
Abstract
Procedures for the evaluation of tissue-engineering processes, including those used for the testing of the relevant biomaterials, have not been developed in a logical manner. This perspectives paper discusses the limitations of testing regimes and recommends a very different approach. The main emphasis is on the existing methods for assessing the biological safety of these biomaterials, which, it is suggested, are irrelevant for evaluating materials that are intended to facilitate the generation of new tissue. An algorithm is proposed that sets out the pathway from materials design and characterization through to the production of a file that sets out full biocompatibility, functionality, and tissue incorporation data that are suitable for regulatory consideration for first-in-man experiences. Central to this algorithm is the choice of animal models and the real-time monitoring of the implanted construct performance.
Introduction
T
There is no doubt that both the preclinical assessment of tissue engineering/regenerative medicine (TERM) products and their validation in clinical trials have posed significant difficulties for those involved in product development and those in regulatory agencies. The essential difficulty is that TERM products are neither conventional medical devices nor classical pharmaceuticals, so that the regulatory pathways that have been developed over decades for these groups of products, with varying degrees of success, are not necessarily, or indeed highly unlikely to be, suitable for safety and efficacy testing systems in the new regime of tissue engineering.
With pharmaceuticals, the preclinical assessment is aimed at demonstrating that the product is safe enough to take to humans in clinical trials and is likely to be effective in patients. The relevant studies may address acute, sub-chronic, and chronic toxicity, carcinogenicity, reproductive toxicology, genetic factors, immune system effects, mucosal surface irritation, as well as pharmacokinetic studies (specifically ADME, that is absorption, distribution, metabolism, and excretion studies). These may involve rats, mice, hamsters, rabbits, dogs, and nonhuman primates. Even with decades of refining these processes, only 1 out of each 1000 potential drugs succeeds in preclinical testing, allowing approval for clinical trials, whereas 9 out of every 10 of these will fail in those trials. 1
These procedures are not the ideal starting point to test TERM products since their mechanism of action will not be the same. It is important to recognize that the classification of healthcare products, and their route for regulatory assessment, is based on the primary mechanism of action. Definitions vary with different jurisdictions although concepts are equivalent; pharmaceuticals are considered as substances that exert their effects by pharmacological, immunological, or metabolic activity, whereas medical devices specifically cannot have a principal intended action in the human body that involves any of these effects. Put even more simply, medical devices cannot function through chemical actions and cannot be metabolized, which are the essential features of drugs. TERM products fit neither category.
With medical devices, the evaluation regime is quite different to that for pharmaceuticals. Most product development and preclinical risk assessments are carried out through engineering-based laboratory procedures. For example, total hip replacement mechanical performance is evaluated through hip simulator systems, and prosthetic heart valve hemodynamics are assessed by pulse duplicators and similar devices. In the former case, in vivo studies are largely irrelevant since there are no animal models that can replicate the mechanical environment of the functioning human hip. Heart valves may be tested in animal models, largely for demonstration of safety, although there have always been controversies over the suitability of porcine, ovine, and bovine models for predicting performance in humans. 2
With respect to regulatory approval, there are some device-specific international standards for testing performance, for example the ISO series for cardiac pacemakers 3 and the series for intraocular lenses 4 but, by far, the most widely used standards are those of the ISO 10993 series, which specify tests for biological safety of biomaterials. 5 These involve both in vitro and in vivo procedures and form the basis of decisions about placing medical devices on the market in all global jurisdictions. These tests are based on the principle that biological safety is essentially derived from a lack of any biological or physiological interactions between biomaterials and the tissues of the host, again, as demonstrated later, hardly the optimal starting place for TERM product testing.
It is intuitively obvious that TERM products do not have a primary function that is the same as that for either a pharmaceutical agent or a medical device and, therefore, should not necessarily be evaluated by the same procedures used for those products. It is equally obvious that, as new medical therapies and products are introduced, regulatory authorities are most likely to use the tools that they already have available to facilitate getting these new therapies to patients with adequate safety. Such regulators, of course, have already recognized that some medical products have features of both drugs and devices, often referred to as combination products, 6 and deal with them through a combination of existing procedures. However, these procedures tend to treat the components separately, assuming that there is no synergistic activity associated with them.
This may not be the best way to deal with a complex situation. For example, drug-eluting stents used for the treatment of stenosed coronary arteries rely on the release of powerful agents such as antiproliferative drugs from metallic or polymeric stents, where the biocompatibility of the stent is assessed by normal device procedures and the safety of the agent is determined by normal drug procedures. However, the pharmacokinetic properties of such drugs may be different when released over a period of time from an implant; Yang and Burt have shown that the drug distribution in vessel walls is heterogeneous, where factors such as hydrophobicity/hydrophilicity of the drug, diffusivity, blood flow, arterial structure and pathological status, endothelium resistance, and protein binding all contribute to the release and distribution profiles. 7
Similar arguments prevail in the situation where Bone Morphogenetic Protein-2 is incorporated into a biomaterial sponge, to be released in vivo for the enhancement of spinal fusion, and where side effects have been associated with uncertainties over dosing, release rates, and differential effects on the various tissues around spinal vertebrae. 8
It is already clear, therefore, that there are significant concerns about using, either for research or regulatory purposes, standard in vitro and in vivo procedures for the assessment of therapies and products other than stand-alone drugs and devices. This inevitably impacts many of the procedures under development within TERM. This article reflects on these difficulties, with particular reference to the biomaterials used in these procedures, and concludes with the derivation of a new algorithm that addresses the preferred sequence of events in product evaluation. It is also relevant to mention here the role of good laboratory practice (GLP) principles. It is usually the case that product and process development procedures are not carried out under GLP conditions, with these only becoming applicable for testing that is carried out for regulatory approval. It will be suggested later in this article that much could be gained by using GLP procedures at much earlier stages.
