
Abstract
Introduction:
Cell-based therapies are becoming a valuable tool to treat osteoarthritis (OA). This study investigated and compared the regenerative potential of bone marrow concentrate (BMC) and mesenchymal stem cells (MSC), both engineered with Hyaff®-11 (HA) for OA treatment in a sheep model.
Methods:
OA was induced via unilateral medial meniscectomy. Bone marrow was aspirated from the iliac crest, followed by concentration processes or cell isolation and expansion to obtain BMC and MSC, respectively. Treatments consisted of autologous BMC and MSC seeded onto HA. The regenerative potential of bone, cartilage, menisci, and synovia was monitored using macroscopy, histology, immunohistochemistry, and micro-computed tomography at 12 weeks post-op. Data were analyzed using the general linear model with adjusted Sidak's multiple comparison and Spearman's tests.
Results:
BMC-HA treatment showed a greater repair ability in inhibiting OA progression compared to MSC-HA, leading to a reduction of inflammation in cartilage, meniscus, and synovium. Indeed, the decrease of inflammation positively contributed to counteract the progression of fibrotic and hypertrophic processes, known to be involved in tissue failure. Moreover, the treatment with BMC-HA showed the best results in allowing meniscus regeneration. Minor healing effects were noticed at bone level for both cell strategies; however, a downregulation of subchondral bone thickness (Cs.Th) was found in both cell treatments compared to the OA group in the femur.
Conclusion:
The transplantation of BMC-HA provided the best effects in supporting regenerative processes in cartilage, meniscus, and synovium and at less extent in bone. On the whole, both MSC and BMC combined with HA reduced inflammation and contributed to switch off fibrotic and hypertrophic processes. The observed regenerative potential by BMC-HA on meniscus could open new perspectives, suggesting its use not only for OA care but also for the treatment of meniscal lesions, even if further analyses are necessary to confirm its healing potential at long-term follow-up.
Introduction
T
Successful therapeutic effects of the bone marrow transplantation have been reported in some musculoskeletal diseases, such as the osteonecrosis of the femoral head, fracture nonunions, and lately in OA.17–21 Some authors argue that the therapeutic potential of BMC is due to its constitutive mononuclear cell population that enables the tissue regeneration through the secretion of growth factors that would modulate the heterogeneous population in the niche.22,23 Nevertheless, a full knowledge of the role of BMC for OA treatment is still scarce due to the complexity of this biological system. Our working hypothesis was to study the regenerative potential of BMC engineered with Hyaff®-11 (HA), a hyaluronan-based scaffold widely studied by our group,24–26 in counteracting OA via cartilage and meniscus repair in an OA sheep model and comparing these results with expanded MSC. This is the first work that showed the greatest regenerative profile of BMC in enhancing cartilage healing and meniscus regeneration in OA setting by downmodulating some inflammatory, catabolic, and hypertrophic mediators involved in the onset and progression of this disease.
Materials and Methods
Ovine meniscectomy model and experimental design
All in vivo experiments were performed in accordance with the European and Italian Law on animal experimentation and the principles stated in the NIH Guide for the Care and Use of Laboratory Animals. The research protocol on animals was approved by the Ethical Committee of the Rizzoli Orthopedic Institute and then by the Italian Ministry of Health. Twenty adult female sheep (Bergamasca–Massese, aged 30 ± 5 years, 60 ± 10 kg b.w.) were housed in single boxes at controlled room temperature (RT) and relative humidity (RH) of 22°C ± 1°C and 50% ± 5% RH with controlled ventilation. Animals were fed with a standard pellet diet (Mucedola), clover, and water ad libitum. Animals were selected for uniformity of size, conformation, and absence of lameness. Radiological analysis was performed before the surgery to assess the general health status of the knee joint. After a quarantine period, animals underwent unilateral medial meniscectomy (MMX) to induce OA in the right knee under general anesthesia and aseptic conditions as already reported in the literature.27–29 Sheep were randomized into four groups as follows: untreated group at 12 weeks from MMX (OA) (n = 4), treatment with Hyaff®-11 (HA) (Anika Therapeutics) (n = 4), treatment with autologous MSC-HA (n = 6), and treatment with autologous BMC-HA (n = 6). During the postoperative period, antibiotic and analgesic therapies were performed as described in our previous study. 27 Sheep were allowed to fully weight bear and to move freely without any constraints. Animals were pharmacologically euthanized with the intravenous administration of 10 mL m-butamide, mebenzonium iodine, and tetracaine chloride (Tanax; Hoechst) under general anesthesia at 12 weeks post-op. Macroscopic, histological, immunohistochemical, and micro-computed tomography (micro-CT) analyses were carried out.
Bone marrow harvest: BMC preparation and MSC isolation
Bone marrow was harvested from both iliac crests in multiple sites into plastic syringes containing sodium heparin (1000 U/mL) through a 16-gauge bone marrow needle to perform BMC and MSC treatments. In the BMC group, ∼60 mL of bone marrow was collected and then concentrated into a cell separator device using the sterile and disposable IOR-G1 Kit (Novagenit) to yield 6 mL of BMC as described elsewhere.
