
Abstract
Our bilayered self-assembled skin substitutes (SASS) are skin substitutes showing a structure and functionality very similar to native human skin. These constructs are used, in life-threatening burn wounds, as permanent autologous grafts for the treatment of such affected patients even though their production is exacting. We thus intended to shorten their current production time to improve their clinical applicability. A self-assembled decellularized dermal matrix (DM) was used. It allowed the production of an autologous skin substitute from patient's cells. The characterization of SASS reconstructed using a decellularized dermal matrix (SASS-DM) was performed by histology, immunofluorescence, transmission electron microscopy, and uniaxial tensile analysis. Using the SASS-DM, it was possible to reduce the standard production time from about 8 to 4 and a half weeks. The structure, cell differentiation, and mechanical properties of the new skin substitutes were shown to be similar to the SASS. The decellularization process had no influence on the final microstructure and mechanical properties of the DM. This model, by enabling the production of a skin substitute in a shorter time frame without compromising its intrinsic tissue properties, represents a promising addition to the currently available burn and wound treatments.
Introduction
I
Our group previously presented bilayered self-assembled skin substitutes (SASS) made of a dermal substitute underlying a fully differentiated epidermis, which generated an engineered tissue similar in structure and function to native human skin4–6 for clinical use in wound healing 7 and burn treatment.8,9 SASS are currently used in a clinical trial for the permanent coverage of full-thickness wounds (ClinicalTrials.gov NCT02350205). The self-assembly strategy used to produce a reconstructed dermal substitute entails that adult or neonatal fibroblasts, cultured under adequate conditions, produce and organize their own extracellular matrix (ECM) without an exogenous scaffold.10–13 With our current standard protocol, the production of the dermal substitute of the SASS requires 3–4 weeks and is the most time-consuming step.12,14 Our aim was to modify the SASS production process to obtain a significant reduction in the dermal production time from the point where the patient's cells have been harvested and expanded in culture, allowing quicker grafting of the skin substitute on the patient. The chosen approach was to use a self-assembled preproduced acellular dermal matrix (DM) for autologous cell seeding.
Some available dermal matrices use xenogenic material (bovine collagen, chondroitin-6-sulfate, polyglactin, polyglycolide [PGA], etc) that can eventually stimulate an untoward immunologic response in some patients.15,16 The ECM of the acellular DM presented herein is produced from the cells themselves, thus generating substitutes with an ECM composition quite similar to native tissue.4–6 Cells are then removed, leaving the self-assembled ECM available for later autologous cell repopulation and in situ basement membrane formation. One must note that a single population of newborn cells, vetted for adventitious infectious agents, was used for the matrix bank production. This minimizes the risks of infectious disease transmission from grafts composed from multiple donors, as seen with acellular human cadaver skin. Many different protocols for dermis decellularization have been proposed to generate such matrices using various chemical, enzymatic, and physical agents. 17 Aggressive decellularization processes can be more effective for removing cell residues, but are also generally more disruptive for the ECM elements.17,18
To preserve the ECM integrity as much as possible following the decellularization process, a minimally disruptive decellularization technique without any chemical or enzymes was used to produce the acellular dermal matrices. Moreover, the long-term preservation of acellular dermal matrices allows the generation of readily available scaffolds, which can be used at a later appropriate time.
This study describes a method that reduced the production time for autologous bilayered SASS up to at least 3 weeks by using a decellularized self-assembled DM. Our results demonstrated a significant reduction in production time from patient biopsy to clinical availability as well as the generation of a skin substitute that presented similar characteristics and functionality compared to the standard bilayered SASS, as shown by histological, immunofluorescence mechanical testing and transmission electron microscopy (TEM) analyses.
Materials and Methods
Cell culture
Neonatal fibroblasts and keratinocytes were extracted from a single donor (4 days old) foreskin biopsy by the two-step thermolysin and trypsin isolation procedure, as previously described.12,19 Briefly, the epidermis and dermis were gently separated after a thermolysin incubation step using fine forceps (0.5 mg/mL; Sigma, St. Louis, MO). Fibroblasts were isolated from the dermis using collagenase H (Roche Diagnostics, Laval, QC, Canada), while keratinocytes were extracted from the epidermis using a trypsin/EDTA solution (0.05% trypsin (Intergen Company, Purchase, NY), 0.01% EDTA/disodium salt (J.T. Baker, Phillipsburg, NT)). Cells were then collected by centrifugation and inoculated into culture flasks.
