
Abstract
Intestinal failure is a serious clinical condition characterized by loss of motility, absorptive function, and malnutrition. Current treatments do not provide the optimal solution for patients due to the numerous resulting complications. A bioengineered bowel that contains the necessary cellular components provides a viable option for patients. In this study, human tissue-engineered bowel (hTEB) was developed using a technique, whereby human-sourced smooth muscle cells were aligned and neoinnervated using human-sourced neural progenitor cells, resulting in the formation of intrinsically innervated smooth muscle sheets. The sheets were then rolled around hollow tubular chitosan scaffolds and implanted in the omentum of athymic rats for neovascularization. Four weeks later, biopsies of hTEB showed vascularization, normal cell alignment, phenotype, and function. During the biopsy procedure, hTEB was transplanted into the same rat's native intestine. The rats gained weight and 6 weeks later, hTEB was harvested for studies. hTEB was healthy in color with normal diameter and with digested food in the lumen, indicating propulsion of luminal content through the hTEB. Histological studies indicated neomucosa with evidence of crypts and villi structures. This study provides proof of concept that hTEB could provide a viable treatment to lengthen the gut for patients with gastrointestinal disorders.
Introduction
I
The different functions performed by the intestine require specialized cells. 6 Motility and propulsion of luminal contents are produced by smooth muscle layers, the enteric nervous system, and the interstitial cells of Cajal. Contraction of the longitudinal muscle causes shortening of the length of the gut, and contraction of the circular muscle leads to narrowing of the lumen of the gut for mixing or for peristalsis. On the contrary, secretions and absorption of nutrients are controlled by the epithelial or mucosal cells of the intestine. Regeneration of a fully functional epithelium with maintenance of the native characteristics also imposes a challenge in the field of intestinal tissue engineering. In addition to identifying and maintaining cell types, successful reconstruction of intestinal segments is also dependent on recapitulating the architecture of the native intestine, which increases the complexity of this process. Each cell type in the intestine acquires a certain alignment that is specific to its function.
Recent advances in intestinal tissue engineering used organoid units seeded onto polymeric scaffolds. The regenerated tissues acquired all cell layers and demonstrated functionality in vivo.7–9 Decellularized matrices have also shown potential for intestinal reconstruction with further evaluations needed.10,11 Chitosan is a natural polymer that has been tested in different tissue engineering applications. Recently, chitosan has been introduced in the field of intestinal tissue engineering. Chitosan promoted smooth muscle and neural cell survival, alignment, phenotype, and functionality, both in vitro and in vivo.12,13
In this study, we combined our previously established technique of engineering intrinsically innervated aligned smooth muscle sheets and designed tubular chitosan scaffolds for the development of human tissue-engineered bowel (hTEB) segments for transplantation into rats. The objectives of this study were (1) to achieve vascularization and maturation of hTEB following implantation in the omentum and (2) to demonstrate the feasibility of transplanting hTEB into the rat's native small bowel. After 4 weeks of implantation in the omentum, hTEB was vascularized, maintained cell phenotype, alignment, and function. The hTEB was then transplanted into the rat's native intestine. The transplanted hTEB maintained its neuromuscular characteristics and acquired an epithelial component through migration of native epithelial cells into the lumen. hTEB provides a promising approach to lengthen the gut and helps treat patients with intestinal failure.
Materials and Methods
Reagents
Cell culture reagents were purchased from Life Technologies (Grand Island, NY) unless otherwise specified. Smooth muscle growth medium consisted of Dulbecco's modified Eagle's medium, 10% fetal bovine serum, 1.5% antibiotic–antimycotic, and 0.6% L-glutamine. Neural growth medium consisted of neurobasal, 1× N2 supplement, recombinant human Epidermal Growth Factor (EGF 20 ng/mL, PeproTech, Rocky Hill, NJ), recombinant basic Fibroblast Growth Factor (bFGF 20 ng/mL, PeproTech, Rocky Hill, NJ), and 1× antibiotic–antimycotic. Neural differentiation media consisted of neurobasal medium-A supplemented with 2% fetal bovine serum, 1× B27 supplement, and 1× antibiotic–antimycotic. Medium molecular weight chitosan (190,000–310,000 Da, 75–85% deacetylation), Acetylcholine (ACh), and neuronal nitric oxide synthase (nNOS)-blocker Nω-Nitro-L-arginine methyl ester hydrochloride (L-NAME) were purchased from Sigma (St. Louis, MO). Sylgard [poly(dimethylsiloxane); PDMS] was purchased from World Precision Instruments (Sarasota, FL). Type I rat-tail collagen was purchased from BD Biosciences.
Cell isolation
Human small intestinal biopsies were ethically obtained from organ donors through Carolina Donor Services and Wake Forest Baptist Medical Center (IRB No. 00007586).
