
Abstract
The combination of biomatrices and induced pluripotent stem cell (iPSC) derivatives to aid repair and myocardial scar formation may soon become a reality for cardiac regenerative medicine. However, the tumor risk associated with residual undifferentiated cells remains an important safety concern of iPSC-based therapies. This concern is not satisfactorily addressed in xenotransplantation, which requires immune suppression of the transplanted animal. In this study, we assessed the safety of transplanting undifferentiated iPSCs in an allogeneic setting. Given that swine are commonly used as large animal models in cardiac medicine, we used porcine iPSCs (p-iPSCs) in conjunction with bioengineered constructs that support recovery after acute myocardial infarction. Histopathology analyses found no evidence of p-iPSCs or p-iPSC-derived cells within the host myocardium or biomatrices after 30 and 90 days of follow-up. Consistent with the disappearance of the implanted cells, we could not observe functional benefit of these treatments in terms of left ventricular ejection fraction, cardiac output, ventricular volumes, or necrosis. We therefore conclude that residual undifferentiated iPSCs should pose no safety concern when used on immune-competent recipients in an allogeneic setting, at least in the context of cardiac regenerative medicine.
Introduction
T
Porcine iPSCs (p-iPSCs) have also been generated,3–6 opening up a wide range of possibilities to conduct preclinical testing in swine, the animal model with the closest cardiovascular physiology to humans, and therefore the animal model of choice for research on regenerative cardiology. So far, iPSC safety as a future treatment has been addressed mainly in autologous, syngeneic, and xenogeneic settings. However, allogeneic transplantation would be of much greater interest due to its convenience to treat patients with iPSCs from distinct sources. In this regard, whether undifferentiated allogeneic p-iPSCs are safe and support cardiac function in engineered heart constructs are, as yet, unanswered. One of the main concerns for the application of iPSC technology is the possibility of uncontrolled tumorigenesis postdelivery, leading to teratoma formation. 7 Avoiding the use of immune-deficient pigs with allogeneic transplantation could discern if the immune system is able to keep in check undifferentiated cells that may remain after transplantation. Whether iPSCs interact with the immune system and cause rejection when transplanted is a topic that currently holds much discussion. However, very little evidence is available on any of the opposing positions, and explicit experimentation focusing on this issue should come as a prerequisite to elucidate it completely.
