
Abstract
In cartilage regenerative medicine, autologous chondrocyte implantation (ACI) has been applied clinically for partial defects of joint cartilage or nasal augmentation. To make treatment with ACI more effective and prevalent, modalities to evaluate the quality of transplanted constructs noninvasively are necessary. In this study, we compared the efficacy of several noninvasive modalities for evaluating the maturation of tissue-engineered auricular cartilage containing a biodegradable polymer scaffold. We first transplanted tissue-engineered cartilage consisting of human auricular chondrocytes, atelocollagen gel, and a poly-
Introduction
I
ACI in humans was first reported in 1994 in which autologous chondrocytes obtained from a healthy nonbearing site of cartilage in a knee joint were cultured in vitro and then transplanted into the defective sites. 2 Recently, the indications for ACI have been expanded to nasal augmentation and there have been reports of injection of chondrocytes in gelatinous chondroid matrix into subcutaneous pockets in the nose.3,4 Regardless of the site—joints or nose, these protocols utilize chondrocytes in solution or gel, having difficulty providing rigidity and a three-dimensional structure. To overcome such issues, our group has developed tissue-engineered cartilage consisting of autologous chondrocytes and a biodegradable polymer scaffold and conducted clinical research in patients with nasal deformities associated with cleft lip and palate (JPRN-UMIN000005472). The outcomes of our clinical research have been nonproblematic, with no major complication thus far, and the patients have been happy with the change in their facial features, judging from a questionnaire conducted to gauge their satisfaction. However, there are several issues to be considered for cartilage regenerative medicine to become more widespread. One is that we need proper and noninvasive evaluation modalities that can monitor the quality of the constructs after transplantation.
In animal models, tissue-engineered cartilage can be evaluated by conventional histological analysis such as hematoxylin and eosin (HE), TB, and safranin O staining. The content of cartilage matrix can be measured by biochemical analysis, including sulfated glycosaminoglycans (sGAG) and type II collagen. These evaluations for cartilage maturation are well established, but they involve a destructive procedure in the process. Therefore, the establishment of noninvasive, qualitative, and preferably quantitative monitoring methods is imperative to obtain objective results clinically. Meanwhile, imaging of cartilage is well developed in osteoarthritis (OA) research, since even small biochemical and morphological changes in cartilage need to be detected to avoid irreversible structural damage. Considering that the components of cartilage do not differ widely between hyaline cartilage of joints and elastic cartilage of the ear, the modalities used in OA evaluation could also serve to evaluate tissue-engineered cartilage containing auricular chondrocytes. There has been a recent review of original research articles related to imaging of OA, 5 in which MRI and radiography were shown to remain the primary imaging modalities in OA studies, while fewer studies used computed tomography (CT) and ultrasound. In another study assessing the disease activity in patients with rare relapsing polychondritis (RPC), their bronchial/laryngeal/auricular cartilage was examined with CT and MRI. 6 It was shown that imaging diagnosis in RPC using CT and/or MRI delivered information about the degree of disease activity in cartilage that correlated better with clinical features than nonspecific inflammatory laboratory markers.
