
Abstract
The human periodontium is a uniquely complex vital structure, supporting and anchoring the teeth in their alveolar sockets, thereby playing a decisive role in tooth homeostasis and function. Chronic periodontitis is a highly prevalent immune-inflammatory disease of the periodontium, affecting 15% of adult individuals, and is characterized by progressive destruction of the periodontal tooth-investing tissues, culminating in their irreversible damage. Current periodontal evidence-based treatment strategies achieve periodontal healing via repair processes, mostly combating the inflammatory component of the disease, to halt or reduce prospective periodontal tissue loss. However, complete periodontal tissue regeneration remains a hard fought-for goal in the field of periodontology and multiple in vitro and in vivo studies have been conducted, in the conquest to achieve a functional periodontal tissue regeneration in humans. The present review evaluates the current status of periodontal regeneration attempted through tissue-engineering concepts, ideal requirements for experimental animal models under investigation, the methods of induction and classification of the experimentally created periodontal defects, types of experimental defects employed in the diverse animal studies, as well as the current state of knowledge obtained from in vivo animal experiments, with special emphasis on large animal models.
The Periodontium and Periodontitis
T
Chronic periodontitis is a highly prevalent immune-inflammatory disease of the periodontium, affecting 15% of adult individuals, and is characterized by progressive destruction of the periodontal tooth-investing tissues, causing their irreversible damage. 6 Studies on periodontitis have associated it, although not demonstrating clearly a causal relationship, with major systemic disorders, including cardiovascular diseases, 7 rheumatoid arthritis, 8 adverse pregnancy outcomes, 9 diabetes mellitus,10,11 and gestational diabetes, 12 as well as shown a relationship between effective periodontal treatment and a good glycemic control. 13 The initiation of chronic periodontitis, with its associated periodontal destruction, commonly involves challenging the host's immune response through complexly orchestrated subgingival biofilms, harboring specific periodontal pathogens, chiefly Gram-negative anaerobes, and their associated virulence factors. 14 The pathological process initiated by these pathogens and their expressed virulence factors in the oral microbial biofilm incites the host's immune response, which primarily governs the disease's progression. 15 Polymorphonuclear lymphocytes (PMNs) release proteinases, lysozymes, and reactive oxygen species, through their respiratory burst,16–20 in addition to other mediators of periodontal and osseous destruction and remodeling, 21 inducing further oxidative damage, with catabolic changes to the adjoining periodontal tissues. The induced inflammatory response, in turn, triggers the activation of multiple cells, especially M1 macrophages, to start a massive production of pro-inflammatory cytokines, including tumor necrosis factor alpha (TNF-α), interleukin-1 beta (IL-1β), interleukin-4 (IL-4), interleukin-6 (IL-6), and interferon gamma (IFN-γ), which further contribute to and modulate the periodontal disease's severity and progression.15,21
Current periodontal evidence-based treatment strategies focus on a long-term control of bacterial plaque accumulation, both professional and through patient-performed oral hygiene measures (nonspecific plaque hypothesis), on changing the ecological niches favoring bacterial retention and pathological transformation (ecological plaque hypothesis), or additionally through eradicating certain bacterial species, which, even in very minute amounts, demonstrate an ability to manipulate the native immune system and change the microbial composition (specific or keystone-pathogen hypothesis). 22 These treatment strategies are mostly successful in eradicating the active inflammatory component of the periodontal disease, slowing down the rate of periodontal destruction and disease progression, as well as allowing long-term teeth retention and eventually periodontal tissue repair to occur. Although successful in these aspects, the disrobed strategies do not usually regenerate the lost periodontal tissues, but they mostly combat the inflammatory component to halt or reduce prospective periodontal tissue loss. However, through replacing lost tissue by healthy, but not regenerated, ones, the periodontium remains more susceptible to further periodontal breakdown and disease recurrence in the medium- and long term. 6
Periodontal Regeneration Through Tissue-Engineering Concepts
Periodontal regeneration is the complete restoration of lost tissues, after trauma or destructive periodontal disease, including the PDL, the gingival connective tissue, the cementum, and the alveolar bone, to their original structure and function. 23 Regeneration of these lost periodontal tissues remains a perplexing but ideal goal and a major challenge in the field of periodontology, requiring the harmonization of numerous molecular and cellular events.24,25 The first steps in the long way for periodontal regeneration through tissue engineering were paved by two early investigations describing the “compartmentalization” concept of the periodontium.26,27 In these pioneering studies, it was postulated that during a periodontal wound-healing process, four different tissue types compete to repopulate the defect: namely, the junctional epithelium, the gingival connective tissue, the PDL, and the alveolar bone cells. According to the “first come-first served” principle, the cellular types, which repopulate the defect first, subsequently dictate which tissues are formed. It was further hypothesized that, due to the difference in the mitotic rates, cells of the junctional epithelium, possessing the shortest cell-doubling time, usually repopulate the instrumented periodontal defects at a faster rate. The resultant healing is mostly a repair process, in the form of a hemi-desmosomal root-surface adherent “long-junctional epithelium,” isolating the root surface, preventing a reinsertion of the PDL fibers and a regeneration of the lost periodontal attachment. Accordingly, it was early assumed in a tissue-engineering concept that for any periodontal regeneration to succeed, a compartmentalization scheme has to be applied, excluding the junctional epithelium and the gingival connective tissue through a physical barrier, stabilizing the underlying blood clot, thereby allowing time and space for cells from the PDL to effectively divide and repopulate the defect area. This was subsequently tested, providing the proof-of-principle and the foundation for the guided tissue regeneration (GTR) techniques.28–32 From then onward, numerous animal and clinical trials attempted to build up the lost tissues to their original structure and function, employing multiple surgical techniques and materials in isolation and combined with GTR, including autogenous bone, freeze-dried bone allograft (FDBA), demineralized freeze-dried bone allograft (DFDBA), xenografts, alloplasts, various growth and differentiation factors, P-15 peptides, enamel matrix derivative (EMD), recombinant human platelet-derived growth factors (rhPDGF), platelet-rich plasma (PRP), platelet-rich fibrin (PRF), and, recently, neodymium:yttrium-aluminum-garnet (Nd:YAG) laser (Table 1).33–39 The magnitude of their regenerative effect was, however, variable, with capricious success in their outcomes and the obtained periodontal tissues were sometimes low in amount and of questionable quality compared with the originally lost ones.40–43 The procedure proved to be technically demanding, thus highly surgeon dependent, and demonstrated a great variability in attachment gain, with an average of eight sites that needed to be treated, for GTR to achieve one extra site gaining 2 mm or more attachment over open flap debridement.43,44 Many complexly interacting factors, including poor oral hygiene, an elevated plaque index score, cigarette smoking,45,46 the presence of specific periodonto-pathogenic bacteria, 47 early GTR membrane exposure, host response factors, 46 and defect morphology,48,49 have been further proved to affect the desired regenerative outcomes. The newly formed tissue showed high inconsistency in composition and quality, with random incidences of root resorption and ankylosis, as possible unfavorable outcomes50,51 and occasional detachment of the newly regenerated acellular cementum from the originally present root cementum on histological sections. 52 These factors, in addition to the elevated cost linked to GTR procedures and their low gain in clinical attachment, questioned their clinical significance and necessitated further developments to achieve a reliable periodontal regenerative outcome.
BDNF, brain-derived neurotrophic factor; BMPs, bone morphogenetic proteins; CGF, cementum growth factor; EMD, enamel matrix derivative; FDBA, freeze-dried bone allograft; bFGF, basic fibroblast growth factor; GDF, growth/differentiation factor; IGF, insulin-like growth factor; PRF, platelet-rich fibrin; PRP, platelet-rich plasma; PTFE, polytetrafluoroethylene; PTH, parathyroid hormone; SOST, sclerostin; TGF-β, transforming growth factor-β; VEGF, vascular endothelial growth factor.
