
Abstract
Platelet-rich plasma (PRP) has been used for different applications in human and veterinary medicine. Many studies have shown promising therapeutic effects of PRP; however, there are still many controversies regarding its composition, properties, and clinical efficacy. The aim of this study was to evaluate the influence of different platelet concentrations on the rheological properties and growth factor (GF) release profile of PRP-gels. In addition, the viability of incorporated bone marrow-derived human mesenchymal stem cells (MSCs) was investigated. PRP (containing 1000 × 103, 2000 × 103, and 10,000 × 103 platelets/μL) was prepared from human platelet concentrates. Platelet activation and gelification were achieved by addition of human thrombin. Viscoelastic properties of PRP-gels were evaluated by rheological studies. The release of GFs and inflammatory proteins was measured using a membrane-based protein array and enzyme-linked immunosorbent assay. MSC viability and proliferation in PRP-gels were assessed over 7 days by cell viability staining. Cell proliferation was examined using DNA quantification. Regardless of the platelet content, all tested PRP-gels showed effective cross-linking. A positive correlation between protein release and the platelet concentration was observed at all time points. Among the detected proteins, the chemokine CCL5 was the most abundant. The greatest release appeared within the first 4 h after gelification. MSCs could be successfully cultured in PRP-gels over 7 days, with the highest cell viability and DNA content found in PRP-gels with 1000 × 103 platelets/μL. The results of this study suggest that PRP-gels represent a suitable carrier for both cell and GF delivery for tissue engineering. Notably, a platelet concentration of 1000 × 103 platelets/μL appeared to provide the most favorable environment for MSCs. Thus, the platelet concentration is an important consideration for the clinical application of PRP-gels.
Introduction
P
PRP can be produced using whole-blood centrifugation or apheresis. Several commercial centrifugation systems are available and offer a simple, minimal manipulative preparation of autologous PRP; however, the platelet counts and enrichment levels are variable (ranging from physiological platelet concentrations to 18-fold enrichment), and only few systems allow adjustments by the user (according to the manufacturer's brochures and Mazzucco et al. 20 ). Platelet concentrates from whole-blood centrifugation contain erythrocytes and leukocytes. In contrast, apheresis allows the exclusion of components, which are undesired, since the accumulation of leukocytes might be deleterious for the healing process.21,22
The form in which PRP is used depends on the application and target tissue. Many clinicians use PRP in an inactivated liquid form that can be easily injected. After application, platelets are activated by contact with the surrounding tissue collagen. 23 Alternatively, an exogenous activator, such as chitosan, batroxobin, thrombin, calcium chloride, or a combination of the latter two, can be used to form a PRP-gel.24–28 PRP-gels have been used as an autologous hydrogel containing bioactive molecules, locally enhancing tissue healing.29–34 The composition of PRP-gels in these studies was, however, highly variable, mainly because of differences in PRP preparation and activation methods, which in turn leads to significant differences in platelet concentration, leukocyte content, and GF release. 20 Previous studies have reported a successful culture of cells incorporated into PRP-gels, suggesting that the gel environment enhances viability and proliferation of encapsulated cells.33,35 Kawasumi et al. encapsulated rat bone marrow (BM) mesenchymal stem cells (MSCs) in PRP-gels containing different platelet concentrations, ranging from 0.05 to 4.4 × 106 platelets/μL. The authors demonstrated a platelet concentration-dependent stimulation of cell proliferation in vitro as well as enhanced bone formation in a rat osteotomy in vivo. 35
Although previously applied for various applications in vivo, in our opinion, PRP-gels have not been sufficiently characterized. PRP may be homemade or obtained using clinical systems, and all these protocols/systems result in different platelet and leukocyte concentrations, with additional variability introduced by donor variations. 36 In this study, we investigated three different platelet concentrations in PRP-gels (1000 × 103, 2000 × 103, and 10,000 × 103 platelets/μL), referring to as 5×, 10×, and 50× platelet enrichment, assuming an average concentration of 200 × 103 platelets/μL in healthy human donors. Most studies using PRP-gels, particularly in the context of bone repair, have used similar concentrations (e.g., 48–4358 × 103 platelets/μL 35 and 1040 × 103 platelets/μL 34 ), while other studies do not indicate the platelet concentration in their PRP preparations. The aims of this study were to systematically characterize different compositions of PRP-gels created from platelet concentrates, to compare these gels with respect to their rheological properties, the content, and release profile of GFs, and finally to assess the viability of incorporated MSCs.
