
Abstract
The three-dimensional (3D) printing of large-volume cells, printed in a clinically relevant size, is one of the most important challenges in the field of tissue engineering. However, few studies have reported the fabrication of large-volume cell-printed constructs (LCCs). To create LCCs, appropriate fabrication conditions should be established: Factors involved include fabrication time, residence time, and temperature control of the cell-laden hydrogel in the syringe to ensure high cell viability and functionality. The prolonged time required for 3D printing of LCCs can reduce cell viability and result in insufficient functionality of the construct, because the cells are exposed to a harsh environment during the printing process. In this regard, we present an advanced 3D cell-printing system composed of a clean air workstation, a humidifier, and a Peltier system, which provides a suitable printing environment for the production of LCCs with high cell viability. We confirmed that the advanced 3D cell-printing system was capable of providing enhanced printability of hydrogels and fabricating an ear-shaped LCC with high cell viability. In vivo results for the ear-shaped LCC also showed that printed chondrocytes proliferated sufficiently and differentiated into cartilage tissue. Thus, we conclude that the advanced 3D cell-printing system is a versatile tool to create cell-printed constructs for the generation of large-volume tissues.
Introduction
T
We developed a multi-head tissue/organ building system (MtoBS) and reported fabrication of a 3D cell-printed structure for regeneration of osteochondral and ear tissue by dispensing a cell-laden hydrogel in the desired position according to the geometrical and anatomical properties of the target tissue. 11 One study used 3D cell-printing systems and various cell types to regenerate composite tissue; however, the resulting tissues were of a simple shape. 9
Human tissue/organs have various shapes and sizes. In particular, defective or recycled tissue/organs are much larger than any artificially fabricated constructs produced to date for tissue regeneration.12,13 Native tissue-mimetic cellular constructs with dimensions larger than 3.8 × 3.8 × 3.8 mm3 can be classified as large-volume cell-printed constructs (LCCs).14,15 Conceptually, several tactics to create LCCs have been developed; however, there are few reported studies on the subject. One reason why LCCs have not been created widely is the absence of established fabrication conditions for making constructs, controlling the appropriate factors.
The fabrication of LCCs with sizes that are similar to human tissue/organs requires establishing various factors, such as process duration, residence time, and hydrogel temperature. In the fabrication of LCCs, the prolonged fabrication process and residence times cause reduced cell viability and lower the proliferation and differentiation capabilities of the cells. In extrusion- or inkjet-based cell-printing technology, most encapsulated cells are exposed to the hydrogel solution. This is a harsh environment for cell survival during construct fabrication, because evaporation phenomena from the previously printed cell-laden hydrogel during the long-term printing process may have bad effects on cellular behaviors. 16 In addition, cells on the bed of the 3D cell-printing system are exposed to harsh conditions and can readily become contaminated. 17 Despite this, the printed cells survive and exhibit high levels of proliferation and differentiation both in vitro and in vivo, enabling regeneration of the target tissue. Thus, an environment for 3D LCC fabrication that maintains a high level of cell viability, proliferation, and differentiation is required.
In the current study, an advanced MtoBS, composed of a clean air workstation, a humidifier, and a Peltier system, was developed to provide a suitable fabrication environment for tissue formation in LCCs. In addition, factors that were important for the fabrication of LCCs with high cell viability, such as process duration, residence time, and hydrogel temperature, were determined. The suitability of the fabrication conditions was assessed by using live/dead and cell proliferation assays. An ear-shaped LCC was fabricated by using the optimum fabrication conditions; the ear-shaped LCC enabled chondrogenesis in vivo, suggesting the successful establishment of a method for fabricating LCCs for the regeneration of target tissue/organs.
Materials and Methods
Materials
Polycaprolactone (PCL, molecular weight 70,000–90,000 Da; Polyscience, Inc.), 4% w/v alginate (Sigma-Aldrich), and 2% w/v porcine ear cartilage-derived decellularized extracellular matrix (ear-cdECM) were used as a framework for production of hydrogels.