Biomaterials in Tissue Engineering
The present author has discussed some important issues regarding the selection and performance of biomaterials in tissue engineering9,10 and placed these in the context of new perspectives on biocompatibility,11,12 in several recent publications.
Tissue engineering may be defined as “the creation of new tissue by the deliberate and controlled stimulation of selected target cells through a systematic combination of molecular and mechanical signals.” 13 Molecular and mechanical signals do not directly imply the use of biomaterials, and tissue engineering may be carried out in the absence of biomaterials. However, the tissue generated in this way usually needs form and structure, and injected cells are unlikely to provide this without the assistance of biomaterials. In addition, neither molecular nor mechanical signals are easy to deliver with the appropriate spatial and temporal characteristics; a biomaterial that contains and delivers such signals to the required cells would be very beneficial. It is noted that not all tissue-engineering processes involve cells cultured with the biomaterial in vitro before implantation; in some situations, a porous biodegradable construct can be implanted, after which the host's own cells invade the structure where they express new tissue matrix.
It has been common practice to describe the material constructs used in tissue engineering as scaffolds. Conventional scaffolds tend to be discrete porous constructs, usually of polymers or ceramics, where appropriate cells infiltrate the pores and are intended to express new tissue within these spaces, with the biomaterial degrading and resorbing at the same time. However, a scaffold is required to provide an environment, or niche, that favors the natural behavior of cells.
The in vivo microenvironment of a cell, in general, is composed of the relevant extracellular matrix (ECM), homotypic or heterotypic cells surrounding that cell, and cytokines and other bioactive agents around the cells associated with endocrine, autocrine, and paracrine secretions. The microenvironment should also involve topographical and architectural features and mechanical forces. It is obvious that typical synthetic porous materials will have considerable difficulty in replicating this type of microenvironment and do not represent the ideal format for a so-called tissue-engineering “scaffold.” Further, the term “scaffold” falls far short of the characterization and specification required for these supporting constructs. The overarching term “template” is far preferable.
An important question immediately arises from this position: If template materials are intended to replicate the microenvironment of cells, and, over time, facilitate the delivery of mechanical and molecular signals that are responsible for new tissue generation, what are the critical specifications for these structures? The present author has recently produced a list of such specifications, 9 at the focal point of which is the nature of the interactions between the materials and the tissue environment.
Generically, these interactions have been discussed under the heading of “biocompatibility.” It is essential at this stage to identify the specific nature of biocompatibility phenomena in tissue engineering and to see how these phenomena differ from those associated with biomaterials used in other areas of medical technology. Only when the mechanisms of biocompatibility of tissue-engineering templates are understood can acceptable models for its assessment be defined.
Biocompatibility is a term that has been used for many years, but it is still poorly understood. It was first seriously defined in the 1980s when it was determined that biocompatibility refers to “the ability of a material to perform with an appropriate host response in a specific application.” 14 This implies that biocompatibility has to be considered in terms of the precise situation in which a biomaterial is used. It follows that biocompatibility phenomena associated with any one biomaterial will vary depending on the application, meaning that biocompatibility is not a property of a material but of a biomaterial–host system, 15 and that there is no such thing as a universally biocompatible material. 11
This calls into question the whole paradigm of testing the biological safety of a biomaterial that has the ultimate objective, in conventional language, of demonstrating that the materials used in products are “biocompatible,” language that is subsequently used by manufacturers and regulators to justify the use of the materials.
Paradoxically, this approach has served the medical device sector quite well over the years, although there have been, as discussed later, several situations where major misunderstanding of biocompatibility mechanisms has resulted in “approved” products and the materials of their construction causing significant clinical problems. The reason for this has been the inexorable trend toward the selection of biomaterials that are maximally inert, both chemically and biologically, for the construction of implantable medical devices. The functionality of such devices is almost exclusively of a mechanical or physical nature, and it is determined by design features and the nature of those materials that have the optimal properties related to those functions; examples are the optical properties of intraocular lenses, the electrical properties of pacing leads and insulators, and the tribological properties of joint replacement articulating surfaces.
Once these properties have been characterized, the final choice of material will be controlled by the known biocompatibility of the candidate materials, which, in practice, means their inertness. Rarely will a manufacturer stray outside the relatively short list of candidates; almost always the materials will be on a short list, including titanium alloys, cobalt-chromium alloys, alumina and zirconia ceramics, PTFE, polyethylene, polypropylene, and some acrylics, which have been shown time and time again to have acceptable resistance to degradation and no known biological activity. Hence, the standard series of tests included in the ISO 10993 series are adequate for this purpose in implantable devices since they are intended to show that the approved biomaterial has no biological effect on the tissues of the body. There are some obvious exceptions to this paradigm, of course, especially those medical devices that are intentionally degradable and those that are intended to exhibit “bioactivity.”