At the turn of the century, a clearer vision of a periodontal tissue-engineering concept emerged, relying on the regulation of an array of early biologically orchestrated series of events, involving cell transplantation, with suitable scaffold materials and inductive biomolecules in the presence of sufficient blood supply (Fig. 1A), to further augment the aforementioned GTR approaches (Fig. 1B).6,24,53
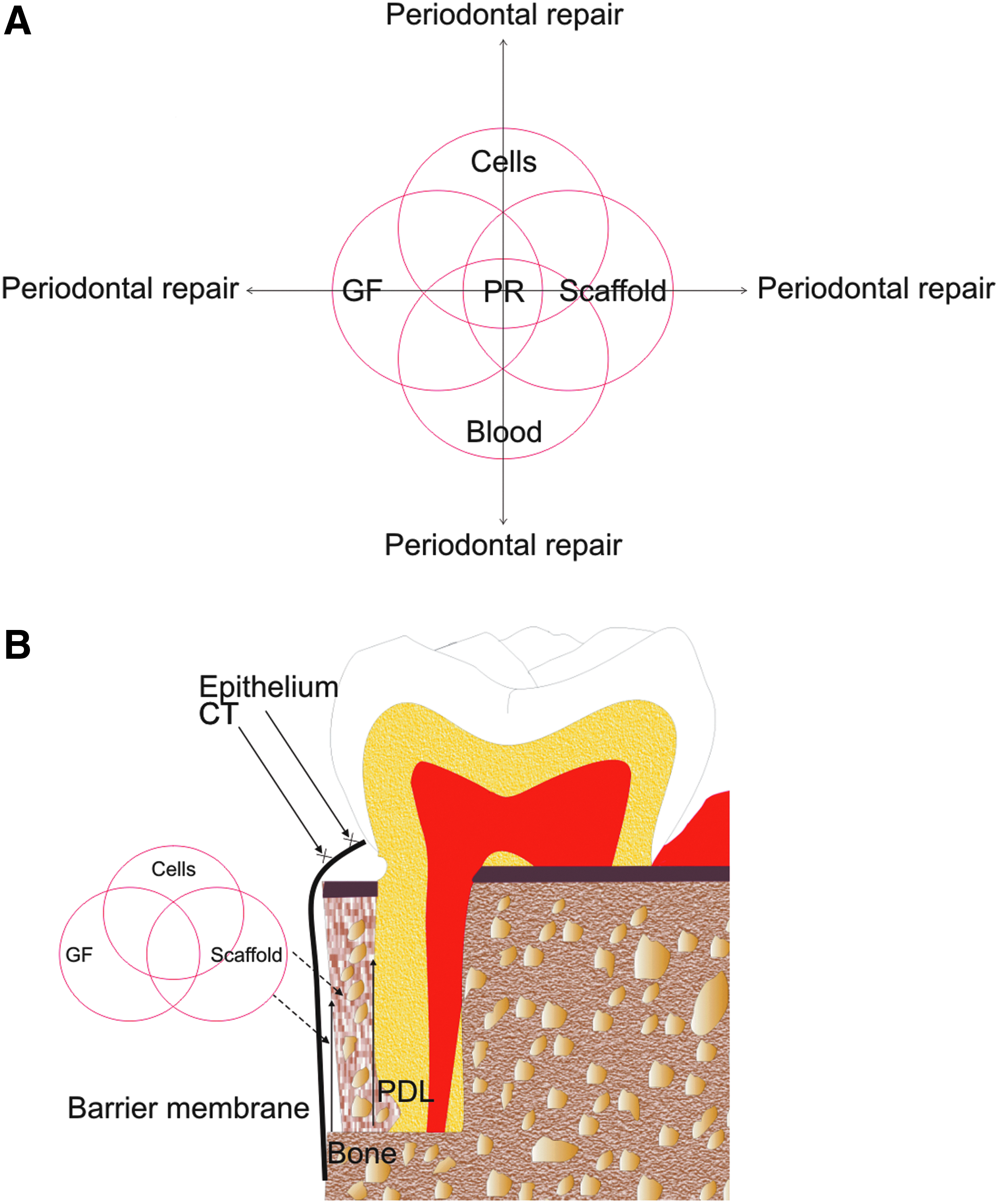
Periodontal regeneration through a tissue-engineering concept.
Cell transplantation
Cell transplantation in the field of periodontal tissue regeneration started relatively early, after the introduction of the compartmentalization theory, based on the postulation that after a periodontal destruction the residual cells in the PDL and alveolar compartments, especially the progenitors, would not be adequate to effectively divide and repopulate the diseased root surface, for a complete periodontal regeneration to occur. Initial trials involved the transplantation of ex vivo cultured fibroblasts 54 or mucoperiosteal free grafts 55 to provide the defect area with diverse cells, including undifferentiated mesenchymal cells, fibroblasts, periosteal cells, collagen fibers, extracellular matrix components, and native biomolecules. On the turn of the millennium and with the characterization of the first oral mesenchymal stem/progenitor cells (MSCs), the dental pulp stem cells (DPSCs), 56 a new area in the field of regenerative dentistry was inaugurated. This was quickly followed by the depiction of stem/progenitor cells from multiple oral tissue sources, 57 including stem cells from human exfoliated deciduous teeth (SHED), 58 periodontal ligament stem cells (PDLSCs), 2 dental follicle stem cells (DFSCs), 5 stem cells from the apical papilla (SCAP), 59 progenitors derived from the human adult salivary gland, 60 gingival mesenchymal stem cells (G-MSCs), 61 and alveolar bone proper-derived stem cells 4 (Fig. 2). The technical difficulty linked to the isolation and enrichment of these cells and the fact of their presence in very minute amounts in their native tissues, subsequently, opted the investigation into the possibility of inducing the widely available oral fibroblasts into induced pluripotent stem cells.62–64 Multiple cell delivery mechanisms have been proposed, including cell sheet transplantation, cell homing, cellular injection, and cellular transplantation in combination with a suitable scaffold. 65 Especially the introduction of these multipotent as well as pluripotent cellular lines appeared to solve a major problem in periodontal regeneration, through a tissue-engineering approach, providing a sufficient number of cells with the aptitude to differentiate into three different mesenchymal lineages: namely bone, cementum, and PDL, at least in theory.

Developmental scheme of human oral stem/progenitor cells. AB-MSCs: Alveolar bone proper-derived mesenchymal stem cells; DFSCs, dental follicle stem cells; DPSCs, dental pulp stem cells; G-MSCs, gingival mesenchymal stem cells; PDLSCs, periodontal ligament stem cells; SCAP, stem cells from the apical papilla; SHED, stem cells from human exfoliated deciduous teeth.
Growth factors and matrix proteins
Growth factors represent a large family of polypeptide molecules, binding predominantly to their cell-surface G protein-coupled receptors to modulate cellular responses. 23 Through their activity they regulate the signaling between cells and their environment, as well as control inter- and intracellular signaling processes, 66 thereby playing crucial roles in cellular proliferation, migration, chemotaxis, attachment/adhesion, differentiation, as well as tissue-healing responses. 67 The impact of multiple growth/differentiation factors has been tested both in vitro and in vivo in the field of periodontal tissue regeneration. The investigated biomolecules included bone morphogenetic proteins (BMPs), transforming growth factor-β (TGF-β), PDGF, insulin-like growth factor (IGF), vascular endothelial growth factor (VEGF), epidermal growth factor (EGF), parathyroid hormone, and fibroblast growth factor (FGF). More complex preparations and matrix proteins, including EMD, a collagen-binding peptide, utilizing a combination of anorganic bovine matrix and a synthetic clone of the 15-amino-acid sequence of type I collagen (P-15), PRP, PRF, and extracellular matrix proteins (e.g., collagen I, fibronectin, fibrinogen and hyaluronic acid),23,37,68–70 have further been tested with varying degrees of success in the field of periodontal regeneration (Table 2).
EGF, epidermal growth factor; OP-1, osteogenic protein-1; PDL, periodontal ligament.
Therapeutic application strategies, relying on utilizing growth/differentiation factors to restore damaged or lost periodontal tissues in a tissue-engineering concept, aim at mimicking early biological processes, occurring during embryonic and postnatal development. 71 Still, due to the complexity of the periodontal structures, stemming from distinctive tissues of different germ layers' origin, it remains challenging to date to identify the appropriate combination and quantities of growth/differentiation factors that are necessary to achieve a complete regeneration. 72 This intricacy necessitates a continuous development of optimal regenerative conditions, through combining different growth/differentiation factors, sequentially expressed during natural periodontal regenerative processes, in the presence of adequate cellular quantities and types and on suitable scaffolds.
Scaffolds
Multiple challenges are linked to the simplified approach of applying appropriate cells, growth/differentiation factors, and matrix proteins to influence periodontal cellular behavior. Delivery systems (carriers or scaffolds) play pivotal roles in the cellular regenerative response through their micro-environment-influencing attributes, including their surface area, their surface properties for cell-surface interactions, their possible inflammatory and immune reactions, and their degradation kinetics. 37 Ideally they should provide a biocompatible 3D design that supports the volume, shape, and mechanical strength of the desired tissues, with advantageous physical characteristics, such as hydrophilicity and porosity, necessary for cellular and tissue infiltration, and finally a degradation rate that would match the newly regenerating periodontal tissues' growth. 69 Well-designed scaffolds act as infrastructures, mimicking the natural cellular niches, thereby enhancing the innate regenerative potential of the host's tissues.73,74 Recently, 3D printing technologies have been introduced to provide defect-customized scaffolds with superior properties. 75
Investigated delivery systems in the field of periodontal tissue engineering include collagens (sponges, membranes or gels), gelatin with varying degrees of cross-linking, alloplastic and xenogeneic bone substitutes, synthetic resorbable materials, and hyaluronic acid-based gels.76–83 In the living organism, the release and degradation of growth factors is timely synchronized and rigidly controlled, in both concentration and duration before disappearance, which has not been fully elucidated yet. 23 This, however, poses a great challenge for any delivery system, attempting to imitate these normal but tightly controlled biological processes. The degradation and release kinetics of the biomolecules' carriers as well as their physical properties and pore size affect the cellular behavior and their differentiation capacities, as was seen with BMPs. A fast degradation and fast release of BMP-2 from its carrier induces bone formation to a greater extent, whereas cementum formation is significantly higher with a slow degrading and releasing BMP gelatin carriers.76,78 Whether the current technical and biomolecular developments will result in different optimized delivery materials, which could allow a sequential release and degradation of various growth/differentiation factors and differentiated cellular release in a pattern mimicking the regenerating human periodontium, remains to be a major challenge.
