
Abstract
Liver tissue obtained from partial hepatectomy is a common source for isolation of primary human hepatocytes. Until now, liver resections were most commonly performed by conventional open surgery. Although the laparoscopic approach is currently emerging in liver surgery, data on the outcome of hepatocyte isolation from laparoscopically resected liver tissue are not available. A total of 22 hepatocyte isolations were performed using the two-step collagenase perfusion technique from October 2015 to March 2016. Liver tissue was obtained from n = 15 open liver resections (OLRs) and n = 7 laparoscopic liver resections (LLRs). Isolation parameters (cell yield, viability, and Percoll survival) were assessed and hepatocyte function (plating efficiency, urea, albumin, and aspartate aminotransferase) was measured over a culture period of 6 days (OLR: n = 13; LLR: n = 3). Total cell yield (OLR: 36.81 ± 6.77 × 106 cells/g vs. LLR 16.84 ± 10.66 × 106 cells/g, p = 0.0318) as well as viable yield (OLR 31.70 ± 6.05 × 106 cells/g vs. LLR 14.70 ± 9.89 × 106 cells/g, p = 0.0260) was significantly higher in the OLR group. Subgroup analysis revealed that the worse outcome of isolation of laparoscopically resected liver tissue was associated with right-lateral LLRs, whereas hepatocyte isolation from left-lateral LLRs was as effective as from open surgery. Hepatocyte function did not differ between hepatocytes from openly resected versus left-lateral laparoscopically resected liver tissue. We here present the first data on hepatocyte isolation from laparoscopic liver surgery. Although the overall outcome is worse compared with open surgery, our data suggest that liver tissue from laparoscopic resection of the left lobe is an excellent source for primary human hepatocytes.
Introduction
H
Even though stem cell research is generating promising results with regard to genetically engineered hepatic cells,15–17 primary human hepatocytes still remain the gold standard for the applications mentioned before. 18 Still, the lack of donor tissue suitable for hepatocyte isolation makes it difficult to meet the needs for hepatocytes, mainly for in vitro studies. Hence, there is a constant need for hepatocytes, which urges laboratories to maximize the efficiency of the isolation process. Given that the isolation of human hepatocytes is a very time-consuming and expensive process, it is crucial to assess whether a particular liver specimen is worth the efforts of the isolation procedure so that any potential source of liver cells is effectively utilized.
Specimens obtained from liver resections are the most common source for isolation of primary human hepatocytes. Liver tissue for hepatocyte isolation can be retrieved from most major liver resections, 19 in which healthy tissue has to be resected during surgery due to anatomical reasons. Until now, the conventional open surgical approach has been the gold standard for liver resections. However, minimally invasive, laparoscopic surgery is emerging as the preferential surgical approach in certain cases due to less postoperative pain, less morbidity, easier subsequent surgery, and better cosmetic results than open surgery.20,21
In liver surgery, the laparoscopic approach differs from open surgery in a few aspects: The abdomen is accessed by small incisions through trocars instead of opening up the abdomen. The abdominal cavity is inflated with CO2 to enable the surgeon appropriate range of movements and good visibility, whereas in open surgery the abdominal organs are directly accessible. Thus, laparoscopic procedures are performed at 37°C in the patient's abdominal cavity, whereas the abdomen is widely opened in the conventional open surgery and, therefore, surrounding of the liver specimen is cooler.
Despite this surgical evolution, literature on hepatocyte isolation from laparoscopically resected liver tissue is currently not available. Here, we present the first results of hepatocyte isolation from a specimen obtained from laparoscopic partial liver resection and compared the results with those of conventional surgery.