The situation with tissue-engineering biomaterials is, however, quite different. At the very simplest level, it should not be expected that a material that has been shown to have no interactions, biologically or physiologically, with components of the body can, at the same time, facilitate the “deliberate and controlled stimulation of selected target cells through a systematic combination of molecular and mechanical signals.” The ultimate scenario is, therefore, that a tissue-engineering biomaterial is shown to pass all relevant ISO 10993 tests, and is consequently labeled “biocompatible,” but which, when used as a porous construct, is unable to stimulate any biological process and merely becomes partially filled with functionally useless scar tissue.
This is likely to be one of the major factors (although there are several other candidates) in the clinical failure to regenerate tracheas by using synthetic degradable polymers. 16 There are also many examples where simple biodegradable polymers fail to generate adequate functional tissues, but biologically modified polymers fare much better. For example, the incorporation of self-assembling peptides into poly(caprolactone) improves cartilage regeneration by human expanded articular chondrocytes. 17 In a clinical setting, Atala et al. were able to engineer bladder tissue with autologous urothelial and muscle cells by using a composite structure of a biodegradable polymer and collagen. 18
A comparison between the essential requirements of biomaterials for long-term implantable medical devices, tissue-engineering templates, and combination products is provided in Table 1. It is a striking conclusion from an analysis of these requirements that the same biocompatibility testing regimes should not be used for the materials used in these different types of products. Returning to the crucial point made earlier about biocompatibility not being a property of a biomaterial but rather of a biomaterial–host system, it does not make any sense to determine the biocompatibility of a tissue-engineering template by itself, outside of the context of its use as a template/cell/biomolecule system.
To determine the types of regime and the optimal animal models for tissue-engineering biomaterials, it is necessary to review briefly the relevant mechanisms of biocompatibility.
Mechanisms of Biocompatibility to be Addressed by Animal Models
Biocompatibility has for long been considered a perturbation of the wound healing process that inevitably occurred after a surgical procedure to implant a medical device. Not surprisingly, animal models used to assess the biocompatibility of these materials involved the implantation of samples in subcutaneous or intramuscular sites and after the time course of histological changes, where the goal was minimal fibrosis and little or no chronic inflammation. Wound healing, however, is not a good starting point to discuss mechanisms of biocompatibility in tissue-engineering applications.
Arising from an extensive analysis of biocompatibility phenomena, which takes into account clinical outcomes after the use of biomaterials in all technology sectors, it has been possible to identify a new paradigm that generically defines the mechanisms that drive the events of the host response and the pathways that determine the eventual outcomes. 12
As soon as a biomaterial comes into contact with components of a living system, three events are simultaneously triggered. These are a perturbation of the mechanical environment, the perturbation of the physiological environment, and the adsorption of macromolecules of the environment onto the biomaterial surface. Under most circumstances, the protein adsorption process and any rearrangements of the interfacial region have only minor effects on subsequent events and are not considered here. On the other hand, the perturbation of mechanical and physiological environments initiates the two essential (and related) biocompatibility pathways, mechanotransduction and sterile inflammation.
Mechanotransduction is concerned with the molecular and cellular processes involved with the conversion of mechanical stimuli into biochemical signals,19,20 and it is the primary baseline phenomenon in biocompatibility. Specifically, in the context of tissue engineering, it plays a major role in determining stem cell differentiation pathways within hydrogels, especially seen through the effect of hydrogel stiffness.21–23
Sterile inflammation, referred to here as biomaterials-induced sterile inflammation (BISI), is superimposed on mechanotransduction to guide and determine the balance between inflammation and fibrosis. Central to the mechanisms of BISI are the damage-associated molecular patterns (DAMPs)24–27 that are initiated at the moment of biomaterial–host contact, and the activation of one or more inflammasomes, 28 in association with pattern recognition receptors, and the subsequent cytokine and chemokine activity.
Importantly, the degree of inflammation in response to any challenge, and the temporal profile of the process, will determine the resulting host response. Pro-inflammatory, anti-inflammatory, and pro-fibrotic pathways are all available, 29 the orchestration of which is mediated by the nature of the DAMPs, and the ensuing balances between matrix metalloproteinases and tissue inhibitors of matrix metalloproteinases, between ECM deposition and breakdown, and crucially between M1 and M2 macrophages. 30 Again, in the context of tissue-engineering templates, BISI will control the host response to any degrading biomaterial and the degradation products.
Microtopography is of minor importance in biocompatibility pathways. Nanotopography may play some role through the modulation of focal adhesion formation, cytoskeletal development, and integrin-specific signaling in the functional differentiation of cells, 31 although these processes may be considered variations of mechanotransduction phenomena. More important than topography is material or construct architecture, especially with the role of the 3D nanoarchitecture of hydrogels in the differentiation and function of stem cells. 32 It is possible to modulate biocompatibility through the sustained release of biologically active agents. So far, the clinically applied processes have been rather crude, with little control over pharmacokinetics and the avoidance of side effects. However, considerable opportunities arise if highly specific targets associated with inflammasomes and the inflammation–fibrosis balance are used.