Smooth muscle cells
Smooth muscle cells were isolated from the duodenal portion of the small intestine following our previously established protocols. 14 Tissues were cleaned of any luminal content and washed extensively in ice-cold Hank's balanced salt solution (HBSS). Tissues were then chopped into smaller pieces followed by stripping off the mucosal layer and the longitudinal muscle layer. Circular muscle tissues were then extensively washed and then minced and washed several times in HBSS. Tissues were then subjected to two collagenase digestions (1 mg/mL type II collagenase, Worthington, Lakewood, NJ) at 37°C with agitation for 1 h each, with centrifugation in between the two digestions. The digested tissues were then washed, and the pelleted cells were resuspended in warm smooth muscle growth media.
Neural progenitor cells
Neural progenitor cells were isolated from human small intestinal tissues following our previously published protocols. 14 Tissues were finely minced and extensively washed in HBSS. Tissues were then subjected to two digestions in a mixture of type II collagenase (0.8 mg/mL) and dispase (0.8 mg/mL). The recovered cells were passed through 70 μm cell strainer followed by extensive washing. The cells were then passed through 40 μm cell strainers and resuspended in neural growth media.
Preparation of wavy plates
Plates with wavy patterns (6 μm apart and 1700 nm deep) were prepared as previously described. 15 Sylgard was poured into the prepared wavy molds and allowed to cure for 2 days at room temperature. Rectangular sections were obtained and were inserted into 100 mm deep dishes. The wavy surface was facing upward for cell seeding. The molds were then sterilized inside the hood using 70% ethanol and UV light. Following sterilization, the plates were coated with 10 μg/cm2 laminin. Silk sutures were pinned down onto the plates to mark the direction of the grooves and for sheet lifting following formation.
Engineering innervated smooth muscle sheets
Human smooth muscle cells were grown until confluency followed by trypsinization. About 750,000 smooth muscle cells were suspended in 3 mL of smooth muscle growth media and seeded onto each wavy plate (2 × 4 cm). The cells were allowed to attach and align along the grooves for up to 5 days. After the cells aligned, human neural progenitor cells were collected. About 200,000 neural progenitor cells were resuspended in a collagen/laminin gel as previously described. 16 The cell/gel suspension was then evenly poured on top of the aligned smooth muscle. Neural differentiation medium was added to the plates to promote neural differentiation. The smooth muscle sheet will delaminate to form aligned innervated smooth muscle sheet held in place by the silk sutures.
Development of hTEB
Tubular chitosan/collagen scaffolds were engineered following our protocols.12,17 In brief, 2 wt% chitosan was mixed with 0.1 mg/mL type I rat-tail collagen in a 1:1 volume ratio. The solution was poured into a custom made mold and frozen at −80°C for 3 h followed by lyophilization overnight. The scaffolds were then neutralized in NaOH and extensively washed in 1× phosphate-buffered saline (PBS) and distilled water. The scaffolds were sterilized in 70% ethanol for up to 7 days and then washed extensively with sterile 1× PBS before seeding.
hTEB was developed as previously described. 16 The aligned innervated smooth muscle sheets were wrapped circumferentially around the tubular chitosan scaffolds with the cells facing the inside, in a manner to mimic the circular muscle layer. The tissues were incubated in neural differentiation medium and prepared for implantation.
Experimental design of the surgeries
Stage 1 of surgery consisted of two consecutive procedures: Procedure 1: hTEB was implanted in the omentum of all rats. Procedure 2: bypass/loop was formed (described in section 2.7). Stage 2 of surgery: after 4 weeks, the implants were reaccessed to collect biopsies for analysis. At the same time, hTEB was transplanted into the loop in the small intestine (described in section 2.10). Rats were euthanized after 6 weeks of transplantation.
Stage 1 surgery: implantation of hTEB in the omentum and bypass formation
Implantation of the hTEB in the omentum is a first step of a two-step surgical approach to prepare the hTEB for transplantation. Athymic rats (n = 4) were used in this study. Surgical procedures described in this work were performed following the guidelines set forth by the Institutional Animal Care and Use Committee (IACUC). Rats were anesthetized by continuous isoflurane masking throughout the surgery. The surgical area was shaved and aseptically prepared. A midline laparotomy of up to 5 cm was made in the abdominal wall. In the first procedure of stage 1 surgery, the peritoneal cavity was accessed, and the greater omentum was located and fully exposed. hTEB was wrapped in the omentum avoiding any occlusion of the omental vascular tree. hTEB was secured in place using sutures and returned back to the abdominal cavity.