Animal Models in the Field of Periodontal Tissue Engineering
Over the history of scientific medical research, animal models have significantly contributed to the generation of substantial knowledge in the field of physiology, progression, treatment modalities, and pharmacology of multiple human diseases and their interactions, including diabetes mellitus,11,84 obesity,85,86 heart diseases,87–89 autoimmune arthritis, 90 and periodontitis.91–94 Animal models were initially employed to determine the bacterial etiology and the host's response in an effort to understand the pathogenesis of periodontal diseases95,96 and their progression mechanism. 97 The initial knowledge gained was priceless and incomparable to data obtained from even the most complexly concerted in vitro studies. The latter, apart from explaining multiple indispensable cellular mechanisms of the disease processes, cannot fully reproduce the complexity of living organisms and their inflammatory interaction with multispecies bacterial biofilms, which, in turn, change their composition in response to the biological tissue reactions. 98 In addition to studying the pathogenesis of periodontal diseases, animal models serve as valuable tools to scrutinize possible reparative, regenerative, and tissue-engineering periodontal treatment concepts and modalities, to provide histological evidence of their outcomes and to offer a means for translation of successful results into the clinical setting. 69
Animal models used to study various disease and tissue regeneration/repair modalities are generally classified under the following experimental sub-categories, according to their ability/inability to express certain pathological conditions comparable to humans
99
:
1. Experimental (Induced) model: an animal in which an experimentally reproduced condition mimics the human disease. 2. Spontaneous (genetic, mutant) model: an animal with a disease that occurs naturally and resembles a human disease, at least in some aspects. 3. Negative (None) model: an animal in which a particular disease cannot be induced. 4. Orphan model: an animal species demonstrating a disease that does not mimic a human disease. 5. In the past years, a fifth category of a genetically modified model, in which the genetically modified animal can be orchestrated to mimic the human disease in various specific aspects, has been added and is gaining clear importance in the field of experimental animal models.
Given the biological complexity of living organisms, animal models are a necessary standard for successful translation of regenerative materials and approaches to the clinical setting. Multiple animal species, comprising mice, rats, rabbits, dogs, sheep, pigs, and nonhuman primates, have been employed with variable degrees of success to test different disease and healing aspects in the fields of periodontitis and periodontal tissue regeneration. In the field of periodontal research, an animal model of interest should fulfill a number of prerequisites before considering it in experimental settings, mimicking human periodontal disease and healing processes.
Ideal Requirements for Experimental Periodontal Animal Models
• Availability and relevance to the research community
• Reasonable life expectancy
• Systemically healthy
• Background knowledge of indigenous factors peculiar to a species or a strain
• Background knowledge of animal's periodontal physiology, etiology, and pathogenesis
• Human analogy in dental periodontal characteristics in size and morphology
• Human analogy in periodontal disease occurrence and progression
• Human analogy in oral/periodontal microbiota
• Human analogy in healing mechanisms and properties
• Ease of periodontal disease induction
• Commercial availability of verified biomolecules for animal cells' manipulation
• Possibility of genetic modification of the organisms
• Genetic uniformity of the organisms
• Transferability of the obtained information to humans
• Eating habits not interfering with the induced defect model
• Reasonable costs, husbandry effort, nutrition, and availability
• Ethical approval
Experimental Defect Models
Periodontitis in animals can occur naturally, in certain species, or can be experimentally induced. To date, a number of standardized experimental defect models exist.
According to defect morphology
1. Periodontal pocket defects: The interdental alveolar bone related to a mesial or distal root surface and superficial root covering PDL as well as cementum layers are removed to produce one-, two-, or three-wall osseous defects, with well-defined dimensions 100 (Fig. 3A).
2. Keyhole defects: The alveolar bone filling the furcation between the roots in a molar is removed in a buccolingual direction partly (Class-II) or completely to form a “through and through” (Class-III) defect, in combination with superficial root cement and PDL denudation 101 (Fig. 3B).
3. Dehiscence defects: The alveolar bone covering the mid-buccal portion of the roots, superficial root cement, and PDL are removed. Usually performed on single rooted teeth as premolars 102 (Fig. 3C).
4. Recession defects: The facial gingiva is excised, and the root surfaces are exposed to the oral cavity 103 (Fig. 3D).
5. Irregular-shaped defects: Produced through spontaneous periodontitis, the inflammatory extension and irregular periodontal tissue loss after surgically inducing one of the defect shapes described earlier, ligature-induced periodontitis, the introduction of virulent bacterial species into the oral microbiota (oral gavage), or the injection of their virulence factors (e.g., lipopolysaccharide [LPS]) in the periodontal tissues (Fig. 3E).
6. Combined defects: A combination of all that has been just mentioned.

Currently employed experimental defect designs in the animal models for periodontal tissue regeneration investigations.
According to defect induction method
1. Naturally occurring periodontal defects: as in nonhuman primates and old beagle dogs.69,104,105
2. Foreign body introduction into the gingival sulcus (with or without addition of specific periodontal pathogens): as resin blocks, 106 impression materials, 101 orthodontic elastics, 107 ligature wires,11,108 or Porphyromonas gingivalis adhering to ligature wires109,110 introduction.
3. Surgically created periodontal defects: in one of the morphological forms described earlier.
4. Oral gavage method: the introduction of virulent bacterial species into the oral cavity: as P. gingivalis90,111 or P. gingivalis with Fusobacterium nucleatum 112 or P. gingivalis, Treponema denticola, and Tannerella forsythia. 113
5. Injection of periodontal destructive virulence factors into the periodontal tissues: as the periodontal injection of Aggregatibacter actinomycetemcomitans LPS, 114 to induce a periodontal inflammatory response with tissue destruction.
6. Exposure of the animals to chronic stress: as the exposure to chronic cold stress 115 or chronic stress in combination with ligature introduction around the teeth. 116
7. A combination of what has been just mentioned.
In the attempt to mimic the naturally occurring periodontitis, great emphasis is being placed on simulating the nature of the accompanying inflammatory response in addition to the defect's morphology. 107 Currently, controversies still exist among periodontal researchers, regarding the “chronic” versus the “acute” nature of the inflammation, culminating in the periodontal tissue loss, and whether periodontal breakdown occurs in bursts or as a slow and continuous destructive process. Thus, some studies resorted to chronicity induction with foreign body introduction into the surgically created defects for a certain period before treatment, whereas others immediately attempted periodontal tissue regeneration after the defects' induction.
Small Animal Models for Periodontal Tissue Engineering
Small animal models, including mice, ferrets, rats, and rabbits, represent clearly defined, predictable, and cost-effective biological systems, being previously and extensively tested in various medical disciplines. 98 Their dental formulas are very different to humans (mice and rat: I1/1, C0/0, Pm0/0, and M3/3; ferret: I3/3, C1/1, Pm 3/3, and M1/2; rabbit: I2/1, C0/0, Pm3/2, and M3/3). Their dentition demonstrates little similarity to humans, and their jaws are very small to allow for the surgical induction of human-similar periodontitis-mimicking defects.
Still, small animal models are extremely cost-effective compared with large ones. With the sequencing of the mouse genome, a new area in the field of animal models was inaugurated, enabling the investigation into the specific roles of genes in the regulation of multiple disease processes, inflammation, and regeneration. 98 Their major advantage lies in the fact that possible disease mechanisms and their impact on periodontal reparative/regenerative processes can be elaborated in vivo, using their genetically produced transgenic or knockout variants, especially in the mouse model, 117 which are usually very hard to develop in larger animal models. A further major advantage lies in the wide commercial availability of antibodies against mouse as well as rat antigens, similar to human panels, with great biological and immunological advantages for research.
Still, periodontal disease and inflammatory processes can be induced in diabetic mice or in mice with a certain predisposition to cardiovascular diseases.118–123 Periodontal disease can be successfully induced via the oral gavage method117,124 or alternatively through ligatures introduction around murine teeth, which, however, is an extremely difficult task,125,126 especially due to the very small sizes of their periodontal tissues anatomically. Although not a true periodontal disease model, the mouse calvarial defect model can provide valuable data on the efficacy of many regenerative agents, studying soft- and hard-tissue healing as well as the role of various molecules in the regulation of bone turnover and its regeneration. 98 Calculus accumulation rates and the effect of diet composition and dentifrices can further be well studied in ferrets. 127
In the field of periodontal tissue regeneration using small animal models, rats proved most suitable for dehiscence or recession-type experimental periodontal defects, encompassing multiple root surfaces. Surgical dehiscence-type128–132 or ligature-induced88,116,133–145 defects have been especially induced in the rat model. In rare cases, in which an interdental bone defect model is resorted to, it is usually very small 146 and a visual magnification of the surgical field is to be recommended.
Rabbits represent an interesting animal model, with human resemblance in periodontal physiology and pathology. 98 Their major disadvantage lies in the limited availability of commercial anti-rabbit antibodies. Analogous to the mouse model, transgenic rabbits have been also produced, to study periodontal and atherosclerotic diseases. 98 In contrast to the murine and rat models, ligature introduction alone into the periodontal crevice is not sufficient to induce a periodontal disease in the rabbit model. Periodontitis, however, can be generated in rabbits through ligatures introduction in combination with topical application of periodontitis-specific microorganism, for example, P. gingivalis.147–151 Although not truly representing a periodontal tissue regeneration study, recently beta tricalcium phosphate (β-TCP), 5 × 106/mL PDLSCs/β-TCP, or 5 × 106/mL human osteoprotegerin (hOPG)-transfected PDLSCs/β-TCP were transplanted into segmental critical-size alveolar bone defects. Histological evaluation at 12 weeks demonstrated that the implantation of hOPG-transfected PDLSCs significantly contributed to the newly formed bone. 152
Hence, small animal models, although due to their anatomical minuteness, not representing the ideal human-simulating periodontal regeneration model, could generate valuable data on the interactions between various body cells and tissues, especially during inflammation and healing processes. Their major advantage lies in the possibilities of producing transgenic or knockout variants to answer precise research questions related to a single biological aspect. In case these animals answer the specific research questions adequately, they eliminate the further need for larger species use. A direct human clinical translation of the data obtained from these small animal models is, however, uncommon, before verifying the experimental findings in a larger animal model, with greater biological complexity and human resemblance.