In the present work, three cell-supporting biomatrices were studied: the adipose graft transposition procedure (AGTP), 8 an acellular human pericardial scaffold (scaffold), and a combination of the two (AGTP-scaffold). The study design included the three-biomatrix test groups, either implanted with (p-iPSC-AGTP, p-iPSC-scaffold, and p-iPSC-AGTP-scaffold) or without (AGTP, scaffold, and AGTP-scaffold) p-iPSCs. Surgical constructs were then implanted following acute myocardial infarction (MI) in the immune-competent swine model. The main objective of the present study was to evaluate the safety and efficacy of three different bioengineered approaches delivering iPSCs in a swine model after MI.
Methods
Experimental design
Fifty-seven crossbred Landrace × Large White swine (28.5 ± 3.3 kg) were subjected to MI and randomly distributed into six groups (Fig. 1):
(i) p-iPSC-free + AGTP (n = 6) (AGTP) (ii) p-iPSC-free + acellular pericardial scaffold (n = 13) (scaffold) (iii) p-iPSC-free + acellular pericardial scaffold + AGTP (n = 7) (AGTP-scaffold) (iv) Green fluorescent protein (GFP)-p-iPSC-enriched + AGTP (n = 9) (GFP-p-iPSC-AGTP) (v) GFP-p-iPSC-enriched + acellular pericardial scaffold (n = 11) (GFP-p-iPSC-scaffold) (vi) GFP-p-iPSC-enriched + acellular pericardial scaffold + AGTP (n = 11) (GFP-p-iPSC-AGTP-scaffold)
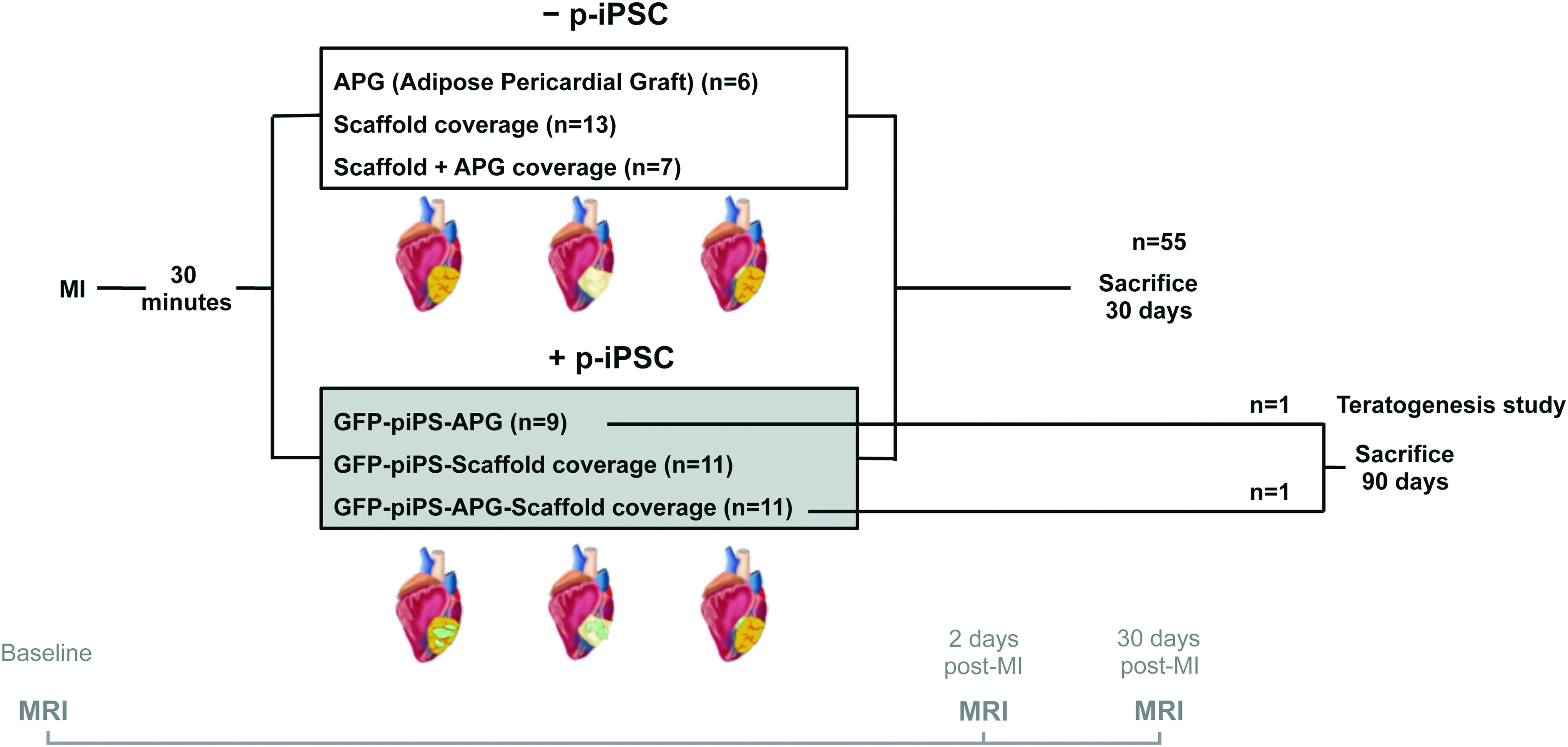
Study design. n, number of pigs; iPSC, induced pluripotent stem cell; MI, myocardial infarction; AGTP, adipose graft transposition procedure; GFP, green fluorescent protein; MRI, magnetic resonance imaging. Color images available online at
Animal studies were approved by the Jesús Usón Minimally Invasive Surgery Centre Animal Experimentation Unit Ethics Committee (Number: ES 100370001499) and complied with guidelines concerning the use of animals in research and teaching as defined by the Guide for the Care and Use of Laboratory Animals (NIH Publication No. 80-23, revised 1996). Human pericardial samples were obtained after written informed consent from patients undergoing cardiac surgery. The local ethics committee approved this study and our protocols conformed to the principles outlined in the Declaration of Helsinki.
