
Abstract
Implantable biomaterials supporting extended release of pharmacologic agents may permit localized intra-articular delivery of drugs that modulate the fibrotic response to injuries and surgery. Oligo[poly (ethylene glycol)] fumarate (OPF) is an attractive organic carrier, but its safety profile within synovial joints remains unclear. Here, we assessed the safety of OPF sponges using a validated in vivo model of knee arthrofibrosis. A cohort of 102 rabbits was divided into five groups: arthrotomy only (24), arthrotomy with OPF scaffold placement (24), surgically induced contracture (24), surgically induced contracture with OPF scaffold placement (24), and control without any surgical intervention (6). Six rabbits per surgical group were sacrificed at 72 h, 2, 8, and 24 weeks. Outcomes included biomechanical testing of range of motion, histologic analysis of synovial and cartilage tissues, and scaffold degradation. Cartilage histology and biomechanical measurements were comparable between groups with and without OPF. Synovial inflammation scores were similar among most groups with a minimally elevated score in the rabbits with arthrotomy and OPF versus those with arthrotomy alone. Scores for synovial tissues in rabbits with contracture and OPF were clinically equivalent to those with contractures alone. Most animals (92%) retained scaffold fragments at 24 weeks. Thus, OPF scaffolds implanted into native or arthrofibrotic rabbit knees neither induce nor aggravate cartilage damage, synovial inflammation, or contractures. The apparent safety of OPF scaffolds suggests that they are suitable carriers for the controlled delivery of reagents into the intra-articular joint space to treat arthrofibrosis.
Introduction
T
This rabbit knee model of arthrofibrosis provides an opportunity to investigate potential therapeutic agents. Because systemic administration may lead to adverse side effects, it is desirable to deliver drugs in the intra-articular space. Yet, intra-articular injections may be difficult to administer in contracted joints and do not provide prolonged doses of medicine.15,16 Therefore, intra-articular carriers implantable at the time of surgery would be preferred, provided that the drug delivery vehicle is not toxic, immunoreactive, damaging to cartilage, or inductive of fibrosis. In addition, the material would need to degrade safely and allow for a drug release that is slow and constant.16,17
Biodegradable scaffolds have been used in many tissues to provide localized drug delivery and some have focused on the intra-articular use of these scaffolds from a tissue engineering standpoint.18–20 However, the safety of biodegradable scaffolds must be rigorously established to permit clinical drug delivery within synovial joints. Contracture release in arthrofibrosis requires surgical exposure of the joint, thus providing an immediate opportunity for direct implantation of scaffolds that slowly elute a pharmacologic agent. 17 Hydrogels such as OPF have inert breakdown products, desirable in vitro dissolution rates, and non-deleterious effects on tissues outside synovial joints.21,22 In addition, the mesh size, molecular weight, crosslinking polymer ratio, and other characteristics of this hydrogel are customizable to desired drug elution and degradation rates. This study tests the safety of OPF for drug delivery in synovial joints by investigating the biomechanical and histologic effects of OPF scaffolds in our in vivo rabbit model of arthrofibrosis. Our main finding is that OPF inserted into the joint space neither harms synovial joints nor causes adverse systemic effects in rabbits with either native or contracted knee joints.
Materials and Methods
Study design
One hundred two female New Zealand white rabbits were divided into three main groups (Fig. 1): arthrotomy group (24 animals without scaffold and 24 animals with OPF scaffold), contracture group (24 animals without OPF scaffold and 24 animals with OPF scaffold), and nonoperative control group (N = 6). Each 24-animal group was further subdivided into four 6-animal subgroups based on time of sacrifice (72 h, 2, 8, and 24 weeks after surgery), as per our contracture model. 11 All animal studies were carried out with approval from the institutional animal care and use committee. Rabbits were separately housed and postoperative wound healing was monitored for pain and infection, with administration of antibiotics and analgesia as appropriate to mitigate discomfort. On sacrifice, necropsy was undertaken, followed by biomechanical testing and sampling for histology.

Graphical representation of the study flow.
We note that one animal died during induction of anesthesia by the veterinary technicians. No discernible general health or musculoskeletal issues were present, and so, this animal was used as a control animal. One animal's extensor hallucis longus tendon (which is intra-articular in rabbits) was transected during surgery. This rabbit remained in the experiment and no further complications occurred with this animal. All other animals included in this research survived until the time of sacrifice without complication.