The Tissue-Engineering Biocompatibility Testing Paradigm
The consequences of the analysis summarized earlier is that, generically, biomaterials influence their host through their perturbation of the mechanical environment and through the manner by which they act as DAMPs and influence, over time, the inflammatory and fibrotic responses. Optimal control of these phenomena in the tissue-engineering context, however, will not guarantee the regeneration of the desired tissue. It is the responsibility of the target cells to do this, but they must be assisted by, and not opposed by, the biocompatibility characteristics of the biomaterial.
A tissue-engineering template may come into contact and interact with its ultimate host either by in vitro/ex vivo incubation with cells (and biological molecules) followed by implantation of the resulting construct into the host, or by direct insertion (injection or implantation) into the host. The evaluation regime used in any particular application should take the precise details of these processes into account.
The parameters by which the biomaterial may influence the tissue-engineering process and the overall health of the host are given in Table 2. Also given in this table is a summary of all nonmaterial-related variables that control, to greater or lesser extents, these processes. It is obvious, once again, that tissue engineering is too complex to be adequately explained by independent observations on each of its components. As argued by the present author a decade ago, tissue engineering should be tackled by using a systems-engineering approach, 13 which implies that it should be addressed as a whole complex system and not the sum of its parts. In developing a template testing paradigm, therefore, which has significant implications for the animal models used for evaluation purposes, we cannot take individual phases of the process and draw significant conclusions about either the safety or efficacy of tissue engineering from them.
At the outset, it should be mentioned that one ultimate objective here could be the development of computational models of tissue-engineering processes, and, indeed, that is one possible implication of the need to use systems-engineering approaches. This, of course, is not a trivial process. Several authors have attempted to lay some ground rules here, including Neagu et al., 33 Diaz-Zuccarini and Lawford, 34 and Sanz-Herrera and Reina-Romo, 35 and recently an influential review by Walpole et al. has been published. 36 While emphasizing that this is a laudable intention, which should be pursued, it is unlikely that computational modeling of biocompatibility will play any meaningful role in the evaluation of tissue-engineering templates in the near future.
The use of ISO 10993 standard tests in tissue-engineering products
It is not easy to discern just how many laboratories use ISO 10993 procedures for the evaluation of the biocompatibility or biological safety of tissue-engineering biomaterials since few such studies are placed in the public domain. Regulatory agencies may still require or accept the data provided by these tests as proof of biological safety, and a recent (2014) workshop on standard tests and procedures for tissue-engineering scaffolds promoted ISO 10993 as the success story in the evaluation of the biological safety of such scaffolds. 37 Many studies involving ISO 10093 procedures are published in academic journals as demonstration of good biocompatibility and indications for clinical use, for example, in bone engineering,38,39 cartilage engineering, 40 and for polymers in general.41–45
The US Food and Drug Administration (FDA) has recently published guidelines on the use of ISO 10993 Part 1. 46 This is a helpful document with respect to conventional medical devices. However, it does not address risk management within tissue engineering; although a scaffold does comply with one of the two alternative descriptions of a medical device used by the FDA in the sense that it is “intended for use in the diagnosis of disease or other conditions, or in the cure, mitigation, treatment, or prevention of disease, in man or other animals,” it does not comply with the second description of being “intended to affect the structure or any function of the body of man or other animals, and which does not achieve any of its primary intended purposes through chemical action within or on the body of man or other animals and which is not dependent upon being metabolized for the achievement of any of its primary intended purposes.”
These definitions were introduced before tissue-engineering products were developed, and the concepts of risk management based on the need to avoid harmful biological effects simply do not apply to tissue-engineering templates. It would be preferable to avoid equating a tissue-engineering template with a medical device. It should be noted that although the FDA recommends the use of ISO 10993, it also considers that these tests are only a framework for the selection of analyses, and that it is up to the product developer to provide a rationale for the selection and/or waiving of the tests performed. 47
Currently, there are twenty parts to ISO 10993, most being concerned with in vitro tests and characterization methods, with just a small number involving animal models. Phenomena under scrutiny include cytotoxicity (Part 5), sensitization (Part 10), genotoxicity and reproductive toxicity (Part 3), local tissue responses (Part 6), systemic responses (Part 11), interactions with blood (Part 4), and degradation (Part 13).
Phase I of the preclinical assessment of tissue-engineering templates
It is suggested here that there is little place for these standard tests in either the development or regulatory control of tissue-engineering templates. A few examples of the inappropriateness of such standards will suffice to demonstrate this point. Cytotoxicity is carried out by exposing some samples to extraction media and then exposing certain cells to the resulting extract, with the effects on the cells being determined semi-quantitatively in comparison to controls. This has no relevance to the interaction between the target cells of tissue regeneration and porous scaffolds, hydrogels, or ECM-derived substances.
Polymer degradation is evaluated by mass loss of samples placed in either a hydrolytic (a buffer) or oxidative (hydrogen peroxide) solution together with some form of material characterization. Again, this has no relevance to the performance of templates under either in vitro or in vivo situations, where both the cellular/molecular environment and mechanical stresses are important. Local effects on tissues are observed after samples are placed in certain sites for periods of time, the tissues being examined on explantation, with features such as fibrosis, necrosis, and inflammation being documented and scored.