Large Animal Models for Periodontal Tissue Engineering
However, showing phylogenetically the closest human resemblance, the major limitation linked to the routine use of larger animals in periodontal experimental studies lies in their elevated cost and their requirement of specialized breeding and maintenance facilities in expert centers, equipped with pertinent staff. Resembling human dento-alveolar architecture more closely than smaller animals, the dental anatomy of larger species, such as nonhuman primates, dogs, miniature pigs, and sheep, allows more unambiguous interpretation and mostly direct translation of the obtained knowledge on periodontal disease and regeneration to human clinical settings. Their oral structures show different grades of human similarities histologically and functionally, with naturally occurring dental oral microbial plaque, calculus, and periodontal diseases, with their characteristic inflammatory cellular infiltrate. 91
Nonhuman primates
Nonhuman primates exhibit great resemblance to human organisms in structure, function, and disease occurrence. Their sizes vary from 300 to 350 g in certain marmosets to large sizes approximating humans (e.g., chimpanzees and gorillas). Macaques, chimpanzees, and baboons demonstrate the same dental formula as humans: I2/2, C1/1, Pm2/2, and M3/3; whereas cotton-ear marmosets (Callithrix jacchus), cotton-top marmosets (Saguinus oedipus) (both I2/2, C1/1, Pm3/3, and M2/2), squirrel monkeys (Saimiri sciureus), and bushbabies (Galago senegalensis) (both I2/2, C1/1, Pm3/3, and M3/3) show different patterns. 104 Their teeth and periodontal structures show human similarities, with naturally occurring dental plaque harboring periodontal pathogens (e.g., P. gingivalis), calculus, and destructive periodontal disease.91,153 In particular, cynomolgus monkeys (Macaca fascicularis), rhesus monkeys (Macaca mulatta), and baboons (Papio anubis) exhibit Gram-positive rods and cocci in their supragingival as well as Gram-negative rods in their subgingival plaque and are susceptible to spontaneous periodontal disease development.69,104,105 Multiple earlier animal experiments employed nonhuman primates in an endeavor to explore the pathogenesis of periodontal disease.104,154
In clinical settings, multiple experimental devices were employed to accelerate plaque accumulation, including orthodontic elastics or nonresorbable suture material, which were commonly placed apical at the gingival margin as well as interproximally around selected molars. 107 Ligatures were changed every 1 to 2 weeks, 155 until periodontitis with its hallmarks of bleeding and periodontal pocket formation were confirmed. Investigations at 2 and 10 weeks after ligature introduction demonstrated dense connective tissue inflammatory cellular infiltrate, primarily granulocytes and macrophages with small percentages of lymphoid and plasma cells, apical to the buccal and interproximal gingival sulci. 156 Being nonresorbable, these materials, in addition to their physical plaque accumulation action, incite chronic inflammation in the adjoining periodontal tissues. A second strategy to induce periodontitis in these nonhuman primates was later introduced, relying on the oral inoculation of virulent human pathogens to disturb their native oral microbiota. An investigation involved the introduction of P. gingivalis, which were not previously detectable in Cynomolgus monkeys' oral microbiota. Five months later, the established P. gingivalis infection resulted in visible plaque formation and alveolar bone loss.157,158
Apart from periodontitis induction, nonhuman primates were successfully employed in periodontal tissue regeneration approaches employing tissue-engineering strategies. 159 The periodontal regenerative potential of various proposed surgical techniques has been intensely investigated in studies on rhesus monkeys.160–162 Periodontal regeneration, using the principle of selective and guided cell repopulation of the root surface via the GTR principle, was further histologically investigated in primates. Experimental osseous defects extending 2 mm apically from the alveolar ridge after root-surface denudation and notch marking, followed by a 6 month placement of millipore filter barriers, demonstrated new cementum formation, with inserting fibers in the apical and connective tissue attachment in the coronal defects' root surfaces. 29 The same principle was examined histometrically in a fenestration model in squirrel monkeys 163 and M. fascicularis monkeys. 164 A study, using an adult Taiwan monkey model, designed to determine the histologic response of tissues regenerated through GTR to the presence of plaque, imitated a periodontitis condition, through surgically creating experimental standardized two-walled periodontal defects at the mandibular lateral incisors (5 mm deep × 3 mm wide), followed by an 8 week placement of 3-0 braided silk sutures to induce chronicity. At 8 weeks, the defects were exposed, instrumented, and covered by expanded polytetrafluoroethylene (ePTFE) membranes for compartmentalization for 6 months, with the presence of plaque retentive silk sutures for the initial 2 to 10 weeks. Histological and histometrical results indicated that plaque-induced inflammation was less at sites treated by GTR, though the newly formed osseous tissue was compromised under these inflammatory conditions. 165 Further, a study examined the amount of defect fill after a GTR treatment of surgically created Grade-II furcation defects in baboons' molars volumetrically and histologically. It concluded that the overall defect fill was 70.75–74.98%, with the undesirable histological result that connective tissue occupied a major proportion of the newly formed tissues, representing a periodontal repair response instead of a desired true regeneration. 166 The impact of the original defect morphology and treatment material on the periodontal regenerative outcome was examined in an additional study. Adult baboons (P. anubis), with three-wall as well as two-wall intrabony defects (5 mm deep × 3 mm wide) and ligature placement for 8 weeks to induce chronicity and plaque retention were treated by GTR, GTR+DFDBA, or GTR+DFDBA+DFDB-glycoprotein sponge matrix. After a 6 month follow-up, three-wall defects showed no differences between treatments, whereas superior results were demonstrated in the two-wall defects treated by GTR+DFDBA in terms of clinical parameters and histological tissue formation. 167
In a tissue-engineering manner, root-surface bio-modification/conditioning to remove the smear layer and expose residual cementum-inserted intact collagen fibrils has been proposed to encourage periodontal regeneration, through favoring fibroblasts attachment, fibrin linkage deposition and discouraging long junctional epithelium attachment and migration along the exposed root surface. Dehiscence defects with root-covering bone and cementum removal in adult monkeys (M. fascicularis) were treated with 24% Ethylenediaminetetraacetic acid (EDTA; pH = 7) for 8 min or citric acid (pH = 1) for 3 min, the flaps were repositioned, and the healing was histomorphometrically evaluated after 8 weeks. EDTA root-surface bio-modification appeared to improve periodontal healing, with reduced long junctional epithelium and increased connective tissue attachment. In contrast to citric acid, EDTA showed no tissue-necrotizing effect. 102
The induction of periodontal regeneration through tissue engineering via growth/differentiation factors to stimulate and direct the selective differentiation of tissue resident cells, through differential signaling, into the desired regenerative phenotypes was further attempted. The importance of the presence of fibrin linkage on a successful periodontal attachment to the root surface was examined in an extraction-replantation study in squirrel monkeys. Histological examination at 1, 3, 7, and 21 days 168 demonstrated the importance of its presence as a prerequisite for any successful periodontal tissue regeneration. Topical application of basic fibroblast growth factor (bFGF or FGF-2) with fibrin gel to the exposed root surface was examined in surgically created alveolar bone defects (4 mm apical × 3 mm horizontal two-wall, three-wall, and furcation Class-II defects, with cementum and bone removal) in beagle dogs and primates. At 6 or 8 weeks, significant periodontal regeneration with PDL formation, new cementum, and new bone deposition was evident in amounts greater than in control sites, with no epithelial down-growth, ankylosis, or root resorption. 169 A further investigation in M. fascicularis topically applied 0.1% or 0.4% human recombinant FGF-2 on a gelatinous carrier into surgically created Class-II furcation defects (4 mm apical × 3 mm horizontal, with bone and cementum removal), where inflammation was chronically induced by the introduction of vinyl polysiloxane impression material into the defects for 4 weeks. Eight weeks later, significant periodontal regeneration was dose dependently evident, with no epithelial down-growth, ankylosis, or root resorption observed. 170 BMP-2 induces the recruitment and differentiation of MSCs lines into mature osteoblasts and adipocytes, 171 and it regulates alkaline phosphatase expression and osteoblast mineralization. 172 Studies on BMP-2 demonstrated its aptitude to enhance osteoblastic markers' expression of multipotent and pluripotent cells,173,174 fibroblasts, 175 stromal cells,176,177 and myoblasts 178 in cultures, as well as showed osteoinductive properties in the regeneration of critical-sized calvarial bony defects in rats. 179 BMPs on collagenous matrix transplantation further demonstrated periodontal regeneration in baboons (Papio ursinus) in large Class-II furcation defects (10–12 mm in depth) after 60 days. 180 In a further study, chronic Class-II furcation defects in adult baboons (P. ursinus) were treated by heterotopic ossicles induced within the rectus abdominis muscle, 40 days after an intramuscular injection of TGF-β in a matrigel carrier or of recombinant human TGF-β combined with recombinant human osteogenic protein-1 (OP-1) in insoluble collagenous bone matrix carrier. The defects receiving the tissue-engineered ossicles showed substantial periodontal regeneration compared with their controls. 181
EMD is composed of a mixture of hydrophobic enamel matrix proteins, nearly 90% amelogenin, along with amelin, enamelin, tuftelin, and ameloblastin, 182 in a polyglycolic acid (PGA) carrier. During embryonic tooth germ development, EMD is usually produced by the epithelial root sheath of Hertwig and plays a pivotal role in root cementogenesis as well as in the development of the PDL, anchoring the root cementum to the surrounding alveolar bone. 183 Various in vitro studies reported on the aptitude of EMD to induce proliferation, migration, adhesion, mineralization, and differentiation as well as the increased collagen and protein production in alveolar bone, PDL, and dental follicle cells in culture.174,184–186 The combined treatment of 6–8 mm deep chronic periodontal defects (metal strips were used to induce chronicity and retain plaque) in adult monkeys (M. fascicularis) by GTR+EMD was examined after 5 months, showing no substantial differences to GTR or no-treatment sites immunohistochemically, apart from a stronger immunostaining for Collagen-III. 187 EMD in combination with autogenous bone grafting and EDTA root-surface treatment was further applied into surgically created periodontal defects in baboons (P. anubis) (chronicity induced by ligature wire for 2 months), stimulating statistically significant periodontal regeneration histologically after 5 months, with new alveolar bone, cementum, and PDL formation. 188
Generally, results from studies on nonhuman primates clearly demonstrated their great validity as human-resembling experimental animal models in the field of periodontal disease induction and treatment. The initial investigations of various periodontal regeneration endeavors outlined earlier, employing GTR in combination with bone substitutes, various growth/differentiation factors, and root-surface bio-modification in a tissue-engineering concept, provided great insight into the potential as well as possible shortcomings needing further improvement. Apart from conflicting results on EMD, bFGF and BMP-2 (the important member of the TGF-β family) appeared to be growth/differentiation factors, clearly fostering periodontal regeneration. In addition, EDTA root-surface bio-modification appeared to provide biologically enhanced environmental conditions for periodontal healing outcomes. The results paved the way for a direct human clinical translation and shed new light on areas needing deeper investigations and improvement.