Biomaterials and rabbit arthrofibrosis model
The OPF scaffold material for joint insertion was produced by our group as described previously.23,24 Surgical procedures for the rabbit arthrofibrosis model were completed as documented to create animals with contractures, contractures with release, or sham surgeries (arthrotomy).1,11–13 On exposure of the joint, the operative groups were separated into rabbits with arthrotomy or contracture. In rabbits with arthrotomy, a right knee arthrotomy was performed, but no contractures were induced, while half of this group received an OPF implant. In rabbits with contractures, contractures were induced by disrupting the cruciate ligaments and posterior capsule, inducing an intra-articular hematoma, and by keeping the knee in hyperflexion with wire fixation for 8 weeks1,11–13; as above, half of these rabbits received an OPF implant. For implantation in rabbits with arthrotomy, a saline-soaked OPF scaffold (1 × 1 × 0.5 cm) was placed in the suprapatellar pouch by visual inspection. For animals with contractures, scaffolds were inserted on intracapsular joint injury.
Biomechanical testing and analysis
All animals were sacrificed under sedative anesthesia and intravenous barbiturate overdose. Both lower extremities were harvested at the mid-femur. Each lower extremity underwent biomechanical testing for range of motion (ROM), with the left side serving as an internal control. Joint stiffness was measured using a custom-made, validated device that measures joint angles as previously described.1,11–14 An extension torque was applied to the femur at a rate of 1° per second up to a maximum torque of 20 NCm or extension past 190°, whichever came first. Contracture was quantified as the difference between operative and nonoperative limbs. The data were plotted and analyzed for flexion contracture angles.
Necropsy and tissue sample handling
After mechanical testing, necropsy by knee joint dissection was performed for gross inspection of scaffold status, cartilage damage, and inflammatory changes. Synovium tissue was sampled from the medial parapatellar area due to its position away from the scaffold implantation and arthrotomy sites. Cartilage samples were then procured from the medial femoral condyle (MFC), lateral femoral condyle (LFC), and tibial plateau (TP) using a surgical saw. Cartilage/bone cuts were made in the parasagittal plane to maximize the joint surface analyzed. Synovial tissue samples were preserved in 10% formalin, sectioned, and stained using hematoxylin and eosin (H&E). Cartilage/bone samples were decalcified using sequential washes of formic acid and stained with safranin O/fast green, as is common practice for cartilage tissue.25,26
Histologic analysis
All histologic analyses were performed by a blinded veterinary pathologist. Any type of damage to the cartilage surface would be unacceptable for scaffold use in clinical practice. Therefore, a simple binary scale of no-damage (0) or damage (1) was used. See Figures 2 and 3 for examples. Each rabbit knee was sampled three times (i.e., MFC, LFC, and TP) and the binary score from each sample was summed for a total joint score, with a possible range of 0–3. The expectation before histologic analysis was that nonoperative legs would show no cartilage changes (score of 0). In contrast, transection of the anterior cruciate ligament (ACL) is a key model used in rabbit osteoarthritis research and so animals in the contracture groups were expected to show higher scores.
