
Abstract
Objective:
The aim of the present split-mouth study in sheep was to assess the influence of in situ hardening properties of a biphasic calcium phosphate (BCP) bone graft substitute (BGS) (ratio hydroxyapatite/β-tricalcium phosphate = 60/40) compared with a particulate BGS with the same biphasic core-granule composition without in situ hardening properties on sinus floor augmentation.
Materials and Methods:
Therefore, bilateral sinus floor augmentation was performed in eight sheep. Poly(lactide-co-glycolide) (PLGA)-coated, in situ hardening biphasic BGS (PLGA-NMP [N-Methyl-2-pyrrolidone]-BCP) was placed at the test site, and a particulate biphasic BGS without PLGA coating (BCP) was used for the contralateral site as a control. Animals were sacrificed after 21 weeks. Sinus augmentation sites were analyzed histologically. The volume was analyzed by computed tomography. Histomorphometric parameters were assessed for the 12 and 21 weeks' time points. Slopes of new bone formation over time were compared with a linear growth regression model.
Results:
Bone formation after 12 and 21 weeks of healing was 8.94% (±3.74) and 19.82% (±6.29) for PLGA-NMP-BCP and 7.00% (±2.58) and 14.38% (±4.51) for BCP, respectively. The bone growth rate for PLGA-NMP-BCP was higher than the growth rate for BCP (probability 97.5%). The total fraction of calcified hard tissue (% bone fraction + % biomaterial) was around 46% for both tested biomaterials, 21 weeks after sinus floor augmentation.
Conclusion:
The in situ hardening BGS (PLGA-NMP-BCP) performed better than the particulate material (BCP) in terms of bone formation rate. The in situ hardening properties of the PLGA-NMP-BCP material mediated by the PLGA coating and NMP solution as plasticizer had no negative influence on the bone formation.
Introduction
C
Most of these synthetic materials are available as granules below 1 mm so that they can be applied in any irregularly shaped defect site. However, the handling of granular BGSs may be cumbersome and containment of the granular graft material in the defect has to be assured with membranes in combination with mucoperiosteal flaps. Due to these shortcomings of granular BGS, in situ hardening materials have been developed (GUIDOR easy-graft CLASSIC and easy-graft CRYSTAL; Sunstar Suisse SA, Etoy, Switzerland).
These materials are composed of calcium phosphate particles that are coated with a thin layer of poly(lactide-co-glycolide) (PLGA). PLGA is a synthetic polymer that degrades by hydrolysis within weeks, and it is known to be well biocompatible.7,8 These PLGA-coated biomaterials are mixed with a temporary plasticizer, consisting of an aqueous N-Methyl-2-pyrrolidone (NMP) solution (BioLinker), which renders the materials soft and moldable. In the defect, body fluids remove the temporal plasticizer from the PLGA coating, and the material forms a solid but porous body in the defect.
This in situ hardening of PLGA-coated biomaterials showed good biocompatibility and bone formation in animal models 9 comparable to other BCPs as well as deproteinized bovine bone matrix material.10,11 However, the effect of the in situ hardening properties on the bone formation of calcium phosphate particles has not yet been addressed. It remains to be elucidated as to how far the in situ stabilization of the individual calcium phosphate particles within a PLGA lattice is advantageous in a specific anatomical location such as the maxillary sinus.
Therefore, the purpose of this study was to compare the performance of PLGA coated in situ hardening BCP particles for sinus augmentation with the uncoated control biomaterial in a sinus model in sheep.
Materials and Methods
Animal model
This study was approved by the federal animal trial council in Vienna. Eight female adult sheep weighing 80 kg were included in the study. All animals were kept under the same conditions and observed by a specialist for veterinary surgery.
A split-mouth design was chosen for the controlled parallel group study. The bilateral sinus floor augmentation (lateral approach) was performed by using 2.0 mL grafting material at each side.
Surgical procedure
All animals received preanesthetic medication consisting of midazolam 0.2 mg/kg, methadone 0.1 mg/kg, and ketamine 5 mg/kg intramuscularly. Anesthesia was induced intravenously with 2–4 mg·kg−1 propofol (1% Propofol; MCT Fresenius; Fresenius Kabi, Bad Homburg, Germany), followed by tracheal intubation. Anesthesia was maintained by using a mixture of oxygen and isoflurane (Forene; Abbott, Wiesbaden, Germany) at an end-tidal concentration of 1.8% in oxygen/air and a bolus of 0.002 mg (kg·h)−1 fentanyl citrate (Fentanyl-Janssen; Janssen-Cilag, Neuss, Germany) followed by continuous infusion of 0.001 mg (kg·h)−1 fentanyl citrate.