Materials and Methods
Preparation of PRP and PRP-gels
PRP was produced from human leukocyte-depleted platelet concentrates (blood bank; Kantonsspital Graubünden, Chur, Switzerland) obtained by apheresis and collected into transfusion bags containing acid citrate dextrose (ACD-A), with a thrombocyte concentration of 2.4 × 1011 per 240 mL of plasma (1000 × 103 thrombocytes/μL) and containing less than 5 × 105 leukocytes. Based on the assumption that the average platelet count in healthy human adults is 200 × 103/μL, this platelet concentrate was considered to be five times enriched. To produce PRP with higher platelet concentrations, the platelet concentrates were centrifuged at 2000 g for 20 min, and the resulting pellet was resuspended in the appropriate volume of platelet-depleted plasma. PRP was sonicated for 15 min and stored at −20°C until use. If not stated otherwise, PRP-gels were produced by pipetting 3 μL of human thrombin (final concentration 5 U/mL, TISSEEL; Baxter) into a well of a 48-well cell culture plate (Falcon). The plate was placed on an orbital shaker, and 312 μL of PRP was slowly added. Gels were incubated at room temperature for 15 min for gelification.
Rheology
The viscoelastic properties of PRP-gels were investigated through oscillatory rheology. Discs of PRP-gels of 25 mm diameter and 0.2 mm thickness were prepared with a dedicated mold. Thrombin concentrations were 5, 8, and 16 U/mL. All rheological measurements were performed using an Anton Paar MCR-302 rheometer equipped with a 25 mm parallel plate, a Peltier temperature control system, and an insulating thermostatic hood. First, the samples were screened with an amplitude sweep at 10 rad/s at 20°C. This measurement allows the individuation of a suitable deformation range, which should be within the linear viscoelastic region. A strain of 1% was verified to be within this limit for all tested gels and further used for each sample. A frequency sweep (measure of viscoelastic shear moduli as a function of the frequency of deformation) between 0.1 and 25 rad/s at 20°C was finally performed. For each specimen, three independent freshly prepared samples were measured, and the results are reported as mean ± standard error of the mean (SEM).
GF release from PRP-gels
GF release was measured from PRP-gels incubated with 800 μL of phosphate-buffered saline (PBS) at 37°C at different time points after gelification (30 min–168 h). At every time point, 400 μL of conditioned PBS was collected for analysis, and removed volume was replaced with a new 400 μL of PBS. Enzyme-linked immunosorbent assays (ELISAs) were performed to quantify CCL5/RANTES (DuoSet®; R&D Systems), TGFβ-1, VEGF, PDGF-AB, and PDGF-BB (all Quantikine®; R&D Systems) according to the manufacturer's instructions. Samples were diluted according to the platelet concentration of the gels. Absorbance was measured at 450 and 560 nm to eliminate background signal using a VICTOR3™ plate reader (PerkinElmer).
The presence of inflammatory proteins in conditioned PBS from different PRP-gels (pooled samples from two PRP donors, collected 12 h after gelification) was investigated using a human inflammation protein array (RayBio®, C-Series AAH-INF-3-4) according to the manufacturer's instructions. Briefly, the membranes were incubated with 1 mL of PRP supernatant overnight at 4°C on an orbital shaker. Chemiluminescence (20-min exposure time) was detected using the ChemiGenius Bio-Imaging System (Syngene). Semiquantification was performed by averaging values from duplicated spots and measuring signal intensity using ImageJ (Rasband, NIH). Data are presented as relative abundance following normalization to the RayBio intrinsic positive control.
