
Abstract
Periprosthetic osteolysis and subsequent aseptic loosening of total joint replacements are driven by byproducts of wear released from the implant. Wear particles cause macrophage-mediated inflammation that culminates with periprosthetic bone loss. Most current animal models of particle-induced osteolysis are based on the acute inflammatory reaction induced by wear debris, which is distinct from the slowly progressive clinical scenario. To address this limitation, we previously developed a murine model of periprosthetic osteolysis that is based on slow continuous delivery of wear particles into the murine distal femur over a period of 4 weeks. The particle delivery was accomplished by using subcutaneously implanted osmotic pumps and tubing, and a hollow titanium rod press-fit into the distal femur. In this study, we report a modification of our prior model in which particle delivery is extended to 8 weeks to better mimic the progressive development of periprosthetic osteolysis and allow the assessment of interventions in a setting where the chronic particle-induced osteolysis is already present at the initiation of the treatment. Compared to 4-week samples, extending the particle delivery to 8 weeks significantly exacerbated the local bone loss observed with μCT and the amount of both peri-implant F4/80+ macrophages and tartrate-resistant acid phosphatase-positive osteoclasts detected with immunohistochemical and histochemical staining. Furthermore, systemic recruitment of reporter macrophages to peri-implant tissues observed with bioluminescence imaging continued even at the later stages of particle-induced inflammation. This modified model system could provide new insights into the mechanisms of chronic inflammatory bone loss and be particularly useful in assessing the efficacy of treatments in a setting that resembles the clinical scenario of developing periprosthetic osteolysis more closely than currently existing model systems.
Introduction
P
In the periprosthetic tissue, wear debris is recognized and phagocytosed by macrophages that become activated into an inflammatory phenotype secreting proinflammatory cytokines and chemokines.2,3 The chemokines sustain macrophage recruitment to the periprosthetic tissue, while the proinflammatory cytokines exacerbate the condition by stimulating osteoclast formation and suppressing osteoblast function. Ultimately, this macrophage-mediated inflammation leads to net bone loss in periprosthetic tissues, resulting in implant loosening.2–4 This process progresses slowly with the continued wear of the implant components and typically takes years to develop. 1
Several animal models have been developed to elucidate and recapitulate this sequence of events.5–8 Most of these are based on implantation or injection of biomaterial wear debris into tissues that causes an acute inflammatory reaction and subsequent bone loss. For example, in one of the most popular models of aseptic loosening, wear particles are implanted directly on the surface of the murine calvarium resulting in rapid macrophage-mediated inflammation and bone resorption.5,9,10 This model of wear particle-induced osteolysis is fast, simple, and has been used to elucidate mechanisms of wear particle-induced bone loss and in the evaluation of novel treatment approaches.5,11,12
However, the calvarial model and other similar model systems do not fully recapitulate the microenvironment prevailing in the periprosthetic tissue. For example, the type and developmental origin of bone are different (flat calvarial bone of intramembranous origin vs. long bones of endochondral origin) and the models lack an intramedullary implant. Importantly these models do not capture the chronic nature of periprosthetic bone loss. In the calvarial model, bone loss peaks 7 days after particle implantation and is largely healed at day 14 postimplantation. 10 This dynamic of rapid bone loss followed promptly by bone formation probably does not entirely reflect the clinical scenario of slowly advancing implant wear and subsequent periprosthetic osteolysis.
To address the limitations of prior model systems, we previously developed a murine model of aseptic loosening that is based on slow continuous delivery of wear particles into the mouse distal femur.13–15 This was achieved by utilizing a small osmotic pump that was filled with particle solution. The subcutaneously implanted pump and tubing were then connected to a hollow titanium rod that was press-fit into mouse distal femur. Over the course of 4 weeks, the contents of the pump were slowly released into the distal femur resulting in local bone loss and systemic recruitment of macrophages to the area of continued low-grade inflammation.
In this study, we report a further development of our model system with the goal of modeling the progressive nature of wear particle-induced osteolysis and to allow the assessment of interventions in a setting where the chronic particle-induced osteolysis is already present at the initiation of treatment. To this end, we replaced the subcutaneous pump after 4 weeks of in vivo service through a simple operation and continued the particle delivery for an additional 4 weeks. We found that after 4 weeks of particle delivery, a local osteolytic reaction with an increased amount of peri-implant macrophages and osteoclasts had developed. Extending the period of particle delivery to 8 weeks, and thus increasing the overall particle load at the periprosthetic tissues, significantly exacerbated local bone loss and further increased the number of both periprosthetic macrophages and osteoclasts.
This modified model system with progressive inflammation and osteolysis might provide new insights into the molecular mechanisms of chronic inflammatory bone loss. In particular, the model system allows the assessment of treatment interventions in a setting that resembles the clinical scenario of developing periprosthetic osteolysis more closely than currently existing model systems.
Methods
Particles and pumps
Conventional UHMWPE particles were a generous gift from Dr. Timothy Wright, Hospital for Special Surgery. Particles were generated in knee joint simulators as described in detail by Cottrell et al. 16 and isolated from test supernatants following established protocols.14,15 After isolation, particles were washed twice in ethanol (96% and 70%). Ethanol was evaporated, particles suspended in PBS, and stored at −80°C. The Limulus Amebocyte Lysate Kit (BioWhittaker, Walkersville, MD) was used to confirm the absence of endotoxin contamination. Electron microscopy was used to determine the shape and diameter of the particles (Fig. 1): the majority of particles were globular spheroids with a mean diameter of 0.48 ± 0.10 μm (range 0.26–0.81 μm).
