
Abstract
Tissue-engineered heart valves are developed in bioreactors where biochemical and mechanical stimuli are provided for extracellular matrix formation. During this phase, the monitoring possibilities are limited by the need to maintain the sterility and integrity of the valve. Therefore, noninvasive and nondestructive techniques are required. As such, optical imaging is commonly used to verify valve's functionality in vitro. It provides important information (i.e., leaflet symmetry, geometric orifice area, and closing and opening times), which is, however, usually limited to a singular view along the central axis from the outflow side. In this study, we propose ultrasound as a monitoring method that, in contrast to established optical imaging, can assess the valve from different planes, scanning the whole three-dimensional geometry. We show the potential benefits associated with the application of ultrasound to bioreactors, in advancing heart valve tissue engineering from design to fabrication and in vitro maturation. Specifically, we demonstrate that additional information, otherwise unavailable, can be gained to evaluate the valve's functionality (e.g., coaptation length, and effective cusp height and shape). Furthermore, we show that Doppler techniques provide qualitative visualization and quantitative evaluation of the flow through the valve, in real time and throughout the whole in vitro fabrication phase.
Introduction
T
Approximately, 300,000 heart valve replacements are performed annually worldwide and this amount is expected to triple by the year 2050. 1 Despite the life-saving benefits of available commercial valves, they also possess a variety of detrimental qualities, which include the propensity for calcification, the need for anticoagulation therapies, and the lack of any remodeling and regenerative properties.2,3 These drawbacks have encouraged focused interdisciplinary research to develop living heart valves with repair, remodeling, and growth capabilities by tissue-engineering. To this end, different approaches have been implemented relying on the appropriate combination of cells, biomaterials, and bioreactor conditioning.4,5
In the traditional paradigm, living cells are seeded in or onto constructs of synthetic or natural origin, termed scaffolds, which initially provide the three-dimensional geometry and the microenvironment for the cells to proliferate, differentiate, and produce extracellular matrix.6,7 TEHVs are cultivated in ad hoc-developed bioreactors to provide biochemical and mechanical stimuli for the neotissue formation until they reach adequate mechanical properties and functionality to be implanted. During the conditioning phase, the monitoring possibilities are limited by the need to maintain the sterility and integrity of the valve. Therefore, noninvasive and nondestructive techniques are needed.
Optical monitoring is an intrinsic part of TEHV production as it is used to tune the dynamic conditioning of each valve and identify malfunctions. Typically, TEHVs are imaged from the outflow side to visualize the opening and closing. 8 However, no side and cross-sectional views are available to gain information on the three-dimensional (3D) geometry and its evolution in time. Furthermore, important indicators of valvular functionality such as cusp height, coaptation length, flow patterns, and velocities cannot be obtained with a simple optical system as conventionally used. In clinical practice, such indicators are derived from echocardiographic data.
Cardiac ultrasound imaging is performed by directing high frequency sound waves from the transducer that produces them toward the heart and recording the waves reflected back (echoes) to the same transducer, which then acts as a receiver. This information is processed into a gray-scale image based on the time each echo needs to travel back to the transducer (i.e., the distance to the probe) and its intensity (i.e., the brightness on the screen). This is the commonly used two-dimensional (2D) brightness mode (B-mode), which gives a cross-sectional view of the heart where it is intersected by the ultrasound beam. Multiple images of the field of view are generated every second resulting in the visualization of movement.
Particularly important for the assessment of valvular functionality is the Doppler ultrasound, a mode that allows detection of the direction and velocity of moving blood within the heart. Transthoracic echocardiography is the most commonly performed imaging procedure: by positioning the transducer on the chest or abdomen of the patient, different planes of view of the heart are obtained.
Ultrasound monitoring is routinely performed to enable the noninvasive assessment of healthy, diseased, prosthetic, and repaired heart valves9–16 according to published guidelines and recommendations.17–20
Therefore, we propose ultrasound imaging as a nondestructive, noninvasive, real-time technology, which can add significant value to the current monitoring and evaluation methods in the development of TEHVs.
The aim of this study was to evaluate the applicability of ultrasound monitoring to TEHVs in vitro and assess the benefits associated with it. Ultrasound imaging was used to conduct analysis on TEHVs in poly(methyl methacrylate) (PMMA) bioreactors. This article shows that ultrasound techniques can, in conjunction with optical monitoring, be used to optimize conditioning protocols and allow nondestructive evaluation of TEHVs from design to fabrication and maturation.