MSC isolation, culture, and encapsulation in PRP-gels
BM aspirates were obtained from the iliac crest or vertebral body of patients undergoing elective orthopedic surgery (mean age: 56.5 years, range: 26–89 years; one male and eight females). Informed consent was given by all patients, and approval from local ethical authorities was obtained (KEK Bern 126/03). Mononucleated cells (MNCs) were isolated from BM aspirates by density centrifugation with Ficoll™ (Histopaque-1077; Sigma). MNCs were seeded in tissue culture flasks at a density of 5 × 104 cells/cm2 in an alpha-minimum essential medium (αMEM; Gibco) containing 10% fetal bovine serum (FBS; PAN) and 5 ng/mL bFGF (R&D Systems). After 4 days in culture, nonadherent hematopoietic cells were removed. MSCs selected by adherence to cell culture plates were further expanded with a change of medium every 3 days. Cells were passaged when 80% confluency was reached. All experiments were performed with cells at the second passage. MSCs used as monolayer controls were seeded at a density of 3 × 103 cells/cm2 in six-well tissue culture plates.
For the incorporation of MSCs into PRP-gels, PRP aliquots were thawed, and to avoid donor variability, three PRP donors with the same blood group were pooled. MSCs were seeded in PRP-gels at a density of 1.25 × 105 cells per gel in a total volume of 315 μL. Gelification was performed using a final concentration of 5 U/mL thrombin as described above. Gels were incubated at 37°C in αMEM containing 10% FBS, 5 ng/mL bFGF, 100 U/mL PenStrep, and 5 μM ɛ-aminocaproic acid (Sigma).
Viability of MSCs
The viability of MSCs encapsulated in PRP-gels was determined at days 0 (3 h after seeding), 3, and 7. PRP-gels were stained with a solution of 100 pg/mL calcein AM and 1 pg/mL ethidium homodimer-1 (both Sigma) in 1 mL of αMEM for 30 min at 37°C and visualized with an inverted phase contrast microscope (Olympus CK40) equipped with a fluorescence lamp.
For semiquantitative analysis of cell viability following recovery from PRP-gels, 1 h and 3 and 7 days after cell encapsulation, PRP-gels underwent enzymatic digestion in type II collagenase (600 U/mL; Worthington). The number of retrieved viable cells was determined by trypan blue (Sigma) exclusion. Cell viability was further determined by propidium iodide (PI; 4 μg/mL; Sigma) staining and flow cytometry (BD FACSAria III). To define the forward scatter and side scatter region for the analysis, a PRP-gel without cells was used to exclude platelet debris.
DNA content
At days 0 (5 h after seeding), 3, and 7, PRP-gels were subjected to digestion in proteinase K (0.5 mg/mL; Roche) for 16 h at 56°C. The DNA content was measured using an ultrasensitive fluorescent nucleic acid stain PicoGreen® (Invitrogen), which allows quantitating double-stranded DNA at concentrations as low as 25 pg/mL. A calf thymus DNA standard (Invitrogen) was used to create a five-point standard curve from 2 ng/mL to 2 μg/mL. Measurements were performed using a VICTOR3 (PerkinElmer) plate reader at 485 nm excitation and 535 nm emission wavelengths.
Statistical analysis
All values are shown as mean ± SEM. Statistical analysis was performed with the Kruskal–Wallis test using the GraphPad Prism. p-Value <0.05 was considered as statistically significant.
Results
Formation of PRP-gels
All gel formulations could be cultured for 7 days without evident visual changes in shape or size (Fig. 1). Rheological measurement revealed that for all tested gels, the G′ was over G", demonstrating an effective cross-linking of samples. Neither the platelet concentration (Fig. 2A) nor the thrombin concentration (Fig. 2B) significantly affected the viscoelastic properties of the gels. However, we found that PRP-gels with 2000 × 103 platelets/μL were slightly stiffer than those with 10,000 × 103 or 1000 × 103 platelets/μL (Fig. 2A), with the lowest values observed for the lowest platelet concentration. When testing the influence of different thrombin concentrations on PRP-gels with the same platelet content, we found that the lowest final thrombin concentration (5 U/mL) showed the highest values of storage and loss moduli and was therefore chosen for further experiments (Fig. 2B).
Platelet-rich plasma (PRP) with 2000 × 103 platelets/μL forms an elastic cross-linked gel releasing growth factors. Macroscopic view of PRP-gels prepared from 315 μL of PRP and activated with 5 U/mL thrombin. Scale bar depicts 30 mm. Color images available online at

Rheological analysis of PRP-gels. Storage (G′) and loss (G") moduli as function of the angular frequency showing effective cross-linking of gels.