The earlier discussion is not intended to disparage standard tests with medical products, which clearly have an important role, as already discussed. 37 Indeed, there have been recent attempts to place standard tests on a more scientific footing to facilitate their interpretation, 48 but these refer to conventional medical devices and not to tissue-engineering templates. It should also be noted that standard tests such as these are not necessarily predictive of clinical performance even with conventional medical devices, and especially have difficulties in anticipating responses under complex biological circumstances. For example, standard cobalt-based alloys, shown numerous times to have good biological safety profiles in many circumstances, produced idiosyncratic immunological responses in some patients with metal-on-metal hip replacements when the bearing surfaces generated nanoparticulate rather than microparticulate debris. 49
There are several other factors about standards and regulatory bodies that should be considered. The first concerns chemical characterization. Part 18 of ISO 10993 is concerned with methods of chemical characterization. For polymers, this includes recommendations for the parameters to be analyzed, including chemical structure, pendant group analysis, copolymer characterization, cross-linking, branching, additives, residues and impurities, residual monomer and catalysts, and molecular mass/distribution.
The FDA recommends that very serious attention should be paid to the chemical assessment. 46 In particular, it is stated that with some combination products, it may not be possible to mitigate the toxicological risks with traditional biocompatibility testing conducted on the device in its final form; for example, genotoxicity, carcinogenicity, and developmental toxicity endpoints may be better assessed through chemical characterization and toxicological data from the literature. The same argument is used for products that change over time. In the same document, the FDA places significant emphasis on a literature review; if literature is used to waive testing for certain biocompatibility endpoints, a regulatory submission should include information on the applicability of the dose, and on the route and frequency of exposure derived from the literature as compared with the proposed device use.
The inescapable conclusion from the earlier analysis of the effectiveness of preclinical assessment of tissue-engineering biomaterials is that this process requires a radical overhaul. Abandoning the whole process would not satisfy regulatory authorities, who are, understandably, charged with the responsibility of ensuring safety as far as that is possible. It is suggested here, however, that such requirements may be fulfilled by the combination of full chemical characterization and literature review; this should not be considered a trivial exercise but a very detailed process, carried out by experienced scientists, where every possible constituent of the biomaterial product is identified and their biological (including toxicological and immunological) properties, and therefore potential effects on cells and tissues, determined from information in the peer-reviewed scientific literature.
This would be far more effective than the use of ISO 10993 tests discussed earlier, and this should constitute the first phase of preclinical assessment, to be followed by the second phase discussed in the next section. It should be noted parenthetically that one recommendation from the workshop on standard tests previously mentioned 37 stipulated that standard methods should be simple and low cost, on the grounds that tissue-engineering products are becoming prohibitive and complex measurements are difficult to standardize. This is not an appropriate basis for the future development of testing paradigms in TERM.
As a final point in this section, and following on from the discussion of literature reviews, it may be relevant to consider whether the FDA concept of substances generally regarded as safe (GRAS), widely used in the context of food additives, could be applied to tissue-engineering biomaterials. These FDA procedures have been redefined recently, 50 and it is recommended here that similar procedures should be considered in this first phase of TERM assessment. The possibility of using the GRAS concept in TERM was briefly mentioned by Webber et al. recently. 51
Phase II of the preclinical assessment of tissue-engineering templates
Phase I of the preclinical regime should determine that the template has the characteristics and properties that will allow “safe” use. It does not predict biocompatibility since the template has been considered in isolation and not as a part of a biomaterial–host system. The second phase is aimed at determining the biocompatibility and functionality of the system in the context of regenerating the appropriate tissue. Again, the procedures used will have to be different from those used to determine the host response to an implanted medical device since such devices provide the functionality themselves whereas biocompatibility is concerned with the long-term incorporation of the device in the host without causing any detrimental effects on the host.
With tissue engineering, the template, the initially seeded cells and biomolecules, and the host environment all contribute to the expression of the required tissue matrix and its reorganization/remodeling into the functional construct that is integrated into that host. It is not sufficient to implant the template into a host and to wait a defined period before carrying out postmortem qualitative or semi-quantitative pathological analysis.
It is necessary for all processes involving both cells, biomaterials, and the newly generated tissue to be monitored, preferably in real time. This should be undertaken during both in vitro and in vivo stages. It is important to recognize that this is relevant to both product R & D and regulatory procedures so that the methods used have to be consistent with the requirements of both procedures, and preferably performed together. Again, this is in sharp contrast to medical device procedures, where design and functionality evaluations are performed first and the resulting design-freeze product is later tested to detect any biological risks. This, of course, has implications for the use of quality systems, especially GLP systems, at all stages.
In view of the wide variety of potential tissue-engineering applications, involving different disease states and tissue/organ types, it is impossible to prescribe standard series of test procedures and standard animal models; indeed, at the present time, there is insufficient scientific knowledge to identify best practices here. What can be done is to evaluate the existing literature to identify which experimental procedures appear to have provided sufficient data, of sufficient quality and relevance, to justify the use of specific tissue-engineering procedures in clinical trials and clinical studies.
