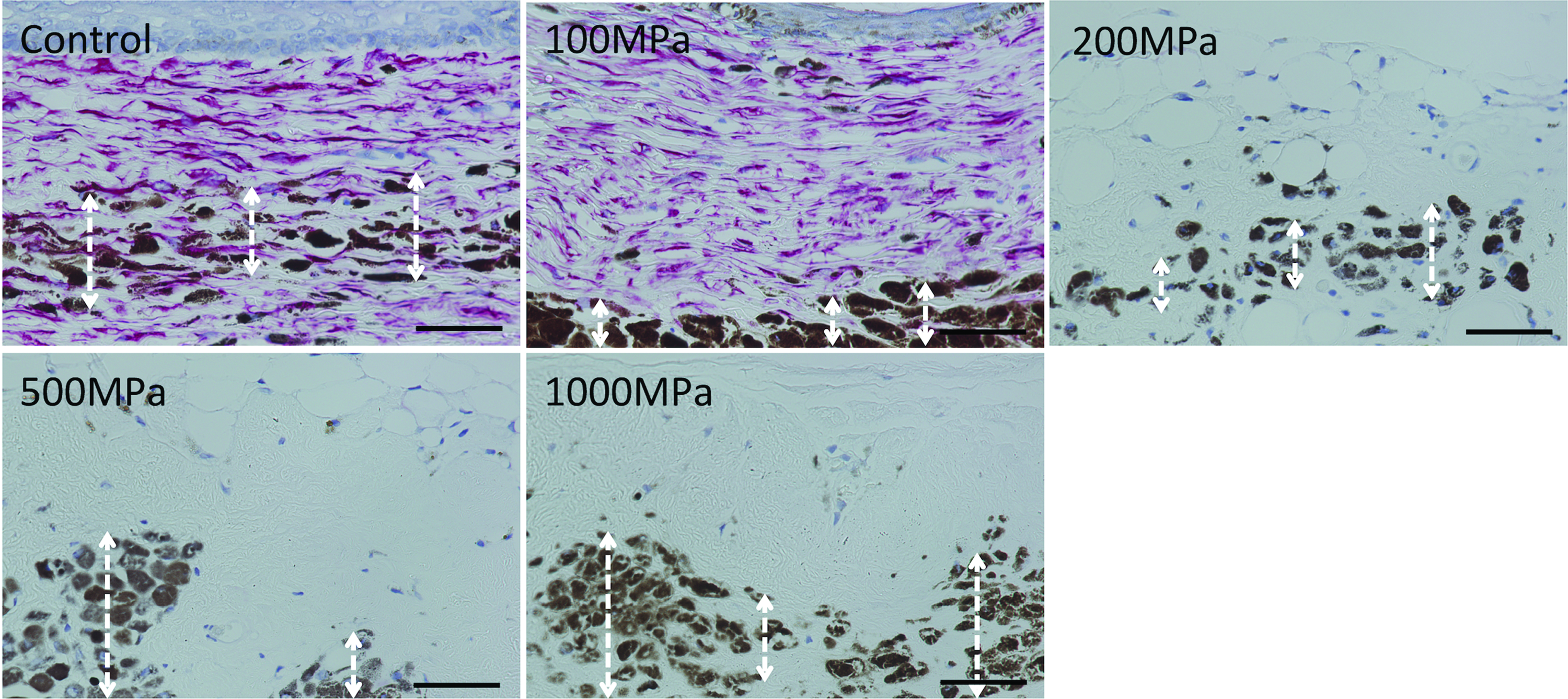
Micrographs of hematoxylin and eosin (H&E)-stained sections of pressurized nevus specimens. The epidermis remained intact in the control and 100 MPa groups. In contrast, the epidermis was separated from the dermis in the 200, 500, and 1000 MPa groups. The nuclei of cells in the nevus were observed in all specimens. Two-headed arrows indicate the epidermis. Scale bar: 100 μm. Color images available online at

Micrographs of immunohistochemical staining of type IV collagen. Closed arrowheads indicate the basal lamina of epidermis and open arrowheads indicate that of capillaries. Scale bar: 100 μm. Color images available online at
Pressurized nevus specimen after implantation for 6 months
The gross appearances of pressurized specimens after implantation are shown in Figure 6. Specimens in the control and 100 MPa groups were round in shape; in contrast, those in the 200, 500, and 1000 MPa groups were square, like the nevus before implantation. On H&E sections, epidermis of the control and 100 MPa groups remained intact, whereas epidermis of the 200, 500, and 1000 MPa groups was not observed, as shown in Figure 7. Melanin pigment of nevus was observed in all groups. Immunohistochemical staining of collagen type I showed the arrangement of collagen fiber of the dermis was regular in all specimens (S2B). Immunohistochemical staining for human vimentin showed remaining human cells in the dermal part in the control and 100 MPa groups, whereas no human cells were confirmed in the other three groups, as shown in Figure 8. We confirmed that murine cells were not stained by this antibody.