GF release from PRP-gels
First, the release of GFs that are known to be important signaling molecules in tissue repair was examined. 1 TGFβ-1, PDGF-AB, PDGF-BB, and VEGF could be detected in conditioned PBS by PRP from all tested PRP-gels from all platelet concentrations (Fig. 3). Additionally, the cumulative and temporal release of GFs from PRP-gels was investigated (Fig. 3). A positive correlation between protein secretion and platelet concentration was observed at all time points and platelet concentrations. Overall, most of the release of GFs appeared within the first 4 h after gelification. A comparatively lower sustained release of GFs was observed at later time points (Fig. 3). Twelve hours after gelification, the cumulative release of activated TGFβ-1 (Fig. 3A, right) showed the highest values in PRP-gels with 10,000 × 103 platelets/μL reaching 13.08 ± 3.48 ng, followed by 2000 × 103 platelets/μL PRP-gels with 4.07 ± 0.61 ng and 1000 × 103 platelets/μL PRP with 2.62 ± 0.26 ng. Compared to TGFβ-1, the values of cumulative release of PDGF-AB (Fig. 3B) were lower for the highest (9.34 ± 1.9 ng) and middle (3.54 ± 0.84 ng) platelet concentrations but higher (3.81 ± 0.29 ng) for PRP-gels with 10,000 × 103 platelets/μL. Release of PDGF-BB at 12 h was clearly lower for all PRP-gels reaching 0.23 ± 0.03, 0.34 ± 0.04, and 1.05 ± 0.25 ng in 1000 × 103, 2000 × 103, and 10,000 × 103 platelets/μL gels, respectively. VEGF release was the lowest compared to the other GFs.
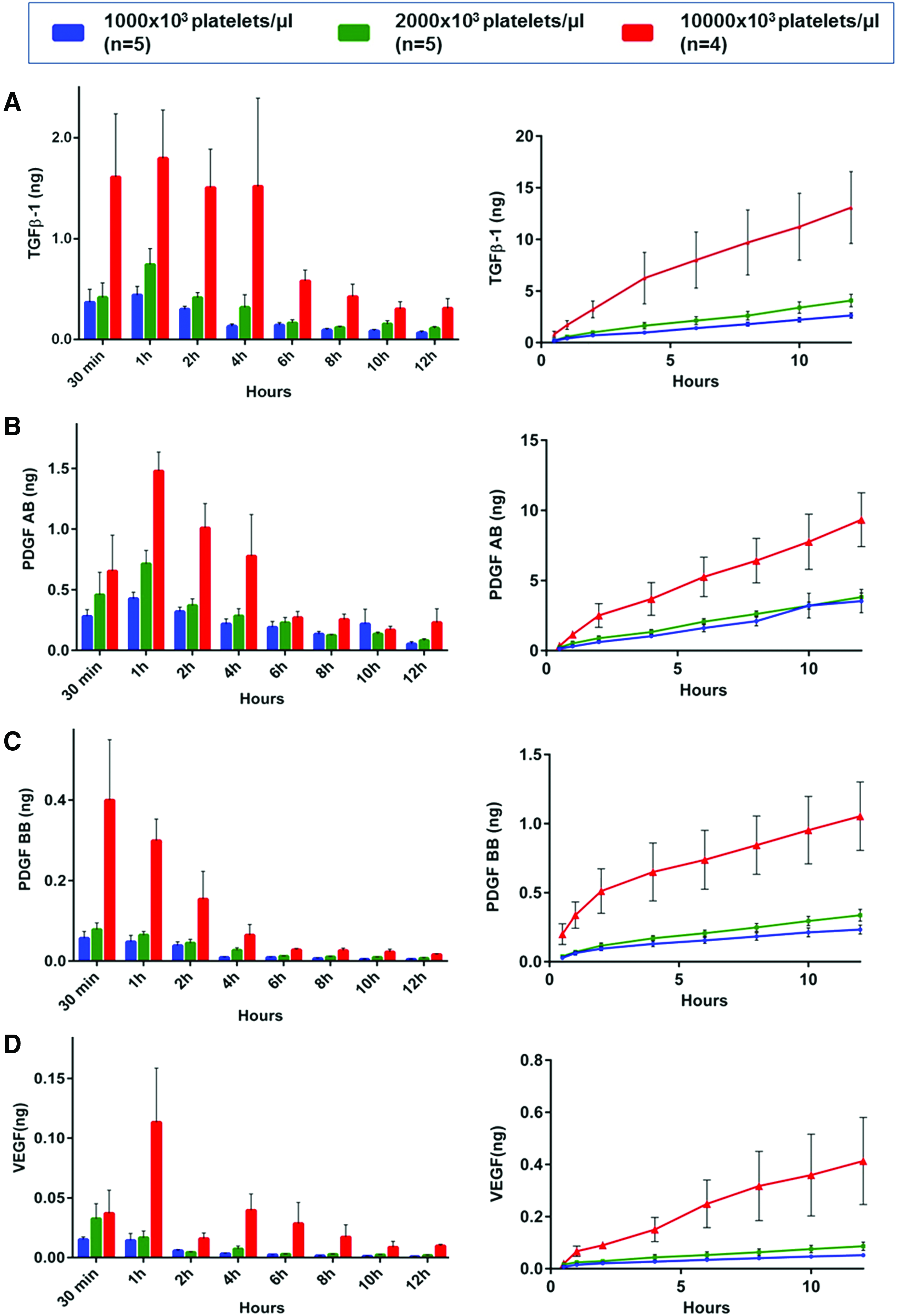
Growth factor release from different PRP-gels. Temporal (left) and cumulative (right) release of transforming growth factor-β-1
PRP-gels release inflammatory proteins