In this study, we explored the feasibility of MRI, X-ray, and ultrasound for detecting the properties of subcutaneously transplanted tissue-engineered cartilage. We first transplanted tissue-engineered cartilage consisting of human auricular chondrocytes, atelocollagen gel, and poly-
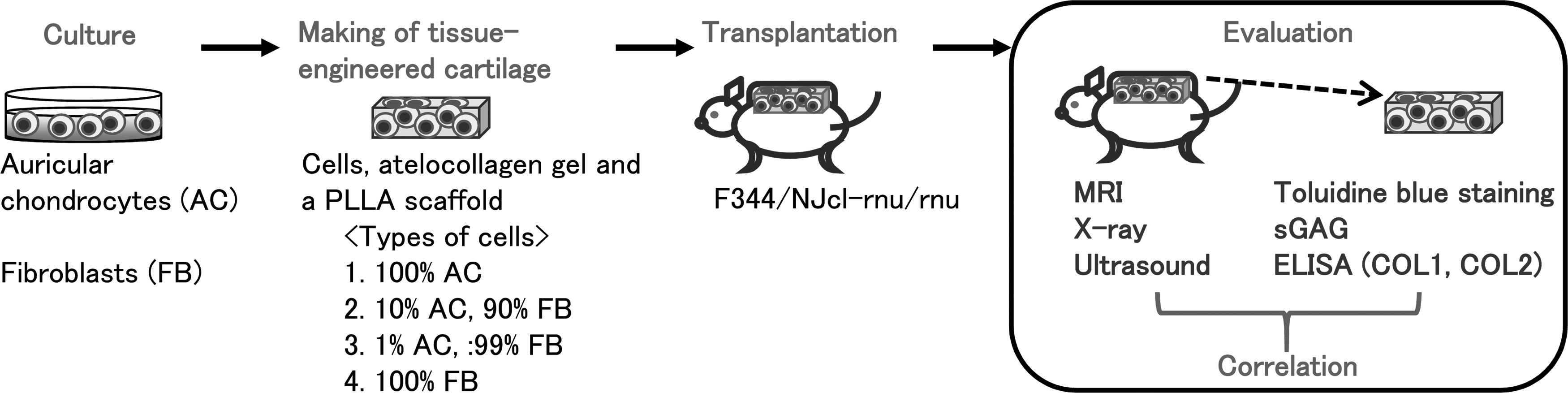
Outline of study. Human AC and human FB were cultured, and applied to poly-
Methods
Materials
Normal human dermal fibroblasts were purchased from Takara Bio, Inc. (Shiga, Japan). Dulbecco's Modified Eagle's Medium: Nutrient Mixture F-12 (DMEM/F12), phosphate-buffered saline, and TrypLE Select were from all Life Technologies (Carlsbad, CA). Penicillin and streptomycin were purchased from Meiji Seika Pharma Co., Ltd. (Tokyo, Japan). Insulin (Novolin R) was from Novo Nordisk Pharma Ltd. (Tokyo, Japan), FGF-2 was from Kaken Pharmaceutical Co., Ltd. (Tokyo, Japan), and human serum was from Sigma-Aldrich Co. LLC (Tokyo, Japan). Other materials included Liberase MNP-S from Roche Diagnostics (Mannheim, Germany), gelatin-coated flasks from Nippi Biomatrix Research Institute (Tokyo, Japan), 3% atelocollagen implants from Koken Co., Ltd. (Tokyo, Japan), anti-type I, II, and III collagen antibody from LSL (Tokyo, Japan), and Maeda resorcin-fuchsin fluid, Weigert's iron hematoxylin, and Van Gieson solution from Muto Pure Chemicals Co., Ltd. (Tokyo, Japan). The Human Type I Collagen Detection Kit and Human Type II Collagen Detection Kit were from Chondrex, Inc. (Redmond, WA), and the GAG kit was from Wieslab AB (Lund, Sweden). F344/NJcl-rnu/rnu rats were purchased from Nisseizai (Tokyo, Japan).
Cell culture
Human auricular chondrocytes were obtained from remnant auricular cartilage of patients with microtia who underwent surgery at Nagata Microtia and Reconstructive Plastic Surgery Clinic (Saitama, Japan), with informed consent. All the procedures for these experiments were approved by the ethics committee (Ethics permission 2573) or institutional committee for animal research of the University of Tokyo Hospital. The experiments were conducted according to the principles expressed in the Declaration of Helsinki. Isolation of human auricular cartilage and culture of chondrocytes were conducted as follows: human chondrocytes were isolated from remnant auricular cartilage by 0.6% Liberase digestion at 37°C for 18 h. Isolated chondrocytes were seeded in 2.5 cm2 gelatin-coated cell culture flasks at a density of 8.33 × 104 cells/cm2 and cultured in DMEM/F12 containing 100 units/mL penicillin, 0.1 mg/mL streptomycin, 100 ng/mL FGF-2, 5 μg/mL insulin, and 5% human serum, in a 37°C/5% CO2 incubator. The medium was changed thrice during 2 weeks of P0 culture. Then, the cells were treated with TrypLE Select, collected cells were seeded in 175 cm2 gelatin-coated cell culture flasks at a density of 1.5 × 105 cells/cm2, and cultured in the same conditions as described above. The medium was changed five times during 3 weeks of P1 culture. For the culture of human dermal fibroblasts, the cells were expanded in the same medium as that used for chondrocytes.
Fabrication of tissue-engineered cartilage
PLLA porous scaffolds were purchased from GC R&D Center (Tokyo, Japan). The molecular weight of PLLA was around 85,000–115,000. Compressive strength of the scaffolds was more than 0.1 MPa and average porosity was 85–91%. To make tissue-engineered cartilage, the cells were suspended in 1% atelocollagen gel, which was diluted from the original 3% atelocollagen gel (Koken Co., Ltd.) with DMEM/F12, and then the cell suspension was applied to a 3 × 6 × 50 mm PLLA scaffold (3.5 × 107 cells/700 μL). Since some constructs with poor maturation of cartilage were needed for comparison, we prepared four types of constructs that differed in the ratio of chondrocytes to total cells: Group 1, 100% chondrocytes; Group 2, 10% chondrocytes and 90% fibroblasts; Group 3, 1% chondrocytes and 99% fibroblasts; and Group 4, 100% fibroblasts.