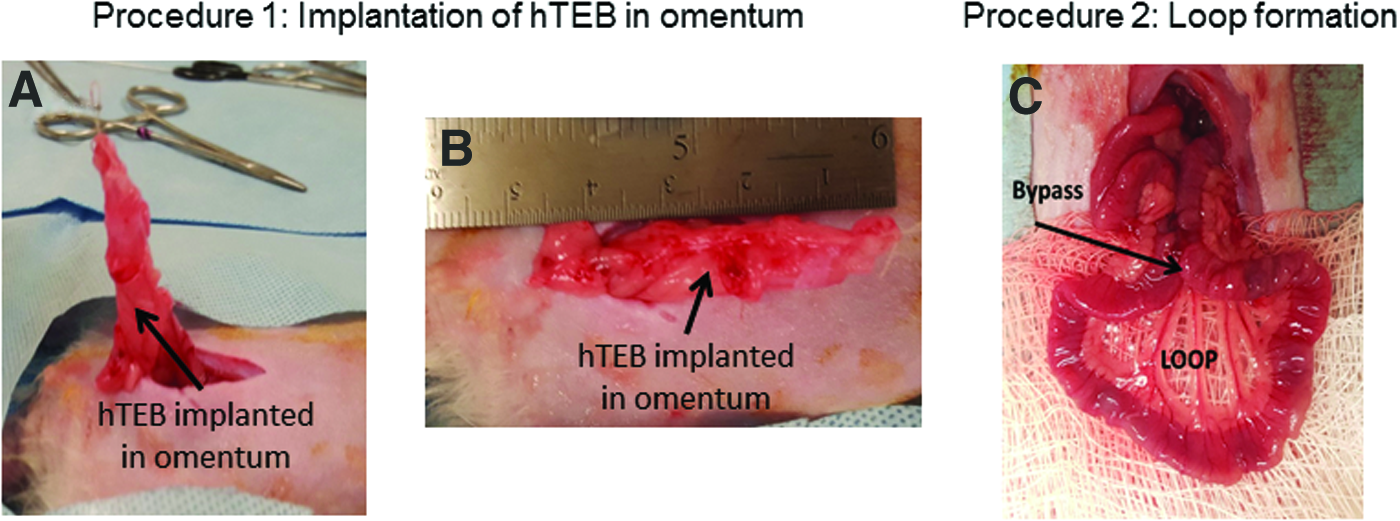
In the second procedure of stage 1 surgery, a 10 cm long segment of small bowel was exposed. Two enterotomies of ∼0.5 cm each were performed on the antimesenteric border of the small bowel. The two enterotomies were then closed in a side to side manner. This resulted in the creation of the bypass on top of the formed bowel loop (See Fig. 2C). The bypass site was checked for any leakage. The bowel was returned back to the abdominal cavity. The muscular fascia was closed followed by skin closure. The rats were allowed to recover in their cages in standard manner and were given the appropriate analgesics.
Functional assessment of hTEB postomentum implantation
Four weeks following implantation of the hTEB in the omentum, the rats were brought back to the procedure room and were anesthetized by continuous isoflurane masking. In all four rats, the implant site was reaccessed. Circular strips of hTEB were obtained for organ bath studies. Real-time force generation was conducted using a force transducer setup (Harvard Apparatus, Holliston, MA). Tissues were hooked between the transducer arm and a fixed pin in the organ bath. The tissues were maintained at 37°C in 4 mL of 4-(2-hydroxyethyl)-1-piperazineethanesulfonic acid) (HEPES) buffer. At the end of each experiment, the tissues were washed with fresh warm buffer. Tissues were allowed to equilibrate and reach baseline before any treatment. Physiological functionality of the tissues was evaluated following our established protocols: (i) electromechanical coupling integrity was assessed by depolarization of the smooth muscle using 60 mM potassium chloride (KCl). (ii) Contractile response was evaluated using 10 μM Acetylcholine (ACh) in the absence and presence of muscarinic receptor antagonist, atropine. (iii) Neural functionality was assessed using electrical field stimulation (EFS) in the absence and presence of neuronal nitric oxide synthase (nNOS)-blocker Nω-Nitro-L-arginine methyl ester hydrochloride (L-NAME). Baseline was arbitrarily set to zero, and all contraction/relaxation responses are reported as delta force (μN).
Histological assessment of hTEB postomentum implantation
Sections of hTEB were also obtained for histological evaluation of the tissues. Tissues were immediately fixed in 10% neutral-buffered formalin followed by processing and paraffin embedding. Cross sections of 6 μm thickness were obtained and stained with hematoxylin and eosin (H&E) and Masson's trichrome for morphological analysis. Maintenance of smooth muscle was evaluated using primary antibodies against smoothelin and smooth muscle Myosin heavy chain. Neural phenotype was evaluated using primary antibody against β-III tubulin. Labeling of synapses was conducted using primary antibody against Synapsin I. Appropriate fluorophore-conjugated secondary antibodies were used.
Stage 2 surgery: transplantation of hTEB to native intestine
After 4 weeks of stage 1 surgery, two out of the four rats were sacrificed for histological and functional evaluation of hTEB. hTEB segments from the other two rats were used for transplantation. After 4 weeks of implantation of hTEB in the omentum, the rats were anesthetized by continuous isoflurane masking throughout the surgery. The surgical area was shaved and aseptically prepared. A midline laparotomy of up to 5 cm was made in the abdominal wall in the same location of the previous surgery. The peritoneal cavity was accessed, and hTEB and the created loop were located and fully exposed. The edges of hTEB were refreshed to expose the lumen. Full-thickness biopsies were obtained for in vitro assessment.
The transplantation of hTEB with omentum into the native intestine was performed in the previously created bowel loop. Two 0.5 cm enterotomies were performed on the antimesenteric borders of the native bowel loop. hTEB along with its omental vascular pedicle was anastomosed to the enterotomies created in the native intestine. The anastomosis sites were checked for leakage. The muscular fascia was closed followed by the skin closure. The rats were then allowed to recover in their cages in standard manner and were given the appropriate analgesics.