Because of existing controversies regarding possible proinflammatory effects of PRP, a screening array was performed to identify the most abundant inflammatory proteins released from PRP-gels. A total of 28 proteins known to play a role in inflammation were detected (Fig. 4). The chemokine CCL5 was released in the highest amounts compared to other factors, followed by PDGF-BB, interferon-gamma-induced protein 10 (IP10), interleukin-6 soluble receptor (IL-6sR), macrophage inflammatory protein 1-beta (MIP-1β), metallopeptidase inhibitor 2 (TIMP2), and intracellular adhesion molecule (ICAM) (Fig. 4A). Other proteins, such as tumor necrosis factor-beta (TNFβ), interferon-gamma (INF-γ), chemokine I-309 (I-309), and eotaxin-2, were found at comparably lower levels, while some factors, including TNFα, interleukin 2 (IL-2), IL-3, IL-5, and IL-16, were detected only in supernatants from PRP-gels with 10,000 × 103 platelets/μL. Overall, the relative abundance of inflammatory proteins positively correlated with increasing platelet concentration in PRP-gels. Based on these findings, the release of CCL5 over time was investigated by ELISA (Fig. 4B, C). The total amount of secreted CCL5 was significantly higher compared to TGFβ-1, PDGF, and VEGF, also measured by ELISA. After 12 h postgelification, the cumulative release of CCL5 (Fig. 4C) showed the highest values in 10,000 × 103 platelets/μL gels (211.2 ± 97.5 ng), followed by 2000 × 103 platelets/μL gels (77.1 ± 6.8 ng), with lowest values in 1000 × 103 platelets/μL gels (37.3 ± 3.1 ng). The peak of CCL5 release appeared within the first 2 h after gelification and was sustained at moderate levels over the next 5 days (Fig. 4B).