Patients and Methods
Design of the study
The study was conducted at the Department of Surgery, Campus Charité Mitte and Campus Virchow-Klinikum, Charité—Universitätsmedizin Berlin. All experiments were performed with the informed consent of the patients and following the institutional and ethical guidelines (approval of the local ethics committee: EA2/137/09). Tissue samples were prospectively collected from 22 patients undergoing partial hepatectomy between October 2015 and March 2016. Patients were retrospectively grouped either to the open liver resection (OLR) or to the laparoscopic liver resection (LLR) group. The surgical approach had been chosen by the operating surgeons in consideration of the anatomical situation and clinical characteristics of the patient. Exclusion criteria for tissue collection were infectious diseases such as viral hepatitis, multiresistant bacteria, or echinococcosis.
Liver resection
Partial hepatectomy (left-lateral: segments II+III; right-sided: segments V–VIII) was either performed openly through an L-shaped laparotomy or laparoscopically through three to four incisions for trocar placement.
After mobilization of the respective liver lobe and preparation of the liver hilum, the portal and arterial branch, the hepatic vein, and the bile duct of the segments to be resected were ligated and dissected. In OLR, the liver parenchyma was dissected by ultrasonic dissection using the Cavitron Ultrasonic Surgical Aspirator (CUSA; Tyco Healthcare). In LLR, a harmonic scalpel and vascular stapler were used for transection of the major intrahepatic vascular trunks. After completion of dissection, the resected liver segments were retrieved from the surgical site. In LLR, an additional removal incision or an extension of the subumbilical incision was made to remove the resected liver tissue with a special retrieval bag at the end of the procedure.
Tissue collection
The resected liver tissue was then immediately examined to identify the tumor-free areas. A tissue specimen was obtained from the tumor-free margin of the liver with only one cut side and the rest of the surface being covered by the Glisson's capsule. The mass of the tumor-free specimen that was used for hepatocyte isolation was 20.77 g on average (standard error of the mean [SEM]: ±3.3 g). The yield is normalized to the corresponding weight of the liver specimen.
The tissue specimen was stored in ice-cold Williams E-Medium and transferred immediately to the laboratory under sterile conditions. The hepatocyte isolation procedure was started within 30 min after retrieval of the tissue.
Hepatocyte isolation and culture
Hepatocyte isolation was performed under sterile conditions using an established two-step collagenase perfusion protocol. 22 In short, the major vessels of the liver specimen were cannulated with three to five cannulas and then flushed with prewarmed (37°C) perfusion solution (1.42 M NaCl, 67 mM KCl, and 100 mM 4-(2-hydroxyethyl)-1-piperazineethanesulfonic acid [all chemicals from Carl Roth GmbH]) supplemented with ethylene glycol tetraacetic acid (Serva) for 11.5 (±0.6) min. Afterwards, the tissue was perfused with 100 mL digestion solution containing 1 mg collagenase P per mL (Roche Diagnostics GmbH) at 37°C. Perfusion was stopped when the tissue was optically and tactically considered digested (mean digestion time: 8.5 ± 0.4 min).
The digested tissue was then transferred into a petri dish filled with perfusion solution without EGTA but containing 4% human albumin to stop the enzymatic activity. The cannulas were removed and the tissue was mechanically disrupted afterwards. After a first centrifugation (5 min, 50 g, 4°C) to eliminate cell debris, the cells were counted and viability was estimated through the trypan blue exclusion test. Density gradient centrifugation (25% Percoll [Biochrom GmbH] in phosphate-buffered saline) was then performed at 1474 g for 20 min (4°C).
Hepatocytes were seeded at a density of 1 million cells per well onto collagen-coated six-well plates (Biochrom GmbH) for cultivation. The cells were washed with PBS (37°C) 4 h after seeding to discard nonattaching cells. Cells were cultured with modified Williams medium E for 6 days (supplements: 1 μM insulin [Lilly], 1 μM Fortecortin [Merck Serono GmbH], 1 mM sodium pyruvate, 10 mM HEPES buffer, 100 U/mL ·100 μg penicillin/streptomycin, and 10% fetal calf serum [all from Biochrom]). Every 24 h of the cultivation period, culture medium was changed and the cells were examined microscopically (Fig. 1).