Mechanical ventilation was provided by an anesthesia ventilator (Julian; Dräger, Lübeck, Germany). Respiratory rates and inspired O2 concentration were adjusted to maintain endexpiratory CO2, tension between 38 and 42 mm Hg, and percutaneous O2 saturation between 95% and 100%. Intravenous Ringer's solution [10 mL (kg·h)−1] was administered continuously, to ensure the fluid balance. Postoperative analgesia was achieved with subcutaneous carprofen (Rimadyl; Pfizer, Karlsruhe, Germany) (4 mg·kg−1 in 24 h) for 4 days, and a first dose was given after the induction of anesthesia. Also, buprenorphine (Richter Pharma) 0.01 mg/kg 2–4 × daily was administered subcutaneously.
The sinus floor augmentation was done through an extraoral bilateral approach (lateral window) that is also described in the publication by Sauerbier et al. 12 The anterior wall of the maxillary sinus was exposed inferiorly to the lower orbital rim by mobilization of the masseter muscle and the adherent periosteum before preparing the lateral window.
The sinus received either of the following treatments: The left side was augmented with 2.0 mL test material that was activated with a plasticizer that was called BioLinker (5 × 0.4 mL GUIDOR easy-graft CRYSTAL; Sunstar Suisse SA), hereafter referred to as PLGA-NMP-BCP; the contralateral, right side was augmented with 2.0 mL control material (GUIDOR calc-i-oss CRYSTAL; Sunstar Suisse SA) that was mixed with physiological saline, hereafter referred to as BCP.
The PLGA-NMP-BCP biomaterial consisted of PLGA-coated porous BCP granules (granule size 450–1000 μm). Before application, the coated test granules were mixed with the plasticizer consisting of an NMP solution to render the material moldable. On application into the bone defect, blood extracted the NMP from the PLGA coating and the material hardened into an inherently stable graft body. The control material (BCP) was made of pure porous BCP granules (granule size 450–1000 μm). In both groups, the BCP core granules are composed of hydroxyapatite and β-TCP in the ratio 60:40.
The lateral window sites were covered with a resorbable dental membrane (GUIDOR bioresorbable matrix barrier; Sunstar America, Inc., Chicago, IL).
The wounds were closed with resorbable suture material, and the animals received analgesics postoperatively. All the surgeries were carried out by the same surgeon.
Computed tomography analysis
The volume of the augmented site was analyzed by the program Vitrea.fx-Software Version 6.3 of Toshiba VITAL based on radiological data from a computed tomography analysis of SOMATOM Definitions AS (Siemens Healthcare). Each test site was imaged twice, immediately postoperatively and after 21 weeks at sacrifice.
Fluorescence marking
The amount of newly formed bone was assessed for two time points (12 and 21 weeks) within the same animal and for all histological slides by labeling the new bone (NB) with fluorescent in vivo injections of calcein green during the first 12 weeks, detectable as fluorescent bone at sacrifice, and comparing the final amount of NB at sacrifice (21 weeks' time point) stained with Azur II and Pararosaniline.
Calcein green (Sigma-Aldrich, Item No. C 0875) for the fluorescent labeling of newly formed bone was injected into each sheep weekly during the first 84 days at a dose of 10 mg/kg body weight according to the method as described by Gutwald et al.13,14
Histological and histomorphometrical evaluation
At sacrifice after 21 weeks, the samples from augmented sites were fixed in formalin, dehydrated, infiltrated with resin (Heareus Kulzer, Hanau, Germany), and polymerized under ultraviolet (UV) light. Sections from the resin-embedded sinus were cut with a diamond micro saw (Microslice; IBS, Cambridge, GB, United Kingdom), placed on an acrylglas carrier (Maertin, Freiburg, Germany), and reduced to a thickness of 100 μm on a rotating grinding plate (Struers, Ballerup, Denmark).
Analysis of the fluorescent calcein markings of newly formed bone during the first 12 weeks was performed before staining the slices with Azur II and Pararosanilin (Axiovert 135; Carl Zeiss AG, Oberkochen, Germany; AnalySISLD Soft Imaging System; Olympus Europa GmbH, Hamburg, Germany). Three slides of each augmentation site per animal were prepared, one from the center of the graft and one each from the center of the halves. Evaluation was performed by a blinded investigator. This led to n = 24 data points from totally eight animals with three sections per augmentation site for each tested group, fluorescently discriminable for the 12 and 21 weeks' time points.
The tissue at the site of augmentation was described qualitatively: kind of tissue found in the augmented sites, signs of bone formation and remodeling (osteoclasts/osteoblasts), and signs of inflammation or foreign body reactions.
The following parameters were evaluated histomorphometrically for each histological slide: % NB, % residual biomaterial (RB), and % connective tissue (CT).