Keratinocytes were grown on a feeder layer of irradiated human fibroblasts in the Dulbecco–Vogt modified Eagle's medium (DMEM; Invitrogen, Burlington, ON, Canada), supplemented with HAM's F12 in a 3:1 ratio (DMEM HAM; Invitrogen), containing 5% newborn calf serum (FetalClone II; HyClone, Logan, UT), 0.4 μg/mL hydrocortisone (Calbiochem, La Jolla, CA), 5 μg/mL insulin (Sigma), 10−6 M isoproterenol (Sandoz Canada, Boucherville, QC, Canada), 10 ng/mL epidermal growth factor (Austral, San Ramon, CA), penicillin (Sigma), and gentamicin (Schering, Pointe-Claire, QC, Canada). Fibroblasts were grown in DMEM supplemented with 10% fetal calf serum (FCS; HyClone, Scarborough, ON, Canada) and antibiotics (penicillin 100 UI/mL and gentamicin 25 μg/mL). Both cell types were maintained at 37°C in a humidified incubator containing 8% CO2, and culture media were changed thrice per week during the culture period.
Production of SASS
Standard SASS were obtained using the self-assembly reconstruction method, as previously described.7,12 Briefly, fibroblasts were first expanded for 7 days in DMEM 10% FCS. After expansion (7 days), fibroblasts were seeded in flasks (Falcon) at 4 × 103 cells/cm2 and cultured for 25 days in DMEM 10% FCS and 50 μg/mL ascorbic acid. Fibroblasts secreted their own ECM and produced cohesive sheets. These sheets were then stacked to form a dermal substitute composed of fibroblasts and their ECM. These dermal substitutes were cultured for 1 week to allow for sheet fusion. Keratinocytes were then seeded on the dermal substitutes at 1 × 105/cm2 to form the epidermal layer. Keratinocyte proliferation onto the dermal substitute was allowed by culturing immersed in a medium for 1 week. Final keratinocyte differentiation took place after the skin substitute was raised at the air–liquid interface 20 for an additional 10 days.
Thus, the total production duration was 8 weeks (56 days). This duration is calculated from a starting point that occurs 9–10 days after cells have been harvested from a patient's biopsy and subjected to an initial culture (see Fig. 1A).

Representation of the in vitro production timeline of standard self-assembled skin substitutes (SASS) and the self-assembled skin substitute reconstructed from a decellularized dermal template (SASS-DM), from the patient biopsy to clinical availability.
Production of a decellularized self-assembled dermal template (DM)
Neonatal fibroblasts were seeded at 4 × 103 cells/cm2 in a 75-cm2 flask (Falcon; BD, Franklin Lakes, NJ) and cultured for 19 days in DMEM supplemented with 10% FCS containing 50 μg/mL ascorbic acid to produce tissue sheets. 12 Three dermal sheets were superimposed to form a tissue-engineered dermal template comprising fibroblasts and their self-secreted ECM and cultured for a week to allow an appropriate cohesion between the sheets. 7
Following this culture period, the dermal templates were decellularized using two cycles of osmotic shock, followed by a rinsing, and a dehydration process. 21 The dermal templates were first immersed in hypo-osmolar sterile apyrogen water (Milli-Q; EMD Millipore, Billerica, MA) for 5 h at 4°C. The dermal templates were then gently rinsed once using sterile apyrogen water. Following supernatant aspiration, they were left overnight, dishes open, in an actively operating laminar flow cabinet. The next day, they were submitted to a second cycle of the previously described process to result in the decellularized DM. Finally, the DMs were frozen at −20°C and stored until further usage.
Decellularized DM rehydration
Frozen DMs were thawed overnight at 4°C in cold DMEM containing penicillin 100 UI/mL, gentamicin 25 μg/mL, and 0.5 μg/mL amphotericin B. The next day, they were immersed in DMEM containing 10% FCS with penicillin 100 UI/mL and gentamicin 25 μg/mL and kept in an incubator for 1 day. Rehydrated DMs were then used for further SASS using decellularized dermal matrices (SASS-DM) reconstruction.
Production of bilayered SASS-DM
Fibroblasts were expanded in culture for a week in DMEM 10% FCS and then seeded at a 4.2 × 104 cells/cm2 density on thawed matrices. The recellularized matrices were cultured in DMEM containing 10% FCS and 50 μg/mL ascorbic acid for a week to allow repopulation by the seeded cells, resulting in a tissue-engineered dermal substitute. Following that culture step, keratinocytes were seeded as described above for SASS production. The total production duration of SASS-DM was thus 4 and a half weeks (31 days). This duration is calculated from a starting point that occurs 9–10 days after cells have been harvested from a patient's biopsy and subjected to an initial culture, before the selected start point where they are seeded for a 7-day expansion time (see Fig. 1B).