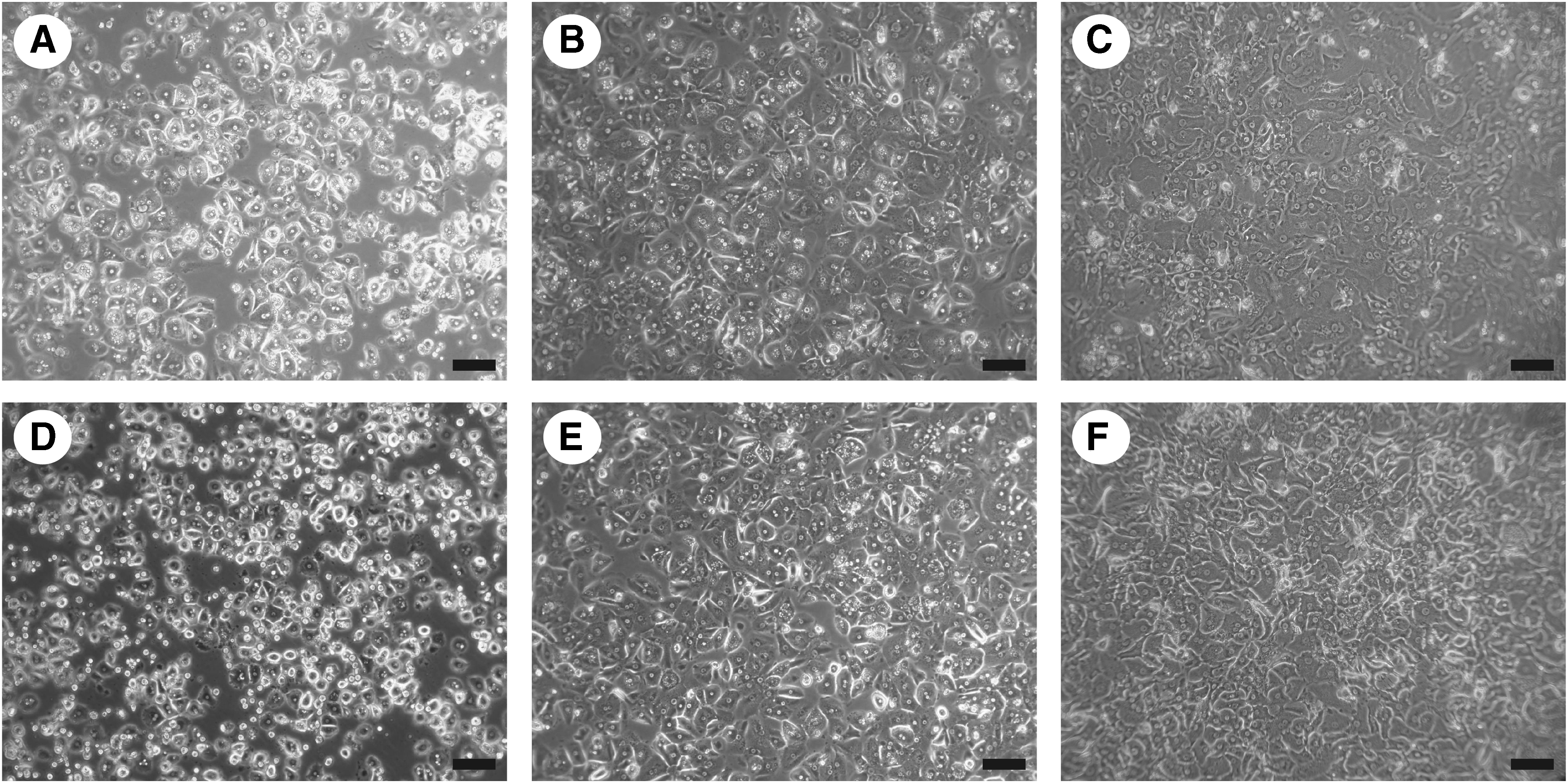
Light microscopy of hepatocytes isolated from laparoscopically resected
Clinical laboratory and procedure-related parameters
All relevant parameters that are known from the literature to affect the outcome of hepatocyte isolation were collected to exclude a bias on the OLR versus LLR analysis. 22 Preoperative laboratory parameters of the patients, surgical features, and the results of the histopathological analysis of the resected liver tissue were collected from the patient's hospital records. Severity of steatosis and fibrosis/cirrhosis was assessed on the basis of the pathology report using a classification by Desmet and Scheuer as descibed elsewhere. Steatosis was categorized in “nonsteatotic” (no fatty hepatocytes in histology), “mild steatosis” (≤30% of hepatocytes contain fat), or severe steatosis (>30%).