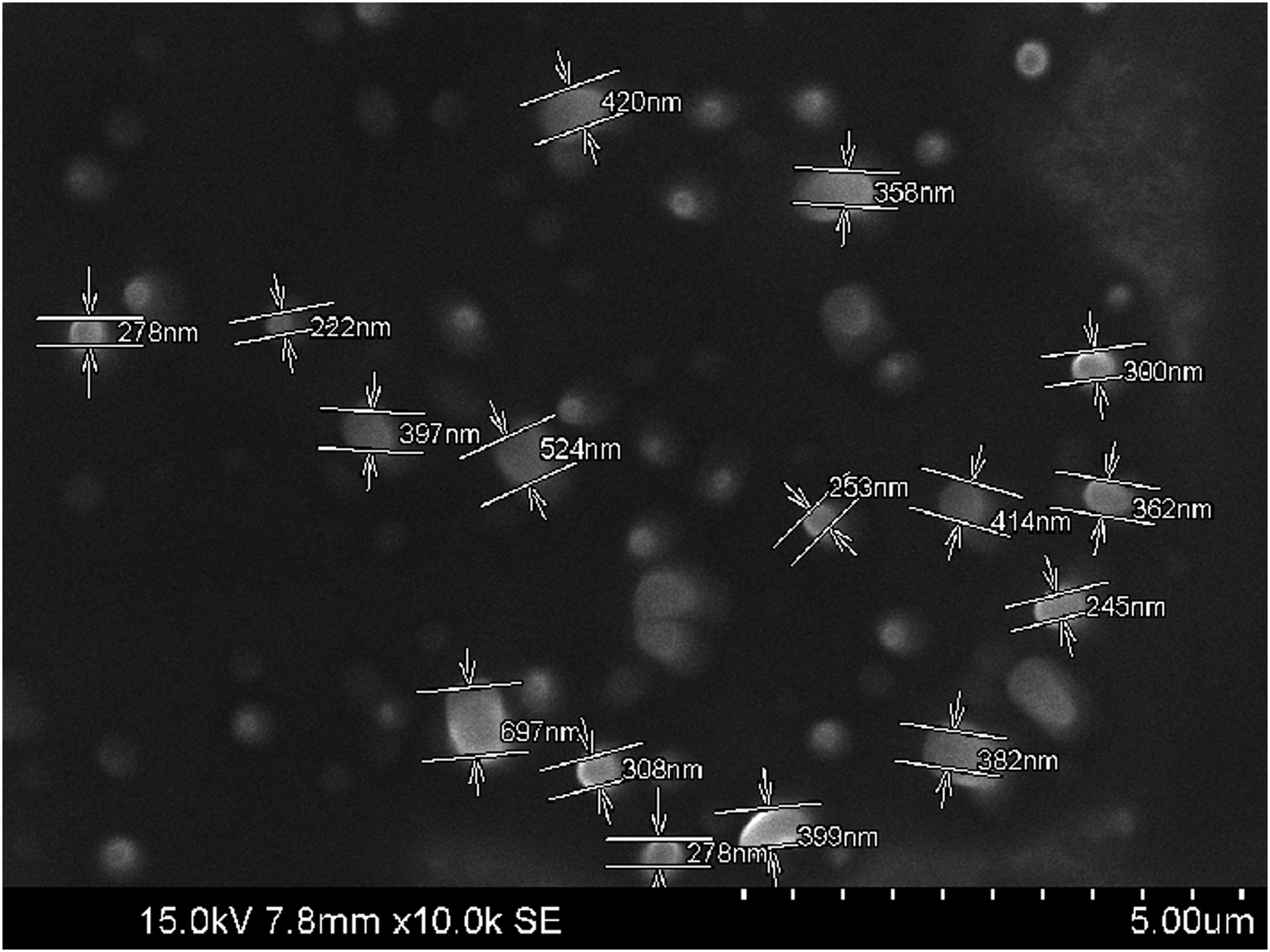
The UHMWPE particles. Scanning electron microscopy image of the UHMWPE particles used in the study. Notice the submicron size and globular shape. UHMWPE, ultra-high molecular weight polyethylene.
Alzet model 2006 osmotic pumps (Durect Corporation, Cupertino, CA) were loaded either with carrier solution (1% bovine serum albumin–phosphate-buffered saline [BSA-PBS]) or carrier solution with 15 mg/mL UHMWPE particles. Six centimeter long vinyl tubing (Durect Corporation) was prefilled with the appropriate solution and used to connect the pumps to the hollow titanium rods.
Mouse model
The murine intramedullary particle infusion model was created following our previously established protocols (Fig. 2a)13–15 Briefly, 60, 10- to 12-week-old male BALB/cByJ mice (The Jackson Laboratory, Bar Harbor, ME) were placed under isoflurane inhalation anesthesia and the right distal femur exposed by performing a lateral parapatellar arthrotomy. A series of hypodermic needles was used to create an axial drill-hole through the intercondylar notch into the medullary cavity. The hollow titanium rod was subsequently press-fit into the distal femur.
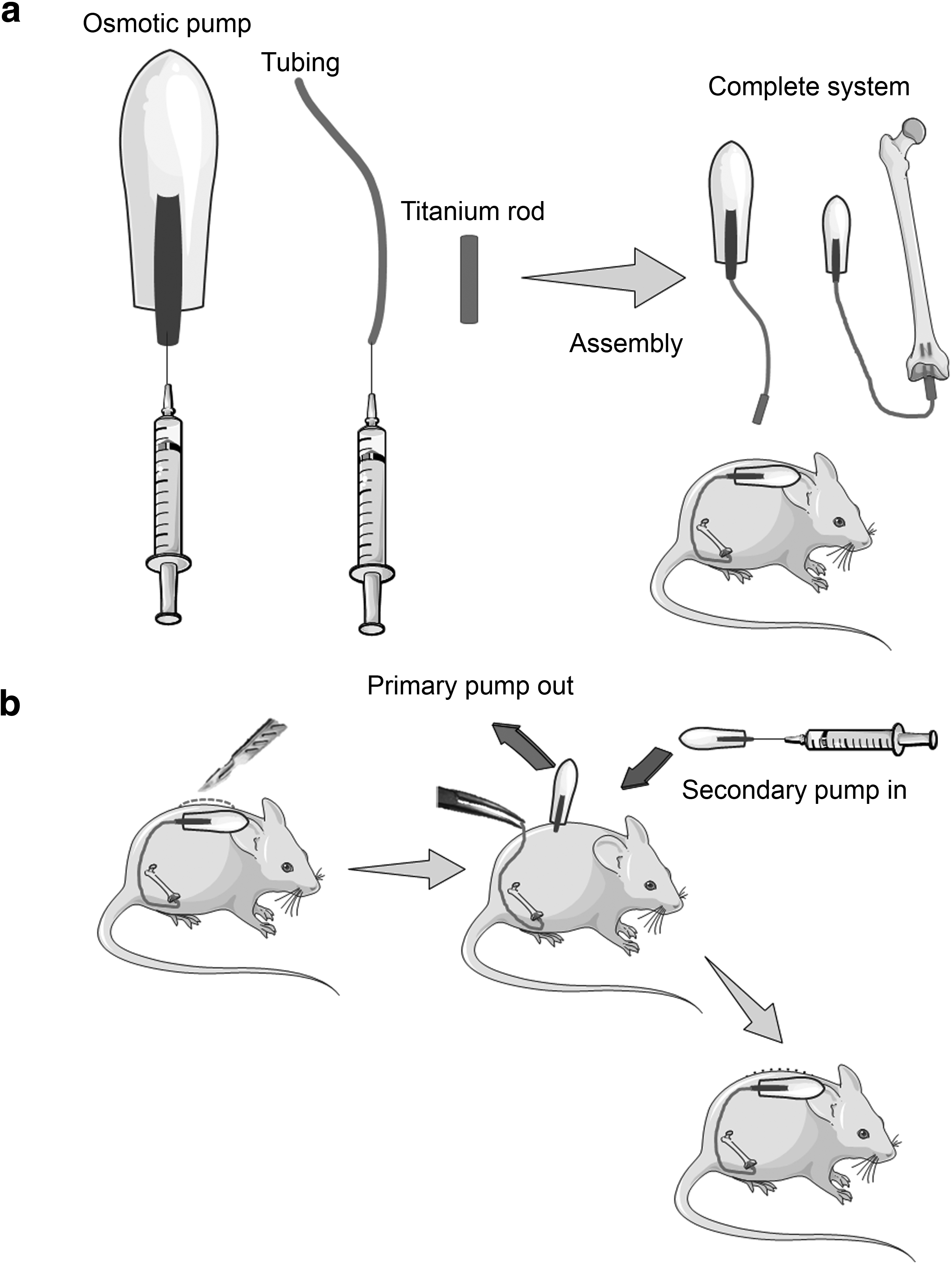
The model system. To model continued wear of total joint replacement components, polyethylene wear particles are continuously delivered to the mouse distal femur using an osmotic pump, tubing, and a hollow titanium rod.