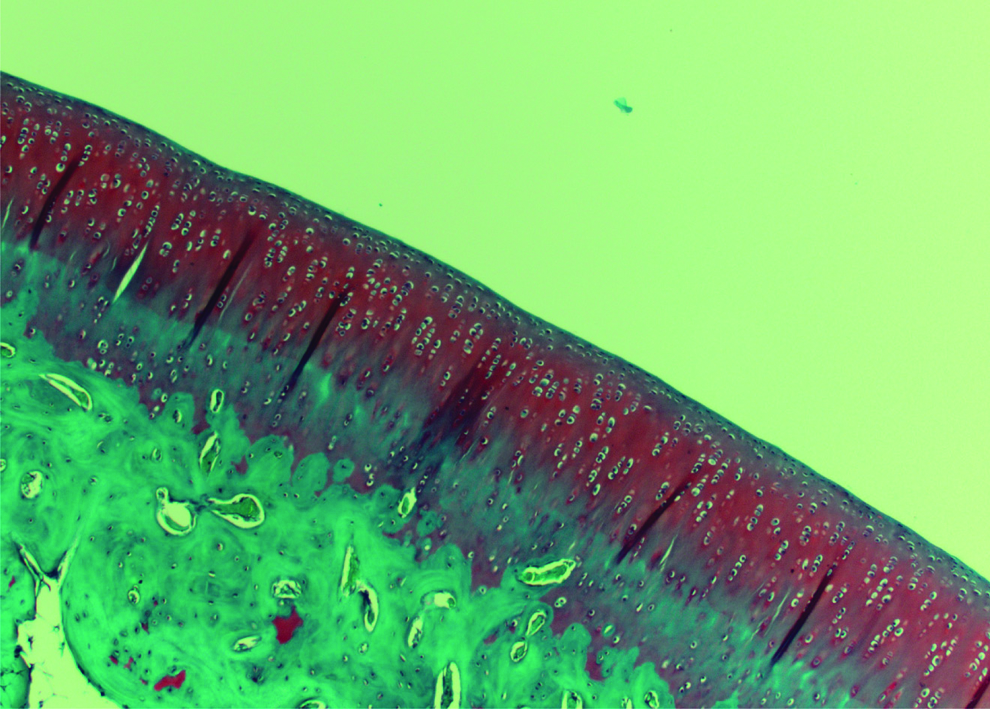
Normal cartilage and bone at 4× magnification. Note the regularity in both contour and layer differentiation. Color images available online at

Abnormal cartilage and bone at 4× magnification. Note the irregular shape and thinning of the superficial cartilage layer. Color images available online at
Synovial samples were evaluated for acute and chronic inflammation. 25 The scoring system used has been validated as useful in distinguishing between osteoarthritis, inflammatory arthritis, and post-traumatic arthritis. 26 The scoring system gives points based on status of the synovial lining cell layer, density of resident cells, and presence of inflammatory infiltrate, with a scale of 0 to 9. A score of 0 or 1 is considered “No Synovitis,” 2–4 “Low-grade Synovitis,” and 5–9 “High-grade Synovitis.” For all rabbits undergoing surgery, some minor synovial inflammation was expected, due to the known inflammatory response associated with healing.
Biostatistical analysis
Because the primary research question centered on safety of OPF, an equivalence approach was used to evaluate the ROM in joints with or without OPF implants. For ROM data, an equivalence limit difference of ±17.5 was identified a priori and 95% confidence intervals (CIs) were constructed for differences in the means between two groups. When the lower and upper limits of the 95% CIs were contained within the equivalence limits, the groups were considered to be similar (i.e., statistically equivalent) with respect to ROM. Comparisons were made for all groups, as well as separately by subgroups based on sacrifice time.
Cartilage histological changes were analyzed as binary outcomes that either occurred or did not occur. This approach scored histological changes in at least one of three anatomical sites in the joint: MFC, LFC, and TP. Differences in the proportion of animals with histological changes in at least one site were calculated and reported with 95% CIs. Because there is no published precedent for this approach, the equivalence limit difference in this outcome was not specified and instead differences reported descriptively. Differences in the mean synovitis scores between the study groups were reported with 95% CIs and compared with two-sample t-tests. The association of the development of pseudotrochlea and synovial score was evaluated using chi-square tests and univariate logistic regression models. All statistical tests were two sided and p < 0.05 was considered to be statistically significant for comparative analyses. Analyses were conducted using SAS version 9.2 (SAS Institute, Inc., Cary, NC).
Results
Cartilage histology
Comparing the groups subjected to arthrotomy with or without implantation of OPF, the 95% CI for the difference in proportions was −0.15 to 0.24 (Fig. 4). As such, these groups were considered to be statistically equivalent.
