
Abstract
The reconstruction of defects in the mandible are still challenging. Despite several adequate microvascular bone reconstruction techniques, there is a need for ectopic bone endocultivation without drawbacks by donor-site morbidity. The omentum majus is described as a good vascularized fleece with undifferentiated cells with potential for bone culturing. In the omentum majus of six rabbits, two hydroxyapatite blocks were incorporated for 12 weeks each. The blocks were prepared with recombinant human bone morphogenetic protein-2 (rhBMP-2) or VEGF165 + rhBMP-2 and wrapped into the omentum. For ectopic bone endocultivation observation computed tomography (CT) scans were performed, and fluorescence markers were applied. After harvesting the block, histological sections were performed with hematoxylin and eosin and toluidine blue staining. In the CT scans, the Hounsfield units of the blocks increased within the trail. In some sections, new bone formation was observed within the hydroxyapatite blocks, however, the histological staining showed soft-tissue invasion only, no gross bone formation was observed. The ectopic bone endocultivation in the omentum majus is technically a good approach. An adequate mixture of osteoinductive proteins is still missing.
Introduction
P
Research in tissue engineering leads to promising in vitro results creating bone-like structures with vital osteoblasts. 5 Researchers tested a variety of different protocols for bone engineering. The fundamental components needed are cells that grow and differentiate on osteoconductive scaffolds under the influence of osteoinductive growth hormones in a biological environment. The outer dimension of the scaffold gives shape to the engineered bone tissue, which fits to the defect. The inner microarchitecture must allow seeding of bone cells, synthesis of extracellular bone matrix, and support vascularization of the tissue. They can be of allogeneic, xenogeny, phytogenic, or synthetic origin and be degradable or permanent.6–8 A widely used bone substitute material is a bovine xenogene hydroxyapatite, which provides a porous matrix that supports bone tissue ingrowth and sufficient vascularization. 9 The biocompatibility was proved in vitro 10 and in vivo. 11
The most important growth factors in bone tissue engineering are bone morphogenetic proteins (BMPs), which were identified first in 1988.12,13 BMPs belong to the transforming growth factor superfamily and play a role in bone remodeling, cell proliferation, and stem cell differentiation. 14 In vitro BMPs can stimulate mesenchymal stem cells and precursor cells to differentiate to osteoblasts, which produce bone tissue matrix. The most potent protein is BMP-2 which can be produced recombinant. 15 Its osteoinductive effect was proved in several in vitro and in vivo studies.16–18
As reported before, vascularization is fundamentally important for bone engineering. Researchers could identify some of the hormones that influence vascularization. Vascular endothelial growth factors (VEGFs) signal molecules play a role in vascularization and angiogenesis while embryogenic growth and tissue regeneration and wound healing. They stimulate the growth and differentiation of endothelial cells under hypoxic conditions. Therefore, VEGFs are used in tissue engineering to address vascularization of the tissue. 19 There are hints that the combination of BMP and VEGF leads to improved bone tissue formation.20,21
However, the promising in vitro results of tissue engineering failed when trying to engineer bone constructs of clinical relevant dimensions. Vascularization and nutrition of large bone structures were limitations that could not be solved in vitro. Transferring tissue engineering techniques to in vivo application seems to be a milestone in regenerative medicine. The own body as bioreactor with its known and also the not yet identified regenerative factors can be the fundamental for successful bone tissue growth. Choosing the most suitable in vivo bioreactor is of great importance. In reconstruction cases after cancer, the defect site suffers from compromised vascularity because of ablative surgery and irradiation. 22 The use of growth factors at the cancer site would be a risk factor for recurrence.23,24 These facts have been addressed by heterotopic prefabrication and vascularization. Past research has concentrated on muscular tissue as bioreactor. There are reports of successful bone regeneration in the dorsal latissimus muscle in different animal studies.21,25–27 It seems that repetitive application of BMP results in better ossification than single application. 28 The use of BMP and xenogene hydroxyapatite leads to bone tissue that provides similar stability that of original bone tissue. 29 Warnke et al. were the first who could reconstruct a mandible defect with a bone flap that was regenerated in the dorsal latissimus muscle in a human. 11
As described before, bone engineering is successful in the patient's muscle, but muscular tissue is not optimal as bioreactor. It has a thick soft tissue coverage which is disadvantage for facial reconstruction. Surgical interventions at the extremities lead to donor-site morbidity and limitations in the range of movement can result. Therefore, our research focuses on the improvement of heterotopic bone prefabrication. We chose the gastrocolic omentum as bioreactor. The omentum is well known in head and neck surgery for reconstruction of complex soft-tissue defects because of its great regenerative capacity.30,31 The omentum tissue consists of a high angiogenic potential by VEGF liberation. 32 In the omentum, there are many precursor cells that can differentiate to bone forming cells such as osteoblasts. 33 It is beneficial that the tissue is thin and flexible and has a long vascular pedicle with sufficient blood supply. The harvest of the omentum tissue results in very little donor-site morbidity. Patients do not suffer any side effects when the omentum is removed. Recent animal studies proved that mineralization of scaffolds or mineralization of periosteum tissue in the greater omentum is possible.33,34 In this study, we aimed to prefabricate bone grafts in the greater omentum in rabbits using hydroxyapatite scaffolds with BMP and vascular epithelial growth factor.