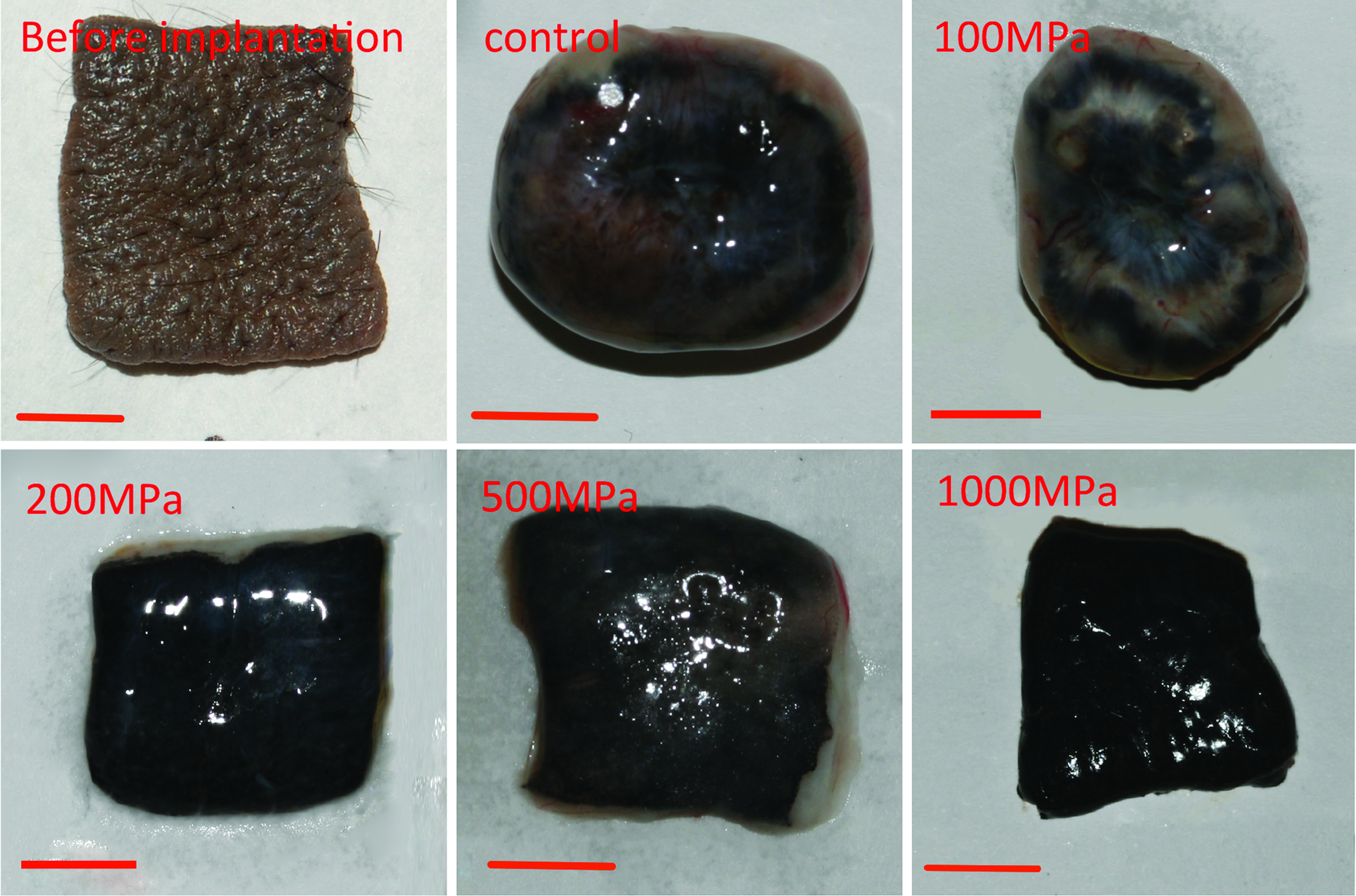
Gross appearance of the pressurized nevus specimens after 6 months of implantation. Scale bar: 5 mm. Color images available online at

Micrographs of H&E sections of the pressurized nevus specimens 6 months after implantation. The epidermis of the control and 100 MPa groups was intact, whereas the epidermis of the 200, 500, and 1000 MPa groups was not observed. White two-headed arrows indicate melanin pigment. Black two-headed arrows indicate the epidermis. Scale bar: 100 μm. Color images available online at
Micrographs of immunohistochemical staining of antivimentin sections of specimens 6 months after implantation. Antivimentin sections of control and 100 MPa groups indicated abundant remaining human cells stained with fast red, whereas no human cells were confirmed in the 200, 500, and 1000 MPa groups. Melanin pigment, which was indicated by two-head arrows, remained in all groups. Scale bar: 50 μm. Color images available online at
Implanted pressurized nevus specimens with CE