Measurement of cell culture parameters
The supernatant of the cell culture was analyzed for transaminase enzyme activity, urea and albumin content after overnight culture as well as after 2, 4, and 6 days of culture. The supernatant of three wells was, therefore, centrifuged at 3000 g for 5 min (4°C). Aspartat aminotransferase activity and urea content were measured by Labor Berlin–Charité Vivantes GmbH within 12 h using an enzymatic assay (Roche Hitachi cobas c 6000 system; Roche Diagnostics GmbH). Albumin production was assessed using the human albumin ELISA kit (Bethyl Laboratories) after supernatant sample storage at −80°C. ELISA samples were measured as duplets and according to the manufacturer's instructions.
Plating efficiency was quantified using a modified version of a protocol reported by Gramignoli et al. 24 In short, 4 h after seeding, the supernatant of three wells was pooled and kept, whereas the other three wells were washed with warm PBS and the supernatant was discarded. Twenty-four hours after cell seeding, the supernatant of the wells was kept, respectively, discarded again and the latter three wells were washed three times with PBS. The supernatants were centrifuged at 12.800 rpm and the pellets were pooled in RIPA buffer and stored at −80°C immediately.
The remaining adherent protein was suspended with RIPA buffer, scratched off the surface, and pooled. The remaining adherent protein of the washed three wells was then set in relation to the absolute protein of the other three wells ([supernatant 4 h+supernatant 24 h+remaining protein] divided by [carefully washed protein after 24 h]). The protein content was analyzed with BCA reagent (Pierce, Thermo Fisher Scientific) using a photometric assay with all samples measured in triplets.
Statistical analysis
All data are expressed as the mean ± SEM unless indicated otherwise. Statistical analysis was performed using GraphPad Prism 6.0 (GraphPad Software, Inc.). The nonparametric Mann–Whitney test was used to analyze quantitative parameters with non-Gaussian distribution. For contingency analyses for categorical parameters, the chi-square test was used. A p value ≤0.05 was considered significant.
Results
General characteristics and surgical features of the open and LLR groups
Out of all hepatocyte isolation procedures in this study, n = 15 livers were resected through the open approach and n = 7 livers were resected using laparoscopic technique. Both groups did not significantly differ regarding the most common parameters known to affect the isolation outcome 22 —neither with respect to the surgical and isolation-related parameters such as duration of surgery, cold ischemic time, collagenase digestion time, and liver weight, nor regarding the preoperative clinical chemistry parameters (Table 1), such as bilirubin, alanine aminotransferase and aspartate aminotransferase (AST), alkaline phosphatase, gamma-glutamyl transpeptidase, international normalized ratio, and activated partial thromboplastin time (aPTT).
Data are shown as mean ± SEM and p values. A p value <0.05 was considered statistically significant. Significant p values are printed in bold.
AP, alkaline phosphatase; aPPT, activated partial thromboplastin time; ALT, alanine aminotransferase; AST, aspartate aminotransferase; CIT, cold ischemic time; CRLM, colorectal liver metastasis; GGT, gamma-glutamyl transpeptidase; HCC, hepatocellular carcinoma; INR, international normalized ratio; LLR, laparoscopic liver resection; OLR, open liver resection; SEM, standard error of the mean.