However, although representing these clear advantages and the highest resemblance to the human organisms, nonhuman primates demonstrate chief concerns, including their aptitude to show seriously infectious human disease, including tuberculosis, 104 in addition to various ethical concerns expressed in connection to their trafficking and current use in preclinical experimental settings. To overcome these concerns, other large animal models, showing lesser human resemblance phylogenetically, including dogs, miniature pigs and sheep, have been suggested as suitable alternatives.
Dogs
Dogs provide an excellent animal model to study surgical techniques, periodontal disease, wound healing, and regeneration.189–195 They demonstrate naturally occurring gingivitis and periodontitis, with dense inflammatory cellular infiltrate, bleeding on probing, bone loss, and recession,196–198 increasing in severity with age and frequently resulting in tooth loss. 91 Especially, the beagle dog is commonly used due to its suitable size and its extremely cooperative temperament, 199 though multiple investigations have also employed the mongrel dog. 98 Their permanent dentition formula is I3/3, C1/1, Pm4/4, and M2/3. 199 Similar to humans, their periodontal supragingival microbiota harbors Gram-positive cocci, whereas the subgingival microbiota harbors predominantly virulent anaerobic Gram-negative cocci and rods, especially Capnocytophaga, P. gingivalis, and F. nucleatum.95,200 Their teeth, gingival sulcus (2–3 mm), periodontal tissue size, and characteristics are comparable to humans.98,199,201 Susceptibility or resistance to periodontal disease observed between different breeds was mainly ascribed to genetic variations 202 rather than to diet. 197 However, major differences to humans exist in their oral occlusal function, lacking lateral movements of the jaws as well as occlusal contacts at the premolar level, the absence of lateral contacts between their teeth, and the different compositions for periodontal plaque and calculus.198,199
Gingivitis in dogs may be accelerated by a special soft-minced diet and can eventually progress to experimental periodontitis,95,200,203–205 with inflammatory cellular infiltrate, bone resorption, and deep narrow pocket formation. 95 Furcation areas and first and second premolars are more frequently affected by periodontitis compared with interdental regions. 199 Apart from spontaneously occurring periodontitis, especially in furcation areas of old dogs, experimental periodontitis can be induced in dogs through a 4- to 6-month placement of silk ligatures around teeth. 206 In addition, surgically created interdental periodontal defects in dogs, measuring 4 mm in depth and width (one- or three wall), 207 buccal fenestration defects, 208 or soft tissue recession defects, 103 are considered reproducible models, mimicking human periodontal diseases and allowing the evaluation of various biomaterials and concepts in periodontal regeneration and tissue engineering. Extent and localization of the resultant periodontal lesions may, however, not always be predictable, as further inflammatory-induced bone loss may alter the induced morphologies. 190
The dog experimental animal model has always been a very popular one in periodontal regeneration approaches employing tissue-engineering concepts, testing various cellular, biomaterial, and scaffold variants, isolated or in combination. 98 In one of the earliest periodontal cellular transplantation approaches, the transplantation of gingival and PDL cells, in combination with roots demineralized for 48 h in 0.5 M EDTA (pH = 7.4), revealed that only roots cultured with PDL cells showed new PDL ligament formation. 209 The early notion that bone substitutes' transplantation into periodontal defects could result in complete reconstitution of the cementum, PDL, and alveolar bone has been tested in dogs. In a study on surgically induced mandibular bicuspid interproximal 3 mm circumferential defects, notches were created on the root at the alveolar bone level and chronicity was assured via tin foil introduction for 30 days. Calfskin collagen-mineral gel was then introduced, after the tin foil removal and cleaning of the defects. Eight weeks follow-up demonstrated no periodontal regeneration. 210 In a second study, β-TCP-collagen complex was inserted into three-wall bony defects (5 mm depth × 5 mm mesiodistal × 3 mm buccolingual) in the fourth premolar and second molar areas in mongrel dogs. Chronicity was induced via a resin block introduction into the defects for 6 weeks, followed by its removal for 2 weeks, before hydroxyapatite (HA)-β-TCP-collagen 211 or β-TCP-collagen 106 complex introduction. Four weeks after implantation, histological evaluation demonstrated a suppression in junctional epithelial down-growth, increased cementum/cementoid, and PDL fiber formation with bone regeneration. In a further investigation, nonresorbable calcium-layered polymers of polymethyl-methacrylate and hydroxyethyl-methacrylate were surgically placed in surgically created acute buccal furcation defect areas in the premolar area, with notches placed on the roots at alveolar bone level. Histological results after 4 months contrastingly failed to demonstrate a periodontal regeneration. 212 Thermosensitive biodegradable chitosan hydrogel prepared from autoclaved chitosan powder (121°C, 10 min) and β-glycerophosphate (chitosan-PA/GP; 9:1) was further introduced into mixed-breed dog chronic 5 mm deep Class-III furcation defect models (chronicity induced via introduction of impression material for 21 days). Twelve weeks after treatment, histological evaluation demonstrated a good biocompatibility of the material, with the ability to support periodontal regeneration with new cementum, alveolar bone, and PDL formation. 213 These initial investigations on the introduction of various biomaterials into dogs' experimental periodontal defects gave early insights into the biocompatibility and regenerative aptitude of various material categories used in dentistry.