Materials and Methods
Twelve rabbits (New Zealand White Rabbits, Charles River, Sulzfeld, Germany) with a total weight between 3.5 and 4.0 kg and an average age of 8 month were used. They were separated into two groups with six animals each, according to the used growth factor (recombinant human bone morphogenetic protein-2 [rhBMP-2] or rhBMP-2 + VEGF165). The veterinary ethics commission of Schleswig-Holstein permitted this trail according to the law (No. V 312-72241.121-14 73-6/11)
Anesthesia
The operation was performed in general anesthesia. A mixture of 0.5 mL Ketamin (Ketamin 10%; Bremer GmbH, Warburg, Germany) and 0.25 mL Xylazin per kilogram bodyweight (Rompun®; Bayer AG, Leverkusen, Germany) was given intraperitoneal. When required, 1/3 of the maintenance dose was given during the operation. Further local anesthesia was performed with 1.2 mL citocain (Sopria Citocain, 40 mg/mL articaine hydrochloride, 10 mg/mL epinephrine; Heraeus Kulzer GmbH, Hanau, Germany).
Up to 5 days after the operation, 0.3 mL carprofen (Rimadyl, 4 mg/kg bodyweight; Zoetis Deutschland GmbH, Berlin, Germany) and 0.5 mL penicillin G (40,000 U/24 h; Grünenthal GmbH, Aachen, Germany) were given subcutaneous for analgesia and infection prophylaxis.
Operation procedure
Two hydroxyapatite scaffolds (Bio-Oss®; Geistlich Pharma, Wolhusen, Switzerland) were implanted in the greater omentum of each rabbit, soaked with rhBMP-2 (200 μg in 1 mL NaCl-solution; Wyeth Pharma GmbH, Münster, Germany) or VEGF165 (250 μg in 1 mL NaCl-solution). A central gap was milled in every block to put a blood vessel from the omentum majus inside to imitate the mandibular canal (Figs. 1 and 2).
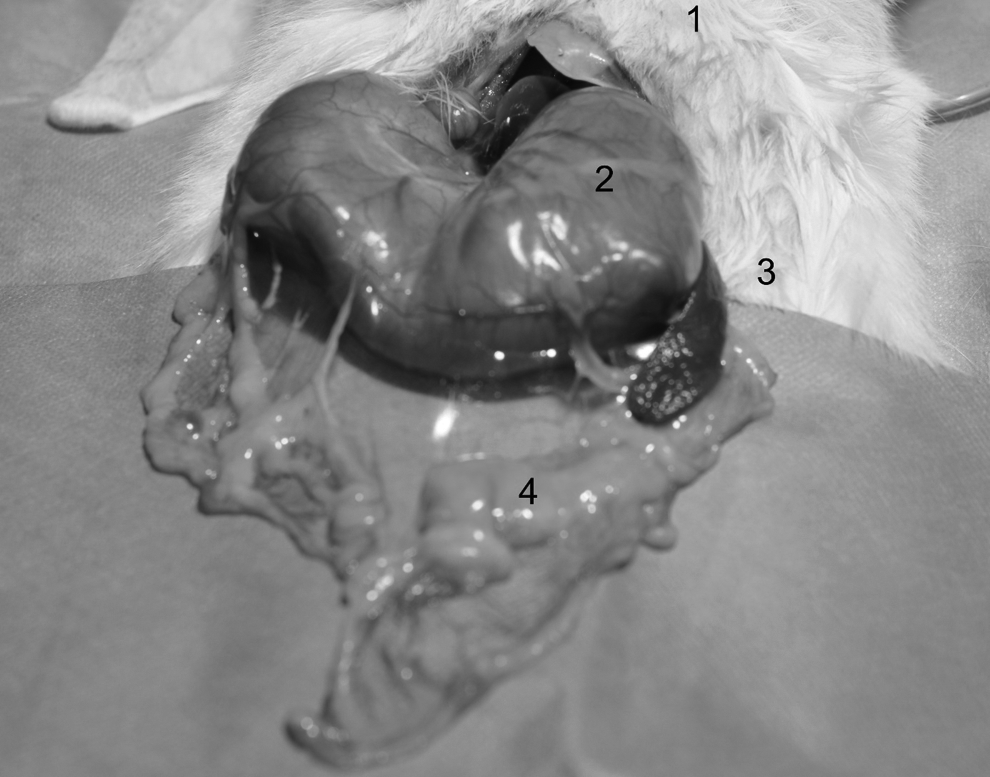
The omentum majus after preparation. (1) Animal; (2) stomach; (3) left caudal site of the animal; (4) omentum majus.