Harvest of hTEB following transplantation
Six weeks following hTEB transplantation, the rats were euthanized, and the hTEB with anastomoses site was reaccessed. Circular sections of hTEB were obtained for physiological and histological analysis as described above. H&E stains were performed for morphological analysis, and Alcian blue was performed for mucin stain.
Statistical analysis
Analysis of acquired force data was conducted using PowerLab and exported to GraphPad Prism 5.0 for Windows (GraphPad Software, San Diego CA;
Results
Development of hTEB
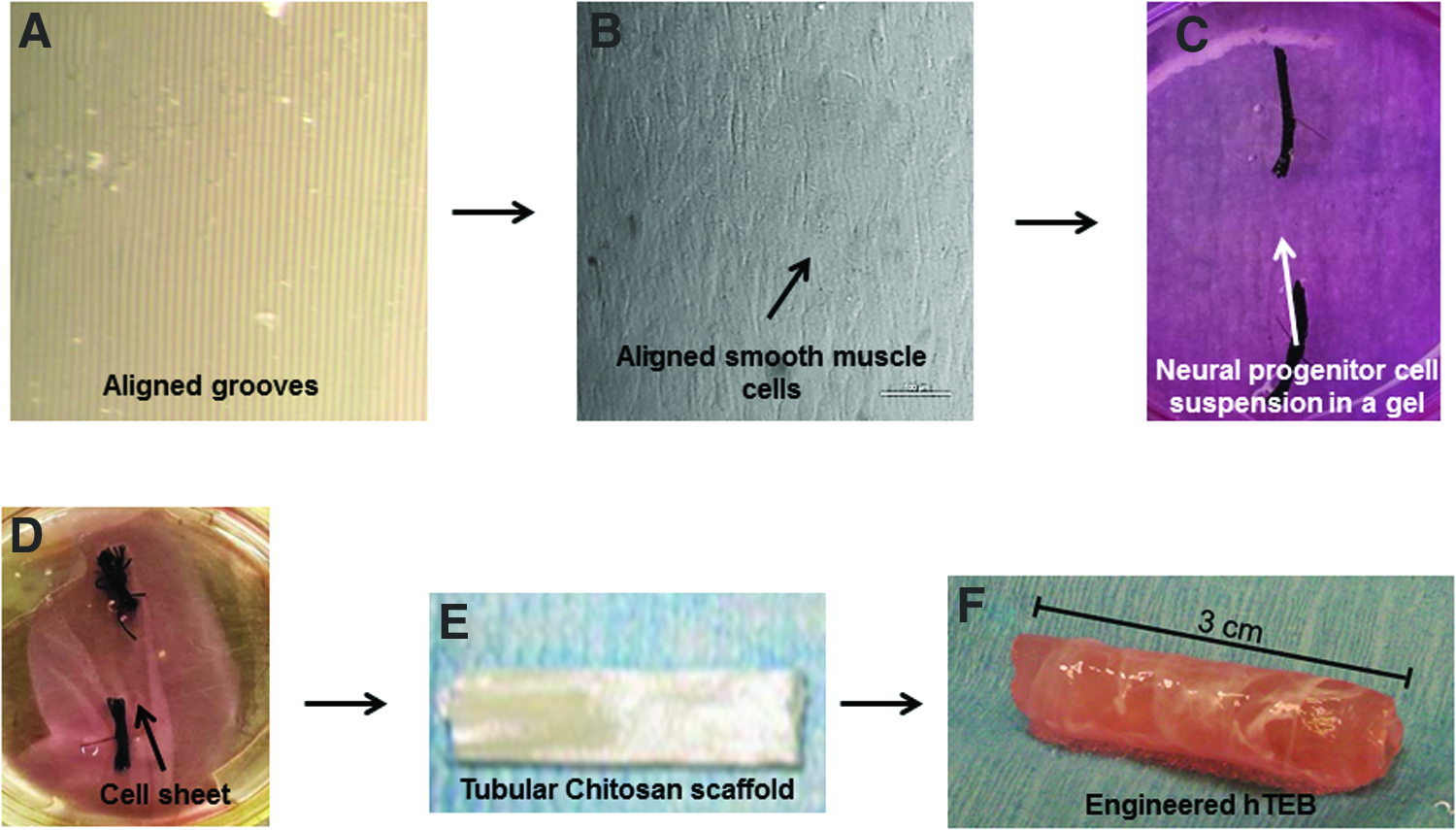
Wavy plates were coated with laminin and prepared for seeding (Fig. 1A). Smooth muscle cells attached and proliferated on the plates, and they started acquiring the alignment along the grooves on day 1. By day 5, the cells were fully aligned (Fig. 1B). Neural progenitor cells were collected and suspended in a collagen/laminin gel. The gel was overlaid on top of the aligned smooth muscle cells (Fig. 1C). The neural progenitor cells differentiated into neurons when placed on top of the smooth muscle. This led to the formation of an intrinsically innervated smooth muscle sheet (Fig. 1D). Hollow tubular chitosan scaffolds were also prepared (Fig. 1E). The sheets were then wrapped circumferentially around the engineered tubular hollow chitosan scaffolds to form the innervated circular muscle layer of hTEB (Fig. 1F). hTEB was 3 cm long with a luminal opening of 0.3 cm internal diameter. hTEB was prepared for implantation in the omentum.