Osmotic pumps with UHMWPE particles (n = 36) or carrier solution (n = 24) were then implanted in the subcutaneous tissue on the left dorsal side of the mouse and a subcutaneous tunnel reaching the right knee was created to connect the tubing to the implanted rods. Skin incisions were closed with 5-0 Ethicon sutures and subcutaneous buprenorphine injections (0.1 mg/kg, twice a day for 3 days postoperatively) were given for postoperative analgesia. In strict adherence to the institutional guidelines, the postoperative recovery of the mice was comprehensively evaluated daily during the first postoperative week and then every 2–3 days for the rest of the experiment. The weight of the mice was recorded at the beginning, middle, and end of the experiment. Mice were individually housed at Stanford University animal housing facilities in a temperature-controlled environment on a 12-h light–12-h dark cycle. Food and water were provided ad libitum.
After 4 weeks, a subgroup of mice were euthanized with CO2 inhalation followed by cervical dislocation, while another subgroup of mice underwent a minor operation to replace the pump and the experiment continued for another 4 weeks (Fig. 2b) The study was carried out in strict accordance with the recommendations in the Guide for the Care and Use of Laboratory Animals of the National Institutes of Health. The protocol was approved by the Administrative Panel on Laboratory Animal Care (APLAC) at Stanford University.
Green fluorescent protein and luciferase expressing reporter macrophages
Green fluorescent protein (GFP) and luciferase (FLUC) expressing mouse primary reporter macrophages were produced using lentivirus transduction as previously described in detail. 17 Briefly, human immunodeficiency virus-1 based vesicular stomatitis virus-G (VSV-G) pseudotype lentivirus particles were generated by cotransfecting the pFU-Luc2-eGFP lentivirus vector, psPAX2 packaging vector, and pMD2G VSV-G envelope vector into 293T cells using calcium phosphate transfection kit (Clontech, Mountain View, CA) with 25 μM chloroquine.
Mouse bone marrow macrophages (mBMMs) derived from 8- to 10-week-old male BALB/cByJ mice were isolated and cultured following established protocols. 17 mBMMs were transduced by exposing them to the lentivirus vector (MOI = 10) with 10 μM cyclosporine (Sigma-Aldrich, St. Louis, MO) twice for 24 h. Successful gene transfer with typical efficacy of ∼50% was confirmed by fluorescence microscopy, flow cytometry, and a Luciferase Assay System kit (Promega, Madison, WI) with a Turner BioSystems Luminometer TD-20/20 (Promega).
Bioluminescence imaging
Five weeks after the beginning of the particle infusion, 6 × 106 reporter macrophages suspended in 150 μL of HBSS were injected into the tail vein of a subgroup of mice (n = 12). The trafficking of the reporter cells was observed by obtaining prone bioluminescence images immediately after the injection of the cells into systemic circulation and then at 2-day intervals up to 20 days postinjection using In vivo imaging system (IVIS) 100 (Xenogen, Alameda, CA). Ten minutes before imaging, mice received 3 μg intraperitoneal injection of D-luciferin (Biosynth, Staad, Switzerland). The bioluminescence (BLI) images were quantified by measuring the total flux (photons/s) from uniformly sized regions of interest drawn over the right and left distal femur using Living Image (V 4.1. Perking Elmer, Waltham, MA) image analysis software.
μCT imaging
At 4 or 8 weeks after the initial surgery, femurs were collected, titanium rods removed, and femurs imaged with an eXplore Locus RS150 MicroCT (GE Healthcare, Fairfield, CT). The 49 μmm scans were performed with 70 kVp, two frames per view, 360° rotation, and 2 × 2 binning. A 3 × 2.5 × 3 mm volume of interest focusing on the metaphyseal region was defined to the distal femur using the epiphyseal plate as an anatomical landmark and the tissue mineral content (TMC) and bone volume fraction (BVF) determined.
Histological analyses
Immediately after μCT imaging, the right femurs of four representative mice per group were dissected free of soft tissues, fixed in 4% paraformaldehyde for 1 day, decalcified in 0.5 M ethylenediaminetetraacetic acid (EDTA)-PBS for 2 weeks (with EDTA-PBS changed twice a week), and then embedded in OCT compound. The distal metaphyseal region of the right femur representing the area of biomaterial inflammation was sectioned into 8-μm-thick frozen sections in the transverse plane. The sections were imaged (Axio Observer 3.1; Zeiss, Oberkochen, Germany) and the amount of peri-implant trabecular bone was quantified from H&E-stained tissue sections using ImageJ (National Institute of Health).