Histological and immunofluorescence analysis
SASS and SASS-DM biopsies were embedded in a Tissue-Tek Optimal Cutting Temperature Compound (OCT; Bayers, Etobicoke, ON, Canada) and frozen for further immunofluorescence analyses or fixed in HistoChoice (Amresco, Solon, OH), embedded in paraffin, and sectioned and stained with Masson's trichrome 22 for histological analysis. Other samples were fixed in 2.5% glutaraldehyde (Canemco, Lakefield, QC, Canada) in a 0.1 M sodium cacodylate (Mecalab, Montreal, QC, Canada) buffer overnight at 4°C, washed in a 0.1 M sodium cacodylate buffer, and embedded in PolyBed 812 (Polysciences, Warrington, PA) according to standard procedures for TEM analysis. 14
Indirect immunofluorescence assays were performed on 5-μm-thick cryosections of the skin substitutes fixed in acetone as previously described. 23 Cell nuclei were stained with Hoechst 33258 (Sigma Chemical, St. Louis, MO). Primary antibodies were replaced by a phosphate-buffered saline-bovine serum albumin 1% for negative controls. The primary and secondary antibodies used for immunofluorescence analysis are presented in Table 1. Slides were observed under a Zeiss microscope equipped with Zeiss Axiocam HRm Rev 3 and Axiocam ICc1 digital cameras for immunofluorescence and histological imaging, respectively. Images were processed with the AxioVision 4.8.2 software (Carl Zeiss Canada Ltd., Toronto, ON, Canada).
mAb, monoclonal antibody; pAb, polyclonal antibody.
Mechanical properties analysis
Uniaxial tensile tests were performed on tissue specimens prepared using a dog bone-shaped die cut and a Tytron™ 250 Microforce Testing System (MTS Systems Corporation, Eden Prairie, MN) as previously described. 24 The skin specimens were placed between a static and a dynamic anchorage. The movement of the dynamic anchorage at a constant displacement rate of 0.2 mm per second pulled on the tissue until rupture, while a load cell recorded the load applied on the sample.
The ultimate tensile strength (UTS) and failure strain were defined, respectively, by the peak stress (MPa) and maximum deformation (%) withstood by the samples before failure. The tensile modulus was defined as the slope of the linear portion of the stress—strain curve in the 25–80% range of the UTS of the sample, 24 thus producing information about tissue stiffness. The applied stresses and strains were calculated by dividing the recorded load level by the initial cross-sectional area of the sample using the width of the die cut and the thickness of the sample based on histology. A minimum of four specimens were tested per condition, and stress–strain curves were plotted and analyzed using a MATLAB© script (The MathWorks, Natick, MA). 24