Materials and Methods
Ultrasound system
The ultrasound system, Vivid-I (S/N 3642VI General Electric), a linear transducer, and a phased array transducer were used for the experiments. High frequencies result in a higher image resolution, but also a smaller depth of field. The linear probe (8L-RS, Frequency: 3.2–7.5 MHz; General Electric) allows brightness mode (B mode), motion mode (M-mode), and color flow Doppler imaging (CFI) and it is suited for distances up to 10 cm, as specified by the manufacturer. The same modes are provided by the phased array probe (3S-RS, Frequency: 1.5–3.6 MHz; General Electric) in addition to the pulsed and continuous wave Doppler mode (PWD and CWD, respectively). According to the GE Healthcare transducer guide, this probe has a depth of field of up to 30 cm.
In each experiment, once the region of interest (ROI) was identified, the ultrasound image quality could be optimized by tuning brightness, gain, sampling rate, and frequency. For all images, the focus distance was set at the ROI and one or two focus points were used. Ultrasound gel (Arne Maass GmbH, Germany) was applied to the transducer head. All measurements were done by means of the built-in software of the Vivid-i or postprocessed by ImageJ (National Institutes of Health, Maryland).
Valve fabrication
Valves with different designs, as routinely produced in our laboratory,21–23 were used in this study. They were produced by molding techniques using fibrin as scaffold material, with or without textile reinforcement. Cells were isolated from human umbilical veins as previously described. 21 Specifically, trileaflet valves with geometry reproducing the native one and without textile reinforcement were used to show the in vitro cell-mediated tissue contraction, resulting in shortening of the leaflet and therefore insufficient coaptation.
All other valves had a tubular leaflet design. The valves consisted of simple tissue-engineered tubular constructs to be sutured in the aortic or pulmonary root at three commissures at the sinotubular junction and circumferentially at the annulus. 21 The tube collapses under diastolic pressure closing the conduit and opens with the systolic flow. The valves were sutured into silicone constructs mimicking the aortic root, including the sinuses of Valsalva. These were obtained also by molding technique with a two-component silicone rubber. 21 Alternatively, the tubular constructs were sutured into self-expandable nitinol stents to obtain valves for minimally invasive transcatheter implantation. 22 All tubular valves had a warp-knitted polyethylene terephthalate mesh as coscaffold for mechanical reinforcement. 22
In general, the valves were conditioned for 3 weeks under low pressure and flow conditions in ad hoc bioreactors manufactured in our group, 21 while physiological pressure and flow conditions were obtained for testing of the valves according to ISO guidelines (ISO-5840). 22
Valve functionality