Implantation of the scaffold. One artery of the omentum was fixed into the canal of the scaffold to guarantee adequate vascularization. (1) left caudal site of the animal; (2) scaffold; (3) artery of the omentum.
The access to the omentum majus was performed with an abdominal incision about 10 cm long. Two arterial blood vessels were implanted into the milled gaps of the blocks, and the whole blocks were completely wrapped by the greater omentum and fixed with absorbable suture material Vicryl 3-0 (Ethicon GmbH, Norderstedt, Germany). The wound was closed in layers and the rabbits were cleaned with NaCl-solution and hydrogen peroxide. At the end of the operation, every animal was injected a subcutaneous deposit of 4 mL hand warm NaCl solution for better regeneration.
Before the operation, the hydroxyapatite blocks were extensively flushed with NaCl solution for 5 min. Afterward, 12 blocks (10 × 10 × 20 mm) were soaked with rhBMP-2 (200 μg) dissolved in 1 mL NaCl solution, and the other 12 blocks were soaked with rhBMP-2 (200 μg) dissolved in 1 mL NaCl solution and VEGF165 (250 μg) dissolved in 1 mL NaCl solution and stored for 30 min until the insertion in the omentum majus.
Computer tomography/bone density measurement
In the second, fifth, eighth, and tenth week after the implantation of the scaffolds a computer tomography (CT; SOMATOM Sensation64; Siemens Healthcare GmbH, Erlangen, Germany) was used to determine the bone density (120 kV, 20 mm). The software which was used for the measurement is IMPAX 6 (Agfa HealthCare GmbH, Bonn, Germany). Two areas of 2 mm3 from the block were measured. The first area named “centre” is located at the central canal were the blood vessel was implanted, and the second area is 2 mm above the canal in the middle of the block. The density of these volumes is indicated in Hounsfield Units (HUs) (Fig. 3).

Section of the CT data for HU evaluation. The animal lies to left site. The two inserted scaffolds are captured in one section. Left: Scaffold; axial plane with the two scaffolds; frontal plane with the two scaffolds. Right: Three-dimensional reconstruction of CT data for spatial orientation. CT, computed tomography; HU, Hounsfield unit.
Fluorochrome sequence labeling
Every week after the operation, fluorochrome sequence labeling was performed by giving the fluorochomes via intraperitoneal injection with a peripheral venous accesses (Braunüle®, green: 1.3 × 45 mm, G 18, Fa; B. Braun Melsungen AG, Melsungen, Deutschland) (Fig. 4).