Culture and expansion of p-iPSCs
The p-iPSCs used in the current studies were a kind donation from Dr. Nuria Montserrat and were generated from adult Landrace × Large White pig fibroblasts and characterized as previously reported. 6 p-iPSCs were expanded by manual dissection of colonies and cultured at 37°C, 5% CO2, in basal medium consisting of a 1:1 mixture of knockout-Dulbecco's Modified Eagle's Medium (DMEM) and high-glucose DMEM (both from Invitrogen), supplemented with 10% knockout serum replacement (Invitrogen), 10% fetal bovine serum (Invitrogen), 5 ng/mL recombinant human basic fibroblast growth factor (PeproTech), 500 U/mL leukemia inhibitory factor (Chemicon), 1 mM GlutaMAX (Invitrogen), 100 μM nonessential amino acid solution (Invitrogen), 100 μM 2-mercaptoethanol (Invitrogen), and 100 U/mL penicillin and 100 mg/mL streptomycin (Sigma). The plasmid encoding the four reprogramming factors, Oct4, Sox2, Klf4, and c-Myc, and GFP (pMXs-OSKMG) was then also used to transfect and label the p-iPSCs, as previously described. 6
p-iPSC delivery
p-iPSCs were suspended in 100 μL of 10% sucrose in distilled water. One hundred microliters of 0.3% RAD16-I (Corning) in 10% sucrose solution was then added to obtain a cell hydrogel mixture. The resultant cellular suspension was seeded (200 μL) on the surface of the scaffold and left for 20 min to embed into the scaffold. Then, 200 μL of culture medium was added to the recellularized scaffold to induce hydrogel gelation and then applied to the MI scar.
Biomatrix generation: the acellular pericardial scaffold and AGTP
The acellular pericardial scaffold was obtained from the pericardium of patients undergoing cardiac surgery. Pericardial decellularization, lyophilization, and sterilization were performed as previously described.9,10 Next, the scaffold was either rehydrated with 200 μL of hydrogel (for controls) or enriched with hydrogel +0.5–1 × 106 p-iPSCs.
AGTP was performed as previously reported. 8 Briefly, pericardial adipose tissue was identified and detached, taking care to preserve vascularization, to create an adipose flap to cover the MI scar. In p-iPSC-AGTP animals, 200 μL (100 μL of culture medium plus 100 μL of 10% sucrose) containing 0.5–1 × 106 cells was injected into the adipose graft.
MI model
After a left lateral thoracotomy, MI was induced by a double-ligation of the first marginal branch of the circumflex artery, 1.5 cm distally from the atrioventricular groove (Prolene 5/0W-8556 12-S; Ethicon). After 30 min, all animals (p-iPSC-free n = 26; and p-iPSC-enriched n = 31) received either the AGTP and/or pericardial scaffold, with or without p-iPSCs; these were placed over the infarcted myocardium and secured with 0.1–0.2 mL of surgical glue (Glubran2®; Cardiolink). Finally, animals were recovered and housed before sacrifice.
Magnetic resonance imaging
Cardiac magnetic resonance imaging (MRI) was performed at 1.5 T (Intera; Philips) in all animals using a four-channel, phased-array surface coil (SENSE Body Coil) as previously described. 8 Left ventricular ejection fraction (LVEF), cardiac output (CO), end-systolic volume (ESV), end-diastolic volume (EDV), and necrotic mass were measured at baseline, 2 days post-MI (to avoid acute-phase malignant arrhythmias and early edema), and before sacrifice. Two independent experimenters then performed blinded analyses of the MRI collected data.
Tissue collection and infarct morphometric analyses
Animals were euthanized at 34.9 ± 6 days after MI, using an overdose of anesthesia. Hearts were then harvested and the left ventricular infarct size was measured in sections obtained 1.5 cm distally to the arterial ligation. 8 Quantitative morphometric 8 and histological measurements were accomplished using the Image-Pro Plus software (6.2.1 version; MediaCybernetics, Rockville, MD). The MI area with the attached biomatrices and distal myocardium were either fixed in 10% formalin and paraffin embedded or snap-frozen.