hTEB development:
Harvest of hTEB following omentum implantation
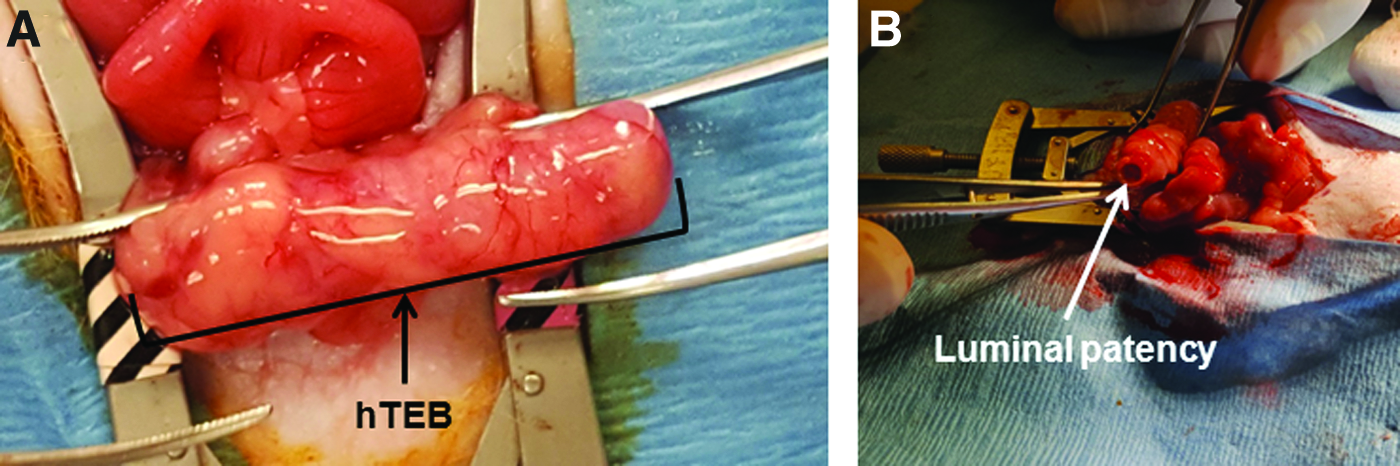
hTEB was implanted in the omentum and secured in place as a first step for neovascularization (Fig. 2A, B). During the same surgery, a bypass/loop in the small intestine was created in preparation for transplantation of hTEB in the loop (Fig. 2C). The loop was formed to alleviate any potential blockage that could result from transplantation of hTEB. The loop provides an alternative route for luminal content to propel through the bypass site or through the loop. Four weeks following omentum implantation, the surgical site was reaccessed, and hTEB was located. hTEB showed healthy pink color with maintenance of luminal patency and with no signs of inflammation, infection, or tissue necrosis (Fig. 3A). Neovascularization was visualized with blood vessels surrounding hTEB. Luminal patency was also maintained (Fig. 3B). hTEB biopsies were obtained from all four rats for further analysis.
Stage 1 Surgery: Implantation of hTEB in the omentum and loop formation:
Postomentum implantation: After up to 6 weeks of implantation of hTEB in the omentum, the surgical site was reaccessed.
Organ bath studies following omentum implantation
Circular strips were obtained for physiological assessment. Tissues were allowed to establish baseline before any treatment.
Electromechanical coupling integrity
When baseline was established, addition of 60 mM KCl caused a rapid and robust contraction that averaged 645 ± 10 μN (Fig. 4A). This contraction was partially inhibited in the presence of calcium channel blocker, nifedipine. This indicated the maintenance of smooth muscle membrane integrity after implantation in the omentum.

Physiological analysis of hTEB following omentum implantation: Circular strips of hTEB were obtained before transplantation for organ bath evaluation.
Cholinergic response
The tissues were washed and supplied with fresh warm buffer. When baseline was reached, addition of 10 μM ACh caused smooth muscle contraction with an average peak contraction of 410 ± 16 μN (Fig. 4B). The tissues were then washed and incubated in buffer with muscarinic receptor antagonist, atropine. The same concentration of ACh did not cause a contraction of the smooth muscle. This indicated that ACh-induced contraction was mediated through muscarinic receptors, which were preserved in hTEB following implantation in the omentum.
EFS
The tissues were washed and again allowed to establish baseline. EFS caused relaxation of the smooth muscle (Fig. 4C). The average maximal relaxation was −350 ± 26 μN. This relaxation was abolished when hTEB was treated with tetrodotoxin, indicating that the relaxation of the smooth muscle in hTEB was purely neural response. The tissues were then washed and allowed to equilibrate again before pretreating them with LNAME. Following EFS, relaxation was partially inhibited (50%). This indicated that about half of the initially observed neurally mediated smooth muscle relaxation was mediated by nitrergic neurons present in hTEB.