The amount of peri-implant macrophages was determined using F4/80 immunostaining. First, the tissue sections were fixed in ice-cold acetone for 10 min, followed by washing in PBS and blocking with 1% BSA-PBS for 1 h in room temperature. Monoclonal rat anti-mouse F4/80 AlexaFluor 647 conjugated antibody (BioRad, Hercules, CA) or corresponding isotype control (BD Biosciences, San Jose, CA) was diluted 1:25 (F4/80 antibody) or 1:100 (isotype control) to reach final concentration of 2 μg/mL in 1% BSA-PBS and applied to tissue sections overnight at +4°C. Sections were washed thrice in PBS, mounted with ProLong Gold with DAPI (Life Technologies), and imaged with Axio Observer 3.1. Total area of F4/80 positive cells was quantified using ImageJ and normalized to the total area of cells in the image.
Tartrate-resistant acid phosphatase (TRAP) histochemical staining kit (Sigma- Aldrich) was used to detect osteoclasts. Osteoclasts were defined as multinucleated TRAP-positive cells located within resorption lacunae either in endosteal or trabecular bone surfaces and their total number per section was counted manually.
Statistical analysis
Statistical analyses were conducted using GraphPad Prism version 6.03 (GraphPad Software, La Jolla, CA). Student's t-test was used for the statistical comparison and p < 0.05 was chosen as the threshold for significance. Values are presented as mean ± standard error of mean.
Results
The pump change surgery did not cause complications
The postoperative period after the primary pump implantation was generally uneventful with mice showing good recovery. During the experimental period, the mice gained 10–15% weight, with none of the mice losing weight. Changing the pump at 4 weeks after original implantation was a straightforward procedure. To avoid placing the pump directly underneath the wound, the skin incision was made to the right side of the back and a short subcutaneous tunnel was used to reach the pump located on the left dorsum/flank. A thin foreign body membrane surrounding the pump was removed.
After disconnecting the primary pump, it was critical to secure the proximal end of tubing with hemostatic forceps to avoid losing the tubing in subcutaneous tissues (Fig. 2b). Before connecting the tubing to the secondary pump, a 2 mm segment of the proximal tubing was cut to refresh the connection. No postoperative complications related to pump change were observed. The residual volume of all of the primary and secondary pumps was measured to confirm successful particle delivery and was found to be within expected range.
Systemic macrophage recruitment continued even at the chronic stage of particle-induced inflammation
To observe the systemic recruitment of macrophages at the later stages of particle-induced inflammation and bone loss, GFP/FLUC expressing reporter macrophages were injected through the tail vein to the systemic circulation 5 weeks after the beginning of continuous particle delivery. After systemic injection of reporter macrophages, a BLI signal localizing to the lungs was detected immediately after the cell injection. Starting from day 2 postinjection, a BLI signal originating from the right distal femur was observed (Fig. 3a, b). Although relatively weak, this signal significantly exceeded the background signal from the left femur. During the course of the 20-day imaging period, the signal from both femurs progressively decreased, but the difference between left and right femur was maintained (p < 0.001, all time points).
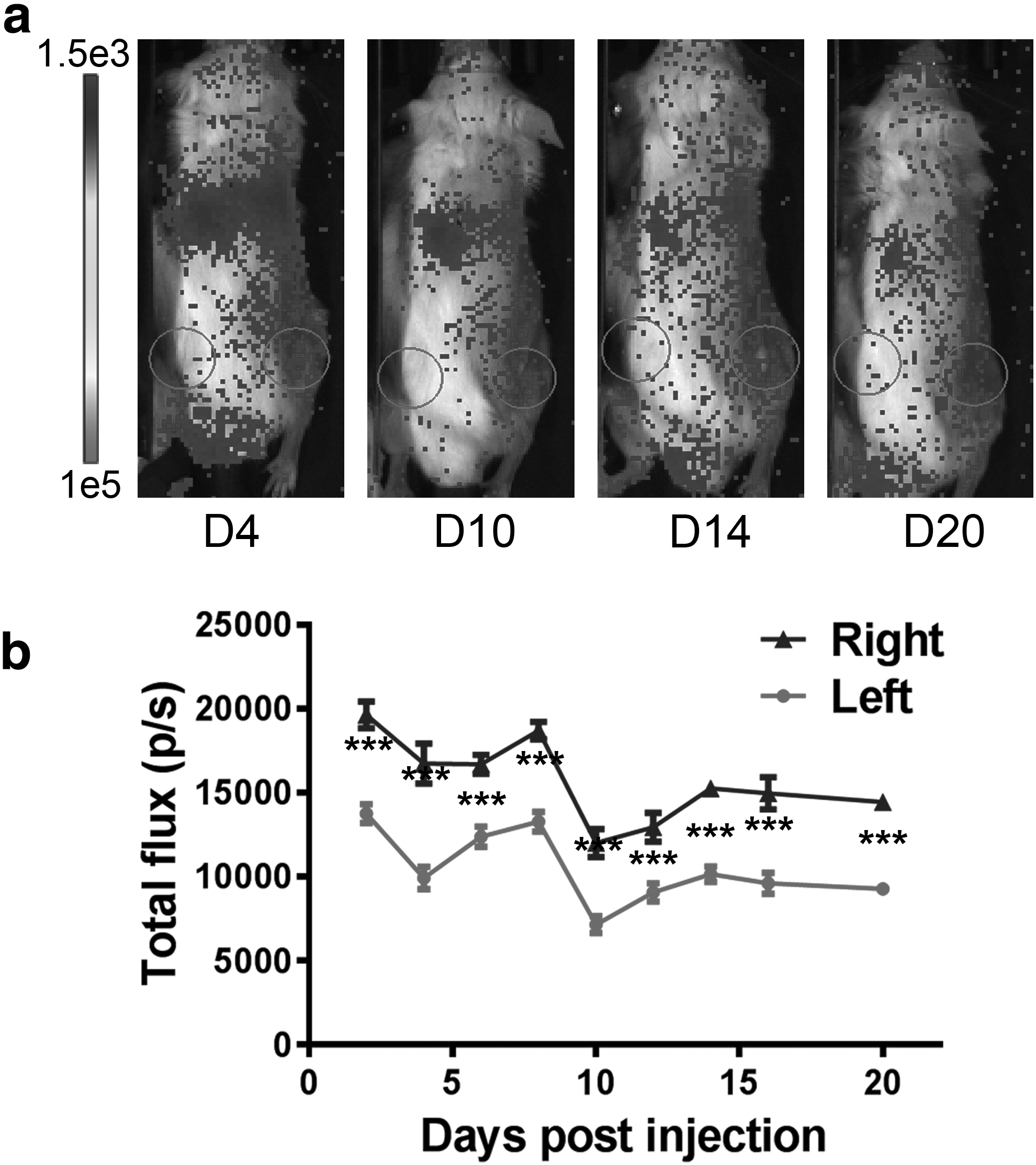
Recruitment of reporter macrophages to the area of particle-induced chronic inflammation in bioluminescence imaging. UHMWPE particles were delivered to the right distal femur for 8 weeks. The systemic recruitment of macrophages to the distal femur at the later stages of particle-induced bone loss was studied by injected GFP/FLUC expressing reporter macrophages to the systemic circulation 5 weeks after the beginning of continuous particle delivery. Luminescence emanating from the right and left distal femur was determined from BLI images obtained every other day up to 20 days postinjection.