30
Briefly, 54 mL of bone marrow aspirate was injected into the posterior portion of a closed device system and centrifuged at 3200 rpm for 12 min to allow the separation of plasma and red cells. Following cell concentration, this tube was placed on a dedicated system for ∼1 min to allow the resuspension of mononuclear cells. Once separated from the red cells, the BMC was recovered from the anterior chamber with a syringe. One milliliter of BMC was seeded in sterile conditions onto 2 × 2 cm2 HA scaffold and incubated for 30 min at RT before transplantation; the remaining part was used for in vitro studies. The concentration factor of BMC was calculated from the quotient of mononuclear cells in bone marrow aspirate and BMC. In the MSC group, isolation and culture of MSC from the bone marrow aspirate were performed as described elsewhere.
31
Cells were expanded in monolayer cultures for two passages using α-MEM (Sigma) supplemented with 15% FBS (Gibco; Invitrogen), 0.1 M glutamine, penicillin–streptomycin 10,000 U/mL and 10,000 μg/mL, respectively (Gibco), 50 mg/mL gentamycin (Biological Industries), and once a week 50 μg/mL
Autologous grafting procedure
Knee joints from HA, BMC, and MSC groups underwent the right knee arthrotomy to expose the trochlear groove and medial condyle of the distal femur at 12 weeks post-op.
HA meshes either unseeded or seeded with BMC and MSC were inserted on the cartilage surfaces of the tibial plateau without the need for any fixation due to their intrinsic adhesive properties. 33
Flexion and extension of the hind limb were carried out to check the stability of the constructs.
Gross morphological assessments
Both knee joints were aseptically opened through the same parapatellar incision used for surgeries. The anterior and posterior cruciate ligaments were dissected, and the femur and tibia were carefully separated. Macroscopic assessment of cartilage was carried out using the International Cartilage Repair Society (ICRS) grading based on the Outerbridge score of the anterior, middle, and posterior sections of the femur and tibial plateau. 34 This score has a range from 0 (within normal limits) to 4 (complete cartilage degradation). The presence of meniscal lesions in terms of fibrillations, tears, and measurements of the meniscal width and length was used to evaluate the effectiveness of treatments. The length was measured with a graduated ruler from the visible meniscosynovial junction in the anterior zone to the same junction posteriorly; the mediolateral width was measured from the peripheral edge of the medial meniscus to a line connecting approximately the anterior and posterior meniscus horns. Five measurements were performed on each specimen separately and independently by three investigators who were blinded to the treatment received by each animal (G.D., B.G., and F.S.).
Microtomographic analysis
The analysis was performed on both femoral condyles and tibial plateau harvested. Samples were scanned with the microtomograph system SkyScan 1176 (Bruker MicroCT) applying a voltage of 65 kV and a current of 385 μA. The nominal resolution was set at 35 μm pixel size. Reconstructions were performed using software NRecon (version 1.6.8.0; Bruker MicroCT) to obtain μCT sections maintaining the relative pixel size. Three-dimensional morphometric analysis was performed via CTAn software (version 1.13; Bruker MicroCT) defining two specific volumes of interest (VOIs): VOI1, related to the cortical subchondral bone, and VOI2, related to the epiphyseal trabecular bone. The following morphometric parameters were calculated: subchondral bone thickness (Cs.Th, mm) in VOI1 and bone volume fraction (BV/TV, %), trabecular thickness (Tb.Th, mm), trabecular separation (Tb.Sp, mm), and trabecular number (Tb.N, mm−1) in VOI2.
Histological assessments
Synovia from suprapatellar fold, menisci, tibial plateau, and femurs were fixed in 10% neutral buffered formalin and decalcified, when bone component was present before paraffin embedding, according to validated histological guidelines.35–37 Sections (5 μm) were stained with hematoxylin and eosin (Bioptica) and 0.04% toluidine blue/0.1% fast green (Sigma) to assess general morphology and proteoglycan content, respectively. Thirteen frontal osteochondral sections, spaced 20 sections apart, were graded for the level of severity with modified Mankin score on the entire slide using a scale from 0 (normal) to 25 (severe OA) for the following parameters: cartilage structure, chondrocyte density, cell cloning, proteoglycan content, and tidemark integrity.36,37 Seven sagittal sections from the synovial membrane, spaced 20 sections apart, were graded on the entire slide using modified Smith score on a scale from 0 (normal) to 12 (severe OA) for the following parameters: intimal hyperplasia, inflammatory cell infiltration, subintimal fibrosis, and vascularity.35,37 Anterior and posterior thirds of each meniscus were trimmed to obtain vertical sections. Ten sections, spaced 20 sections apart, were graded using a modified Pauli scoring system on a scale from 0 (healthy meniscus) to 18 (OA meniscus) for surface, cellularity, matrix organization, and matrix staining with a modification of this last parameter that was inversely proportional to the original score.38–40 Histological assessments were performed on all the groups by three blinded researchers (G.D., B.G., and F.S.) with Eclipse 90i microscope (Nikon).