Histological assessment of hTEB following omentum implantation
Cross sections of hTEB were also processed for histological assessment. Cross sections were stained with H&E and Masson's trichrome. H&E revealed maintenance of smooth muscle circular alignment around the lumen of hTEB (Fig. 5A) along with dense collagen layer (Fig. 5B). Chitosan remnants were observed with loss of complete integrity of the scaffold. This indicated that chitosan was almost completely resorbed. Immunohistochemistry analysis showed maintenance of smooth muscle contractile phenotype indicated by positive stain with smoothelin (Fig. 5C) and positive stain for smooth muscle myosin heavy chain (Fig. 5D). 4′,6-Diamidino-2-phenylindole, dihydrochloride (DAPI) stain confirmed the preservation of the circular cell alignment. The presence of differentiated neurons was also confirmed by positive stain with β-III tubulin (Fig. 5E). The presence of synapses was confirmed by positive stain for the synaptic marker Synapsin I (Fig. 5F).

Histological evaluation of hTEB following omentum implantation: Biopsies obtained from hTEB before transplantation were evaluated histologically.
Harvest of hTEB 6 weeks after transplantation into the native intestine
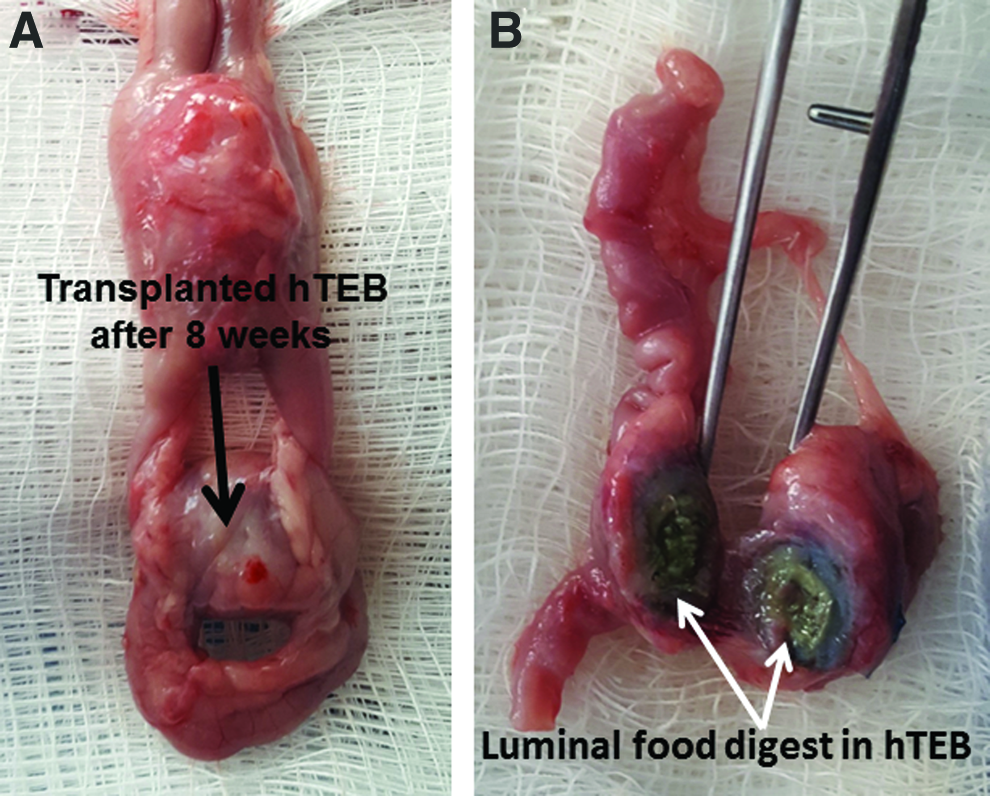
After the first week of transplantation, body weights were reduced. The rats then regained their weights and restored their normal appetite. At the time of harvest, hTEB looked healthy and pink in color (Fig. 6A). There was no distention or dilation of the hTEB. Anastomosis sites were completely healed. Vascularization was also seen. An incision in the middle of hTEB showed the presence of fresh digested food particles in the lumen (Fig. 6B).
hTEB following transplantation:
Histological assessment of hTEB following transplantation
Sections of hTEB were obtained for histological evaluation. H&E stains of hTEB cross sections revealed neoepithelialization of the lumen of hTEB with evident crypts and villi structures (Fig. 7A), although the middle part of hTEB was still lacking full epithelialization. Full neoepithelialization reached about one third the length of hTEB, starting from the anastomosis sides. There was evidence of epithelial cells that have migrated to the center of hTEB and started forming crypts, however, fully formed and differentiated villi structures were lacking. Positive Alcian blue stain revealed the presence of goblet cells indicating the capacity of mucus secretion in hTEB (Fig. 7B).