Results
The aim of the work described herein was to reduce the fabrication time required for the production of autologous SASS from patient biopsy to clinical availability. In the current study, the dermal culture phase was circumvented by the use of a self-assembled decellularized and dehydrated DM, produced using nonautologous cells and allowing the initiation of patient cell culture further along in the reconstruction process (Fig. 1). Thus, this strategy allowed the standard 8-week SASS reconstruction protocol to be shortened to about 4 and a half weeks (Fig. 1A, B).
The obtained SASS-DM were resistant, could be handled easily, and presented a macroscopically uniform stratum corneum as SASS (Fig. 2A). Histological analysis of the SASS-DM after 10 days of culture at the air–liquid interface (Fig. 2B) revealed a fully differentiated epidermis similar to the standard SASS used for comparison purposes (Fig. 2C). Both engineered tissues presented normal human skin histological aspects and features (Fig. 2D), such as a stratified epithelium and a dermal component, with dense collagen fibers stained blue with Masson's trichrome.
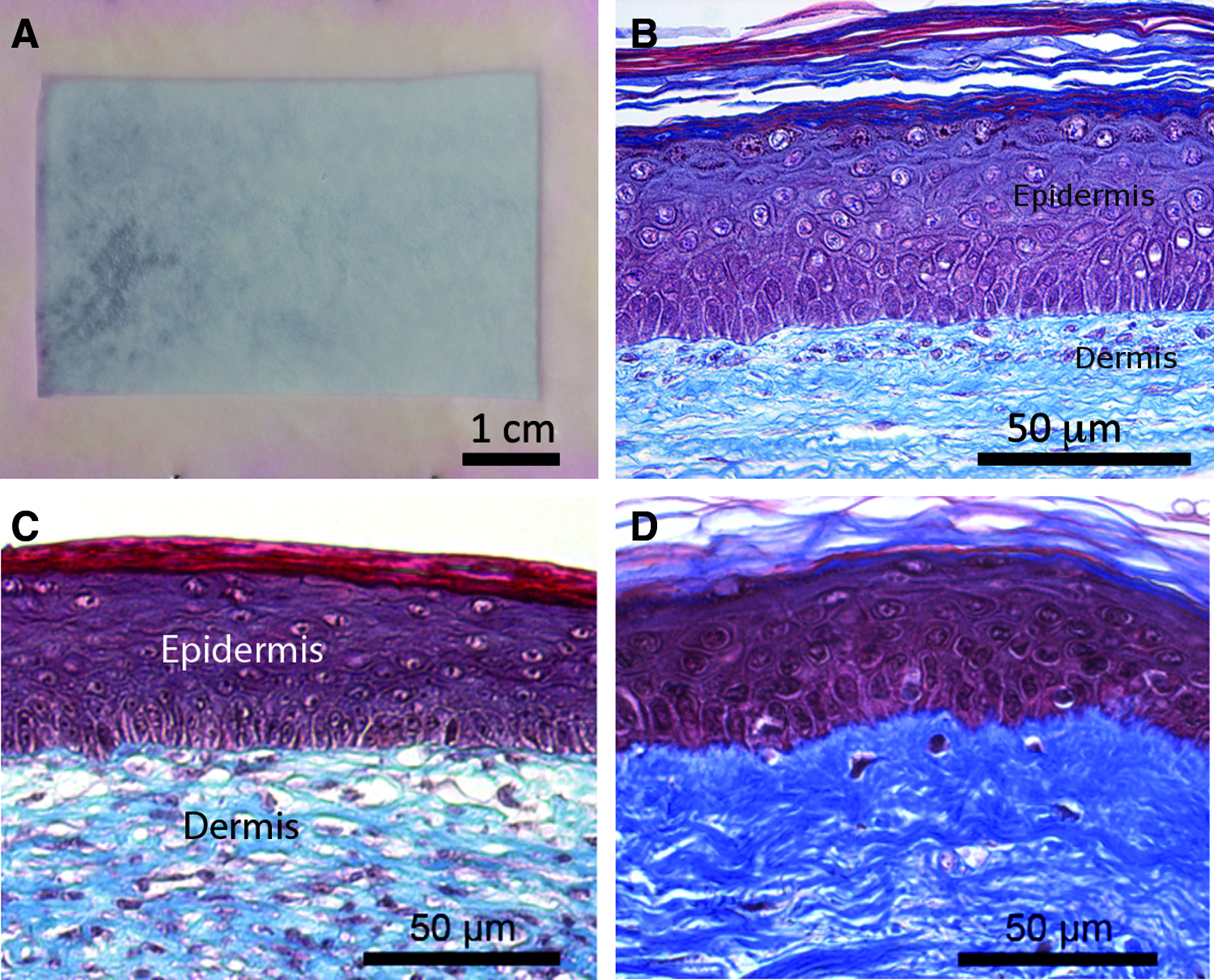
Macroscopic aspect of the SASS-DM after 10 days of culture at the air–liquid interface
Immunofluorescence assays showed in SASS-DM, the expression of epidermal differentiation-specific protein markers, such as keratin 10 (K10), filaggrin, involucrin, and transglutaminases. As expected, K10 expression began at the first suprabasal cell layer (Fig. 3A), while involucrin, a transglutaminase protein substrate incorporated in the differentiating keratinocytes' cornified envelope, transglutaminase-1, and filaggrin were seen in the upper cell layer of the SASS-DM (Fig. 3B–D, respectively). 14 The proliferation marker Ki67 was expressed in basal cells of the epithelium as expected 14 (Fig. 4C). Some basal cells were also found to express keratin 19 (K19), a marker of epidermal stem cells,23,25 suggesting the maintenance of a pool of basal regenerative cells within the engineered tissue (Fig. 4D). The expression of those markers suggests adequate epidermal differentiation as well as stem cell preservation into the skin substitute.