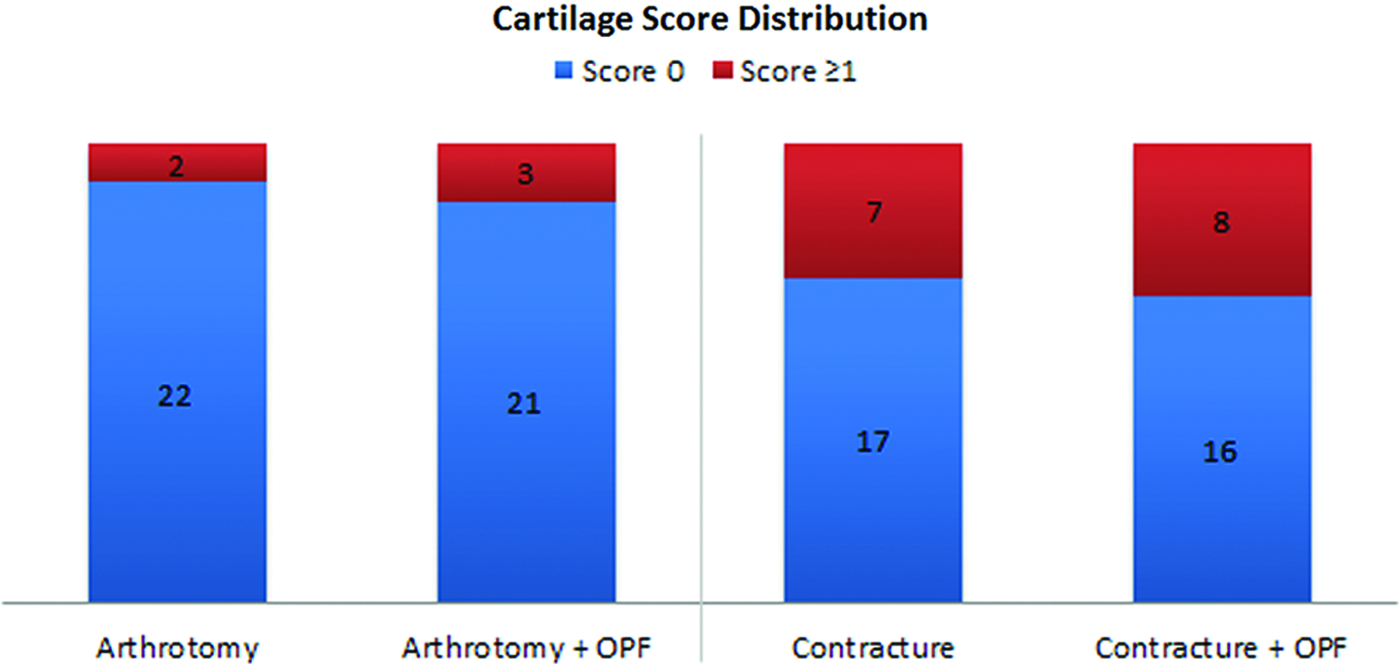
Cartilage score distribution for experimental right limbs, suggesting equivalence between groups. Color images available online at
Comparing the groups that underwent contracture with and without implantation of OPF, the 95% CI for the difference in proportions was −0.21 to 0.28. As such, these groups were considered to be statistically equivalent.
Cartilage samples from the left (nonoperative) limbs were also analyzed to serve as internal controls. In these limbs, both the arthrotomy and the contracture groups had animals with cartilage scores of one or greater (Table 1).
A comparison between the cartilage samples of right (operative) and left (nonoperative) limbs showed no difference in the arthrotomy animals. However, in the contracture group, right (operative) knees had statistically significantly higher cartilage damage scores than the left (nonoperative) knees in the same animals (p = 0.002).
Synovial histology
The highest synovial inflammation score in any animal was three (on 0–9 scale, with 9 being the highest). The difference in means showed rabbits undergoing arthrotomy and receiving OPF scaffolds (arthrotomy+OPF group) have a mean score 0.92 higher than animals that underwent arthrotomy alone. The 95% CI was from −1.56 to −0.28. Thus, overall, the groups are not considered to be statistically equivalent. Synovitis score in the arthrotomy animals was analyzed at time of sacrifice. A wide range of differences among means were observed depending on time of sacrifice, with OPF-implanted knees having higher synovial inflammation scores at early time points (Fig. 5). Arthrotomy groups (±OPF) were not statistically different within or among samples taken from animals sacrificed after 2-, 8-, and 24-week periods.
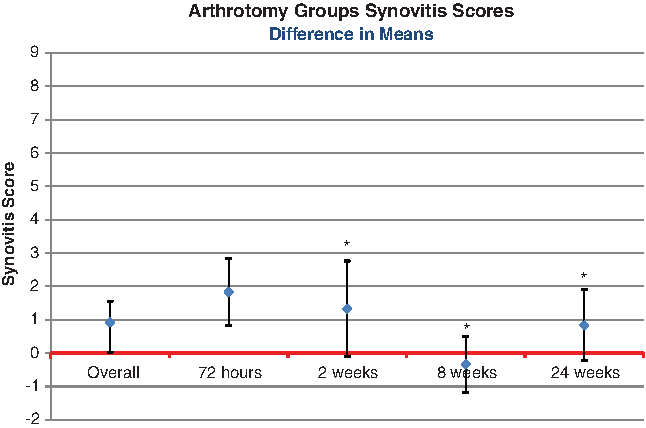
Difference in mean synovitis scores between arthrotomy-only group and arthrotomy+OPF group. A positive value reflects a higher synovitis score in the arthrotomy+OPF group. Confidence intervals, 95%, are shown around the difference in means [*arthrotomy groups (±OPF) are likely equivalent]. Color images available online at
Contracture animals showed a similar difference in means between groups as seen in the arthrotomy animals, with an overall 95% CI from −1.37 to 0.03 (statistically equivalent). Contracture animals were analyzed for difference in mean synovial score at each time point (Fig. 6). Contracture animals (±OPF) were considered to be statistically equivalent overall at all time points examined (up to 24 weeks). The left, nonoperative synovium was also analyzed as an internal control. Synovial inflammation scores for the nonoperative limbs of animals that were subjected to arthrotomy showed a difference of 0.08 in mean scores, with a 95% CI of −0.20 to 0.03 (statistically equivalent). Synovial inflammation scores for contracture animals' nonoperative limbs showed a difference of 0.16 in mean scores, with a 95% CI of −0.55 to 0.22 (statistically equivalent).