Increasing the duration of particle delivery from 4 to 8 weeks exacerbated bone loss by μCT
Continuous delivery of UHMWPE particles to the distal femur for 4 weeks resulted in local bone loss evident by μCT as reduced TMC and BVF in the distal femur compared to controls (3.9 ± 0.15 vs. 3.4 ± 0.14 mg, p < 0.05; 0.27 ± 0.01 vs. 0.24 ± 0.01). Increasing the duration of particle delivery from 4 to 8 weeks exacerbated this particle-induced bone loss with the difference in TMC and BVF between corresponding controls and particle-treated femurs being more pronounced (5.6 ± 0.15 vs. 4.8 ± 0.09 mg/cc, p < 0.001; 0.38 ± 0.01 vs. 0.31 ± 0.01, p < 0.001, Fig. 4a, b).
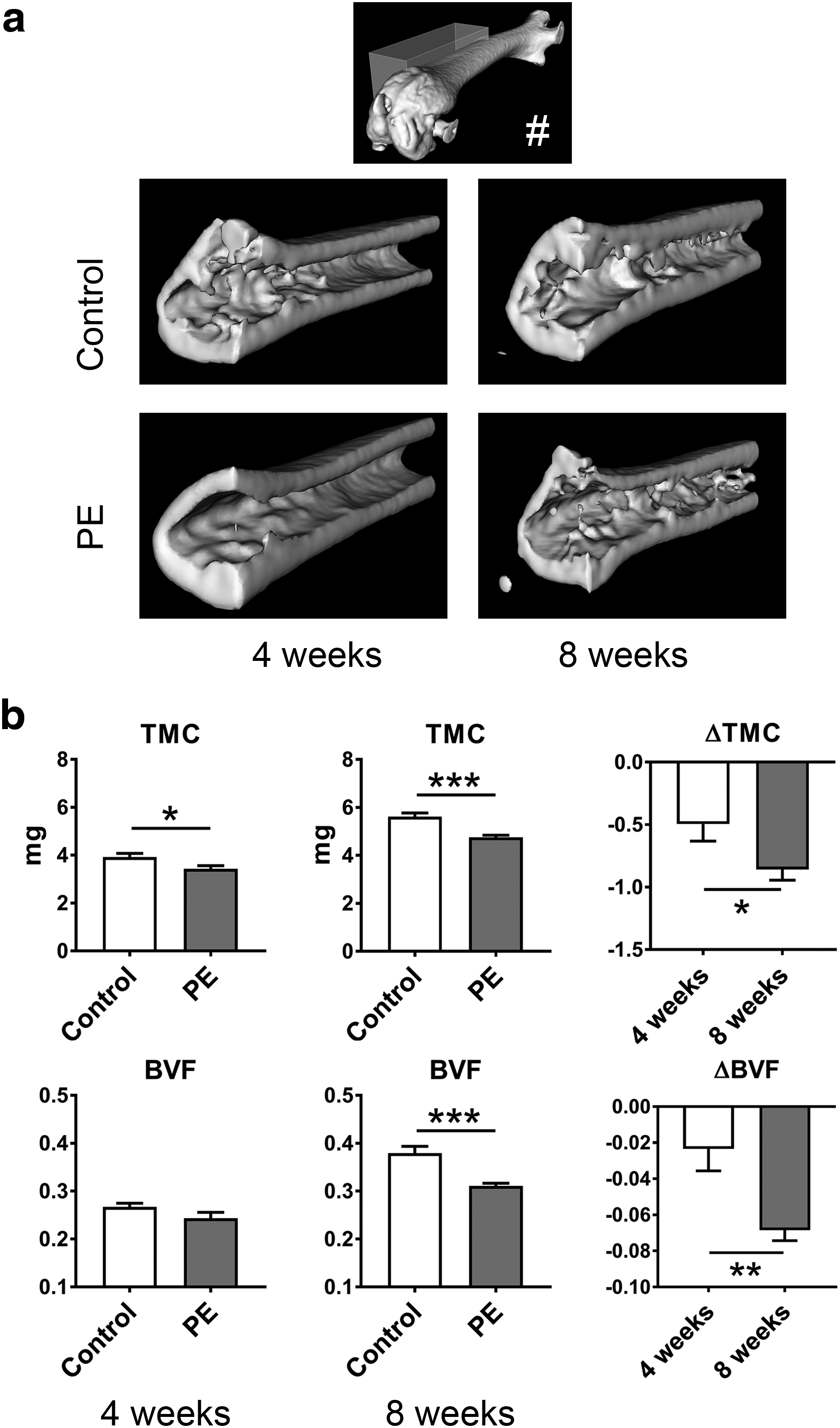
Bone loss at the area of chronic particle-induced inflammation in μCT. UHMWPE particles were delivered to right distal femur for 4 or 8 weeks through hollow titanium rod and the amount of bone at the distal femur was quantified by μCT imaging.
Particle delivery resulted in loss of trabecular bone and increased the amount of macrophages and osteoclasts in histology
Numerous birefringent UHMWPE particles could be seen in histological sections from particle-infused samples examined under polarized light (Fig. 5a). The particles were located in the metaphyseal bone marrow immediately adjacent to the outflow channel of the titanium rod.