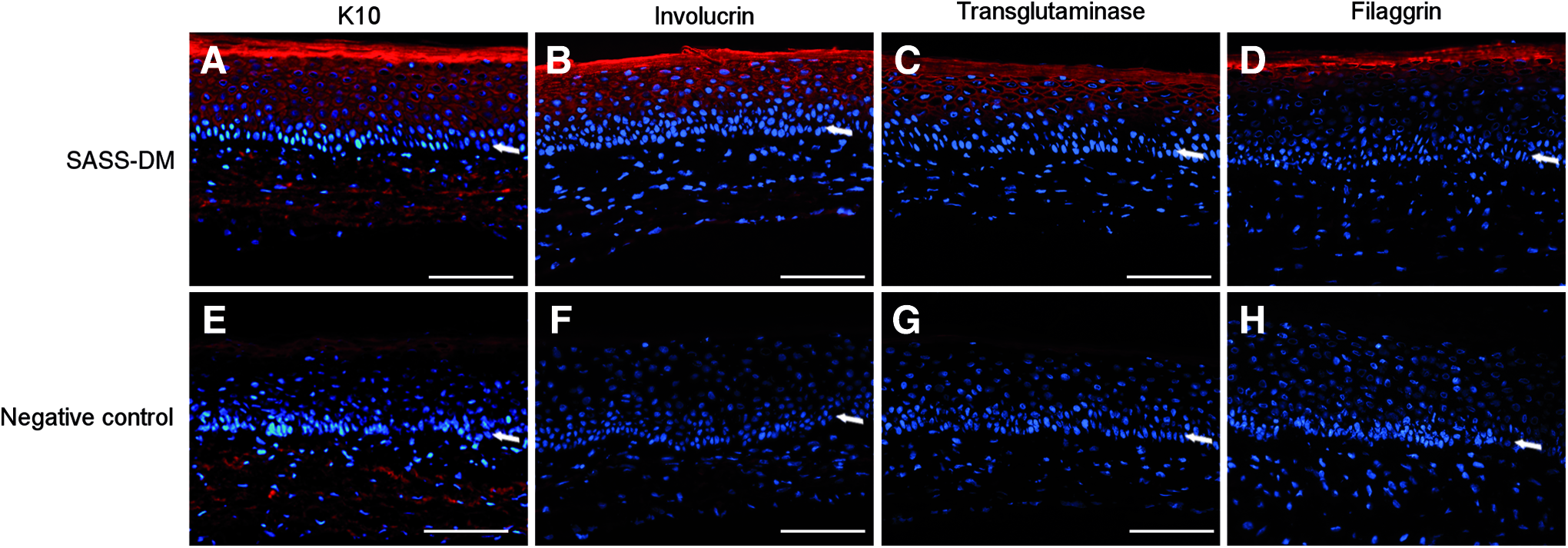
Immunofluorescence labeling of keratin 10 (K10)
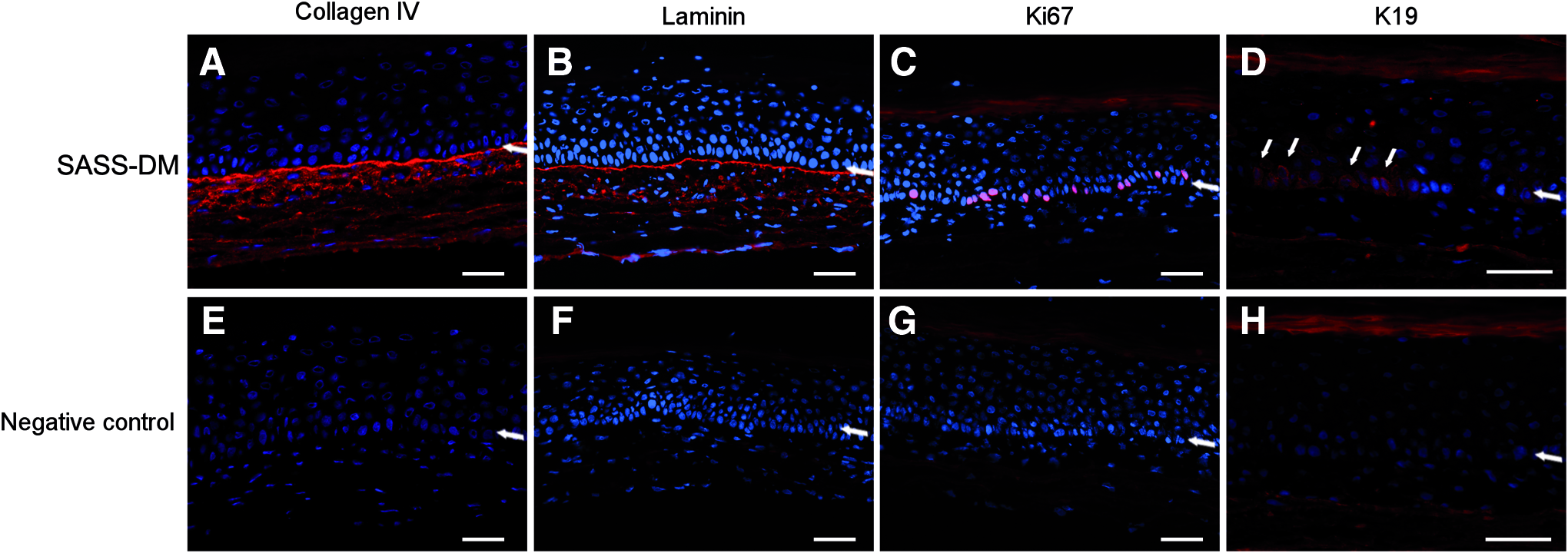
Immunofluorescence labeling of collagen IV
The presence of type IV collagen and laminin, both essential components of the basement membrane structure, was evaluated, since the basement membrane is very important for the cohesion at the dermoepidermal junction. As expected, type IV collagen and laminin were expressed at the interface between the dermal template and the epithelium within the SASS-DM (Fig. 4). The presence of hemidesmosomes and a basement membrane in the SASS-DM was further confirmed by TEM (Fig. 5).