Immunohistochemical evaluations and image analysis
Protein expression of collagens I, II, and X, MMP-13, and IL-1β was assessed by immunohistochemistry on tissue slides. Antigen retrieval was performed on sections through enzymatic treatments with 0.1% (w/w) pronase (Sigma) in PBS for 20 min, followed by 2.5% (w/w) hyaluronidase (Sigma) in PBS for 30 min at 37°C for collagen assessments. All the sections were blocked with 2% bovine serum albumin in PBS for 30 min at RT. Samples were incubated at RT with mouse monoclonal antibodies, diluted in Trizma saline buffer with 0.1% Triton, to detect MMP-13 (R&D), IL-1β (AbD Serotec), type I and X collagens (Sigma), type II collagen, and MMP-13 (all from Chemicon). Biotinylated secondary anti-mouse antibody and alkaline-labeled streptavidin (Biocare Medical) were used. Histochemical detection was performed with Fast Red Substrate Kit (Biocare). Negative controls were performed by either omitting the primary antibodies or using isotype-matched controls. A semiquantitative analysis of the positive signals from tissue sections was executed by two blinded investigators (G.D. and I.B.) using hue/saturation/intensity to define a positivity threshold with NIS-Elements software and Eclipse 90i microscope (Nikon). Because all negative control pixels showed values ranging from 0 to <160, we set hue (H) thresholds for positive pixels at 160–255. Ranges of 0–255 were established as threshold values for saturation (S) and intensity (I). The percentage of positive cells and/or area for each marker was carried out on six random microscopic fields ( × 10 objective lens) for each tissue and reported as percentage of positive cells and/or area on a scale from 0 (no protein expression) to 100% (high protein expression).
Statistical analysis
Statistical analysis was carried out using Statistical Package for the Social Sciences software version 15.0 (SPSS, Inc.). Data were reported as mean ± standard deviation. The general linear model (GLM) with adjusted Sidak's multiple comparison test with group (OA, HA, MSC-HA, and BMC-HA) as fixed effects was used for the analyses of macroscopic, histological scores, immunohistochemistry, and micro-CT to compare the effectiveness of MSC-HA versus BMC-HA in OA setting. Nonparametric Spearman's test was used to test the correlation between cartilage scores and those ones from menisci and synovial membrane. p-Value <0.05 was statistically considered significant.
Results
HA did not affect cell viability and clonogenic potential in both cell treatments
The centrifugation-based point-of-care device concentrated mononuclear cells approximately eightfold over baseline. The number of nucleated cells counted within the BMC from our samples displayed a high variability ranging from 6.0 × 106 cells/mL to 53.0 × 106 cells/mL, with a mean value of 39.0 × 106 cells/mL. It would seem that the number of concentrated cells within BMC contributes to influence clinical results since we observed the lowest healing ability in the cases treated with the lowest