Preferred animal models
It is appropriate to start at the extreme end of the spectrum and consider the use of nonhuman primates. It is recognized that such use is associated with significant ethical issues, and strong cases have been made to phase out the use of nonhuman primates in medical research. 52
Nevertheless, this option should be considered. If there is strong evidence that high-quality evaluation of tissue-engineering products and procedures using nonhuman primates allow clinical studies to take place with a good level of confidence, which could not have been obtained with different species (and, incidentally avoiding many studies with lower-order animals that provide useless or misleading data), then they should proceed. The case for the use of primates in regenerative medicine has recently been made by Daadi et al., 53 although it is noted that the authors work for an organization that is partly based on a primate research center. It is agreed that due attention should be given to the practical consequences of the ethical issues, including consideration of the so-called Replacement, Reduction, and Refinement concept with nonhuman primates, as recently discussed by Burm et al. 54
There is evidence that some such studies have, indeed, proved to be valuable, especially with applications in the central cardiovascular and central nervous systems. In the domain of heart valve tissue engineering, Weber et al. developed valves by using autologous bone-marrow-derived mononuclear cells that were seeded onto nonwoven biodegradable synthetic composite structures and completed preclinical studies with pulmonary valve replacement in nonhuman primates. 55 In vivo functionality was assessed by echocardiography for up to 4 weeks, and the valves were analyzed biomechanically and immunohistochemically at autopsy.
Menasche et al. worked with human embryonic stem cell-derived cardiac progenitors embedded in fibrin scaffolds for the treatment of the infarcted heart. Preclinical animal studies involved 350 rats, 50 immunodeficient mice, and 32 nonhuman primates; their recently published review of all of these steps leading to the submission and approval for first-in-man clinical use in France documents the critical role of the nonhuman primates in this type of application. 56 With tissue-engineered blood vessels, L'Heureux et al. have used a variety of animal models, including nude rats, dogs, and primates. 57 The latter choice was based on the need to use a model with a more representative biomechanical environment, specifically a relevant circumferential wall stress in the artery.
Within the central nervous system, it has long been standard practice to use nonhuman primates in neural interface technology, 58 therapies for Parkinson's disease, 59 and stroke research. 60 Recently, nonhuman primates have been widely used in stem cell therapy research in the brain 61 and in the development of cell therapeutic and tissue-engineering approaches to spinal cord injury. 62 In the latter context, it is instructive to follow the work of Slotkin et al., who used nonhuman primates to evaluate tissue-engineered solutions for acute spinal cord injury, where kinematic and locomotion studies were undertaken during 12 week experiments in hemisected animals. 63 It is also considered by some that spinal disk tissue-engineering products need nonhuman primates for final stages of evaluation. 64
It is not suggested here that nonhuman primates are an essential component of tissue-engineering strategies, even with complex organ tissue engineering. There are several organ replacement projects that have reached the clinical level without primate experience; for example, the bladder regeneration work of Atala was based on several models, up to the dog. 18 However, it is clear that in those situations where lower-order mammals provide neither the biomechanical, biophysical, biochemical, or physiological environment, nor mechanisms of time-dependent functional assessment, that allow the acquisition of meaningful data that can support clinical use, nonhuman primates should be considered.
A review of reports on significant series of animal studies on tissue-engineering procedures suggests that optimal results are obtained with combinations of immunodeficient rodents and suitable large animals, especially ovine, canine, or primate models. The former are used for the examination of discrete phenomena as part of systems optimization, especially related to biocompatibility issues, whereas the latter incorporate realistic functional tests, which are discussed in the next sections.
Biocompatibility
Bearing in mind the previous discussion about biocompatibility mechanisms and pathways, it is important that the evaluation procedures and animal models are designed to determine as many of the relevant processes that take place, and in as much quantitative detail as possible. Three specific factors are the most significant, biodegradation, mechanotransduction, and sterile inflammation.
As already mentioned, it is unlikely that simple in vitro tests for biodegradation will yield clinically relevant data. There have been, of course, many studies published in which samples of biomaterials have been implanted, usually in rodents, and degradation assessed by end-point mass loss or chemical changes, but these do not allow real-time tracking of the processes. As discussed by Artzi et al., 65 the difficulties with both standard in vitro and in vivo degradation studies may be potentially overcome by the use of techniques that monitor in vivo degradation processes by tracking some property that reflects the degradation profile. They chose fluorescence imaging in which degradation (or more specifically in their experiments, erosion) was determined from the decay in total material fluorescence signal by using a noninvasive imaging system.