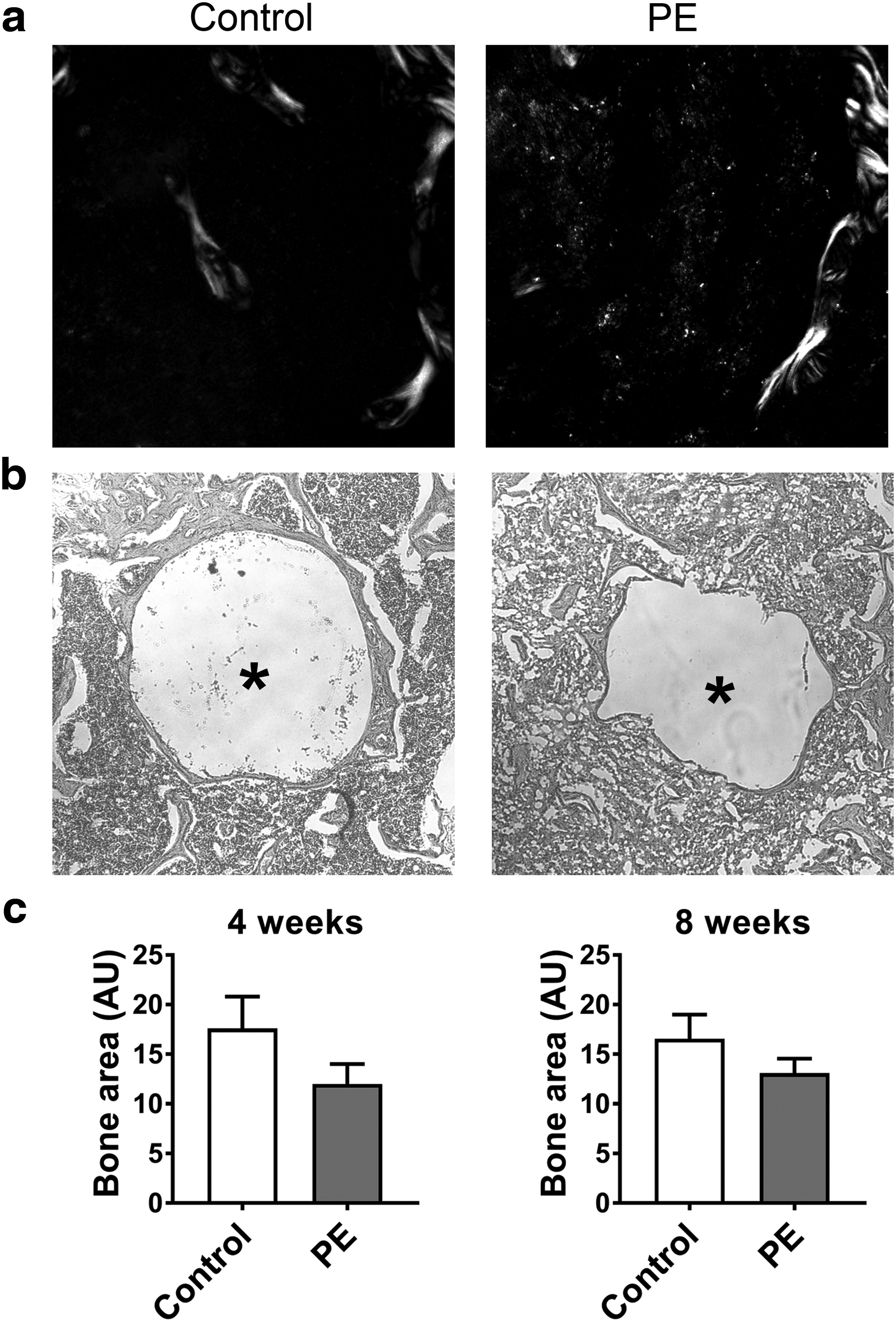
Impact of chronic particle-induced inflammation on tissue histology. UHMWPE particles were delivered to right distal femur for 4 or 8 weeks and the tissue morphology at the distal femur metaphysis was evaluated from H&E-stained tissue sections.
The continuous delivery of UHMWPE particles to the distal femur resulted in qualitative reduction in the amount and quality of peri-implant trabecular bone as assessed from histological sections obtained from the distal metaphyseal region. Moreover, the layer of peri-implant cortical bone that formed around the titanium rod was strikingly thinner, and at times even absent in particle-treated groups (Fig. 5b, c). However, there were no statistically significant differences in the total area of peri-implant trabecular bone either in 4- or 8-week particle delivery groups compared to corresponding controls (17.6 ± 3.2 vs. 12.0 ± 2; 16.6 ± 2.4 vs. 13.1 ± 1.4 AU).
However, particle delivery for 4 weeks resulted in a significant increase in the amount of F4/80+ macrophages in the bone marrow adjacent to the implant (0.13 ± 0.01 vs. 0.17 ± 0.01, p < 0.05) (Fig. 6a, b). Increasing the duration of particle delivery from 4 to 8 weeks further increased the amount of peri-implant macrophages compared to corresponding controls (0.12 ± 0.01 vs. 0.23 ± 0.03, p < 0.05).