Porcine ear cartilage from a 6-month-old pig was obtained from a nearby slaughterhouse and used with the approval of the supplier. Ear cartilage tissue decellularization was carried out by using a method previously described, with slight modifications.18,19 Briefly, ear cartilage tissues were cut into pieces of ∼1 mm thickness. The chopped tissues were placed into hypotonic Tris-HCl buffer (10 mM Tris-HCl; pH 8.0) and underwent three cycles of freezing (−80°C) and thawing (37°C). The cartilage slurry was treated with 0.25% trypsin in phosphate-buffered saline (PBS) at 4-h intervals for 24 h at 37°C. The trypsinized cartilage slurry was washed with a hypertonic buffer solution (1.5 M NaCl in 50 mM Tris-HCl; pH 7.6) and treated with nuclease solution (50 U/mL DNAse and 1 U/mL RNAse A in 10 mM Tris–HCl; pH 7.5) at 37°C for 4 h to remove enzymes. The treated cartilage slurry was washed with 1% Triton-X-100 solution for 24 h and then placed in 10% 3-[(3-Chloamidopropyl)dimethyl-ammonio]-1-propanesulfonate (Biosesang) for 24 h. The decellularized cartilage slurry was washed with PBS at 6 h intervals for 3 days. The slurry was then lyophilized overnight by using a lyophilizer, Labconco Freezone 2.5 (Labconco). The lyophilized ear-dECM powders were added to 0.5 M acetic acid and 2 mg/mL pepsin in pure water for 48 h. A pre-gel solution of ear-dECM (pH 7.4 with 10 M NaOH) was prepared for encapsulating and printing cells.
Cell culture and bioink preparation
Human auricular chondrocytes were isolated from auricular cartilage tissues (tragus) of a patient (man, 21 years). This procedure was approved by the Institutional Review Board of the St. Mary's Hospital, The Catholic University of Korea. More specifically, human ear cartilage tissues obtained after surgery with the informed consent of the patient were chopped into pieces that were ∼1 mm in thickness and subjected to digestion at 37°C with 0.15% collagenase for 12 h while shaking at 300 rpm. Human auricular chondrocyte solution was filtered through 100-μm cell strainers and isolated by centrifugation at 2000 rpm (917 g) for 10 min.20,21 The isolated chondrocytes (1–3 × 105 cells/mL) were seeded in a 100 mm cell-culture dish and subcultured every 2–3 days for 1 week in Dulbecco's modified Eagle's medium (DMEM; Gibco BRL) containing 10% fetal bovine serum (FBS; HyClone, GE Healthcare Life Sciences), 1% penicillin–streptomycin (Thermo Fisher Scientific), 40 μg/mL
Confluent auricular chondrocytes were detached by using 0.05% trypsin containing 0.53 mM ethylenediaminetetraacetic acid for 3 min at 37°C. The cell pellet was collected by using centrifugation at 1000 rpm (229 g) for 5 min (1580 MGR; Gyrozen). 11 The collected cells were suspended in 10 × DMEM containing 10% FBS and gently mixed with 2% ear-cdECM (pH 7.4) while avoiding unwanted bubbles and gelatin. A final cell density of 5 × 106 cells/mL was reached. The cells encapsulated in 2% ear-cdECM pre-gel were printed in the desired positions on a porous PCL framework and thermally crosslinked in 5% (v/v) CO2 at 37°C for 1 h.
Advanced MtoBS
A previously reported 3D cell-printing system 9 was enhanced by the addition of a clean air workstation, a humidifier, and a Peltier system to produce 3D large-volume tissues/organs. A cell-printed construct on the bed of the 3D cell-printing system might become contaminated with airborne bacteria or fungi. We designed and installed a glove box (1300 × 1200 × 1618 mm; thickness, 12 mm) in the system, which functioned as a barrier to contamination (Fig. 1A). In addition, an high-efficiency particulate arrestance (HEPA) air filter was installed in the upper part of the glove box to filter and circulate the air (Fig. 1A). An ultraviolet lamp was installed in the MtoBS to sterilize the atmosphere. The humidity in the MtoBS is important to prevent drying of cells; therefore, a humidifier was installed to maintain >95% atmospheric humidity (Fig. 1B). A Peltier system consisting of a Peltier device, an insulator, a temperature sensor, and a controller was used to control the temperature of the cell-laden hydrogel. The Peltier system was installed in the bed and heads of the MtoBS and contained a water cooler to remove the heat generated by the Peltier module (Fig. 1B). The Peltier system facilitated controlling temperature in the range 0–40°C with an error of 0.1°C. The Peltier system in the bed enhanced construct shape by increasing the fidelity of the dispensed PCL line and controlling the temperature of the bed surface and surrounding air. The Peltier system in the heads improved printing fidelity and cell viability.