Statistical analysis
Three slices per site were analyzed to protect against sampling randomness. For the parameters, NB, RB, and CT, values were expressed in percentage of the evaluated area. The primary endpoint was a comparison of bone growth between the control (BCP) and the test group (PLGA-NMP-BCP) within a noninferiority protocol. Growth curves were analyzed with a Bayesian variant of the mixed model mentioned in the protocol with R 15 and R-package rstanarm. A linear growth regression model was used. Bayesian analysis gives 95% credible intervals (CrIs) for the difference in slopes and handles outliers gracefully. The correlation of bone growth due to nesting was taken into account as random effects in the model. 16 Ordering sequence of slices was not used; slices were treated as within-site repeats. The growth rate was defined by the percentage of NB per week and was weighted in the model to take into account the nesting structure imposed by the split-mouth design and the multiple slices per site. The growth curve shown is the population mean computed from the Bayesian posterior. In all plots, data were jittered randomly in the horizontal direction around the exact values of 12 and 21 weeks to better separate overlapping points.
Results
Bilateral defect creation and the augmentation procedures were performed without any intraoperative complications for both biomaterials in all eight animals. Likewise, the postsurgical healing was generally uneventful; thus, all animals (n = 8) could be evaluated throughout the whole study period of 21 weeks. At the time of animal sacrifice, there were no signs of wound dehiscence, infections, or any other healing complications.
The clinically observed good healing process was further corroborated by the histological findings. Newly formed bone occupied 8.94 ± 3.74% of the area of interest at the PLGA-NMP-BCP site and 7.00 ± 2.58% at the BCP site after 12 weeks. At 21 weeks, the histomorphometric analysis revealed the percentage of bone in the newly formed tissue to be 19.82 ± 6.29% with PLGA-NMP-BCP and 14.38 ± 4.51% with BCP, respectively (Fig. 1).
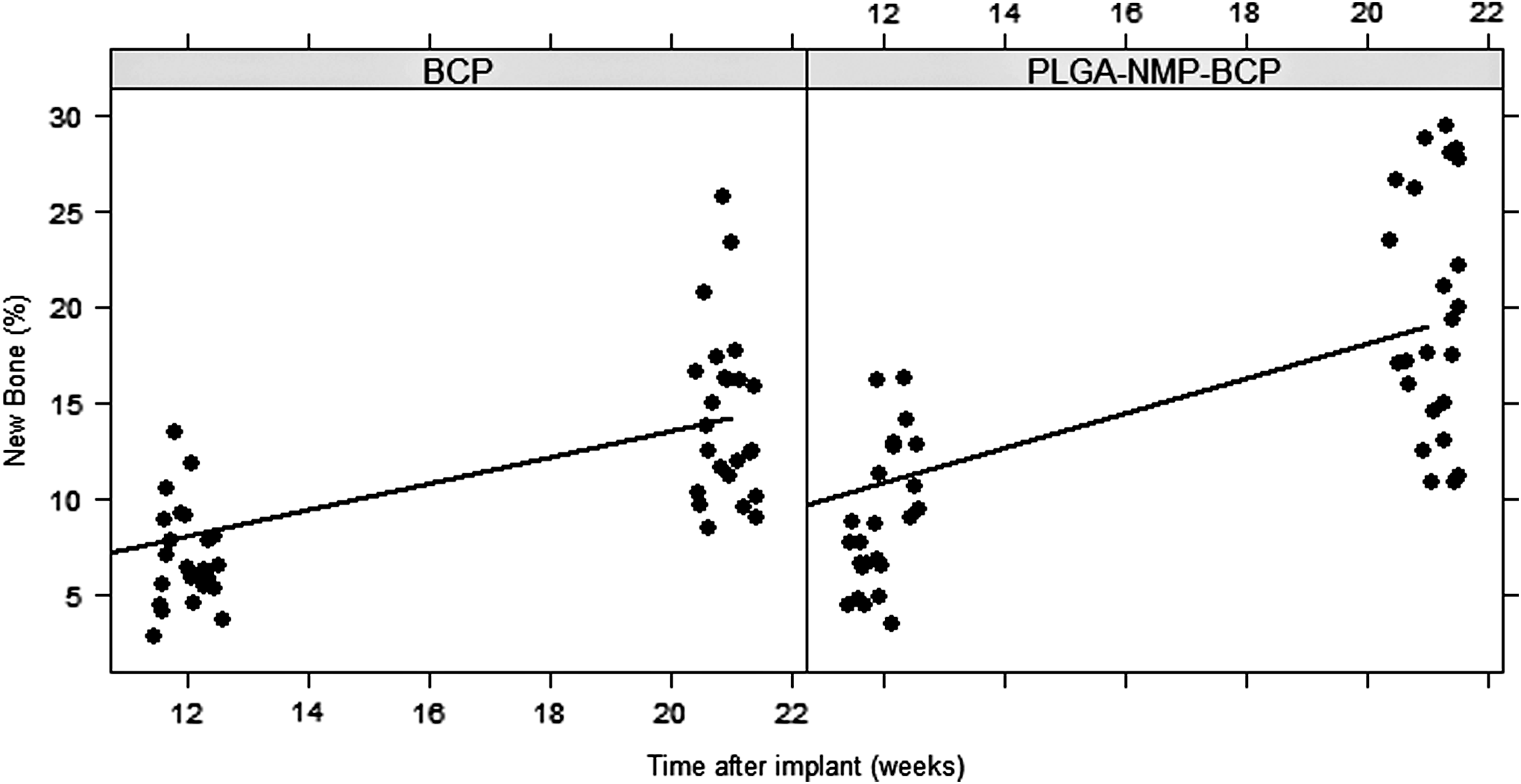
Sinus grafting new bone formation; the solid line shows the prediction from the regression model. Each point corresponds to one slice. Data jittered horizontally to better separate overlapping points. BCP, biphasic calcium phosphate; NMP, N-Methyl-2-pyrrolidone; PLGA, poly(lactide-co-glycolide).