Transplantation of tissue-engineered cartilage and analysis with noninvasive modalities
Athymic nude rats (44/NJcl-rnu/rnu, male, 8 weeks) were anesthetized by intraperitoneal injection of sodium pentobarbital (50 mg/kg). An incision was made in the lower back, and each construct was inserted subcutaneously (n = 6 for each group). Eight weeks after the operation, anesthesia was conducted with intraperitoneal injection of a mixture of ketamine (87 mg/kg), xylazine (13 mg/kg), and 0.05 mL atropine. Under 1–5% isoflurane in air, the rats underwent MRI, X-ray, and ultrasound.
Magnetic resonance imaging
Quantitative MRI experiments were performed using a 2.0-T Biospec 20/30 System with a B-GA20 Gradient System (Bruker, Karlsruhe, Germany) with a maximum gradient strength of 100 mT/m. A 72-mm inner diameter birdcage coil tuned to 85 MHz for proton resonance was used for all measurements. MRI data acquisition and reconstruction were performed using the ParaVision (Bruker) software system. The parameters included longitudinal (T1) and T2 relaxation time and ADC. A T1 map was calculated from the images obtained using a short echo time (TE) spin-echo sequence with different repetition time (TR) values (saturation recovery method). The imaging parameters of the T1-map were TR: 5000, 3000, 1000, 500, 200, 100, and 50 ms and TE: 15 ms. A T2 map was calculated from the images obtained using a long-TR spin-echo sequence with different TE values (multi echo method). The imaging parameters of the T2 map were TR: 5000 ms and TE: 30–450 ms (15 ms intervals). An ADC map was calculated from the images obtained using diffusion weighted imaging with conventional spin-echo (SE-DWI) method. The imaging parameters of the ADC map were TR: 5000 ms, TE: 45 ms, diffusion gradient strength: 0, 24.6, 42.7, 67.5, and 77.9 mT/m, diffusion gradient interval (Δ): 19.5 ms, diffusion gradient duration (δ): 14 ms, and b-values: 0, 100, 300, 750, and 1000 s/mm2. All sequences were performed with a field of view (FOV) of 105 × 105 mm2, matrix size 256 × 256, and slice thickness 5 mm. Relaxation time (T1 and T2) and ADC were calculated as the average of the specimen from the obtained T1, T2, and ADC maps. All MRI measurements were carried out with no contrast agent and at room temperature (23°C).
X-ray measurement
Since X-ray from W tubes causes beam hardening due to its broadened spectrum, we employed the 17.5 keV characteristic X-ray from a Mo tube, which is normally used for mammography, to improve the accuracy of measurement of thickness. The X-ray system was specifically arranged for the inspection of cartilage and soft tissue, consisting of a 10 μm focus Mo tube (I-0301; Softex Co., Ltd., Ebina, Japan) and a 100 μm pixel flat panel detector (C7942CA-02; Hamamatsu Photonics K.K., Hamamatsu, Japan). The Mo tube was operated at 40 kV, 120 μA. The magnification factors were 2.63. X-ray transmission through tissue-engineered cartilage in rats was projected on the detector. The longitudinal axis of the sample within the extended skin was placed parallel to the detector surface to measure the X-ray attenuation along the lateral axis. X-ray attenuation due to the skin was cancelled by measuring a region away from the embedded sample.
Ultrasound
The speed of sound (SOS) was measured noninvasively on the basis of geometrical measurements using an MRI system and an ultrasound diagnostic device. 7
First, the thickness of tissue-engineered cartilage was calculated on the MR images using the full width at half maximum of the high-contrast region. Next, ultrasound images (USIs) of the same position were acquired using an ultrasound diagnostic device (EUB-8500; Hitachi, Tokyo, Japan) with a center frequency of 13 MHz. Then, the thickness of tissue-engineered cartilage in the USIs was determined by detection of the boundary of tissue-engineered cartilage. The thickness in the USI is generally determined by multiplying the time of flight (TOF) by a specific SOS (1530 m/s). Therefore, when the thickness obtained in the MR image equals the actual thickness, the SOS can be calculated as follows:
SOS = 1530 × thickness (MRI)/thickness (USI)
Macroscopic evaluation and biochemical analysis
After noninvasive measurement, including MRI, X-ray, and ultrasound, as described above, the constructs were excised from the body to measure the length, width, and thickness using an electronic ruler. Pictures of the constructs held with biceps were taken, and the volume of deflection was examined to evaluate the rigidity. Specific deflection was induced by dividing maximum deflection by the length of the constructs. Then, one third of them were cut into small pieces with scissors and suspended in 10 mg/mL pepsin and 0.05 M acetic acid. After digestion at 4°C for 48 h, 1 mg/mL pancreatic elastase, 0.1 mM Tris, 0.02 M NaCl, 5 mM CaCl2 (pH 7.8–8.0) were added, and the samples were kept at 4°C overnight. The samples were then centrifuged at 9100 g for 5 min, and the sGAG content in the supernatant was measured using an Alcian blue binding assay according to the manufacturer's instructions. 8 Also, centrifuged samples were subjected to enzyme-linked immunosorbent assay (ELISA) for type I and type II collagen. Measurements were performed thrice, and the mean values were used for statistical analysis.