Design and development of
Performance evaluation
The surface temperature of the bed and heads of the MtoBS was measured by using an infrared thermography camera (FLIR E60; FLIR Systems) to evaluate its performance. To evaluate the bed temperature, the temperature controller was set to 6°C, 12°C, and 18°C and the temperature of the bed surface and printed PCL structure were measured (n = 3) at 2-mm intervals in height (Supplementary Fig. S1; Supplementary Data are available online at
The width of printed hydrogel lines was measured at 6°C, 12°C, and 18°C. A 4% alginate hydrogel and 2% ear-cdECM hydrogel solution were prepared. The two hydrogels were drawn into a plastic syringe and dispensed at a velocity of 0.00664 mm/s, corresponding to feed rates of 200, 600, and 1000 mm/min. Three hydrogel lines were dispensed. The width of a single printed line was measured by using a digital microscope (Dino-lite Premier). All tests were performed in triplicate.
Cell viability
To assess cell viability, 2% ear-cdECM hydrogel and human auricular chondrocytes were used. A cell-laden hydrogel was prepared by mixing 2 × 105 cells/mL suspension with hydrogel at a 1:10 ratio. The cell suspension solution was composed of 10 × DMEM (Gibco BRL) and 10% FBS (Gibco BRL). The chondrocyte-laden ear-cdECM hydrogel was drawn into a plastic syringe, and 18.5 μL was dispensed by using the MtoBS (n = 4) after residence times of 1, 2, 4, and 8 h at 6°C, 12°C, and 18°C. Residence time is the amount of time that the chondrocyte-laden hydrogel remains inside the plastic syringe. The 0 h residence time represents the control. After printing, the cell-laden hydrogel was incubated in cell culture medium (10% FBS, 100 U/mL penicillin [Gibco BRL], and 100 μg/mL streptomycin [Gibco BRL]).
Cell viability was assayed on day 1 by using a Live/Dead Kit (Lonza). Ethidium homodimer (EthD-1; 2 μL) and 0.5 μL calcein AM were mixed with 1 mL sterile PBS (Hyclone), added to the cell-laden hydrogel, and incubated for 30 min in 5% (v/v) CO2 at 37°C. 9 Live and dead cells were observed by using a confocal microscope (IX81; Olympus) as green (Calcein AM) and red (EthD-1) cells, respectively.
Printed chondrocyte-laden hydrogel was incubated in cell culture medium for 11 days, during which time the medium was changed 2–3 times per week. A Cell-Counting Kit-8 (Dojindo Laboratory) was used to measure the optical density of the cell-laden hydrogels to evaluate cell proliferation on days 1, 4, 7, and 11 (n = 4). 22
Fabrication of an LCC for ear regeneration
Ear-cdECM hydrogel (2%), chondrocytes (2 × 105 cells/mL), PCL, and poly(ethylene glycol) PEG were used to fabricate an LCC. A computer-aided design model was designed by using SolidWorks (ver. 2010; Dassault Systems) and MeshMixer (Autodesk Research) based on human ear computed tomography data for fabrication of an ear-shaped cell-printed construct, as previously reported. 22 Briefly, a porous framework of PCL was first dispensed, onto the secondary pores of which a cell-laden hydrogel was printed. Through a layer-by-layer process, an ear-shaped cell-printed construct with a PCL line width and a pore size of 250 and 1200 μm, respectively, was fabricated. The ear-shaped cell-printed construct was 40% smaller than a human ear. After fabrication, the ear-shaped cell-printed construct was crosslinked by incubating it at 37°C for 45 min and washed by using DMEM medium, which was replaced three times (i.e., every 15 min). A live/dead assay was used to evaluate cell viability on day 1. Live and dead cells were observed by using a combined confocal and multi-photon microscope (TCS SP5 II; Leica).
For evaluation of the two types of dispensed cell-laden hydrogel, MC3T3 (preosteoblast) cells were first labeled with DiO and DiI kits, and then encapsulated in 2% ear-cdECM hydrogel containing 2 × 106 cells/mL. An ear-shaped cell-printed construct was fabricated with a PCL framework and two types of cell-laden hydrogel. DiO- and DiI-labeled cell-laden hydrogels were printed in the cartilage and adipose tissue regions, respectively, and they were observed by using an inverted microscope with fluorescence equipment (Axiovert 200M; Zeiss). 11 The imaging results were obtained by scanning 126 pictures of the ear-shaped constructs in conjunction with × 4 magnification objective lens.