The compartmentalization theory, the foundation of the periodontal regeneration through a tissue-engineering concept, was primarily tested almost 37 years ago in a dog model. 28 GTR principles were verified in a naturally occurring periodontist model in a beagle dog model, with interdental contact closure between the investigated teeth, via an orthodontic wire.214–216 The principle of GTR, its biocompatibility, and the efficacy of different membrane designs and materials, whether nonresorbable or resorbable, have been subsequently extensively tested in the dog model,217–226 demonstrating histologically that GTR is realizable in different defect types, including furcation areas and infrabony resorption sites, with various degrees of success. The studies demonstrated the existence of a significant linear relationship between cementum, PDL, and bone regeneration. These studies further outlined limitations and challenges in the field of GTR related to defect morphology, 227 as horizontal bone loss, reduced number of osseous walls, or Class-III furcation involvement,228–232 as well as to membrane properties, providing the foundation for decision making for GTR periodontal regenerative approaches, 37 combining GTR membranes with various root-surface treatment, cellular, biomolecular, scaffolds, or hard tissue substitute materials. They further underlined the importance of space provision as a determining factor for the possibly regenerated periodontal tissue. A study on GTR polylactic acid (PLA) membranes of various compositions showed that all possessed equal periodontal regenerative aptitudes in beagle dogs. 233 Overall, 3 × 4 mm keyhole defects, with plaque retentive impression material placed in the furcation areas of the third molars in beagle dogs, were treated by resorbable or nonresorbable GTR membranes (removed after 30 days) and followed up for 5 months. Histological evaluation revealed that periodontal tissue regeneration was achievable in both groups, provided flap coverage was maintained, with no difference between GTR membrane categories. 101 Further, the treatment of naturally occurring Class-II furcation defects via resorbable PLA GTR barrier demonstrated successful periodontal regeneration of 71% of the original defects' size at 6 months, histologically. 234
Root-surface conditioning, testing a variety of chemical agents to remove the root-surface smear layer, expose collagen fiber bundles, discourage epithelial down-growth, and encourage connective tissue attachment, was extensively investigated in the dog experimental model, with contrasting results. Periodontal furcation pockets in Labrador retriever dogs treated by root-surface instrumentation, followed by 3 min citric acid (pH = 1), showed furcation closure, with cementum regeneration by 6 weeks, histologically. 235 Repeating the procedure after a further 6 weeks with additional antibiotic or gel foam application did not improve the outcome.236,237 In a second investigation, buccal fenestration defects (4 × 7 mm) and two cylindrical cavities 2 and 1 mm in diameter were prepared over the root surfaces, followed by 4 min citric acid application (pH = 1) and 2 min washing by physiological saline and flap suturing. Follow-up ranged between 60 and 126 days followed by histological evaluation. Cementum with sometimes functionally oriented PDL fibers and regenerated alveolar bone was evident in some but not all test sites. 238 In a further investigation, alveolar bone around mandibular premolars was surgically reduced 3–6 mm from the cemento-enamel junction and the denuded root surfaces were exposed to the oral environment for 3 months, without plaque control. At 3 months, the roots were instrumented to remove plaque/calculus and citric acid conditioning of the exposed root surfaces was applied for 3 min followed by coronally positioned flaps. Six months later, histologic evaluation revealed new attachment over extended portions of the root surfaces, with mostly no epithelial down-growth apical to the cemento-enamel junction and variable amounts of bone regeneration. A similar study induced periodontitis via silk ligatures in combination with soft diet for 8 months. After scaling and root planning, citric acid root conditioning was applied for 3 min, followed by tetracycline salt application. After 48 days, histological evaluation revealed a new periodontal attachment, with increased cementum and PDL formation compared with their controls. 239 In contrast, a study testing citric acid or tetracycline HCl root-surface treatment showed no favorable effect for their application. 68 However, although numerous investigations on root-surface bio-modification agents demonstrated encouraging results, root resorption and ankylosis were very widespread features. 240 A study in beagle dogs, using fenestration wound models, 2–3 mm apical to the alveolar ridge, applied citric acid (pH = 1) for 3 min, showing variable attachment level formation, with lower cementum and higher incidences of ankyloses and root resorption in the test group after 3 months, histologically. 241
Various growth/differentiation factors and biomolecules have been extensively tested for their periodontal tissue regenerative potential in the dog model, employing a tissue-engineering scheme. rhBMP-2 on gelatin/polylactic-polyglycolic acid copolymer sponge was applied into experimental circumferential and furcation defects, induced through silk ligature placement in adult beagle dogs. Twelve weeks later, histological assessment demonstrated considerable new bone formation, new cementum, and regenerated PDL fibers. 242 OP-1 in three different concentrations on a collagen vehicle (0.75, 2.5, or 7.5 mg/g) was further applied into 5 mm deep Class-III furcation osseous defects in beagle dogs. Eight weeks later, histological assessment demonstrated osteogenesis, regenerated cementum, and new attachment formation with all three concentrations. 243 Three microgram 244 and 1 or 3 μg 105 of PDGF/IGF-I in methylcellulose gel surgically placed after periodontal flap reflection enhanced periodontal regeneration, resulting in a significant increase in new bone formation, new cementum, and periodontal attachment in 5–7 year-old beagle dogs with naturally occurring periodontal disease. In six mongrel dogs, 4 × 4 mm fenestration defects were treated with PDGF and ePTFE GTR membranes. Results at 1, 3, and 7 days demonstrated enhanced fibroblast proliferation, with no additional benefits obtained from the GTR membrane. 245 Collagen sponges, impregnated with 200 ng IGF-II, 20 ng bFGF, and 6 ng TGF-β1 and fitted into 3 mm-diameter fenestration defects, showed impaired bone formation and did not enhance fibroblasts or collagen density at 10 and 14 days after surgery. 246 The combination of PDGF-BB with root-surface citric acid preconditioning in the treatment of experimental 4-week ligature induced Class-III furcation defects in beagle dogs, shown at 5 and 8 weeks effective periodontal regeneration, with new bone and PDL and without significant ankylosis or root resorption. 247 Autologous fibrinogen and absorbable GTR membrane combination in the treatment of surgically induced chronic Grade-III furcation defects in beagle dogs enhanced the amount of periodontal healing at 3 months, with the positive effect disappearing at 6 months compared with their controls. 248 ePTFE GTR membrane in combination with Anorganic Bone Matrix/Synthetic Cell-Binding Peptide (P-15) was employed to treat mongrel dogs' chronic 5 mm-deep Class-III furcation (chronicity induced via introduction of impression material for 21 days) defects model. Four weeks later, the GTR membranes were removed. At 12 weeks, no differences were noted for ePTFE+P-15 and ePTFE, with both being unable to fully re-fill the Class-III defects. 249 GTR treatment of experimental dehiscence defects with fibronectin solution rehydrated collagen membranes in mongrel dogs for 30 days demonstrated no difference in epithelial down-growth and cementum or bone formation. 250 Recombinant human growth differentiation factor-5 (rhGDF-5)/PLGA was tested in the regeneration of 3 × 6 mm (width × depth) periodontal defects in Hound Labrador mongrel dogs. PDL and cementum regeneration was twofold greater for the control sites at 4 weeks, whereas bone formation increased at sites receiving rhGDF-5/PLGA. 202 The effects of FGF-2 in hydroxypropyl cellulose in the treatment of three-wall periodontal defects (mesiodistal width × buccolingual width × depth: 5 × 3 × 4 mm, no chronicity induced) were investigated in beagle dogs. Cell proliferation around the existing bone and PDL, connective tissue formation on the root surface, and new bone formation were significantly promoted by FGF-2, with an increase in the number of blood vessels at 7 days. At 28 days, new cementum and PDL were extended by FGF-2 treatment and FGF-2 increased the expression of BMP-2 and osteoblast differentiation markers (osterix, alkaline phosphatase, and osteocalcin) in the regenerated tissue. 251
In a similar tissue-engineering approach, EMD has been extensively tested for its potential in the field of periodontal tissue regeneration. 252 In a pilot dog animal study, EMD applied to spontaneously induced periodontitis lesions via an open flap access showed increased bone and clinical attachment levels at 1 and 4 months. 250 Enamel matrix protein was applied to spontaneously occurring periodontal defects in dogs, resulting in an increase in periodontal attachment and bone level. 253 Surgically created recession defects on the upper cuspids in mongrel dogs were treated by EMD and coronally repositioned flaps, demonstrating, in contrast, no additional benefit of EMD application. 254 EMD and root-surface bio-modification via 36% orthophosphoric acid were compared in an experimental periodontitis model in Turkish sheep dogs (defect: 1 mm in depth buccolingual × 6 mm from the cemento-enamel junction apically, with chronicity induced via 45 days of ligature inclusion). Results at 7, 14, 21, and 28 days demonstrated significant periodontal regeneration in the EMD group, with inhibition of gingival epithelium down-growth, stimulation of connective tissue proliferation and attachment to the root surfaces, and acellular cementum and new alveolar bone regeneration, compared with the root-surface conditioning group. 255 EMD application has also been found to reduce the deleterious effect of nicotine on periodontal tissue regeneration. 256 The 15-, 17-kDa sheath protein in enamel proteins, EMD, or TGF-β1 was applied to surgically induced 5 mm-deep dehiscence defects in beagle dogs, after partial cementum removal, notching, and root-surface treatment via EDTA. Eight weeks later, histological analysis revealed that 17-kDa sheath protein produced the thickest cementum regeneration. 257 In a gingival recession study in adult beagle dogs (defects measuring 6 × 5 mm, with two notches on the root surfaces at the most coronal and apical defect extents), defects were treated with GTR+EMD or GTR alone. Results at 2, 4, or 8 weeks showed a statistically significant increase in new bone and cementum formation in the GTR+EMD compared with the GTR group. 258 Statins, including levostatins, are lipid-lowering drugs, with anti-inflammatory, antioxidant, as well as periodontal and bone-forming properties. 259 Tetracyclines are broad spectrum antibiotics with additional anti-collagenolytic effects. 260 Local delivery of combined PLGA-lovastatin-chitosan-tetracycline 0.3% nanoparticles prepared as a hydrogel by mixing with gelatine (10 mg/100 mm3) in three-walled defects in beagle dogs (4 × 4 × 5 mm: buccolingual, mesiodistal, and depth, respectively, no chronicity induced), with residual cementum removal via scaling and root planning, was investigated. Eight weeks later, micro-computed tomography and histological examination revealed significantly periodontal regeneration, with increased new bone formation, new cementum, and connective tissue. 261