Applying a linear growth regression model, with the assumption that the amount of NB at the day of surgery was zero, and analyzing the differences in the slopes, it was found that the mean bone growth with PLGA-NMP-BCP was 0.91% per week, with a 95% CrI of 0.79–1.04%. With BCP, the mean bone growth was 0.67% per week, with a 95% CrI of 0.54–0.81%. Therefore, according to the Bayesian analysis, the bone growth rate was faster in the PLGA-NMP-BCP group than in the BCP group (97.5% probability).
Connective tissue/bone marrow values were found to be 64.01 ± 4.50% and 53.13 ± 6.70% for PLGA-NMP-BCP at 12 and 21 weeks, respectively, and 60.77 ± 3.74% and 53.38 ± 4.87% for BCP at 12 and 21 weeks, respectively (Table 1). The connective tissue (CT) fraction decreased with −0.82% per week in the BCP group (CrI −1.26% to −0.38% per week) over the period of the investigation. In the PLGA-NMP-BCP group, mean CT change was noncredibly different by −0.39% per week (CrI −1.00% to 0.23% per week) compared with the BCP group.
These were computed from raw data and might differ slightly from the data given in the detail sections.
BCP, biphasic calcium phosphate; BR, biomaterial residuals; CT, connective tissue; NB, new bone; NMP, N-Methyl-2-pyrrolidone; PLGA, poly(lactide-co-glycolide).
The biomaterial fraction at 12 weeks could not be evaluated directly because, based on the injected fluorescent marker, only fluorescently labeled tissue could be analyzed for this time point. However, as in both treatment groups only partially degradable BCP was used, it has to be presumed that the fraction of biomaterial did not change considerably from weeks 12 to 21 (see intact granular shape for both materials after 21 weeks, Figs. 2–4). For the PLGA-NMP-BCP group, biomaterial residual fractions were found to be 27.05 ± 3.44% at 21 weeks. The values of the contralateral sites were found to be 32.23 ± 3.81 for the BCP group, respectively (Table 1).