In vivo evaluation of an ear-shaped LCC
To confirm chondrogenesis, ear-shaped LCCs were fabricated by using PCL, PEG, and human auricular chondrocytes that were encapsulated in 2% ear-cdECM hydrogel (2 × 106 cells/mL) and subjected to in vivo evaluation for 8 weeks. The ear-shaped LCCs were implanted subcutaneously into nude mice (n = 3, female, 8 weeks old, average weight 15–20 g). The animal study protocols were approved by the IACUC of Pohang University of Science and Technology, Pohang, Republic of Korea (POSTECH-2015-0029). Routine antibiotics were prescribed preoperatively to prevent infection, and general anesthesia was induced with 50 mg/kg ketamine (Yuhan Co.) and 3 mg/kg xylazine (Bayer Korea Ltd.). To visualize cartilage regeneration, samples were harvested and fixed in 10% formaldehyde. The ear constructs were embedded in paraffin and sectioned (6-μm thickness). The sections were stained with hematoxylin and eosin (H&E) and Alcian blue, for type II collagen, and visualized by using an optical microscope.
Statistical analysis
Statistical analyses were performed by a one-way analysis of variance with post hoc Tukey's test by using MINITAB software version 14.2. Differences were considered statistically significant at a value of p < 0.05.
Results
Bed and head temperature distribution in the advanced MtoBS
Figure 2 shows the evaluation results of Peltier system performance with regard to the temperature in the bed and heads of a 3D cell-printing system. The bed of the system was cooled to the desired temperature with an error of 0.2–1.8°C (Fig. 2A). The surface temperature of the PCL structure at 2-mm intervals in height is shown in Figure 2B. The temperature of the bed was 6°C, and the PCL temperature increased by 2°C for each 2-mm increase in height. The temperature of the polymerase chain reaction structure was maintained at 15°C at >10 mm in height. The room temperature in the MtoBS was 20°C.

Performance of the Peltier system in the advanced 3D cell-printing system:
Figure 2C and D shows the air temperature in syringes when the Peltier system was set to 6°C, 12°C, and 18°C in heads of the MtoBS. At a set temperature of 18°C, the temperatures of the Z and B heads were 18°C with an error of 0.2°C for all three syringes. At a set temperature of 12°C, the temperatures in the normal and plastic syringes were 12°C with an error of 0.5–0.7°C, but the temperature in the glass syringe was 14°C. At a set temperature of 6°C, the temperatures in the normal and plastic syringes were 7.6–7.8°C, and the temperature in the glass syringe was 9.8°C. The temperature in the glass syringe was 8–10°C.
Evaluation of hydrogel printing performance
Figure 3 shows the line width of ear-cdECM and alginate hydrogels according to temperature (6°C, 12°C, and 18°C) and dispensing head speed (200, 600, and 1000 mm/min). First, the line width of the alginate and ear-cdECM hydrogel decreased with decreasing Peltier head temperature and increasing feed rate. The line width of the alginate hydrogel printed at 1000 mm/min was as follows: 317.9 ± 12.8 μm at 18°C, 279.6 ± 4.9 μm at 12°C, and 243.8 ± 2.0 μm at 6°C (Fig. 3, left panel). However, at 12°C and 18°C, the printed alginate hydrogel line width was reduced by printing at 200 and 600 mm/min. The minimum line width of the ear-cdECM hydrogel printed at 1000 mm/min decreased significantly while decreasing Peltier head temperature: 640.0 ± 12.8 μm at 18°C, 339.9 ± 12.2 μm at 12°C, and 188.5 ± 5.2 μm at 6°C (Fig. 3, right panel).

Line width using a 4% alginate hydrogel and 2% ear-cdECM according to temperature and feed rate. #Indicates p < 0.05 compared with 6°C, and *indicates p < 0.05 compared with 12°C. cdECM, cartilage-derived decellularized extracellular matrix.
Cell viability according to temperature and residence time
Figure 4 shows live/dead-stained images obtained on day 1 of cell-laden hydrogels printed at 6°C, 12°C, and 18°C with residence times of 1, 2, 4, and 8 h. In the control (0 h), >99% of cells survived (Fig. 4).