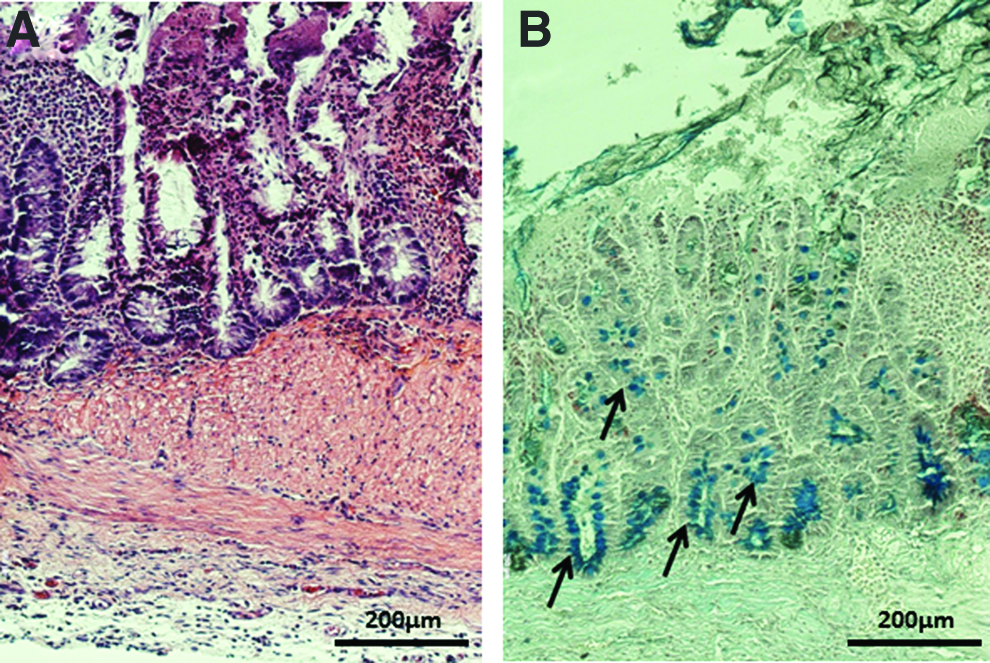
Histological evaluation of hTEB following transplantation: Cross sections of hTEB were obtained for histological evaluation.
Discussion
Unmet needs and challenges
Patients with intestinal failure suffer from dysfunctional motility, poor absorption of nutrients, and malnutrition. Current treatments include TPN and intestinal transplantation. In addition to the high cost of those treatments, they are associated with multiple complications, which lead to increased morbidity and mortality rates. Bioengineered intestine can offer a long-term solution for these patients. The ideal bioengineered bowel would include regeneration of the mucosa for absorption of nutrients and the reestablishment of the neuromuscular apparatus necessary for motility.
Gut reconstruction using bioengineering methods remains a challenge given the complexity of this system. Even though it is a hollow tubular organ, the different cell types that makeup the gut have a highly specialized function under the control of the gut's own nervous system. This makes the cell source a major challenge in intestinal tissue engineering. In our approach, we first engineered the circular muscle layer and its intrinsic innervation using human gut-derived smooth muscle and neural progenitor cells. Our results indicate that autologous cells are an option for sourcing neuromuscular cells required or bioengineering tissues for the gastrointestinal tract. The selection of matrix materials for gut reconstruction is another challenge. Tubular chitosan scaffolds were selected as the matrices for the engineered human neuromuscular component. Our in vitro studies have previously characterized the mechanical characteristics of tubular chitosan scaffolds. 17 We have also demonstrated the biocompatibility of chitosan in vitro using gut-derived smooth muscle and gut-derived neurons.12,13 In the current study, we combined our techniques of engineering intrinsically innervated smooth muscle sheets and fabricating tubular chitosan scaffolds to develop hTEB for transplantation. Chitosan scaffolds supported maintenance of the alignment, phenotype, and function of the neuromuscular components as well as the neoepithelialization of the tissues. Vascularization of the hTEB was clearly seen after following implantation. Histological studies showed few chitosan residues after 4 weeks omentum implantation and almost no evidence of chitosan following transplantation. This indicated that chitosan degradation takes place within a 10-week implantation period. In a recent report, chitosan was used as a hydrogel sheet to repair a full thickness defect in the colon of rabbits. 18 Results have shown partial regeneration of the smooth muscle after 60 days of implantation. Our approach provides a tubular gut replacement with a functional, differentiated neuromuscular apparatus, and mucosal components that were maintained after a total of 10 weeks in vivo (omentum and transplantation). The transplanted segment had expected food residue in the lumen and was not distended or dilated. The neuromuscular apparatus appeared to have produced propulsion of food residua within the lumen along hTEB.
Omentum implantation
Our previous in vivo studies have evaluated hTEB implanted in subcutaneous tissues.14,16 The results of those studies were promising in that the hTEB appeared well vascularized. The next hurdle to overcome was the more practical site of implantation. Thus, a key objective of this study was to implant hTEB in a clinically relevant site (omentum) in preparation for transplantation. Thus, we conducted a two-step surgical approach. The first step was implantation of hTEB in the omentum as an in vivo bioreactor for neovascularization and maturation. This approach has been previously used for maturation of engineered intestines. 8 During the same surgery, a loop/bypass formation was performed to prepare for the subsequent transplantation of hTEB into the native intestine. The rationale behind the loop/bypass formation was to alleviate any potential obstruction caused by failure of the subsequent transplantation of hTEB.