number of nucleated cells. However, a larger number of animals are necessary to confirm these findings and provide statistical evidence apart from considering other critical aspects, including the growth factors released in the microenvironment. In general, BMC and MSC were viable onto HA at starting point and longer follow-up, with no signs of cell damages (data not shown). Both MSC and BMC displayed a clonogenic ability with the formation of different numbers of CFU colonies but without showing some relationships with the healing potential of both cell strategies (data not shown).
Regeneration of the medial meniscal tissue was more efficient following BMC-HA treatment
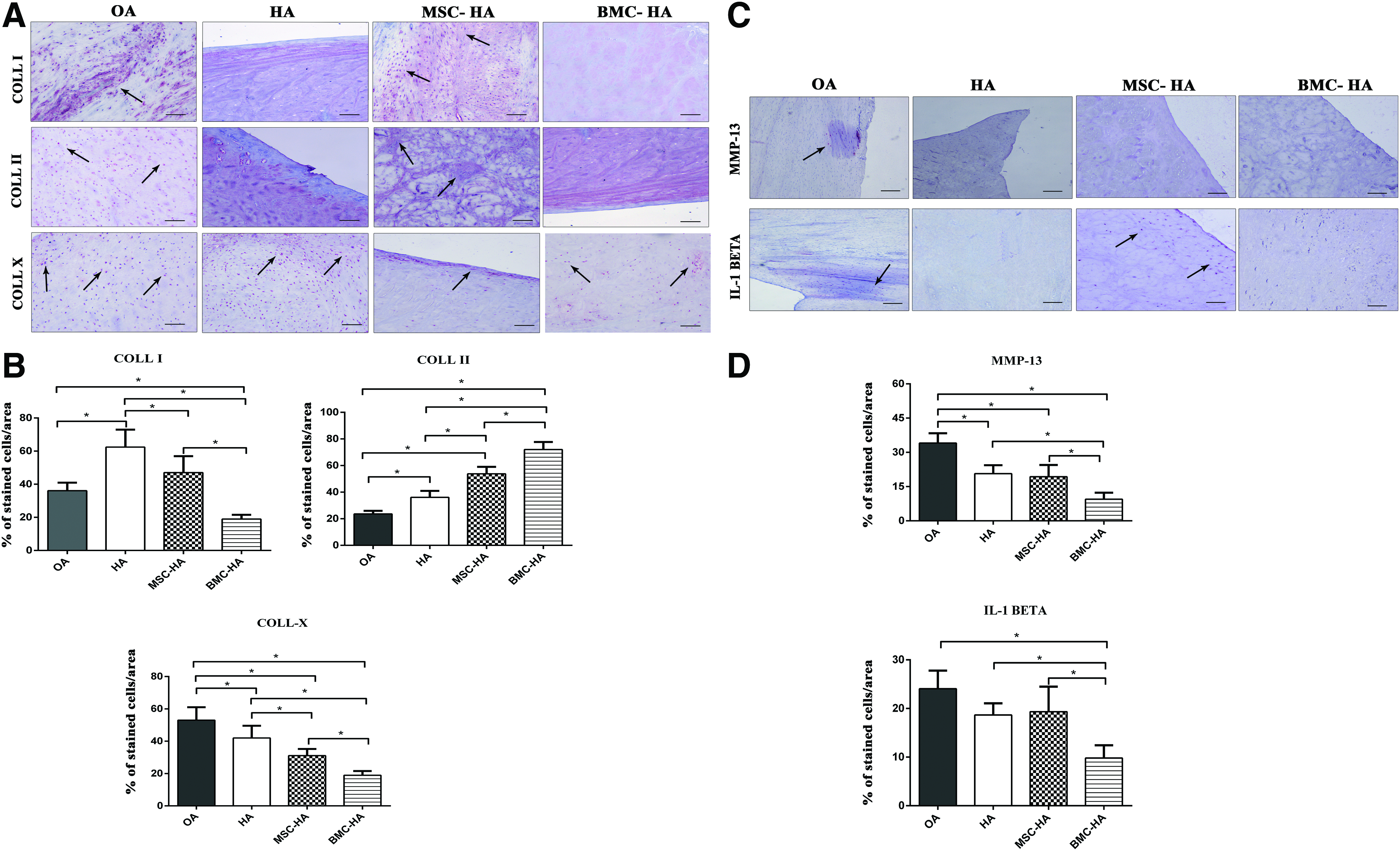
An intrinsic regenerative potential of the medial meniscus was noticed in the OA group through macroscopic assessment reporting an unorganized tissue with multiple tear patterns and the presence of various fibrillations. Conversely, a meniscus-like tissue was observed for the different treatments, especially following the therapy with BMC-HA; however, some vertical tears in the mid body were evident. Measurements on meniscus length did not give evidence of any significant differences between MSC-HA and BMC-HA, whereas some repair processes were noticed for meniscus width between the two treatments (p < 0.05) (Fig. 1A–C). In general, menisci from OA and HA groups histologically displayed a fibrous aspect, acellular areas, many tears, and a low proteoglycan content. Both cell therapies combined with HA were capable of supporting the regeneration of a good meniscal tissue reporting the lowest score in the posterior region (p < 0.05) (Fig. 2A, B). The presence of a meniscus-like structure was also noticed in the anterior region following BMC-HA treatment (p < 0.05). However, differences between the two cell treatments were noticeable only in the posterior region, where BMC-HA treatment showed more beneficial effects than MSC-HA (p < 0.05) (Fig. 2A, B). In general, the neo-formed meniscal tissues following both cell strategies displayed a regular smooth surface along the tibia and femoral sites, a good cell density with no or low cell clusters, and a good proteoglycan content in its inner body, especially in the posterior region (Fig. 2A). Both MSC-HA and BMC-HA therapies displayed a marked positivity for type I and II collagens compared to OA and HA groups at cellular and extracellular levels throughout the meniscus in the posterior region (p < 0.05). Moreover, the transplantation of BMC-HA showed a higher expression for type II collagen and lower expression for type I collagen compared to the MSC-HA group (p < 0.05). Low protein expression for type X collagen, MMP-13, and IL-1β was evident for both cell treatments compared to OA and HA groups at cellular level, especially in the posterior region (p < 0.05) (Fig. 3A, B). BMC-HA treatment showed lower positivity for MMP-13 and IL-1β compared to MSC-HA approach (Fig. 3A, B).

Regenerative potential of MSC-HA and BMC-HA in promoting the meniscus repair.