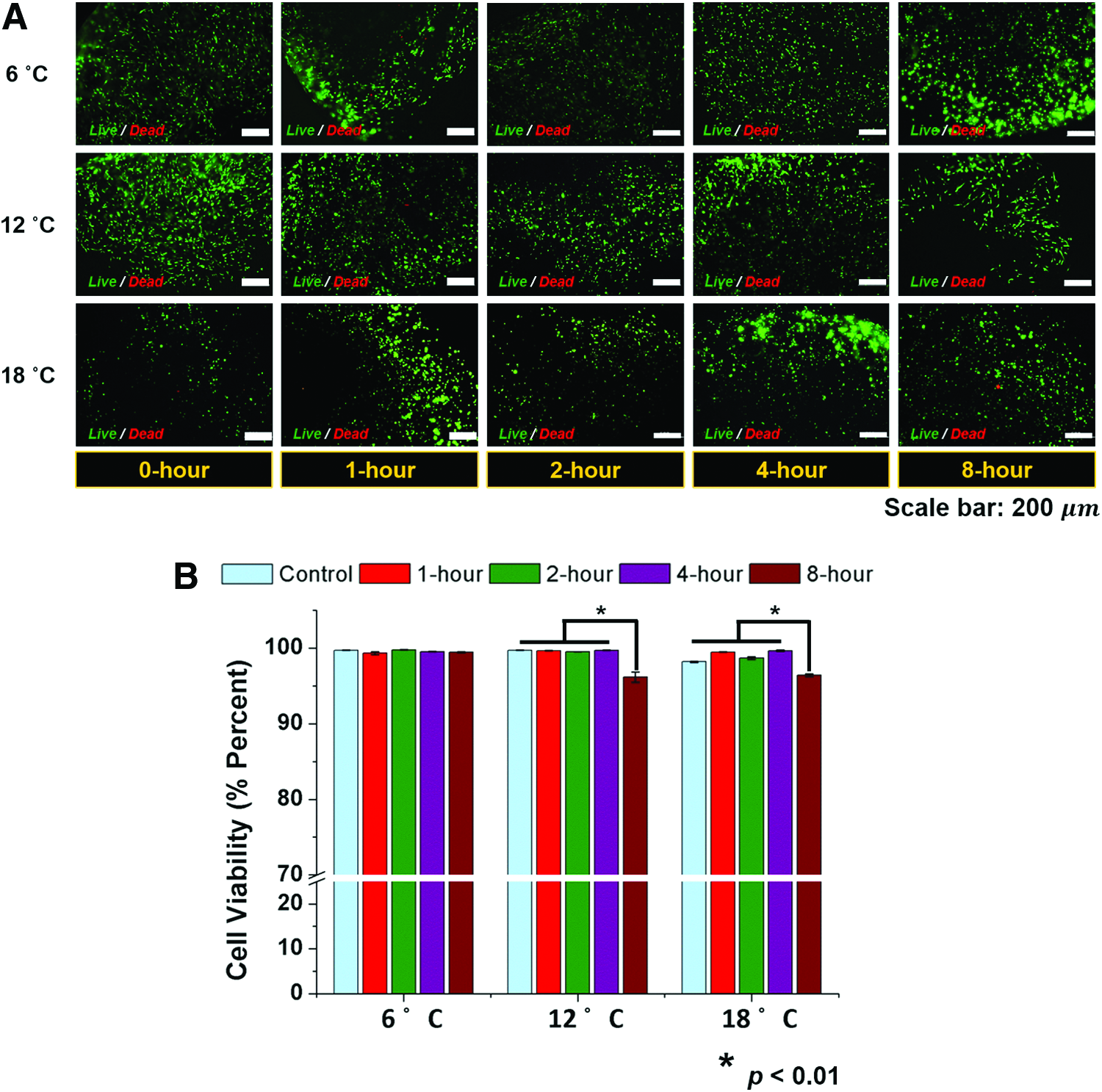
Live/dead-stained images of printed chondrocyte-laden hydrogels at 6, 12, and 18°C with residence times of 0, 1, 2, 4, and 8 h
Figure 5 shows chondrocyte proliferation in cell-laden hydrogels over 11 days according to residence time and temperature. Chondrocytes proliferated at 6°C regardless of residence time (Fig. 5A). However, with a residence time of 8 h, the proliferation rate at days 3–7 was lower than that for other residence times. Most chondrocytes proliferated well over 11 days (Fig. 5B, C); however, the proliferation rate for an 8 h residence time at 12°C and 18°C was lower than that for other residence times. In particular, the proliferation rate at days 7–11 for a 4 h residence time at 12°C was lower than that for residence times of 1 and 2 h. At days 7–11 at 18°C, the proliferation rates for 2, 4, and 8 h residence times were lower than those of the control and a 1 h residence time (Fig. 5C). Therefore, the optimum printing conditions were 6°C and the residence time was <4 h.