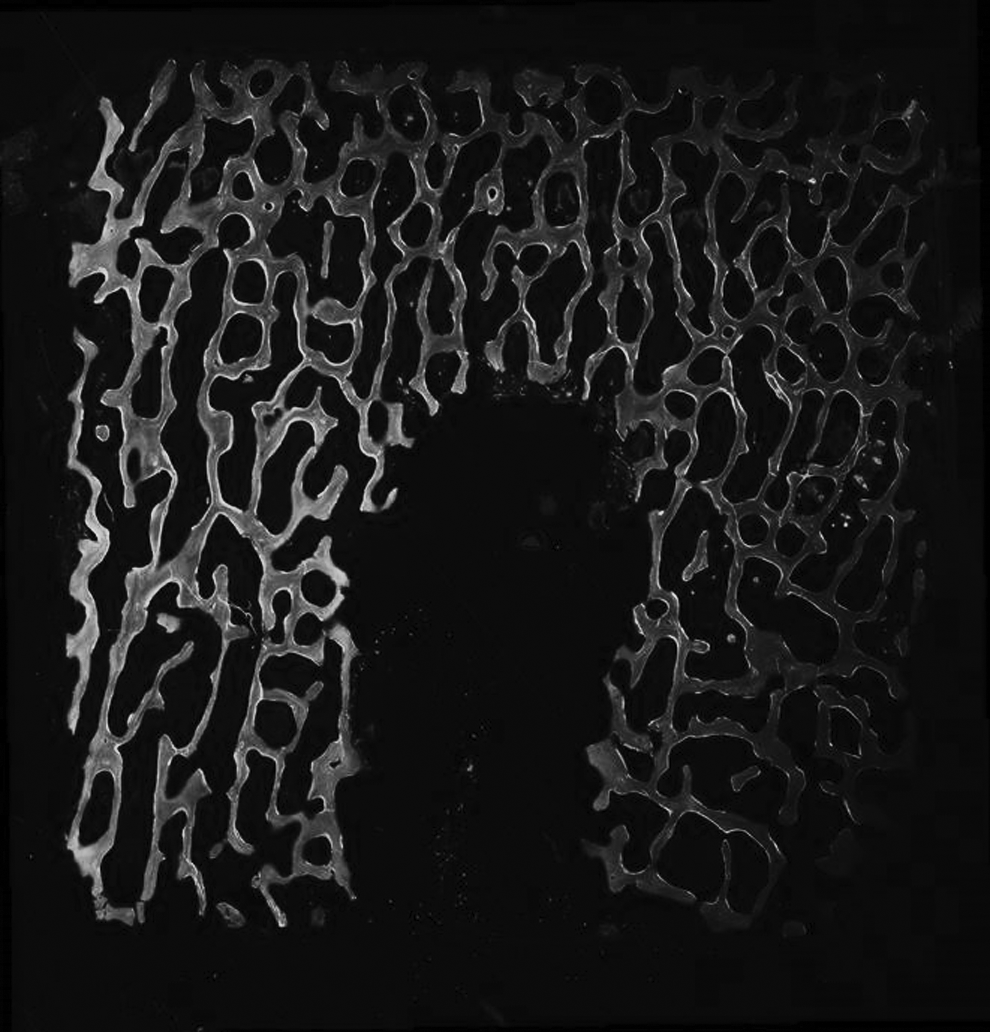
Fluorescence labeled scaffold. After the fluorescence labeling, the scaffold was investigated with fluorescence microscopy.
Harvesting of the scaffolds
Ten weeks after the implantation, the rabbits were sacrificed. The same general anesthesia was applied, which was used for the implantation of the blocks. During deep narcosis 5 mL of potassium chloride were applied intracardiac. The inserted scaffolds with the omentum were harvested and prepared for the further histological evaluations.
Histological sections
Every hydroxyapatite scaffold was fixed in formalin solution (10%) for 14 days split into two parts.
One part was used to analyze the fluorochome labeling and stained with toluidine blue after that. First, the preparations were dehydrated (PSI-embedding station, Pool of Scientific Instruments; Grünewald GmbH and Co KG, Laudenbach, Germany) and soaked with an embedding medium at 6°C. After hardening in a glass vessel at 37°C, all preparations had been sawed (Metabo® GmbH, Bochum, Germany), grinded (Struers® GmbH, Erkrath, Germany), and bonded to a slide with the help of an adhesive film (Technovit®; Exakt Apparatebau GmbH and Co. KG, Norderstedt, Germany). After bonding the preparations to the slide, they were grinded and polished again (Exakt Apparatebau GmbH and Co. KG) up to an approximate thickness of 40 μm. The finished slides were photographed on a microscope suitable for epifluorescent illumination, with 25× magnification (Axio Scan.Z1; Carl Zeiss AG, Oberkochen, Germany). To stain the preparation in toluidine blue, they had to be immersed into formic acid (0.1%) for 3 min, cleaned with distilled water, immersed into methanol for 90 min, and stained in a toluidine blue solution for 2 min.
The second part was decalcified, embedded in paraffin, and used for hematoxylin and eosin (H&E) staining. First, the parts had to be decalcified with 12.5% ethylenediaminetetraacetic acid solution (pH 7.4) in an ultrasonic bath (Ultraschall-Entkalker USE 33; Medite, Burgdorf, Germany). After dehydrating, the preparations were embedded in paraffin (TES 99; Medite) and cut into slices of about 5 μm (Microm International GmbH, Walldorf, Germany). The deparaffined and rehydrated histological preparations were stained in H&E and photographed with 25× magnification (Fig. 5).