On day 14, CE was observed on pressurized nevus in the 200 and 500 MPa groups; in contrast, it was not observed in the 1000 MPa group, as shown in Figure 9. No apparent inflammatory response was observed. Immunohistochemical staining of type IV collagen showed that the basal lamina remained intact in all groups, as indicated in Figure 10. On the other hand, laminin 5 was detected in the 200 and 500 MPa groups and type VII collagen was stained only in the 200 MPa group (S1).

H&E sections of implanted pressurized specimens with cultured epidermis (CE) on day 14. CE took on pressurized nevus specimens in the 200 and 500 MPa groups. However, CE was not observed in the 1000 MPa group. Two-headed arrows indicate CE on pressurized specimens. Scale bar: 100 μm. Color images available online at
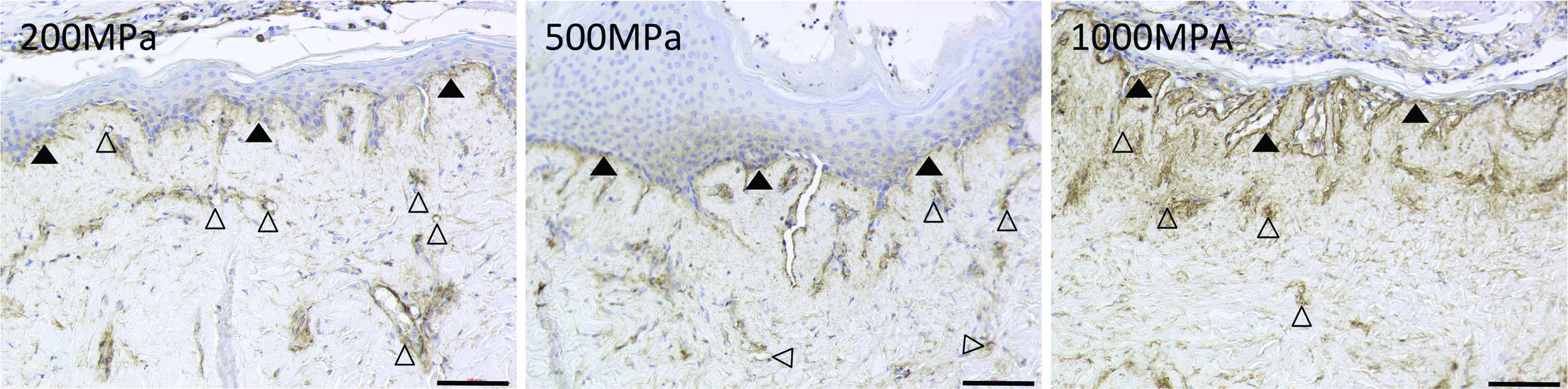
Micrographs of immunohistochemical staining of type IV collagen of implanted pressurized specimens with CE on day 14. The basal lamina in the 200, 500, and 1000 MPa groups remained intact. Closed arrowheads indicate the basal lamina of epidermis and open arrowheads indicate that of capillaries. Scale bar: 100 μm. Color images available online at