TEHVs were visualized in various PMMA bioreactors available in our group. All systems allowed for two possible ultrasound probe locations (Fig. 1A): from the side of the chamber and from the top. A common characteristic of all bioreactors was the presence of a PMMA lid for optical and ultrasound monitoring. These lids featured a compartment descending below the level of the medium to break the air–medium interface. The probe was located in the compartment in contact with ultrasound gel as shown in Figure 1A.
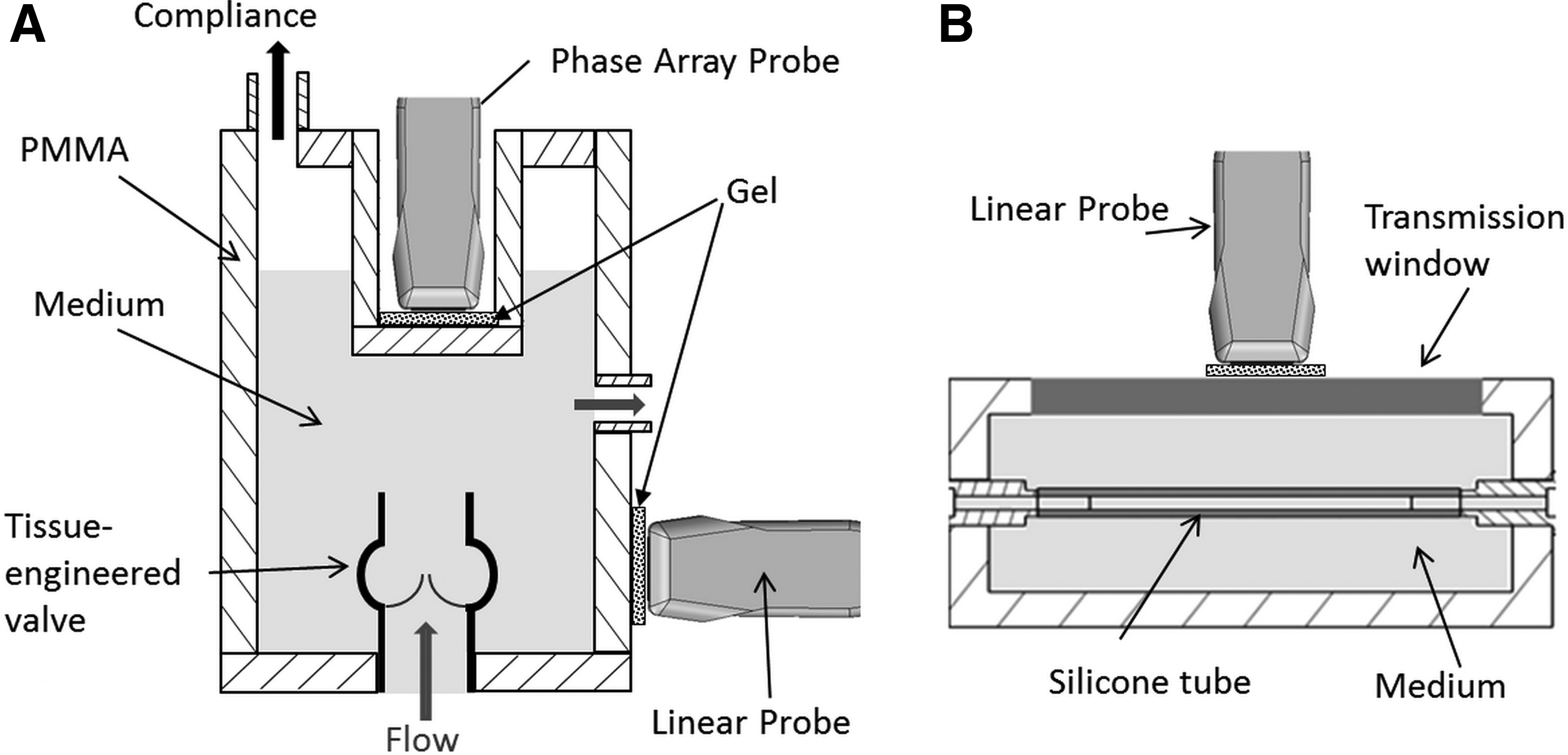
Schematic representation of used setups.
The thickness of the bioreactor components varied between 5 and 15 mm. The possibility to vary the probe location (side or top), the probe type (linear or phased array), and the mode (B mode, M mode, CFI, PWD) resulted in a variety of views and information that could be obtained. The choice was made for each experiment depending on the desired information. The used probe type and the angle between the beam and the flow in the bioreactor are specified for each application.
For comparative purposes, the geometric orifice area (GOA) of a TEHV was evaluated by both ultrasound and optical means. The valve was placed in a bioreactor and subjected to opening and closing cycles. Ultrasound movies were taken at the commissural plane and images were extracted (n = 6). The equivalent optical images (n = 6) were obtained from high-speed movies (Exilim EX-ZR100 Casio, Japan). The GOA of each ultrasound image was estimated using the in-built software in the Vivid-I machine, and the GOA of each optical image was estimated by using ImageJ.
Material suitability
To verify the suitability for ultrasound monitoring of materials typically used for the construction of bioreactor systems, an in-house-designed vascular graft bioreactor 24 was used (Fig. 1B). A silicone tube (ISMAPREME, IDEX Health & Science; inner diameter = 6 mm, outer diameter = 10 mm) functioned as a mock vascular graft. The tube was visualized through five different material inserts, which were each in turn positioned to close the bioreactor chamber filled with purified water (Milli-Q™, Millipore, Germany). The inserts were made of polyoxymethylene (POM), poly(methyl methacrylate) (PMMA), polyvinyl chloride (PVC), glass, and silicone (2-component silicone rubber, Elastosil ADDV M4641, polymer to crosslinker ratio 9:1). The inserts' thickness was 10 mm except for glass, for which it was 4 mm. All measurements were performed with the linear probe.
Results
B-mode: 2D ultrasound
Figure 2 illustrates ultrasound images of a TEHV in comparison to those obtained by optical monitoring. A TEHV with a tubular leaflet design 21 is shown in open and closed positions by camera (Fig. 2A, B) and ultrasound (Fig. 2C, D) recordings, respectively. Such a view is suitable for the evaluation of the valve's symmetry during opening and closing, and the estimation of the GOA, which was quantified as 2.05 ± 0.04 cm2 and 2.07 ± 0.03 cm2 from the ultrasound and optical images, respectively.