Histological and immunohistochemical analyses
Using 4-μm paraffin-embedded slices, Movat's pentachrome and hematoxylin/eosin staining were used to analyze histological morphology and teratoma presence. Calponin (1:500; Dako) and caldesmon (1:60; Dako) antibodies and the ultraView Universal DAB Detection Kit (Ventana Medical Systems, Inc.) were used to detect myofibroblast infiltration of granulomatous scarring within the pericardial scaffold and AGTP. To quantify vessel area, 10-μm frozen sections (distal and infarcted myocardium with the adipose pericardial graft [APG], scaffold, and APG/scaffold zones) were stained using biotinylated GSLI B4 isolectin (1:50; Griffonia simplicifolia lectin I B4; Vector Labs), with Alexa Fluor 488-conjugated streptavidin (1:500; Molecular Probes). CD3 (1:100) and CD25 (1:10) (AbD Serotec, Kidlington, United Kingdom) antibodies were used to identify lymphocytes and any activated lymphocyte fraction, respectively, in the infarct zone and within the engineered construct. Briefly, frozen sections were 10% formalin-fixed and permeated with phosphate-buffered saline (PBS)-Triton. After horse serum (Sigma-Aldrich, Madrid, Spain) blockage for 1 h at room temperature, primary antibody incubation was carried out overnight at 4°C. Then, after PBS washing, Cy2, Cy3, and Cy5 secondary antibodies (1:500; Jackson ImmunoResearch, West Grove, PA) were incubated for 45 min at room temperature. Finally, nuclei were counterstained with 4′,6-diamino-2-phenylindole (1:10,000; Sigma-Aldrich). Images were captured under a laser confocal microscope (Axio Observer Z1; Zeiss, Madrid, Spain). Histological and immunohistochemical measurements were finally completed with Image-Pro Plus software.
Polymerase chain reaction analysis
To verify the long-term presence of GFP-p-iPSCs in heart and distal locations, two swine from the p-iPSC-AGTP and p-iPSC-AGTP-scaffold groups were euthanized at 90 days. 11 Samples from the heart, pericardial scaffold and/or APG, lung, mediastinal lymph node, liver, spleen, pancreas, and kidney were collected and stored frozen until further use. Genomic DNA was extracted from frozen tissue with a QIAamp DNA Mini Kit (Qiagen). Tissue was carefully cut in small pieces and homogenized by adding 100 μL of lysis buffer containing 20 μL of proteinase K enzyme. The sample was mixed by vortexing and incubated at 56°C for 2–3 h until the tissue was completely lysed. DNA was extracted following the manufacturer's instructions. DNA purity was measured with a spectrophotometer (NanoDrop® ND-100; Thermo Fisher Scientific) by calculating the ratio of absorbance at 260 nm to absorbance at 280 nm (A260/A280). Samples with an A260/A280 ratio of 1.7–1.9 were considered pure samples of DNA. GFP expression was analyzed by polymerase chain reaction (PCR) (GFP forward primer: 5′-AAGTTCATCTGCACCACCG-3′; GFP reverse primer: 5′-TCCTTGAAGAAGATGGTGCG-3′). Amplification conditions were as follows: 94°C for 5 min, followed by 25 cycles at 94°C for 30 s, 58°C for 30 s, and 72°C for 30 s, plus an extension phase at 72°C for 10 min. All samples were also amplified for GAPDH (GAPDH forward primer: 5′-ACCTGCCGCCTGGAGAAACC-3′; GAPDH reverse primer: 5′-GACCATGAGGTCCACCACCCTG-3′) as control for the presence of amplified DNA. Amplified products were finally detected in 1% agarose gel with SYBR Green staining.
Statistical analyses
Data are represented as mean ± standard error of the mean. Student's t-test, one-way analysis of variance (ANOVA) with Tukey's procedure for multiple comparisons, and the Mann–Whitney test for nonparametric data were performed using SPSS, version 19.0.1 (SPSS, Inc., Chicago, IL). MRI data were analyzed as replicates using ANOVA, with the Greenhouse–Geisser correction. Values of p < 0.05 were considered significant.
Results
Histopathology and PCR analysis
Histopathological examination of the heart, pericardial scaffold, and APG, ruled out at 30 days of follow-up, confirmed the absence of teratoma formation (Fig. 2).

Histological and teratogenic analyses.
Hemosiderin deposits (Fig. 2A), inflammatory cells (Fig. 2A), and abundant myofibroblasts (calponin+ caldesmon−) (Fig. 3A), still present in p-iPSC-AGTP-scaffold animals after 90 days of follow-up (Fig. 3A), were identified in all constructs enriched with p-iPSCs (Fig. 3A). CD3- and CD3/CD25-positive lymphocytes were counted in four fields from two different infarct sections per animal. Despite the CD3-CD25/CD3 ratio being significantly lower in p-iPSC-scaffold animals (p = 0.006), there were more CD3 (p = 0.005) and CD3–CD25 (p = 0.002)-positive lymphocytes in the infarct zone of iPSC-AGTP-scaffold animals (Fig. 3B–D).