Chondrocyte proliferation over 11 days with residence times of 0, 1, 2, 4, and 8 h at
Fabrication of LCC for ear regeneration
An ear-shaped cell-printed construct was fabricated by using the advanced MtoBS (Fig. 6). An avascular construct (Fig. 6A) was fabricated with PCL and red and blue 4% alginate hydrogels, which were separately printed onto the cartilage and fat regions of the porous PCL framework. Two cell-laden hydrogels containing cells labeled with DiO (green) and DiI (red) were printed in positions corresponding to cartilage and fat regions (Fig. 6B). Figure 6C shows a live/dead-stained image of a cell-printed construct that was fabricated by using the optimum conditions; the majority of printed cells were viable. It indicates that the cell-printing process for 4 h might not adversely affect cell viability.
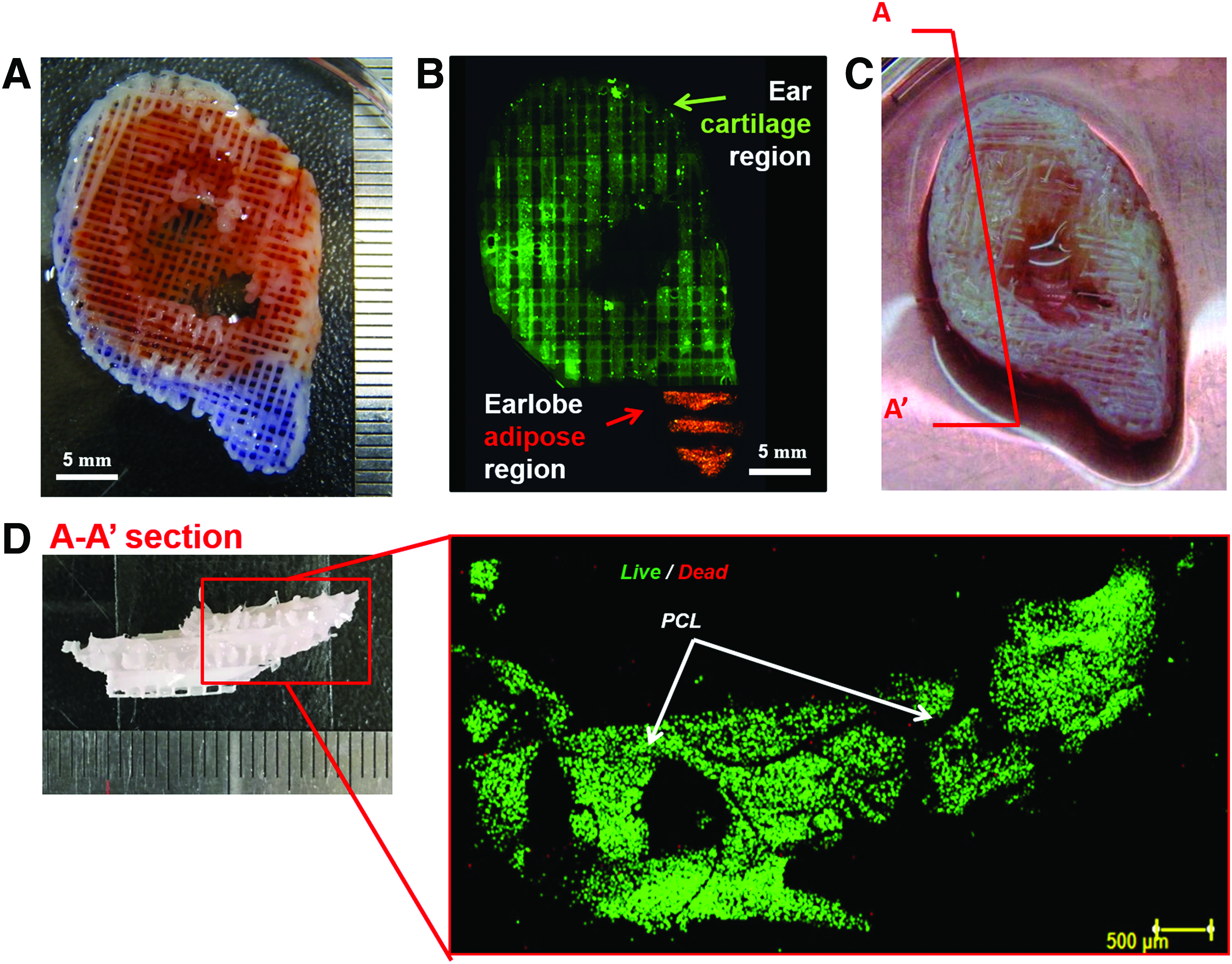
Fabrication of an ear-shaped LCC.