Histological staining and immunohistochemical staining
The sections were stained with TB to detect proteoglycans, as well as with HE. 8 The area of metachromasia in TB staining was measured with a BZ-II analyzer planimetrically (Keyence Corporation, Osaka, Japan). The sections were also subjected to Elastica van Gieson staining to detect elastic fibers. Immunohistochemical staining for type I, II, and III collagen was conducted according to previous studies8,9 and the manufacturers' instructions.
Analysis of correlation
The average values of noninvasive modalities were calculated, respectively, and then the correlations between the average of each noninvasive modality and area of metachromasia, sGAG, COL1, and COL2 (ELISA) were evaluated using the coefficient of determination (R2).
Statistical analysis
Data are expressed as mean ± standard deviation. Statistical significance was evaluated using Bonferroni's multiple comparison tests. A value of p < 0.05 was considered to indicate statistical significance.
Results
Morphological changes of tissue-engineered cartilage
To explore noninvasive modalities that would reflect the maturation of tissue-engineered auricular cartilage, constructs with various degrees of cartilage maturation were compared. We mixed human auricular chondrocytes with human fibroblasts at a ratio of 100:0, 10:90, 1:99, and 0:100 when making tissue-engineered cartilage (Fig. 1). Eight weeks after transplantation in athymic rats, we measured the length, width, and thickness of the transplants and found that the 100:0 constructs maintained their original shape compared to the other three constructs (Fig. 2). When held with forceps, the 100:0 constructs showed greatest rigidity and specific deflection, which was induced by calculating the volume of deflection per length, was significantly smaller in the 100:0 constructs (Fig. 2).
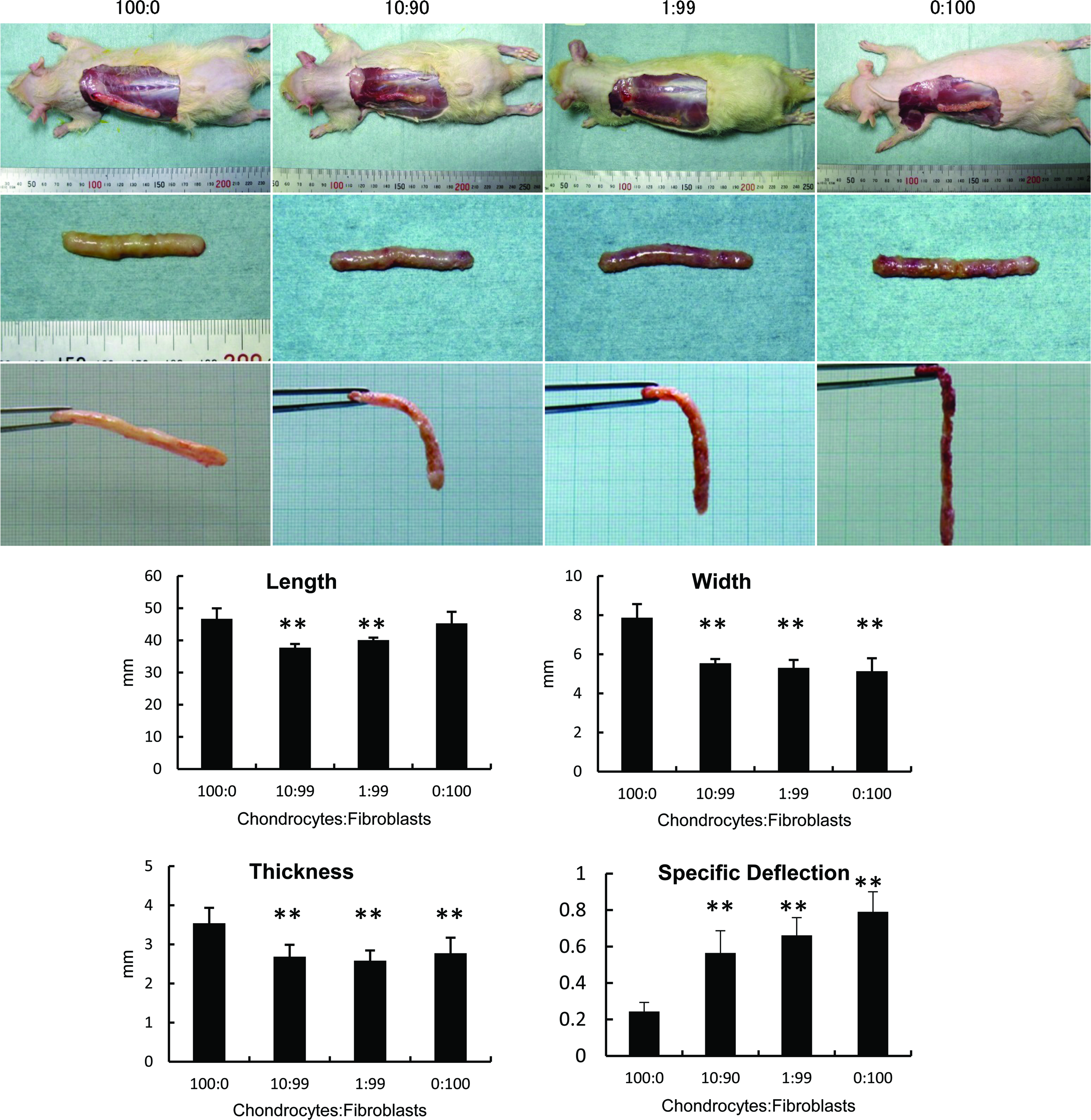