Healing and inflammation in engineered constructs.
Infarct size was similar for all treatment groups, irrespective of p-iPSC codelivery (Fig. 4A, B). The arm that combined scaffold with AGTP, used on the presumption of a beneficial additive effect, showed the opposite, with a trend toward larger infarct size than the scaffold group (6.2 ± 1.4% vs. 2.9 ± 0.8%, respectively; p = 0.09; Fig. 4B). Positive GSLI B4 isolectin area was measured from four different fields in infarct and border zones from one to two infarct sections per animal. The AGTP-scaffold arm also showed significantly higher vascularization, irrespective of p-iPSC delivery, compared with the other treatment groups both in infarct (p = 0.018) and border (p < 0.001) zones (Fig. 5).

Morphometric analyses.
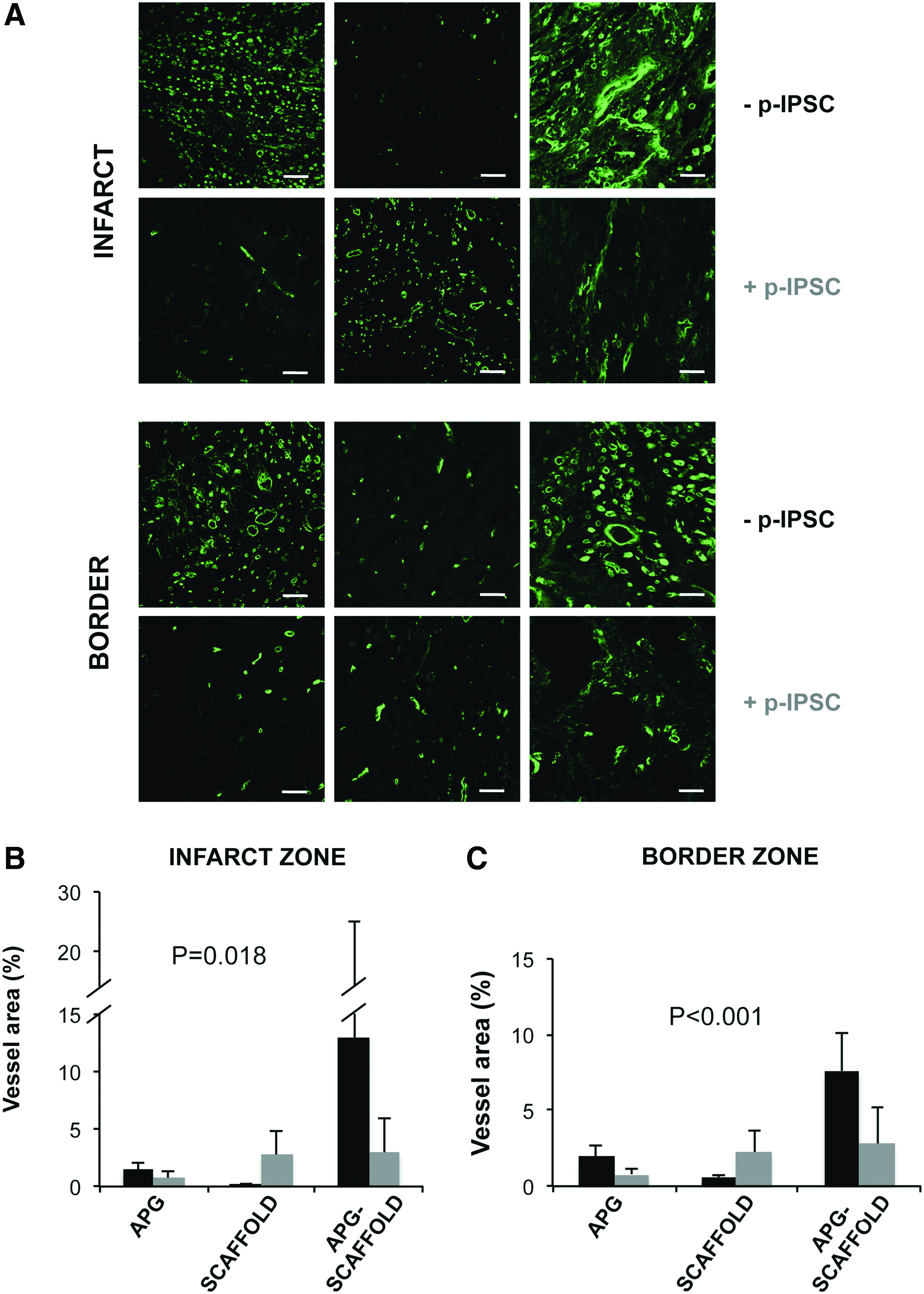
Myocardial vascularization and neovascularization in scaffolds.