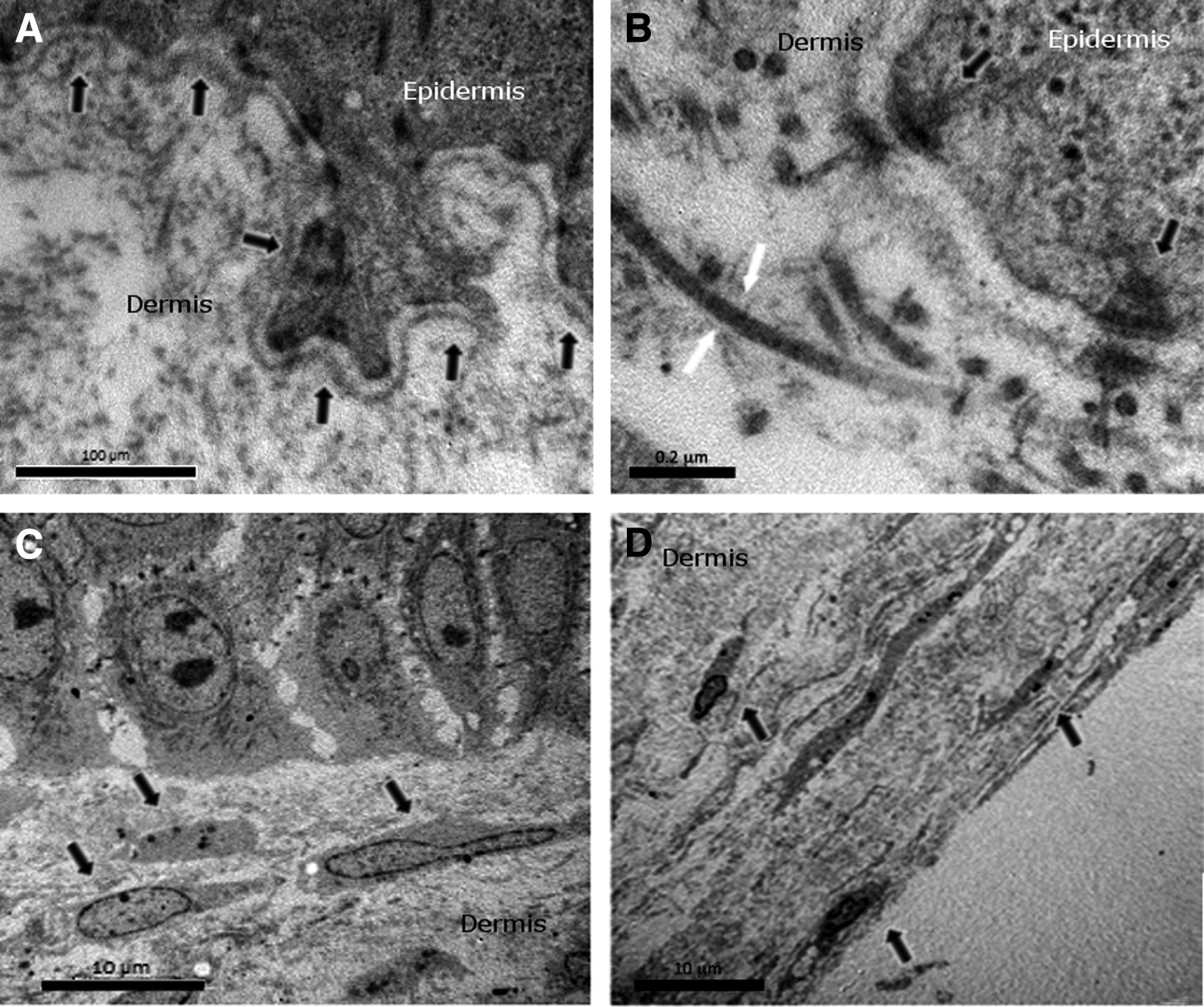
Transmission electron microscopy analysis of the SASS-DM. Presence of a continuous basement membrane (arrows)
Immunofluorescence assays performed on the DM after decellularization showed expression of key native dermal constituents, such as type I and type III collagens, decorin, 26 and tenascin-C 27 (Fig. 6). The intensity of these markers was preserved once final SASS-DM reconstruction was achieved (Fig. 6). TEM analysis showed dense bundles of collagen, without disruption of the ECM microstructure following decellularization (Fig. 5). Fibroblasts were shown to be surrounded by a dense matrix found in both superficial and deeper portions of the SASS-DM dermal layer (Fig. 5).

Immunofluorescence labeling of collagen I
Mechanical testing was conducted on the tissues to compare the resistance of SASS with SASS-DM (Fig. 7). A characteristic viscoelastic stress–strain curve was obtained for every sample submitted to tensile testing, displaying a toe region followed by a linear segment and a rupturing point (not shown), defining the UTS and failure strain of the tissue. Results showed no significant differences between the tested samples. Thus, the use of a decellularized DM in tissue-engineered skin reconstruction was not shown to interfere with its mechanical characteristics.