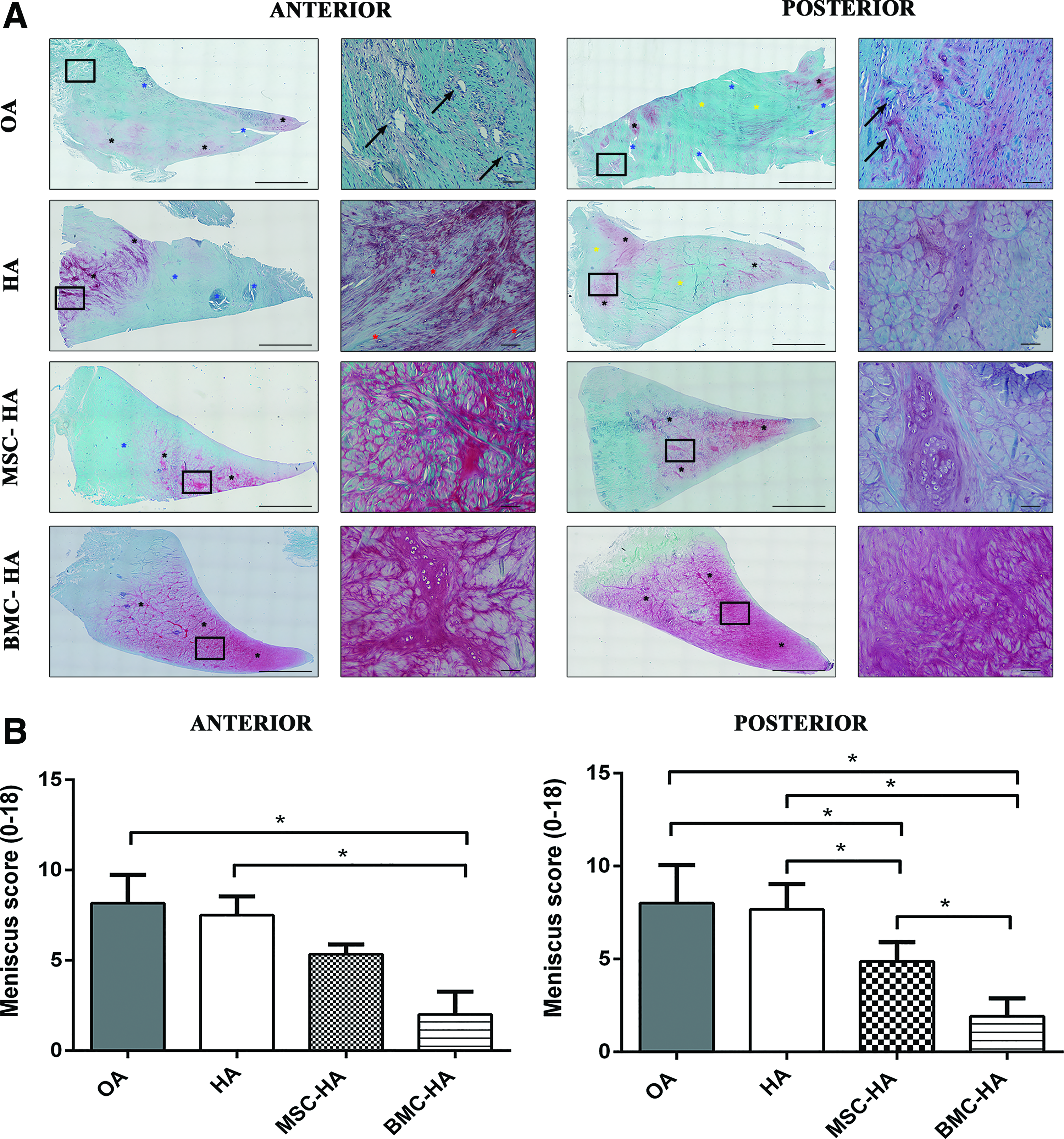
A reduction of degenerative processes in the medial meniscus was noticed, especially following BMC-HA treatment.
Various regenerative processes for meniscus repair were evident following both cell therapeutic strategies.
BMC-HA treatment was more chondroprotective than HA carrying MSC
Macroscopic analysis of cartilage surfaces of the femur and tibial plateau showed a positive