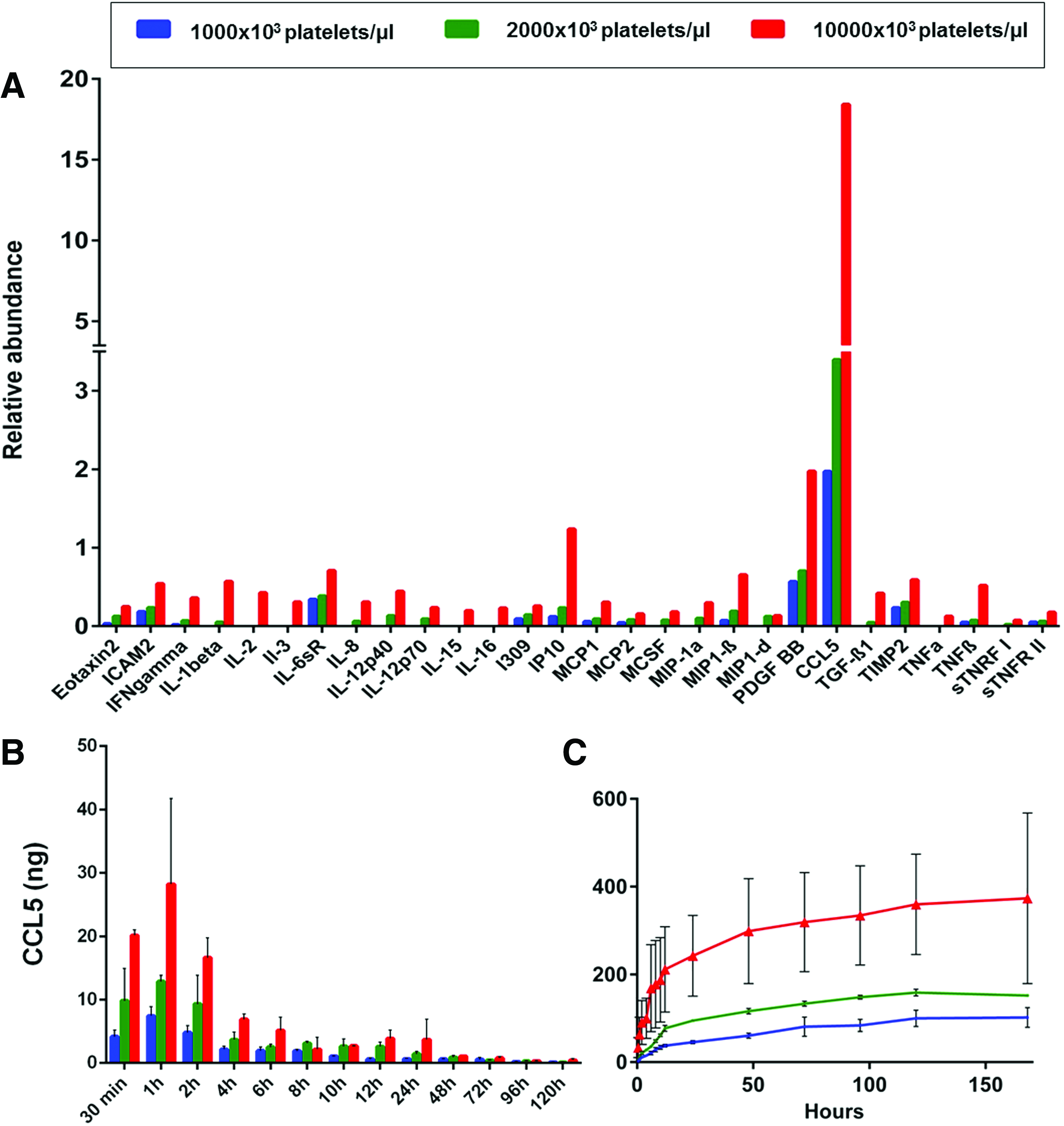
PRP-gels release inflammatory proteins. Supernatants from PRP-gels from two donors were collected after 12 h of incubation and pooled, and the relative abundance of inflammatory proteins was analyzed using an antibody protein array
Platelet concentration in PRP-gels influences MSC behavior
MSCs could be successfully cultured for 7 days in all PRP-gels, regardless of the platelet concentration. A difference in DNA content between different platelet concentrations was observed directly after cell encapsulation (Fig. 5A). The highest DNA content was found in 1000 × 103 platelets/μL gels, followed by 2000 × 103 and 10,000 × 103 platelets/μL gels. The same trend was noticed at days 3 and 7. Overall, the DNA content at day 7 in all tested PRP-gels was approximately twofold higher compared to that at day 0.

Proliferation and viability of mesenchymal stem cells (MSCs) in PRP-gels.