Histological analysis of in vivo ear regeneration
H&E, Alcian blue, and type II collagen staining of sections at 8 weeks showed chondrocytes undergoing chondrogenesis in the ear-shaped LCC (Fig. 7). A lacuna, which indicated cartilage regeneration, was formed, and glycosaminoglycan (GAG) was abundant in the region containing chondrocytes. Type II collagen production was also evident.

Histological and immunohistochemical images of an LCC at 8 weeks postimplantation.
Discussion
A cell-printed construct with a structure similar to the target tissue/organ plays an important role in the regeneration of human tissue/organs.23,24 Printing of various cell types depending on the composition of the target tissue is also required for appropriate construct functionality. In the fabrication of LCCs, maintaining high cell viability and using printed cells to regenerate the target tissue are essential. In this study, an advanced cell-printing system was developed to provide a suitable fabrication environment and to determine the factors that are important for the fabrication of LCCs with high cell viability, such as process duration, residence time, and hydrogel temperature. Based on appropriate fabrication factors, an LCC in the shape of an outer ear was fabricated and analyzed as an example for regenerating large-volume human mimetic tissue/organs.
The 3D cell-printing system was enhanced to enable the fabrication of LCCs. A clean air workstation, a glove box, a humidifier, and a Peltier system were added to the MtoBS to enhance cell survival. The glove box in the clean air workstation prevented contamination by outside air, and the HEPA filter installed in the glove box increased the air quality. The humidifier maintained high atmospheric humidity within the clean air workstation to prevent rapid evaporation of printed cell-laden hydrogel, thereby facilitating extended-duration fabrication.
The Peltier system controls the temperature of the MtoBS bed with an error of 0.15°C. A set bed temperature of 6°C resulted in cooling of the air in the 10-mm-layer directly above (Fig. 2B). This enabled cooling of the PCL filament immediately after being dispensed from the syringe (which is heated to 85°C), thereby enhancing the structural completeness of the construct. This also benefits the injection of hydrogels or cell-laden hydrogels by reducing the temperature of the syringe.
The construct pore shape and size are important for tissue regeneration.25–27 Also, controlling the hydrogel line width influences fabrication of tissue-like constructs. In particular, the width of a printed line of thermal-sensitive hydrogel is markedly affected by temperature. The minimum line width of thermal-sensitive hydrogels was investigated according to dispensing head speed and temperature, which was controlled by using the Peltier system (Fig. 3). At Peltier head temperatures of 6°C, 12°C, and 18°C, single hydrogel lines of a constant width were printed, which was likely because hydrogel viscosity increases with decreasing temperature.17,27 The line width of ear-cdECM differed significantly according to temperature, because the viscosity of collagen-based hydrogels is markedly affected by temperature. The hydrogel line width was controlled to 200 μm by controlling the printing-head temperature. In addition, the ear-cdECM hydrogel has greater ear-regeneration capability, because it is derived from porcine ear cartilage tissue and contains higher quantities of tissue components than do other gels.19,20 Maintaining a temperature of <15°C is essential for dispensing of the temperature-sensitive dECM hydrogel. 19 The Peltier system enables reproduction of the target tissue/organ by dispensing dECM materials. Moreover, the advanced MtoBS enables use of a wide range of printable hydrogels, increasing the likelihood of successful target tissue regeneration.
Fabrication of an LCC with the size of a human organ requires considerable time, which affects cell viability and proliferation. The following factors must be considered in the fabrication of LCCs: fabrication time, hydrogel residence time in the syringe, and the temperature of the bed and heads of the 3D cell-printing system.28,29 The advanced cell-printing system developed enables the fabrication of LCCs with high cell viability (Figs. 4–6). LCCs are fabricated as follows: A pore-containing structure is first dispensed and stacked five times at a height of 200 μm. Then, a cell-laden hydrogel is dispensed onto the pores 20 in a layer-by-layer manner, resulting in fabrication of an ear-shaped cell-printed construct (Fig. 6A). The fabricated construct then undergoes hydrogel crosslinking before incubation. Fabrication of the ear construct takes 160 min, and crosslinking 15–60 min, depending on the type of hydrogel used. The first cells printed during fabrication of the LCCs were exposed to the bed at 6°C and 12°C, and the last cells in the printing sequence were encapsulated in ear-cdECM solution in a syringe at 6°C for 2 h. The effect of this process on cell viability and reproducibility was then evaluated.