Upon sacrifice, no p-iPSCs were found in the p-iPSC-enriched constructs, neither at the infarct zone nor within the border and remote locations. No trace of GFP was also detectable in the heart, lung, lymph node, liver, spleen, pancreas, or kidney after 30 and 90 days of follow-up, as shown by PCR analysis (Supplementary Fig. S1; Supplementary Data are available online at
Cardiac function
Baseline cardiac function assessed by LVEF, CO, ESV, and EDV did not differ between the studied groups (all p values >0.05, not shown). Our analyses of parameters for cardiac function over time (sacrifice vs. baseline) using ANOVA with Greenhouse–Geisser post hoc correction showed no differences in LVEF, CO, volumes, or necrotic mass, as assessed by late gadolinium enhancement between groups (Table 1).
p-iPSCs, porcine induced pluripotent stem cells; AGTP, adipose graft transposition procedure; LVEF, left ventricular ejection fraction; CO, cardiac output; EDV, end-diastolic volume; ESV, end-systolic volume.
Discussion
In this study, we examined the safety of transplanting allogeneic p-iPSCs using three different engineered constructs implanted into immune-competent swine. The main findings of the study included the absence of teratomas after 30 and 90 days of follow-up, no remaining p-iPSCs at least after immunohistochemistry or PCR analyses, and the absence of cardiac function improvement associated with the inclusion of p-iPSCs in the three bioengineered constructs tested.
Before iPSC-based treatments can be fully established as a treatment, many concerns about their safety have to be covered. Several studies have approached different settings regarding iPSC post-transplantation safety, but it is rarely their main goal. This inconsistency has led to a lack of reliable information that needs to be put to test. 7 Previous studies in immune-deficient hosts had confirmed the propensity of iPSCs to generate teratomas. Invasion is clearly a desirable feature for a regenerative cell that would necessitate low immunogenicity; at the same time, invasion would be of concern if those transplanted cells underwent tumorigenic changes. Therefore, we studied the safety and efficacy of p-iPSCs using immune-competent hosts. In immune-competent mice, iPSCs have been shown to support cardiac function, following their differentiation into cardiomyocytes, vascular smooth muscle cells, and endothelial cells.12,13 These studies used iPSCs derived from adult murine fibroblasts 12 and the embryonic ventricle 13 with low numbers of transplanted cells (2.5 × 104 and 2 × 105 cells; respectively) following experimental MI induction. In contrast, the transplantation of iPSCs generated from adult vascular smooth muscle generated teratomas, irrespective of cell dose, in immune-competent rats. 14 In immune-competent horses, when allogeneic iPSCs were dermally delivered, there was no rejection of implanted cells despite local inflammation. 15 In swine, previous studies have shown tumor-like formation after p-iPSC intramyocardial delivery in an MI immune-competent model despite the cells inside these tumors showing a homogeneous phenotype with no signs of differentiation into any cell lineages. 11 However, others did not detect teratomas at short- and long-term follow-ups after p-iPSC delivery in immunosuppressed pigs. 16 Taken together, the presented results suggest no evidence of teratoma formation following transplantation of allogeneic p-iPSCs in an immune-competent porcine model. However, further studies are needed to validate this relevant issue.