contribution by both cell treatments in favoring cartilage repair mainly in the femur (Supplementary Fig. S1; Supplementary Data are available online at
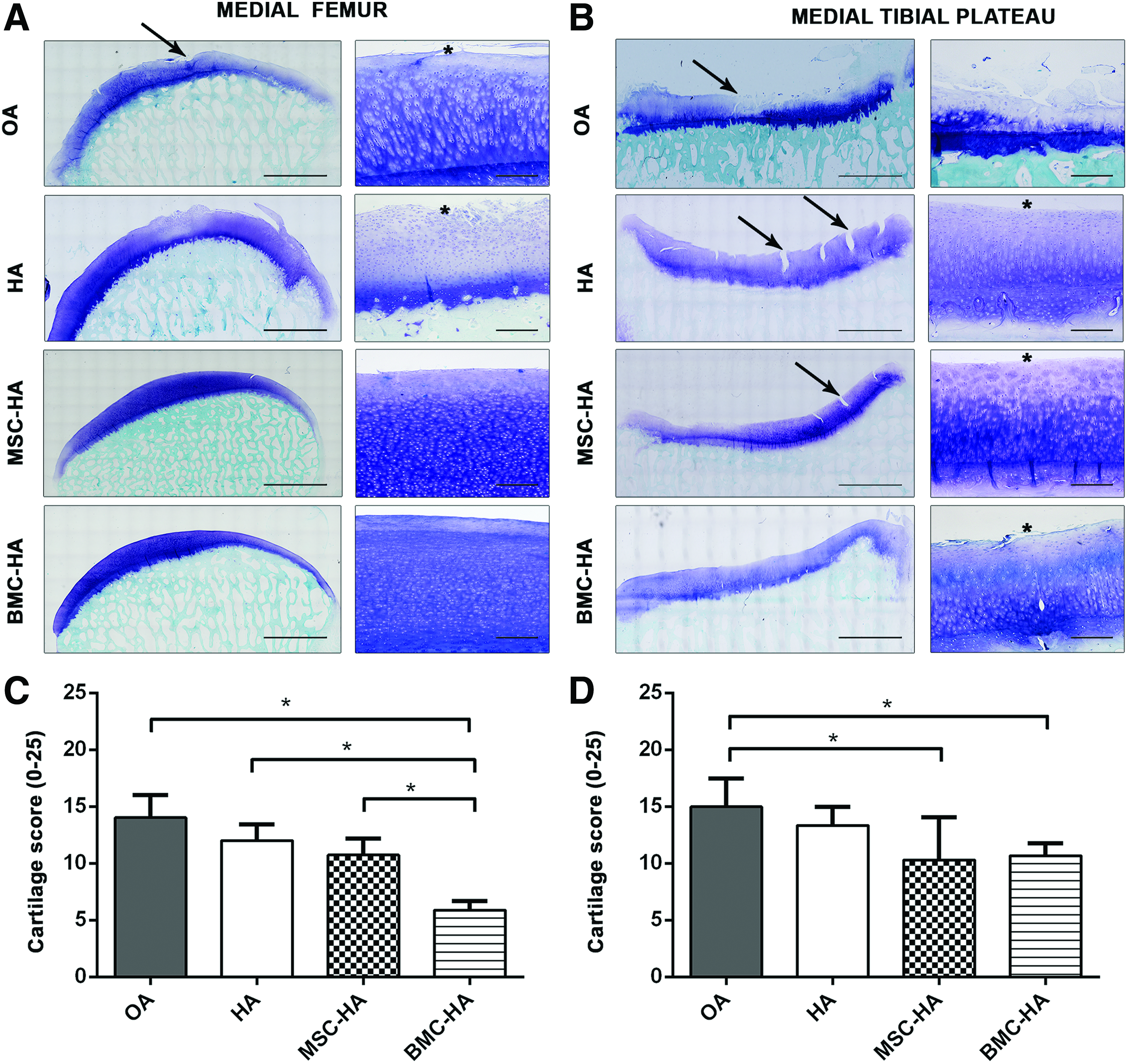
A marked reduction of cartilage damage was noticed following both cell treatments.
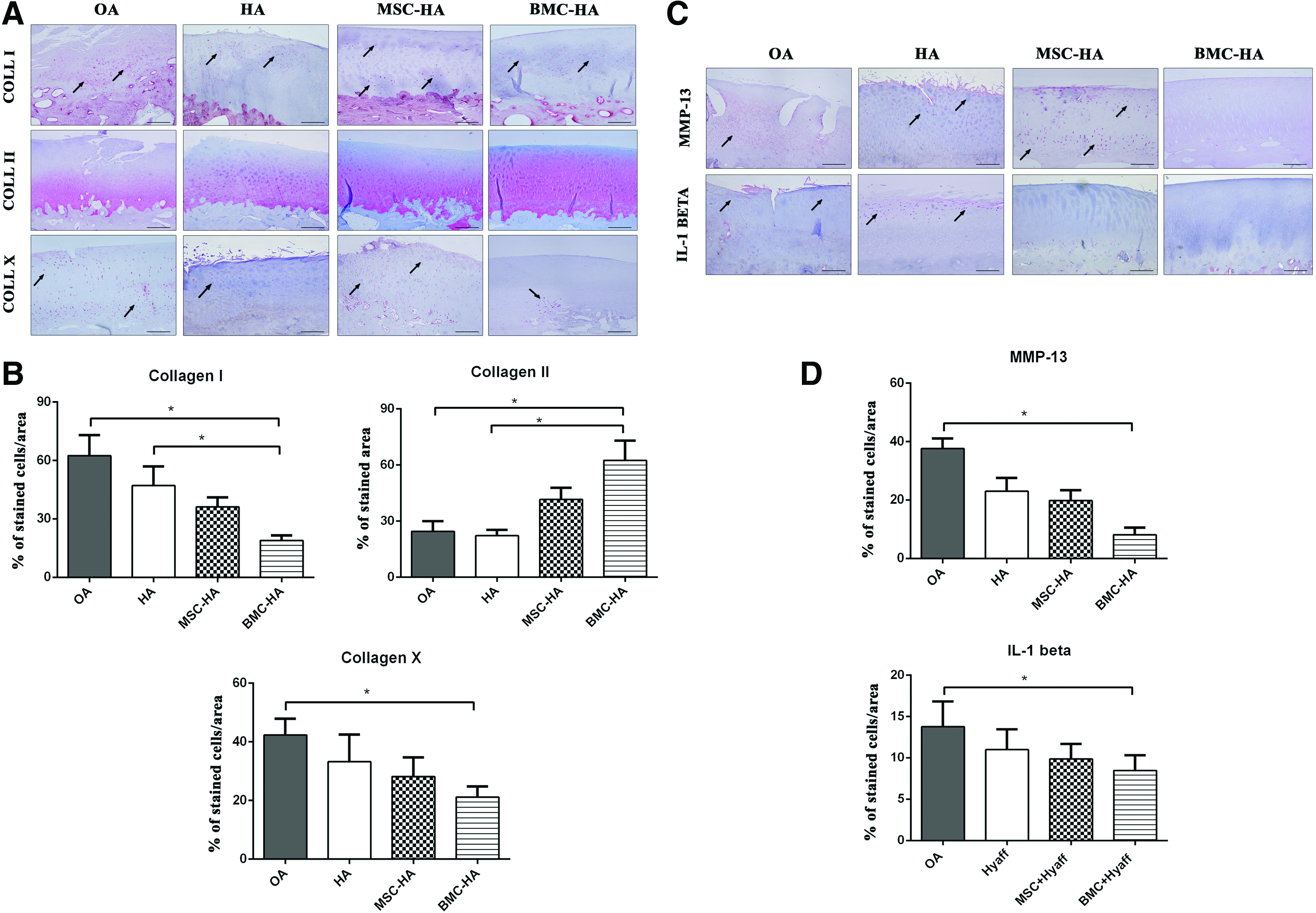
HA carrying BMC considerably led to a decrease of catabolic and inflammatory mediators in the cartilage tissue.