Histologically, hTEB maintained the circular muscle alignment around the lumen after omental implantation. Alignment of regenerated smooth muscle in vivo has been a challenge. In a previous study, smooth muscle seeded onto small intestinal submucosa (SIS) showed regeneration in vivo, however, appropriate alignment was lacking. 19 In addition to alignment, smooth muscle plasticity and maintenance of the contractile phenotype have been the focus of many studies.19,20 In a previous study, preseeding SIS scaffolds with mesenchymal stem cells promoted smooth muscle layer regeneration with the appropriate architecture in vivo. 21 The muscle contractile phenotype of hTEB was maintained as indicated by positive smoothelin staining. Ensuring proper muscular function in addition to histological assessment is necessary for motility purposes. The smooth muscle contractile phenotype of hTEB was further confirmed by ACh-induced contraction. This contractile response was sensitive to atropine, a muscarinic receptor antagonist, indicating that ACh muscarinic receptors were maintained in hTEB. We then assessed the neural function in hTEB following implantation. EFS induced smooth muscle relaxation, which was partially inhibited by LNAME, indicating nitrergic contribution to the response. The harvested hTEB was compared with native small intestine forces. hTEB exhibited contractions that were lower in magnitude but similar in force patterns compared with native small intestine contractions (time to contraction peak, contractile plateau, slope of contraction, and percentage of inhibition in the presence of inhibitors). 16 Lower force generated by engineered intestinal tissues following implantation has been previously reported. 11 Increasing contractile force may relate to finding an optimal number of smooth muscle and neural progenitor cells to seed the scaffolds.
Transplantation surgery and the epithelial component
Besides contractile smooth muscle tissue, intestinal reconstruction requires a mucosal, absorptive component. Previous studies have adopted different approaches to bioengineer the gut with the focus on either specific biomaterials or cell types. Studies have looked at engineering the luminal geometry of the gut to regenerate the epithelium. 22 Most notably, the use of organoid units has gained special attention in the last couple of decades. Vacanti and colleagues have extensively used organoid units seeded onto polymers followed by implantation.7–9 This resulted in the formation of a tissue-engineered intestine with a well-characterized differentiated mucosa. However, there was little focus on the neuromusculature, which is essential for motility and propulsion of luminal contents. In our approach, we bioengineered sheets of innervated circular smooth muscle, wrapped them around the scaffolds, and then implanted them in the omentum. Organ bath studies indicated that the neuromuscular apparatus function was maintained.
Our second surgical step was to transplant the hTEB into the previously created loop of native intestine as a test for viability, neuromuscular viability, and neoepithelialization. Our hypothesis was that epithelial cells from the native intestine would proliferate and migrate into hTEB to form the neomucosa. Our hypothesis was driven by previous findings that documented the proliferation and migration capacity of the epithelial cells.23,24 Our histological results showed that after transplantation, native mucosal cells migrated into hTEB. Our study was conducted for 6 weeks posttransplantation. This resulted in partial neoepithelialization of hTEB. Cross sections of hTEB tissue from the center of the segment lacked a fully formed epithelium with villi structures. However, the rats were able to maintain their weights. Previous studies have shown that a fully differentiated neomucosa can take up to 12 weeks to develop. 10 Thus, longer periods of maturation are needed for full formation of neomucosa of the hTEB. Digested food residua were observed in the lumen of hTEB and no signs of bowel obstruction were seen, indicating that the hTEB produced propulsion of luminal content. hTEB motility patterns and neomucosa absorption characteristics require further study.
Our studies provide a successful proof of concept that hTEB can be developed from human cells, and that (1) hTEB was adequately vascularized and maintained its neuromuscular phenotype and function in vivo, (2) hTEB produced movement of luminal content, (3) neomucosa developed in the hTEB after anastomosis with native intestine, and (4) finally rats maintained weight and survived the hTEB anastomosis for 6 weeks as per protocol design. Our plan is to use the methods in this study to bioengineer hTEB for preclinical large-animal studies. The results in this study were promising and showed the feasibility of neoepithelialization of hTEB following anastomosis to native intestine. The size of the rat is a limiting factor when performing multiple surgeries involving the access of the abdominal cavity. Our future studies include the use of large-animal model, where hTEB will be evaluated in continuity with the native small intestine instead of its transplantation in the created loop. hTEB possesses the necessary cellular components for motility, digestion, and absorption and thus provides a novel therapeutic approach to restore and provide critical intestinal functions.
Conclusion
In conclusion, the work presented in this study is a proof of concept of the feasibility of transplanting hTEB in the small intestine of rats. hTEB was developed with an innervated prealigned smooth muscle component. hTEB was first implanted in the omentum as an internal bioreactor for maturation and vascularization purposes. Transplantation of hTEB resulted in the formation of a neomucosa, suggestive of epithelial cells' migration into the lumen of hTEB. Additional studies will look at the function of the neomucosa that formed.
Footnotes
Acknowledgment
This work was supported by Wake Forest School of Medicine Institutional Funds.
Disclosure Statement
No competing financial interests exist.