For the swine model, most studies have involved human iPSC transplantation into animals with experimentally induced MI that have also been immunosuppressed by the administration of cyclosporine A, glucocorticoids, tacrolimus, or combinations thereof.17–19 While being a sound proof-of-concept studied for iPSC integration and therapeutic effect, the species mismatch needs persistent immunosuppression, which lessens the authenticity of the model, and clinical value of these data. Herein, we have tested the safety and efficacy of allogeneic p-iPSCs in immune-competent swine, the preferred model for cardiovascular preclinical testing. Of note, after 90 days of follow-up, p-iPSC delivery was safe since we could not find macroscopical evidence of teratoma formation at the implant site or in the peripheral tissues tested. After 30 days of follow-up, we verified the absence of teratomas in both the heart and biomatrices by histological analysis. Remarkably, upon sacrifice, GFP+ p-iPSCs could neither be identified in the scaffold nor the myocardium; GFP protein expression was also absent in the lungs, mediastinal lymph node, liver, spleen, kidneys, and pancreas. Despite the low immunogenic response elicited by immature iPSCs, our data suggest that in swine, the p-iPSCs delivered through AGTP or the scaffold covered by APG were totally absent, suggesting that adipose vascularized tissue may react against allogeneic p-iPSCs. In line with these findings, Mizukami et al. have recently shown that administration of major histocompatibilty complex (MHC)-matched iPSCs can attenuate cellular and humoral immune responses, but remain susceptible to innate immunity in pigs. 20 Thus, the main observation of our study was that allogeneic p-iPSCs, administered at low dose (106 cells in each animal) in immune-competent swine, were not responsible for any benefits in host animals. Thus, there was no enhanced cardiac function after MI and improvements detected in terms of infarct size were irrespective of the use of p-iPSCs. However, iPSCs were not deleterious for cardiac function after MI. In light of these results, despite iPSCs being safe, but not effective in restoring cardiac function, it may be preferable to assess the effectiveness of alternative approaches (i.e., based on iPSC-derived cardiomyocytes) in human therapeutics.
In this study, we focused on the AGTP and the acellular pericardial scaffold. We had already developed the AGTP and demonstrated its use in salvaging ischemic myocardium, both in the acute and chronic MI settings, in swine.8,21 We also recently identified positive effects on infarct size reduction and cardiac function following implantation of an acellular pericardial scaffold in swine.10,22 By combining the two constructs, we were trying to achieve a synergistic effect that could boost the therapeutic treatment. Unfortunately, the results of our current studies do not support this hypothesis. Instead, infarct size was slightly greater in the AGTP-scaffold arm.
Conclusions
Allogeneic p-iPSC delivery in the context of three different engineered constructs was found to be safe. No surviving p-iPSCs could be identified upon sacrifice at 90 days in either condition. In light of these results, undifferentiated iPSCs should pose no safety concern when used on immune-competent recipients in an allogeneic setting, at least in the context of cardiac regenerative medicine. Further studies using fully reprogrammed p-iPSCs with robust differentiation ability will be necessary to assess the efficacy of allogeneic p-iPSC-derived cell therapy in swine so that we can harness the potential of iPSC technology to restore and regenerate damaged tissue.
Study limitations
Two Landrace × Large White prepubertal pigs were used for the teratogenesis study. Further studies (including more animals) to track teratoma formation and growth after iPSC delivery are needed.
Sources of Funding
This work was partially supported by grants from the Ministerio de Economía y Competitividad-MINECO (SAF2014-59892 and SAF2015-69706-R), (FIS PI14/01682), Red de Terapia Celular-TerCel RD16/0011/0024 and RD16/0011/0006, and the CIBER Cardiovascular (CB16/11/00403) projects, as part of the Plan Nacional de I+D+I, and it was cofunded by ISCIII-Sudirección General de Evaluación y el Fondo Europeo de Desarrollo Regional (FEDER). This work was also funded by “la Caixa” Banking Foundation, Generalitat de Catalunya-AGAUR (2014-SGR-1460 and 2014-SGR-699), Fundació La Marató de TV3 (201502, 201516, and 201534), and CERCA Programme/Generalitat de Catalunya. This work has been developed in the context of AdvanceCat with the support of ACCIÓ (Catalonia Trade and Investment; Generalitat de Catalunya) under the Catalonian ERDF operational program (European Regional Development Fund) 2014–2020.
Footnotes
Acknowledgments
The authors would like to thank Lola Mulero and Maite Fernanadez-Figueras for their technical assistance in histological and immunohistochemical analyses and Dr. Nuria Montserrat for the kind gift of p-iPSCs.
Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.