Morphological features of tissue-engineered cartilage. Eight weeks after transplantation of tissue-engineered cartilage, the constructs were excised from the rats (upper and middle photos). The constructs were held with forceps to examine their rigidity (bottom photos). The length, width, and thickness of the constructs and specific deflection were measured. The 100:0 constructs maintained their original shape compared to the other three constructs. 100:0, 10:90, 1:99, and 0:100 represent the ratio of chondrocytes to fibroblasts contained in the transplanted constructs. Data are expressed as mean (bars) ± SD (error bars). **p < 0.01 versus 100:0. SD, standard deviation. Color images available online at
Histological and biochemical analysis of tissue-engineered cartilage
After examination with MRI, X-ray, and ultrasound in vivo at 8 weeks, the tissue-engineered cartilage was excised from the rats for histological and biochemical analysis. Regarding the histological findings, the 100:0 constructs showed distinct metachromasia in TB staining, suggesting the accumulation of cartilage matrix. While the 10:90 constructs demonstrated sparse metachromasia, the other two constructs did not show any cartilage formation (Fig. 3A, D). HE staining also showed mature cartilage in the 100:0 constructs, while fibrous tissues were prominent in other constructs (Fig. 3B). In immunohistochemical staining of the 100:0 constructs, distinct expression of type II collagen was noted, although type I and III collagen were not so apparent. Also, localization of elastic fibers was shown in Elastica van Gieson staining (Fig. 3C), demonstrating the maturation of elastic cartilage in the 100:0 constructs. Meanwhile, in biochemical analysis, including the measurement of sGAG content and ELISA for type II collagen (COL2), the 100:0 constructs showed the significantly highest values, suggesting increased maturation of the tissue-engineered auricular cartilage. On the other hand, the level of type I collagen (COL1) did not significantly differ among the groups (Fig. 3E).