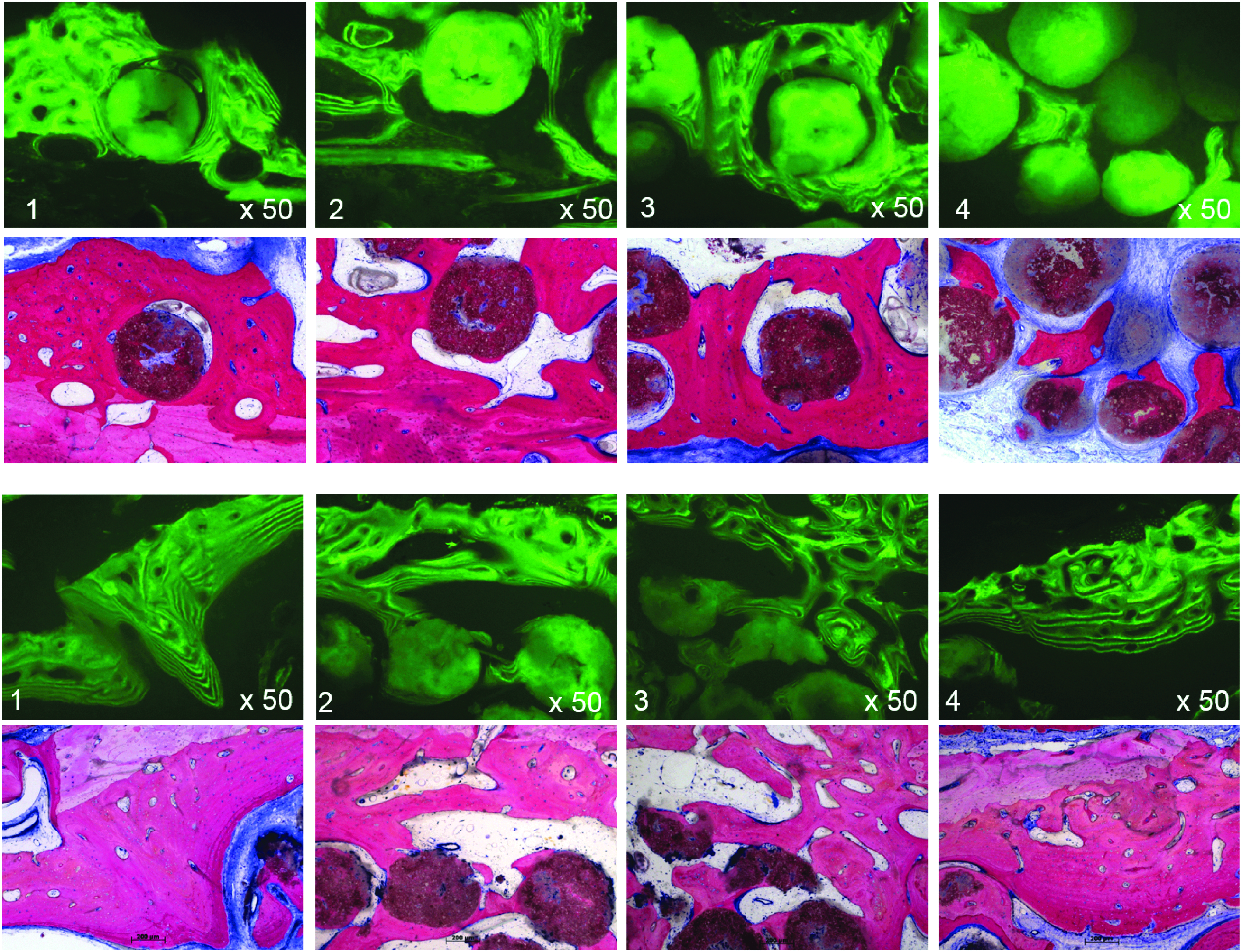
Comparison of fluorescence- and light microscopy details from histological sections showing the new bone formation in contact with the bone graft materials after 21 weeks. Upper two rows: BCP; lower two rows: PLGA-NMP-BCP.
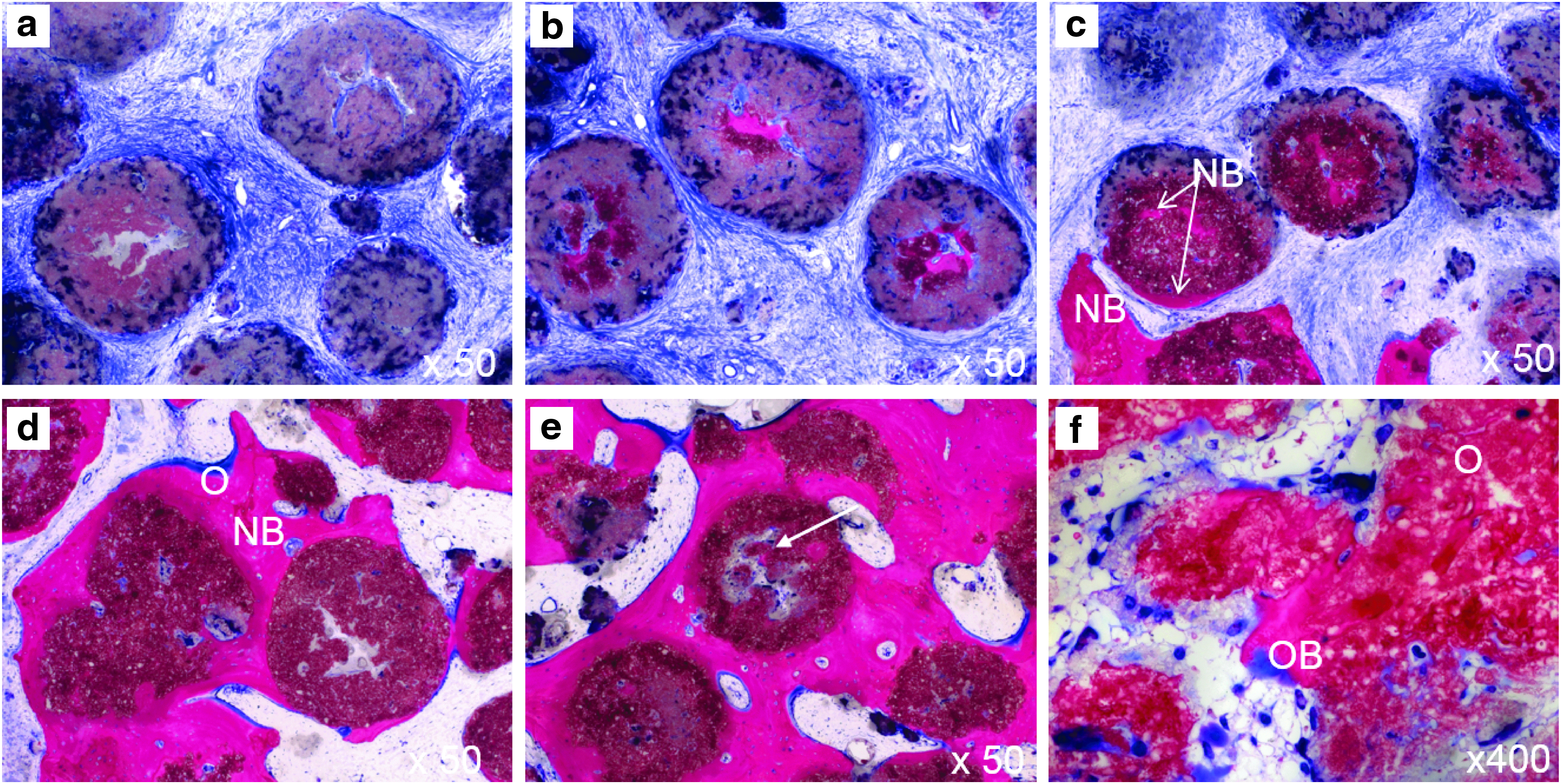
Histology illustrating the situation after 21 weeks with BCP.
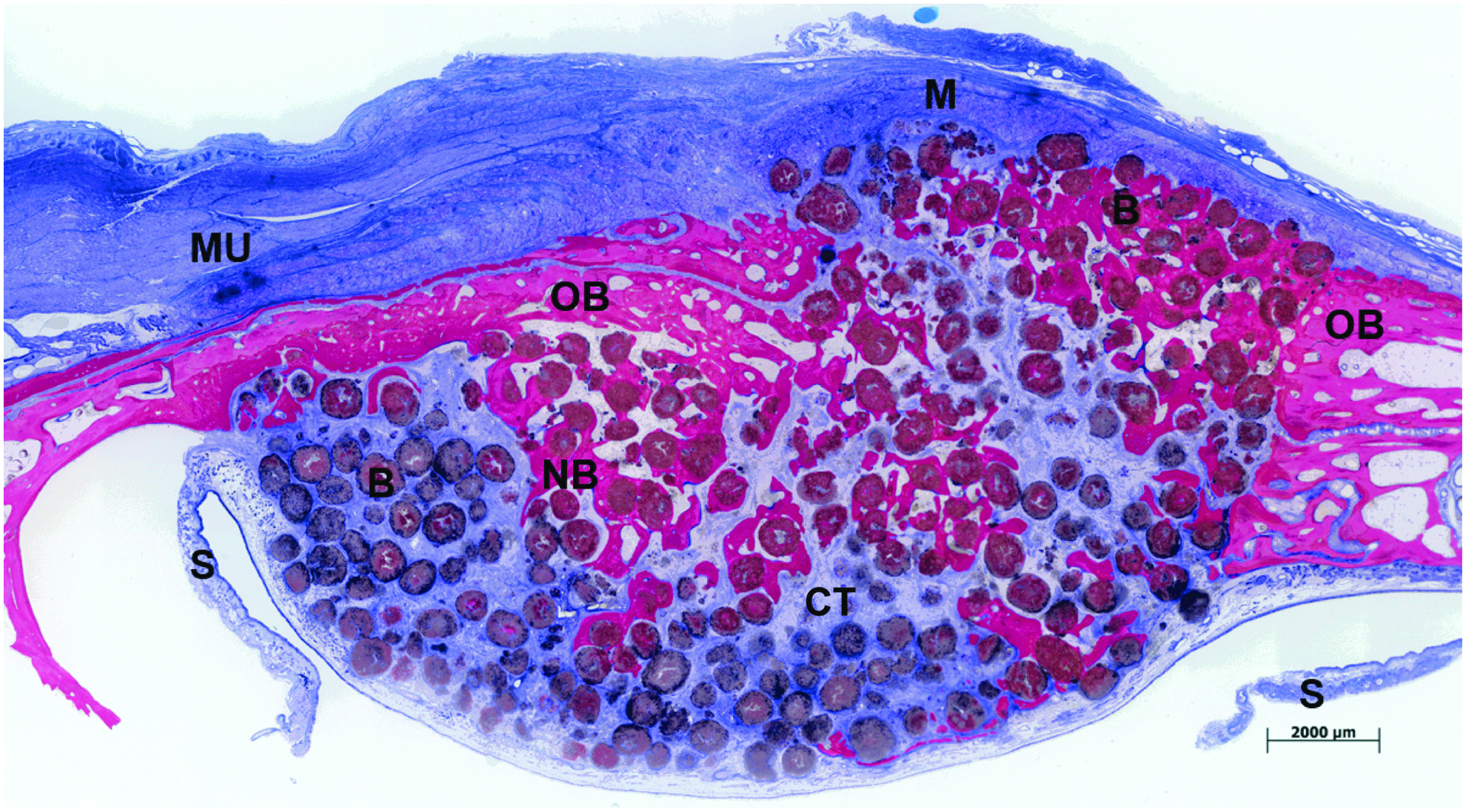
Ground section of histological sample illustrating the situation after 21 weeks with PLGA-NMP-BCP. Frontal slice through left maxillary sinus: membrane (M), biomaterial (B), newly formed bone (NB), old bone (OB), connective tissue (CT), muscle (MU), detached Schneiderian membrane (S) (nondecalcified tissue slices, stained with Azur II and Pararosanilin, assembled overview from single slices).