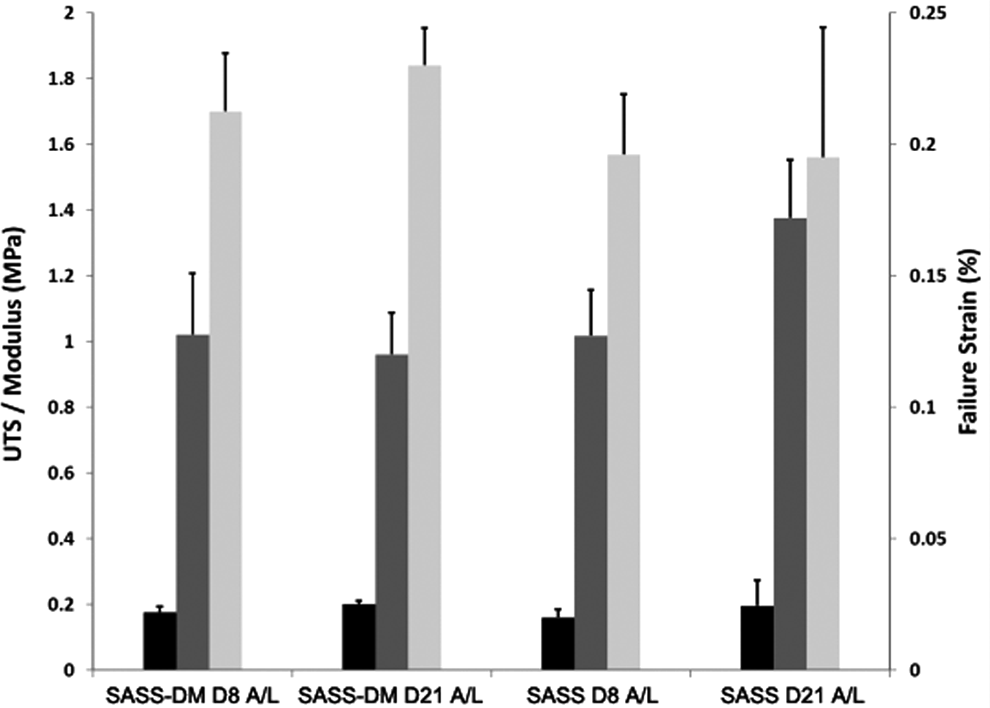
Mechanical properties of SASS-DM and SASS after 8 and 21 days of air–liquid interface maturation. Results showed no significant difference for the tensile testing parameters, as ultimate tensile strength (UTS) (black), linear modulus (dark gray), and failure strain (light gray) were all within the same range regardless of the tissue or culture condition. These results demonstrated the capacity of the new fabrication method (SASS-DM) to generate tissues presenting a similar mechanical behavior compared with SASS.
Discussion
In this study, we described the production of a bilayered skin substitute using a decellularized DM that allowed us to reduce the production time up to 3 and half weeks. In the standard protocol, the culture of fibroblast until the formation of a manipulable tissue sheet can take 21–28 days depending on the fibroblast capacity to secrete ECM, which is donor dependent. The new fabrication protocol presents significant clinical interest since it considerably reduces the culture period with patient cells required for autologous tissue production and results in skin substitutes with resistant DM from any patient, regardless of their fibroblasts' ability to synthesize ECM.
The use of this previously prepared decellularized DM for skin tissue engineering allowed the bypassing of the longest phase of the SASS culture, the production of an adequate dermal component (Fig. 1). Furthermore, this approach allowed the production of banks of standardized self-assembled dermal templates that can be frozen and used as clinical need arises.
A production time frame of 4 and a half weeks is comparable to some currently available autologous skin substitutes. Tissue-Tech Autograft System™ is a skin substitute in which autologous fibroblasts and keratinocytes are seeded in a microperforated hyaluronic acid template and grafted onto patients in two steps. The dermal equivalent is first grafted after a week of cell culture and then the epidermal substitute is apposed on top of the dermal equivalent after another week of cell culture. Thus, the skin substitute is available in a minimum of 2 weeks and it requires two operations for the patient. PermaDerm© is another bilayered autologous skin substitute in which fibroblasts are seeded into a dermal template composed of a polymer of bovine collagen and glycoaminoglycans. Autologous keratinocytes are seeded on top of the dermal equivalent, to produce a differentiated epidermis, after a period of dermal template maturation. The production timeline of this substitute is 4 weeks. PolyActive™ is a substitute composed of autologous fibroblasts seeded into a synthetic biodegradable DM made of polyethylene glycol terephthalate and polybutylene terephthalate (PEGT/PBT). After a maturation period of 3 weeks, autologous keratinocytes are seeded on top of the dermal equivalent and cultured for an additional 2 weeks. This product is clinically available within 5 weeks. MyDerm™ is a skin substitute using fibrin produced from the patient's plasma as a template for bilayered autologous skin reconstruction. This skin substitute is available in 4 weeks. Thus, the other comparable models are clinically available between 2 and 5 weeks. Moreover, SASS-DM are grafted in a single operation procedure, while some other skin substitutes require two interventions for the patient.