Poly(ethylene glycol)-dextran and collagen constructs were evaluated in a nude albino mouse model, using either fluorescein or Texas Red labeling, with appropriate corrections to eliminate tissue autofluorescence. More recently, Wang et al. used rhodamine B as the fluorescence tag to monitor the degradation of a poly(caprolactone)-based copolymer in real time in balb-c mice, 66 and Kim et al. used a Cy3 fluorescent dye for real-time tracking of the changes in porcine collagen, also in a murine model. 67 There are alternative tracking methods: Kim and Wagner have recently reviewed the use of ultrasound imaging technologies for this purpose, 68 whereas Zhang et al. report on the use of photoacoustic microscopy. 69
As vital as mechanotransduction processes are, it is difficult at this stage to identify methodologies that can yield clinically meaningful, quantitative data about the mechanical effects within tissue-engineering templates; the science here is at an early stage and much more needs to be known about the precise pathways that are involved. There has been some progress with real-time imaging of mechanotransduction signaling pathways in ex vivo models, such as that reported by Ishihara et al. for the fluorogenic monitoring of calcium signaling in bone in response to shear stresses. 70 The field of live cell imaging of mechanotransduction, in general, has been reviewed by Liu et al., with an emphasis on fluorescence resonance energy transfer (FRET). 71
The noninvasive evaluation of inflammation in vivo is in a similar, although slightly more advanced position. Tang and colleagues have published several papers in this area. In 2012, they published a paper regarding the use of a chemiluminescent probe to noninvasively monitor the production of reactive oxygen species, which was directly correlated with the numbers of polymorphonuclear leukocytes around implanted materials. 72 This was followed by the description of a macrophage-specific positron emission tomography imaging probe, involving the conjugation of folic acid to poly(ethylene glycol) and labeling with Ga-68, which was able to quantify the inflammatory response in a murine model. 73
Suri et al. used near-infrared fluorescence molecular probes injected locally around implants to monitor inflammation and infection. 74 Bioluminescence imaging was used by Allen et al. to monitor mesenchymal stem cell numbers within hydrogel constructs, 75 with similar studies being reported by Bago et al. 76 and Vila et al. 77 In vivo imaging of the inflammasome (although with respect to viral infection rather than biomaterials) has been undertaken by using an in vivo probe to follow activation within macrophages and subsequent cell death and release of extracellular apoptosis-associated speck-like proteins. 78
Functionality
The ultimate marker of the success of a tissue-engineering procedure is the functional incorporation of the tissue or organ into the host. The degree of incorporation in any animal model may be determined at the end of the test by pathological means, and it is clearly very important that all relevant tools, including immunohistochemistry 79 and microCT, 80 are used. It is equally important that analyses are performed rigorously and quantitatively wherever possible: With immunohistochemistry, quantitative image analysis techniques have been available for some time, 81 but only infrequently used.
The functionality evaluation of tissue-engineering processes will clearly be dependent on the specific intended function. Imaging techniques have been proposed and investigated for some time. The challenges here have been reviewed by Appel et al. 82 The modalities potentially available include ultrasound, optical, photoacoustic, magnetic resonance, X-ray, and nuclear imaging; the authors state that optical imaging and ultrasound/photoacoustic methods are better for in vitro monitoring, whereas MRI, X-ray, and nuclear imaging show more promise for in vivo applications due to the spatial resolution and imaging depth capabilities they offer.
In most situations so far published, the emphasis has been on the quality of the tissue generated, along with the tracking of the cells responsible for that generation. For example, Hegenmuller et al. used microCT to monitor and quantify bone-like tissue generated in silk fibroin scaffolds in culture. 83 Leferink et al. used label-free MRI to assess tissue growth in human bone marrow stromal cells seeded in 3D polymer scaffolds, developing a new image processing method to overcome the limitation of inhomogeneous background intensity. 84 These latter two examples were aimed at the characterization of bone tissue quality during and after bioreactor culture before implantation.
In the vascular space, Gurjarpadhye et al. have used optical coherence tomography to characterize the development of bioengineered blood vessels, based on a biodegradable polymer and seeded mesenchymal stem cells, in a bioreactor. 85 Di Corato et al. used MRI dual cell imaging for tissue-engineered vessels, labeling both endothelial cells and mesenchymal stem cells with gadolinium and iron oxide nanoparticles, under both in vitro and in vivo conditions. 86 Harrington et al. also used serial MRI techniques for both in vitro and in vivo assessment of tissue-engineered vascular grafts 87 ; this work is particularly important since it was able to show how seeded cells may be rapidly lost from scaffolds once the construct is implanted.
Functionality is more clearly determined where there are electrophysiological or behavioral outputs, for example in spinal cord injury treatments. Electrophysiological measurements, including patch clamp techniques, may be made when either central nervous system cells (such as hippocampal cells) or peripheral nerve system cells (e.g., dorsal root ganglion cells) are cultured within biomaterial templates. 88 In animal models of spinal cord injury, several methodologies are available to assess recovery, with the most widely used being the Basso-Beattie-Bresnahan functional scoring system for rats.89,90 Such tests will usually be performed over a period of time, and the results will be correlated with histological findings postmortem. With tissue-engineering approaches in the bladder and urinary tract, there are several urodynamic parameters to assess function, including contraction, elasticity, compliance, and urinary bladder motor activity. 91
An Algorithm for Tissue-Engineering Evaluation
Taking the earlier points into account, it should be possible to construct an algorithm for the procedures of tissue-engineering products and processes, particularly with reference to the biomaterials and templates used.