Histomorphometric analysis revealed that the CT reduced by the same amount as NB was formed in the time compared at 12–21 weeks in both treatment groups.
In summary, after 21 weeks of healing, the total amount of calcified tissue represented a fraction of 46.87% of the total area (19.82% NB, 27.05% biomaterial) with PLGA-NMP-BCP and 46.62% (14.38% NB, 32.23% biomaterial) of the total area with BCP (Table 1).
Histologically, all analyzed samples contained newly formed bone, RB, and well-vascularized uninflamed CT (Fig. 4). No necrosis or foreign body reactions were detected. The biomaterials were surrounded by or in contact with active osteoblasts forming osteoid and new woven bone, demonstrating persistent osteogenesis (Figs. 2 and 3). Active bone remodeling was evident not only around but also within the biomaterial, as seen on the fluorescent histologies stained with calcein green showing different levels of intragranular calcification (Fig. 2). In both treatment groups, biomaterial could also be identified as being embedded in CT with no histological signs of inflammation.
Immediately after surgery, the CT-based volume analysis revealed mean augmentation values of 1.60 ± 0.21 cm3 at the PLGA-NMP-BCP sites and 2.24 ± 0.34 cm3 at the BCP sites. After 21 weeks, values found for the augmented volume were 1.52 ± 0.22 cm3 for BCP and 1.74 ± 0.32 cm3 for PLGA-NMP-BCP.
Discussion
The goal of this study was to assess the influence of in situ hardening properties of a PLGA-coated BCP BGS (PLGA-NMP-BCP) in sinus augmentation in comparison to an equivalent but uncoated, particulate BGS (BCP) in sheep. The sheep model has been described as a suitable large animal model for maxillary sinus augmentation surgery in terms of volume and shape. Further, various experimental studies have investigated alloplastic BGSs such as calcium phosphates in the sheep sinus.17–19
This study shows that the tested materials supported sufficient new bone formation (NBF), leading to a total calcified tissue fraction of ∼46% for both biomaterials after 21 weeks of healing.
Moreover, a positive effect of the in situ stabilization on bone healing within the PLGA-NMP-BCP group could be observed. With a statistical probability of 97.5%, the bone formation expressed as the slope of a linear regression was more than 0.08% per week higher by using in situ hardening coated calcium phosphate particles than for the uncoated BCP material. Noteworthy, the values for the mean bone fraction were lower than the values reported for the same biomaterial tested in the same animal model, 17 in rabbit, 9 or for other materials in similar experimental models.18–20 This can be explained by the faster bone formation rate and a smaller augmentation volume in rodents.
Interestingly, Favero et al. found no increase in NBF over time. 17 They found between 18.0 ± 12.9% and 12.3 ± 7.9% NBF after 4 weeks of healing, which is a high NBF rate for this healing time for sole biomaterial without added autologous bone compared with another trial in a similar experimental model by Sauerbier et al. 12 In the study by Favero et al., 17 the 12-week NBF ranging between 16.7 ± 8.0% and 12.3 ± 7.9% was comparable to the aforementioned one. 12
The different results of the experiments might be due to the different amounts of augmentation material used or due to differences in the experimental settings such as packing density of biomaterial, which varies from surgeon to surgeon. In this study, the plot from the regression model (Fig. 1) suggests ongoing bone formation, which indicates that a later time point than 21 weeks might have revealed a potential further increase of the bone fraction.