Difference in mean synovitis scores between contracture versus contracture+OPF groups. A positive value reflects a higher synovitis score in the contracture+OPF groups. Confidence intervals, 95%, are shown around the difference in means (*contracture vs. contracture+OPF groups are likely equivalent). Color images available online at
Biomechanical data
Analysis between groups (24 animals in each group) and subgroups (6 animals at each time point) revealed that arthrotomy animals had better ROM on their operated knee (Fig. 7) than control knee (nonoperated). Further analyses showed statistical equivalence between the arthrotomy only and the arthrotomy+OPF group, both overall and when broken down by time after surgical intervention. Animals in the contracture group were analyzed in a similar way. Wide variation was seen between time points in the degree of contracture (Fig. 8). Statistical equivalence between the groups was observed at 24 and 72 h. The negative results at 72 h are due to lack of scar tissue formation necessary for contracture. Nonequivalent time points showed minimal clinical differences, but experimental variability of the measurements contributed to the statistical nonequivalence.
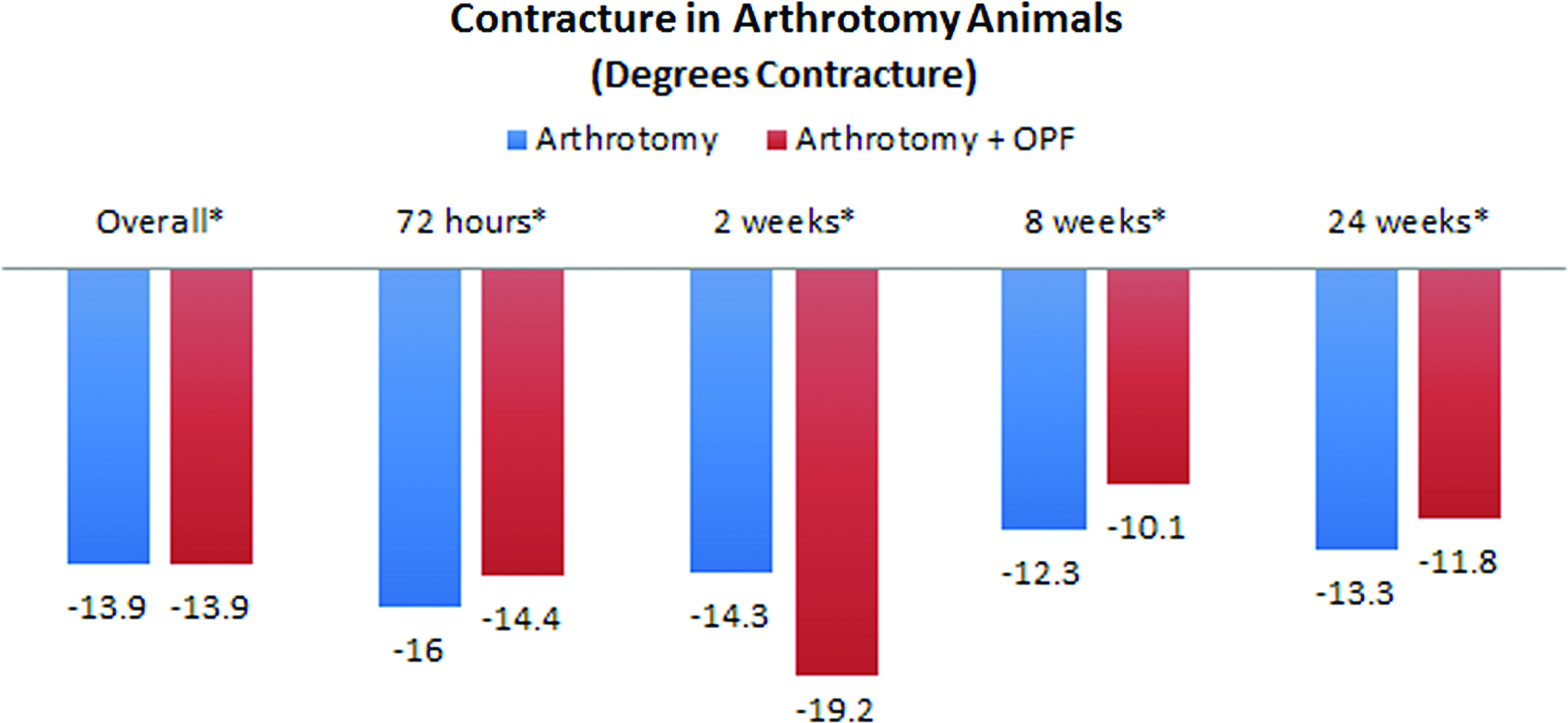
Contracture in arthrotomy animal groups overall, and subdivided by time of sacrifice (*arthrotomy vs. arthrotomy+OPF groups are likely equivalent). Color images available online at

Contracture in contracture animal groups overall, and subdivided by time of sacrifice (*contracture vs. contracture+OPF groups are likely equivalent). Color images available online at
In vivo scaffold degradation rates