The guiding principles are as follows:
• Tissue-engineering products should not be evaluated as if they were combination products since their performance is determined by the synergistic activity between components as well as the individual characteristics of those components. • The biomaterials used in tissue-engineering templates should not be tested in the same way as those used in medical devices since the intended modes of action are so different; it is preferable that these templates are not described and considered as medical devices in regulatory guidelines and rules. • The algorithm, shown in Figure 1, represents a pathway from the quasi-design freeze of the product through to comprehensive large animal model evaluation of biocompatibility, functionality, and incorporation into the host. • It is recommended that the ISO 10993 series of tests for biological safety should not be used for the evaluation of tissue-engineering biomaterials since they are not relevant and are prone to deliver results of acceptability that are contrary to the mechanisms, and requirements, of tissue engineering. • Instead, a major emphasis should be placed on the rigorous chemical characterization of the materials (and any time-dependent changes in chemistry) and a thorough literature review of the biological properties of any component identified during this process. • Confirmation of the lack of any evidence of potential adverse effects with any components, together with the absence of any evidence of potential mechanisms of adverse reactions, should allow complete in vitro/ex vivo characterization of template performance, including degradation, mechanotransduction effects, and tissue matrix expression. • From this point onward, all experiments and tests should be performed under conditions that are appropriate for both final product/process development and regulatory approval, especially with due consideration of GLP. • Small animal models (including immunodeficient rodents) should be used for the study of specific mechanisms associated with the template performance and tissue development, with the product and process replicating as far as possible the intended use. • Large animal models should be used for the final preclinical tests. Again, the product and process should replicate the intended clinical use. The model used should be appropriate for the tissue or organ system being targeted, with ovine and canine models being suitable for most applications. Nonhuman primates should be considered for procedures in central circulatory and nervous systems. These large animal models should, as far as techniques allow, monitor in real time all relevant biocompatibility and functional parameters, as well as provide full postmortem analyses. • The data derived from the large animal models should be suitable for evaluation of fitness for purpose in limited first-in-man experiences under regulatory authority guidance.
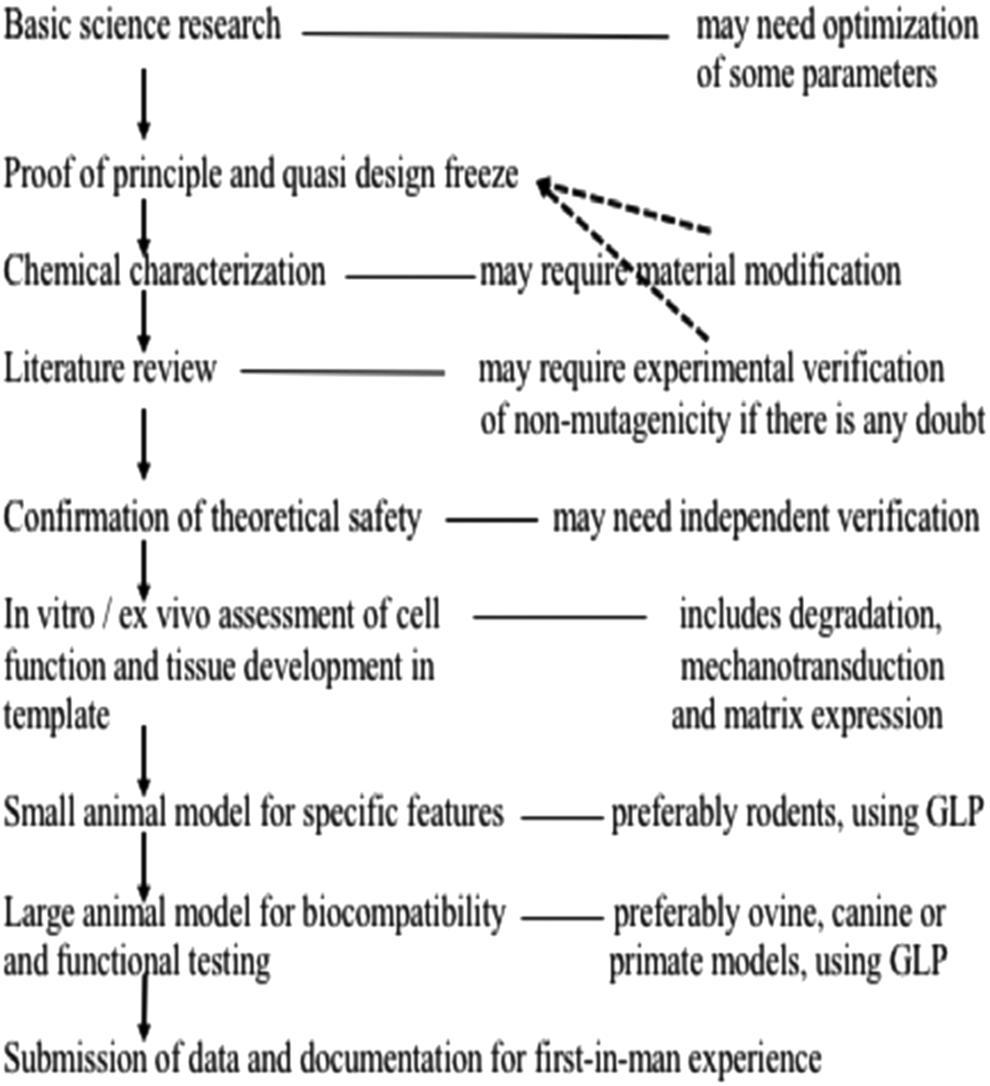
A proposed algorithm for the process of tissue-engineering product development, testing, and assessment.
Conclusions
This article has shown that existing procedures for the evaluation of tissue-engineering processes are not suitable for this purpose. It is concluded that an algorithm for the complete process, from product characterization to large animal model demonstration of biocompatibility and functionality, should be used for both product development and regulatory purposes. Central to these arguments are the need to avoid ISO 10993 biological safety tests, the need to perform complete biomaterial characterization and assess risks through literature analyses, and the need to develop further the techniques for the real-time monitoring of the biocompatibility and functionality of tissue-engineering constructs in appropriate large animal models.
Footnotes
Disclosure Statement
No competing financial interests exist.