SASS-DM showed similar features compared to SASS in terms of structure, cell differentiation, and mechanical strength. The SASS-DM presented an ECM microstructure similar to native human skin, which was preserved after the decellularization process. Thus, SASS-DM could be a critical adjunct to current burn treatment options, generating tissues suitable for permanent coverage in a shorter time period compared with SASS.
SASS-DM presented a mechanical strength similar to SASS, with a well-preserved ECM microstructure following the decellularization and dehydration processes. Decellularization using hypotonic solutions causes cell lysis by osmotic shock, with minimal change in matrix molecule content, architecture, and cell growth potential.28,29 In contrast, hypotonic water has been shown to decrease matrix growth factor content, due to a rinsing effect. 28 However, considering the conservation of cell growth potential and the context that DMs are expected to be repopulated with fibroblasts, one can presume that lost growth factors will be promptly replaced by newly cell secreted ones. Therefore, preservation of growth factors in the DM used in this study would not have the same importance compared to other matrix models where efficiency depends on such a phenomenon.30,31 The elimination of the possible risk that exogenous cytotoxic chemicals, enzymes, or detergents could be retained within the matrix also represents an important benefit of osmotic decellularization.17,18
Matrix freezing contributes to tissue decellularization with intracellular ice formation causing cell lysis. 32 Interestingly, it has been demonstrated that cells frozen in tissues contain more intracellular ice than cells frozen in suspension due to cell–cell and cell–matrix interactions. 33 Indeed, tissue deformation following freezing, associated with an increased porosity and microstructure damage, is dependent upon matrix density linked to these interactions. 34 Decellularization and dehydration before freezing might minimize matrix deformation, explaining, in part, the microstructure preservation observed in the DM produced in this study. One must note that no decellularization process completely eliminates all cell content residues,35,36 while the preservation of an intact ECM structure helps to conserve tissue function 37 as well as minimize immunological reactions triggered by denatured matrix components. 38
The DM substitute proposed herein is reconstructed from newborn allogeneic cells that will be destroyed by a decellularization process before DM is used for the production of an autologous SASS. Newborn allogeneic cells have previously been used safely and successfully in skin substitutes grafted as temporary coverage in the treatment of severely burned patients. 39 Neonatal allogeneic fibroblasts alone seeded in a bioabsorbable polyglactin mesh or on bovine collagen-coated mesh, or neonatal allogeneic fibroblasts together with keratinocytes seeded in a bovine collagen scaffold40,41 resulted in no adverse reaction,42–44 while final rejection of the grafts can be observed when living cells were grafted. 45
In a clinical setting, these allografts are applied on burns to cover, prepare, and stabilize extensive wounds before the definitive skin autograft. These temporary allografts are gradually rejected by the immune system, the initiation of rejection occurring at a mean of 2 weeks after grafting. 45 Once rejected, these grafts need to be removed and replaced until the final treatment is available. Thus, the reduction of the production time from 8 to 4 weeks can be of critical benefit from a clinical standpoint, since only one cycle of allograft or xenograft application may be necessary, instead of multiple courses, before the application of a product that offers a final treatment. This is expected to reduce the clinical morbidity of patients.
Conclusion
We described a novel production technique to accelerate the fabrication of bilayered SASS. The use of a preproduced decellularized self-assembled DM allowed us to circumvent the time-consuming dermal reconstruction phase of the standard tissue-engineered skin reconstruction protocol. This strategy allowed a reduction of 3 and a half weeks from the 8 weeks standard production time required to produce the SASS. This should represent a significant clinical gain for burn patient treatment. The SASS-DM showed structural features, cell differentiation behavior, and mechanical properties similar to a standard bilayered SSAS. Thus, this model could be an important adjunct to current burn treatment options. In vivo grafting of these faster produced SASS is ongoing.
Footnotes
Acknowledgments
The authors would like to thank Todd Galbraith and Sophie Roberge for technical assistance, as well as the Fonds de Recherche du Québec—Santé (FRQS), the Cell and Tissue therapy network of the FRQS (ThéCell), and the Fondation des Pompiers du Québec pour les Grands Brûlés for financial support.
Disclosure Statement
No competing financial interests exist.