One set of rabbits (n = 48) underwent placement of OPF scaffolds and groups of 12 rabbits were sacrificed as a function of time after surgery. The structural integrity of the scaffold demonstrated progressive resorption over time (Table 2). After 72 h and 2 weeks, the general shape of the scaffold was recognizable and occasionally fragmented. After 8 and 24 weeks, the remaining scaffold was highly degraded. In addition, after 24 weeks, scaffolds were entirely encapsulated in the suprapatellar pouch, which can be described grossly as a film of tissue enveloping the remaining scaffold. It was seen only in animals sacrificed at 24 weeks, with four animals from the arthrotomy group and five animals from the contracture group presenting this finding. Histology of this encapsulation tissue showed chronic inflammatory changes, consistent with the known foreign body reaction caused by OPF scaffolds in soft tissues.21,22 In animals with encapsulation of the scaffold, the synovial inflammation score was 0 in six animals, 1 in two animals, and 3 in one animal.
Percentages are reported out of the number of scaffolds present at each time point. The difference between fragmentation and degradation was based on the presence or absence of the original cuboid architecture of the scaffold.
Pseudotrochlea formation
Eleven animals were found to have medially dislocated patellae with formation of a trochlea-like groove on the medial femur (Fig. 9). This pseudotrochlea formation was found only in the arthrotomy groups, with none found in the contracture animals. Post hoc analysis on the relationship between pseudotrochlea formation and synovial inflammation scores was undertaken, specifically looking at odds ratios for increased synovial inflammation. The odds ratio was 1.44 (95% CI 0.83–2.50), indicating no statistically significant relationship between pseudotrochlea formation and synovial inflammation (Table 3).