MSC-HA treatment showed the best repair potential in the synovial membrane
Hyperplasia processes, high vascular component, and presence of inflammatory cells were observed in the synovial membrane in the OA group. Some healing effects were evident following HA treatment in terms of the reduction of cell hyperplasia and inflammation. The MSC-HA group reported the lowest score for the synovial membrane, displaying a regular lining layer and a sublining containing mostly adipocytes with a low vascular component. The BMC-HA group displayed a less organized lining layer with some processes of angiogenesis within the sublining (Fig. 6A, B). A reduction of catabolic and inflammatory processes was observed following both cell therapies. In particular, a weak reduction of protein expression for MMP-13 and IL-1β was noticed in the fibroblast-like cells of the lining layer after HA treatment; however, such a process is strongly evident in the BMC-HA group (p < 0.05) (Fig. 6C, D). No significant differences were noticed between MSC and BMC treatments combined with HA. No correlation of the healing potential was noticed among the synovial membrane and cartilage and meniscus tissues in MSC-HA (ρ = 0.4, p = 0.4; ρ = 0.3, p = 0.4) and BMC-HA groups, respectively (ρ = 0.5, p = 0.3; ρ = 0.4, p = 0.4).

BMC-HA treatment displayed the strongest effects in downregulation of catabolic and inflammatory mediators in the synovial membrane.
Modulation of Cs.Th was evident following treatments
In the current study, we did not detect any changes for BV/TV, Tb.Th, Tb.N, and Tb.Sp. for all treated groups compared to OA. Micro-CT analysis showed the worst scenario in terms of subchondral bone thickness (Cs.Th) in the OA group in both medial femoral condyle (MFC) and MTP. A significant downregulation of Cs.Th was found in both cell treatments compared to the OA group in MFC (p < 0.05) and for all the treatments, including those ones with HA in MTP (p < 0.05) (Table 1). In general, both cell treatments contributed to modify cortical but not trabecular microarchitecture at 12 weeks post-op.
Data are reported as mean ± standard deviation. Adjusted Sidak's multiple comparison test: MSC-HA, BMC-HA, and HA versus OA.
p < 0.05.
BV/TV, bone volume fraction; BMC-HA, bone marrow concentrate–hyaluronan; Cs.Th, subchondral bone thickness; MFC, medial femoral condyle; MSC-HA, mesenchymal stem cells–hyaluronan; MTP, medial tibial plateau; OA, osteoarthritis; Tb.N, trabecular number; Tb.Sp, trabecular separation; Tb.Th, trabecular thickness.