The majority of cells survived, regardless of residence time and temperature (Fig. 4). Moreover, the fabrication process did not affect cell viability. The cell proliferation rate at 6°C with a residence time of <4 h was similar to that of the control (Fig. 5). Cells printed at 18°C with a 4 h residence time survived but proliferated poorly. Therefore, the optimum conditions for cell proliferation were 6°C and the residence time was <4 h.
An ear-shaped cell-printed construct was successfully fabricated (Fig. 6). Red- and blue-labeled alginate hydrogels were independently dispensed on cartilage and fat tissue regions of a porous PCL structure by using the advanced MtoBS (Fig. 6A). In addition, green- and red-labeled cells were separately printed onto the cartilage and fat regions (Fig. 6B). Two percent of ear-cdECM was printed in the desired positions, and the human auricular chondrocytes encapsulated in the hydrogel survived and exhibited high viability (Fig. 6C, D). This proves that the advanced 3D cell-printing system includes an appropriate fabrication environment for cell-printed constructs without vaporization and high cell viability of the printed hydrogel. Thus, LCCs on which the majority of cells survived were produced successfully by using the advanced 3D cell-printing system.
Figure 7 shows the results of in vivo evaluation of an ear-shaped cell-printed construct that was fabricated by using the optimum conditions. The cell-printed constructs were implanted subcutaneously in nude mice and harvested after 8 weeks. An immunohistochemical analysis was performed to evaluate cartilage production. H&E staining showed that the cell-laden hydrogel was printed successfully, and the encapsulated chondrocytes exhibited chondrogenesis. Many lacunae were observed, and GAG and type II collagen were evident. Moreover, the ear-shaped cell-printed construct promoted chondrogenesis similarly to native cartilage tissue (Fig. 7). Therefore, cell printing using the advanced MtoBS enabled fabrication of LCCs with enhanced cell viability and proliferation, and that promoted tissue formation.
The construct fabrication time, cell-laden hydrogel residence time in the syringe, and the bed and head temperature influenced the fabrication of ear-shaped LCCs. An LCC fabrication method was also established in this study and demonstrated the potential to regenerate composite tissue similar to the target tissue/organ. This 3D cell-printing technology facilitates tissue generation by printing multiple cell types in the desired positions to mimic native tissue/organs.
Ideally, LCCs should contain a vascular network to facilitate tissue regeneration, because the cells in the LCCs can suffer from a hypoxic condition by the low oxygen level, particularly in those >1.5 mm in thickness. 13 It indicates that the vascular network in the fabrication of large cell-printed constructs would be necessary.30,31 Despite the challenge, we verified that few chondrocytes were dead in our cell-printed construct (Fig. 6). It is probably because our ear structure included varying shapes when observed in flanks, leading to the amelioration of medium penetration inside the construct. It could also influence the fact that the chondrocytes are relatively tolerant to low oxygen concentration compared with other cells. However, vascularization is indispensable in preventing cell death by hypoxia in engineered 3D LCCs.32–34 Thus, with the established printing conditions for long-term fabrication, several strategies based on 3D cell-printing technology will be required to construct vascularized human-scale tissues/organs in the future. Specifically, the vascularized large-volume constructs could be reconstructed by positioning vascular-related cells or vascular endothelial growth factor around the hypoxic region. 35 Still, such an approach may take several days in forming new blood vessels, probably resulting in cell death and dysfunction. As an approach to overcome such limitations, perfusable blood vessels have been recently engineered by using a coaxial cell-printing technique and printable sacrificial materials.36,37 This approach is also under investigation and is considered to be reported in the future.
In addition to the issue of hypoxia, FBS used in this study may not be suitable for clinical applications due to the regulatory bodies; therefore, FBS should probably be replaced with human serum in constructing human-scale tissues/organs in the future.
Conclusions
In this study, an advanced 3D cell-printing system was developed for the fabrication of LCCs. Moreover, the following factors were found to be important for the fabrication of an ear-shaped LCC: fabrication time, residence time, and temperature. The fabricated LCCs showed good cell viability, proliferation, and differentiation, and they promoted chondrogenesis, despite the long fabrication time. We also demonstrated that human-scale composite tissue could be regenerated by using the LCC fabrication method described here.
Footnotes
Acknowledgment
This work was supported by the National Research Foundation of Korea (NRF) grant funded by the Korea government (MSIP) (No. 2010-0018294).
Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.