However, the values found for the materials in this study are within the range of the values summarized in the review of Klijn et al. 21 This meta-analysis of sinus floor augmentations in humans compared the outcomes on total bone volumes for different bone graft materials. The review showed comparable results for total bone volume for different types of allogenic, xenogenic, and alloplastic materials, such as calcium phosphates, besides autologous bone, which was significantly better and still considered the gold standard. 21 Noteworthy, a reduction in total bone volume was found for particulate bone grafts. 21
Dislocation of particulate BGS, after the lateral sinus augmentation procedure, is difficult to control inside the sinus and might jeopardize the results of sinus floor augmentation, especially in the case of membrane ruptures.17,22 Therefore, stabilization of the BGS is essential for predictable bone augmentation procedures. 23
To improve the initial stability of bone graft particulates in the defect site, synthetic calcium phosphate BGSs were developed with in situ hardening properties. These injectable, moldable, and in situ hardening BGSs have been shown to improve the clinical handling and form a stable body in the defect that serves as a solid scaffold for bone formation.5,10,24 It has been previously shown in an animal model that such in situ properties hold the potential to provide sufficient stability to support bone formation even in the presence of a membrane rupture without the need of placement of a collagen membrane to cover the rupture. 17 Moreover, the stabilization and immobilization of particulate BGS at the recipient site might help to prevent micro-movement between bone and implanted material that is known to promote ingrowth of fibrous tissue and obstructs de novo bone formation at the defect site. 25
In former publications, it was speculated that the PLGA layer or the NMP-containing plasticizer, required to provide these unique properties, might jeopardize the osseointegration of the material. 11 However, this study showed that the PLGA coating did not influence the osseointegration of the calcium phosphate particles. NBF was found to be in close contact with, as well as within the individual calcium phosphate particles that were evident as intergranular calcification, in both groups after 21 weeks (Figs. 2 and 3).
The mean percentage of RB was slightly but significantly (p < 0.001) higher in the BCP group (32.23% ± 3.81) than in the PLGA-NMP-BCP group (27.05% ± 3.44) at 21 weeks after the augmentation procedure. One might hypothesize that the BCP without the PLGA coating was condensed from the exactly gauged 2 cm3 to 1.60 cm3 within the augmented sinus cavity. Thus, directly after surgery, the volume of the PLGA-NMP-BCP was 2.24 cm3 slightly higher. This could be due to moisture expansion of the PLGA coat. Still, the histomorphometric mean percentage of the residual graft is in alignment with other published results on the same material 17 and with other synthetic (26.5–28.5%)3,6 or xenogenic materials (26.0%). 6
Remnants of nonresorbed but integrated biomaterials have been reported to be crucial to preserve the augmented volume at the grafted sites,10,26 especially under conditions with constant pneumatic pressure changes such as in the maxillary sinus. 9 Further, volumetric reduction is a known drawback when using autologous bone.27,28
Recent investigations in a minipig model for sinus augmentation found that rapid resorption of the autologous bone graft was unable to maintain the initially augmented volume. 20 On the other hand, under similar conditions using a cranial epidural space model in rabbits, a good and comparable volume maintenance was shown for alloplastic biomaterials made of pure resorbable β-TCP and partially resorbable BCP, identical to the PLGA-NMP-BCP material tested in this study, with a trend for better volume stability for the latter. 9
In this study, the condensed BCP lost only 5.08% of its volume, leading to 1.52 cm3; whereas the PLGA-NMP-BCP shrank 22.51%, still leading to a higher final volume of 1.74 cm3 after 21 weeks. Overall, both provide a comparable long-term volume and showed no significant volume shrinkage such as reported for autologous bone. 20
Although the parameter of dental implant stability and survival has not been investigated in this study, the observed dense network of bone and grafting material will provide a stable and resilient bed for the accommodation of dental implants.
Conclusion
Within the limits of this study, it can be concluded that the PLGA and the NMP-containing plasticizer that facilitate the in situ hardening properties of the material have no negative influence on the osseointegration or biocompatibility of the calcium phosphate material but might improve bone formation due to improved stability of the material in situ. The site treated with the in situ hardening biomaterial (PLGA-NMP-BCP) showed faster bone formation, and the total fraction of NB was higher when compared with the particulate BCP. In addition, the clinical handling of the PLGA-coated material is easier.
Footnotes
Acknowledgments
The authors are grateful to Annette Lindner (Hard Tissue Research Laboratory, Department for Oral- and Maxillofacial Surgery, University of Freiburg, Freiburg, Germany) for excellent technical assistance. Dr. Dieter Menne (Menne Biomed Consulting, Tübingen, Germany) performed the statistical analysis.
Disclosure Statement
The study was financially supported by Sunstar Switzerland. No competing financial interests exist.