Hematoxylin and eosin staining of the scaffold. Center and top indicate the areas for histological evaluation.
Statistical evaluation of the CT
First of all, the normal distribution was tested with Kolmogorov–Smirnov test. To analyze the bone density measurements, the analysis of variance post hoc Tukey test was used. The average of all measurements was taken as reference values. Several graphs were designed (GraphPad Prism 6; GraphPad Software, Inc., La Jolla, CA). The statistical significance is p > 0.05.
Results
Gross observations
Up to the fifth day after the implantation into the omentum, every animal had been kept in a separate cage, to reduce the risk of injury. Except one animal, all rabbits had adequate wound healing. One wound infection was disinfected and cleaned every day and healed. One animal died a few days after the operation, probably due to an acute abdomen. It was replaced by another animal, which tolerated the procedure without any problems.
Computer tomography
In both groups (rhBMP-2 and rhBMP-2 + VEGF165), there was an increase of the HUs from week 2 to 10. However, there were significant differences between week 2 and 10 only. In rhBMP-2 group, the increase was in the center of the scaffolds, and in the rhBMP-2 + VEGF165 group, in the top of the scaffold only. The value of the increase was about 250 HU. Overall, there is no significant difference in bone density in the rhBMP group and the rhBMP + VEGF-group. There is no significant difference between the “centre” and the “top” area of the block (Figs. 6 and 7).

Measurements of the HUs.

Measurements of the HUs. rhBMP-2 + VEGF165 group showed in both blocks
Fluorescence microscopy
The fluorescence microscopic sections show bone apposition in a chronological order. Isolated yellow (xylenol orange, second and sixth week) and green (calcein green, third and seventh week) color bands can be seen in nearly all specimens. There are no differences between the BMP- and the BMP + VEGF group. The two other fluorochromes do not occur. The staining is only located at the margin area of the preparations.
Toluidine blue staining
The bone substitute shows up in a dark purple color and the connective tissue in light purple color. The area around the central blood vessel is very well vascularized and shows a lot of connective and fat tissue. Bone apposition occurs in a few areas. Partially there are Haversian canals. There are no differences between the rhBMP- and the rhBMP + VEGF group.
H&E staining
The cavities of the hydroxyapatite block are lined with connective and fat tissue. Many blood vessels are shown in the specimens. Any bone apposition cannot be detected in the H&E stains. Also, there is no difference between the two groups.
Discussion
The reconstruction of the mandible after ablative surgery is challenging. Autologous bone transplants can lead to a higher morbidity. Therefore, today is a need of ectopic bone engineering. In the present study, the bone formation of hydroxyapatite blocks treated with rhBMP-2 and VEGF165 inserted in the omentum majus was investigated in an animal model.
There is an osteogenic potential in the omentum majus due to a good vascularization and a high number of stemcells. 33 In an individual treatment attempt, the omentum was used for the implantation of a titanium mesh with hydroxyapatite. 35 The omentum as a soft tissue with an adequate size can be used to wrap scaffolds and keep them for a longer period, moreover, the high vascularization of this tissue can be used to supply and support regeneration processes.
However, there is a need for proteins to enable tissue reactions. In this investigation hydroxyapatite blocks rinsed with rhBMP-2 and VEGF165 were used to enable bone formation in the omentum majus in an animal model. There are several studies that support the effect of bone formation of BMP and hydroxyapatite.11,21,28,36 In the present study, bone formation was observed in a minimum only. The rabbit as bioreactor was used in a few studies only. In 1994, a bone defect of the ulnar bone of rabbits was closed by stimulation with 6.25 μg rhBMP-7. 37 In rats, only a few amount of BMP is enough to induct bone formation. 36 The simultaneous stimulation with rhBMP-2 and VEGF165 showed an increase in bone formation in an animal model. 21
Liu et al. 21 used 660 μg rhBMP-7 and 4 μg VEGF165 in a minipig to induce bone formation. All these trials were performed in muscles. In muscles, there is not so high amount of proteins needed for osteoinduction.25,38 The correct amount of the proteins needed in the omentum majus was not evaluated until now, linear or exponential release kinetics are possible. In the present study, the proteins were not enough for new bone formation in the omentum majus. Despite the used vessels in the center of the hydroxyapatite block and the possibility of rhBMP-2 storage by the block, there was no success. 39 The release kinetics of hydroxyapatite were investigated in several studies.21,40 Within 24 h, half of the proteins were released and the other half within the next 27 days. Therefore, there is a peak of proteins at the beginning of the trail. It is believed to be the comparable kinetics of VEGF165. 21 This kinetic may be the reason of the missing bone formation, however, there are studies where the peak kinetic leads to bone formation.21,36 Therefore, the kinetic may not be the key factor for disappointing result.