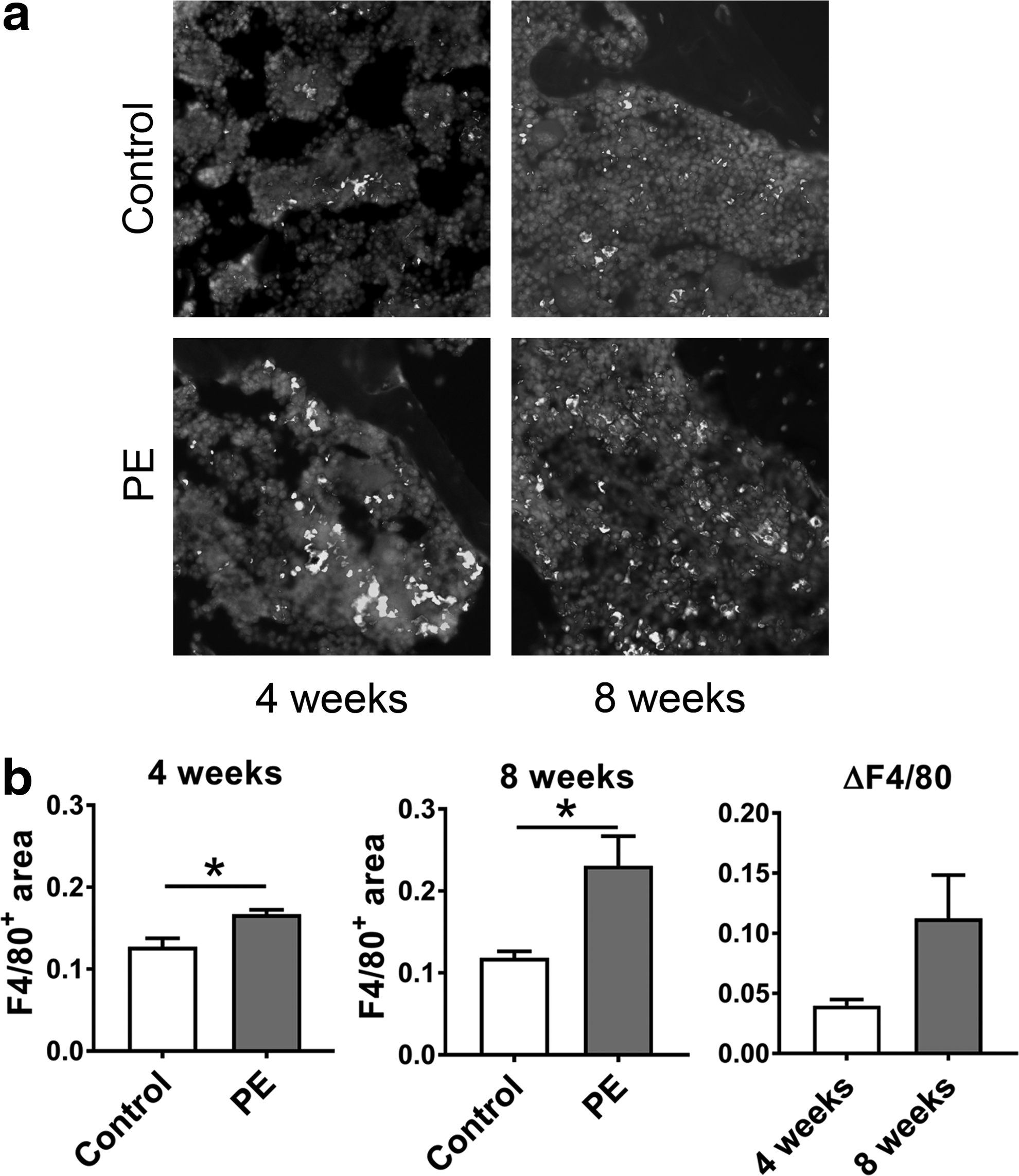
Impact of chronic particle-induced inflammation on the amount of peri-implant macrophages. UHMWPE particles were delivered to right distal femur for 4 or 8 weeks and the amount of peri-implant macrophages was evaluated by F4/80 immunostaining.
Corresponding changes were seen in the amount of peri-implant osteoclasts identified by TRAP histochemical staining (Fig. 7a, b). Particle delivery for 4 weeks resulted in a modest increase in the number of local osteoclasts (0.75 ± 0.14 vs. 1.67 ± 0.30, p = 0.051), while increasing the duration of particle delivery to 8 weeks significantly increased the number of osteoclasts compared to corresponding controls (1.1 ± 0.22 vs. 4.0 ± 0.68, p < 0.05).
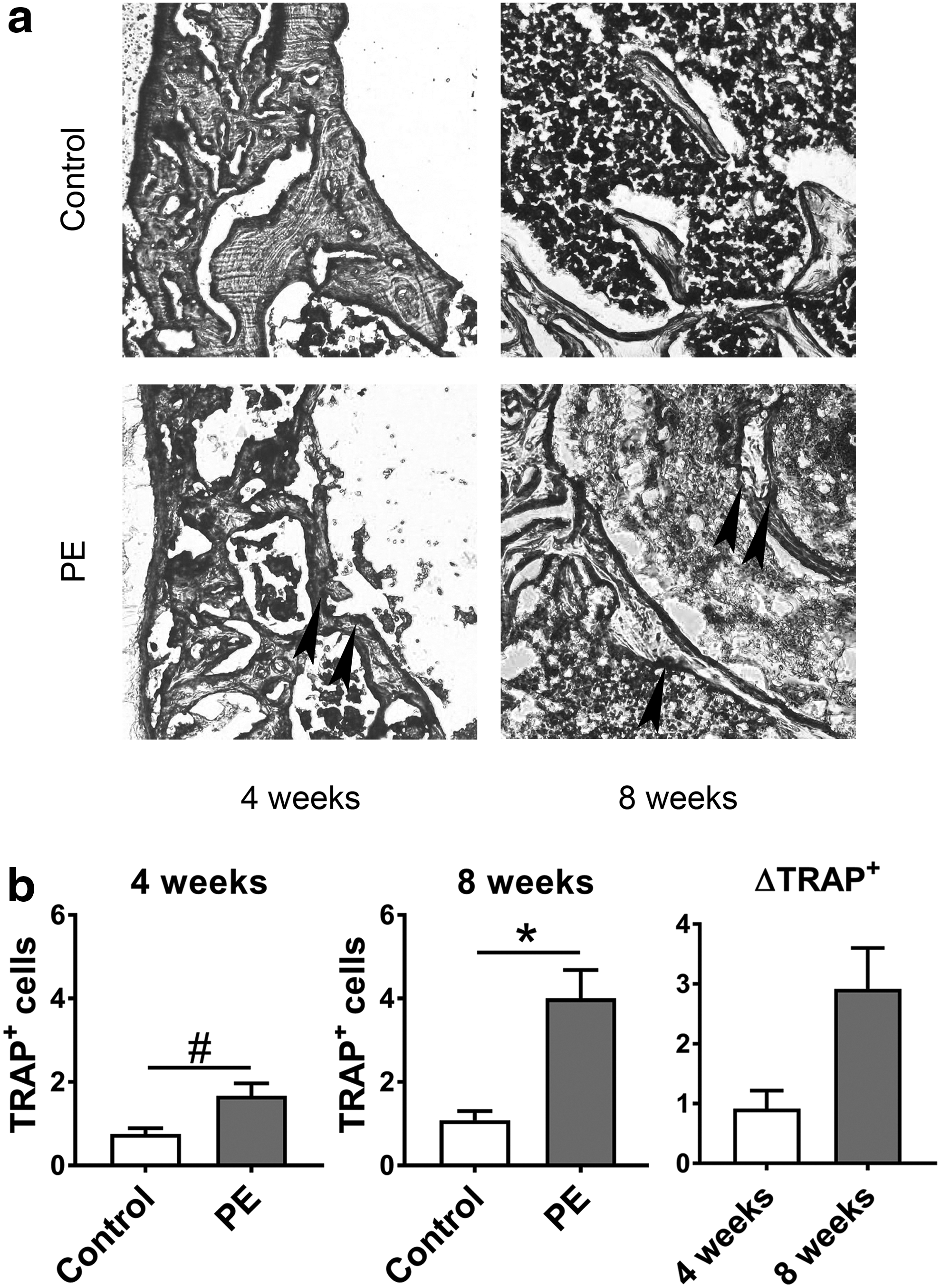
Impact of chronic particle-induced inflammation on the number of peri-implant osteoclasts. UHMWPE particles were delivered to right distal femur for 4 or 8 weeks and the number of peri-implant osteoclasts evaluated by TRAP histochemical staining.