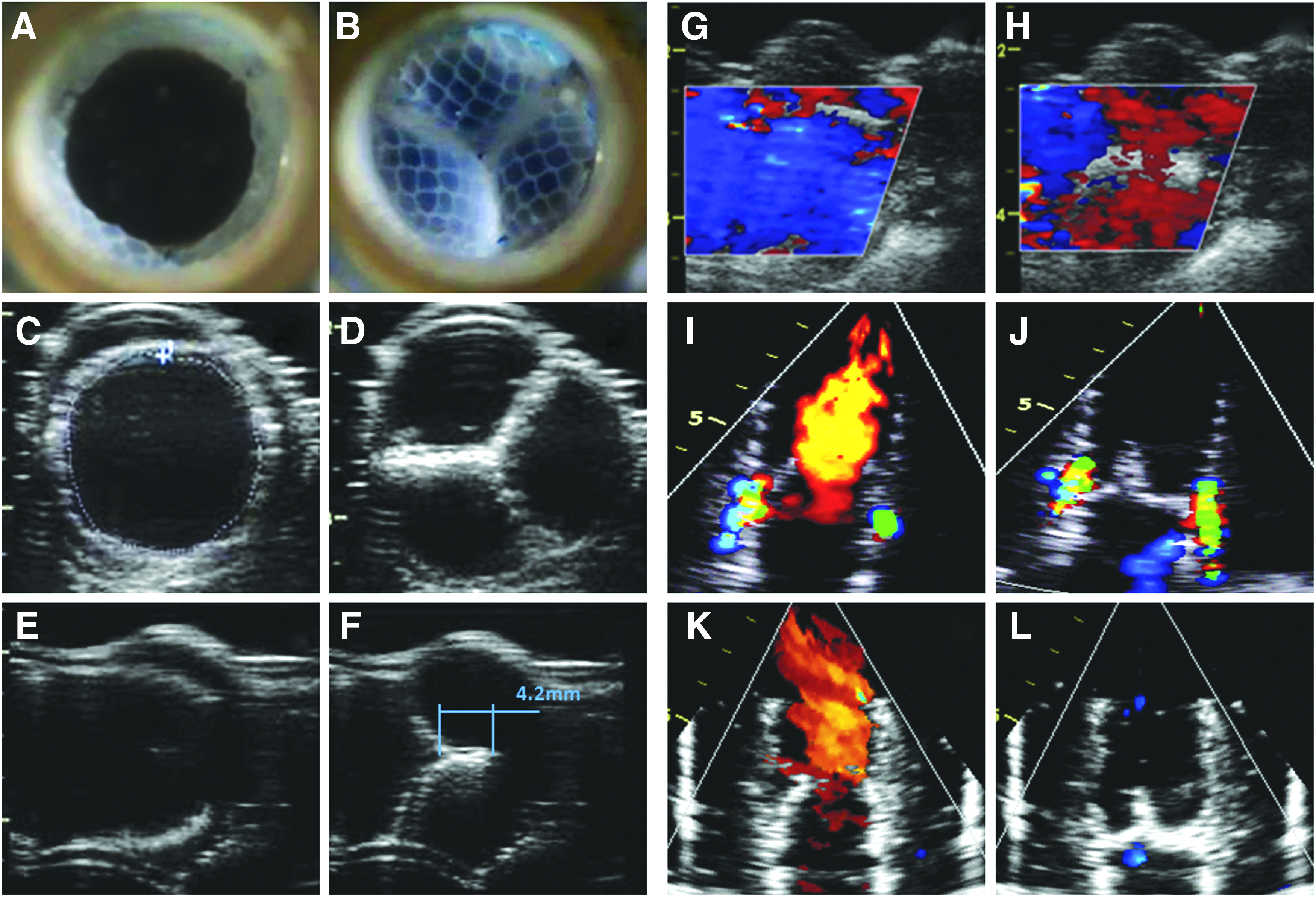
Heart valve in vitro monitoring. Optical monitoring of TEHVs in
The ultrasound images were obtained by positioning the linear probe on the side wall of the bioreactor so that the viewing plane was transversal to the valve's axis (Fig. 2C, D). Simply by changing the probe's orientation by a 90° rotation, the valve could be visualized in the longitudinal plane (Fig. 2E, F) where leaflet coaptation can be evaluated and quantified (4.2 mm).
Ultrasound was used to monitor the maturation process of a fibrin-based valve during 21 days of dynamic conditioning in a bioreactor. Cell-mediated tissue contraction was observed and documented (Fig. 3). Figure 3A shows the original semilunar shape of the valve's leaflets. By postprocessing of the obtained images with ImageJ, the leaflets with planar geometry were estimated to be reduced to 45% of the original size (Fig. 3B).
Cell-mediated tissue contraction leading to valvular insufficiency.
Doppler imaging
CFI was performed with the linear probe to visualize the flow during the opening and closing of the valve to confirm unobstructed opening and complete closure (Fig. 2G, H). The slant of the color box indicates that the CFI beam was electronically steered to obtain flow information even in the case of a poor Doppler angle between the linear probe and the flow. The flow direction is displayed correctly; however, no precise quantitative information on the flow velocity can be obtained under these conditions.
Figure 2I–L gives an example of how ultrasound in CFI mode can critically support the development of TEHVs by design optimization. The images were obtained with the phase array probe positioned above the valve on the vessel side. In this case, a TEHV designed for transcatheter implantation 22 was monitored to evaluate the newly developed design. Figure 2I and J show paravalvular leakage due to the way the TEHV was sutured onto the nitinol stent. After optimization of the suturing procedure, no paravalvular leakage was detected (Fig. 2K, L).