PI staining revealed an average percentage of viable cells at day 0 (3 h after seeding) of 98.3% ± 0.14%, 93.3% ± 2.43%, and 93.2% ± 1.70% in 1000 × 103, 2000 × 103, and 10,000 × 103 platelets/μL gels, respectively (Fig. 5B). At day 3, the highest cell viability was detected for PRP-gels with 1000 × 103 platelets/μL (96.8% ± 0.07%) and significantly different (p < 0.05) compared to 89.8% ± 2.14% in 10,000 × 103 platelets/μL gels. At day 7, the cell viability in gels containing the lowest concentration of platelets was the highest, reaching 92.4% ± 0.88%. For PRP-gels with 2000 × 103 and 10,000 × 103 platelets/μL, the viability was 86.73% ± 2.46% and 87.13% ± 2.75%, respectively. Live–dead staining showed a change in the cell morphology over time, with rounded cells on day 0 to a spindle-shaped morphology at days 3 and 7. The density of cells seeded in gels increased over time (Fig. 5C).
Discussion
An in vitro characterization of PRP-gels created from platelet concentrates, activated by human thrombin, and composed of different platelet concentrations was performed. It could be shown that the platelet concentration within PRP is a crucial factor determining gel properties and influencing behavior of encapsulated cells.
To the best of our knowledge, no study has investigated the viscoelastic properties of PRP-gels. For the PRP-gels prepared in the present study, a prevalence of storage over loss modulus was observed for every platelet and thrombin concentration. This is a direct consequence of the cross-linking at the molecular level. Macroscopically, this means that the material tends to maintain its shape rather than creeping and spreading like a viscous fluid. This property, in combination with a composition that is more than 95% water, allowing nutrition and waste transport, makes hydrogels effective cell carriers. In this study, it was shown that the highest storage modulus was achieved by PRP-gels with 1000 × 103 and 2000 × 103 platelets/μL gelified with 5 U/mL thrombin. Higher platelet content in PRP-gels did not result in increased stiffness. A possible explanation for this is that a proper balance between concentration of platelets and thrombin has to be reached to effectively gelify PRP; otherwise, some of the platelets stay in inactivated form and do not contribute to gel formation. Furthermore, a dense matrix of PRP-gels containing highly concentrated platelets may prevent a proper diffusion of thrombin within the gel. Additionally, platelets at a higher number may act as external bodies hindering the contact between the fibrinogen strands and their effective cross-linking. Despite the efficient cross-linking, PRP-gels do not have a stiffness of a load-bearing structure; hence, their mechanical properties are very limited. However, previous reports indicate that stiffness of hydrogels may influence behavior and differentiation potential of incorporated MSCs.37,38
The importance of the platelet activator is not only limited to induction of platelet aggregation; an exogenous triggering factor is also necessary to ensure a complete release of GFs. 39 In the current study, thrombin was used, and it was hypothesized that this will result in a rapid gel formation, degranulation of platelets, and an immediate release of GFs. It was demonstrated that the majority of GFs were, indeed, released within the first 6 h after the gel has formed. The results of this study agree with previous reports indicating that most of the release occurs between 1 and 6 h after clot formation.40,41 Interestingly, even 12 h after gelification, GF release could be detected, however, at clearly lower concentrations. One possible explanation for this is that some of the GFs remain captured in the PRP-gel and as a consequence are secreted at later time points. It is likely that GFs located peripherally in the gel may diffuse faster than the centrally situated ones. Furthermore, some GFs may be initially captured within the fibrin mesh of PRP-gel; hence, their release occurs at later time points. In addition, the presented in vitro investigation does not completely reflect the in vivo situation, where tissue-specific factors, proteins, and body fluids would interact with the applied material. In addition, various cells migrating into the PRP-gel may further influence the process of gel degradation and GF release. Rademakers et al. studied PRP degradation (platelet concentration ∼1000 × 103 platelets/μL) in an animal study and found that the weight of autologous platelet clots was reduced to 16% of the initial weight after 30 min of incubation in the pericardial sac. 42 In vivo tissue-related factors regulate the secretion of GFs from platelets. In addition, recruited or cotransplanted cells may also secrete GFs. 43 Another question is whether the released amount of GFs is physiologically relevant. Further studies are necessary to investigate the optimal concentration of GFs at the injury site and whether lower amounts still have a positive effect on tissue repair. Interestingly, a study investigating the mRNA profile of human platelets suggests that platelets may synthesize some cytokines and GF de novo. 44
The results of this study support the hypothesis that release of proteins from PRP-gels is correlated with the platelet concentration. Similar results have been reported previously 39 ; however, also opposite findings, indicating a poor correlation between platelet number and GF content, have been reported.36,45 Among the screened GFs in supernatants from our PRP-gels, CCL5 was released in the greatest amounts, followed by TGFβ-1. TGFβ has been proposed for the treatment of chronic inflammatory diseases, soft and hard tissue regeneration, and autoimmune diseases. 46 It has been shown that TGFβ signaling enhances maturation of osteoblasts and bone matrix deposition. 47 Accordingly, several studies suggest positive effects of TGFβ when used for bone repair.48–51 PDGF-AB and PDGF-BB were other GFs found in supernatants from PRP-gels in this study. PDGFs are known to promote the proliferation of bone cells and influence osteoblastic mitogenesis. 52 Based on this, PRP-gel may serve as a local delivery system of TGFβ and PDGF into bone defects. Considering the proangiogenic effects of PDGF and VEGF, 6 PRP-gels may further enhance bone healing by supporting revascularization.