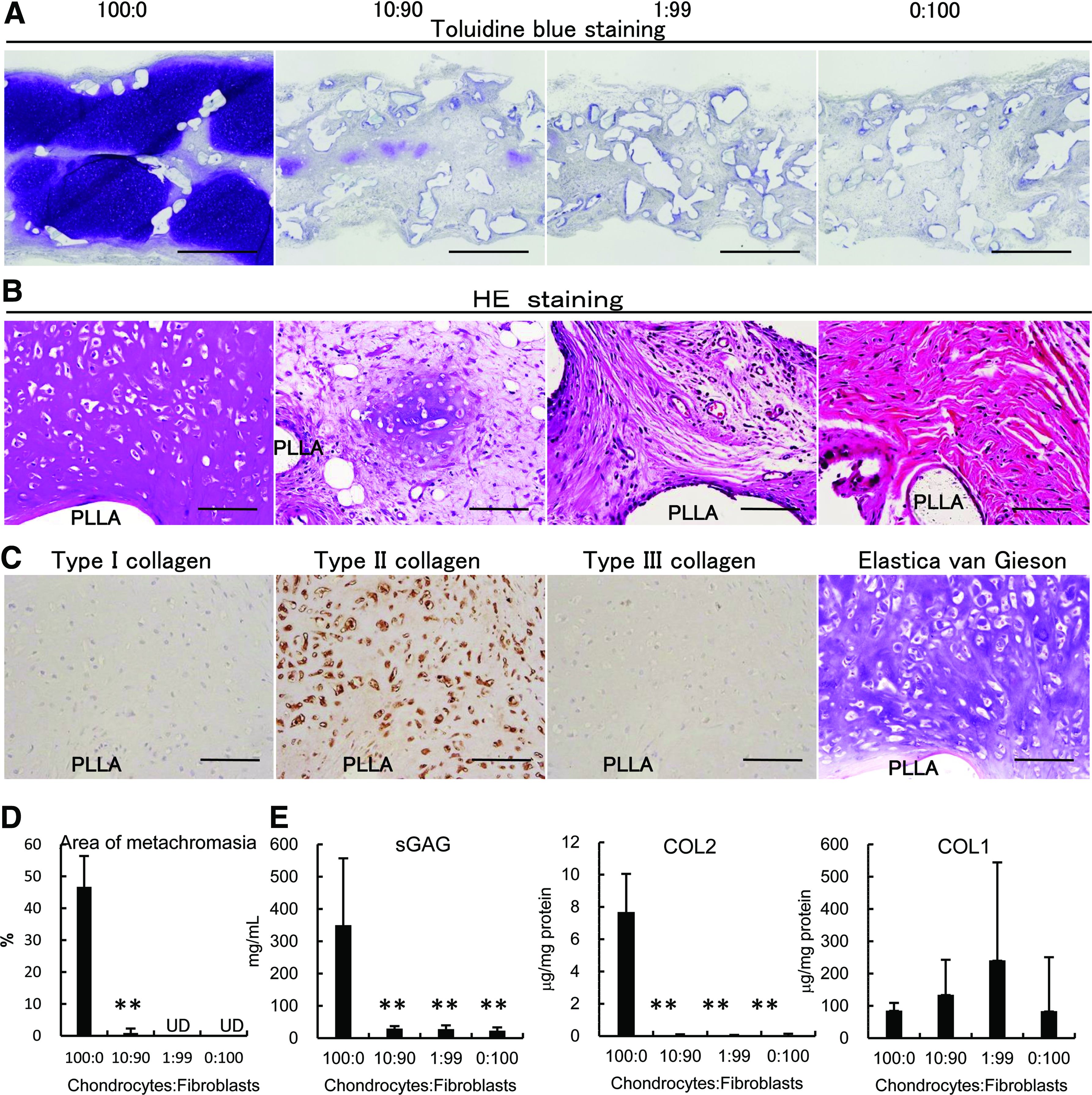
Histological and biochemical analysis of tissue-engineered cartilage. Eight weeks after transplantation, the constructs were analyzed histologically and biochemically.
Correlation of results of noninvasive modalities with histological and biochemical analysis
We examined MRI (T1, T2 and ADC), X-ray, and ultrasound as candidate modalities to detect auricular cartilage maturation noninvasively (Fig. 4). Since metachromasia in TB staining and high values of sGAG and COL2 are considered to reflect cartilage maturation, we examined the correlation of these parameters with the results of the candidate modalities. In MRI-T2 and MRI-ADC, the values were highest in the 100:0 constructs compared with the other three groups, indicating the possibility that these modalities may be able to detect maturation of tissue-engineered auricular cartilage (Fig. 5A). Indeed, the correlation of MRI-T2 or MRI-ADC with the area of metachromasia in TB staining, sGAG, and COL2 was quite high, with coefficients of determination (R2) of more than 0.9 (Fig. 5B). Regarding COL1, which reflects tissue fibrosis, its correlation with MRI-T2 and MRI-ADC was low. Although MRI-T1 showed a similar rise and fall with MRI-ADC (Fig. 5C), it showed a lower correlation with the area of metachromasia in TB staining, sGAG, and COL2. Meanwhile, the X-ray did not show any tendency to reflect the maturation of tissue-engineered auricular cartilage (Fig. 5D) and did not show a high R2 with histological and biochemical parameters. The values of ultrasound showed an inverse relation with those of MRI, and with the area of metachromasia in TB staining, sGAG, and COL2 (Fig. 5E). It was therefore suggested that MRI-T2 and MRI-ADC could be sensitive noninvasive modalities reflecting the maturation of tissue-engineered auricular cartilage.

Examination of tissue-engineered cartilage by noninvasive modalities. Eight weeks after transplantation, the constructs were examined by MRI (T1, T2, and ADC), X-ray, and ultrasound.