The phase array probe, with the ultrasound beam aligned to the flow, was used in the PWD mode to visualize the flow profile and the flow velocity at the level of the commissures, along the valve longitudinal axis. A systolic phase equivalent to 35% of the cycle duration with a peak velocity of 1.75 m/s was registered. The valve showed good behavior with only a limited regurgitation during the diastolic phase. No significant spectral broadening was displayed, indicating that the flow was laminar and therefore the valve was not stenotic.
M-mode
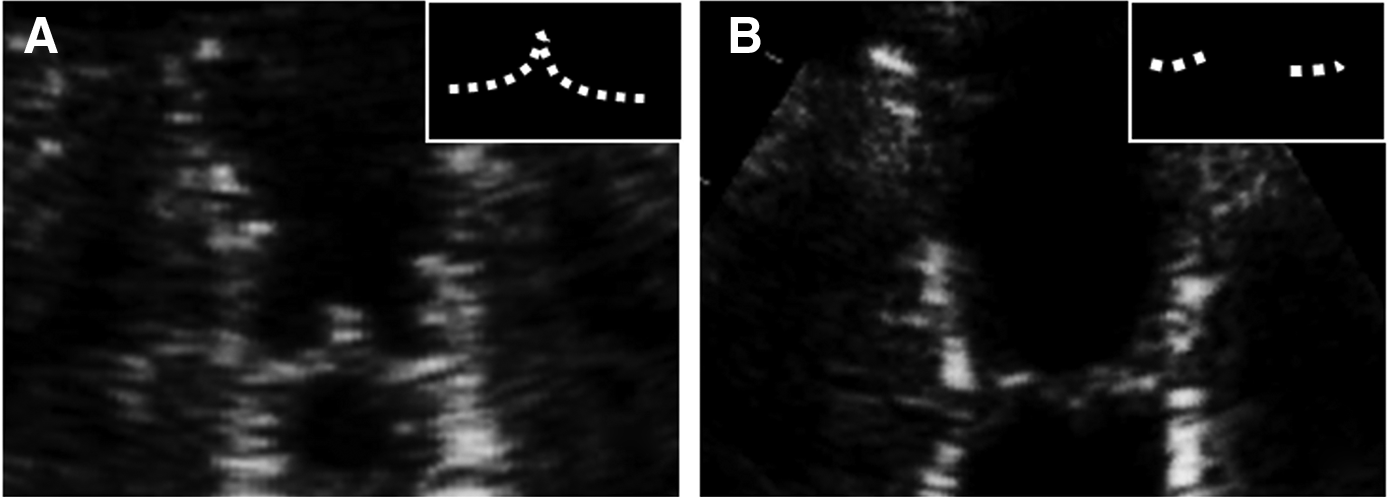
The dynamic performance of TEHVs in the bioreactor was estimated by the M-mode ultrasound as shown in Figure 5, where opening/closing cycles are displayed. The M-mode shows how the structures intersected by a single line placed along the area of interest on a 2D image move toward or away from the probe over time. Specifically, the positions along the dotted line in Figure 5A were followed in time. By checking the central point where the leaflets meet, it is possible to estimate opening and closing times of the valve during a specific conditioning protocol. Analysis of the ascending slope showed that the valve took approximately 0.04 s and 0.01 s to open and close, respectively. The open and closed phases lasted 0.36 s and 0.38 s, respectively. In addition, irregularities in the leaflets' movement can be detected such as in the case of Figure 5 where, circled, a small, but noticeable leaflet reverberation could be detected in the valve closed phase.

M-mode to evaluate valve's dynamic performance.
Material suitability
Figure 6 shows ultrasound images of a silicone tube positioned within a flow chamber visualized with the probe in direct contact with the chamber medium (water) (Fig. 6A) or through an insert of PMMA (Fig. 6B), POM (Fig. 6C), PVC (Fig. 6D), glass (Fig. 6E), and silicone (Fig. 6F). The images show that it was possible to obtain the longitudinal cross-section of the silicone tube through all the materials, with glass presenting the highest noise and capture complexity.