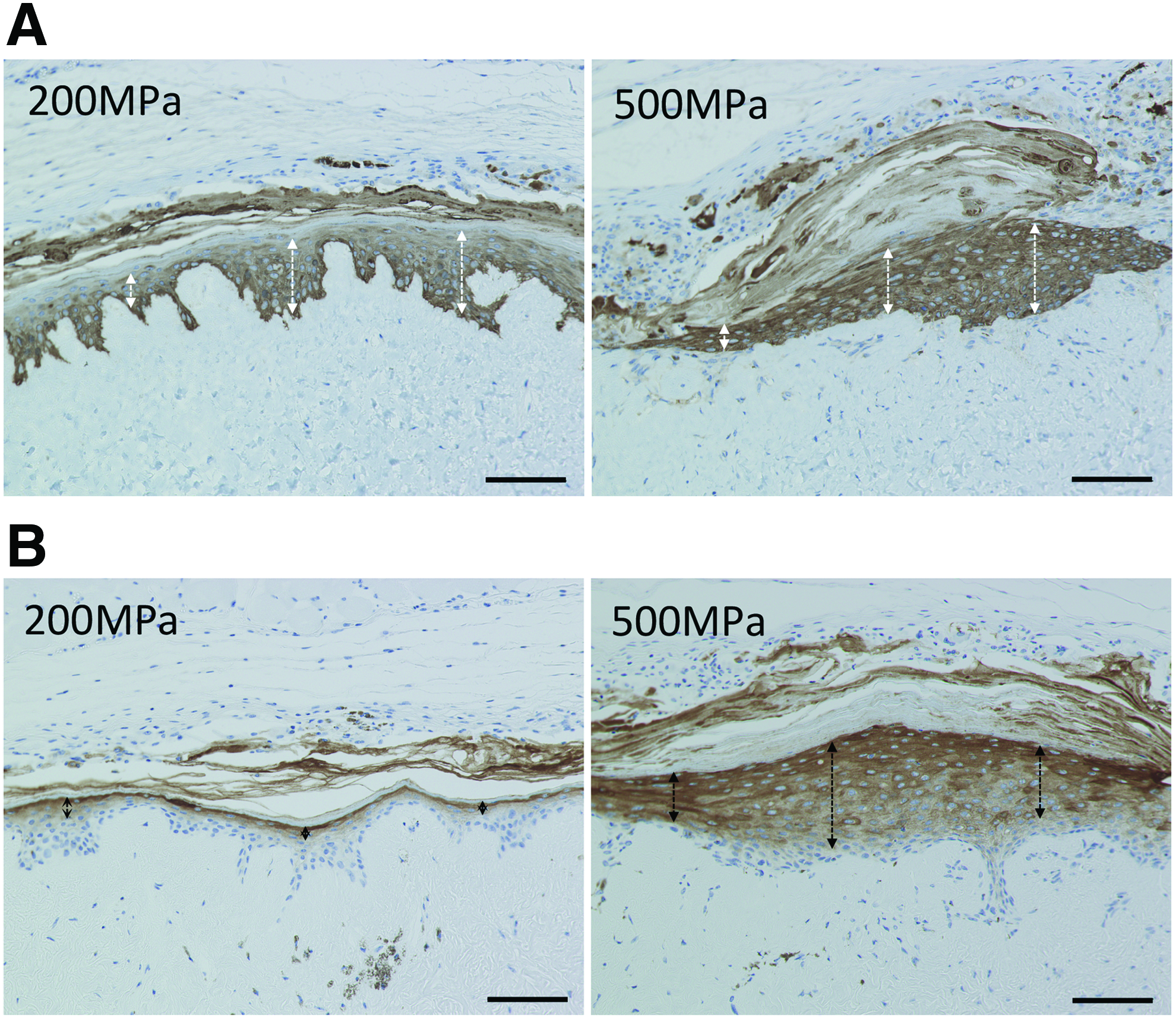
In the 200 and 500 MPa groups, the basal cell layer of CE was stained with cytokeratin 14 (Fig. 11A) and its granular cell layer was stained with involucrin (Fig. 11B). This indicates that the implanted CE took successfully and maintained its differentiation and keratinization on the pressurized nevus.
Discussion
Surgical excision of GCMN in early childhood is recommended to avoid the risk of malignant melanoma, although it is difficult to excise the nevus completely because autologous skin available after its removal is limited. Skin consists of epidermis and dermis. The regeneration of epidermis using CE by Green's method was established more than 30 years ago.24,25 In contrast, the regeneration of dermis with sufficient strength and elasticity compatible to those of native dermis remains to be achieved and this is a crucial issue in the treatment of large skin defects because the regeneration of dermis is indispensable for the successful take of CE. 26 Allogeneic skin grafts or xenografts have been used widely in the treatment of burn patients, although these are used as biological dressings and long-term survival is not expected because of rejection.27–29 Dermal substitutes such as AlloDerm (LifeCell Corp.), Integra (Integra Life Science Corp.), and Pelnac (Gunze Ltd.) in combination with a split thickness skin graft have been used for the treatment of GCMN.30–33 However, it is still difficult to apply CE on dermal substitutes and the long-term efficacy of these substitutes in terms of their quality is still controversial.34,35
As mentioned above, autologous skin graft or autologous dermis graft is the only material for permanent skin or dermal reconstruction. Therefore, we established novel treatment to inactivate a patient's nevus and reconstruct skin defects after its removal using inactivated nevus in combination with autologous cultured dermis. It is theoretically possible to reconstruct any amount of GCMN up to 100% of the total surface area. The key point of this treatment is the complete inactivation of nevus without damaging its native dermal structure with sufficient strength and elasticity that support the engraftment of CE.