The measurements of the bone density performed in the CT scans and the observation period showed increased HUs in some cases. The rhBMP-2-treated blocks showed a significant increase, however, there was no difference between the top and center of the scaffold. We postulated a higher increase of bone density in the circumference of the vessel pedicle, which cannot be proved here. In the group with the combination of rhBMP-2 + VEGF165, there was also an increase of the HU, however, less than in the other group. In a study with rats the bone density was increased by the combination of rhBMP-2 and VEGF165. 41 In a trail with minipigs, the bone density could be increased by the use of rhBMP-7 and VEGF165. 21
The effect by BMP can be modulated by factors of the environment. 38 The specific pathways are investigated by current studies.
The histological evaluations showed soft tissue in growth of the hydroxyapatite blocks. There were lots of blood vessels, however, no signs of infections or necrosis. The sections with toluidine blue staining showed new bone formation in some areas only, however, without ectopic osteogenesis. The same signs were shown by the H&E sections, too. Therefore, the CT data detected soft-tissue invasion in the porosities of the scaffolds and not bone formation. In other studies, there were reports of overwhelming ectopic bone with similar setups, but these results could not be confirmed by us.27,42
The application of the growth factors into the canal of the block seemed to be favorable. The growth factors could not penetrate into the surrounding soft tissue. A comparable situation was observed during the endocultivation in the rat model. 36
It can be accepted that the neo osteogenesis was disturbed by the proliferation of the soft tissue. The proliferation of the soft tissue is faster than new bone formation stimulated by rhBMP-2 and VEGF165. This situation can be managed in further investigations by using collagen membranes to separate the soft tissue from the hard tissue. Collagen membranes are used widely. 43 There are lots of different types with different degradations times. After the resorption of the membrane the omentum majus could develop its full benefits.
The fluorescence microscopy confirmed the results of CTs and staining. The fluorchromes applied in the weeks 2 and 6, and 3 and 7 could be detected only. The new bone formation was detected in these weeks only. There was no difference between the two test groups.
In this study, the rabbit was used for the first time as bioreactor in combination of hydroxyapatite blocks with rhBMP-2 and VEGF165. The histological structure of the rabbit bone is comparable with these of human beings, 44 however, the bone remodeling is two times faster than the human one. 45
The omentum majus in principle is an adequate region for ectopic endocultivation of bone blocks, however, in our study no positive results could be demonstrated. The omentum showed a good vascularization into the hydroxyapatite blocks, however, despite growth factors without new bone formation. One reason may be inadequate concentration of the growth factors or the release kinetic. The combination of rhBMP-2 with VEGF165 showed no advantage compared with single application of rhBMP-2. There are lots of different proteins and receptors involved in the bone metabolism, for example, receptor activator of nuclear factor-κB (RANK)-ligand and RANK. 46
The limitations of this study are the short time of observation of only 10 weeks. A prolonged observation period may show an induction of bone in the circumference of the hydroxyapatite scaffold. A bone fracture healing is awaited within 6–8 weeks, however, a complete new bone formation with a critical size defect in an ectopic space may take longer time. Moreover, the scaffolds were wetted with rhBMP-2 and VEGF165 + BMP-2 solution. This solution may keep active for several hours only. A continuous application with different releasing kinetics may improve the local influence of these proteins on bone formation. Next, the single application of proteins may not be adequate due to fast resorption time. A simultaneous application of cancellous bone may increase the new bone formation due to prolonged resorption time.
In further studies, combinations of several proteins that have influence on the bone metabolism are a possible approach, for example, matrix-metalloproteinases or their inhibitors tissue inhibitors of matrix-metalloproteinases (TIMPs). 47 The easiest way to improve the bone formation may be the use of a collagen membrane to separate the soft tissue and the hard tissue with their different proliferations, moreover, a longer period of the experiments of about 3–6 months may be enough time for bone formation.
Conclusion
The omentum majus is an adequate space for new bone formation with respect to the technical part, however, the single-shot application of proteins to induce new bone formation seems too simple to be successful. Adequate protection of the osteoconductive scaffold against soft-tissue ingrowth by resorbable membranes and cancellous bone particles for a longer stimulation period may improve the bone formation.
Footnotes
Disclosure Statement
No competing financial interests exist.