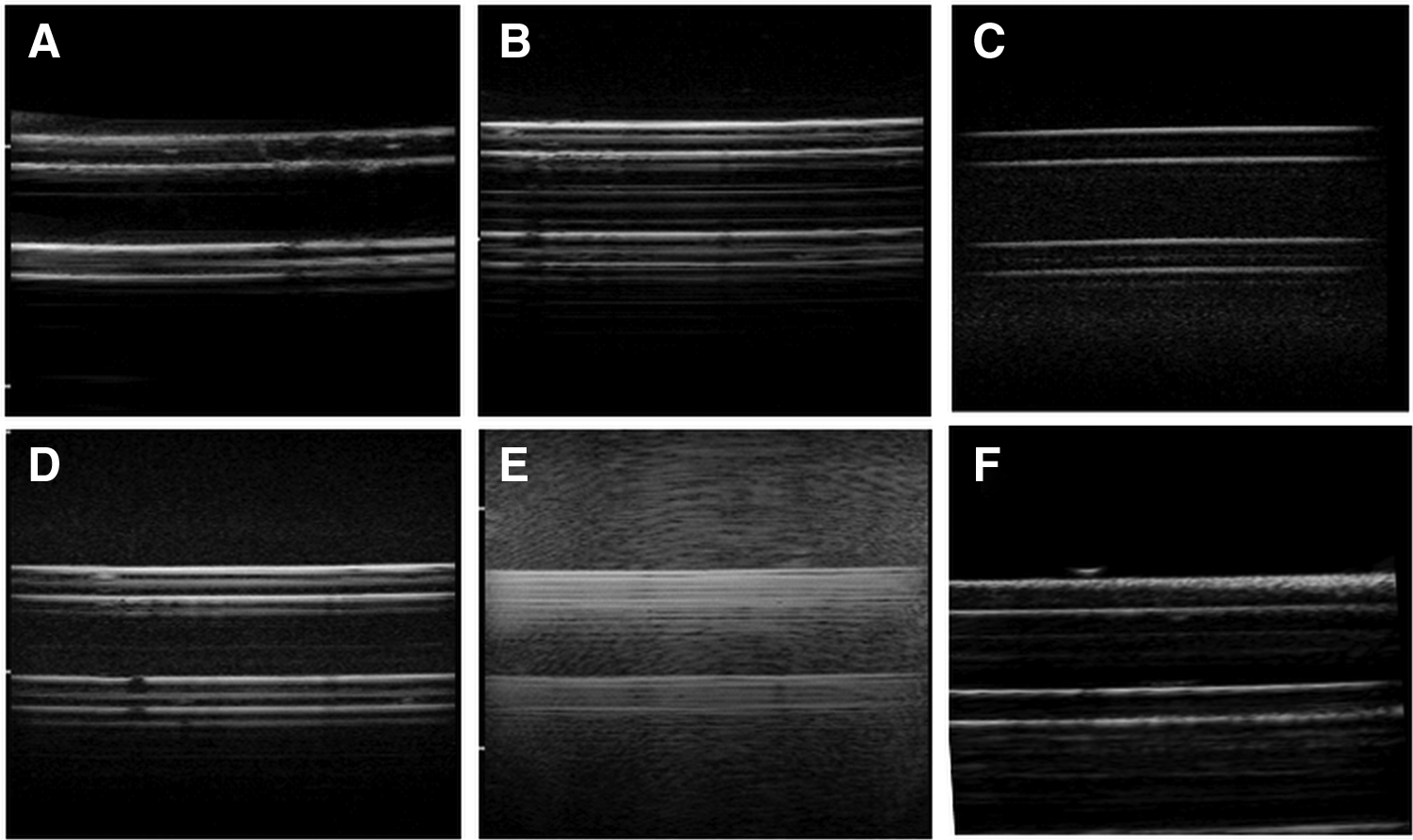
Ultrasound images of a silicone tube through
Discussion
In this study, we have proposed the use of ultrasound for noninvasive in vitro monitoring of TEHVs as a valuable tool to further advance their development, from the design to the maturation process.
TEHVs are normally imaged optically from the outflow side (Fig. 2A, B) to gain information on the symmetry of the leaflets during opening and closing, the GOA, and, if a high speed camera is used, on the closing and opening times, which can be calculated by counting the frames needed for such events. Although this is undoubtedly valuable information, it is limited to the plane of view and does not provide information on the 3D geometry of the valve or its evolution during the maturation process. By ultrasound imaging, exactly the same view, and therefore information, can be gained (Fig. 2C, D), for example, with a linear probe positioned on the side of the bioreactor so that the beam intersects the valve transversally. In this way, the GOA can be estimated even in bioreactors that do not have a direct vertical line of sight.
Furthermore, by simply changing the beam orientation by rotating the probe 90°, the valve can also be monitored in the longitudinal plane (Fig. 2E, F). This gives the possibility to benefit from the vast clinical ultrasound data on heart valves for the evaluation of TEHVs according to criteria otherwise not taken into account. For example, the longitudinal view allows to determine whether the cusp coaptation is above the annular plane, whether the effective cusp height is >8 mm, and whether the coaptation length is >4 mm, all three of which are predictors of aortic valve repair durability. 25 Furthermore, geometry-based criteria suggested as guidelines to obtain functional valves can be verified.26,27
Such considerations can help greatly not only during the design phase of the valve but also during its in vitro maturation. For TEHVs, it is, in fact, of paramount importance to follow their evolution during the remodeling process. Again, the longitudinal view is crucial for the evaluation of the changes in geometry due to cell-mediated tissue contraction,28,29 a well-known phenomenon that leads to valvular insufficiency. This can be clearly observed in Figure 3 where a reduction to 45% of the original leaflet length was estimated. The ultrasound longitudinal monitoring showed that the leaflets lost their original 3D shape for a more planar geometry and shortened in the radial direction similar to what was shown in vivo by ultrasound when decellularized TEHVs were implanted in the sheep model. 30
The ability to observe and quantify tissue shrinkage at different stages during conditioning can be extremely valuable in evaluating the efficacy of strategies employed to combat it and prevent valvular failure (e.g., adjusting conditioning protocols and changing valve design and scaffold's constituent concentrations).