Histopathological scores for fibrosis, cirrhosis, and steatosis were evenly distributed in the OLR and LLR groups (Table 1). The LLR group does not contain histologically healthy tissue, that is, tissue without steatosis or fibrosis. However, due to the smaller number of patients in the LLR group, the difference is statistically not significant. Both groups did only significantly differ in indication for surgery since there were no livers diagnosed for biliary tree carcinoma in the LLR group (p = 0.023, Table 1). Thus, with the exception of the indication for surgery, the OLR and LLR groups did not differ in regard to the parameters and patient characteristics that are known to affect the outcome of hepatocyte isolation (Table 1).
Comparison of the mean hepatocyte isolation outcome (OLR vs. LLR)
With a total yield of 36.81 × 106 cells/g liver tissue (± 6.77) in the OLR group and 16.84 × 106 cells/g liver tissue (± 10.66) in the LLR group, there was a significant lower cell yield for livers resected by laparoscopy (p = 0.032). The viable yield was lower in the LLR group as well (OLR: 31.70 ± 6.05 × 106 cell/g vs. LLR: 14.70 ± 9.89 × 106 cell/g; p = 0.026). The viability was significantly reduced in hepatocyte isolations in the LLR group (OLR: 84.26% ± 1.46% vs. LLR: 38.17% ± 17.80%; p = 0.106, Figure 2). Also Percoll survival was lower in LLR group than in OLR group, however, without reaching statistical significance (Figure 2).

Comparison of hepatocyte isolation from open and laparoscopic resected human liver tissue regarding total yield
Subgroup analysis in the LLR group
In the LLR group, (n = 3) three left-lateral partial hepatectomies (left-LLR) and (n = 4) four right-lateral partial hepatectomies (right-LLR) were performed. In right-LLR, three out of four isolations were stopped before Percoll purification due to insufficient cell yield. The fourth isolation in the right-LLR brought a yield before Percoll purification but no cell yield after Percoll purification, whereas in the left-LLR, every isolation was successful. This observation prompted us to exclude the isolations from right-LLR and perform a subgroup analysis between left-LLR and OLR.
Comparison of open vs. left-lateral LLR