Cellular transplantation approaches for periodontal tissue engineering have been attempted in the dog model with various successful outcomes. Overall, 2 × 106, 5 × 106, 1 × 107, or 2 × 107 bone marrow stromal cells (BMSCs)/mL mixed with atelocollagen (2% type I collagen) were auto-transplanted into experimental Class-III defects in beagle dogs. After 1 month, histological evaluation revealed significant periodontal regeneration, with higher cementum formation in the 5 × 106 and 2 × 107 BMSCs/mL groups and higher bone formation in the 2 × 107 BMSCs/mL group. 262 Autologous 1 × 105 PDLSCs sheets in combination with hyaluronic acid carriers have been applied in surgically induced fenestration defects (5 × 5 mm) in beagle dogs. Histological and histometric results after 8 weeks demonstrated periodontal tissue regeneration with bone, cementum, and PDL formation and signs of ankylosis in some specimens. 263 Autologous 2 × 107 BMSCs/mL in atelocollagen transplantation for Class-III furcation defects treatment in premolars showed regenerated PDL, connecting the new bone and cementum, but an incomplete alveolar bone reconstruction. 264 Tri-layered cell sheets formed of 9 × 104 PDLSCs and polyglycolic acid (PGA) in combination with β-TCP were applied into three-wall osseous defects (5 × 5 × 4 mm in depth, mesiodistal width, and buccolingual width, respectively), resulting in complete periodontal regeneration, with newly formed bone and cementum connected via well-oriented collagen fibers. 265 Overall, 5 × 106 BMSCs on collagen membranes were transplanted into fenestration defects (5 × 5 mm) in beagle dogs and covered by ePTFE membranes. Eight weeks later, histological evaluation demonstrated periodontal regeneration with newly formed cementum, alveolar bone, and PDL. 266 Next, 5 × 106 autogenous periosteal cells combined with β-TCP were transplanted into surgically created Class-III furcation defects in beagle dogs. Histological evaluation after 12 weeks revealed increased PDL, bone, and cementum formation. 267 Then, 7.5 × 105 autologous cementum or PDL-derived cells on collagen sponge were transplanted into three-wall osseous defects (3 mm wide × 4 mm deep) in dogs. Histologically, both groups demonstrated periodontal regeneration, with no signs of root resorption or ankyloses and rich capillary vessels. Greater new-bone formation was observed in the PDLSCs group. 268 Then, 6 × 106 autologous dental pulp, PDL, or peri-apical follicular stem cells transplanted apically in 3 mm-wide circumferential deep defects showed a favorable healing response. Eight weeks later, the PDLSCs group demonstrated incremental (reversal) lines of neo-cementum, with PDL fibers inserted. 269 Autologous 9–15 × 104 alveolar periosteum-derived stromal cells, PDLSCs, or BMSCs cell sheets constructed using PGA were transplanted into one-wall infrabony defects (5 × 5 mm in depth, mesiodistal width) with β-TCP in dogs. Eight weeks later, histologically periodontal regeneration with new bone, new cementum, and connective tissue fibers inserted vertically were evident in the Class-II furcation defects. 270 Autologous 3 × 105 PDLSCs on collagen sponges were transplanted into Class-II 271 or Class-III 272 furcation defects of dogs. Histological evaluation revealed periodontal regeneration with greater new cementum, PDL fibers, and less connective tissue and epithelium along the root surface in the cell transplantation groups. PRP (1.8–2.4 × 106 platelets/μL) mixed with 1 × 107 BMSCs/mL and autogenous cortical bone were transplanted into inflamed Class-II furcation defects (5 mm in height × 2 mm in depth) of dogs (inflammation induced via impression material insertion). Eight weeks later, regeneration of cementum in the cell transplantation group was significantly higher than in the noncell transplantation group, with no difference between transplantation and noncell transplantation groups observed for bone formation. No root resorption or ankylosis was present. 273 Overall, 1.5 × 107 cells/mL autologous adipose tissue-derived stem cells mixed with PRP were transplanted into 5 mm-deep Class-III furcation defects of dogs. After 2 months, new bone and PDL was regenerated with osteocalcin-positive cells found on the dentin surface. 274 In a further study, G-MSCs sheets were transplanted into Class-III furcation defects of beagle dogs (surgically created defects, 5 mm from the furcation fornix to the bottom of the defect followed by placement of cotton ball saturated with anaerobic bacteria for 2 weeks) on 17% EDTA root-conditioned root surfaces. Eight weeks later, histological evaluation revealed significantly enhanced regeneration of the damaged periodontal tissue, including the alveolar bone, cementum, and functional PDL. 275 In a later investigation, 2 × 107 autologous DPSCs on anorganic bovine bone matrix were transplanted into surgically created three-wall osseous defects (3 × 5 × 7 mm, chronicity induced with ligature) in beagle dogs. Eight weeks after surgery, significantly higher periodontal regeneration with new cementum, bone, and PDL was observed in the defects. 276 Overall, 2 × 107 autologous BMSCs loaded on anorganic bovine bone mineral were transplanted into bilateral acute and chronic infrabony periodontal defects (4 × 4 mm, chronicity induced by ligature for 5 weeks). Eight weeks after transplantation, histological evaluation revealed periodontal regeneration with significantly higher cementum and PDL formation. 277
Recently, the first gene therapy approaches in the field of periodontal tissue engineering were tested in the dog model. Overall, 1 × 106 OPG-modified autologous bone marrow stromal cells (BMSCsOPG; transduced via Lipofectamine 2000) on PLGA were transplanted into surgically created window defects (4 × 4 × 3 mm) on the buccal root aspect of beagle dogs. Six weeks postsurgery, histological evaluation demonstrated significantly greater alveolar bone, cementum, and connective tissue formation. 278 In a second investigation, mesoporous bioglass/silk fibrin scaffold combined with BMP-7 (OP-1) and/or PDGF-B adenovirus transfection were transplanted into acute-type buccal dehiscence periodontal defects (mesiodistal width × depth: 5 × 5 mm). Eight weeks later, histological evaluation revealed that the combined application of the two adenoviruses yielded two times higher periodontal tissue regeneration, with new bone, cementum, and PDL. 279
Apart from major differences in oral occlusal function, lacking lateral movements of the jaws as well as occlusal contacts at the premolar level, the absence of lateral contacts between their teeth, and the different compositions for periodontal plaque and calculus compared with humans, dogs represent affordable and extensively studied animal models in the field of periodontal disease and tissue regeneration. The eminent earlier periodontal studies conducted in the dog model provided pivotal insights into the potential and limitations of various proposed regenerative methods, and they resulted in the first testing of the compartmentalization concept and the establishment of the GTR technique. The periodontal regenerative investigations employing this animal model were subsequently further expanded to involve the established GTR technique in combination with a diversity of bone substitutes, growth/differentiation factors, biomolecules, root-surface bio-modifying agents, cellular transplantation, scaffold materials, and gene therapy for achieving the ideal periodontal tissue-engineering formula. The studies were extensive, and the results provided pivotal new insights. Compared with nonhuman primates, dogs as animal models remain linked to less ethical concerns, are easier to manage and their obtainability and size are practical. However, animal care regulations, including daily companionship, exercise, space, and maintenance, have evolved over the past years to make dogs' use increasingly less desirable and unsuitable in today's periodontal disease and tissue regeneration studies. 91 This, in turn, necessitated the search for further suitable large experimental animal model options.
Miniature pigs
More than 60 years ago, the first Minnesota miniature-pig breed was introduced in the field of medical research. 280 From then onward, miniature pigs continued to represent virtuous models for studying treatment modalities for human diseases,281,282 with a dental formula I3/3, C1/1, Pm4/4, and M3/3. 283 The anatomy, development, disease incidence, and pathophysiology in the oral-maxillofacial region284,285 as well as the morphology of their teeth and the anatomical structure of their periodontal tissues 281 are analogous to humans. Their gingival sulci depth range between 2 and 3 mm, with a long junctional epithelium formation 98 and naturally occurring gingival recession. 286 Spontaneous gingivitis in miniature pigs occurs from 6 months and periodontitis occurs from 16 months of age onward, demonstrating pocket depth up to 5 mm, inflammatory changes comparable to human periodontal disorders, with periodontal tissue loss and bleeding on probing. 82 Finally, their PDL, similar to the human one, harbors cells with pluripotent properties. 287
Various techniques have been employed to induce experimental periodontal disease in miniature pigs, manifesting clinical signs and symptoms similar to human periodontitis. Numerous models were employed to promote experimental periodontitis, including the surgical creation of bony defects 262 and its chronic-inflammatory response induction by a 4 to 8 week introduction of plaque retentive orthodontic elastics 54 or suture ligatures 82 or through periodontal pathogens' introduction of A. actinomycetemcomitans, P. gingivalis, and Streptococcus mutans.281,288 When ligatures and human periodontal pathogens were introduced, periodontitis with all its pathognomonic signs and symptoms developed in 4 weeks, increasing in severity for up to 8 weeks, with no further deterioration observed for up to 20 weeks. 281 Ligature removal did not result in spontaneous resolution of the periodontitis and the associated tissue destruction, analogous to the clinical situation seen in humans, underlying again the suitability of this model in periodontal disease research. Miniature pigs were further used to establish a mucogingival defect examination model, where facial gingiva was excised from the primary incisors, to establish recession by 3 months, comparable to humans.289,290
In light of periodontal regeneration via tissue-engineering approaches, multiple growth/differentiation factors have been tested in the miniature-pig model. The periodontal connective tissue regeneration effect of EMD was tested in a Yucatan miniature-pig model in combination with Ca(OH)2, gutta percha, and mineral trioxide aggregates, materials that in isolation do not support periodontal regeneration, using the GTR principles described in depth earlier. Defects were 3 mm in depth and 5 mm in width, with no chronicity induced. EMD application resulted in the formation of fibrous insertion into the cementum and alveolar bone, similar to the naturally occurring PDL observed in humans. 291 A study evaluating the effect of autologous PRP on the flap strength in the Yucatan miniature-pig model at 2, 7, 10, and 28 days postsurgically concluded that it had no effect. 292
Approaches for cell transplantation for periodontal regeneration in a tissue-engineering concept were set off by a study transplanting 8 × 106 ex vivo expanded first-passage cells isolated from the PDL or alveolar bone of miniature pigs into trough-shaped palatal bone defects with autologous roots. Histological results demonstrated that the transplanted cells formed tissue irrespective of their origin, where bone cells formed cellular cement-like tissues and PDL exhibited no calcified tissues, but formed well-oriented fiber bundles. 100 This was followed by a second investigation transplanting 2-8 × 106 ex vivo expanded first-passage primary cell cultures from the alveolar bone or the PDL into furcation and interdental experimental defects. At 90 days, significantly new cementum, alveolar bone, and the development of new attachment were observed histologically. 54 Dental MSCs, SCAP, and PDLSCs were transplanted on root-shaped HA/trichroloacetic acid (TCA) carriers resembling a lower incisor tooth into fresh extraction socket sites of miniature pigs. After 3 months, computed tomography and histologic analysis confirmed the regeneration of root/periodontal similar structure. 293 Further studies transplanted 2 × 107 PDLSCs on HA/TCP, 82 allogenic 2 × 106 PDLSCs as cell sheets, 294 Vitamin C pretreated PDLSCs cell sheets ± gelfoam scaffold, 295 Vitamin C pretreated allogeneic 1 × 106 SHED stem cell sheets on HA/TCP, 296 2 × 107 G-MSCs on deproteinized bovine bone allografts or Collagen scaffolds, 81 or 1 × 106 G-MSCs on IL-1ra releasing hyaluronic acid-based hydrogel, 80 1 × 107 human DPSCs (hDPSCs) in 0.6 mL of 0.9% NaCl injection or as cell sheets 297 in standardized 3 × 5 × 7 mm periodontal defects, with ligature-induced chronicity. After a 12-week follow-up period, all studies demonstrated that complete periodontal regeneration was achievable through these tissue-engineering approaches.