The capabilities of ultrasound imaging have increased enormously with the introduction of Doppler techniques reaching a new powerful way to noninvasively evaluate valvular heart disease and cardiovascular hemodynamics. 31
These techniques rely on the frequency shift of the ultrasound signal when reflected by a moving object. The shift is a function of the cosine of the angle between the direction of movement and the ultrasound beam. Therefore, the optimal situation is when such an angle is 0°. However, ultrasound devices like the one used in this study have the capability to electronically steer the beam, so that even in the least convenient case with a 90° angle between the flow and the beam, information on the flow direction can be obtained. We were, therefore, able to visualize the unobstructed opening during systole, complete coaptation, and absence of regurgitation during diastole by positioning a linear probe on the sidewall of the bioreactor (Fig. 2G, H). However, in the case of a close to 90° angle between the flow direction and the ultrasound beam, it is not possible to measure the flow velocity correctly.
An ad hoc developed bioreactor could then foresee a chamber featuring a slanted wall with respect to the chamber's central axis. Ideally, the correct measurement is achieved by a phase array transducer positioned on top of the bioreactor so that the beam is aligned with the flow. The PWD allows determining the velocity profile as a function of time in a defined ROI (Fig. 4). The operator defines the ROI on the 2D ultrasound as a small segment along the ultrasound beam. In this way, the flow velocity can be measured locally at desired points. We could measure a peak flow velocity of 1.75 m/s, which is well within the physiological range measured in adults. The velocity profile gives an evaluation of the dynamic performance; in the case of Figure 4, the valve was closing properly with limited regurgitation and physiological peak flow velocity. For higher velocities (>2 m/s), the continuous Doppler mode must be used to correctly measure the flow.
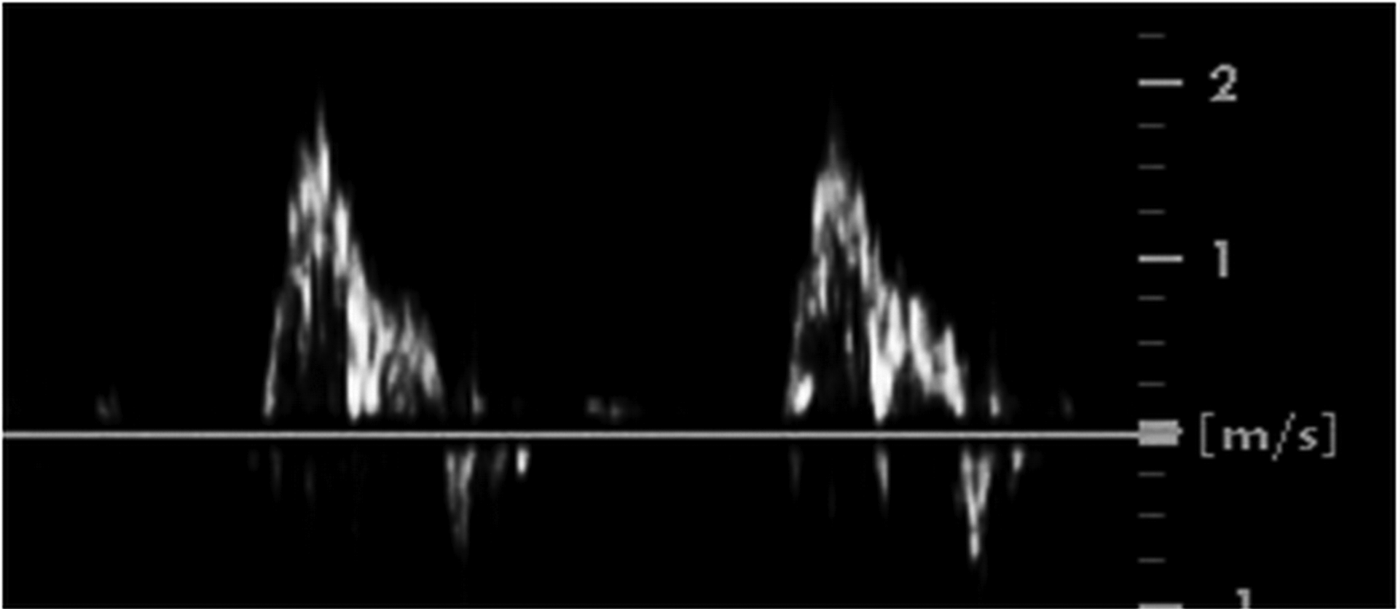
Flow profile by pulsed wave Doppler monitoring of a TEHV inside the bioreactor system.