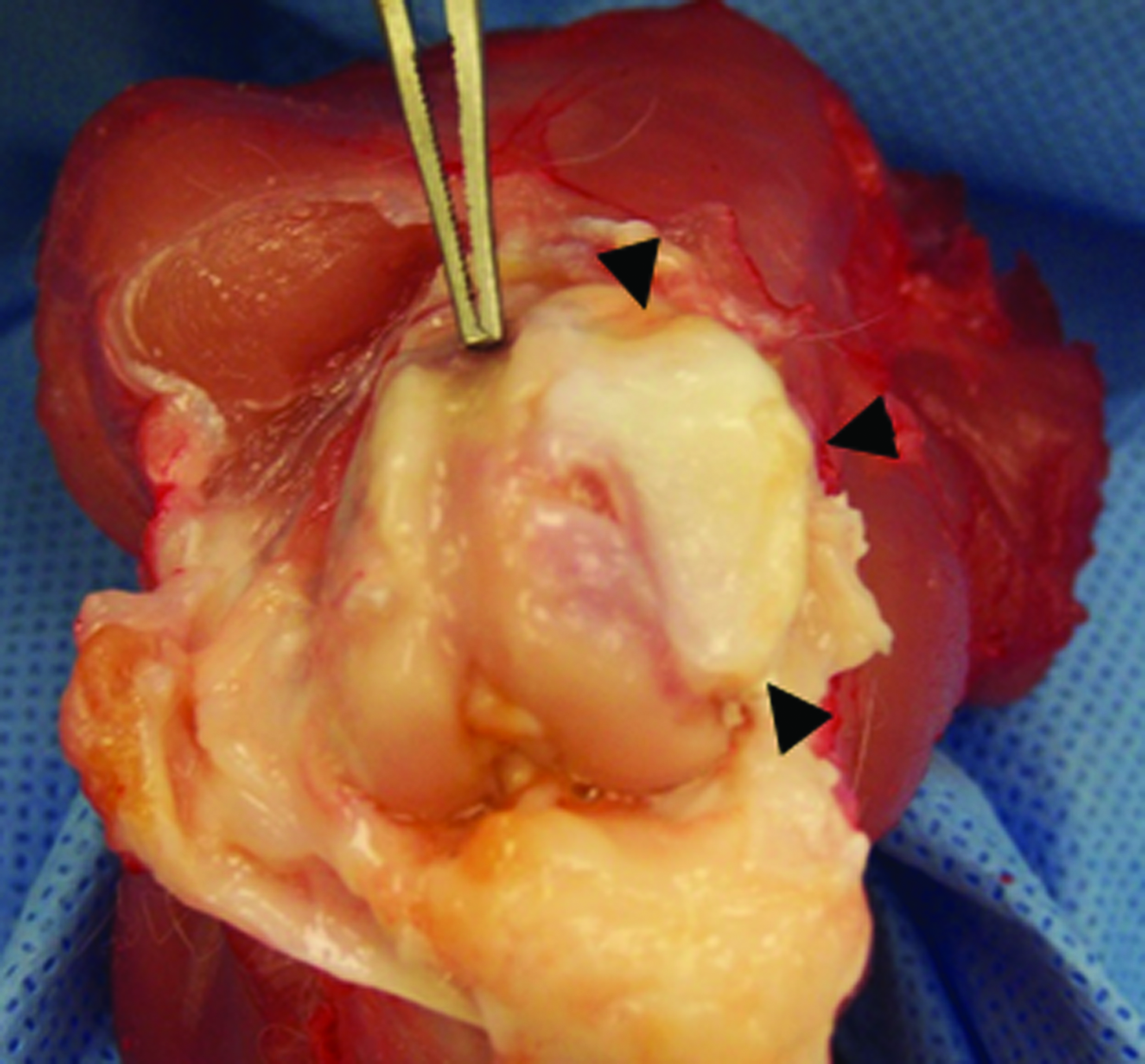
Pseudotrochlea formation is seen just medial to the trochlea. For orientation, the Adson forceps is pointing down the trochlear groove from proximal to distal in a right knee. The black arrowheads identify the periphery of the pseudotrochlea. Color images available online at
No significant relationship was seen between synovitis score and pseudotrochlea formation.
CI, confidence interval.
Discussion
Joint contractures after trauma or surgery represent a difficult problem to manage clinically. Contracture prevention and treatment strategies are unpredictable, and motion is difficult to restore and maintain in a number of patients. Pharmacologic inhibition of fibrosis represents an attractive alternative to current approaches, although systemic administration of pharmacologic agents is not guaranteed to achieve sufficient levels within the intra-articular joint space, and may be associated with systemic side effects. Similarly, localized intra-articular injections (including pump-based delivery methods) of fibrosis therapeutics or prophylactics may not provide sustained levels or predictable outcomes and may require multiple administrations.
Implantable scaffolds loaded with therapeutic agents represent an attractive method for sustained intra-articular delivery of drugs. However, there is limited information on the potential side effects and safety of scaffolds that could induce cartilage damage, inflammation, and fibrosis. Of the various scaffolds available, OPF hydrogel is inert, dissolvable, and has benign effects on nonsynovial tissues.21,23 Our study is the first to demonstrate the safety of intra-articular implantation of OPF and specifically documents a lack of cartilage damage, major inflammatory response, or worsened contracture in knees subjected to a simple arthrotomy, as well as in knees with induced contractures.