Discussion
Despite the extensive research efforts in the field of OA, there is a largely unmet medical need for durable and minimally invasive disease-modifying treatments. 41 MSC have given promising results as therapeutic strategies in different musculoskeletal pathologies, including OA; however, their healing potential is dependent on the isolation procedure and culture expansion, which affect their phenotype and clonogenic ability.11,42 Many scientists believe that a possible way of ameliorating the use of MSC can be achieved through the direct implantation of the entire bone marrow niche, thus avoiding culture-related changes.8,10 Indeed, the discovery of point-of-care systems capable of enriching the mononuclear cell fraction led to the development of a therapeutic approach based on the use of BMC, with a great focus in the orthopedic field,18,19,21,43,44 where the number of cells needed for tissue regeneration is often inadequate. However, few data are available on the role of BMC in a complex environment system, such as in the knee joint affected by OA.18–20,45 Thus, we decided to assess the regenerative potential of BMC in a sheep model of OA, where catabolic and inflammatory processes, mainly affecting the MTP, are evident and similar to human pathology. In particular, the main goals of this study were to find out whether BMC-HA was able to counteract OA allowing cartilage and meniscus repair and to compare its effects with the use of expanded MSC. Both cell types were seeded onto a hyaluronan-based scaffold, known as Hyaff®-11, already demonstrated to enhance cartilage repair thanks to its multiple activities for cell homeostasis.24,25,46,47 In previous in vitro studies, we demonstrated the chondrogenic potential of BMC and MSC under specific culture conditions and when combined with HA, thus supporting their use for the treatment of osteochondral defects.31,48
The repair potential of both cell strategies was evaluated considering their ability to inhibit the development/progression of degenerative and inflammatory processes and compared to an untreated OA group. Both BMC and MSC seeded onto HA did not lead to local inflammation and/or immobilization of the joint and strongly improved tissue morphology reducing catabolic processes in cartilage and meniscus, even if some remodeling processes using empty HA were also evident, as already demonstrated in a previous work. 26 In particular, BMC-HA was more efficient than MSC-HA treatment in inhibiting OA changes, targeting some of the most frequent drawbacks occurring during tissue repair, such as fibrosis and endochondral ossification. Indeed, the observed downregulation of fibrous and hypertrophic markers could guarantee a long-lasting stability, although further experiments with long-term follow-ups are necessary to confirm these findings. A common feature found in both cell strategies was the decrease of IL-1β, which is well known to drive many biological processes involved in joint destruction during OA. 49 We could speculate that their healing effects can be linked to IL-1ra, a cytokine inhibiting IL-1β activity reported by some authors to have a clinical significance in counteracting inflammation.13,50
Recently, the scientific interest toward meniscus regeneration is growing due to the new definition of OA as an organ joint disease. It is well known that meniscus has a poor regenerative capacity likewise cartilage; thus, the identification of therapeutic strategies, including the use of MSC from different sources, capable of improving its intrinsic healing potential could provide new insights in this field of research.51–53 In our study, the observed meniscus regeneration after both cell treatments contributed to render the knee joint relatively protected from an altered loading, thus avoiding OA progression. An intrinsic regenerative capacity was observed in the untreated OA group, in which the formation of an unorganized and fibrous tissue was observed being in agreement with the literature. 38 The observed low amount of IL-1β together with the low expression of collagen X and MMP-13, especially after BMC-HA treatment, would suggest to consider BMC as an alternative strategy for the treatment of meniscal lesions. Although BMC-HA treatment showed the best findings already at 12 weeks post-op, some aspects mirroring an early stage of tissue maturation were found. It has been demonstrated by some authors that growth factors play a crucial role in enhancing meniscal regeneration; thus, we could speculate that the growth factor cocktail released by BMC could be involved in the repair processes we observed in meniscus as already seen by other authors for platelet-rich plasma. 54
To properly consider what are the biological processes during cartilage and meniscal repair, we considered also the role of the synovial membrane and bone tissue. Our findings demonstrated that both cell strategies were able to enhance healing processes in the synovial membrane, reestablishing tissue architecture and leading to a downregulation of IL-1β. Thereby, we could speculate that the decreased expression of IL-1β could be due to a reduced presence of M1 macrophage subset population in the synovial membrane, responsible for an inflammatory phenotype. This process might be driven by the combination of cells with HA since some authors recently showed how this molecule is able to modulate macrophage phenotype. 55
In general, BMC-HA treatment showed many angiogenesis processes in synovium, likely due to the presence of the endothelial cells within BMC. It is not too clear what are really the effects of blood vessels in tissue repair, whether they are only inflammatory parameters or they are good indicators since they contain pericytes expressing MSC markers as reported by Caplan. 56 Besides the benefits of BMC on articular tissues, no effects were detected for the examined bone parameters, except for Cs.Th. Both MSC and BMC treatments were able to downregulate Cs.Th in the femur and tibial plateau, although some remodeling processes were also evident with the use of the empty scaffold. Indeed, the beneficial effects observed in cartilage, meniscus, and synovium had a great impact in maintaining the homeostatic equilibrium of bone. Nevertheless, the few signs of regenerative processes observed in the cortical but not in trabecular bone microarchitecture could derive from its late repair process. Limitations of this study include those related to (1) the difficulty in the standardization of the number of cells within BMC, (2) the lack of studies on local cytokine production, and (3) the lack of studies on tissue biomechanics.
In conclusion, findings from this work portray a picture of a higher regenerative potential of BMC-HA compared to MSC-HA in reestablishing the impaired homeostasis in cartilage, meniscus, and synovium and simultaneously opening new insights on its possible use for the treatment of meniscal lesions.
Footnotes
Acknowledgments
The authors make particular mention of the late Professor Andrea Facchini, an eminent scientist with a great love of science. We also thank Dr. Elettra Pignotti for statistical evaluation and Patrizia Rappini for her assistance in the preparation of the article. This work was supported by grants from the Italian Ministry for Health.
Disclosure Statement
Dr. B.G. declares conflict of interest because she is one of the inventors of the European Patent Granted No. EP 2 129 384 “Composition containing a medullary concentrate supported by a scaffold” in the name of Istituto Ortopedico Rizzoli, Bologna, and licensed to Novagenit, Mezzolombardo (Trento), Italy. Other authors declare they have no competing interests.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.