In comparison between OLR and left-LLR isolations, no differences in the total cell yield and the viable cell yield before Percoll were found (Figure 3). Likewise, the difference regarding viability was no longer detectable (OLR: 84.26% ± 1.46% vs. left-LLR: 88.44% ± 2.68%; p = 0.498). Percoll survival was slightly better in the left-LLR group but without reaching statistical significance (OLR: 60.12% ± 4.59% vs. left-LLR: 81.46% ± 7.46%; p = 0.082; Figure 3).
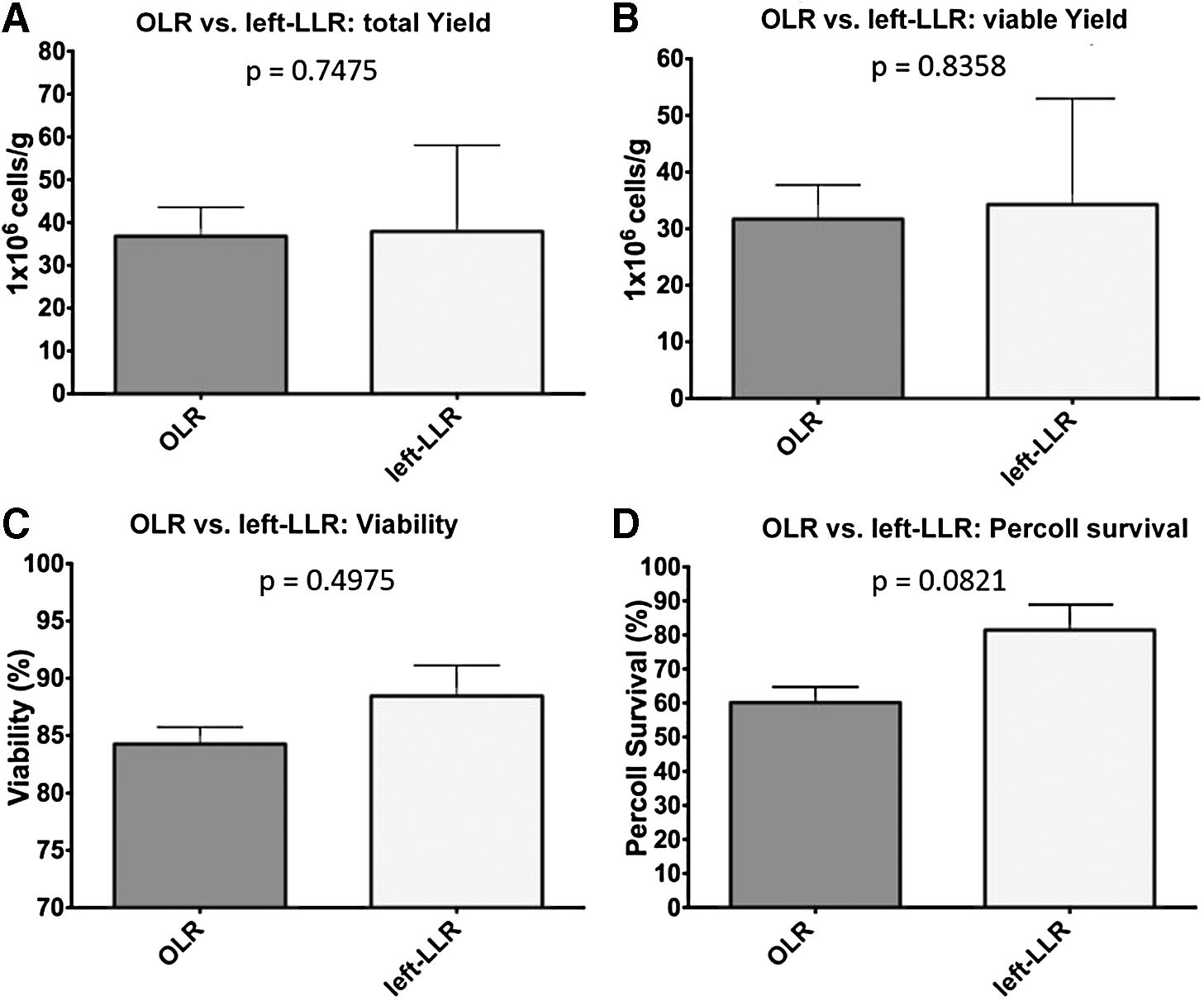
Comparison of hepatocyte isolation from open and left-lateral laparoscopic resected human liver tissue regarding total yield
In vitro hepatocyte function after open vs. left-lateral LLR
Hepatocytes isolated from left-lateral laparoscopic resected livers did not show higher levels of AST leakage nor did they show a worse plating efficiency after 24 h than hepatocytes obtained from livers operated through the open approach (Table 2).
Data are shown as mean ± SEM and p values (p). A p value <0.05 was considered statistically significant.
Left-LLR, left-lateral laparoscopic liver resection.
Also, hepatocytes from both groups did not differ significantly in urea and albumin synthesis (Table 2).
Discussion
Hepatocyte isolation from tissue obtained after liver resections is an established procedure in many hepatobiliary surgery centers and their affiliated research laboratories. Although not suitable for therapeutic application due to the risk of transmission of malignancy, primary human hepatocytes from this source serve for basic research in regenerative medicine and for pharmacological studies.3–5
Although open surgery has been the standard for liver resections so far, the laparoscopic approach is increasingly gaining importance. Even though technically more demanding, the results of laparoscopic liver surgery in the hands of experienced teams are convincing.20,21 Compared with the open approach, laparoscopic liver surgery is associated with significantly reduced surgical trauma, which results in faster recovery. Moreover, it is superior regarding the cosmetic result. Although not yet the standard, the laparoscopic approach is the forward-looking technique for liver surgery and it can be assumed that in the near future, this approach will be used in a majority of cases.