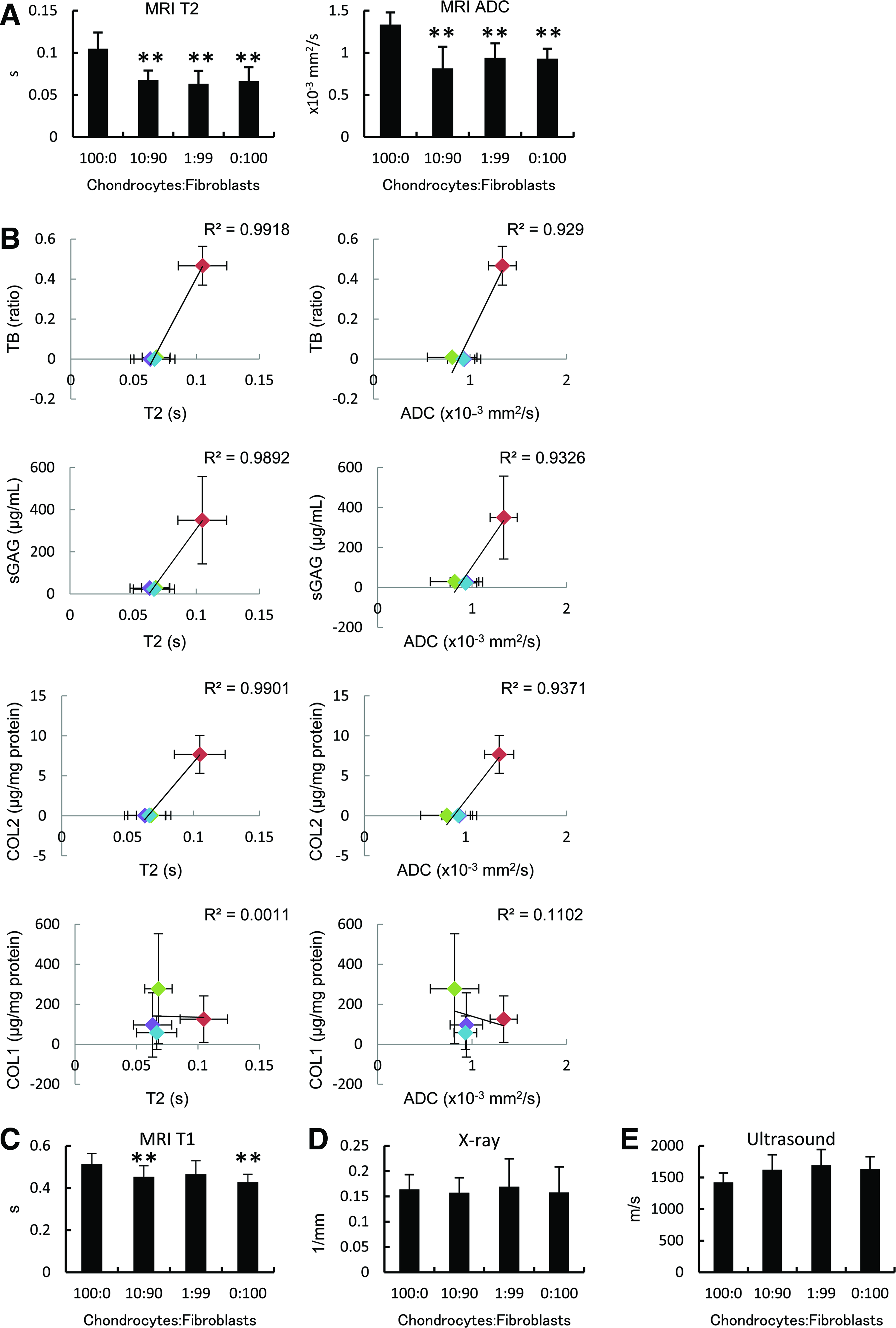
Correlation of results of noninvasive modalities with data of histological and biochemical analysis of tissue-engineered cartilage. Eight weeks after transplantation, the constructs were examined by MRI (T1, T2, and ADC), X-ray, and ultrasound.