The potential of ultrasound in the CFI mode was shown by the evaluation of a new TEHV designed for transcatheter delivery 22 in the initial stage of development. Paravalvular leakage was detected during conditioning (Fig. 2I, J) and attributed to the unsatisfactory suturing procedure at the annulus; after optimization of the procedure, the valve showed no paravalvular leakage (Fig. 2K, L). Identifying a design problem at this stage saves time and effort and critically helps to guide the progress of valve development. This is yet another case in which the information could not be gained through a conventional optical inspection.
The M-mode is commonly used in cardiac and fetal cardiac imaging to analyze moving tissue because of the good temporal resolution.32–34 In our study, we could determine the closing/opening times and velocities of a TEHV as important parameters describing the valve functionality 35 and point out irregularities in the closing behavior. In the example shown in Figure 5, the postprocessing determined opening and closing times of 0.04 and 0.01 s, respectively.
In this study, the bioreactors were made in PMMA, one of the materials of choice in our group because of its noncytotoxicity, transparency for optical monitoring, machinability, and compatibility with sterilization procedures. However, the ultrasound monitoring is not limited to this specific case and can be generally applied to bioreactors in use in tissue engineering laboratories. Indeed, bioreactor components made of other polymeric materials are also receptive to ultrasound as shown in Figure 6.
Ultrasound imaging can, therefore, be applied to systems that were not specifically developed for this application, even if they are made of opaque materials such as POM or the PVC used in this study, provided that a careful image calibration (i.e., contrast, frequency, and brightness adjustments) is performed. Glass showed a high level of noise, making it not the preferred material of choice.
In any case, air gaps between the ultrasound probe and the ROI must be avoided. This is because the majority of the ultrasound beam will be reflected at any interface between air and other media, making imaging below that interface impossible. This issue is avoided at the probe location by coupling the probe to the external bioreactor surfaces with ultrasound gel, as commonly done in clinical practice.
Within the bioreactor, where for compliance reasons, an air–medium interface is normally present, one possible solution is to completely fill the chamber housing the valve with medium and consign the air–medium interface to a secondary compliance chamber. An alternative solution, as adopted in this study (Fig. 1), is a chamber lid featuring a compartment descending below the level of the medium to break the air–medium interface. This is equally beneficial for the acquisition of optical images.
Further aspects in the bioreactor designs should be taken into account when the use of ultrasound is foreseen as a monitoring method to improve the quality. Valve holders should be minimized to avoid the formation of artifacts; similarly, a reduction of the bioreactor's wall thickness would be beneficial, as well as the presence of dedicated windows to enable accurate and reproducible positioning of the ultrasound probe, as close as possible to the valve. In this way, probes with higher frequencies could be used to gain better resolution.
Besides those enabled by the probes used in this study, there are other imaging modalities that could be applied to a bioreactor system, such as 3D imaging, tissue Doppler, and speckle tracking. Furthermore, because of the crucial importance of ultrasound monitoring in clinical practice, new systems and algorithms are continuously developed and improved. However, the affordability of such sophisticated systems for a tissue engineering laboratory, together with the need of the expertise to operate them properly, has to be evaluated with respect to the additional value that might be gained.
In conclusion, the potential benefits of ultrasound diagnostics for monitoring TEHVs in vitro have been explored in this study, showing possible applications of the different ultrasound modes. The use of ultrasound diagnostics, in conjunction with optical monitoring, offers a more complete nondestructive and noninvasive analysis of TEHVs function. The ability to visualize tissue shrinkage, assess flow profiles, and analyze leaflets' behavior can further accelerate improvements in the design and conditioning of TEHVs. While not explored in this study, ultrasound also has the potential to monitor in vitro extracellular matrix development in tissue-engineered constructs as previously investigated by our and other groups.36–39 Another interesting aspect enabled by ultrasound monitoring is the investigation of calcification potential of TEHVs in model systems for rapid ex vivo calcification and eventually the evaluation of anticalcification therapies. 40
Footnotes
Acknowledgments
The research leading to these results has received funding from the People Programme (Marie Curie Actions) of the European Union's Seventh Framework Programme FP7/2007–2013–ITN “TECAS” under REA grant agreement no. 317512 and from the START-Program of the Medical Faculty of RWTH Aachen University [Fond No. 691348].
Disclosure Statement
No competing financial interests exist.