In supernatants from PRP-gels, many chemokines and mediators that are known to possess proinflammatory properties could be detected in this study. CCL5 was released at the highest levels, peaking at 1 h after platelet activation and still detectable up to 5 days after. Interestingly, in a study investigating the release of GFs from equine platelets, it was found that secretion of CCL5 was not associated with platelet activation and persisted longer than other GFs, suggesting that CCL5 release may be regulated differently. 41 CCL5 may have deleterious effects on the healing process since it attracts activated leukocytes to the injury site and their accumulation may abolish beneficial effects of GFs.53,54 Increased infiltration of leukocytes may lead to tissue damages and a persistent inflammatory phase.55,56 In contrast, an early inflammatory phase is an essential component initiating the healing process, even though many mediators can either stimulate or suppress tissue repair during inflammation. 57 Furthermore, it has been shown that CCL5 is a main chemoattractant released by degenerated discs, and its presence may enhance the migration of MSCs and progenitor cells toward injury sites. 58 Another study investigating the role of CCL5 in mouse wound healing suggests that this protein induces migration of endothelial progenitor cells. 59 These findings are particularly interesting for tissue engineering strategies because application of PRP-gels that locally release CCL5 may intensify cell mobilization, enhance vascularization, and therefore improve the healing process.
In this study, MSCs could be successfully cultured in all tested PRP-gel compositions. The rationale behind encapsulating MSCs into gels was to investigate whether PRP-gels could be used as a scaffold and delivery system of GFs and cells at the injury site. From a clinical point of view, it could be potentially beneficial in patients suffering from impaired wound healing and tissue loss, such as bony defects or cartilage lesions, when GFs and cells are needed to enhance repair. We found that cell survival and proliferation were greatest in gels containing the lowest platelet concentration (1000 × 103 platelets/μL). A study investigating the proliferation of MSCs and adipose tissue-derived stem cells encapsulated into PRP-gels has shown a three to fivefold increase of the cell number after 7 days of culture. 33 In that study, the platelet number in PRP-gels was sixfold higher than the average concentration in the whole blood. Similar findings were reported in a study investigating the effect of platelet concentration on bone healing, suggesting that a moderate platelet concentration (two to sixfold concentrated) gives optimal results. 18 These studies along with our results suggest that a lower platelet content in PRP seems to be more favorable for incorporated cells. Thus, most of the commercially available systems based on whole-blood centrifugation usually yield to 2× to 3× platelet enrichment levels compared to baseline when used in standard settings. 25 Therefore, our preparation method of PRP-gels allows obtaining optimal platelet concentration in a clinically feasible manner.
In summary, the results of this study demonstrate that PRP-gels are stable hydrogels, which can effectively deliver bioactive substances and MSCs for various clinical applications. Importantly, the platelet concentration seems to determine the efficacy and properties of PRP-gels. It was shown that a concentration of 1000 × 103 platelets/μL in PRP provides an optimal environment for encapsulated MSCs. With regard to clinical application, the concentration and balance of pro- and anti-inflammatory substances should be further investigated to maximize efficacy.
Footnotes
Acknowledgment
The FACSAria III was donated by the Innovationsstiftung Graubünden.
Disclosure Statement
No competing financial interest exists.