Thus, the outcome of hepatocyte isolation from laparoscopically resected liver tissue has to be evaluated to find out whether or not this source can continue to meet the needs for primary human hepatocytes.
Our study shows that the overall result of hepatocyte isolation from laparoscopically resected liver tissue is significantly worse than the result of open surgery. The parameters that are known to be predictive for the outcome of hepatocyte isolation 22 are inapplicable to forecast the isolation outcome when using tissue obtained from laparoscopic surgery, since both groups did not significantly differ in this analysis. Only the number of patients with biliary tree carcinoma was significantly higher in the OLR group, which is a negative predictor for the outcome of hepatocyte isolation, but which nonetheless resulted in a better outcome in the OLR group than in the LLR group.
However, when looking at left-lateral laparoscopic partial hepatectomies, hepatocyte isolation was as effective as from open surgery. This was true for all analyzed parameters, which are cell viability, isolation yield, and the metabolic function of cultured hepatocytes.
We hypothesize that these findings are primarily due to the prolonged warm ischemia time resulting from right-sided LLRs: When operating through laparoscopic approach, the resected liver tissue remains in the surgical site at 37°C until it is evacuated by the end of the entire procedure to maintain the capnoperitoneum. In contrast, in open surgery, the specimen is cooled by the surrounding air and removed from the surgical site immediately after resection.
Given the technical and anatomical facts, the parenchymal dissection of the left lateral segments (II and III) can be completed in short time, whereas it is more time consuming for the right liver lobe. This does not take as big as an effect in open surgery as it impacts laparoscopic surgery. Due to the warmer conditions inside the body, the liver specimen is exposed to a longer warm ischemia than in the open approach. Also, it requires more time to retrieve the liver tissue out of the patients' body with the specimen retrieval bag than when surgery is performed openly. The extended warm ischemic time causes hepatocytes to induce cell death and, therefore, affects the isolation outcome.
The almost significantly longer duration of surgery for the right-sided LLR than for the left-lateral LLR (r-LLR: 433 ± 44 min vs. l-LLR 246 ± 33 min, p = 0.0571) supports our assumption. Moreover, the fact that none of the established predictive parameters for the hepatocyte isolation outcome (such as tissue quality, liver weight, digestion time, and bilirubin levels of the patient before surgery) differed between the left- and right-sided liver resections, whereas the outcome of the hepatocyte isolation was significantly worse, indicating that other factors might influence this result.
Our study is limited by the low number of cases in the laparoscopic liver surgery group. For example, there was no tissue in the LLR-group without steatosis or fibrosis. Moreover, both cohorts consist of a disproportionate number of male versus female patients (17 out of 22). However, this is true for both groups. Although it might be reasonably assumed that the decreased isolation outcome of right-sided liver resections is caused by the longer warm ischemia time, we cannot prove this hypothesis by an appropriate multivariate analysis, yet. In general, hepatocyte isolation can only be performed when a sufficient mass of tumor-free tissue can be obtained from the specimen during surgery—which applies for both open and laparoscopic surgeries.
In conclusion, we show for the first time that hepatocyte isolation from left-lateral LLRs is feasible. It can be speculated that the outcome from right-sided LLR might improve by the further establishment of the surgical technique and experience of the surgeons. Since hepatocyte isolation is an expensive and complex procedure, we consider isolating cells from the specimen after right-sided laparoscopic liver surgery as not worth the efforts, whereas laparoscopic resections of the left lobe (segments II and III) are an excellent source for primary human hepatocytes.
Footnotes
Acknowledgments
The authors thank Dr. Moritz Schmelzle and Prof. Dr. Daniel Seehofer for performing the surgical procedures, and Steffen Lippert and especially Peter Tang for their expert technical assistance. Moreover, we thank Anja Schirmeier for assistance with tissue collection from the operation room.
Disclosure Statement
No competing financial interests exist.