Discussion
MRI is advancing as a tool for assessing the development of engineered tissues, since it has great potential to evaluate the biophysical and biochemical properties of engineered tissue noninvasively. 10 The application of MRI for assessing cartilage in joints has been established clinically, 11 and quantitative MRI-based analysis of cartilage morphometric measurements is regarded to be noninvasive, accurate and precise, and displays high potential diagnostic value in OA. 11 Recently, it has been considered that identifying the structure of cartilage by MRI could be an important step in assessing chondrogenesis. 12 Othman et al. compared normal articular cartilage and safranin O-stained histological sections and demonstrated that MRI images showed a high correlation with the corresponding histological images, 13 suggesting the feasibility of MRI for monitoring cartilage matrix in human subjects and tissue-engineered cartilage. When it comes to monitoring tissue-engineered cartilage in vitro, there have been several studies monitoring cell growth and tissue development with MRI.14,15 In one study, 15 chondrocytes of chick embryo sternum were inoculated into an MRI-compatible bioreactor, and the tissue formed over a period of 2–4 weeks was examined biochemically, histologically, and with MRI. They demonstrated that T1 and T2 correlated well with GAG and collagen concentrations in the matrix, as well as with tissue hydration, while ADC correlated with tissue hydration. They concluded that MRI could be a promising modality for assessing biochemical properties of cartilage. In another study, autologous chondrocytes in alginate scaffolds were transplanted into a focal patellar cartilage defect in rats, and the patellar cartilage was examined ex vivo after a certain period of time. 16 They found that T2 values from MRI images could discriminate different types of neocartilage, which were confirmed by histological analysis. Although most of these researches targeted hyaline cartilage in joints, we speculated that the modalities used to assess joint cartilage could be applicable to elastic cartilage transplanted subcutaneously, because the composition of these types of cartilage does not differ so widely. Indeed, in a study by another group, auricular chondrocytes were expanded and injection transplanted into a patient's lower abdomen to create tissue for nasal/chin reconstruction. 17 The transplants regenerated into larger chondrofat composite tissue in 6 months, which was clearly depicted with MRI T1. Meanwhile, in this study, T1, T2, and ADC showed a good correlation with histological and biochemical parameters of tissue-engineered cartilage based on a biodegradable scaffold. Especially, T2 and ADC showed a high coefficient of more than 0.9. Recently, there have been an increasing number of parameters of MRI, and imaging of tissues could vary depending on the choice of parameters. In general, T2 is considered to be sensitive to tissue hydration, collagen content, and collagen orientation against the main magnetic field,14,18 while ADC is particularly sensitive to macromolecular content and hydration. 19 The production of cartilage matrix in tissue-engineered cartilage was increased after 2 weeks and was almost complete by 8 weeks. Since the coefficients of T2 and ADC with histological and biochemical parameters were around 0.5 at 2 weeks (data not shown), it was suggested that these parameters may not be sufficiently sensitive to detect the initial increase of cartilage matrix at around 2 weeks.
Ultrasonography is an ultrasound-based diagnostic imaging technique, which is used for visualizing tendons, muscles, joints, vessels, and internal organs. Compared to other modalities, ultrasound may have several advantages as it can generate images in real time and does not emit harmful radiation. Although there has been a report indicating a good correlation between ultrasound and MRI measurements of the thickness and erosion of cartilage in joints, 20 our results showed that ultrasound measurements had an inverse relation with MRI parameters and biochemical and histological results. This is possibly due to the remnants of PLLA scaffold affecting the ultrasound measurement, and so we consider that ultrasound may not be suitable for the evaluation of tissue-engineered cartilage containing a biodegradable polymer scaffold.
The values of T2 and ADC in this study may be used for deciding the threshold of success/failure in the transplantation of tissue-engineered cartilage. Based on the histological and biochemical data in this study, we can regard the 100:0 construct as the success group, while the other three groups, including the 10:90, 1:99, and 0:100 constructs, as failure groups. The average values of T2 and ADC in all the failure groups were 0.066 s and 0.89 × 10−3 mm2/s, respectively, which may serve as the failure reference in clinical settings as well. Although the values may fluctuate depending on the machine or scan conditions, we consider that these measurement errors can be adjusted by including a certain phantom during the MRI scan and inducing correction factors.
Conclusion
In this study, we examined several noninvasive modalities that may reflect the maturation of tissue-engineered auricular cartilage transplanted subcutaneously. By calculating the correlation of the values of these modalities with histological and biochemical parameters, we found that T2 and ADC on MRI could be the most precise modalities for evaluation of tissue-engineered cartilage based on a biodegradable polymer scaffold. Since these noninvasive modalities would realize time-course analysis of the maturation of tissue-engineered auricular cartilage, the obtained data with these modalities would provide substantial insights to improve the quality of tissue-engineered cartilage in the head and neck region. Our results and interpretation could be applicable to other tissue-engineered cartilage applied in various areas, including the nose, ear, and joints in future, leading to the development of cartilage regenerative medicine.
Footnotes
Acknowledgments
We are grateful to Tomoaki Sakamoto and Makoto Watanabe for their technical assistance. This work was supported by a Health Labour Science Research Grant from the Ministry of Health, Labour and Welfare (Japan).
Disclosure Statement
No competing financial interests exist.