Discussion
Accurate model systems are essential for studying the underlying biology of periprosthetic osteolysis and for the development of novel therapeutic approaches to osteolysis and other conditions characterized by chronic inflammatory bone loss. Through current cell culture and animal models, significant advances have been made in understanding the pathophysiology of inflammatory bone loss. These discoveries include identifying the key roles that macrophages, osteoprogenitor cells, and osteoclasts and their secreted inflammatory and chemotactic mediators play in the process, as well as characterizing the different biological responses elicited by various types of implant-derived wear products.2–4,18 Similarly, in vitro and in vivo models have been used to demonstrate the therapeutic potential of pharmacological agents such as statins, NF-κB blocking agents, and CCL2 inhibitors.19–21
However, it is well recognized that the complex cellular interactions involved in the inflammatory bone loss can only be modeled to a limited extent in single cell-type culture studies. Similarly- most of the existing animal models entail acute biomaterial particle-induced inflammation, while the periprosthetic osteolysis seen in patients is a chronic condition. As such, it is possible that controversies existing over such topics as the importance of strong proinflammatory mediators, for example, tumor necrosis factor-alpha (TNF-α), and the status of peri-implant macrophage activation are partially due to this discrepancy between model systems and the clinical condition. TNF-α and proinflammatory M1 macrophage polarization undeniably play roles in particle-stimulated cell cultures and acute in vivo models of particle-induced inflammation.2–4 However, retrieval studies characterizing the production of strong proinflammatory mediators as well as the status of macrophage polarization at the periprosthetic tissues have been inconclusive, and a small clinical trial with TNF-α blocking antibody was not successful in mitigating the condition.22–26
Surprisingly, little is known concerning the effects that chronic inflammation has on bone and how exactly the foreign body response evolves over time. To address these questions, we developed a novel modification of our 4-week intramedullary particle infusion model. An 8-week intramedullary particle infusion was achieved by changing the subcutaneous osmotic pump after 4 weeks in a minor surgery. The model system incorporates several key elements of the clinical pathological process, including a distal intramedullary bone implant, continuous particle release over an extended period of time, and continued, low-grade, macrophage recruitment to the peri-implant tissues. Importantly, extending the particle delivery to 8 weeks significantly exacerbated the local bone loss and the amount of both peri-implant macrophages and osteoclasts similar to what is observed in clinical setting.
These results closely mirror clinical studies showing that accumulative particle load is the key culprit in the osteolytic process and the extent of implant wear is directly correlated with the degree of osteolysis.27–29 Whether the exacerbated bone loss also resulted in poor implant integration and/or implant loosening in the model remains a topic for further studies. In our prior study, a 4-week particle delivery did not lead to loosening of the titanium rod, presumably because particles were delivered to the proximal end of the rod rather than directly to the bone/implant interface. 30 With the exacerbated and more widespread bone loss following the 8-week particle delivery, it is possible that even implant integration would be compromised, although most of the particles were still seen at the proximal end of the rod immediately adjacent to the outflow channel.
Interestingly, the extent of systemic macrophage recruitment was reduced at this later stage of particle-induced inflammation compared to what we have observed before in our 4-week model.14,15,17 The exact mechanisms of this phenomenon remain a topic for further studies, but suggest a change in the inflammatory and chemotactic microenvironment during the transition from 4 to 8 weeks of particle delivery.
In this study, ∼3.3 × 1010 particles (∼1.8 mg) were delivered to the intramedullary space during the 4-week infusion period and double the number during the 8-week infusion period. For consistency, the particle dosage was chosen based on our previous work using the 4-week model.13–15,17 Although extrapolation of particle dosages from other murine models such as the calvarial model is difficult due to the unique nature of the current model system, the amount of particles is within the same order of magnitude as in these systems.19,31,32 It is possible that the osteolysis would be exacerbated further with increasing particle concentrations.
In addition to the amount, physical characteristics of the wear particles, including their size, shape, and material, could impact the biological response.1–3 Several particle retrieval studies have shown that the size of the clinically relevant UHMWPE particles varies widely ranging from 0.1 to 10 μm with most of the biologically active particles being in the same 0.5 μm range as the particles used in this study.33–36 Similar to the size, the shape of the retrieved UHMWPE particles varies widely from globular to elongated, with elongated ones being biologically most active.37,38
Since the particles used in this study were mostly globular and of a single material, rather than being a mixture of plastics and metals as often is the case in clinical setting, it is possible that all the aspects of wear particle disease were still not fully recapitulated. However, all these parameters can easily be changed and, indeed, the model can be easily adapted to study the reaction caused by different types of particles and various particle concentrations.
Since the ultimate goal of this model system is to study continuous or delayed drug delivery in conjunction with the particle delivery, BSA was added to the particle carrier solution. A wide variety of murine models utilizing osmotic pumps for continuous drug delivery have used BSA as a carrier protein.39–41 Due to the common practice of using BSA in similar experiments, we conclude that significant BSA-induced immunoreaction that might confound the results is unlikely, but still remains a possibility.
The greatest strength of this model system might be that it enables the study of pharmacological and tissue engineering interventions in a setting in which the chronic particle-induced osteolysis has already been established when the treatment is initiated. For example, to model the clinical scenario of a patient with an early peri-implant osteolytic lesion, particle-induced osteolysis is first established with a 4-week particle infusion followed by pharmacological or tissue engineering treatment in an attempt to limit or even reverse the development of osteolysis during the subsequent 4 weeks.
In conclusion, the model developed herein has clear advantages over prior acute models of inflammatory bone loss, but it also is slow, labor intensive, technically somewhat demanding, and hindered by the general well-known limitations of the small animal models. The model is best suited to study the mechanisms of chronic inflammatory bone loss and validate treatment concepts derived from faster model systems, such as the calvarial model, under the conditions that resemble the clinical condition more closely than prior model systems.
Footnotes
Acknowledgments
This work was supported by NIH grants 2R01AR055650 and 1R01AR063717, and the Ellenburg Chair in Surgery at Stanford University. J.P. was supported by a grant from the Jane and Aatos Erkko foundation.
Disclosure Statement
No competing financial interests exist.