One of our criteria for using an implantable drug delivery device is that no cartilage damage occurs as a result of scaffold implantation. As such, the binary scale of damage or no damage was used. The contracture animals did have cartilage damage in the operative leg, which is concordant with the results of other rabbit models that involve ACL-transections (e.g., rabbit knee osteoarthritis27,28). Interestingly, left (nonoperative) limbs were damaged at the same rate as right knees in arthrotomy animals. There is no putative reason for having cartilage damage in the nonoperative knee, so it may be that our conservative approach to cartilage histologic analysis may have over-estimated damage across all samples. Altogether our results indicate that OPF does not cause cartilage damage.
Slight increases in synovitis score were observed in joints with and without OPF. This difference was 0.92 (on a scale of 0–9) in the arthrotomy animals, and the groups did not reach statistical equivalence. In the arthrotomy animals, the small differences in overall mean scores were due to higher differences in synovitis score 72 h after surgery. This difference between means normalized over time, reaching statistical equivalence at the 2-, 8-, and 24-week time points for both the arthrotomy and the contracture groups. As expected, synovitis scores were increased in operative limbs due to the physiologic response to surgery. Although some comparisons of synovitis scores between OPF and non-OPF groups did not reach statistical equivalence, the question of clinical significance must be considered. The maximum synovitis score seen in these animals was 3 (considered “mild synovitis”). We would not expect the very small increases in synovitis for a short time after surgery to be detrimental to the joint over longer time scales, although this outcome deserves further study.
A major important feature for a scaffold to be safe in the prevention and treatment of joint contracture is to ensure that the scaffold itself does not contribute to fibrosis. In our study, the arthrotomy and contracture animals showed statistically equivalent or improved contracture results if implanted with OPF, including at the 24-week time point. Contracture animal data were consistent with previous work from our group.11,14 In particular, the arthrotomy animals showed negative contracture values (i.e., increased ROM in the operative leg vs. the nonoperative leg), suggesting an iatrogenic reaction. Thus, OPF scaffolds did not cause increased contracture in our study.
Ensuring satisfactory patellar tracking and watertight arthrotomy closure is an important step in wound closure of the human knee. During this investigation, closure of the arthrotomy was performed in a similar manner to human knee joints (interrupted, absorbable suture). Patellar tracking was found to be excellent at the end of each surgery. However, this closure was not tight enough to ensure proper long-term patellar tracking in some animals that received an arthrotomy. This allowed chronic medial dislocation of the patella in animals allowed to move after index surgery, resulting in pseudotrochlea formation. The likely reason for pseudotrochlea formation is iatrogenic laxity in the lateral parapatellar soft tissues. This phenomenon has been reported previously. 29 No increase in synovial scores was seen in rabbits with pseudotrochlea formation. To prevent this issue, future studies involving arthrotomy in rabbits should attempt a tighter capsulotomy closure and/or short-term limb immobilization (as often done in human clinical practice).
OPF degradation has been reported in other tissue types at 2 to 12 weeks.21,23 In our study cohort, a large number of animals had observable scaffold remaining at 24 weeks. Animals with scaffold present at 24 weeks also showed encapsulation and chronic localized inflammation, although this did not seem to affect the synovial scoring of the total joint. Encapsulation was not observed in any of the animals sacrificed at 8 weeks. Long-term fibrous capsule formation is consistent with results seen in bone and soft tissue from previous research.21,23 To diminish late encapsulation, future studies of intra-articular OPF implantation should use scaffolds that degrade faster than the scaffolds used in this study.
Our investigation had some inherent limitations. Due to the nature and timing of our contracture model, established time points did not allow for statistical analysis of scaffold degradation rates. In addition, the scoring systems we used for cartilage damage and synovitis were lacking a positive control that is typically possible with more established protocols. The pseudotrochlea formation was an unexpected finding, reported only once before. 27 This added a stochastic element to the study, although it did not affect the main outcomes. The strengths of our study include a large number of rabbits providing power enough to calculate statistical equivalence, modeling of both native and arthrofibrotic knees, and safety assessments of intra-articular OPF implantation over short and long time periods. All outcomes were analyzed with in-animal controls (the nonoperative limbs) and separate animal controls. The OPF scaffold that was deemed safe in this study is currently undergoing animal studies for applications that have high potential for translation to human clinical settings, particularly in cases that permit surgeon-directed combination of such materials and therapeutic reagents.
Footnotes
Acknowledgments
The authors acknowledge Ronald Marler, DVM, PhD, and Mahrokh Dadsetan, PhD, for their assistance with histologic analysis and expertise with OPF scaffolds, respectively.
Disclosure Statement
No competing financial interests exist.