As for the inactivation or killing of cells by HHP, pressurization at 200 MPa for 10 min induced complete killing of cultured mammalian cells. 21 Cells are inactivated through apoptosis at around 200 MPa, but cell death occurs through necrosis at pressures higher than 300 MPa. 12 Pressures above 300 MPa cause irreversible protein denaturation at room temperature and pressures above 600 MPa inactivate most bacteria, viruses, yeasts, and mold cells. 15 In this study, the WST activity of nevus tissue just after pressurization for 10 min was abolished at pressures higher than 200 MPa. This WST-8 assay detects the activity of mitochondria located on the surface of specimens, but cannot evaluate the activity of cells in deeper parts. To check the viability in deeper parts, nevus specimens of 3 mm in diameter were punched out from pressurized nevus of 8 mm in diameter and outgrowth of cells was confirmed. The WST-8 assay was performed after cultivation to check whether cells had been reactivated after cultivation because some effects of relatively low pressurization below 100 MPa were reversible. 12
We also evaluated the survival of human cells 6 months after implantation in vivo to check such reactivation. The gross appearance of the pressurized nevus after implantation in the control and 100 MPa groups was round in shape and obviously different from the square shape in the 200, 500, and 1000 MPa groups. This may have been the effect of the remaining epidermis or, possibly, contracture caused by remaining human fibroblasts. Fast red was used as a chromogenic substrate in the staining of antivimentin because a brown color of DAB was difficult to distinguish from the melanin remaining in the nevus specimens. Our results show that all cells in nevus were inactivated at pressures higher than 200 MPa and they were not reactivated after cultivation in vitro and implantation in vivo. The absorbance level at 1000 MPa just after HHP was slightly positive in Figure 1; however, all other results showed inactivation at above 200 MPa, including at 1000 MPa. The inactivation of various tissues at 1000 MPa has been confirmed in previous studies,16–19 so we suspect that this activity might be the result of the modulated enzyme activities in nevus at 1000 MPa. 12
As for damage to the ECM by HHP, H&E staining and immunostaining for type IV collagen could not detect any apparent damage. We could also not detect any damage to the dermis using scanning electron microscopy in our previous study using normal porcine skin and no damage to the matrix of other tissues has been reported.16–19,22 We confirmed the vascularization of implanted nevus in the 200, 500, and 1000 MPa groups by anti-type IV collagen staining, and the take of CE maintaining differentiation and keratinization in the 200 and 500 MPa groups. The take rate of CE on reconstructed dermis is satisfactory in clinical practice; however, the take rate of CE on full-thickness skin wound or granulation tissue is low. 25 This indicates that some damage or denaturation of ECM occurs when CE does not take and suggests that HHP at 1000 MPa caused damage to the dermis and is not suitable for skin reconstruction. We must characterize this damage in further study.
Another concern of this treatment is remaining cellular debris, which is likely to yield an inflammatory response and cause graft loss. Cellular debris is usually removed in the preparation of decellularized tissue; however, our treatment uses autologous tissue and inflammation by cellular debris would be slight or moderate compared with that for allografts or xenografts. In this study, CE took on nevus pressurized at 200 and 500 MPa, which contained cellular debris, without an inflammatory response. We think that it is difficult to evaluate the inflammatory response using the nude mouse model because the murine immune response is deficient. To evaluate the effects of cellular debris, we are preparing autologous transplantation experiments using porcine skin and will report the results as our next step.
The main advantages of HHP are the short processing time and complete cell killing regardless of the thickness or hardness of tissue. In the clinical application of this treatment, we will excise and inactivate nevus by HHP at between 200 and 500 MPa for 10 min during the first operation. Although HHP at between 200 and 500 MPa is insufficient for the disinfection of all pathogens, this treatment is autologous and disinfection has no clinical importance. Then, inactivated nevus is grafted to the original site and a small normal skin sample for CEA (JACE®; Japan Tissue Engineering Co., Ltd.) is taken. JACE is a CEA product approved in Japan in 2007 and it was prepared using Green's method as well as other CEA products. 36 CEA is prepared after 3 weeks. Fibroblasts and capillaries infiltrate into the nevus within a few weeks and CEA is grafted on this reconstructed autologous dermis derived from nevus tissue in the second operation. As we show in Figure 7, melanin pigment remains; however, melanin pigment can easily be treated by conventional laser therapy.37,38
Conclusion
Human nevus can be inactivated by HHP at between 200 and 500 MPa without detectable damage to the dermal structure. CE took on nevus inactivated by HHP at between 200 and 500 MPa, whereas it did not take on that at 1000 MPa. This combination therapy with inactivated nevus and CE could be a breakthrough treatment of GCMN.
Footnotes
Acknowledgment
This work was supported partially by the Center of Innovation Program from the Japan Science and Technology Agency (JST), by Health and Labor Sciences Research Grants, and by a Grant of Translational Research Network Program from the Ministry of Education, Culture, Sports, Science and Technology, Japan.
Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.