In a pioneering investigation, bioengineered tooth constructs, consisting of two components, corresponding to those of the naturally formed tooth—the enamel organ (EO) and the pulp organ (PO)—were designed ex vivo. Dental stem cells obtained from the pulp organ of porcine teeth buds were seeded on PGA/poly-l-lactic acid (PLLA) spherical scaffolds (PO), whereas cells of the enamel organ were cultured on gelfoam absorbable gelatin sponge strip scaffolds (EO). The EO construct was then carefully put on the PO organ to wrap it, the construct secured with 7-0 prolene sutures, creating a bioengineered tooth bud. After securing it to a thin film coat of silicone elastomer, covered with osteogenically induced bone marrow progenitor cells obtained from the iliac crest, the construct was transplanted back into surgically created mandibular defects in the same miniature pig. The constructs were revaluated radiographically, histologically, immunohistochemically, and through transmission electron microscopy at 12 and 20 weeks, demonstrating the formation of tissue-engineered organized structures of enamel, dentin, pulp, cementum, and PDL, surrounded by regenerated alveolar bone. 61
Recently, primary gene therapy approaches have been tested in the miniature-pig animal model to further explore the potential for periodontal regeneration via a tissue-engineering scope. Hepatocyte growth factor transfected 1 × 107 hDPSCs injection or 1 × 105 hDPSCs sheets were transplanted into 3 × 5 × 7 mm periodontal defects in Wuzhishan miniature pigs. Twelve weeks later, significant periodontal regeneration with PDL, new cementum, and alveolar bone was evident by both treatments. 298
Miniature-pig experimental results have provided great insight into various medical fields, 283 including periodontology. In light of the advantages described earlier and the many ethical and infection-transmission concerns linked to the use of nonhuman primates as well as the increasingly complex animal care regulations linked to the use of dogs as animal experimental models, miniature pigs evolved to provide a suitable alternative for a large animal model with human analogy in oral and periodontal structures. Their periodontal tissue-engineering investigations present a continuation of the process of knowledge generation that commenced with nonhuman primates and continued in dog experiments, giving a greater insight into various periodontal tissue-engineering treatment modalities, including GTR in combination with cellular transplantation, growth/differentiation factors, gene therapy, and bioengineered tooth constructs. Although miniature pigs remain relatively expensive, and could present husbandry issues, they are in light of all aforementioned developments currently being regarded as the mainstream animal models in periodontal tissue regeneration and engineering research.
Sheep
Sheep have been suggested as additional appropriate experimental large animal models for dental research. Their metabolic rate is similar to that of humans, with similarities in size, weight, and general physiology. 299 Their permanent dentition comprises 32 teeth, with a dental formula: I0/3, C0/1, Pm3/3, and M3/3. Their incisors show a very short root and physiological mobility. Periodontitis may affect these anterior teeth quite rapidly, and it is accompanied by deep periodontal pockets, plasma cell infiltrate, and severe bone loss. 300 Their premolars and molars are similar to humans with analogous periodontal structures and naturally occurring periodontitis. 301 Their subgingival plaque demonstrates the presence of human periodontitis-associated pathogens, including P. gingivalis, Bacteroides forsythus, Prevotella intermedia and F. nucleatum. 302 Experimental surgical models were developed, using the bifurcation region of the second mandibular premolar, with proportions similar to that of a small human mandibular molar, in addition to a zero-wall dehiscence defect model,303,304 for testing periodontal regenerative procedures. 305
Only limited initial studies are currently available on the sheep (ovine) model in the field of periodontal regeneration and tissue engineering. Periodontal regeneration of Class-II furcation defects in the second mandibular premolar sites was attempted in 22 teeth in 11 sheep by using nonresorbable GTR membranes. Seven weeks later, histological evaluation revealed periodontal regeneration with new cementum, epithelium, and connective tissue fill. 306 In 2006, the first ovine PDLSCs were isolated, characterized, 307 and later compared with ovine BMSCs and DPSCs. 308 Overall, 1 × 107 ovine allogenic PDLSCs on gelfoam were transplanted into zero-wall dehiscence defects in merino ewes. Histological evaluation at 4 weeks demonstrated significantly greater new cementum and alveolar bone formation, with osteoblast-like cell lining and organized PDL fibers. 303 In a further study, autologous 2 × 106 ovine PDLSCs on gelfoam were transplanted into surgically created acute 5 mm dehiscence defects of merino ewes, with cementum and PDL removal. All implants were clotted with fibrinogen and thrombin before implantation. Histological assessment 8 weeks later revealed PDL, cementum, and bone-like structure. 304
Although little periodontal regenerative investigations have been conducted on sheep, the initial results obtained from these studies suggest that this large animal model could provide a promising alternative in the field of periodontal tissue engineering with minimal ethical or husbandry issues.
Conclusion
Over the long history of medical research, experimental animal models considerably contributed to the generation of extensive knowledge in the field of physiology, disease progression, disease treatment modalities, and pharmacology,11,84–90 including the pathogenesis of periodontitis and periodontal tissue-regenerating and -engineering therapeutic modalities. 69 The knowledge obtained is priceless and incomparable to data obtained from even the most complexly strenuous in vitro studies.
However, although animal models have provided a large amount of exquisite data, it is sometimes difficult to determine whether the findings are directly transferable to humans. Animal models are sometimes unable to mimic some fundamental human features, including the spontaneous emergence of disease (even though some periodontal lesions can occur in aged animals, periodontal defects are mostly artificially induced), genetic background, and risk factors (aggressive bacterial microbiota, occlusal overload, tobacco, prosthesis, systemic factors modifying the host's disease, etc.).65,309–311 Although great human similarities can be observed, especially in large animal models, a simple and reproducible model, which truly mimics human pathogenesis of periodontal disease and its response to therapeutic modality in all its aspects, is hard to find.
However, in the light of all the copious investigations mentioned earlier conducted in the experimental animal models, the question arises as to whether or not additional animal experiments are still easily justifiable. The current knowledge status of periodontal regeneration via a tissue-engineering concept has since a long time surpassed the “proof-of principle” phase and clear evidence about the effectiveness of multiple materials, growth/differentiation factors, and cellular transplantation approaches isolated or in combination is present. Most newly planned and performed studies test new materials or cells in line with the same principle outlined earlier and generally demonstrate a successful periodontal regeneration through this tissue-engineering concept. In regards of this as well as in the presence of important ethical considerations, every newly planned experimental animal study should be weighed meticulously in the light of the importance of any possibly obtained experimental results, not only in the light of financial aspects. The sparing of animal lives should remain a clearly untouched priority.
This experimental animal study's results support the concept of stem/progenitor cell-based therapy in conjunction with suitable biocompatible scaffolds for periodontal tissue engineering, indicating innovative techniques that are superior to conventional periodontal clinical treatment modalities. However, multiple biological and technical challenges still need to be tackled before considering these periodontal tissue regeneration approaches a clinical reality in humans. The further optimization of techniques for cellular incorporation and propagation in apposite biocompatible scaffolds and their property advancement for apt clinical handling remain of great importance. Potential ex vivo cellular karyotypic instability with gene mutations in prolonged cell-expansion cultures is potentially hazardous in outcome. Currently, the diverse inductive/growth/differentiation factors and cellular processes involved in stem/progenitor cells' self-renewal and differentiation are not sufficiently elucidated. Most of the current explanation models emerge from in vitro cell culture and in vivo experimental animal models, which do not fully translate to human clinical settings. Finally, in view of existing knowledge gaps of periodontal development and its application to periodontal regenerative therapy, profounder comprehending of biological processes is required, before reliable biologically based tissue engineering therapies can be a clinical reality in the field of periodontal medicine.
Footnotes
Disclosure Statement
No competing financial interests exist.